Emerging zoonotic epidemics in the interconnected global...
7
The Veterinary Record, November 26, 2005 673 Animal and Human Health CHANGING LANDSCAPE OF INFECTIOUS DISEASE AT THE BEGINNING OF THE 21ST CENTURY In contrast with today, the period dur- ing the ‘cold war’ was characterised by few concerns over epidemic diseases. In the late 1960s, the Surgeon General of the USA, William H. Stewart, said that ‘. . . it was time to close the book on infectious diseases and pay more atten- tion to chronic ailments such as cancer and heart disease.’ Who was to doubt the Surgeon General? Smallpox was all but eradicated using a vaccine little changed from the one developed by Edward Jenner in the 1790s. Other dis- eases, such as measles in children and rinderpest in cattle, were also suc- cumbing to vaccination campaigns. A measure of that success came towards the end of the 1970s, when the world rejoiced that smallpox had become the first disease to be eradicated from the human species. Such halcyon days from the 1960s to the early 1980s are now only a memory. The turn of this century has brought with it a succession of disasters, both natural and man-made.We now live in a closely interconnected global commu- nity; a global society that has survived the ‘cold war’ only to be plunged into a ‘war on terrorism’. The emergence of Al Qaeda, the wars in Afghanistan and Iraq – and natural disasters such as the tsunami in Asia, the earthquake in Pakistan, and the hurricanes along the USA’s Gulf Coast – have overshadowed the large number of naturally occurring emerging diseases and epidemics that we have faced around the world in recent years. Amid all the disasters, perhaps we have failed to see the warning signs of possibly even bigger epidemics ahead. Laurie Garrett expressed her con- cern over newly emerging diseases in a ‘world out of balance’ as early as 1994 in ‘The Coming Plague’ (Garrett 1994). Avian influenza is one such threat today; a reminder to society of the potential of disease to wreck commu- nities and nations. It was noted that the earthquake that led to the Asian tsunami in 2004 literally rocked the earth’s rotation for a millisecond. In the 21st century, emerging zoonotic dis- eases have the potential – a possibility more than a probability – to devastate the global human population, the effect of which could be to ‘rock’ the earth for a century or more. Today, it has been estimated that 75 per cent of emerging diseases are zoonotic. Emerging diseases caused by viruses lead the charge of those that have shown their global reach since 1999 (Table 1). It is estimated that the rash of emerging or re-emerging livestock disease outbreaks around the world since the mid-1990s, including bovine spongiform encephalopathy (BSE), foot-and-mouth disease (FMD) and avian influenza, has cost the world’s economies over US $80 billion (Karesh and others 2005). EMERGENCE OF BIOTERRORISM AS A GLOBAL THREAT The attacks on the World Trade Center in New York and the Pentagon in Washington in September 2001 were followed quickly that October by the release of weapons-grade anthrax spores in the Capitol buildings. With the arrival of actual bioterrorism, not just the threat of it, at the heart of the US Government, a sea change has occurred in the way in which the USA and many other countries must view infectious diseases. A new dimension has been added to our concern. The natural biol- ogy, environmental stability and avail- ability of disease agents, and the ease with which they can be obtained, make several prime candidates (Table 1) as potential instruments of bioterrorism. Remember: (a) bioterrorism is not biowarfare, and extensive epidemics are not a prerequisite for creating great pub- lic anxiety; (b) while it is an old adage, it is still true that the only significant dif- ference between a naturally occurring epidemic and one that has arisen through bioterrorism is motive; and (c) Emerging zoonotic epidemics in the interconnected global community E. P. J. Gibbs The rate at which epidemics of zoonotic disease in humans have surfaced over the past 25 years has shaken – some would say shattered – the assumption that zoonotic diseases are under control, says Paul Gibbs. In this review he analyses the global factors that have led to the increased emergence of zoonotic diseases, sketches several recent epidemics (and where relevant, their relationship to bioterrorism), discusses the lessons learned, and concludes by outlining an agenda for action Veterinary Record (2005) 157, 673-679 E. P. J. Gibbs, BVSc, PhD, FRCVS, Professor of Virology, College of Veterinary Medicine, University of Florida, Gainesville, FL 32610, USA ● This article is based on the Wooldridge Memorial Lecture given by Professor Gibbs at this year’s BVA Congress, held at the Royal Society of Medicine from September 30 to October 1. While it attempts to be global in scope, the perspective inevitably draws upon the experience of the author in living both in the UK and the USA, strengthened by visits to many of the countries from which the diseases discussed in the review have emerged Portrait: Royal Society of Medicine At the start of his lecture, Professor Gibbs drew attention to a portrait of Edward Jenner that hangs on the walls of the Royal Society of Medicine. Jenner’s observation that the zoonotic character of cowpox could be used to protect against smallpox was, he suggested, ‘arguably the most important observation in the history of infectious disease’. In honour of Jenner’s scientific approach and the role of the cow in protecting mankind from smallpox, Louis Pasteur named the process of inoculation ‘vaccination’ (from vacca, Latin for cow) – appropriate recognition for the ‘one medicine’ for human and veterinary disease, as practised by Jenner and Pasteur
Transcript of Emerging zoonotic epidemics in the interconnected global...

The Veterinary Record, November 26, 2005 673
Animal and Human Health
CHANGING LANDSCAPE OF INFECTIOUS DISEASE AT THE BEGINNING OF THE 21ST CENTURY
In contrast with today, the period dur-ing the ‘cold war’ was characterised byfew concerns over epidemic diseases. Inthe late 1960s, the Surgeon General ofthe USA, William H. Stewart, said that ‘. . . it was time to close the book oninfectious diseases and pay more atten-tion to chronic ailments such as cancerand heart disease.’ Who was to doubtthe Surgeon General? Smallpox was allbut eradicated using a vaccine littlechanged from the one developed byEdward Jenner in the 1790s. Other dis-eases, such as measles in children andrinderpest in cattle, were also suc-cumbing to vaccination campaigns. Ameasure of that success came towardsthe end of the 1970s, when the worldrejoiced that smallpox had become the
first disease to be eradicated from thehuman species.
