
Endovascular therapy using mechanical thrombectomy devices ... · Endovascular therapy using...
22
Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 1/22 [] 1 2 3 4 Endovascular therapy using mechanical thrombectomy devices for acute ischaemic 5 stroke 6 Project ID: WP5-SB-16 7 8 Project description and planning 9 10 Health Information Quality Authority (HIQA), Ireland 11 Interdisciplinary Centre for HTA and Public Health (IZPH), Germany 12 13 14 15 16
Transcript of Endovascular therapy using mechanical thrombectomy devices ... · Endovascular therapy using...

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 1/22
[]
1
2
3
4
Endovascular therapy using mechanical thrombectomy devices for acute ischaemic 5
stroke 6
Project ID: WP5-SB-16 7
8
Project description and planning 9
10
Health Information Quality Authority (HIQA), Ireland 11
Interdisciplinary Centre for HTA and Public Health (IZPH), Germany 12
13
14
15
16

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 2/22
Contents: 17
18
A. VERSION LOG ......................................................................................................................................................................................................... 3 19
B. PROJECT PLAN ..................................................................................................................................................................................................... 4 20
1.0 PARTICIPANTS .................................................................................................................................................................................................................. 4 21
1.1 PROJECT STAKEHOLDERS............................................................................................................................................................................................ 4 22
2.0 PROJECT INTRODUCTION/ RATIONALE ..................................................................................................................................................................... 5 23
3.0 PROJECT SCOPE AND OBJECTIVES ........................................................................................................................................................................... 5 24
4.0 PROJECT APPROACH AND METHOD .......................................................................................................................................................................... 8 25
5.0 ORGANISATION OF THE WORK .................................................................................................................................................................................. 18 26
5.1 MILESTONES AND DELIVERABLE(S) ......................................................................................................................................................................... 18 27
5.2 MEETINGS ......................................................................................................................................................................................................................... 18 28
6.0 COMMUNICATION ........................................................................................................................................................................................................... 19 29
6.1 DISSEMINATION PLAN ................................................................................................................................................................................................... 19 30
7.0 COLLABORATION WITH STAKEHOLDERS ............................................................................................................................................................... 19 31
8.0 COLLABORATION WITH EUnetHTA WPs ................................................................................................................................................................... 20 32
9.0 RESOURCE PLANNING ................................................................................................................................................................................................. 20 33
9.1 HUMAN RESOURCES ..................................................................................................................................................................................................... 20 34
10.0 CONFLICT OF INTEREST MANAGEMENT .............................................................................................................................................................. 20 35
11.0 EXPECTED OUTCOME(S) ........................................................................................................................................................................................... 20 36
C. REFERENCES ....................................................................................................................................................................................................... 21 37
38
39
Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 3/22
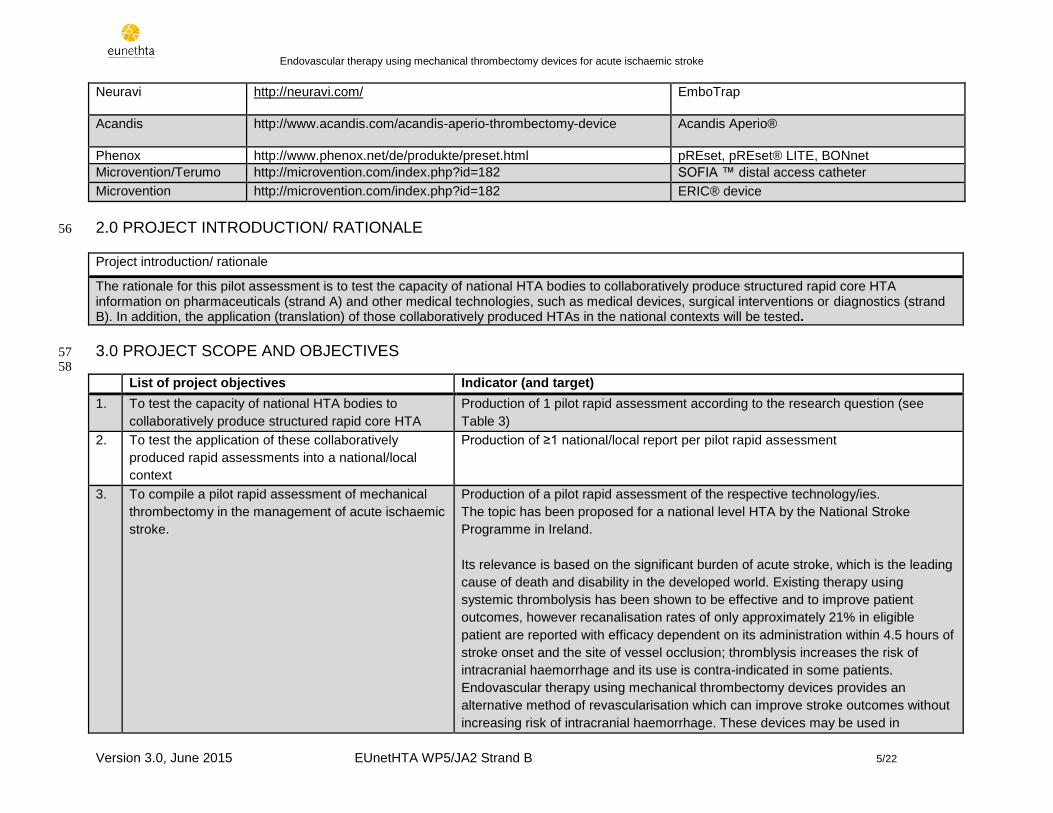
A. VERSION LOG 40
41 Each (significant) modification should be marked with a new version number (Vx). Minor modifications may be marked within versions (Vx.y). Each 42
new version to be communicated with the project team. 43
44
Version number
Date Name (Initials) Modification Reason for the modification
V1 05/05/15 PH, RG First version of a proposed draft project plan.
