Emerging Infections: Pandemic Influenza - NCEASsjryan/PPP/readings/Glezen, 1996.pdf · Emerging...
13
Epidemiologic Reviews Copyright © 1996 by The Johns Hopkins University School of Hygiene and Public Health All rights reserved Vol. 18, No. 1 Printed in U.S.A. Emerging Infections: Pandemic Influenza W. Paul Glezen The report of the Institute of Medicine's Committee on Emerging Microbial Threats to Health in the United States, published in 1992, defines influenza virus as the prototype emerging infection (1). Pandemics of influenza have been recognized since earliest recorded history and, because of the mutability of the virus, still represent a formidable threat to the health of the na- tion. Although much progress has been made in de- scribing the molecular aspects of the virus, in eluci- dating the epidemiology and modes of spread, and in developing methods for prevention and treatment, a rational strategy for control has not been established. The trends of modern society, including the increasing availability of rapid human transportation and the ur- banization of the rapidly expanding human population, tend to facilitate the spread of influenza and increase morbidity. Modern medicine can reduce the mortality that resulted from complications of infection with in- fluenza virus during earlier epidemics, but the cost of medical interventions has increased to the point that effective methods of epidemic control should be con- sidered. This challenge provides an opportunity to develop, test, and have in place a strategy for control of interpandemic influenza before the next pandemic. Pandemics result from the emergence of an influ- enza A virus that is novel for the human population. Evidence for recycling of subtypes of influenza A after intervals of 60 years or more has been derived by determining antibody prevalence in elderly popula- tions prior to the emergence of subtypes H2N2 in 1957 and H3N2 in 1968 (2, 3). A more ominous threat is the reservoir of 14 influenza A subtypes that persist in avian hosts (4). An avian virus can reassort with a human virus, as occurred in 1957 and 1968, to allow the creation of progeny that possess novel surface antigens with the potential to spread in human popu- Received for publication July 10,1995, and in final form February 23, 1996. Abbreviations: CDC, Centers for Disease Control and Prevention; ACIP, Immunization Practices Advisory Committee. From the Influenza Research Center, Department of Microbiology and Immunology, Baylor College of Medicine, Houston, TX. Reprint requests to Dr. W. Paul Glezen, Influenza Research Cen- ter, Department of Microbiology and Immunology, Baylor College of Medicine, One Baylor Plaza, Houston, TX 77030-3498. lations. Both pandemic viruses, A(H2N2) of 1957 and A(H3N2) of 1968, had evidence of gene reassortment with avian viruses (4). Swine are considered the most likely "mixing vessel" for this event, but viruses with avian genetic characteristics have also been recovered from horses and aquatic mammals. As pointed out in the Institute of Medicine report (1), many of the essential components for epidemic control are available. Surveillance of influenza activity is maintained by the network of laboratories sponsored by the World Health Organization. The Influenza Branch of the Centers for Disease Control and Pre- vention (CDC) coordinates surveillance activities in the United States with the worldwide effort. A collab- orative arrangement with the Chinese National Influ- enza Center in Beijing has improved recognition of the emergence of new variants of the currently prevalent influenza viruses (5). In the United States, this has allowed production and distribution of influenza vac- cines with antigens that closely match the viruses that are responsible for epidemics. Improved surveillance in the tropics and in the southern hemisphere, espe- cially in India, Africa, and South America, would enhance the ability to recognize new variants of influ- enza viruses as they arise. Other components of epidemic control are vaccine production and distribution and the availability of antiviral therapy. The routine use of influenza vaccine for one of the groups with highest priority, persons aged 65 years and older, has improved rapidly during the past 3 years; the proportion of the elderly receiving vaccine has risen from 32.9 to 52 percent between 1989 and 1993 (6). Delivery of vaccine to other pri- ority groups is lagging; only 10-15 percent of high risk patients less than 65 years of age receive vaccine each year. Two antiviral drugs against influenza A viruses, amantadine and rimantadine, are available for prevention. Although the prophylactic effect of these drugs is equivalent to vaccine for interpandemic peri- ods, ranging from 66 to 91 percent (7-9), the protec- tion is less for newly emerged pandemic strains (36-52 percent for A(H3N2) trials performed in 1968-1969 (10)) and the newly reemerged A(H1N1) viruses in 1978-1979 (11, 12). As pointed out in the 64
Transcript of Emerging Infections: Pandemic Influenza - NCEASsjryan/PPP/readings/Glezen, 1996.pdf · Emerging...