Such halcyon days from the 1960s tothe early 1980s are now only a memory.The turn of this century has broughtwith it a succession of disasters, bothnatural and man-made.We now live in aclosely interconnected global commu-nity; a global society that has survivedthe ‘cold war’ only to be plunged into a‘war on terrorism’. The emergence of AlQaeda, the wars in Afghanistan and Iraq– and natural disasters such as thetsunami in Asia, the earthquake inPakistan, and the hurricanes along theUSA’s Gulf Coast – have overshadowedthe large number of naturally occurringemerging diseases and epidemics that wehave faced around the world in recentyears. Amid all the disasters, perhaps wehave failed to see the warning signs ofpossibly even bigger epidemics ahead.
Laurie Garrett expressed her con-cern over newly emerging diseases in a
‘world out of balance’ as early as 1994 in‘The Coming Plague’ (Garrett 1994).Avian influenza is one such threattoday; a reminder to society of thepotential of disease to wreck commu-nities and nations. It was noted that the earthquake that led to the Asiantsunami in 2004 literally rocked theearth’s rotation for a millisecond. In the21st century, emerging zoonotic dis-eases have the potential – a possibilitymore than a probability – to devastatethe global human population, the effectof which could be to ‘rock’ the earth fora century or more.
Today, it has been estimated that 75 per cent of emerging diseases arezoonotic.
Emerging diseases caused by viruseslead the charge of those that haveshown their global reach since 1999(Table 1). It is estimated that the rash ofemerging or re-emerging livestock disease outbreaks around the worldsince the mid-1990s, including bovinespongiform encephalopathy (BSE),foot-and-mouth disease (FMD) andavian influenza, has cost the world’seconomies over US $80 billion (Kareshand others 2005).
EMERGENCE OF BIOTERRORISMAS A GLOBAL THREAT
The attacks on the World Trade Centerin New York and the Pentagon inWashington in September 2001 werefollowed quickly that October by therelease of weapons-grade anthrax sporesin the Capitol buildings. With the arrivalof actual bioterrorism, not just thethreat of it, at the heart of the US
Government, a sea change has occurredin the way in which the USA and manyother countries must view infectiousdiseases. A new dimension has beenadded to our concern. The natural biol-ogy, environmental stability and avail-ability of disease agents, and the easewith which they can be obtained, makeseveral prime candidates (Table 1) aspotential instruments of bioterrorism.Remember: (a) bioterrorism is notbiowarfare, and extensive epidemics arenot a prerequisite for creating great pub-lic anxiety; (b) while it is an old adage, itis still true that the only significant dif-ference between a naturally occurringepidemic and one that has arisenthrough bioterrorism is motive; and (c)
Emerging zoonotic epidemics in theinterconnected global communityE. P. J. Gibbs
The rate at which epidemics of zoonotic disease in humans have surfacedover the past 25 years has shaken – some would say shattered – theassumption that zoonotic diseases are under control, says Paul Gibbs. In this review he analyses the global factors that have led to the increasedemergence of zoonotic diseases, sketches several recent epidemics (andwhere relevant, their relationship to bioterrorism), discusses the lessonslearned, and concludes by outlining an agenda for action
Veterinary Record (2005)157, 673-679
E. P. J. Gibbs, BVSc, PhD,FRCVS,Professor of Virology,College of VeterinaryMedicine, University ofFlorida, Gainesville,FL 32610, USA
● This article is basedon the WooldridgeMemorial Lecturegiven by ProfessorGibbs at this year’s BVA Congress, held atthe Royal Society ofMedicine fromSeptember 30 toOctober 1. While itattempts to be globalin scope, theperspective inevitablydraws upon theexperience of theauthor in living bothin the UK and the USA,strengthened by visitsto many of thecountries from whichthe diseases discussedin the review haveemerged
Portrait: R
oyal Society of M
edicine
At the start of hislecture, Professor Gibbsdrew attention to aportrait of EdwardJenner that hangs onthe walls of the RoyalSociety of Medicine.Jenner’s observationthat the zoonoticcharacter of cowpoxcould be used to protectagainst smallpox was,he suggested, ‘arguablythe most importantobservation in thehistory of infectiousdisease’. In honour ofJenner’s scientificapproach and the roleof the cow in protectingmankind from smallpox,Louis Pasteur namedthe process ofinoculation ‘vaccination’(from vacca, Latin forcow) – appropriaterecognition for the ‘onemedicine’ for humanand veterinary disease,as practised by Jennerand Pasteur

674 The Veterinary Record, November 26, 2005
Animal and Human Health
there is always a possibility that bio-terrorism could arise through a novelrecombinant virus created purely for thepurpose of bioterrorism. Were an attackto occur with a novel agent, the effi-ciency of the first response would becritical to nip the epidemic in the bud.Looking for the unknown enemy overthe horizon has always been difficult!
FACTORS PROMOTINGINCREASED NUMBERS OF EPIDEMICS IN THE 21ST CENTURY
There are myriad interconnected fac-tors influencing the increasing rate atwhich diseases have emerged in recentyears, including:
● Extensive global trading and tourismpatterns of the late 20th century(pathogens as hitchhikers);● Speed of mass transportation (lessthan disease incubation time, soinfected people can travel undetected);● Exposure to new pathogens throughecosystem disruption (human popula-tion pressures; exposure to wildlife);● Intensification and monoculture infarming (potentially leading to viralamplification);● Technical sophistication in food processing, masking its true origins(individuals cannot exercise innate pro-tective responses); and● Evolutionary pressures throughoverpopulation and change in tropism(intensive agriculture).