V2 05/27/15 PH V2 of draft plan Amended subsequent to scoping meeting with manufacturers and discussions with co-authors
V3 06/08/15 PH V3 of draft project plan Amended subsequent to comments of dedicated reviewers
V4 DD/MM/YY
V5 DD/MM/YY
45

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 4/22
B. PROJECT PLAN 46
47
48
1.0 PARTICIPANTS 49
50
Table 1. Project participants 51
# Agency Role in the project Country
1. Health Information Quality Authority (HIQA) Author(s) Ireland
2. Interdisciplinary Centre for HTA and Public Health University of Erlangen-Nürnberg (IZPH)
Co-Author(s) Germany
3. Ludwig Boltzmann Institute for HTA (LBI HTA)
Reviewer Austria
4. HTA and Health Services Research, Public Health and Quality Improvement, Central Denmark Region (CFK)
Reviewer Denmark
5. Haute Autorité de Santé (HAS)
Reviewer France
6. A. Gemelli Hospital Reviewer Italy
7. Health Improvement Scotland (HIS) Reviewer Scotland
8. Royal College of Surgeons in Ireland Beaumont Hospital
External Reviewer(s) Ireland
9.. Ludwig Boltzmann Institute for HTA (LBI HTA) Project Coordination Austria
52
1.1 PROJECT STAKEHOLDERS 53
54
Table 2. Project stakeholders (manufacturers) 55
Organisation Contact (webpage) Devices
Stryker Neurovascular / Concentric Medical
http://concentric-medical.com/ http://www.stryker.com/emea/Products/NeurovascularIntervention/TrevoXPProVueRetreiver/index.htm
Trevo® ProVue™ Retrieval System Merci Retrieval System
Covidien/ Medtronic
http://www.ev3.net/neuro/intl/flow-restoration/solitaire-fr-revascularization-device.htm
Solitaire™ FR Revascularization Device MindFrame CaptureTM LP System
Codman Neuro/ DePuy Synthes/ J&J
http://www.depuysynthes.com/hcp/codman-neuro/products/qs/revive-pv
REVIVE™ SE Thrombectomy Device
Balt Extrusion
http://www.balt.fr/technologie http://www.abmedica.org/productcategory/thrombektomie-aspiration/
Catch Vasco+35ASPI
Penumbra
http://www.penumbrainc.com/neuro Penumbra System®/ACE™ (Penumbra 3D Separator)
Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 5/22
Neuravi
http://neuravi.com/
EmboTrap
Acandis
http://www.acandis.com/acandis-aperio-thrombectomy-device Acandis Aperio®
Phenox http://www.phenox.net/de/produkte/preset.html pREset, pREset® LITE, BONnet
Microvention/Terumo http://microvention.com/index.php?id=182 SOFIA ™ distal access catheter
Microvention http://microvention.com/index.php?id=182 ERIC® device
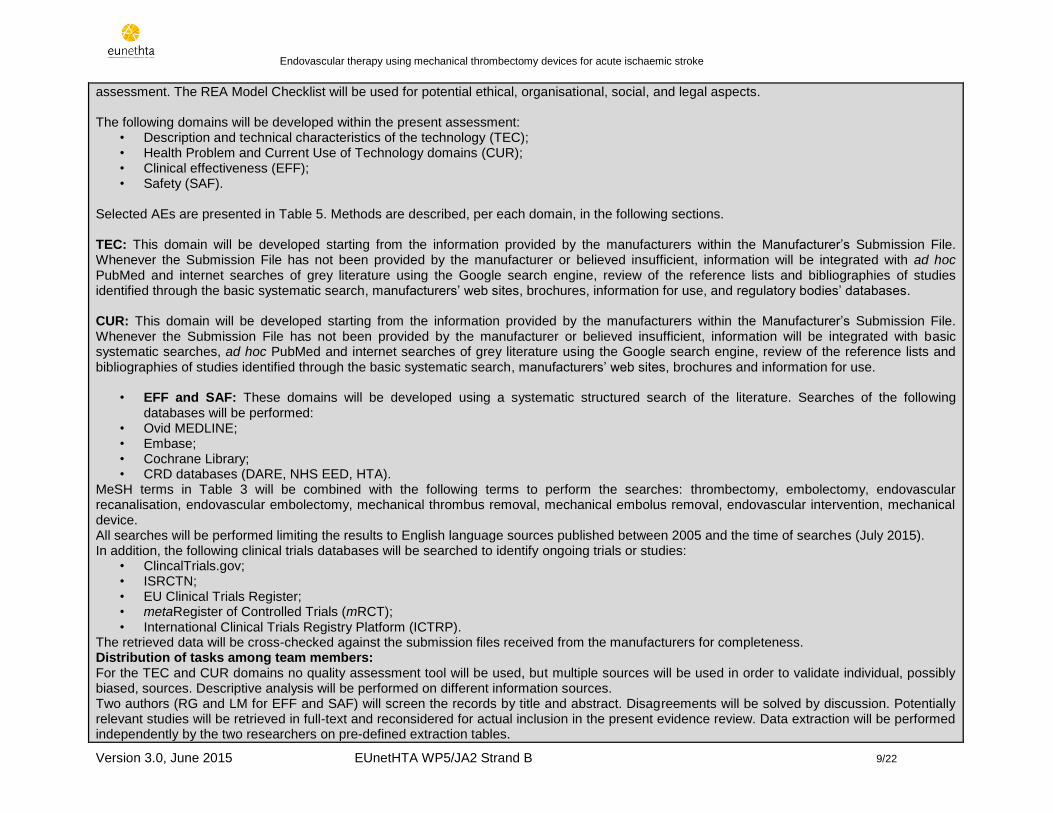
2.0 PROJECT INTRODUCTION/ RATIONALE 56
Project introduction/ rationale
The rationale for this pilot assessment is to test the capacity of national HTA bodies to collaboratively produce structured rapid core HTA information on pharmaceuticals (strand A) and other medical technologies, such as medical devices, surgical interventions or diagnostics (strand B). In addition, the application (translation) of those collaboratively produced HTAs in the national contexts will be tested.
3.0 PROJECT SCOPE AND OBJECTIVES 57 58
List of project objectives Indicator (and target)
1. To test the capacity of national HTA bodies to
collaboratively produce structured rapid core HTA
Production of 1 pilot rapid assessment according to the research question (see
Table 3)
2. To test the application of these collaboratively
produced rapid assessments into a national/local
context
Production of ≥1 national/local report per pilot rapid assessment
3. To compile a pilot rapid assessment of mechanical
thrombectomy in the management of acute ischaemic
stroke.
