Ross, D. (2013) Reliability of EMG/IOPI in OPD/OMD Diagnosis.
Upload
katey-yumulCategory
view
6download
1description
doi: 10.2522/ptj.20070146Originally published online August 8, 2008
2008; 88:1061-1067.PHYS THER. Arajo and Maicon PasiniMarcelo La Torre, Mnica de Oliveira Melo, Lucas DutraMaria Steffens Pressi, Flvio Antonio de Souza Castro, Cludia Tarrag Candotti, Jefferson Fagundes Loss, AnaBack MusclesElectromyography for Assessment of Pain in Low
http://ptjournal.apta.org/content/88/9/1061found online at: The online version of this article, along with updated information and services, can be
Collections
Tests and Measurements Pain
Injuries and Conditions: Low Back in the following collection(s): This article, along with others on similar topics, appears
e-Letters
"Responses" in the online version of this article. "Submit a response" in the right-hand menu under
or click onhere To submit an e-Letter on this article, click
E-mail alerts to receive free e-mail alerts hereSign up
by guest on June 18, 2015http://ptjournal.apta.org/Downloaded from by guest on June 18, 2015http://ptjournal.apta.org/Downloaded from
Electromyography for Assessment ofPain in Low Back MusclesClaudia Tarrago Candotti, Jefferson Fagundes Loss, Ana Maria Steffens Pressi,Flavio Antonio de Souza Castro, Marcelo La Torre, Monica de Oliveira Melo,Lucas Dutra Araujo, Maicon Pasini
Background andPurpose. Pain is currently evaluated with subjective meth-ods (eg, patient self-report). This study aimed to test whether fatigue indexes are ableto accurately discriminate between subjects with and subjects without low back pain.
Subjects. Sixty subjects separated into 2 groupsa group with low back pain(n30) and a group without low back pain (n30)participated in this study.
Methods. Electromyographic (EMG) and force data were obtained during a mus-cle fatigue test. The same test was repeated to monitor recovery. Linear regressionanalysis was used to obtain fatigue indexes.
Results. Subjects with pain produced significantly lower force values than thosewithout pain. The use of fatigue indexes and force values permitted accurate classi-fication in 89.5% of cases.
Discussion andConclusion. The results confirm that subjects with pain showearly myoelectrical manifestations of muscle fatigue and that EMG can be a useful toolin the evaluation of low back pain.
CT Candotti, PhD, is Professor,Curso de Educacao Fsica, Univer-sidade do Vale do Rio dos Sinos,Sao Leopoldo, Brazil.
JF Loss, PhD, is Professor, Escola deEducacao Fsica, UniversidadeFederal do Rio Grande do Sul, RuaFernando Osorio, 1887, CEP91720-330, Porto Alegre, Brazil.Address all correspondence to DrLoss at: [email protected].
AMS Pressi, MSc, is Research Assis-tant, Curso de Educacao Fsica,Universidade do Vale do Rio dosSinos.
FAS Castro, PhD, is Professor, Es-cola de Educacao Fsica, Univer-sidade Federal do Rio Grande doSul.
M La Torre is Physical EducationTeacher and an MSc student inthe Curso de Educacao Fsica, Uni-versidade do Vale do Rio dosSinos.
MO Melo is Physical EducationTeacher and an MSc student inthe Curso de Educacao Fsica, Uni-versidade do Vale do Rio dosSinos.
LD Araujo is Physical EducationTeacher and an MSc student inthe Curso de Educacao Fsica,Universidade do Vale do Rio dosSinos.
M Pasini is Physical EducationTeacher and an MSc student inthe Curso de Educacao Fsica,Universidade do Vale do Rio dosSinos.
[Candotti CT, Loss JF, Pressi AMS,et al. Electromyography for assess-ment of pain in low back muscles.Phys Ther. 2008;88:10611067.]
