
Energy and Protein Requirements Robert Kushner, MD Northwestern University Feinberg School of...
37
Energy and Protein Energy and Protein Requirements Requirements Robert Kushner, MD orthwestern University Feinberg School of Medicine [email protected]
-
Upload
cory-hudson -
Category
Documents
-
view
221 -
download
0
Transcript of Energy and Protein Requirements Robert Kushner, MD Northwestern University Feinberg School of...

Energy and Protein Energy and Protein RequirementsRequirements
Robert Kushner, MDNorthwestern University Feinberg School of Medicine

Starvation and Starvation and Protein-Energy Malnutrition:Protein-Energy Malnutrition:
Importance of Lean Body MassImportance of Lean Body MassHealth 100%
Decreased muscle mass: skeletal, cardiac
Decreased visceral proteins: albumin
Impaired immune response
Impaired wound healing
Impaired organ function
Nitrogen Death 70%
LEAN BODY MASSLEAN BODY MASS

Starvation and Starvation and Protein-Energy Malnutrition:Protein-Energy Malnutrition:
Clinical ImplicationsClinical Implications
Fatigue, general weakness
Lack of initiative
Bedridden
Apathy
Complete Exhaustion
Decreasedmuscle mass
Impaired wound healing
Decreased visceral proteins
Organ failure
10 weeks5 weeks
“Normal”“Catabolic Patients”

Acceleration of Malnutrition Acceleration of Malnutrition due to Metabolic Stressdue to Metabolic Stress
• Energy expenditure is increased• tachycardia, fever, increased RMR
• Catabolism of muscle occurs due to increased protein needs– stress hormones stimulated
– cytokines released• weakness, loss of muscle tissue, increased
urinary urea nitrogen

Mediators of the Mediators of the Metabolic ResponseMetabolic Response
• Cytokines– IL-1, IL-6, TNF-
• Glucagon, Epinephrine, Norepinephrine• Corticosteroids• Eicosanoids
– Leukotrienes, Thromboxanes
• Growth Factors– IGF-1

“Fuels” Energy substrates• Free fatty acids
– Triglycerides• Diet• Adipose tissue
• Glucose– Starches and sugars
• Diet• Glycogen
• Amino acids– Protein
• Diet• Tissue

Energy Reserves of a 70 kg man, Energy Reserves of a 70 kg man, expressed in kcalexpressed in kcal
Adipose tissue135,000
Protein*24,000
Liver glycogen280
Muscle glycogen480
*Body protein, which can readily beconverted to glucose, is not stored for anyreason, since all proteins are functional
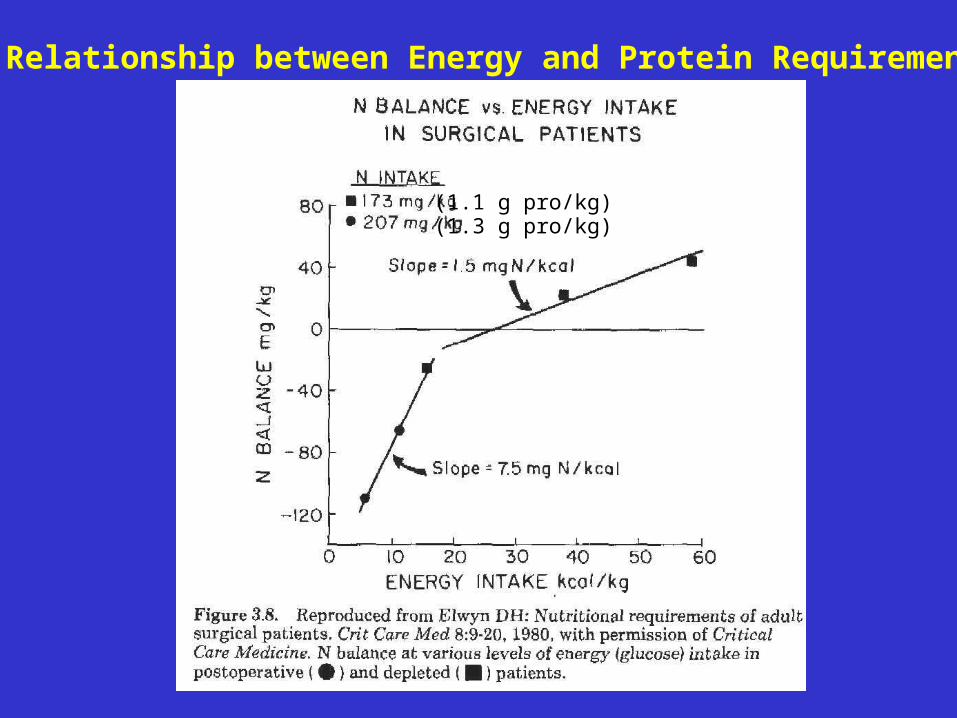
Relationship between Energy and Protein Requirements
(1.3 g pro/kg)(1.1 g pro/kg)

Nitrogen equilibrium attained is at near-energy equilibrium
Slope = 1.4 mg of N/kcal

Components of Total Daily Energy Expenditure
RMRTEF
ET
NEAT
PA
RMR=resting metabolic rate; TEF=thermic effect of feeding;ET=exercise thermogenesis; NEAT=non-exercise thermogenesis