Epidemiologic ReviewsCopyright © 1996 by The Johns Hopkins University School of Hygiene and Public HealthAll rights reserved
Vol. 18, No. 1Printed in U.S.A.
Emerging Infections: Pandemic Influenza
W. Paul Glezen
The report of the Institute of Medicine's Committeeon Emerging Microbial Threats to Health in the UnitedStates, published in 1992, defines influenza virus asthe prototype emerging infection (1). Pandemics ofinfluenza have been recognized since earliest recordedhistory and, because of the mutability of the virus, stillrepresent a formidable threat to the health of the na-tion. Although much progress has been made in de-scribing the molecular aspects of the virus, in eluci-dating the epidemiology and modes of spread, and indeveloping methods for prevention and treatment, arational strategy for control has not been established.The trends of modern society, including the increasingavailability of rapid human transportation and the ur-banization of the rapidly expanding human population,tend to facilitate the spread of influenza and increasemorbidity. Modern medicine can reduce the mortalitythat resulted from complications of infection with in-fluenza virus during earlier epidemics, but the cost ofmedical interventions has increased to the point thateffective methods of epidemic control should be con-sidered. This challenge provides an opportunity todevelop, test, and have in place a strategy for controlof interpandemic influenza before the next pandemic.
Pandemics result from the emergence of an influ-enza A virus that is novel for the human population.Evidence for recycling of subtypes of influenza A afterintervals of 60 years or more has been derived bydetermining antibody prevalence in elderly popula-tions prior to the emergence of subtypes H2N2 in 1957and H3N2 in 1968 (2, 3). A more ominous threat is thereservoir of 14 influenza A subtypes that persist inavian hosts (4). An avian virus can reassort with ahuman virus, as occurred in 1957 and 1968, to allowthe creation of progeny that possess novel surfaceantigens with the potential to spread in human popu-
Received for publication July 10,1995, and in final form February23, 1996.
Abbreviations: CDC, Centers for Disease Control and Prevention;ACIP, Immunization Practices Advisory Committee.
From the Influenza Research Center, Department of Microbiologyand Immunology, Baylor College of Medicine, Houston, TX.
Reprint requests to Dr. W. Paul Glezen, Influenza Research Cen-ter, Department of Microbiology and Immunology, Baylor College ofMedicine, One Baylor Plaza, Houston, TX 77030-3498.
lations. Both pandemic viruses, A(H2N2) of 1957 andA(H3N2) of 1968, had evidence of gene reassortmentwith avian viruses (4). Swine are considered the mostlikely "mixing vessel" for this event, but viruses withavian genetic characteristics have also been recoveredfrom horses and aquatic mammals.
As pointed out in the Institute of Medicine report(1), many of the essential components for epidemiccontrol are available. Surveillance of influenza activityis maintained by the network of laboratories sponsoredby the World Health Organization. The InfluenzaBranch of the Centers for Disease Control and Pre-vention (CDC) coordinates surveillance activities inthe United States with the worldwide effort. A collab-orative arrangement with the Chinese National Influ-enza Center in Beijing has improved recognition of theemergence of new variants of the currently prevalentinfluenza viruses (5). In the United States, this hasallowed production and distribution of influenza vac-cines with antigens that closely match the viruses thatare responsible for epidemics. Improved surveillancein the tropics and in the southern hemisphere, espe-cially in India, Africa, and South America, wouldenhance the ability to recognize new variants of influ-enza viruses as they arise.
