USING DATABASES AND TECHNOLOGY IN CURRICULUM INTEGRATION Presented by Ivey Carey and Carol Richmond.

© 2016 Integrated Healthcare Association. All rights reserved. 1
Encounter Data ProjectMarch 31, 2017
Presented by Carol Wanke, Sharp HealthCare
© 2016 Integrated Healthcare Association. All rights reserved. 2
• Integrated Healthcare Association (IHA) 501c3 • Convenes diverse stakeholders, including physician
organizations, hospitals and health systems, health plans, purchasers and consumers
• Committed to high-value integrated care that improves quality and affordability for patients across California and the nation.
• Promotes the continuing evolution of integrated health care, supported by financial mechanisms that align the incentives of purchasers, payers, and providers, as the best means to achieve the most positive outcomes for patients and the general public in California
About IHA and Payer/Provider Collaboration
© 2016 Integrated Healthcare Association. All rights reserved. 3
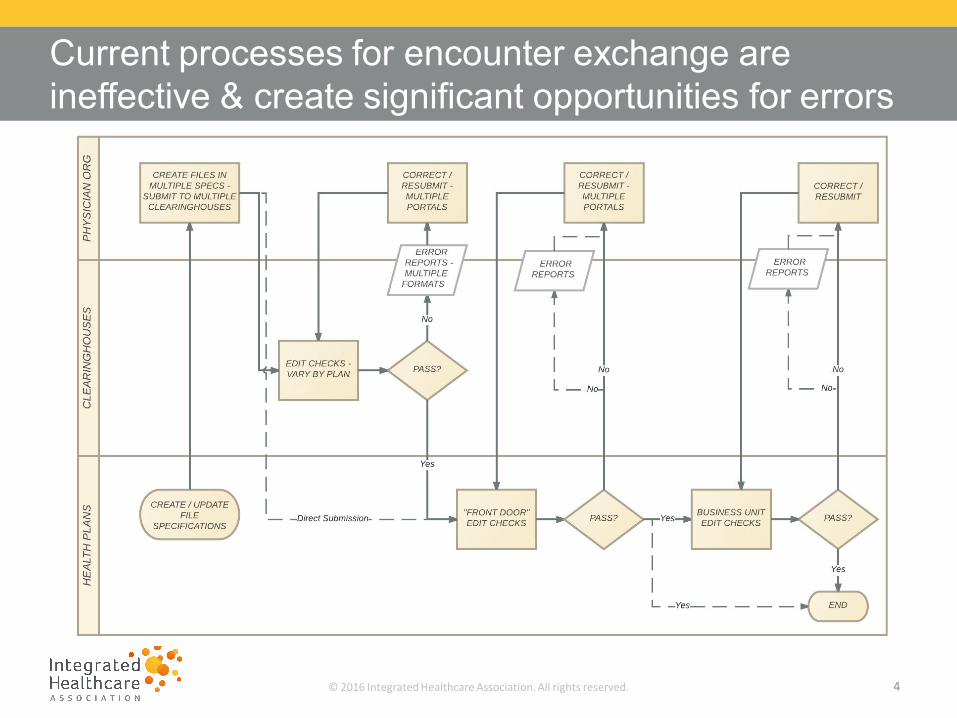
• Few incentives for POs to submit complete, timely, and accurate encounter data vs fee for service
• Multiple handoffs and edit checks between participating organizations
• Lack of standards in all aspects of the encounter data exchange process • Different interpretations of 837 form by plans• Multiple file submission processes (clearinghouse/direct to plan)• Edit checks/acknowledgements vary by plan• Multiple processes for resubmission • No benchmarks for quality and volume
Several barriers exist to the exchange of high quality encounter data
© 2016 Integrated Healthcare Association. All rights reserved. 4
Current processes for encounter exchange are ineffective & create significant opportunities for errors
© 2016 Integrated Healthcare Association. All rights reserved. 5
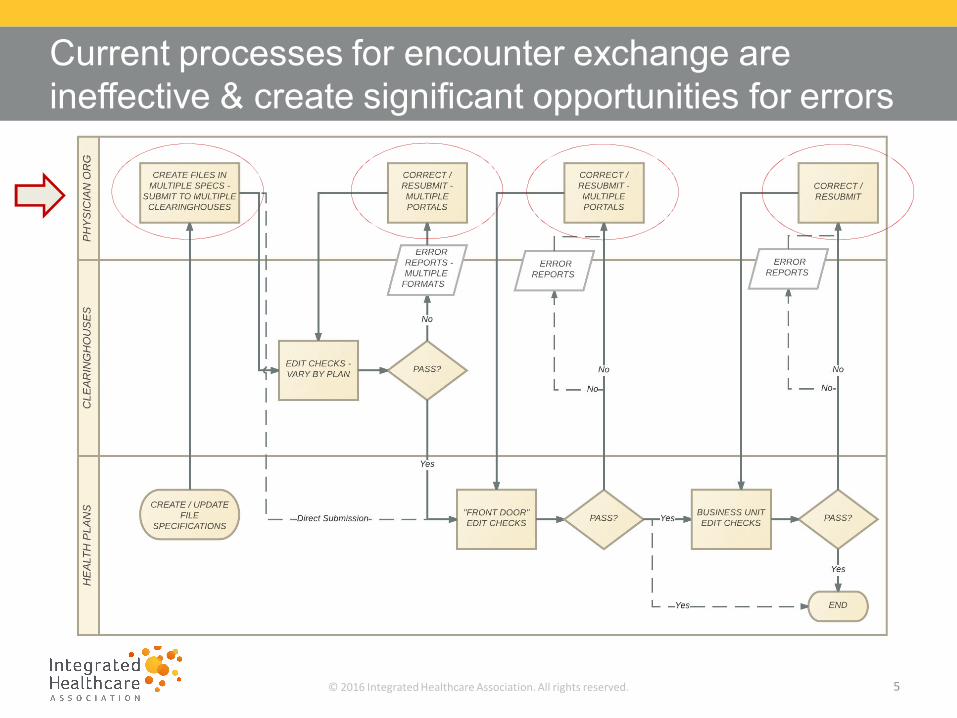
Current processes for encounter exchange are ineffective & create significant opportunities for errors