Often we do not truly understandthe unique combination of factors that
promotes an epidemic of human dis-ease. However, a dispassionate analystquickly recognises the ever increasingpopulation of one species, man, and thesuccess of this species in the 21st cen-tury in colonising virtually the entireland surface; gaining the ability to travelquickly around the world and in largenumbers; and establishing a complexnetwork of global trading. These areimportant factors in explaining theincreasing rate of zoonoses in the 21stcentury.
With so many infectious agentsarguably still waiting to be discovered,defining the probability that a specificdisease will emerge is impossible. Whatis evident is that the ever increasinghuman population brings the speciesinto greater contact with animals, andgreater global connectivity providesrapid dissemination of infectious dis-eases from the initial focus. Whereas inprevious centuries a disease focus mighthave died out through failing to estab-lish a chain of transmission, now it hasthe opportunity to rapidly recruit sus-ceptible hosts on a global stage. To drawan analogy, there is now so much avail-able tinder on the forest floor that theflickering early flame can rapidly befanned into a forest fire.
In support of this thesis, considerthe following:
● The human population of Earthtook until 1800 to reach one billion; by2000 it had exceeded six billion;● In 1800, the time taken to circum-navigate the globe by sailing ship wasapproximately one year. Today, no twocities served by commercial aircraft aremore than 24 hours apart;
● Annually, the world’s airlines carry atotal approaching two billion passen-gers. At any one moment, about half amillion people worldwide are flying incommercial aircraft (Select Committeeon Science and Technology 2000);● In 2003, there were 200 million passenger departures/arrivals at Britishairports; and ● In lieu of precise trade data, BillyKaresh of the Wildlife ConservationOrganization in New York conserva-tively estimates that in east and south-east Asia, tens of millions of wildanimals are shipped each year region-ally and from around the world, forfood or use in traditional medicine(Karesh and others 2005). Live turtlesare even shipped to the markets ofChina from Florida.
CASE STUDIES OF RECENTEPIDEMICS AND THE LESSONS LEARNED
The following overview of epidemics,from 1999 to 2005, focuses on the USA.It illustrates many of the points raisedearlier. By and large, the reactions of thegovernment and citizens of the USA
reflect those of any country. Table 2gives the timeline and the reactionwithin the USA to the events.
1999: West Nile encephalitis inNorth AmericaWhen West Nile virus was confirmed asa cause of encephalitis in humans inNew York in 1999, the pernicious effectof the Surgeon General’s remarks in the1960s, and the consequent extent of theneglect of public health in the USA, were
Animal health Zoonotic Significant bioterrorism Priority diseases impact potential potential Concerns
West Nile encephalitis +++ +++ No Will it spread in Europe? What of the future in South America?
Foot-and-mouth disease (FMD)† ++++ +/– Yes When and how might FMD reappear in Europe or the USA?
Severe acute respiratory – +++ Yes When might this sleeping dragon of Asia syndrome (SARS) re-awake?
Monkeypox + ++ Yes Could it be smallpox next?Bovine spongiform encephalopathy +++ ++ Yes A diminishing epidemic in both cattle
and humans?Bluetongue +++ – No Is global warming aiding spread of the
virus into Europe?Avian influenza ++++ ++++‡ Yes Truly the enemy at the gate of the
H5 and H7 serotypes Western World?
Unknown agent created through ++++ ++++ Yes Technically feasible. The USSR reportedlybiotechnology for use as a developed a smallpox/Ebola recombinantbioterrorist weapon virus
* For brevity, several emerging diseases are not mentioned. The most important is AIDS, the causal virus of which is HIV. HIV is believed tohave its origins in primates in West Africa and thus should also be considered a zoonotic disease. The table also omits several zoonotic viraldiseases, such as Ebola and Nipah virus, which have remained largely localised in Africa and Australasia, respectively, but have the potentialfor pandemic spread† While FMD rarely causes human infection, the draconian ‘stamping out’ strategies to control disease can cause anxiety and grief of publichealth significance‡ Only if adaptation to humans and effective transmission occurs
TABLE 1: Simple analysis of the relative importance and epidemic potential of several emerging diseases*

The Veterinary Record, November 26, 2005 675
finally realised.West Nile virus had neverbeen recorded previously in the WesternHemisphere, and no one had ever con-sidered that it could be introduced.
St Louis encephalitis (SLE) virus, avirus related to West Nile virus andendemic to the USA, was initially diag-nosed as the cause of the epidemic,until an astute veterinarian at the Bronxzoo noticed that several native birdswere dying. Since SLE virus is not recog-nised as pathogenic for indigenousbirds in the USA, the observation quicklyled to the correct identification of thevirus. The delays, first in recognisingthat an epidemic of human encephali-tis was underway in New York (caseswere occurring in several boroughs andwere not initially recognised as linked),and, secondly, in identifying the causalvirus, contributed to problems inimplementing aggressive attempts tocontrol the mosquito vectors and, as aresult, the virus successfully overwin-tered. Each subsequent year the virusspread geographically, and by 2004 thevirus had spread widely across the con-tiguous states of the USA, severalprovinces of Canada, and south to theCaribbean and Mexico. By 2004, over15,000 horses were known to have diedof West Nile encephalitis in the USA. In
2003 and 2004 alone, there were over12,000 confirmed cases of West Nileinfections in humans, with 362 deaths.
Molecular analyses of West Nileviruses from many different geographi-cal sites around the world indicated thatit might have been introduced fromIsrael. The precise origin and method bywhich the virus arrived in the USA areunknown. It is most likely that aninfected mosquito arrived on a flightfrom the Middle East. In contrast withaircraft arriving in Australia, the cabinspaces of intercontinental flights enter-ing the USA are not routinely sprayedwith insecticide before entering the USA.