Production of a pilot rapid assessment of the respective technology/ies.
The topic has been proposed for a national level HTA by the National Stroke
Programme in Ireland.
Its relevance is based on the significant burden of acute stroke, which is the leading
cause of death and disability in the developed world. Existing therapy using
systemic thrombolysis has been shown to be effective and to improve patient
outcomes, however recanalisation rates of only approximately 21% in eligible
patient are reported with efficacy dependent on its administration within 4.5 hours of
stroke onset and the site of vessel occlusion; thromblysis increases the risk of
intracranial haemorrhage and its use is contra-indicated in some patients.
Endovascular therapy using mechanical thrombectomy devices provides an
alternative method of revascularisation which can improve stroke outcomes without
increasing risk of intracranial haemorrhage. These devices may be used in

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 6/22
combination with thrombolysis (as part of standard of care), or as an alternative in
those who are not candidates for thrombolysis or in whom thrombolysis appears to
have failed. However, appropriate patient selection is necessary and the
intervention must be delivered in a timely fashion by trained interventionalists in
facitlities with the capacity for appropriate acute post-procedure care.
59
This pilot rapid assessment addresses the research question whether mechanical thrombectomy plus current standard of care (that may include 60
intravenous and/or intraarterial thrombolysis where appropriate) is more effective and/or safer than current standard of care in acute ischaemic 61
stroke. 62 63 Table 3. Project Scope: PICO 64
Description Project scope
Population
Adults aged 18 years or older with acute ischaemic stroke in the anterior and/or posterior region. ICD-10: I63 MeSH: Stroke
Intervention
Mechanical thrombectomy plus standard of care. (Mechanical thrombectomy may be used in combination with intravenous (and/or intra-arterial) thrombolysis or as an alternative to it in patients experiencing an acute ischaemic stroke who are not candidates for thrombolysis or in whom thrombolysis appears to have failed.) Fourteen CE-marked devices will be considered in this assessment: Aspiration/Suction Devices
Vasco+35ASPI
Penumbra System®/ACE™ (Penumbra 3D Separator)
Sofia™ Distal Access Catheter Stent Retrievers
Trevo® ProVue™ Retrieval System
Solitaire™ FR Revascularization Device
MindFrame CaptureTM LP System
REVIVE™ SE Thrombectomy Device
Catch
EmboTrap
Acandis Aperio®

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 7/22
pREset® LITE
BONnet
ERIC® Clot Retrievers
Merci Retrieval System MeSH-terms: Endovascular procedures; Stents; Tissue Plasminogen Activator; Angioplasty, Balloon
Comparison
Standard of care (which may include intravenous and/or intra-arterial thrombolysis where appropriate). Comparators have been chosen based on CE Mark specific indications, information in published clinical guidelines for treatment of acute ischaemic stroke and EUnetHTA guidelines.
Outcomes
Effectiveness:
Primary outcomes:
o Modified Rankin Score (mRS) at 90 days
o Mortality from ischaemic stroke
Secondary outcomes:
o NIHSS score change at 24 hours
o Barthel Index at 90 days
o Reperfusion at 24 hours
o Revascularisation at final angiography (TICI score)
o Health-related quality of life (EQ5D)
o All-cause mortality
Safety:
Cerebral haemorrhage (symptomatic and asymptomatic) according to the ECAS III trial definition)
Perforation/dissection
Other haemorrhage
New ischaemic stroke in a different vascular territory
New ischaemic stroke in the same vascular territory
Any device-related adverse events
Any procedure-related adverse events Outcomes have been selected based on the recommendations from the clinical guidelines (ESO guidelines) and the EUnetHTA Guidelines on Clinical and Surrogate Endpoints and Safety.

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 8/22
Study design
Effectiveness:
Primary studies o Randomised controlled trials o Prospective clinical controlled studies
Secondary studies o Systematic reviews o Health Technology Assessment (HTA) reports
Safety:
Systematic reviews
Health Technology Assessment (HTA) reports
Prospective clinical studies
Medical device adverse event registers
65
66
4.0 PROJECT APPROACH AND METHOD 67
68
Table 4a. Project approach and method 69
Project approach and method
Distribution of tasks among agencies: As Author, HIQA will:
• Have a leading role in both scoping and production of the pilot; • Be responsible for management of the completed scientific work; • Have ultimate responsibility for quality assurance; • Answer comments.
As Co-authors, the Centre for HTA and Public Health (IZPH) will: • Be responsible for supporting the author in all project phases; • Be responsible for writing TEC and CUR domains independently; • Answer comments.
As Dedicated reviewers, A Gemelli, CFK, HAS, HIS and LBI-HTA, will: • Guarantee quality assurance by thoroughly reviewing the project plan and the assessment drafts; • Review methods, results, and conclusions based on the original studies included; • Provide constructive comments in all the project phases.
Selection of Assessment Elements (AEs) and development of domains A preliminary working version of the HTA Core Model® for Rapid Relative Effectiveness Assessment, based on the “HTA Core Model® for Rapid Relative Effectiveness Assessment of Pharmaceuticals 3.0”, will be the primary source for selecting the assessment elements (AEs). Additionally, assessment elements from other EUnetHTA Core Model Applications will be screened and included if believed relevant to the present
Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 9/22
assessment. The REA Model Checklist will be used for potential ethical, organisational, social, and legal aspects. The following domains will be developed within the present assessment:
• Description and technical characteristics of the technology (TEC); • Health Problem and Current Use of Technology domains (CUR); • Clinical effectiveness (EFF); • Safety (SAF).
Selected AEs are presented in Table 5. Methods are described, per each domain, in the following sections. TEC: This domain will be developed starting from the information provided by the manufacturers within the Manufacturer’s Submission File. Whenever the Submission File has not been provided by the manufacturer or believed insufficient, information will be integrated with ad hoc PubMed and internet searches of grey literature using the Google search engine, review of the reference lists and bibliographies of studies identified through the basic systematic search, manufacturers’ web sites, brochures, information for use, and regulatory bodies’ databases. CUR: This domain will be developed starting from the information provided by the manufacturers within the Manufacturer’s Submission File. Whenever the Submission File has not been provided by the manufacturer or believed insufficient, information will be integrated with basic systematic searches, ad hoc PubMed and internet searches of grey literature using the Google search engine, review of the reference lists and bibliographies of studies identified through the basic systematic search, manufacturers’ web sites, brochures and information for use.