© 2016 Integrated Healthcare Association. All rights reserved. 6
Current processes for encounter exchange are ineffective & create significant opportunities for errors
Quality? Volume?
© 2016 Integrated Healthcare Association. All rights reserved. 7
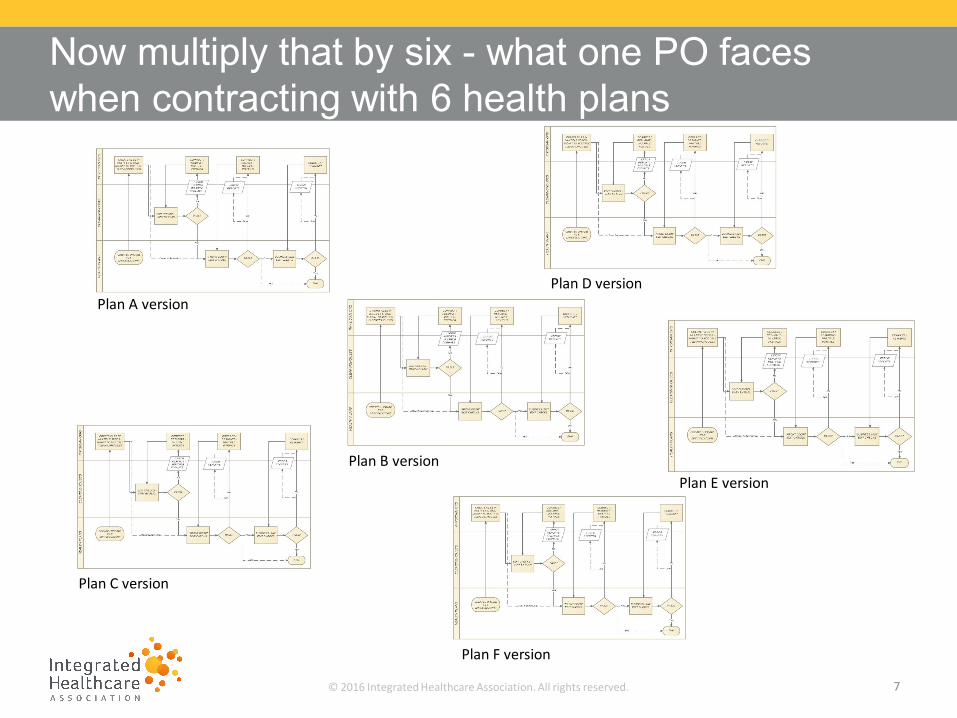
Now multiply that by six - what one PO faces when contracting with 6 health plans
Plan A version
Plan C version
Plan D version
Plan E version
Plan F version
Plan B version