2008 American Physical TherapyAssociation
Research Report
Post a Rapid Response orfind The Bottom Line:www.ptjournal.org
September 2008 Volume 88 Number 9 Physical Therapy f 1061 by guest on June 18, 2015http://ptjournal.apta.org/Downloaded from
Low back pain is a syndrome ofmultifactorial etiology that af-fects 6.8% of the world popula-tion at any given time.1 It is one ofthe principal causes of absenteeismfrom work and impairment of theperformance of daily activities,thereby affecting an individualsquality of life.2
Traditionally, the clinical diagnosisof low back pain has been made by aphysician or physical therapist usingmethods such as palpation, anamne-sis, and the Borg scale.3,4 The evolu-tion of low back pain during physicaltherapy treatment also can be moni-tored with questionnaires and phys-ical performance tasks.5 All of thesesituations involve a great degree ofsubjectivity; that is, they depend onthe patients report or the physicaltherapists interpretation. Therefore,sometimes double-blind tests areused.
In 1993, an alternative low back painevaluation procedure, the Back Anal-ysis System, was proposed. The BackAnalysis System allows for more ob-jective diagnosis and follow-up.6
This system is based on muscle fa-tigue induction monitored by sur-face electromyography (EMG) in thefrequency domain, which allowsmapping of the median frequency(MF) during a sustained muscle con-traction. During the fatigue process,the MF tends to decrease, reflectingthe decrease in the motor unit actionpotential firing rate during a musclecontraction.7 On the basis of thisspectral variable, an index of musclefatigue during isometric contractionshas been proposed as a guide forevaluating low back pain.6
Thus, in recent years, it has beensuggested that chronic low backpain is intimately related to localizedmuscle fatigue. In this sense, musclefatigue is understood to be a contin-uous process that starts with the ini-tiation of neuromuscular activity and
that is capable of causing changes inelectrical activity, electrical propaga-tion, excitation-contraction cou-pling, and various elements of thecontraction process.811 Scientificevidence has shown that peoplewith low back pain exhibit earliermanifestations of muscle fatigue inlow back muscles than people whoare healthy.3,6,1214 However, in stud-ies in which the objective has beento use EMG to discriminate betweenpeople with and people withoutpain, there has been a tendency tofocus on small samples of athletes12;people who are not athletes havereceived little attention. Further-more, although studies have beencarried out with the aim of analyzingthe relationship between the EMGsignal and low back pain, before con-sidering the capacity of the methodto achieve a straight diagnosis, theintrinsic limitations of the techniqueneed to be analyzed. Therefore, thepresent study, which included meth-ods similar to those used in otherstudies, such as discriminant statisti-cal analysis, and which focused onsedentary subjects, represents a con-tribution toward the application ofthe technique to clinical practice.
The purpose of this study was toverify whether muscle fatigue in-dexes calculated in the frequencydomain are capable of discriminatingbetween sedentary subjects withlumbar pain and those without lum-bar pain. If such discrimination isshown to be possible with surfaceEMG, it can be hypothesized that thesame technique can be used to ob-
tain an objective assessment of lowback pain.
MethodSubjectsSixty subjects who did not performregular physical activity participatedin this study. The subjects were sep-arated into 2 groups: a group withlow back pain (n30) and a groupwithout low back pain (n30). In-terviews and anamnesis were usedby a physical therapist to recruit thesubjects. The inclusion criterion forthe pain group was multiple epi-sodes of pain in the low back mus-cles in the preceding 3 months, char-acterized as chronic pain (daily oralmost daily). The pain was notscaled; only the number of episodeswas considered. The inclusion crite-rion for the without-pain group wasthe absence of pain in the low backmuscles in the preceding year. Ex-clusion criteria were as follows: pre-vious surgery, symptoms of nerveroot engagement (ie, pain distal tothe knee), spondylolisthesis, spinalstenosis, inflammatory disease, andcancer. The subjects signed a writteninformed consent form. Table 1shows the age, stature, and bodymass of the subjects and the numberof pain episodes.
ProtocolFor evaluation of the low back mus-cles, the subjects lay in a prone po-sition on an exercise bench with thelow back, hips, and knees securelyfixed by straps. The subjects alsowere secured at the level of the scap-ula by a leather strap, which was
Table 1.Means and Standard Deviations for Various Characteristics of Subjects in thePreceding Year
Group (n)
X (SD) for:
Age, y Stature, cm Body Mass, kg No. of Pain Episodes
With low back pain (30) 27.2 (7.2) 171.0 (10.0) 69.8 (11.4) 11 (3)
Without low back pain (30) 23.7 (5.4) 170.5 (7.5) 69.0 (10.1) 0
Low Back Pain Assessment
1062 f Physical Therapy Volume 88 Number 9 September 2008 by guest on June 18, 2015http://ptjournal.apta.org/Downloaded from
attached to the load cell fixed to theground. While in this position, thesubjects were asked to attempt toextend the trunk; given the impossi-bility of performing this movement,this attempt led to an isometric con-traction of the low back muscles. Allsubjects performed the protocolonce.
