
EMPOWERING NURSES TO LEAD ND Center for Nursing FUTURE OF NURSING CAMPAIGN FOR ACTION.
50
EMPOWERING NURSES TO LEAD ND Center for Nursing FUTURE OF NURSING CAMPAIGN FOR ACTION
-
Upload
kathryn-anthony -
Category
Documents
-
view
217 -
download
3
Transcript of EMPOWERING NURSES TO LEAD ND Center for Nursing FUTURE OF NURSING CAMPAIGN FOR ACTION.

EMPOWERING NURSESTO LEAD
ND Center for NursingFUTURE OF NURSING
CAMPAIGN FOR ACTION

NAVIGATING THE
COMPLEX HEALTH SYSTEM
A Primer for The Nurse

Leadership Program is divided into 4 main areas.
Communication is foundational for learning and understanding about systems. Knowledge of
how systems function is necessary to institute change.
The ability to accept and engage in change is necessary to be an advocate for health
policy.
All nurses are expected to lead!

What is Nursing
• Nursing is the protection, promotion, and
optimization of health and abilities, prevention of illness and injury, alleviation of suffering through the diagnosis and treatment of human response, and advocacy in the care of individuals, families, communities, and populations. ANA
http://www.nursingworld.org/EspeciallyForYou/What-is-Nursing

What is a Complex System• A complex system is a system composed of interconnected
parts that as a whole exhibit one or more properties (behavior among the possible properties) not obvious from the properties of the individual parts

Too Many Silos
System vs Silo
• “System”– OB/Gyn – Oncology – Schedule – Surgery – Follow-up
Fear – Trust - $$
• “Silo” – OB/Gyn
OncologySchedule
SurgeryFollow-up
Fear – Emotional upheaval – Time - Travel - $$$$$http://nursing.advanceweb.com/editorial/content/printFriendly.aspx?CC=275654
2/5/2014

From
Agency for Healthcare Research & Quality
• “it is in inadequate handoffs that safety often fails first”
• “nurses are the health care professionals most likely to intercept errors and prevent harm to patients”– http://www.ahrq.gov/professionals/clinicians-providers/resources/nursing/resources/n
urseshdbk/index.html

Knowledge of “System”
• Recognize “how things work” – and why• Know who is responsible • Ensure transfer of correct information• Provide patient support to wellness—• Track referrals & help resolve problems • Lead your Team to excellent patient service• Help patients identify sources of service &
make appointments – Care Coordination

Why Understand ‘Systems’
• Nurse is primary to patients (leader of the care team)
– First connection in most any setting – Knows diagnosis, plan of care, desired outcome– Knows Patient vulnerabilities– Last connection in most any setting
• Nurse most trusted of care-givers• Nurse facilitates Care Coordination: internal & external

Why Care Coordination?
• Patients and families hate it that we can’t make this work • Happier patients • Poor hand-offs lead to delays, lapses in care, adverse drug
effects, and other situations that may be dangerous to health• Fewer problems – for patient and for health system
• Improve the health of the population • Less waste
• Enormous waste is associated with duplicate testing, unnecessary referrals, unwanted specialist-to-specialist referrals, and failed transitions from hospitals, EDs, & nursing homes.
• Clinical practice will be more rewarding

THE PATIENT
• Life-style• Diagnoses• Treatment options• Family obligations• Hopes/dreams• Support systems

OBJECTIVES• Review the health care system’s care provider types and
levels of service, regulation, and reimbursement mechanisms; • Investigate your organization’s structure and processes;• Describe your position/role within the organizational
structure; and• Demonstrate your knowledge of the health system to help a
patient (and family) consider and access viable options for achieving personally desired health outcomes.