© 2016 Integrated Healthcare Association. All rights reserved. 8
For edits: different processes and formats across plans create operational burden, data gets lost
Front End Edits Back End Edits Excel exporting Option
Payer 277 CA Proprietary Method of Receipt Format Yes
Plan 1 NO YES WEB Combined Yes
Plan 2 NO YES FTP and G-Drive Combined Yes
Plan 3 NO YES FTP and Email Combined Yes
Plan 4 NO YES WEB Combined No
Plan 5 NO YES FTP Combined Yes
Plan 6 YES YES Email Proprietary edit Report Yes
Plan 7 YES YES ENS Separate but behind Yes
Edit process grid by plan:

© 2016 Integrated Healthcare Association. All rights reserved. 9
Work done with a large CA physician organization identified large volumes and variability of edits
-
5,000
10,000
15,000
-
5,000
10,000
15,000
20,000
25,000
22-Nov 11-Jan 2-Mar 21-Apr 10-Jun 30-Jul 18-Sep 7-Nov 27-Dec
2013 edits volume
2014 edits volume
© 2016 Integrated Healthcare Association. All rights reserved. 10
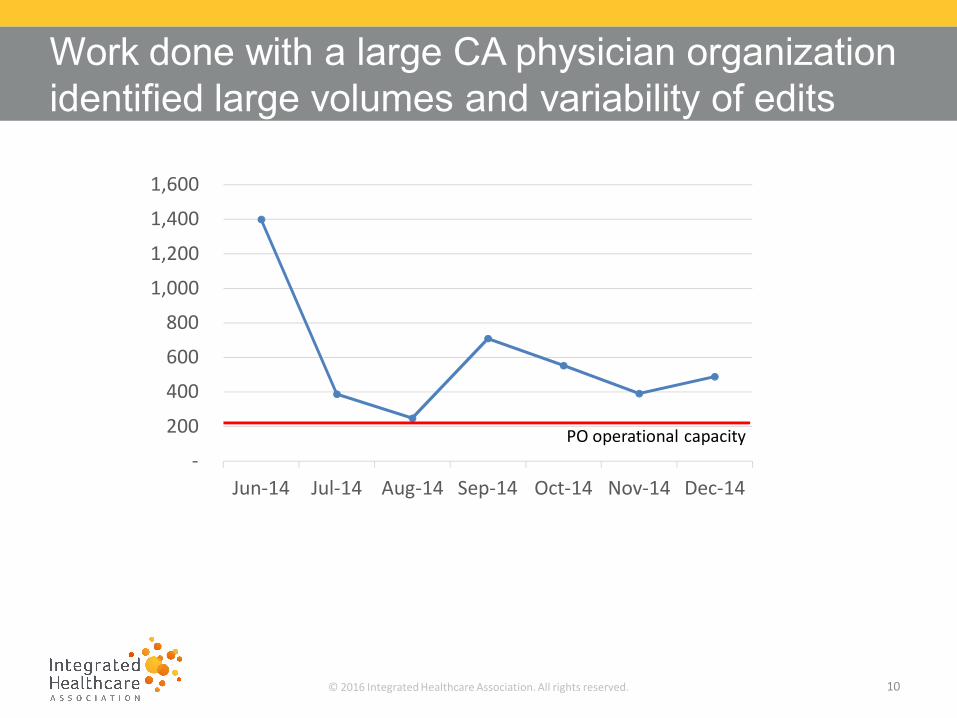
Work done with a large CA physician organization identified large volumes and variability of edits
-
200
400
600
800
1,000
1,200
1,400
1,600
Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14
PO operational capacity

© 2016 Integrated Healthcare Association. All rights reserved. 11
Breaking down PO edits by type will help IHA evaluate potential standard edit/rejection processes
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
1 2 3 4 5 6 7
Edit Types - Monthly Percentage
Eligibility Coding Claim Form Duplicate

© 2016 Integrated Healthcare Association. All rights reserved. 12
Smaller POs - there is more submission variability skewed towards lower volumes
0
5
10
15
20
25
0 10 20 30 40 50 60Thousand member months
Encounter PMPY Vs Member Months
© 2016 Integrated Healthcare Association. All rights reserved. 13
Project Plan

© 2016 Integrated Healthcare Association. All rights reserved. 14
Three main phases for IHA-led end-to-end process standardization project
Physician Groups Plans
Threshold reports
Eligibility reports
Data inquiries
CMSDMHCDHCS
837 form
Edits

© 2016 Integrated Healthcare Association. All rights reserved. 15
Three main phases for IHA-led end-to-end process standardization project
Physician Groups Plans
Threshold reports
Eligibility reports
Data inquiries
CMSDMHCDHCS
837 form
Edits

© 2016 Integrated Healthcare Association. All rights reserved. 16
Three main phases for IHA-led end-to-end process standardization project
Physician Groups Plans
Threshold reports
Eligibility reports
Data inquiries
CMSDMHCDHCS
837 form
Edits