• EFF and SAF: These domains will be developed using a systematic structured search of the literature. Searches of the following databases will be performed:
• Ovid MEDLINE; • Embase; • Cochrane Library; • CRD databases (DARE, NHS EED, HTA).
MeSH terms in Table 3 will be combined with the following terms to perform the searches: thrombectomy, embolectomy, endovascular recanalisation, endovascular embolectomy, mechanical thrombus removal, mechanical embolus removal, endovascular intervention, mechanical device. All searches will be performed limiting the results to English language sources published between 2005 and the time of searches (July 2015). In addition, the following clinical trials databases will be searched to identify ongoing trials or studies:
• ClincalTrials.gov; • ISRCTN; • EU Clinical Trials Register; • metaRegister of Controlled Trials (mRCT); • International Clinical Trials Registry Platform (ICTRP).
The retrieved data will be cross-checked against the submission files received from the manufacturers for completeness. Distribution of tasks among team members: For the TEC and CUR domains no quality assessment tool will be used, but multiple sources will be used in order to validate individual, possibly biased, sources. Descriptive analysis will be performed on different information sources. Two authors (RG and LM for EFF and SAF) will screen the records by title and abstract. Disagreements will be solved by discussion. Potentially relevant studies will be retrieved in full-text and reconsidered for actual inclusion in the present evidence review. Data extraction will be performed independently by the two researchers on pre-defined extraction tables.

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 10/22
Methodological quality of systematic reviews will be based on the ROBIS (Risk of Bias in Systematic Reviews) tool. The methodological quality of RCTs and CCTs will be assessed using the Cochrane risk of bias tables and EUnetHTA Guidelines. The GRADE approach will be used to qualitatively summarise the results from the EFF and SAF domains. Quantitative results based on an intention-to-treat principle will be expressed as point estimates together with associated 95% confidence intervals (95% CI) and exact p-values. Pooled analysis of treatment effect using forest plots and standard meta-analytic techniques will be carried out provided sufficient study data are obtained and taking account of heterogeneity between studies. An assessment of the heterogeneity of included studies will be performed. The I
2 statistic will be examined to
describe the proportion of the variability in the results that reflects real differences in effect size. Chi-squared test for heterogeneity will be performed; if significant heterogeneity is detected, possible explanations will be investigated. The clinical heterogeneity of the populations in included studies will also be assessed. Asymmetry of the funnel plot based on the data for the primary outcome will be taken as an indication of publication bias. Studies will also be assessed to ensure all proposed outcomes in the methods section are reported in the results section to exclude selective outcome reporting. Outcomes specified in the methods that are omitted from the results will be taken as evidence that outcomes were selectively reported. If this occurs the authors of the paper will be contacted to enquire if the results are reported elsewhere. If data permit, subgroup analysis will be performed for the following: 1) Device type 2) Age <80 years vs ≥ 80 years 3) NIHSS score at baseline 2-15, 16-19, or ≥20 4) Time to treatment and reperfusion 5) Use of image-guided patient selection. These subgroups have been identified a-priori based on a plausible rationale. The number of subgroups is kept to a minimum and priority is given to subgroups that are of specific interest to the potential addition of mechanical thrombectomy to standard medical care in the management of acute ischaemic stroke.
70
71
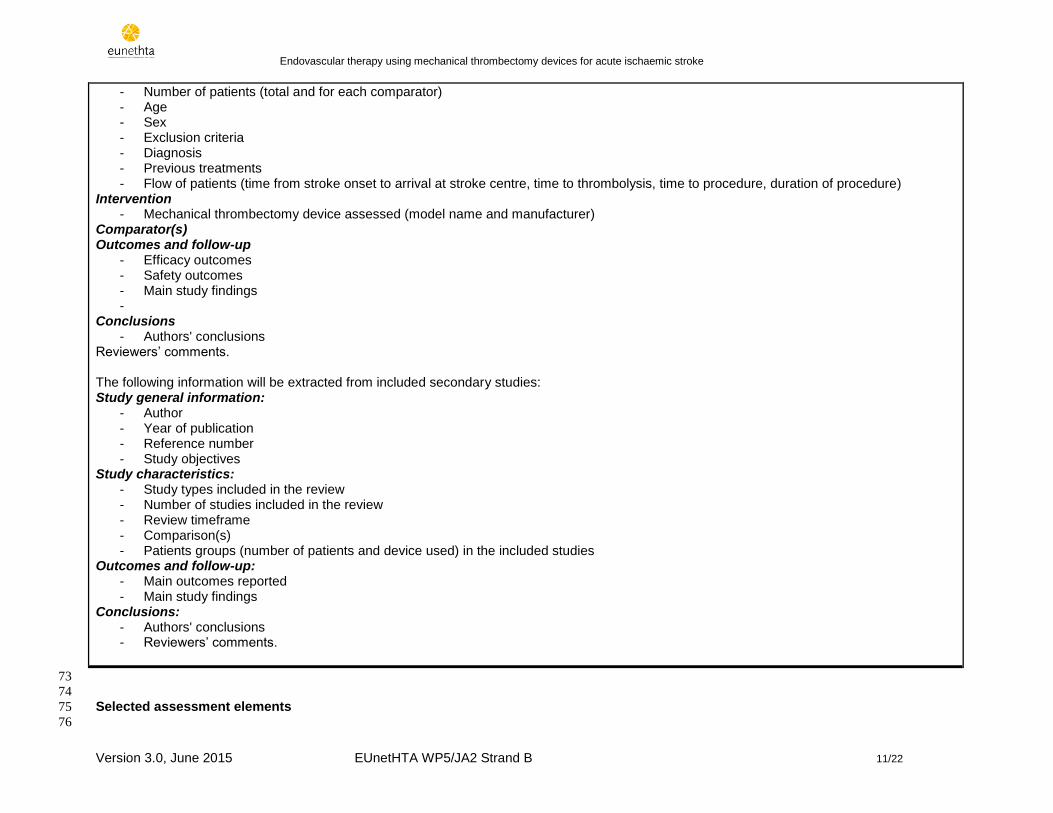
Table 4b. Preliminary Evidence 72
Preliminary evidence table The following information will be extracted from included primary studies: Study general information:
- Author - Year of publication - Reference number - Objectives
Study characteristics: - Study design - allocation concealment (and method), randomisation (and method), blinding (outcome, assessors), intention-to-treat
analysis - Study Registration number (Registry identifier) - Country(ies) of recruitment - Sponsor - Study duration (study start and completion date)
Patients groups:
Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 11/22
- Number of patients (total and for each comparator) - Age - Sex - Exclusion criteria - Diagnosis - Previous treatments - Flow of patients (time from stroke onset to arrival at stroke centre, time to thrombolysis, time to procedure, duration of procedure)
Intervention - Mechanical thrombectomy device assessed (model name and manufacturer)
Comparator(s) Outcomes and follow-up
- Efficacy outcomes - Safety outcomes - Main study findings -
Conclusions - Authors' conclusions
Reviewers’ comments. The following information will be extracted from included secondary studies: Study general information:
- Author - Year of publication - Reference number - Study objectives
Study characteristics: - Study types included in the review - Number of studies included in the review - Review timeframe - Comparison(s) - Patients groups (number of patients and device used) in the included studies
Outcomes and follow-up: - Main outcomes reported - Main study findings
Conclusions: - Authors' conclusions - Reviewers’ comments.