Types of Providers• Community
– Available to the community at large or a specific segment of the population for prevention, support, or treatment
• Outpatient– The patient receives treatment and services; remains less than 24 hours
• Inpatient– The patient stays overnight for treatment, support, and lodging
• A hospital Medicare “Observation” patient is considered an outpatient in terms of reimbursement even though housed for up to 5 days in a hospital bed. This designation is being contested.
• In-home– The patient receives prevention, support, and treatment services in the individual’s
private home or in a current place of residence such as a group home or assisted living facility that does not prohibit such services

Ownership & Management
• General Providers – Available to qualified general population
– Religious Organizations– ‘Community’ owned– Privately owned– Government owned
• Special Population Providers– Veterans Health Administration (VAMC)– Indian Health Service (IHS)– Migrant Health Services– Public Health Services (PHS)– Government owned – Homeless

Community Health Providers• Public Health – Counties/Cities• Rural Health Clinics , FQHC -- Medicare/Medicaid certified – different fee structure
• WIC• School Nurses• Wellness/Fitness Centers• Vaccination Clinics• Faith Community Nurses• Community Action Agencies• Social Service/Mental Health Agencies• Durable Medical Equipment Suppliers• Pharmacies• Industrial Health – may be limited to certain employees

Outpatient Providers• Medical Clinics – 305 est (52 RHC, 7 FQHC)• Ambulatory Surgery Centers - 12• Renal Dialysis Centers (ERSD) - 16• Physical, Occupational, Speech Therapy - 1 CORF, ?? # independent
• Cardiac and Wellness Centers• Addiction/Mental Health Therapy - 54• Telehealth - • Adult Day Care – Respite Care• Diagnostic Services
– Laboratory– Radiology– Screening– Telehealth

Inpatient Providers• Hospital
– Acute General • Critical Access - 37
• Swing Bed (LTC) - 37• Prospective Payment – 6
– Rehabilitation - 1– Long Term Acute Care - 2– Acute Psychiatric - 3– Acute Special – transplantation - 2
• Nursing Facility - 80 12,213 residents in 2012• Basic Care Facility – 68 (may be wing of nursing facility) 4,152 residents in 2012• Assisted Living Facility – 73 3,195 residents in 2012• Hospice – 13• “Treatment” Centers - • Group Homes -

In-Home Providers
• Home Health - 35• Therapy -- Physical, Occupational, Respiratory, Speech
• Personal Care – Family, Private, HCBS • Homemaking• Hospice - 13• Telehealth• Diagnosis -- Lab draws, Mobile radiology

INDEPENDENT HEALTH PROFESSIONALS
• Physicians – Primary and specialty care• Dentists• Pharmacists• Advanced Practice Nurses – 558 with prescriptive authority
• Optometrists/Opticians• Chiropractors• Psychologists• Counselors• Addiction Counselors

Levels of Service
• Preventive – Clinic, Community• Acute Care – Clinic, Hospital• Chronic Care – Clinic, Hospital, Long Term
Care, In-Home Care• Long term Care – Nursing Facility, Basic Care,
Assisted living, In-Home Care
• The goal would be to make Preventive always the first level

Preventive Services• Medical Clinic –screening, diagnosis, education, referral
• Hospital – diagnosis, treatment, education, referral
• Outpatient Providers – screening, diagnosis, treatment, support
• Therapies – diagnosis, treatment, training, education, referral
• Wellness Centers – training, education, support
• Community Services – treatment, education, support, referral
– Family services – domestic, financial– Support Groups– Nutrition– Personal care

Acute Services
• Medical Clinic – diagnosis, treatment, education, referral
• Hospital – diagnosis, treatment, education, referral
• Outpatient Providers – diagnosis, treatment, education, referral, support

Chronic Care Services
• Clinic – screening, diagnosis, treatment, education, referral
• Hospital – diagnosis, treatment, education, referral
• Long Term Care providers – diagnosis, treatment, education,
personal care, support
• In-Home – treatment, personal care, support
• Community – treatment, education, support, referral

Long Term Care Services
• Assisted Living – lodging, meals, optional services (Med Management, diet)
• Basic Care – lodging, personal care, med management, nutrition, activities
• Nursing Facility – lodging, personal care, treatment, skilled nursing,
• Group Homes – specific population housing, treatment, support, supervision,
• Mental Illness• Developmental Delays• Traumatic Brain Injury• Addictions
• •