The protocol6 consisted of 3 stages:(1) 3 attempts at the maximal volun-tary contraction (MVC), each lastingapproximately 5 seconds, with a2-minute interval between attempts;(2) one fatigue test, which consistedof maintaining a calculated submaxi-mal level of 80% of the MVC for 35seconds; and (3) a postfatigue test (atthe same 80% of the MVC) for 10seconds to monitor recovery. Thehighest value obtained in the firststage was used to calculate the sub-maximal level of 80% of the MVC.There were 2-minute intervals be-tween stages. An oscilloscope* wasused to provide visual feedback, andsubjects were given strong verbalencouragement.
Data AcquisitionThe EMG and force signals were ac-quired simultaneously during theprotocol with a Pentium 200-MHzPCcompatible microcomputer,through a 12-bit analog-to-digitalconverter board, with a samplingfrequency of 2,000 Hz per channel.
The EMG activity was recorded bilat-erally from the longissimus (L1) andiliocostalis lumborum (L2) muscles,in accordance with standards for re-porting EMG data.15 Disposablesilversilver chloride surface elec-trodes (1.0 cm in diameter) wereplaced in a bipolar configuration onthe bellies of the muscles, along thesupposed alignment of the muscle
fibers. The reference electrode wasplaced on the left wrist. Preparationfor surface EMG activity detectionincluded shaving and application ofalcohol to cleansed skin. Impedancebetween electrodes was checkedand accepted when maintained atless than 5 k. Recordings weremade by use of a 16-channel EMGsystem with preamplifiers (fixedgain of 20) located approximately10 cm away from the electrodes. Theinput impedance of the system was10 G, the common mode rejectionrate was greater than 100 dB (at 60Hz), and the signal-to-noise ratio was3.0 V root mean square. The forcesignals were obtained by use of aload cell fitted with strain gauges
connected to the same EMG module.
Data Processing and AnalysisForce and EMG data were analyzedwith in-house software. Raw EMGdata were initially submitted to aband-pass filter (Butterworth, thirdorder, 20500 Hz). The filtered EMGsignal was analyzed in the frequencydomain; the MF was calculated fromthe power density spectrum ob-tained after Hamming windowing (1second) by use of the fast Fouriertransform technique. The EMG sig-nal from each muscle was normal-ized on the basis of the maximumfrequency of each trial in the fre-quency domain.16 With the aim ofavoiding possible variations resultingfrom the change in the condition ofthe muscle from nonactivated to ac-tivated (at the beginning of the test)and from activated to nonactivated(at the end), we excluded the first 2seconds from the beginning of thetest and the last 3 seconds from theend. Consequently, 30 windows re-mained, represented by MF valuesattributed to the center of eachwindow.
Linear regression analysis was usedfor 30 points, and a linear equationwas obtained for each muscle. Thisequation supplied the linear slopecoefficient and the y-intercept value,both of which were considered to befatigue indexes.17,18 For inclusion inthe study, the coefficient of determi-nation obtained by linear regressionhad to be equal to or higher than 0.6.Thus, the EMG response from thefatigue protocol was obtained from 5muscle fatigue indexes. The use ofindexes 3 and 4 ( and y, respec-tively; see below) was an attempt todisregard the fluctuations normallypresent in fatigue protocols.
The fatigue indexes were as follows:
1. The slope coefficient () of astraight line that approached all 30MF values12
2. The y-intercept (y) of a straightline that approached all 30 MFvalues12
3. The slope coefficient () of astraight line that approached just thefirst and the last MF values17,18
4. The y-intercept (y) of a straightline that approached just the firstand the last MF values17,18
5. The recovery index (REC), repre-sented by the following equation12:REC[(MFrMFf)/(MFiMFf)]/100,where MFr is the highest MF duringthe recovery period, MFf is the finalMF, and Mfi is the initial MF.