2001: Foot-and-mouth diseasein EuropeIt may seem surprising to see FMD dis-cussed in this review. While FMD viruscan cause human disease, this is onlyrarely reported, even during extensiveepidemics in domestic livestock. WhenFMD occurs in a country that is nor-mally free of disease and that does not vaccinate its livestock, a ‘runaway’epidemic can ensue. To control the epidemic, a draconian ‘stamping out’policy is usually imposed. This is what happened in the UK and theNetherlands in 2001. The psychologi-
cal impact (sometimes even leading tosuicide) of seeing one’s herd slaugh-tered makes this a disease of publichealth importance beyond zoonoticinfection.
The stamping out of FMD in Europein 2001 was carried out in the dailyspotlight of the world’s television cam-eras. Many evenings in the USA, it wasthe lead story for the prime-time news.‘FMD’ even made it as one of the top 10new words for CNN in 2001. The extentof the slaughter in the UK, necessary tocreate the ‘firebreaks’ around infectedfarms, was horrific to most viewers. Forthose in government in the USA, thisreaction illustrated the power of themedia to lead public opinion, sensitisedthem to the genuine anguish of societyover animal welfare and stamping outpolicies, and illustrated the logisticalcomplexity of disease control and car-case disposal. The controversies thatarose through the use of extensiveslaughter to control the epidemic andhow, in turn, the concerns of society arebeing translated into a radical change inpolicy within the European Union (EU)for the control of FMD and other exoticanimal diseases, have been noted withkeen interest by countries outside theEU.
Before the terrorist attacks on theWorld Trade Center and the Pentagonand the intentional release of anthraxspores in Washington DC in the autumnof 2001, the risk that food productionwould be targeted by bioterrorists wasof concern only to those who had inti-mate knowledge of animal and plantpathogens. While there is no evidenceto believe that the epidemic of FMD inthe UK, and its subsequent extension tocontinental Europe, was caused bybioterrorism, the extent of the epidemicindicated to many in the USA that FMD
could be a very powerful bioterroristweapon in causing widespread diseasein livestock and economic disruptionfor the targeted country. Further, whilethe public’s health remains the first pri-ority of the nation, the importance ofprotecting the food supplies has notbeen ignored. The US government,in common with others, takes the threat of a bioterrorist attack using FMD very seriously. For example, theresearch centre for FMD on Plum Island, formerly in the Department ofAgriculture, now has a new administra-tive home in the Department ofHomeland Security, and informationon the stockpile of FMD vaccines is nowrestricted.
The epidemic of FMD in Europe in2001 provided important lessons in thecontrol of highly infectious animal diseases in large populations, and theexpectations of modern society inindustrialised nations.
Animal and Human Health
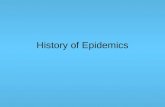
Cattle carcases burning on a farm inGloucestershire duringthe 2001 foot-and-mouth diseaseoutbreak. Such images,widely disseminated bythe media, horrified thepublic, and had animpact on animaldisease control policiesthat extended wellbeyond the UK
Photograph: B
arry Batchelor/P
A/E
mpics
Year Event Comment from USA perspective
1999-ongoing West Nile virus arrives in New York The poor state of preparedness of national public health services in the USA is realised
2001 Foot-and-mouth disease hits UK Reality check! Is the USA equally unprepared?9-11 attack on the World Trade Center War on terrorism beginsAnthrax bioterrorism hits Washington DC The nation feels vulnerable
2003 SARS pandemic Canada is hit hard, but the USA is luckyMonkeypox in the Mid West Could it have been a bioterrorist attack using smallpox?
Do we truly import wildlife from Africa with no import restrictions or health checks?
BSE Did we say we would never get it?2004 H5N1 avian influenza explodes in Asia Some human cases and deaths. Fear of pandemic human
influenza rises2005 H5N1 avian influenza spreads to more Virus adapts to village poultry, ducks and wild birds. More
countries in Asia and then to Europe human cases. Fear of human pandemic increases as migratory birds spread the virus to Europe
TABLE 2: Timeline of epidemic zoonoses of the 21st century from the perspective of the USA
▼

676 The Veterinary Record, November 26, 2005
2003: Severe acute respiratorysyndromeIn an average winter, significant humanmortality is associated with influenza.Death is seen mostly in the elderly fromcomplications such as pneumonia (inthe USA, there are approximately 30,000influenza-related deaths each year). Thewinter of 2002/03 in the NorthernHemisphere was relatively quiet forinfluenza, but a respiratory disease, nowknown as severe acute respiratory syn-drome (SARS) emerged, causing humandeaths in several countries around theworld. While the disease, which is nowknown to be caused by a novel corona-virus, did not cause a major epidemic,either in the UK or the USA, it had a sig-nificant impact in Asia and in localisedareas worldwide. The World HealthOrganization (WHO) declared the epi-demic over in mid-July. A total of 916people died, mostly in China. In NorthAmerica, the Canadian city of Torontobecame the focus of attention as SARS
spread within several hospitals, causing41 deaths. At one time, travellers wereadvised by the WHO to avoid travelling toToronto. Quarantine for the control ofhuman disease fell into disuse in the lat-ter half of the 20th century, but was re-introduced on a limited scale to controlSARS. It was largely voluntary quarantine,but governments quickly reviewed theirlegislative authority to impose manda-tory quarantines on their citizens.
The origin of the virus appears tohave been Guangdong Province inChina, but only when the diseaseappeared in Hong Kong was thisemerging disease recognised. HongKong is a major airport hub for Asia,and international travellers in the incu-batory phase of the disease are believedto have disseminated the virus widelyfrom Hong Kong. The causative viruswas quickly recognised as a novel coro-navirus using traditional and molecu-lar diagnostic techniques. Unlike manycoronaviruses, SARS virus replicates withcytopathic effect in Vero cells, thus sim-plifying study.