73
74
Selected assessment elements 75
76
Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 12/22
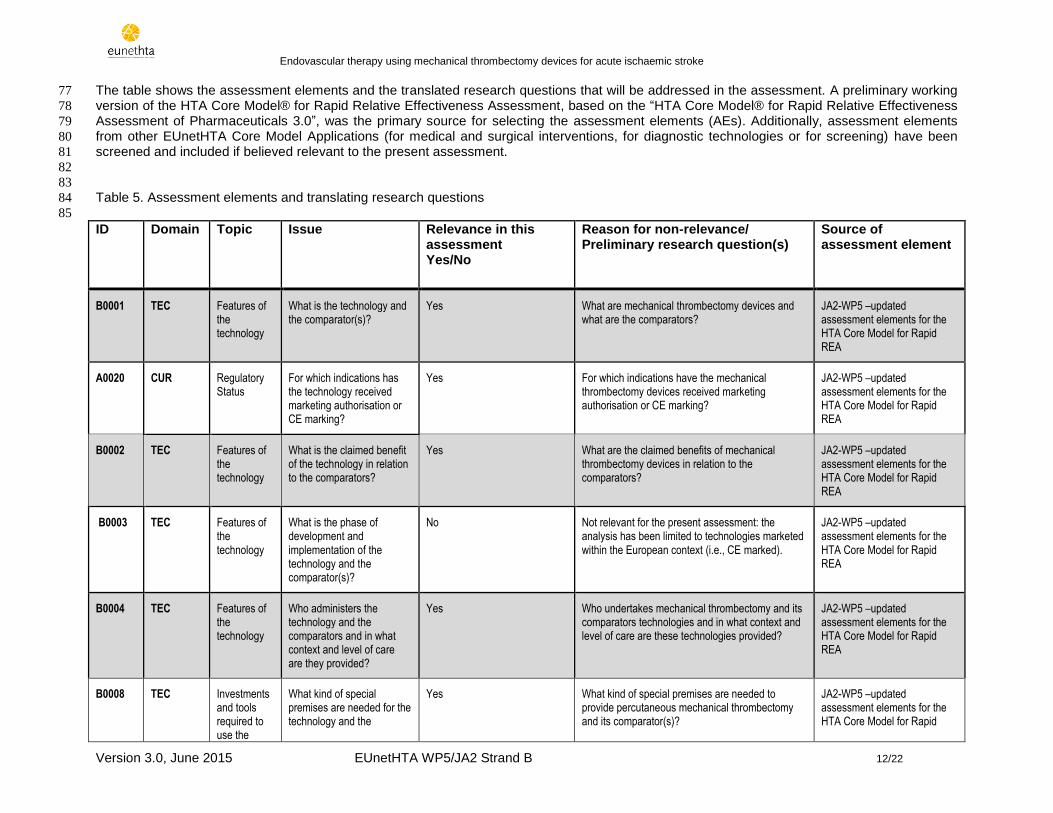
The table shows the assessment elements and the translated research questions that will be addressed in the assessment. A preliminary working 77
version of the HTA Core Model® for Rapid Relative Effectiveness Assessment, based on the “HTA Core Model® for Rapid Relative Effectiveness 78
Assessment of Pharmaceuticals 3.0”, was the primary source for selecting the assessment elements (AEs). Additionally, assessment elements 79
from other EUnetHTA Core Model Applications (for medical and surgical interventions, for diagnostic technologies or for screening) have been 80
screened and included if believed relevant to the present assessment. 81
82
83
Table 5. Assessment elements and translating research questions 84
85
ID Domain Topic Issue Relevance in this assessment Yes/No
Reason for non-relevance/ Preliminary research question(s)
Source of assessment element
B0001 TEC Features of the technology
What is the technology and the comparator(s)?
Yes What are mechanical thrombectomy devices and what are the comparators?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
A0020 CUR Regulatory Status
For which indications has the technology received marketing authorisation or CE marking?
Yes For which indications have the mechanical thrombectomy devices received marketing authorisation or CE marking?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
B0002 TEC Features of the technology
What is the claimed benefit of the technology in relation to the comparators?
Yes What are the claimed benefits of mechanical thrombectomy devices in relation to the comparators?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
B0003 TEC Features of the technology
What is the phase of development and implementation of the technology and the comparator(s)?
No Not relevant for the present assessment: the analysis has been limited to technologies marketed within the European context (i.e., CE marked).
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
B0004 TEC Features of the technology
Who administers the technology and the comparators and in what context and level of care are they provided?
