EMR Incorporation: Evaluating the Benefits for Your...
36
EMR Incorporation: Evaluating the Benefits for Your Organization BHM Healthcare Solutions © BHM 2010
Transcript of EMR Incorporation: Evaluating the Benefits for Your...

EMR Incorporation: Evaluating the Benefits
for Your Organization
BHM Healthcare Solutions
© BHM 2010

Learning Objectives
To evaluate the pros and cons of electronic medical records (EMRs), and determine whether or not EMRs make sense for their practice
Summarize the importance of staff buy in and how to customize EMRs for their individual practice
Identify key components for fluidly incorporating EMRs into practice
© BHM 2010

What is an EMR
• An electronic medical record, or EMR, is simply a patient’s
medical record in digital form
• The digital information is typically stored in a database and
is accessible from anywhere via a secure network
• Prior to EMR, a patient’s medical information was typically
kept as a paper record available at each physician’s office
or the hospital a patient has visited
• EMR’s contain mainstream data normally found on a
patient’s medical records. These include blood type, blood
tests, inoculations, and X-rays--patient specific genomic
information may also be included
© BHM 2010

EMR’s and the Political Climate
• Starting with the Economic Stimulus Package in 2009,
financial incentives were offered to hospitals and
physicians who implemented EMR’s according to
meaningful use criteria
• A recent expansion of this bill is allowing for the same
financial incentives to be applied to:
• Behavioral health and mental health professionals and clinics
• Substance abuse professionals and clinics
• Psychiatric hospitals
• Licensed psychologists
• Clinical social workers
• Many experts are soon expecting a federal mandate for
the use of EMR’s
© BHM 2010

Different Levels of EMRs
• There are two different levels of EMRs--“Basic EMR” and
“Fully Functional EMR. Each have unique advantages in
the clinical setting
• Basic EMRs include all of the following information:
• Patient demographic information
• Patient problem lists
• Clinical notes
• Orders for prescriptions
• Viewing laboratory and imaging results
DesRoches CM et al. N Eng J Med. 2008;359(1):50-60.
© BHM 2010

Different Levels of EMRs (cont)
• The fully functional EMR includes all of the components of
the “Basic EMR” as well as the following features:
• Orders for tests
• Prescription and test orders sent electronically
• Warnings of drug interactions or contraindications
• Highlighting of out-of-range test levels
• Electronic images returned
• Reminders for guideline-based interventions
© BHM 2010
DesRoches CM et al. N Eng J Med. 2008;359(1):50-60.

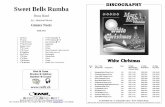
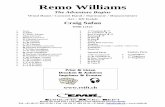
Current EMR Implementation
© BHM 2010
CDC/NCHS. National Ambulatory Medical Care Survey: 2001-preliminary 2009. Available at:
http://www.cdc.gov/nchs/data/hestat/emr_ehr/emr_ehr.htm
Off
ice
-Ba
se
d P
hys
icia
ns
, %

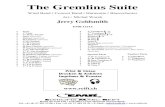
EMR Components
Problem List Diagnostic
Departmental Reports
Images Medications
Laboratory Results
Microbiology Progress
Notes/Narrative Documents
Allergies
Demographics Administrative Transactions
Quality Measures
Privacy and Security
© BHM 2010

Pro: The Benefits of EMR’s
• Minimize errors and aid in standardization of patient health
records
• Ensure safe storage of patient records
• Make health care more cost efficient
• Encourage coordination between health professionals
• Improve the quality of care by increasing the efficiency and
speed of diagnosis, improve the delivery of preventive
health services, and improve adherence to clinical
guidelines
© BHM 2010

Cons: The Drawbacks of EMR’s
• Could constitute threat to
patient privacy
• Can lead to standardized
rather than customized care
• EMRs can be inefficient due
to poor design, or lack of
user knowledge
• EMRs are often not
standardized, which
prevents cross-compatibility
between systems, and
lessens the total benefit of
data sharing
© BHM 2010

Cons: The Drawbacks of EMR’s
(cont)
• EMR’s are not secure, many people are not convinced of
the safety of their personal data when stored on large
servers, and there have been multiple instances of large
health record security breaches which have compromised
thousands of patients
• There is a substantial cost related to the conversion from
paper to electronic records, and those who invest may find
it difficult to qualify for incentives due to the “all or nothing”
meaningful use approach
© BHM 2010