Since so many coronaviruses arecapable of causing disease in domesticanimals, the possibility that the SARS
virus could have originated in wild ani-mals was quickly investigated. Wild ani-mals are still widely used in traditionalChinese cuisine and sold caged in mar-kets. Coronaviruses that appear to bevery closely related to SARS virus havebeen isolated from masked palm civets(Paguma larvata) and raccoon dogs(Nyctereutes procyonoides) sampled inChinese markets. The true reservoir ofthe virus has recently been identified asthe Chinese horseshoe bat (Rhinolophussinicus) (Lau and others 2005).
A US National Intelligence Councilreport stated that, even though SARS has
infected and killed far fewer peoplethan other common infectious diseasessuch as influenza, malaria, tuberculosis,and HIV/AIDS, it has had a dispropor-tionately large economic and politicalimpact. This is because it spread inareas with broad international com-mercial links and received intensemedia attention as a mysterious new ill-ness that seemed able to go anywhereand hit anyone. As the first infectiousdisease to emerge as a new cause ofhuman illness in the 21st century, SARS
underscores the growing importance ofhealth issues in a globalised world (US
National Intelligence Council 2003).
2003: Monkeypox infectshumans in the USAThe SARS epidemic illustrated theimportance of wildlife as a source ofzoonotic viruses, and the extent of theinternational trade in wildlife speciesfor food and traditional medicine. Anoutbreak of a pustular pox disease, thatwas similar to very mild cases of small-pox, in pet owners and handlers(including a veterinarian) in the USA inearly summer of 2003, raised alarm andalso pointed to the importance ofwildlife species in zoonotic disease.
The disease was quickly diagnosedas monkeypox, an uncommon diseaseusually restricted to West and CentralAfrica. The disease was first recorded inthe 1950s in monkeys, hence its name.Subsequently, the virus was recognisedin the 1970s as a cause of a disseminatedpustular skin disease in humans similarto smallpox (but less severe) in the samegeographical areas as the affected mon-keys. The causal virus is an orthopoxvirus closely related to smallpox, vac-cinia and cowpox viruses. Epidemiol-ogical studies of monkeypox have nowestablished that rodents are the reser-voir of the virus and that the disease inmonkeys and humans is incidental. Thespecific role of any particular species as
a reservoir has not been established.While the virus can be transmittedfrom monkeys to humans, and indeedfrom one human to another, a continu-ous chain of transmission is not estab-lished.
Following the use of anthrax for ter-rorism in October 2001, the public inthe USA had been warned that smallpoxcould be used with far greater effectthan anthrax. The risk of a terroristusing smallpox virus has been takenseriously; many first responders andmedical staff throughout the USA havebeen vaccinated. Considering the clin-ical similarity between early cases ofsmallpox and monkeypox, reports ofdisease in humans early in May 2003understandably caused alarm. Couldthis be smallpox? Such fears were rela-tively quickly dismissed once the virushad been characterised. However, theporous nature of the nation’s borders tothe introduction of the virus and theease with which it was spread were bothalarming features of the outbreak. Atthe time, there were no restrictions onthe importation of wild rodents fromWest Africa.
The source of the outbreak wastraced to a legal importation of approx-imately 800 small mammals fromGhana in West Africa to Texas in April2003. The consignment contained 762African rodents, including rope squir-rels (Funisciurus species), tree squirrels(Heliosciurus species), Gambian giantrats (Cricetomys species), brushtail por-cupines (Atherurus species), dormice(Graphiurus species) and striped mice(Hybomys species). The importedrodents were then distributed to severalstates. Native pet prairie dogs (Cynomysspecies) housed near some of theserodents in a distributor’s premises inIllinois became infected, and it was thesubsequent distribution, exhibition andsale of the prairie dogs that spread thevirus to people.
Animal and Human Health
Life goes on . . . awedding in Hong Kongduring the SARSoutbreak in 2003
Photograph: V
incent Yu/A
P/E
mpics

The Veterinary Record, November 26, 2005 677
The Centers for Disease Control(CDC) reported that the illness inprairie dogs was reported to includefever, cough, conjunctivitis and lym-phadenopathy, followed by a nodularrash. Some prairie dogs died, whereasothers apparently recovered. CDC lab-oratory testing of some animals fromthe original shipment of rodents fromWest Africa confirmed the presence ofmonkeypox virus in one Gambian rat,three dormice and two rope squirrels.The Gambian giant rat, believed to bethe index case in the USA, apparentlyexperienced a much milder illness thanthat observed in prairie dogs, with norespiratory signs and limited skinlesions.
A total of 71 cases of monkeypox inhumans was reported. The CDC com-mented that while infection in humansmay be acquired through the respira-tory system, most of the human cases inthis outbreak appeared to have acquiredinfection through the skin. The route oftransmission in animals is less clear.The virus might have been transmittedby aerosol, through skin abrasions, orthrough the ingestion of infected ani-mal tissues.
To prevent the introduction of fur-ther infected rodents into the USA, andto control the distribution of poten-tially infected prairie dogs, the federalgovernment banned, in mid-June, theinterstate movement, sale, exhibitionand release into the environment ofprairie dogs, and those species of WestAfrican rodents already in the USA aslisted above. The order also banned theimportation of all rodents from WestAfrica. The outbreak illustrated thathistorically there has been little over-sight of international trade in pet ani-mals and wildlife species in the USA, andalso that there is no single agency withjurisdiction.
2003: BSE in the USAThe first recognition in the USA inDecember 2003 of BSE, or mad cow dis-ease as it is most commonly called inthe popular press, in a cow previouslyimported into the USA from Canada,was unexpected. Because of the com-plexity of cattle marketing in NorthAmerica, the historical reluctance of thecattle industry to support a robust ani-mal identification scheme, and the sub-sequent confirmation of a second casein a cow born in Texas, the USA hasjoined the list of those countries con-sidered infected with BSE.
