Endoscopic tattoo of the colon Endoscopic Tattoo of the ... · Endoscopic tattoo of the colon...
4
Romanian Journal of Gastroenterology September 2005 Vol.14 No.3, 245-248 Address for correspondence: Endoscopic Tattoo of the Colon might be Standardized to Locate Tumors Intraoperatively Nail Aboosy 1 , Chris J.J. Mulder 1 , Frits J. Berends 2 , Jos W.R. Meijer 3 , Adriaan A. V. Sorge 4 1) Gastroenterology, VU Medical Centre, Amsterdam. 2) General Surgery, Rijnstate Hospital. 3) Histopathology, Rijnstate Hospital. 4) Pharmacy, Rijnstate Hospital, Arnhem, The Netherlands Abstract Background. Small colonic lesions which are identified during endoscopy are usually difficult to locate intra- operatively. Endoscopic tattoo of the colon seems the most efficient method, however it does fail in some cases to identify the lesion peroperatively. We studied this method to evaluate its efficacy. Methods. Nineteen patients were tattooed during colonoscopy with “India ink” (drawing ink Rotring ® ). These patients had lesions in which difficulties were anticipated when retracing them again during colorectal surgery. Seventeen patients underwent colonic surgery. One patient underwent laparoscopic polypectomy and the other TEM (Transanal Endoscopic Microsurgery). Results. The visibility of the “India ink” peroperatively and afterwards during histological examination were evaluated. The tattoos were visible in 68.4 % patients intraoperatively. Histopathological macroscopic examination of the specimens showed ink in 73.6 % patients. In 31.5 % patients the tattoo could not be recognised peroperatively. Conclusions. Endoscopy assisted tattooing of the colon has been reported to be a safe method to landmark lesions in the colon. In the majority of our patients the tattoo was obvious during surgery. Endoscopic tattoo seems an efficient technique in identifying small colonic lesions intraoperatively. Key words Colorectal lesions - endoscopic tattoo - laparoscopy - Rotring® ink - budget - standardization - histology - lymph- nodes intraoperator. Tatuarea endoscopicã a colonului pare cea mai eficientã metodã, deºi s-au descris cazuri de eºec al identificãrii leziunilor peroperator. Scopul studiului a fost stabilirea eficacitãþii acestei metode. Material ºi metodã. 19 pacienþi au fost tatuaþi în timpul colonoscopiei cu „cernealã India” (cernealã de desenat Rotring®). Aceºti pacienþi aveau leziuni dificil de localizat în timpul chirurgiei colo-rectale. 17 pacienþi au fost supuºi chirurgiei colorectale. Un pacient a suferit polipectomie endoscopicã ºi un altul MET (Microchirurgie Endoscopicã Transanalã). Rezultate. A fost evaluatã vizibilitatea „cernelei India” peroperator ºi în timpul examinãrii histologice. Tatuajele au fost vizibile la 68,4% pacienþi intraoperator. La 73,6% pacienþi examinarea macroscopicã histopatologicã a mostrelor a arãtat existenþa cernelei. Tatuajele nu au fost recunoscute peroperator la 31,5% pacienþi. Concluzii. Tatuarea endoscopicã a colonului este o metodã sigurã de topografiere a leziunilor colonice. Tatuajul a fost vizibil în timpul intervenþiei la majoritatea pacienþilor. Tatuarea endoscopicã pare o tehnicã eficientã de identificare a leziunilor colonice mici intraoperator. Prof. Dr. C.J.J. Mulder VU University Medical Center Dept. Gastroenterology P.O. Box 7057 1005 MB Amsterdam, The Netherlands E-mail: [email protected] Introduction Precise localization of lesions within the colon is essential in a number of clinical circumstances, particularly when surgical resection is required or the lesion after polypectomy needs to be reinspected at a later date. Landmarking soft colorectal lesions during colonoscopy for surgical recognition during (laparoscopic) operation is a topic for surgeons. The laparoscopist does not have the ability of palpating the colon between the fingers during exploration. Even in conventional surgery, intra-operative localization of small nonpalpable soft tumours or polypectomy sites has been reported to be a difficult problem. There are many different methods to help the surgeon to find these lesions intraoperatively. Most of the methods which have been reported seem insufficient in recognizing the lesions (1). Distance estimation for instance is a method which roughly gives the location of a lesion, due to the distensi- Rezumat Premize. Leziunile mici ale colonului, identificate în timpul endoscopiei, sunt de obicei dificil de localizat
-
Upload
vuongkhanh -
Category
Documents
-
view
244 -
download
4
Transcript of Endoscopic tattoo of the colon Endoscopic Tattoo of the ... · Endoscopic tattoo of the colon...