Outside Forcesor at least ‘outside’ to individual caregivers
• Regulating• Standardizing• Defining• Measuring• Enabling• Limiting• Improving• Enriching• Challenging• Reimbursing
Much different from most other businesses – multiple ‘layers’ with indirect management and mixed messages
Who Defines Providers & Services• Legislature – Laws
– City - Regulations & Enforcement– State agencies – Regulations & Enforcement
• Licensing Agencies (Health, Human Services, Professional Boards)
• Congress – Laws– Federal Agencies – Regulations & Enforcement
• Department of Health & Human Services – Centers for Medicare and Medicaid, VAMC, IHS
• FDA, DEA, OSHA, CDC, DOL
• Health Care Industry - Financial Viability, Patient Demands, Workforce Availability
• Insurance Carriers – Financial Viability, Population, Marketplace
• Technology -- Pharmaceuticals - Research & Development, Financial Viability
• Public – Liability suits, (Lack of) Advance Directives, Requests and Demands for Service
• Professional/Trade Organizations – Education, Lobbying, Research
• Academia – Education, Research

The Regulation of Health Care• Licensure – State -- description of service & enforcement
• the state or condition of having a license granted by official or legal authority to offer specific services and take specific action not permitted by persons without such a license: i.e. Registered Nurse, Pharmacist, Hospital, etc. (edited)
• Certification – Federal -- Medicare/Medicaid – description of service & payment• The Social Security Act (the Act) mandates the establishment of minimum health and safety and CLIA
standards that must be met by providers and suppliers participating in the Medicare and Medicaid programs. These standards are found in the 42 Code of Federal Regulations. The Secretary of the Department of Health and Human Services has designated CMS to administer the standards compliance aspects of these programs.
• Some individual professions are ‘certified’ rather than ‘licensed’
• Accreditation -- The Joint Commission, etc.• Joint Commission standards are the basis of an objective evaluation process that can
help health care organizations measure, assess and improve performance. The standards focus on important patient, individual, or resident care and organization functions that are essential to providing safe, high quality care. The Joint Commission’s state-of-the-art standards set expectations for organization performance that are reasonable, achievable and surveyable.

Nongovernmental Governing Bodies
• Governing Body(ies) of a Facility (Board of directors, owners, medical staff, and department heads – even the community) establish direction; determine scope of services; determine financial status; establish personality.
• Professional Associations keep membership informed on changes and regional or national issues;
advocate for providers with legislative lobbying; offer education; afford peer support. • Provider Organizations keep membership informed on changes and regional or national issues; advocate
for providers with legislative lobbying and marketing efforts; offer education; afford peer support • Institutions of Higher Learning set the attitude and abilities of students; perform research that leads to
new treatment and technology; develop clinical expertise and standards; contribute to standards of ethics. • Payers of Service define elements of services (allowable/covered vs. non-allowable/uncovered): not
always coherent with regulations and standards of (clinical) practice. Government pays for a lion's share of the health care that is delivered and determines what is covered or not. Insurance companies have stock-holder profit motives. The general public who utilize health care services generally expect to rely on the health care delivery system to fix them when something goes wrong.
• Customers have the least impact on governing the health care system except by seeking alternative providers.

Reimbursement for Health Services• Private Health Insurance (much based on Medicare Rules)
– Premium paid by insured and/or employer– Payment for covered services by participating providers
• Private Self Pay– For uninsured patients or non-covered services
• Medicare – For age and disability qualified– Payment for covered services by participating qualified providers
• Medicaid– For income, age , and disability qualified– Payment for covered services by participating qualified providers
• Population based VAMC, IHS, Public Health,– For specific populations for covered services by participating qualified providers
• Reduced fees (sliding scale based on income) and Free (charity care)– When there is no other pay source– Providers (except hospitals) may choose to not accept/treat patients with no payment source

Definitions• Covered Services
– Medical and health care services defined by the paying agency. Restrictions vary by paying agency and specific coverage plan. i.e., a. May require specific sequence of diagnostic tests or treatments to qualify for payment; b. Pay for specific treatment for only specific diagnosis. Neither the patient nor the provider or practitioner decides what is a covered service although both agree by virtue of the contract.
• Participating Providers/Practitioners– Providers and Practitioners who have an agreement with the paying agency for certain services
under certain conditions
• Qualified Providers/Practitioners– Providers/Practitioners who are licensed or credentialed to perform service for which payment is
requested
• Prospective Payment System – A means of determining reimbursement to hospitals based on predetermined prices, commonly
from Medicare. Payments are typically based on codes such as Diagnosis-related Groups (DRGs), Current Procedural Terminology (CPTs), or Ambulatory Payment Classifications (APCs)
• Fee for Service – Cost-based– Services are unbundled and paid for separately

Employer Organization• Legal Description
– Licensure – www.nd.gov– Certification – www.cms.gov– Accreditation – www.jointcommission.org
• Organizational Governance• Mission Statement• Who is responsible
• Organizational Structure – Ownership - Corporation, proprietorship, partnership, government– For Profit/Nonprofit– Single site? – Multiple sites?– Related Providers
• Mission/Vision Statements
–
–
• • Teaching Facility?