BSE was first identified in the UK in1986 and recognised to be caused by aprion. The extensive epidemic of BSE inthe UK is believed to have been associ-ated with cattle feed supplemented withmeat and bone meal infected with pri-ons. However, it was not until 1996 thatan association was made between BSE
and a newly recognised encephalopathyaffecting young people that becameknown as variant Creutzfeldt-Jacob dis-ease (vCJD). The assumption is that vCJD
is acquired through eating infectedbeef. Since that time, cases of BSE havebeen recognised in cattle born in mostcountries of Europe, Japan and Canada.The incubation period for all prion dis-eases is long and partly determined bythe genotype of the individual, thus theextent of the epidemic of vCJD cannotbe predicted (so far, there have beenapproximately 158 cases in the UK). Theearlier estimates of many thousands ofyoung people developing this fatal dis-ease appear to have been wrong; never-theless, the public fear of vCJD, once BSE
is discovered in a country, has invari-ably had an enormous economicimpact extending far beyond the beefindustry. The economic impact of BSE
has been and continues to be enormousin the UK, but the USA, despite surveil-
lance evidence to indicate that BSE is notextensive in the cattle population, hasfailed to convince Asian buyers to opentheir markets to American beef and thecattle industry is currently losing anestimated US $10 billion per annum inexport sales.
The history of BSE and the biologicaland ecological enigmas posed by prion-associated diseases have highlighted theneed to study the transmissible spongi-form encephalopathies (TSEs) in greaterdetail. Since the 1970s, the USA has alsohad to contend with the problem ofchronic wasting disease (CWD) of deer.This disease, which occurs both in free-living deer and farmed deer over a widearea in both the USA and Canada, doesnot appear to cause disease in humans,but there is an abiding concern thatCWD could also be a public health issue.The control of CWD is a priority withinthe USA and Canada for wildlife andregulatory officials.
A quote from MacKenzie (2004) – ‘Itstarted out as a British disease, but theUK exported it and then its trading part-ners spread it even further afield. Nowno country can be sure it has kept BSE
out. Mad cows have gone global’ – isarresting. Fortunately, the global epi-demic of BSE is, in the opinion of many,now over. Because of the prolongedincubation period, and the stablenature of prions, we can expect to seeoccasional cases of BSE and possiblyvCJD occurring in countries around theworld for many years. However, pre-vention of the cycling and amplificationof prion materials through the supple-mentation of cattle feed with meat andbone meal has been identified as thefocal point for preventing BSE epi-demics, and such supplementation isnow proscribed in most countries ofthe world. But if BSE can occur sponta-neously, as many believe is possiblethrough gene mutation, increased sur-veillance may detect occasional cases inold animals even in the presence ofeffective feed bans. While extensivehuman exposure to prion material, asoccurred in the UK in the late 1980s andearly 1990s, is unlikely to occur, vigi-lance is needed. The use of prions forbioterrorism should not be ignored.
2004 and 2005: Avian influenza(H5N1) in south-east AsiaWhile it is unlikely that another epi-demic akin to that of vCJD in the UK, ofa TSE arising from an animal source, willever occur in humans, this cannot besaid for highly pathogenic avianinfluenza. The threat of mutation of theavian influenza (H5N1) virus that iscausing disease in south-east Asia (andnow Europe), so that it can be success-fully be transmitted between humans, isof great concern. Although by the mid-
Animal and Human Health
Black H’mong womenpursue traditional craftsin north-west Vietnam.As in other parts ofAsia, much of the ruralpopulation of Vietnamlive in close contactwith their livestock(chickens, ducks, waterbuffaloes and pigs)
Photograph: P
aul Gibbs

678 The Veterinary Record, November 26, 2005
dle of November 2005 only 130 con-firmed cases of avian influenza virusinfections of humans had beenreported in people in Asia sinceDecember 2003, the mortality rate hasbeen very high, with 67 deaths (WHO
2005). No convincing evidence exists tosuggest that mutation of the virus toallow human-to-human infection hasoccurred, but the ecology and currentvirus load in the poultry of south-eastAsia significantly elevate the risk of thisoccurring. If the H5N1 virus were tomutate to permit efficient transmissionbetween humans, and if it were to retainthe ability to cause a mortality rate sim-ilar to that of the current infections, theensuing pandemic could be horrific.The Spanish influenza pandemic of1918, which is believed to have killedapproximately 50 million people, hadan overall mortality rate of approxi-mately 2 per cent; the current mortalityrate of H5N1 avian influenza virus inhumans is around 50 per cent.
Since the first identification of H5N1
as a human pathogen in Hong Kong in1997, the virus has widely establisheditself in the chicken, and more recentlythe duck, populations of the rice grow-ing areas of south-east Asia. The‘nomadic’ ducks of the villages are clin-ically normal reservoirs of infection.Earlier in 2005, it was estimated that asmany as 10 per cent of the ducks in theRed River delta of north Vietnam wereshedding infectious virus (T.Van Dung,personal communication). The ducksoften scavenge with the village chickensand pigs, which both may amplify thevirus. The ducks, chickens and in someareas possibly the pigs as well, are anenormous source of potential infectionfor the villagers who unknowinglyexpose themselves by close contact,when killing and preparing poultry formeals, and specifically when ingestinguncooked duck blood on festive occa-sions. The veterinary authorities incountries such as Vietnam have encour-aged the villagers to reduce the duckherds, but the ducks are valuable to theeconomy of the village as gleaners offallen rice after harvesting and for con-trol of the snail and insect populationsin the rice fields.