Data AnalysisAnalyses were carried out with SPSS10.0 software. The normality of thedata (Shapiro-Wilks test) and the ho-mogeneity of the variances (Levenetest) were verified and confirmed. At test for independent samples wasperformed to test for any differences
* Minipa Electronics Co, 33 Alameda dos Tu-pinas, Sao Paulo, SP 04069-000, Brazil. Lynx Tecnologia Electronica Ltda, 358 DrJose Elias, Sao Paulo, SP 05083-030, Brazil.
EMG System do Brasil Ltda, 1380 Scorpius,Sao Jose dos Campos, SP 12230-570, Brazil. Alfa Instrumentos Electronicos Ltda, 138Coronel Mario de Azevedo, Sao Paulo, SP02710-020, Brazil.
SPSS Inc, 233 S Wacker Dr, Chicago, IL60606.
Low Back Pain Assessment
September 2008 Volume 88 Number 9 Physical Therapy f 1063 by guest on June 18, 2015http://ptjournal.apta.org/Downloaded from
between groups in relation to forceand MF. To assess the ability of fa-tigue indexes and force data to dis-criminate between subjects with andsubjects without pain, we performeddiscriminant analysis: Wilks test toevaluate the homogeneity of the vari-ances, canonical correlation to verifythe linear combination of the vari-ables, stepwise Wilks discriminantanalysis to classify subjects intogroups, and the predicted score foreach group. In the discriminant func-tion, all muscles were considered in-dividually and as a single low backmuscle group. Thus, a one-way anal-ysis of variance was applied to verifypossible differences in the fatigue in-dexes of 4 low back muscles. Be-cause there were no significant dif-ferences in the fatigue indexes of the4 muscles investigated, these mus-cles were considered as a single lowback muscle group. The level of sig-nificance used was .05.
ResultsThe results showed that subjectswith low back pain produced forcevalues significantly lower than thoseof subjects without pain (P.002).The means and standard deviationsfor force were 505213 N for thelow back pain group and 678233 N
for the without-pain group. Table 2shows the means and standard devi-ations for MFi, MFf, and MFr. Signif-icant differences between groupswere found only on the left side.
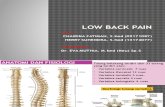
The Figure illustrates the MF changesin the left iliocostal lumbar muscleduring the fatigue test in 2 subjects,one with pain (Figure, left) and theother without pain (Figure, right).The fatigue indexes, slope coeffi-cient (), and y-intercept (y) are in-dicated in the regression linear equa-tion in the Figure. In Table 3, onlythe REC fatigue index showed a sig-nificant difference between subjectswith and subjects without pain.Again, significant differences be-tween groups were found only onthe left side.
Discriminant analysis was used toclassify subjects into pain andwithout-pain groups by use of thefatigue indexes and force values ob-tained from the MVC. The most ac-curate results were achieved whenthe low back muscle group as awhole showed that the variables(force, , y, , y) were able to cor-rectly classify 86.7% of all subjects(Wilks 0.645, 227.102, df17,P.048) (Tab. 4). The analysis in
which only the force value was usedin the discriminant function was ableto correctly classify 63.3% of all sub-jects (Wilks 0.871, 27.970,df1, P.005). When the REC wasadded into the analysis, a decrease inthe prediction accuracy was ob-served; the most accurate results in-dicated that for the low back musclegroup, the variables (, y, y, , REC)were able to correctly classify 64.6%of all subjects (Wilks 0.894,215.591, df5, P .008) (Tab. 4).When the analysis was performedwith all of the muscles individually,the most accurate results indicatedthat for the left longissimus muscle,the force value and 3 fatigue indexes(y, y, and REC) were able to cor-rectly classify 69.4% of all subjects(Wilks 0.804, 29.796, df4,P.044) (Tab. 4).