Endoscopic tattoo of the colon
Romanian Journal of GastroenterologySeptember 2005 Vol.14 No.3, 245-248Address for correspondence:
Endoscopic Tattoo of the Colon might be Standardized
to Locate Tumors Intraoperatively
Nail Aboosy1, Chris J.J. Mulder1, Frits J. Berends2, Jos W.R. Meijer3, Adriaan A. V. Sorge4
1) Gastroenterology, VU Medical Centre, Amsterdam. 2) General Surgery, Rijnstate Hospital.
3) Histopathology, Rijnstate Hospital. 4) Pharmacy, Rijnstate Hospital, Arnhem, The Netherlands
Abstract
Background. Small colonic lesions which are identified
during endoscopy are usually difficult to locate intra-
operatively. Endoscopic tattoo of the colon seems the most
efficient method, however it does fail in some cases to
identify the lesion peroperatively. We studied this method
to evaluate its efficacy. Methods. Nineteen patients were
tattooed during colonoscopy with “India ink” (drawing ink
Rotring ®). These patients had lesions in which difficulties
were anticipated when retracing them again during colorectal
surgery. Seventeen patients underwent colonic surgery. One
patient underwent laparoscopic polypectomy and the other
TEM (Transanal Endoscopic Microsurgery). Results. The
visibility of the “India ink” peroperatively and afterwards
during histological examination were evaluated. The tattoos
were visible in 68.4 % patients intraoperatively.
Histopathological macroscopic examination of the specimens
showed ink in 73.6 % patients. In 31.5 % patients the tattoo
could not be recognised peroperatively. Conclusions.
Endoscopy assisted tattooing of the colon has been reported
to be a safe method to landmark lesions in the colon. In the
majority of our patients the tattoo was obvious during
surgery. Endoscopic tattoo seems an efficient technique in
identifying small colonic lesions intraoperatively.
Key wordsColorectal lesions - endoscopic tattoo - laparoscopy -
Rotring® ink - budget - standardization - histology - lymph-
nodes
intraoperator. Tatuarea endoscopicã a colonului pare cea
mai eficientã metodã, deºi s-au descris cazuri de eºec al
identificãrii leziunilor peroperator. Scopul studiului a fost
stabilirea eficacitãþii acestei metode. Material ºi metodã. 19
pacienþi au fost tatuaþi în timpul colonoscopiei cu „cernealã
India” (cernealã de desenat Rotring®). Aceºti pacienþi aveau
leziuni dificil de localizat în timpul chirurgiei colo-rectale. 17
pacienþi au fost supuºi chirurgiei colorectale. Un pacient a
suferit polipectomie endoscopicã ºi un altul MET
(Microchirurgie Endoscopicã Transanalã). Rezultate. A fost
evaluatã vizibilitatea „cernelei India” peroperator ºi în timpul
examinãrii histologice. Tatuajele au fost vizibile la 68,4%
pacienþi intraoperator. La 73,6% pacienþi examinarea
macroscopicã histopatologicã a mostrelor a arãtat existenþa
cernelei. Tatuajele nu au fost recunoscute peroperator la
31,5% pacienþi. Concluzii. Tatuarea endoscopicã a colonului
este o metodã sigurã de topografiere a leziunilor colonice.
Tatuajul a fost vizibil în timpul intervenþiei la majoritatea
pacienþilor. Tatuarea endoscopicã pare o tehnicã eficientã
de identificare a leziunilor colonice mici intraoperator.
Prof. Dr. C.J.J. MulderVU University Medical CenterDept. GastroenterologyP.O. Box 70571005 MB Amsterdam, The NetherlandsE-mail: [email protected]
Introduction
Precise localization of lesions within the colon is
essential in a number of clinical circumstances, particularly
when surgical resection is required or the lesion after
polypectomy needs to be reinspected at a later date.