Other components of epidemic control are vaccineproduction and distribution and the availability ofantiviral therapy. The routine use of influenza vaccinefor one of the groups with highest priority, personsaged 65 years and older, has improved rapidly duringthe past 3 years; the proportion of the elderly receivingvaccine has risen from 32.9 to 52 percent between1989 and 1993 (6). Delivery of vaccine to other pri-ority groups is lagging; only 10-15 percent of highrisk patients less than 65 years of age receive vaccineeach year. Two antiviral drugs against influenza Aviruses, amantadine and rimantadine, are available forprevention. Although the prophylactic effect of thesedrugs is equivalent to vaccine for interpandemic peri-ods, ranging from 66 to 91 percent (7-9), the protec-tion is less for newly emerged pandemic strains(36-52 percent for A(H3N2) trials performed in1968-1969 (10)) and the newly reemerged A(H1N1)viruses in 1978-1979 (11, 12). As pointed out in the
64

Pandemic Influenza 65
Institute of Medicine monograph on emerging infec-tions, influenza remains an essentially uncontrolleddisease (1).
PANDEMIC INFLUENZA
To address the problem of this uncontrolledemerged and emerging infection, the US governmenthas reactivated the Interagency Group for InfluenzaPandemic Preparedness. This group consists of expertsfrom the interested government agencies and outsideconsultants who are charged with the development ofa national plan to deal with pandemic influenza. Atthis juncture, the characteristics of pandemic influ-enza, particularly as it has occurred during the lastcentury, will be reviewed to provide a framework forstrategies for implementation of control measures.
Excess mortality
The hallmark of pandemic influenza has been ex-cess mortality, defined by William Fair in London,England, in 1847 as the number of deaths observedduring an epidemic of influenza-like illness in excessof the number expected (13). Originally, most of thedeaths were diagnosed as pneumonia or influenza, butover the years an increasing proportion of excessdeaths have been attributed to other causes, usuallycardiac or pulmonary disease (14). The method ofdetermining the baseline, or the expected number ofdeaths for the season, also has evolved over the yearsfrom simply the number observed the previous seasonwhen no influenza epidemic occurred to a forecast ofthe baseline by various mathematical models citedbelow. Obviously, the use of excess mortality to defineand to measure the impact of influenza epidemics wasdeveloped and put in place before the etiology ofinfluenza was known and before virologic surveillancewas available.
After a respite of more than 50 years, pandemicinfluenza struck twice near the end of the nineteenthcentury, in 1889-1890 and again in 1899-1900 (15).Serologic archeology suggests that the hemagglutininof the virus of the 1889-1890 pandemic was similar tothat of the influenza A(H2N2) virus that caused the1957-1958 pandemic, and that the hemagglutinin ofthe virus active in 1899-1900 was similar to that ofthe influenza A(H3N2) virus that caused the pandemicof 1968-1969 (16). The agents of the pandemics ofthe eighteenth and nineteenth centuries were thoughtto have originated in Russia; tracking of outbreaksindicated that they generally spread from east to westthrough Europe (15). More likely, Russia was the siteof the first recognition of the spreading pandemic, butnot necessarily the site where the agent originated. The
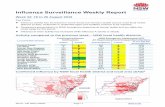
rapidity of spread was remarkable in those days ofsteamship travel. Both of the pandemics of the latenineteenth century crossed the Atlantic to the UnitedStates within 2 months after activity was recognized inEurope. Excess mortality rates by nation were notsystematically determined in those years, but citiessuch as London had rates of pneumonia-influenzamortality that were roughly 10 times that seen cur-rently with a severe influenza A(H3N2) epidemic inthe United States, and the curve for age-specific mor-tality displayed the typical "U"-shape (figure 1) withthe highest rates at the two extremes of the age spec-trum (17).