DiscussionThe results showed that 86.7% of allof the subjects were correctly classi-fied. This result is comparable tothose of other studies, because theaccuracies of the classifications ob-tained from the discriminant func-tion were between 85% and 100%,depending on the people assessed.19
Interestingly, these accuracies wereachieved only when the spectralvariables were associated with theforce values obtained from the MVC.Similarly, in another study with logis-tic regression, which combinedforce and initial MF, between 78%and 86% of the subjects were accu-rately classified.3 However, in still an-other study, in which only the RECand slope coefficient were used andforce value was not used, 100% clas-sification accuracy was achieved for6 rowers with low back pain.12
Although the evaluation methodused in the present study was similarto the methods used in the above-mentioned studies, the highest accu-racy achieved in identifying seden-tary subjects with low back pain was89.5% (Tab. 4). However, the sample
Table 2.Means and Standard Deviations for Normalized Initial Median Frequency (MFi ), FinalMedian Frequency (MFf ), and Highest Median Frequency During the RecoveryPeriod (MFr) in the Iliocostalis Lumbar and Longissimus Muscles
Muscle Group
X (SD) for:
MFi MFf MFr
Right iliocostalis lumbar Without pain 92.63 (14.79) 70.56 (15.22) 96.27 (11.31)
With pain 94.83 (10.25) 67.19 (11.86) 100.57 (11.49)
Right longissimus Without pain 96.45 (8.61) 73.33 (12.21) 100.78 (14.33)
With pain 99.15 (9.46) 70.68 (13.17) 106.07 (15.59)
Left iliocostalis lumbara Without pain 91.97 (11.62) 73.43 (17.99) 97.61 (17.33)
With pain 95.96 (12.98) 65.89 (12.70) 106.06 (15.96)
Left longissimusa Without pain 93.15 (8.21) 74.38 (15.45) 100.12 (10.58)
With pain 97.71 (9.79) 72.65 (10.97) 107.09 (17.03)
a Significant difference at P.05 between group with pain and group without pain on left iliocostalislumbar and left longissimus muscles for all variables (MFi, MFf, and MFr).
Low Back Pain Assessment
1064 f Physical Therapy Volume 88 Number 9 September 2008 by guest on June 18, 2015http://ptjournal.apta.org/Downloaded from
used in the present study was 10times larger (n60); accordingly, thediscriminatory power was propor-tionally greater than that presentedfor the rowers,12 because the largerthe number of subjects, the greaterthe statistical test power.20
Even though the present study failedto accurately classify 100% of thesubjects with low back pain, all pre-dictions were significant. This find-ing confirmed the initial hypothesissuggesting the value of using thisprocedure for the evaluation of lowback pain and the follow-up of itsevolution in sedentary subjects, de-spite the fact that the subjects withpain may not have exerted maximalforce during the MVC, even though
they were strongly encouraged to doso.
Significant differences were foundfor force values between subjectswith and subjects without pain, andthe pain group produced force val-ues that were 26% lower than thoseof the without-pain group. Pain anddisuse, common in people with lowback pain, cause changes in EMG ac-tivity during induced fatigue and de-creases in the force and resistancecapacity of the low backmuscles.3,19,21
It is possible that subjects with painexerted less than 80% of the MVCduring the fatigue test, perhaps be-cause they were unable to produce
their true MVC.3 A pain adaptationmodel22 suggests that pain decreasesmuscle activation when the muscleacts as an agonist and increases mus-cle activation when it acts as an an-tagonist. This model postulates thatchanges in motor recruitment maybe attributable to some strategic con-trol that the nervous system exe-cutes through a specific neural path-way. The effects of this neuralmechanism indicate a decrease inthe activation of agonists and an in-crease in the activation of antago-nists.2 Thus, it is understood thatpain can affect voluntary activity inpainful muscles, producing inappro-priate contractions.
Table 3.Means and Standard Deviations for the Fatigue Indexes in the Iliocostalis Lumbar and Longissimus Musclesa
Muscle Group
X (SD) for:
y y REC
Right iliocostalis lumbar Without pain 1.0 (0.3) 101.87 (15.2) 1.1 (0.5) 98.23 (13.8) 117.57 (42.9)
With pain 0.9 (0.5) 102.19 (12.8) 1.0 (0.6) 99.50 (9.7) 100.14 (33.3)
Right longissimus Without pain 0.9 (0.4) 109.64 (14.8) 1.2 (0.4) 101.44 (12.6) 119.20 (59.0)
With pain 0.8 (0.5) 104.91 (13.8) 1.0 (0.7) 100.60 (12.7) 122.33 (67.52)
Left iliocostalis lumbarb Without pain 0.9 (0.5) 101.09 (13.8) 1.1 (0.4) 98.89 (17.0) 119.00 (48.1)
With pain 0.8 (0.5) 101.62 (16.1) 0.9 (0.6) 97.71 (13.6) 152.39 (72.8)
Left longissimusb Without pain 0.8 (0.5) 102.16 (10.4) 1.1 (0.5) 97.26 (9.9) 127.33 (29.8)
With pain 0.8 (0.5) 102.99 (15.8) 0.9 (0.6) 99.58 (13.0) 162.27 (78.9)
a slope coefficient of a straight line that approached all 30 median frequency (MF) values, yy-intercept of a straight line that approached all 30 MFvalues, slope coefficient of a straight line that approached just the first and the last MF values, yy-intercept of a straight line that approached just thefirst and the last MF values, RECrecovery index.b Significant difference at P.05 between group with pain and group without pain on left iliocostalis lumbar and left longissimus muscle only for REC.