Landmarking soft colorectal lesions during colonoscopy
for surgical recognition during (laparoscopic) operation is a
topic for surgeons. The laparoscopist does not have the
ability of palpating the colon between the fingers during
exploration. Even in conventional surgery, intra-operative
localization of small nonpalpable soft tumours or
polypectomy sites has been reported to be a difficult
problem. There are many different methods to help the
surgeon to find these lesions intraoperatively. Most of the
methods which have been reported seem insufficient in
recognizing the lesions (1).
Distance estimation for instance is a method which
roughly gives the location of a lesion, due to the distensi-
Rezumat
Premize. Leziunile mici ale colonului, identificate în
timpul endoscopiei, sunt de obicei dificil de localizat

Aboosy et al246
bility characteristics of the colon and the fact that during
colonoscopy air is inflated which also will lead to distension
of the colon. Another well-known method is peroperative
endoscopy which is time consuming and needs the
attendance of an additional endoscopist. In laparoscopic
surgery, palpation of colonic tumour is impossible and the
location of these tumours must be defined preoperatively.
Large soft lesions are not well palpable.
Colonic tattoo with “India ink” is a method reported in
1975 by Ponsky and King (2). The safety and the efficacy of
this method was reported in other studies (3,4). We evaluated
the efficacy of this method with a low-budget tattoo ink
(Rotring®) in identifying soft colorectal lesions.
Methods
It is our practice to inject a permanent surgical marker
during the initial colonoscopy if a lesion cannot be removed
or if an endoscopically removed polyp has clinical features
that may require surgical resection or surveillance
colonoscopy.
Between September 2001 and March 2003, 19 patients
underwent surgery for small lesions, such as colonic polyps.
During colonoscopy these patients were prospectively
marked with a low budget, easily available “India ink”
(Rotring ®). The “India ink” suspension was first filtered by
a 5 micron filter, then produced in ampulla, sterilised (15
min. 121 °C) and used. The “ink” was not diluted prior to its
submucosal injection of 1 cc proximal or distal of the lesion,
with a sclerosing needle (Cobra Medical®). India ink is a
black drawing ink made with carbon particles. India ink
Results
None of the patients developed fever, abdominal pain or
tenderness after tattooing the colon. The tattoo was visible
in 13 patients (68.4 %) intra-operatively (Table I). During
post-operative examination of the specimens, the tattoo was
visible in 14 (73.6 %) patients macroscopically. The mean
time-interval between injection of the ink and subsequent
operation was 3 weeks (range 1-8 weeks).
In one patient who underwent laparoscopic polypectomy
no “India ink” could be identified at histopathology,
although the tattooing was clearly visible during the
operation near the resected area. This finding could be due
to the fact that the tattooing had been injected distal of the
lesion. In 6 patients (31.5 %) the “India ink” was not
recognised during surgery. The lesion was easily found by
(Rotring ®) is available from any stationary store for drawing-
materials.
Patients were operated for both premalignant and
malignant diseases of the colon and rectum (13
adenocarcinomas, 6 adenomas).
Seventeen patients underwent surgical intervention: 8
low anterior resection, 3 left hemicolectomy, 3 sigmoid
resection, 1 rectosigmoid resection, 1 transverse colon
resection, 1 subtotal colostomy. One patient underwent
laparoscopic polypectomy and another patient a TEM. We
evaluated these patients regarding the visibility and safety
of the tattooing during operation and in histopathological
investigation.
The local ethical committee approved the study.