© 2016 Integrated Healthcare Association. All rights reserved. 17
Three main phases for IHA-led end-to-end process standardization project
Physician Groups Plans
Threshold reports
Eligibility reports ASM
CMSDMHCDHCS
837 form
Edits
© 2016 Integrated Healthcare Association. All rights reserved. 18
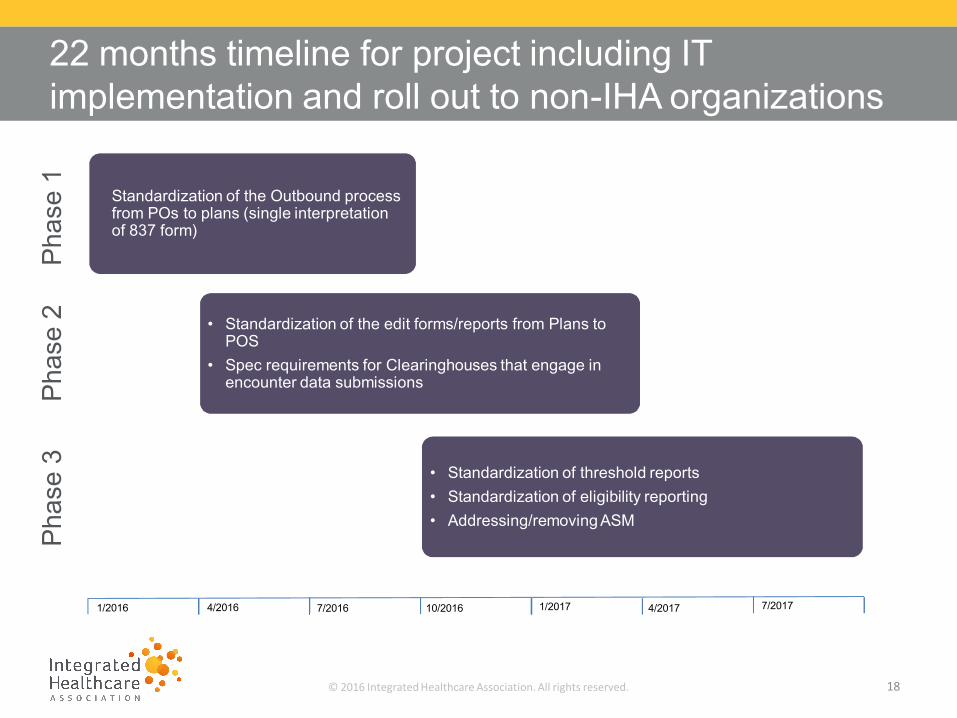
22 months timeline for project including IT implementation and roll out to non-IHA organizations
Phas
e 1
Phas
e 2
Phas
e 3
Standardization of the Outbound process from POs to plans (single interpretation of 837 form)
• Standardization of the edit forms/reports from Plans to POS
• Spec requirements for Clearinghouses that engage in encounter data submissions
• Standardization of threshold reports• Standardization of eligibility reporting• Addressing/removing ASM
1/2016 4/2016 7/2016 10/2016 1/2017 4/2017 7/2017

© 2016 Integrated Healthcare Association. All rights reserved. 19
Project Grid shows alignment on all items discussed in 2016, implementation scheduled for 2017
Aetna AnthemBlue
ShieldCigna
HealthNet
United B&T HCP Hill Monarch Sharp Sutter Dignity Memorial
837 form
Snip level 6 submission
Eligibility processes and logics
277 CA, single
format, front + back
end
Threshold reporting
ASM

© 2016 Integrated Healthcare Association. All rights reserved. 20
• IHA hands off the brainstorming and standardization work to another work group
• ICE Encounter Standardization Team – Industry Collaborative Effort
• Team develops best practices and shares with IHA for broader input and buy in
• Team has developed best practices for:• Encounter Submissions• Newborn Encounter Layout• In process Electronic Misdirected Claim Layout
Collaboration beyond IHA
© 2016 Integrated Healthcare Association. All rights reserved. 21
• Changing long standing claims and encounter workflows• Software is not sufficient to provide data required in an
encounter claim• Payer claims and encounter teams operate in silos• Provider reviewing and working edits• Standardized edit reports• Regulatory agencies have different encounter
requirements
Challenges Remain

© 2016 Integrated Healthcare Association. All rights reserved. 22
Questions

© 2016 Integrated Healthcare Association. All rights reserved. 23
• http://www.iha.org• https://www.iceforhealth.org/home.asp• http://www.iceforhealth.org/library.asp?sf=&cid=392#cid3
92
References