Figure.Median frequency (MF) for left iliocostalis lumbar muscle. (Left) Example of MF throughout the fatigue test performed by a subjectwithout pain. (Right) Example of MF throughout the fatigue test performed by a subject with pain.
Low Back Pain Assessment
September 2008 Volume 88 Number 9 Physical Therapy f 1065 by guest on June 18, 2015http://ptjournal.apta.org/Downloaded from
In the present study, although forceshowed predictive power, thispower was seen only when forcewas used in combination with otherspectral variables in the discriminantfunction. This finding showed theimportance of muscle fatigue in-dexes that indicate early myoelectri-cal manifestations of muscle fatiguein people with low back pain relativeto people who are healthy.5 Thepresence of this hypothesized behav-ior was confirmed and allowed dis-crimination between subjects withand subjects without pain (Tab. 4).
An evaluation of the MFi and MFfvalues for the longissimus and ilio-costal lumbar muscles on both sidesof the trunk revealed higher MFi val-ues and lower MFf values in subjectswith pain than in those without pain(Tab. 2). These findings indicatedthat in subjects with pain, there isalways a greater variation in fre-quency and therefore a steeperslope. This pattern may indicate thatsubjects with pain tend to showearly EMG responses associated withalterations in muscular contractionprocesses, such as propagation ofcell membrane action potentials andexcitation-contraction coupling. TheFigure illustrates the typical behaviorof the MF in the left iliocostalis lum-bar muscle during the fatigue proto-col in 2 subjects (with and withoutpain). Furthermore, with regard tothe spectral variables, the statisticalanalysis showed that significant dif-ferences were found only for the
muscles on the left side of the trunk(Tab. 2). This finding may have beenattributable to the lack of control oftrunk rotation during the fatigue pro-tocol. In a previous study12 in whichconsistent findings were obtainedfor both sides of the trunk, trunkrotation was controlled by use of 2cell loads, thus facilitating visualfeedback of the force used on bothsides simultaneously.
It has been suggested that peoplewith low back pain have a reducedphysiological capacity to remove lac-tate, thereby maintaining metabo-lites within the muscle for a longerduration.12 Although intracellular ac-idosis is considered to contribute tomuscle fatigue, it also plays a role inpreserving excitability when depo-larization occurs within the muscleduring activity; that is, intracellularacidosis has a protective effect dur-ing muscle fatigue.23 Considering re-covery capacity (ie, a return to a non-fatigue condition24) as an importanttool in the analysis of neuromuscularfunction and low back pain, we alsoused REC to evaluate low back mus-cle performance in the presentstudy. In contrast to our initial ex-pectations, the results demonstratedhigher values for MFr and, conse-quently, for REC in subjects withpain than in subjects without pain(Tabs. 2 and 3). Accordingly, we sur-mise that these findings may haveinfluenced the lower level of forceexerted by subjects with pain duringthe MVC. In contrast to a study in
which the REC showed high discrim-inatory power and was probably themost important variable used in clas-sifying subjects with low backpain,12 in the present study, the RECfailed to show any such capacity topredict low back pain. However,when the REC was used in a predic-tion model with spectral variables, itwas found to be useful in discrimi-nating between subjects with andsubjects without low back pain(Tab. 4).
In recent years, there has been re-newed interest in developing a moreeffective method to objectivelyquantify muscle impairment causedby low back pain. In this context,most studies have shown that spec-tral variables are important in dis-criminant functions that identify lowback pain,3,12,2426 because they areable to identify the EMG pattern thatis typical of dysfunction and that canbe identified when muscle fatigue isinduced.