Table I Visibility of the colonic lesions intra- and post-operatively
Patient Location Pathology Operation Intraoperative Postoperative Comments
histopathological
examination
1 DC ACA LHC visible visible, LNV
2 DC TVA STC visible visible
3 RS ACA LAR visible visible
4 DC ACA LHC not visible visible colon adhesion to spleen
5 RS ADE SIR visible visible
6 RS ACA LAR not visible not visible *
7 RS ADE LAR not visible not visible Intraoperative endoscopy
8 RS ACA LAR visible visible
9 TC ADE LPE visible not visible polypectomy
10 DC ACA LHC not visible visible palpable tumour
11 RE ACA LAR not visible not visible palpable tumour
12 RE ACA TEM not visible not visible tumour obvious during TEM
13 TC ADE TCR visible visible,LNV
14 RS ACA RSR visible visible
15 RS ACA LAR visible visible
16 RS ADE LAR visible visible
17 RS ACA LAR visible visible, LNV
18 RS ACA SIR visible visible, LNV
19 RS ACA SIR visible visible, LNV
DC: descending colon, TC: transverse colon, AC: ascending colon, RE: rectum, RS: rectosigmoid; ACA: adenocarcinoma,
ADE: adenoma; LAR: low anterior resection, LHC: left hemicolectomy, SCD segment resection descending colon, SIR:
sigmoid resection; LPE: laparoscopic polypectomy. TCR: transverse colon resection, RSR: rectosigmoid resection, STC:
subtotal colectomy; Visible: macroscopically visible, LNV: tattoo visible in the lymph nodes
* tumour in the small pelvis, difficult to inspect, bimanually per rectum palpable

Endoscopic tattoo of the colon 247
palpation in two patients. In another patient, the lesion was
difficult to detect, due to the location in the small pelvis.
The fourth patient had a colonic lesion with adhesions to
the spleen, after previous surgery. TEM was performed in a
patient with a rectal lesion and the lesion was obvious. The
tattoo was not reported by the surgeon. In the sixth patient
it was necessary to perform an intraoperative endoscopy in
order to locate the lesion.
In 5 patients there were minimal or no lymph nodes in
the specimens during postoperative examination. In the
remaining 14 patients, the lymph nodes were examined and
the “India ink” particles were microscopically visible in 5 of
the patients (35.7 %). In one patient the tattoo was also
macroscopically visible in the lymph nodes. No signs of
inflammatory reaction, granulomas or other complications
were recognised during surgery.
Pathological examination showed adenocarcinoma in 13
patients. In 6 of them, this was recognised preoperatively
either as premalignant lesion or highly suspected lesion.
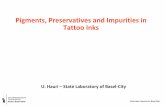
The diameter of the ink particles was approximately 0.1
micron and they were present in the stromal interstitium and
in macrophages especially in the adjacent lymph nodes.
However, no inflammatory reaction was present in the vicinity
of the ink particles (Figs.1,2).
Fig.1 Submucosal deposition of tattoo-particles. Fig.2 Deposition of tattoo-particles in adjacent lymphnodes.
Discussion
Small colorectal lesions are difficult to locate during
colorectal surgery. Endoscopic measurement during
preoperative colonoscopy usually gives a rough estimation.
The colon is a distensible organ and the inflated air together
with the endoscope can lead to misinterpretation easily.
Frager et al (5) reported six patients in whom reliance on
preoperative colonoscopic tumour localisation had led to
errors of the diagnosis and therapy. Three patients required
a relaparotomy because the tumour had been left in place
during the first colorectal surgery.
Intraoperative colonoscopy is a difficult investi-
gation for endoscopists. Poor operative exposure due
to bowel distension is another disadvantage for the
surgeon (1). Endoscopically placed mucosal clips were tried
in the past. However, clips fall off in an average of 10 days,
and laparoscopic recognition therefore seems inadequate
(1).
Laparoscopic clips applied to the serosal surface of the
bowel under the guidance of intraoperative colonoscopy is
less attractive to the surgeon because the clips tend to
dislodge from the serosa (1). Moreover, the clips are too
small to be recognised easily. This method is time consuming

Aboosy et al248
and needs the cooperation of the surgeon and the gastro-
enterologist.
The safety of “India ink” has previously been reported
in several studies. Botoman et al. (6) described the only
case of a clinical complication. A patient underwent snare
biopsy of a sigmoid cancer with cauterisation followed by
“India ink” tattooing of the lesion. However, these findings
could well be attributed to the cauterisation procedure and
not to a possible complication of “India ink” .
Histopathological complications have been reported in
the literature, such as local reactions like fat necrosis with
inflammatory pseudotumour formation, colonic abscess with
localised peritonitis, and chronic inflammation (7-9). In
another study in which “India ink” was used in 195 patients
no complications were recognized (3).
“India ink” is a permanent dye. Ponsky and King who
first described the use of this method, reported a patient in
whom the ink was visible after 22 years.
In our pilot - study with Rotring® India Ink we did not
encounter any clinical or histopathological complications.
Rotring® India Ink is easily available at very low prices (100
cc: • 12,00).