The recent movement of H5N1 virusinto Europe with infected migratoryand imported wild birds is of great con-cern to Europe’s poultry industry. Themigration patterns of the wild birdsalso extend to Africa; thus H5N1 may, inthe waning months of 2005, have thepotential to be a pandemic avianpathogen. Amid the intense focus onthe risk of pandemic human influenza,it is often overlooked by the media thatthe virus can cause very high mortalityrates in domestic poultry and possiblyselected species of wild birds. Certainly,
there is a risk in Europe that the virusmay cause clinical disease in people inclose contact with wild birds and poul-try, and further that the feared muta-tion to allow the virus to be transmittedbetween people could occur in Europe.However, because of the high infectionrates (that is, virus load) in the poultrypopulations of south-east Asia, and theintimacy of the relationship betweenpeople and birds in the region, it ismore probable that Europeans will be affected by a pandemic humaninfluenza strain that arrives with aninfected international human travelleron a commercial flight from Asia, ratherthan from a mutation occurring in avirus that has arrived in a migratorybird.
Virologists and epidemiologists havebeen following the deepening problemof H5N1 in Asia since 1997, and haverepeatedly warned of the emerging riskof a pandemic of human influenza. Totheir credit, the countries of the regionhave wrestled with the problem andinvested heavily to control the disease intheir poultry, but most are developingcountries and lacking resources. Untilrecently, there has been little concertedfinancial support from the interna-tional community in support of theseprogrammes. The presence of H5N1 insouth-east Asia has never been just aregional problem; it has merited atten-tion as a global threat since 1997. In-depth studies are needed to investigatethe epidemiology of the disease in Asia.It is not necessarily the same in eachcountry. Socioeconomic analyses areneeded to optimise disease control pro-grammes in the communities. Let ushope history does not record that ear-lier international intervention in south-east Asia might have prevented acatastrophic pandemic of influenza.
The Spanish influenza epidemic of1918, the reference point for our con-cern that a pandemic is possible with
H5N1, is now believed to have beencaused by a virus that mutated from anavian host to infect humans. Relative tothe emergence of H5N1 in Asia, it isappropriate to note a parallel emer-gence of influenza virus in dogs(Crawford and others 2005). In 2004and again in 2005, epidemics of canineinfluenza occurred across the USA. Thevirus has maintained itself by dog-to-dog transmission and now appears tobe endemic. Similar in character to theSpanish influenza in humans in 1918and cases of H5N1 infections in humansin south-east Asia, some affected dogsdie acutely of a haemorrhagic pneumo-nia. This was the first time that aninfluenza epidemic had ever beenrecorded in dogs. The causal virus hasbeen identified as H3N8 and by molec-ular analysis is closely related to equineinfluenza virus. The origin of the virusremains unexplained, but the exampleillustrates the promiscuous nature ofinfluenza virus to ‘jump species’ andfurther justifies the concern over thepotential of the H5N1 strain of avianinfluenza to initiate pandemic influenzain humans.
WHAT HAVE WE LEARNED ANDHOW ARE WE RESPONDING?
A summary of the lessons learned fromeach of the epidemics mentioned aboveis presented in Table 3. It is beyond thescope of this review to discuss them indetail, but the following are examples ofpolitical and scientific action in the UK
and USA.
● Creation of the Department ofEnvironment, Food and Rural Affairs inthe UK during the FMD epidemic.● Creation of the Department ofHomeland Security in the USA shortlyafter the 9/11 and anthrax attacks.● Presidential Directive HSPD-9 on
Animal and Human Health
Year Event Lessons learned/actions initiated by event
1999 West Nile virus arrives in New York Greater coordination of public health services, improved research and diagnostics
2001 Foot-and-mouth disease hits UK Worldwide, biosecurity is seen as important and the food supply of nations is seen as vulnerable to bioterrorism. The power of the media to direct public opinion to question disease control policies is realised
9/11 and anthrax bioterrorism in the USA Preparedness for bioterrorism accelerates. The USA ‘declares war’ on terrorism
2003 SARS pandemic Global surveillance and international cooperation needs improvement. There is increasing awareness of the importance of wildlife in zoonoses
Monkeypox in the USA Problems of jurisdiction and the need for concerted action in regulating international trade in wildlife
BSE in the USA Awareness of international sensitivity and trade. The interface of complex biology and complex trade
2004/05 H5N1 avian influenza explodes in Asia All of the above. Need for financial support for developing countries. The importance of international agencies such as the World Health Organization and the Food and Agricultural Organization of the United Nations
TABLE 3: Lessons learned from epidemics of the 21st century

The Veterinary Record, November 26, 2005 679
Defense of the USA’s Agriculture andFood against terrorist attacks, majordisasters and other emergencies in theUSA.● Coordination of laboratory net-works across the USA;
● Creation of State AgriculturalResponse Teams (SART);● Identification of select agents in con-junction with the CDC; and● US funding for research on emergingdiseases structured to come largelyfrom bioterrorism preparedness.
However, notwithstanding the cur-rent drive to address both emergingzoonotic diseases and bioterrorism, theTrust for America’s Health and the US
National Academies are critical of theability of the USA to respond to animal-borne epidemics, as detailed below.Other nations can probably identify asimilar list.