Organizational Chart• Nursing Facility/Assisted Living Facility Owner
• Governing Body• Administrator - - -- - - - - - -Medical Director• Consultants - - - Pharmacist
Dietitian - Social Worker
________________________________________________________________________________________________________________________________• Dietary Building/Grounds Nursing Activities Social Work Business Office• FSS Plant Manager Director of Nursing Activities Director Social Work Designee Business Office Manager• Cook Assistant MDS RN Volunteers Purchasing
Dietary Aides Housekeepers Staff Nurses Clerk• Laundry Workers Nurse Aides
• OR
•
•
Examples of Organizational Charts• https://www.google.com/search?q=organizational+chart,
+hospital&tbm=isch&tbo=u&source=univ&sa=X&ei=thsSU9OYLInlyAGXvIDACA&ved=0CCcQsAQ&biw=1101&bih=862

Employer Description • Services Provided• Population Served• Management Team• Hiring, Orientation, Training, Retention• Policies• Procedures/Processes• Quality Assessment/Performance Improvement• Level of Decision-making• Community Involvement
Complete Handout – Employer Organization Worksheet

Reflect on your Employer Organization
• Accurately describe the Provider Type and Services provided• List Operational Priorities - from Your Perspective• Do you understand the political climate -?
– Within the organization– Within the Community
• What are usual referral patterns?
• • • •

36
Nursing Department• Organizational Location -- refer to chart• Intra-Organizational Communication– Clear Expectations– Two-way Interactions
• Patient Care Policies • Staffing Patterns • Contribute to Organizational Decision-
making?

Your Position within the DepartmentLevel of Responsibility & Accountability
• What is your position title?• Do you ‘fit’ your position?• Do you like your position?• Do you have & use opportunities for growth?• more
Complete Handout – Job.Communications

What Can I Do?• Trusted and Trusting
– Accountable– Responsible
• Mindful– Aware of – Considerate of co-workers, patients, families
• Personal skills to influence – from THIS Position– Empower – self, co-workers, patients– Creative, generate positive excitement – – Facilitate (Coordinate !) – work environment, inter-departmental
relationships, patient services,
• •

Develop a plan to assist your patient to move into/access required level of service
• To be expanded and Section to follow for Objective #4
• Diagnosis• Treatment• Preferred site (inpatient, outpatient, home)• Support resources• Transportation• Pay source• Activities of daily living• Instrumental activities of daily living• Supply delivery

Barriers to Access/Success
• Mixed Priorities – Patient vs System
• Financial • Language/Cultural/Belief System• Educational• Generational• Geographic

Generational Differences

Something with Nursing Process and Handoffs
• Nursing Process: a five-part systematic decision-making method focusing on identifying and treating responses of individuals or groups to actual or potential alterations in health. Includes assessment, nursing diagnosis,
planning, implementation, and evaluation. http://www.medilexicon.com/medicaldictionary.php?t=61900
MediLexicon International Ltd, Bexhill-on-Sea, UK, MediLexicon International Ltd © 2004-2014 All rights reserved.
•
• •

“The Patient Experience” copied from NDHCRI
• National Perspective• 1 in 5 Medicare beneficiaries are readmitted to the hospital within 30 days• 1 in 3 beneficiaries are readmitted within 90 days• 2 of 3 patients with medical conditions are either rehospitalized or died one year after discharge• 90% of rehospitalizations were unplanned• 76% of 30-day readmissions are potentially preventable
• Hackbarth, Reischauer, and Miller. Medicare Payment Advisory Committee. 2007
• • • •