ConclusionThe results of this study support thesuppositions that people with no his-tory of performing regular physicalactivity and with pain in the lowback muscles show earlier manifes-tations of muscle fatigue thanhealthy people and that EMG can bea useful tool for diagnosing low backmuscle pain because the discrimi-nant function accurately classified89.5% of subjects with low backpain.
Table 4.Discriminant Analysis of Various Muscles for Correct Classification of Subjects With and Subjects Without Low Back Pain
MuscleVariables Used in theCorrect Classificationa
% Correct Classification by Group
Canonical CorrelationWith Pain Without Pain
Single low back muscle group Force, , y, , y 89.5 84.0 .745
, y, y, , REC 68.2 61.6 .325
Left longissimus muscle Force, y, y, REC 71.4 66.7 .442
a Variables are listed in descending order of discriminatory power. slope coefficient of a straight line that approached all 30 median frequency (MF)values, yy-intercept of a straight line that approached all 30 MF values, slope coefficient of a straight line that approached just the first and the last MFvalues, yy-intercept of a straight line that approached just the first and the last MF values, RECrecovery index.
Low Back Pain Assessment
1066 f Physical Therapy Volume 88 Number 9 September 2008 by guest on June 18, 2015http://ptjournal.apta.org/Downloaded from
Dr Candotti, Dr Loss, Dr Castro, Ms Melo,and Mr Araujo provided concept/idea/research design. Dr Candotti, Dr Loss, DrCastro, and Ms Melo provided writing andconsultation (including review of manuscriptbefore submission). Dr Candotti, Ms Pressi,Mr La Torre, Ms Melo, Mr Araujo, and MrPasini provided data collection and subjects.Dr Candotti, Dr Loss, Dr Castro, Mr La Torre,Ms Melo, Mr Araujo, and Mr Pasini provideddata analysis. Dr Candotti, Mr La Torre, MsMelo, and Mr Araujo provided project man-agement and facilities/equipment. Dr Can-dotti provided fund procurement and insti-tutional liaisons. Dr Loss provided clericalsupport.
This study was approved by the ethics com-mittee of Universidade do Vale do Rio dosSinos.
This article was submitted May 12, 2007, andwas accepted June 9, 2008.
DOI: 10.2522/ptj.20070146
References1 Gudavalli MR. Biomechanics research on
flexion-distraction procedure. In: Cox JM,ed. Low Back Pain: Mechanism, Diagno-sis and Treatment. 6th ed. Baltimore, MD:Williams & Wilkins; 1998:261272.
2 Dieen JH, Selen LPJ, Cholewichi J. Trunkmuscle activation in low-back pain pa-tients: an analysis of the literature. J Elec-tromyogr Kinesiol. 2003;13:333251.
3 Elfving B, Dedering A, Nemeth G. Lumbarmuscle fatigue and recovery in patientswith long-term low-back trouble: electro-myography and health-related factors. ClinBiomech. 2003;18:619639.
4 Dedering A, Nemeth G, Ringdahl KH. Cor-relation between electromyographic spec-tral changes and subjective assessment oflumbar muscle fatigue in subjects withoutpain from the lower back. Clin Biomech.1999;14:103111.
5 Smeets RJEM, Vlaeyen JWS, Hidding A,et al. Active rehabilitation for chronic lowback pain: cognitive-behavioral, physical,or both? First direct post-treatment resultsfrom a randomized controlled trial. BMCMusculoskelet Disord. 2006;7:5.
6 De Luca CJ. Use of the surface EMG signalfor performance evaluation of back mus-cles. Muscle Nerve. 1993;16:210216.
7 Orizio C. Muscle fatigue monitored byforce, surface machanomyogram andEMG. In: Nigg BM, MacIntosh BR, Mester J,eds. Biomechanics and Biology of Move-ment. Windsor, ON, Canada: Human Ki-netics; 2000:409433.
8 Roy SH, De Luca JC, Casavant DA. Lumbarmuscle fatigue and chronic lower backpain. Spine. 1989;14:9911001.
9 Dieen JH, Vrielink OHHE, Housheer AF,et al. Trunk extensor endurance and itsrelationship to electromyogram parame-ters. Eur J Appl Physiol. 1993;66:388396.