● The USA lacks a national programmeto prevent and control diseases thatimpact humans, animals and our food.● There is no coordinated effort or sin-gle agency with a ‘command and con-trol’ responsibility.● There is a lack of effective commu-nications with the public about thesediseases and their impact.● Disease surveillance systems are notlinked.● Funding to combat bioterrorism hasnot adequately supported efforts tocounter zoonotic disease threats, espe-cially from the animal health perspec-tive and infrastructure.● There is a fragmentation of jurisdic-tions, authorities, statutes and research;for example, there are 200 different government offices and programmesresponding to five zoonotic diseases.● Animal and public health are sepa-rated by culture and organisation
So how did this situation arise?Certainly, for reasons mentioned at thestart of this review, neglect of the pub-lic health services and regulatory vet-erinary medicine had begun in the late1960s, with consequent intellectualimpoverishment in the disciplines ofinfectious disease and epidemiology.This situation was accelerated in the1980s by the leaders of the UK and USA.Margaret Thatcher and Ronald Reaganwere the architects of the downfall ofcommunism and the end of the ‘coldwar’; for this they should be applauded.They also championed reduced taxa-tion, and cut government expenditurein the hope that they could reducebureaucracy and improve efficiency.With regard to the USA, as a conse-quence:
● Individual states have shouldered
greater responsibility, but have hadproblems due to the unfunded man-dates;● Public and animal health serviceswere drastically reduced in the 1980sand 1990s;● There has been inadequate supportfor developing countries to promotepublic and animal health; and● The UN (and its agencies) hasbecome a ‘whipping boy’ for ineffi-ciency.
AGENDA FOR ACTION
Because of the myriad interconnectedfactors that promote the emergence ofdiseases, many of the actions needed forthe control and prevention of emergingdiseases and zoonoses are multidisci-plinary and far wider than simple vet-erinary responsibility. Several representan agenda for social reform: humanpopulation control; sustainable devel-opment; balanced farming, with farm-ers as stewards of the land; greatercommitment to and support of inter-national agencies; coordination ofemergency response at the global level;economic support to the developingworld; and improved communicationswith the public. In response, the publichas a responsibility in meeting the challenge of emerging diseases andzoonoses by becoming informed andengaged in seeking relevant socialreform.
At the veterinary level, we must pro-mote cross-disciplinary science; address‘ecology more than economy’; recog-nise the importance of wildlife as reser-voirs of infection; improve vaccines anddiagnostic tests; train and consult fieldepidemiologists as well as molecularscientists and modellers; improve andcoordinate surveillance of disease at theglobal level; and improve communica-tion with the public on the importanceof disease control.
Whether we are involved in clinicalpractice, research, regulatory medicine,academia or industry, our role as vet-erinarians and allied professionals, inmeeting the challenge of emerging dis-eases and zoonoses, is to inform andeducate at all levels, wherever andwhenever we can. We also need torecognise the power of nature, whetherit takes the form of epidemics, hurri-canes or earthquakes, and be ready torespond. The early events of the 21stcentury have taught us that we must tryharder.
ACKNOWLEDGEMENTS
I would like to thank Dr BobMcCracken and Professor Tim Greet,
past-presidents of the BVA, for inviting me to present the 2005 WooldridgeMemorial Lecture, on which this arti-cle is based.
ReferencesCRAWFORD, P. C., DUBOVI, E. J., CASTLEMAN,
W. L., STEPHENSON, I., GIBBS, E. P. J., CHEN,L., SMITH, C., HILL R. C., FERRO, P., POMPEY,J., BRIGHT, R. A., MEDINA, M., INFLUENZAGENOMICS GROUP, JOHNSON, C. M.,OLSEN, C. W., COX, N. J., KLIMOV, A. I., KATZ,J. M. & DONIS, R. M. (2005) Transmission ofequine influenza virus to dogs. Science 310, 482-485
GARRETT, L. (1994) The Coming Plague. NewYork, Farrar, Straus and Giroux. pp 1-750
KARESH, W. B., COOK, R. A., BENNETT, E. L. &NEWCOMB, J. (2005) Wildlife trade and globaldisease emergence. Emerging Infectious Diseases11. www.cdc.gov/ncidod/EID/vol11no07/05-0194.htm. Accessed October 28, 2005
LAU, S. K. P., WOO, P. C. Y., LI, K. S. M., HUANG,Y., TSOI, H., WONG, B. H. L., WONG, S. S. Y.,LEUNG, S., CHAN, K. & YUEN, K. (2005) Severeacute respiratory syndrome coronavirus-likevirus in Chinese horseshoe bats. Proceedings ofthe National Academy Sciences USA 102, 14040-14045
MACKENZIE, D. (2004) American nightmare.New Scientist 2459, August 7, 2004. www.new-scientist.com/article.ns?id=mg18324595.400.Accessed October 28, 2005
NATIONAL ACADEMIES PRESS (2005) AnimalHealth at the Crossroads: Preventing, Detecting,and Diagnosing Animal Diseases. www.nap.edu/catalog/11365.html. Accessed October28, 2005
SELECT COMMITTEE ON SCIENCE ANDTECHNOLOGY (2000) Fifth Report to the UK
Parliament. www.parliament.the-stationery-office.co.uk/pa/ld199900/ldselect/ldsctech/121/12104.htm#a34. Accessed October 28, 2005
TRUST FOR AMERICA’S HEALTH (2003)Animal-borne epidemics out of control.Threatening the Nation’s Health. http://healthyamericans.org/reports/files/Animalreport.pdf. Accessed October 28, 2005
US NATIONAL INTELLIGENCE COUNCIL(2003) SARS: down, but still a threat. www.fas.org/irp/nic/sars.html. Accessed October 28,2005
WHO (2005) Cumulative number of confirmedhuman cases of avian influenza A/(H5N1)reported to WHO. www.who.int/csr/disease/avian_influenza/country/cases_table_2005_11_17/en/index.html. Accessed November 21,2005
Access to the full lectureA PDF file of Professor Gibbs’ WooldridgeMemorial lecture is available on the BVA Congresswebsite at www.bva.co.uk/ press/2005/congress05.asp. It is a large file and will take a few minutes todownload.
A PowerPoint presentation with integratedvideo is available for download at www.vetmed.ufl.edu/distribute/gibbsp. When at the site you willneed to insert the userid as wooldridge (all lowercase) and RoyalMed2005! (exactly as printedincluding the !) as the password. When the file hasdownloaded (about two minutes on a broadbandconnection) you will need to unzip the file to linkthe videos.
Animal and Human Health