Yes Who undertakes mechanical thrombectomy and its comparators technologies and in what context and level of care are these technologies provided?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
B0008 TEC Investments and tools required to use the
What kind of special premises are needed for the technology and the
Yes What kind of special premises are needed to provide percutaneous mechanical thrombectomy and its comparator(s)?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 13/22
technology comparator (s)? REA
B0009 TEC Investments and tools required to use the technology
What supplies are needed for the technology and the comparator(s)?
Yes What supplies are needed to undertake mechanical thrombectomy and the comparators?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
A0021 CUR Regulatory Status
What is the reimbursement status of the technology?
Yes What is the reimbursement status of mechanical thrombectomy devices?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
A0001 CUR Utilisation For which health conditions, and for what purposes is the technology used?
No The AE may have overlaps with A0020 and B0002. JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
A0002 CUR Target Condition
What is the disease or health condition in the scope of this assessment?
Yes What is the health condition in the scope of this assessment?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
A0003 CUR Target Condition
What are the known risk factors for the disease or health condition?
Yes What are the known risk factors for developing an acute ischaemic stroke?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
A0004 CUR Target Condition
What is the natural course of the disease or health condition?
Yes What is the natural course of acute ischaemic stroke?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
A0005 CUR Target Condition
What are the symptoms and the burden of disease or health condition for the patient?
Yes What are the symptoms and the burden of acute ischaemic stroke for the patient?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
A0006 CUR Target Condition
What are the consequences of the disease or health condition for the society?
Yes What are the consequences of acute ischaemic stroke for society?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
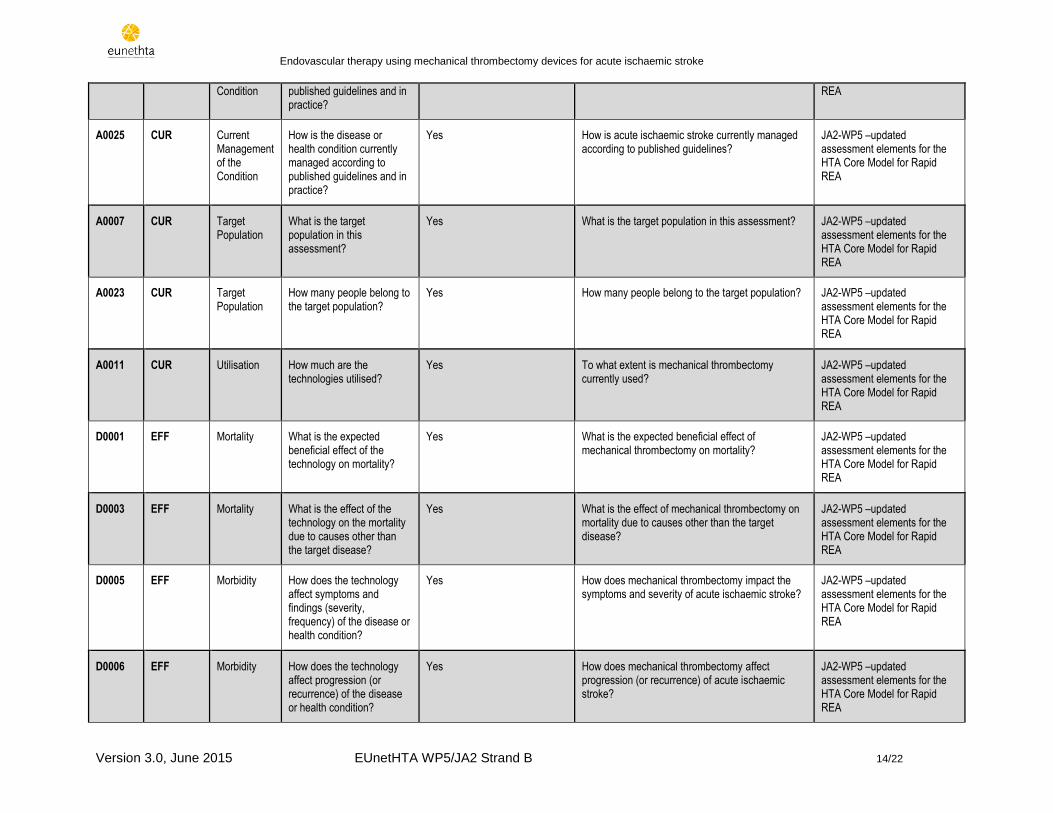
A0024 CUR Current Management of the
How is the disease or health condition currently diagnosed according to
Yes How is acute ischaemic stroke currently diagnosed according to published guidelines?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid
Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 14/22
Condition published guidelines and in practice?
REA
A0025 CUR Current Management of the Condition
How is the disease or health condition currently managed according to published guidelines and in practice?
Yes How is acute ischaemic stroke currently managed according to published guidelines?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
A0007 CUR Target Population
What is the target population in this assessment?
Yes What is the target population in this assessment? JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
A0023 CUR Target Population
How many people belong to the target population?
Yes How many people belong to the target population? JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
A0011 CUR Utilisation How much are the technologies utilised?
Yes To what extent is mechanical thrombectomy currently used?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
D0001 EFF Mortality What is the expected beneficial effect of the technology on mortality?
Yes What is the expected beneficial effect of mechanical thrombectomy on mortality?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
D0003 EFF Mortality What is the effect of the technology on the mortality due to causes other than the target disease?
Yes What is the effect of mechanical thrombectomy on mortality due to causes other than the target disease?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
D0005 EFF Morbidity How does the technology affect symptoms and findings (severity, frequency) of the disease or health condition?
Yes How does mechanical thrombectomy impact the symptoms and severity of acute ischaemic stroke?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
D0006 EFF Morbidity How does the technology affect progression (or recurrence) of the disease or health condition?
Yes How does mechanical thrombectomy affect progression (or recurrence) of acute ischaemic stroke?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 15/22
D0011 EFF Function What is the effect of the technology on patients’ body functions?
Yes What is the effect of mechanical thrombectomy on patients’ body functions?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
D0016 EFF Function
How does the use of the technology affect activities of daily living?
Yes How does the use of mechanical thrombectomy affect activities of daily living?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
D0012 EFF Health-related quality of life
What is the effect of the technology on generic health-related quality of life?