10 Larivie`re C, Arsenault BA, Gravel D, et al.Surface electromyography assessment ofback muscle intrinsic properties. J Electro-myogr Kinesiol. 2003;13:305318.
11 Falla D, Farina D. Muscle fiber conductionvelocity of the upper trapezius muscleduring dynamic contraction of the upperlimb in patients with chronic neck pain.Pain. 2005;116:138145.
12 Roy SH, De Luca C, Snyder-Mackler L, et al.Fatigue, recovery, and low back pain invarsity rowers. Med Sci Sports Exerc.1990;22:463469.
13 Moffroid M, Reid S, Henri S, et al. Someendurance measures in persons with lowback pain. J Orthop Sports Phys Ther.1994;20:8187.
14 Kankaanpaa M, Taimela S, Laaksonen D,et al. Back and hip extensor fatigability inchronic low back pain patients and con-trols. Arch Phys Med Rehabil.1998;79:412417.
15 Standards for reporting EMG data. J Elec-tromyogr Kinesiol. 1997;7:III.
16 Basmajian JV, De Luca CJ. Muscles Alive:Their Functions Revealed by Electromyo-graphy. 5th ed. Baltimore, MD: Williams &Wilkins; 1985.
17 Candotti CT, Guimaraes ACS, CardosoMFS. Detection of low-back pain in volley-ball players and non-athletes using EMG.Braz J Biomech. 2000;1:1519.
18 Candotti CT, Loss JF, Guimaraes ACS. Ef-fects of a muscle relaxation program onlow-back pain of gymnasts: an electromyo-graphic study. Braz J Biomech. 2005;10:1926.
19 Roy SH, Bonato P, Knaflitz M. EMG assess-ment of back muscle function during cy-clical lifting. J Electromyogr Kinesiol.1998;8:233245.
20 Essendrop M, Maul I, Laubli T, et al. Mea-sures of low back function: a review ofreproducibility studies. Phys Ther. 2003;4:137151.
21 Marras WS, Davis KG. A non-MVC EMGnormalization technique for the trunkmusculature, part 1: method develop-ment. J Electromyogr Kinesiol. 2001;11:19.
22 Lund JP, Donga R, Widmer CG, Stohler CS.The pain-adaptation model: a discussion ofthe relationship between chronic muscu-loskeletal pain and motor activities. CanJ Physiol Pharmacol. 1991;69:683694.
23 Pedersen TH, Nielsen OB, Lamb GD, Ste-phenson DG. Intracellular acidosis en-hances the excitability of working muscle.Science. 2004;305:11441147.
24 Elfving B, Liljequist D, Dedering A, Ne-meth G. Recovery of electromyographymedian frequency after lumbar muscle fa-tigue analysed using an exponential timedependence model. Eur J Appl Physiol.2002;88:8593.
25 Farina D, Gazzoni M, Merletti R. Assess-ment of low back muscle fatigue by sur-face EMG signal analysis: methodologicalaspects. J Electromyogr Kinesiol. 2003;13:319332.
26 Klein AB, Snyder-Mackler L, Roy SH, DeLuca C. Comparison of spinal mobility andisometric trunk extensor forces with elec-tromyographic spectral analysis in identi-fying low back pain. Phys Ther. 1991;71:445454.
Low Back Pain Assessment
September 2008 Volume 88 Number 9 Physical Therapy f 1067 by guest on June 18, 2015http://ptjournal.apta.org/Downloaded from
doi: 10.2522/ptj.20070146Originally published online August 8, 2008
2008; 88:1061-1067.PHYS THER. Arajo and Maicon PasiniMarcelo La Torre, Mnica de Oliveira Melo, Lucas DutraMaria Steffens Pressi, Flvio Antonio de Souza Castro, Cludia Tarrag Candotti, Jefferson Fagundes Loss, AnaBack MusclesElectromyography for Assessment of Pain in Low
References
http://ptjournal.apta.org/content/88/9/1061#BIBLfor free at: This article cites 23 articles, 2 of which you can access
Information Subscription http://ptjournal.apta.org/subscriptions/
Permissions and Reprints http://ptjournal.apta.org/site/misc/terms.xhtmlInformation for Authors http://ptjournal.apta.org/site/misc/ifora.xhtml
by guest on June 18, 2015http://ptjournal.apta.org/Downloaded from