Endocrinology Subspecialty Rounds Prudhvi Karumanchi Dr. K. Onyemere 2/26/09.
17
Endocrinology Subspecialty Rounds Prudhvi Karumanchi Dr. K. Onyemere 2/26/09
-
Upload
adrien-ranger -
Category
Documents
-
view
222 -
download
1
Transcript of Endocrinology Subspecialty Rounds Prudhvi Karumanchi Dr. K. Onyemere 2/26/09.

Case
ID: 46 y/o wm CC: Headache x 1 month HPI:
Facial fullness, sinus tenderness and headache x 1 month
Significant worsening of headache x 1 day – Frontal Associated With photophobia 6 episodes of vomiting Swelling and pain in left eye x 1 day

Case.. ROS:
– Positive for fever, chills, vomiting, hearing loss, nasal congestion, productive cough
Home meds: – Keflex 500 mg po QID– Metformin 500 mg po BID– Pravastatin 40 mg po daily– Tylenol Codeine #3 prn
PMH: – COPD– DM-2 (A1c: 7.9%)– Sleep apnea (uses BiPAP)
Social history: – Quit smoking 5 years ago. Used to smoke 1 ppd x 6 yrs– Occasional alcohol
Family history: – DM-2 in both parents. Cancer in maternal grand father.

Case..
Physical Exam: – VS:
T: 100.6 F, P: 76, R: 20, O2: 87% on RA, BP: 140/71– Gen: AOx3, cooperative, fatigued, moderately obese– Head: Atraumatic, sinuses tender to palpation– Eyes: conjunctiva – swollen with hemorrhages. Left eye: Ptosis.
protruded and swollen – Deviated inferiorly and laterally– Lungs: CTA bilaterally– Heart: S1, S2, RRR, no murmur– Abd: Soft, ND, NT, BS+ve, no organomegaly– Extr: no edema, palpable pulses– Neuro: Rt pupil: 3 mm reactive, Left pupil: 5 mm – sluggish
reaction. Afferent pupillary defect

LABS
CBC: – Wbc: 16.3 with N: 71% and L: 21%– Hb: 17.5– Plt: 259
CMP: – Na: 130, K: 3.7, Cl: 97, HCO3: 26, BUN: 8, Cr: 0.6– LFTs: Normal
IMAGING: – CT head: Near complete opacification of the sphenoid
sinuses, mucosal thickening of the ethmoid sinuses and left frontal sinus mucous retention cyst. The globes are intact. No intracranial abnormality.

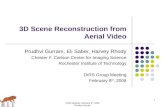
MRI Brain
Hemorrhagic pituitary macroadenoma measuringapproximately 2.3 x 1.8 x 2.4 cm (AP, TR, cc)
Suprasellar component of the mass causes mass effect on optic chiasm
Prominent chronic mucosal disease is present withinsphenoid sinus, which is nearly completely obstructed
Mild mucosal disease is present within ethmoid sinuses bilaterally without significant sinus opacification
MRA brain: Grossly normal study

LABS
Human GH: 0.4 ng/ml (Low - < or = 10) IGF-1 52 ng/mL (86 - 220)
Prolactin: 0.7 ng/dl (2.6 – 13.1 ng/ml)
FSH: 2 mIU/ml (1.3 – 19.3) LH: 0.4 mIU/ml (1.2 – 8.6) Free T4: 0.83 ng/dl (0.61 – 1.12) TSH: 0.48 mcIU/ml (0.4 – 4) Cortisol: 3.3 mcg/dl (5:37 am) (5.0-23.0) 8:00
am Testosterone: < 0.1 (at 5:20 am and 9:20 am)
Normal: 1.75 – 7.81 ng/ml

Pituitary apoplexy
Sudden onset ACTH deficiency Decreased Cortisol At onset, gonadotropin and growth hormone
secretion is decreased. ACTH and TSH deficiency may follow afterwards Rarely, there is isolated TSH deficiency Hence, all hormones need to be tested when
there is clinical suspicion

Cosyntropin stim test
Cosyntropin – Synthetic ACTH 1-24 Healthy person – greatest response in morning Adrenal insufficiency – same response in morning
and afternoon Administer 250 mcg iv bolus 30 – 60 min peak cortisol of 18-20 mcg/dL

Hypogonadism
Decreased FSH and LH – Secondary hypogonadism Inappropriately normal FSH and Low LH with low
testosterone indicate developing sec. hypogonadism Men with hypogonadism
– Testicular hypofunction decreased testosterone– Infertility, decreased energy and libido– Hot flashes is very severe– Decreased bone mineral density
Treatment: – Testosterone replacement if fertility is not desired– Gonadotropins if fertility is desired

Growth hormone deficiency
Clinical features: – Diminished muscle mass and increased fat mass – Increased LDL cholesterol– Decreased bone mineral density – Diminished sense of well being – Increased risk of cardiovascular disease – Increased inflammatory cardiovascular risk markers (IL-6
and C-reactive protein) Diagnosis: Low IGF-1 level Treatment
– known to improve muscle mass and bone mineral density

Pituitary Apoplexy
Risk Factors: – endocrine stimulation tests – bleeding disorders – pregnancy – estrogen therapy – head trauma – pituitary radiation – diabetes – surgery
Diagnosis: MRI scan Treatment:
– High dose corticosteroids– When stable, trans-sphenoidal hypophysectomy– Pituitary and visual functions are restored after surgery– Pts with extensive pituitary necrosis require lifelong hormone
replacement therapy