Summing it All Up
• EMR systems offer substantial opportunities to organize
and manage clinical data in ways that can potentially
improve preventive health care, the management of
chronic illness, and the financial health of clinical
practices.
• The functionality of EMRs as implemented, however, can
vary substantially from that envisaged by their designers,
and even from those who purchase the programs.
• Safety, usability, and overall design continue to be barriers
to successful EMR conversion and implementation
© BHM 2010

EMR OPERATIONAL AND
TECHNICAL COMPONENTS
© BHM 2010

Operational Changes
• Organizations will need to review how the EMR system will
change work flow
• Integrations with appointment and billing systems, as well
as staff access will need to be analyzed
• Business processes on finalization of billable services will
need to be reviewed
• Focus on current paper processes to determine what is
staying, what is going and how are you going to implement
into the new system.
© BHM 2010

EMR Technical Issues
• Operations Security
• Management of “Role Specific” security within the EMR software.
Know who can see what information.
• Data Backup – Must have a strong process tested on a regular
basis.
• Disaster Recovery – Understand and develop strong policy and
procedures. Contract specifics for fully hosted system is critical.
Testing of recovery process is imperative.
• Business Continuity Plan - Closely related to a disaster recovery
plan but encompasses every aspect of the business.
© BHM 2010

EMR Technical Issues (cont)
• System security • Web based applications
• Wireless workstations
including work tablets
• Desktop
• EDI exchanges with other
medical vendors
• Data Capture • Not all EMRs are created
equally, you need to
evaluate based on type of
practice, practitioner and
patient volumes.
© BHM 2010

IMPORTANT EMR
CONSIDERATIONS
© BHM 2010

Infrastructure Questions
• It is important to have full working knowledge of the
systems and networks available to the practice including:
• How old is the server, and what are it’s capabilities?
• How often is data backed up?
• Are there redundant systems in place if the server crashes?
• What encryption capacities are in place to ensure privacy?
• Do I have adequate bandwidth to perform daily activities?
• Are hardware upgrades necessary, and what are the associated
costs?
• Who will be responsible for hardware and software maintenance?
© BHM 2010

Training and Support
• Training and support prior to and during implementation
are key to the successfulness of the project. Some
questions to consider may include:
• Is training covered by the vendor, or is it necessary to have an
internal implementation specialist?
• What is your staff’s current knowledge base, and how does it need
to be expanded for successful implementation?
• What will be the time and financial costs of training and support to
your practice?
• How will follow up training and support be handled after
implementation and who will be responsible for associated costs?
© BHM 2010

Clinical Customization
• During the Customization Process the following should be
considered:
• To what extent will we need customization in our practice?
• What are the goals that we are hoping to achieve with EMRs?
• Will the vendor assist with customization, or will this need to occur
in house?
• To what extent will assistance from the vendor be provided, and
what costs are covered relating to customization?
• Will the new program deliver what both clinical staff and
management need, or will compromises need to be made?
• What specific processes will be automated, and which will not?
© BHM 2010

BARRIERS TO EMR
IMPLEMENTATION
© BHM 2010

#1 Hurdle: Staff Buy-In
• According to a recent survey by Health Data Management,
the No. 1 challenge associated with implementation of
EMRs is staff buy-in (28%) followed by systems integration
(27%) and funding (24%)
• According to a study by Korn/Ferry International one of the
most common mistakes that executives make is failing to
read the corporate culture
• In many instances staff buy-in may be contingent upon
information systems working smoothly and seamlessly
with clinical workflows
© BHM 2010
Health Data Management. Critical Success Factors for EMR Implementation. 18 June 2008. Feb 2010
<http://www.healthdatamanagement.com/web_seminars/-26291-1.html>.
Childress John R, Senn Larry E. In the Eye of the Storm: Reengineering Corporate Culture. 2nd Edition.
New York: Executive Excellence Publishing, 2005.