The presence of “India ink” during surgery helped in
targeting lesions in the majority of our patients. Quick
identification during surgery saves time.
In six patients the tattoo in the colon was not visible,
but in five patients the lesion could be detected with other
means, further intraoperative colonoscopy being not
necessary. In one patient it was necessary to perform an
intraoperative colonoscopy in order to retrace the lesion.
Unfortunately, we marked the lesion with a single injection
of 1 cc. A second injection of 1 cc given contralaterally
would have probably allowed to recognize the tattooing.
Since the colonoscopist cannot know which portion of
the bowel is the superior aspect, multiple injections should
be made circumferentially in the wall around a lesion to
prevent a single injection site from being located in a
“sanctuary” site, which is hidden from the eyes of the
surgeon when the abdomen is opened.
Obviously endoscopic tattooing of the colon mucosa
outperforms the other alternatives in identifying a colorectal
lesion (10).
Safety in performance has been reported in many
studies. It is important to sterilise the ink before its use in
order to avoid infection. India ink itself is not conducive for
culture on media (11). The absence of inflammatory reactions
even after 10 years as reported by King et al. is reassuring
(3). We looked very carefully for secondary inflammation
due to ink in the mucosa and lymph nodes but we did not
find any adverse reaction at the histopathological
examination.
Conclusion
Endoscopic tattooing of the colon seems a safe and
effective low-budget method to landmark small lesions in
the colon. In our patients we did not encounter any adverse
reactions to the “India ink” clinically or histopathologically.
In the presented series the tattoo was clearly visible
during surgery in the majority of patients. The use of endo-
scopic tattoo is an essential and efficient technique to help
identifying small lesions intraoperatively, still underused
and undervalued in many hospitals. We recommend the use
of this method as a standard method of marking small lesions
during colonoscopy when a planned colorectal surgical
intervention is anticipated.
Injecting a second shot contralaterally may help in
decreasing the percentage of undetected tattoos during
surgery. The surgeon should be informed whether the
injections are proximal or distal to the lesions.
References
1. Kim SH, Milsom JW, Church JM, Ludwig KA, Garcia-Ruiz A,
Okuda J, Fazio VW. Preoperative tumor localization for
laparoscopic colorectal surgery. Surg Endosc 1997; 11:1013-
106.
2. Ponsky JL, King JF. Endoscopic marking of colonic lesions.
Gastrointest Endosc 1975;22: 42-43.
3. McArthur CS, Roayaie S, Waye JD. Safety of preoperation
endoscopic tattoo with India ink for identification of colonic
lesions. Surg Endosc 1999; 13:397-400
4. Askin MP, Waye JD, Fiedler L, Harpaz N. Tattoo of colonic
neoplasms in 113 patients with a new sterile carbon compound.
Gastrointest Endosc 2002;56:339-342.
5. Frager DH, Frager JD, Wolf EL, Beneventano TC Problems in
the colonoscopic localization of tumors: continued value of
barium enema. Gasterointest Radiol 1987; 12: 343-346.
6. Botoman VA, Pietro M, Thirlby RC. Localization of colonic
lesions with endoscopic tattoo. Dis Colon Rectum 1994;
37:775-776.
7. Coman E, Brandt LJ, Brenner S, Frank M, Sablay B, Bennett B.
Fat necrosis and inflammatory pseudotumour due to endoscopic
tattooing with India ink. Gastrointest Endosc 1991; 37: 65-
68.
8. Park SI, Genta RS, Romeo DP, Weesner RE. Colonic abscess
and focal peritonitis secondary to India ink tattooing of the
colon. Gastrointest Endosc 1991; 37: 68-71
9. Snider TE, Goodell WM, Pulitzer DR. Gastrointestinal tattoos.
Arch Pathol Lab Med 1994; 118: 640-641
10. Lipof T, Bartus C, Sardella W, Johnson K, Vignati P, Cohen J.
Preoperative colonoscopy decreases the need for laparoscopic
management of colonic polyps. Dis Colon Rectum.
2005;48:1076-1080.
11. Nizam R, Siddiqi N, Landas SK, Kaplan DS, Holtzapple PG.
Colonic tattooing with India ink: benefits, risks, and alternatives.
Am J Gastroenterol 1996; 91:1804-1808