Yes What is the effect of mechanical thrombectomy on generic health-related quality of life?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
D0013 EFF Health-related quality of life
What is the effect of the technology on disease-specific quality of life?
Yes What is the effect of mechanical thrombectomyon disease-specific quality of life?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
D0017 EFF Patient satisfaction
Was the use of the technology worthwhile?
Yes Was the use of mechanical thrombectomy worthwhile?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
C0008 SAF Patient safety
How safe is the technology in relation to the comparator(s)?
Yes Relative to current standard of care alone, how safe is mechanical thrombectomy (technology- and procedure-related adverse events) when used in combination with standard of care relative to standard of care? Specifically:
What is the frequency of serious adverse events (SAE)?
What are the most serious adverse events (SAE)?
What is the frequency of serious adverse events (SAE) leading to death?
What are the most frequent adverse events?
How frequently do they occur?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
C0002 SAF Patient safety
Are the harms related to dosage or frequency of applying the technology?
No Not applicable for the technology under assessment.
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 16/22
C0004 SAF Patient safety
How does the frequency or severity of harms change over time or in different settings?
Yes What are the variables associated with the use of mechanical thrombectomy devices that may impact the frequency and/or severity of harms?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
C0005 SAF Patient safety
What are the susceptible patient groups that are more likely to be harmed through the use of the technology?
Yes Which patient groups are more likely to be harmed by the use of mechanical thrombectomy devices? Are there any relevant contra-indications or interactions with other technologies?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
C0007 SAF Patient safety
Are the technology and comparator(s) associated with user-dependent harms?
Yes – May overlap with C0002 Are mechanical thrombectomy devices associated with user-dependent harms? Specifically, are there potential harms that can be caused by those that undertake mechanical thrombectomy? Is there a learning curve, or potential for intra- or inter-observer variation in interpretation of outcomes, errors or other user-dependent concerns in the quality of care
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
B0010 TEC Investments and tools required to use the technology
What kind of data/records and/or registry is needed to monitor the use of the technology and the comparator?
Yes What kind of data and/or registry is needed to monitor the use of mechanical thrombectomy devices?
JA2-WP5 –updated assessment elements for the HTA Core Model for Rapid REA
86
87
Checklist for potential ethical, organisational, social and legal aspects 88
89
The following checklist should be considered in order to determine whether there are specific ethical, organisational, social and legal aspects 90
which also need to be addressed. Since the assessment is comparative in nature, only new issues should be dealt with, which arise from a 91
difference between the technology to be assessed and its major comparator(s). Already known problems/issues with regard to ethical, 92
organisational, social and legal aspects which are common to the technology to be assessed and its comparator(s) will, as a rule, not be 93
addressed, as it is not to be expected that the addition of a new technology will lead to changes. 94
If a question is answered with ‘yes’, further analysis of these issues may be warranted. If they are answered with no, the domains need not be 95
dealt with further. 96
97
Table 6. Checklist for potential ethical, organisational, social and legal aspects. 98
99
1. Ethical
1.1. Does the introduction of the new technology and its potential use/nonuse instead of the defined, existing comparator(s) No

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 17/22
give rise to any new ethical issues?
1.2. Does comparing the new technology to the defined, existing comparators point to any differences which may be
ethically relevant?
No
2. Organisational
2.1. Does the introduction of the new technology and its potential use/nonuse instead of the defined, existing comparators
require organisational changes?
Yes
2.2. Does comparing the new technology to the defined, existing comparators point to any differences which may be
organisationally relevant?
Yes
Endovascular stoke therapy has major implications for stroke services and for triaging decisions by emergency medical services. Ideally, this procedure should be undertaken within six to eight hours of stroke onset in comprehensive stroke centres by trained interventional (neuro)radiologists. Trial data also suggest a requirement for rapid access to neuroimaging to identify eligible patients with large-vessel occlusion. These criteria require substantial stroke-workflow efficiencies and organisation of specialist stroke services that may not be readily available in many regions.
3. Social:
3.1. Does the introduction of the new technology and its potential use/nonuse instead of the defined, existing comparator(s)
give rise to any new social issues?
No
3.2. Does comparing the new technology to the defined, existing comparators point to any differences which may be
socially relevant?
No
4. Legal:
4.1. Does the introduction of the new technology and its potential use/nonuse instead of the defined, existing comparator(s)
give rise to any legal issues?
No
4.2. Does comparing the new technology to the defined, existing comparators point to any differences which may be legally
relevant?
No
100

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 18/22
101
5.0 ORGANISATION OF THE WORK 102
103
5.1 MILESTONES AND DELIVERABLE(S) 104
105
Table 7. Milestones and Deliverables 106
Project duration 03.2015 12.2015
Pilot’s team building 11.03. 07.04
Scoping phase 07.04 24.07
Identification & contact of manufacturer(s) and external clinical experts 07.04 24.04
Contacting SAG/SF for manufacturer identification 08.04 24.04
Draft Project Plan 1st version + e-meeting pilot team 27.4. 11.5.
Scoping (e-)meeting with manufacturers 20th and 21st of May; e-meeting on 27th of May
Consultation of project plan with dedicated reviewers 25.5. 28.5.
Draft Project Plan 2nd
version 29.5. 4.6.
Consultation of draft Project Plan (public consultation including WP5 SAG, SF) 9.6. 29.6.
Final Project Plan 29.6. 3.7.
Completion of Submission file template by manufacturer(s) 6.7. 24.7.
Formulation of questions regarding missing information in submission file 27.7. 31.7.
Clarification of open questions with manufacturers 3.8. 7.8.
Assessment phase 10.8. 14.12
First draft available 10.8. 11.9.
Review by dedicated reviewers 14.9. 22.9.
Second draft available 23.9. 6.10.
Review by ≥ 1 external clinical expert, manufacturer(s), by Strand B members and other potential stakeholders
7.10. 28.10.
Third draft available 29.10. 12.11.
Medical Editing 13.11. 26.11.
Fourth draft available 27.11. 8.12.