Facilitating Staff Buy In:
Planning is Key
• For most practices, EMRs will constitute a significant
change and proper planning is essential to successful
implementation.
• Planning not only applies to new processes and
procedures to be used, but also pertains to the network
which will be utilized
• A detailed project plan should be outlined with room for
minor tweaks that will need to be made along the way to
best incorporate EMRs into the practice
• The Principles of Change Management (POCM) can be
useful in EMR implementation
© BHM 2010

Principles of Change
Management
Address The Human Side
• Jobs will change, and so
will daily protocol, come
up with a plan to address
these changes and
concerns relating to EMR
implementation
• Facilitate communication
among the staff to
discuss and hear their
opinions and gather
feedback about EMRs
Start at the Top
• It is important for key
staff, and even more
importantly physicians be
on board with EMR
implementation.
• A physician “lead” is
recommended who has a
strong commitment to see
the project through, and
is realistic, but not overly
optimistic
© BHM 2010

Principles of Change
Management
Involve Every Layer
• Everyone needs to feel
that their contribution is
important. Form a
committee of employees
to evaluate different
systems and let them
make proposals to the
physicians. These should
be people who will be
using the system
(administration, business
office, ect.)
Make the Formal Case
• Have a written vision
statement outlining what
this change will mean to
the organization, as well
as what, how, and why
this change is taking
place. Provide reasons
why the EMR system is
superior to the paper
system, or it will not be
used
© BHM 2010

Principles of Change
Management
Create Ownership
• Appoint leaders who will
have ownership of the
project. Train these core
people and then use
them to train the rest of
the practice. Keep
communication open, and
encourage feedback. Lay
out a plan and sequence
of action, and keep staff
informed and involved
Assess the Landscape
• Identify core values in the
current cultural landscape
of the practice. Look for
beliefs, perceptions, and
areas of resistance.
Identify people who may
be lacking technical
knowledge (the employee
who doesn’t know how to
use a mouse, or the MD
who doesn’t use email)
© BHM 2010

Principles of Change
Management
Address Culture Explicitly
• If necessary take small
steps. Employees should
learn to use a computer,
a mouse, email, more
sophisticated programs,
and then finally EMRs.
Keep less enthusiastic
members of management
involved, or they will be
resistant
Prepare for Unexpected
• There will be problems so
take this into
consideration in your
planning. Dates for going
live with the project, or
timelines may be missed,
build in a cushion so that
delays can be dealt with
sans a ripple effect.
© BHM 2010

Principles of Change
Management
Speak to the Individual
• Set out clear guidelines
and expectation for each
individual within the
organization. Be
confident, and realistic
about employees fears
and concerns in relation
to the change
Be Flexible
• Be flexible and optimistic
in dealing with the
change. Take into
consideration the
feedback that you receive
throughout the project
and use it to make
changes to best meet the
needs of your
organization
© BHM 2010

STAFF TRAINING FOR EMR
IMPLEMENTATION
© BHM 2010

Staff Training: The Essential
Steps
• We recommend the following 3 steps in effectively training
and preparing staff for EMR implementation
© BHM 2010
Identify the Current Skill Level
Bring Staff up to the Needed Skill Level
Design a Training Plan for the New Software

Identify the Current Skill Level
• Determining computer proficiency for all staff members is a
vital step in preparing for EMR implementation.
• Staff competency may be determined by asking what
programs the staff are familiar with, and what type of
technology they use on a daily basis in the work
environment
• In addition to this staff competency can be determined by
the technical vocabulary that they are familiar with
© BHM 2010

Bring the Staff up to the Needed
Skill Level
• In EMR implementation that uses a graphic interface, staff
will need basic skills such as drag and drop functioning,
how to transfer between systems, and how and where files
are to be saved
• Most staff will need to know how to use the Electronic
Practice Management system to make or look up
appointment information
© BHM 2010

Bring the Staff up to the Needed
Skill Level (cont)
• Some staff will require the ability to check patients in and
out, while others will need to be able to post payments and
generate claims
• The technical staff may not have to know the claims
process, but will need to be proficient in the EMR process
for successful implementation
© BHM 2010

Implement a Training Plan for
New Software
• The EMR committee must design a training plan that takes
skill level factors into consideration
• The EMR committee will need to determine what the
common tasks for each employee will be, then add
additional skills of increased complexity to the appropriate
departments and jobs
© BHM 2010

Implement a Training Plan for
New Software (cont)
• The entire staff should be taught system basics
• Following this training should be structured from a
departmental perspective, each department receiving
training on the necessary tasks for their particular jobs
• A training manual should be written for the EMR process,
with room for improvements to the manual as the process
progresses
© BHM 2010