How Do we Estimate or Measure our Patient’s Energy
Requirements?• Total energy expenditure = RMR + TEF + PA• 3 common methods used:
– Estimate RMR, then use a stress and PA multiplier
– Measure RMR, then use a PA multiplier
– Use a simple estimate for all patients
RMRTEF
PA

Estimating RMR• Harris Benedict, 1919
– Men: RMR = 66.5 + (13.8 x weight) + (5 x height) – (6.8 x age)
– Women: RMR = 655.1 + (9.6 x weight) + (1.8 x height) – (4.7 x age)
• Mifflin-St. Jeor, 1990– Men: RMR = (10 x weight) + (6.26 x height) – (5 x age)
+ 5– Women: RMR = (10 x weight) + (6.26 x height) – (5 x
age) – 161
• Institutes of Medicine (IOM)• World Health Organization (WHO)

Estimating a Stress Factor


Energy Expenditure in Hospitalized Patients
• 1256 patients in 19 studies– Postoperative (28%)
– Trauma or sepsis (26%)
– Cancer (18%)
– Pulmonary disease (9%)
– **Excluded individuals with fever (11%/C), burns (140% to 150%), and head injuries (120% to 145%)
• Mean stress (SD) factor was 113% (10.9) above predicted by Harris Benedict equation
Miles JM. Mayo Clin Proc 2006;81:809

Fuel + O2
CO2 +
H2OADP
ATP
Reality: multiple steps with multiple intermediates, but this net reaction.
Pot
enti
al e
nerg
y
Captured energy (40%)
Lost as heat
Principles of Indirect Calorimetry
Metabolic Coupling

Principles of Indirect Calorimetry


V02


Assumptions of Indirect Calorimetry
• The gaseous input and exhaust products from the metabolic combustion process (O2 and CO2) pass only through the nose and mouth– Chest tubes, air leaks
• O2 input is fixed and constant– Nasal cannula, ventilator changes
• All nutrients are metabolized to the end products of CO2, H2O and urea– Renal failure, diabetic ketoacidosis
• Other causes of altered respiration, e.g., metabolic alkalosis and acidosis, hyper- and hypoventilation, oxygen debt, are not present
• Protein is assumed to contribute 12.5% of caloric expenditure (Weir equation)– Excessive protein breakdown, high protein diet

Estimated Energy Estimated Energy RequirementsRequirements
Resting state 20-30 kcal/kg d
Uncomplicated postoperative
25-35 kcal/kg d
Nutritionally depleted 30-40 kcal/ kg d
Hypermetabolic (trauma, sepsis)
35-40 kcal/ kg d

Changes with age of mean energy and protein requirements
Millward, D. J. J. Nutr. 2004;134:1588S-1596S

Protein RequirementFeeding High Quality
Protein
-8
-7
-6
-5
-4
-3
-2
-1
0
1
0 0.2 0.4 0.6 0.8 1
Protein Intake, gm/ kg/ d
Nit
rogen B
ala
nce
, unit
s
AverageRequirement

Protein Requirements
• Estimated Average Requirement (EAR) = 105 mg N/kg/d or 0.66 g/kg/d
• Recommended Dietary Allowance (RDA) = – x 2 SD (97.5% of population) – 0.66 x (1 + 2 x 0.125) = 0.80 g/kg/d
• 70 kg male = 56 g/d• 55 kg female = 46 g/d

Usually measured as nitrogen
1 g N = 6.25 g Protein


168 g pro (2.5 g/kg)
70 g pro (1.1 g/kg)

N Balance is Dependent on More than Energy

Measuring Protein (Nitrogen) Balance
• N balance evaluates adequacy of protein intake relative to need
• N metabolism is dependent on both energy and protein intake + adequate minerals
• N balance (g/d) = (protein intake/6.25) – (urinary nitrogen [mostly urea] + fecal losses + obligatory losses)
• Clinically, measure total urinary urea N (UUN) + 2-4 g for non-urea losses


Estimating Nitrogen Losses

Non-urea nitrogen losses(open abdomen)
*Traditional method of estimating N balance = N intake – (24 hr UUN + 4)
Cheatham et al. Crit Care Med 2007;35:127

Effect of Disease and Traumaon Protein Requirements
0
0.5
1
1.5
2
2.5
Normal
Infe
ctio
n
Pancr
eatit
isBurn
Mul
titra
uma
Hepat
itis
Encephal
opathy
Acute
Ren
al
Chronic
Ren
al
g/k
g
(with
out d
ialysis
)
(with
dia
lysis
)

Estimated Protein Estimated Protein RequirementsRequirements
Resting state 0.8-1.0 g/kg d
Uncomplicated postoperative
1.0-1.3 g/kg d
Depleted patients 1.3-1.7 g/kg d
Hypermetabolic (trauma, sepsis)
1.5-2.0 g/kg d

Conclusion
• Adequate energy and protein must be provided to prevent auto-cannibalism, progressive malnutrition and poor clinical outcomes
• Energy and protein balance are inter-related
• Requirements should be estimated and/or measured for each patient


