Patient ExperienceFrom ND HCRI
• Abrupt transitions between settings• Brief hospital days• Sudden self-management with minimal
preparation• Poor communication between care providers
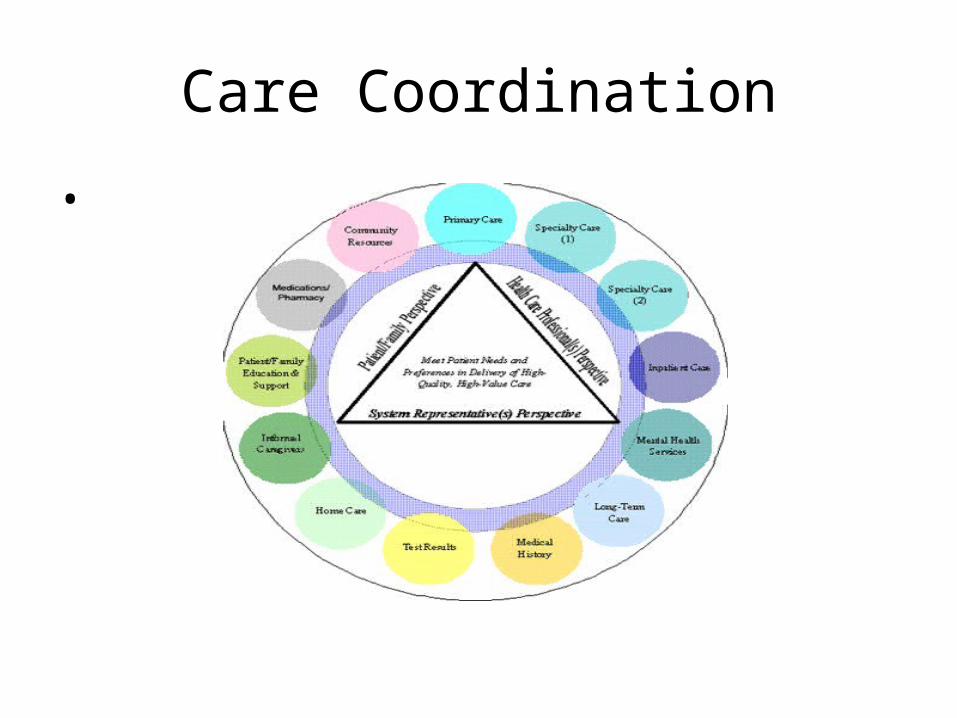
Care Coordination
•

NOT A SILO
• “System”– OB/Gyn – Oncology – Schedule – Surgery – Follow-up
Fear – Trust - $$
• “Silo” – OB/Gyn
OncologySchedule
SurgeryFollow-up
Fear – Emotional upheaval – Time - Travel - $$$$$
http://nursing.advanceweb.com/editorial/content/printFriendly.aspx?CC=275654 2/5/2014

ND Dept of Human ServicesAvailable to all ND residents
• https://carechoice.nd.assistguide.net/site/423/useful_links.aspx• https://carechoice.nd.assistguide.net/site/371/find_a_service.aspx
• http://www.acl.gov/www.acl.gov/About_ACL/FederalInitiatives/VeteransCare.aspx
• http://ndipat.org/
• http://www.agingcare.com/Elder-Care
• http://www.nd.gov/dhs/services/adultsaging/reporting.html
• http://www.nd.gov/dhs/services/adultsaging/ombudsman.html
•

Care Coordination• http://www.raconline.org/communityhealth/care-coordination?
utm_source=racupdate&utm_medium=email&utm_campaign=update022014• • NDDOH – Children’s services• http://www.ndhealth.gov/familyhealth/publications/ConnectionDirectory.pdf• http://www.ndhealth.gov/cshs/docs/cshs-provider-list.pdf• http://nd.bridgetobenefits.org/• http://www.ndhealth.gov/cshs/
• • • • •

Wrap-up
• Reflect on the complexity of the overall healthcare system• Reflect on your organization within the system• Reflect on your position within your organization• Reflect on the result of your patient advocacy experience• How could a different reality have made your experience
more successful and satisfying?• What will you do to move toward that different reality?
• And so we move into the Change & Innovation module

References• Demographics – numbers of providers
– North Dakota Healthcare Association– ND Long Term Care Association
–http://ruralhealth.und.edu/pdf/escan/vol1-2.pdf
• • •
• Closing the Loop with Referral Management, Ed Wagner, MD, MPH, MACP MacColl Center for Health Care Innovation Group Health Research Institute, Linda Thomas-Hemak, MD, The Wright Center for Primary Care. February 26, 2013


