Formatting 9.12. 15.12
Final pilot assessment week from 14.12 - 18.12
Local Reports (if applicable) TBD
107
108
5.2 MEETINGS 109
110
An e-meeting will be held with the pilot team, prior to the scoping meeting with the manufacturer(s)t. Either an e-meeting or a face-to-face meeting 111
will be held with the (co-)authors, the coordination team and the manufacturer(s). 112
113

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 19/22
6.0 COMMUNICATION 114
Please define the communication requirements for the project and how information will be distributed to ensure project success. 115
Here’s an example of organisation of communication - please choose and edit those relevant and add other types as needed. 116
In case of several authors and co-authors we urge you to schedule e-meetings in temporal relationship with major milestones (e.g. finalization of 117
project plan). The coordination team will assist in setting up e-meetings. 118
119
Table 8. Communication 120
Communication Type
Description Date Format Participants/ Distribution
Draft Project Plan with timelines
Review of methods and assessment elements chosen, discussion of time-lines
May 2015 E-mail (e-meetings to be planned here - optional)
Author(s), Co-author(s), dedicated reviewers, Coordinating Team
Final Project Plan
Review of methods and assessment elements chosen, discussion of time-lines considering comments from Stakeholder Advisory Group, public, manufacturer
29/06 - 03/07 2015
E-mail (e-meetings to be planned here - optional)
Author(s), Co-author(s), dedicated reviewers, Coordinating Team
First draft of the pilot assessment
To be reviewed by dedicated reviewers
14/09 - 22/09 2015
E-mail (e-meetings to be planned here -optional)
Dedicated reviewers
To discuss comments of dedicated reviewers (optional)
[DD/MM/YYYY] E-Mail (e-meetings to be planned here -optional)
Author(s), co-author(s), dedicated reviewers
Second draft of the pilot assessment
To be consulted with ≥1 clinical expert, WP5 members, manufacturer(s), other potential stakeholders
07/10 - 28/10 2015
E-mail ≥1 clinical expert, WP5 members, manufacturer, other potential stakeholders
Final pilot rapid assessment
Medical editing by external editor
13/11 - 26/11 2015
E-Mail Medical Editor
6.1 DISSEMINATION PLAN 121
The final pilot rapid assessment will be distributed as laid-out in the Work Plan of WP5. 122
7.0 COLLABORATION WITH STAKEHOLDERS 123
A public consultation of the draft Project Plan will be conducted. The draft Project Plan will be made publicly available on the EUnetHTA website 124
for a period of 15 days. The WP5 SAG, the Stakeholder Forum as well as the manufacturers will be invited to comment on the draft Project Plan 125
for this pilot rapid assessment. 126
In addition, the manufacturers will be asked to attend a scoping (e-)meeting with the authors and co-authors and to submit the submission file 127
developed by WP7 SG4. The 2nd draft version of the assessment will be reviewed by external experts, manufacturers and other potential 128
stakeholders. 129

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 20/22
130
Collaboration with other stakeholders 131
If eligible patient representatives are identified, they are planned to be involved in the public consultation of the draft project plan and in the review 132
of the 2nd draft version of the assessment. 133
134
8.0 COLLABORATION WITH EUnetHTA WPs 135
For the individual pilot rapid assessment, no collaboration with other WPs is planned. 136
9.0 RESOURCE PLANNING 137
138
9.1 HUMAN RESOURCES 139
140
Table 9. Human resources 141
Role Total number of person days Source
Staff of participating organisations Subcontracting
Author 60 person days 60 person days -
Co-Author 30 person days 30 person days -
Reviewer 3 person days each 3 person days each -
External reviewer
10 person days - 10 person days
Medical Editor 5 person days - 5 person days
Layout 4 person days - 4 person days
142
143
144
10.0 CONFLICT OF INTEREST MANAGEMENT 145
146
Conflicts of interest will be handled according to EUnetHTA JA2 Conflict of Interest Policy. As conflict of interest may be topic dependent, conflict 147
of interest declarations will be collected from authors and reviewers involved in a specific pilot assessments. Authors and reviewers who declare a 148
conflict of interest will be excluded from parts of, or the whole work under this specific topic. However, they may still be included in other pilots. 149
If external experts are involved in WP5 a conflict of interest declarations will be collected from them regarding the topic. External experts who 150
declare a conflict of interest will be excluded from parts of, or the whole work under this specific topic. However, they may still be included in other 151
pilots. 152
153
11.0 EXPECTED OUTCOME(S) 154
155

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 21/22
Project outcome(s)
The capacity of national HTA bodies to collaboratively produce structured rapid core HTA and the translation into local reports will have been
proven. Redundancies will have been reduced and therefore efficiency gains achieved.
Applicability of the HTA Core Model for rapid REAs to other technologies will have been elicited and the Model accordingly adapted.
156
C. REFERENCES 157
European Stroke Organisation (ESO) Guidelines for the management of Ischaemic Stroke and Transient Ischaemic Attack2008 (updated 2009) 158
159
ESO-Karolinska Stroke Update, ESMINT, ESNR Consensus Statement on mechanical thrombectomy in acute ischaemic stroke November 2014 160
161
Saver JL, Goyal M, Bonafe A, Diener HC, Levy EI, Pereira VM.. SolitaireTM with the Intention for Thrombectomy as Primary Endovascular 162
Treatment for Acute Ischemic Stroke (SWIFT PRIME) trial: protocol for a randomized, controlled, multicenter study comparing the Solitaire 163
revascularization device with IV tPA with IV tPA alone in acute ischemic stroke. Int J Stroke (2015) 164
165
Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, et al. Randomized assessment of rapid endovascular treatment of ischemic 166
stroke. N Engl J Med (2015) 372(11):1019 167
168
Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, et al. A randomized trial of intraarterial treatment for acute 169
ischemic stroke. N Engl J Med (2015) 372(1):11 170
171
Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, et al. Endovascular therapy for ischemic stroke with perfusion-imaging 172
selection. N Engl J Med (2015) 372:1009 173
174
Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, Larrue V, Lees KR, Medeghri Z, Machnig T, Schneider D, von Kummer R, 175
Wahlgren N, Toni D. ECASS Investigators. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008 Sep 176
25;359(13):1317–29 177
178

Endovascular therapy using mechanical thrombectomy devices for acute ischaemic stroke
Version 3.0, June 2015 EUnetHTA WP5/JA2 Strand B 22/22
179
180


