The site of origin of the great pandemic of 1918 isunknown, but some choose to think that it was in theUnited States (18). Scattered outbreaks of diseasewere detected during the spring and early summer of1918. Excess pneumonia-influenza deaths were evi-dent from later tabulations by Wade Hampton Frost,who directed most of the epidemiologic investigationsof this pandemic for the US Public Health Service(19). Many of the early outbreaks occurred in militaryinstallations as recruits poured into training camps torespond to the call for troops in Europe. Outbreaksalso occurred on troop ships and among the AmericanExpeditionary Forces in France by April 1918. Thedisease was soon evident among allied forces. A pe-riod of quiescence was noted in the United Statesduring the summer. In some areas it was suspected thata reintroduction from Europe occurred in late summerand early autumn. However, in retrospect, it is evidentthat "seeding" of many geographic areas of the UnitedStates had occurred during the previous spring, thattransmission was low during the summer but pickedup rapidly as schools reopened in September. The firstwave of the pandemic reached a crescendo by the endof October 1918. This was followed by a decline andrecrudescence in midwinter 1919. The same pattern ofoccurrence was observed in the United States in 1957with the next pandemic caused by influenza A(H2N2)(20).
By 1918, only about three-fourths of the states andterritories systematically reported deaths to a nationalregistry (21). From this sample an estimate of over550,000 excess deaths was calculated from a rate of598 per 100,000 persons for the biphasic epidemicperiod spanning September 1918 through April 1919.The third peak occurred in February 1920 and pro-duced over 125,000 excess deaths, for a total of>675,000 excess deaths for the pandemic period. Forthe 3-year pandemic period, an annual average of225,000 excess deaths occurred. The designation of a3-year pandemic period is used for the sake of com-parison with similar periods for the 1957 and 1968
Epidemiol Rev Vol. 18, No. 1, 1996

66 Glezen
2,000 T1892Massachusetts
O 1,500
0_O
ooooo
rxLUa.CO
1Q
1,000
500
1918United Statesregistration area
1936United States
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80
AGE
FIGURE 1. Pneumonia and influenza mortality by age in certain epidemic years. (From Dauer and Serfling (17).)
pandemics when virologic surveillance demonstratedthat the pandemic virus in each case produced at leastthree waves before significant antigenic variation wasdetected (20, 22).
The 1918 mortality numbers alone do not ade-quately describe the disaster. It was not just the weakand infirm who were taken away but the flower andstrength of the land (18). The age-specific mortalitycurve did not trace the "U" described above, butresembled a "W" with very high mortality rates inhealthy young adults aged 20-40 years as well as inthose less than 5 years of age and those aged 65 yearsand older (figure 1). No adequate explanation of thismortality pattern has been presented. It was wartimeand young men were crowded together in militarycamps, but the mortality was highest in men of thesame age who remained at home. Pregnancy was a riskfactor, and this may provide some explanation for thehigh mortality in young women (23, 24). The fulmi-nant nature of the clinical course of the fatal pneumo-nia cases suggests that the virus itself possessed avirulence not seen before nor since.
Many of the young men at military encampmentshad perioral cyanosis as a presenting sign of theirillness along with the usual signs and symptoms ofinfluenza (18). Death ensued rapidly within a fewdays. Postmortem examination revealed denudation of
the respiratory mucosa with the airways full of frothy,blood-tinged fluid. Many of those who survived thefirst few days developed a secondary bacterial infec-tion, usually with pneumococcus, group A streptococ-cus, or Hemophilus influenzae, and died with typicalbacterial pneumonia.
The technology for virus isolation had not beendeveloped in 1918, but some evidence for the identi-fication of the putative agent is available. In 1976,more than 90 percent of persons in the United Statesaged 52 years and older had antibodies to the influenzaA/New Jersey(HlNl) virus (25). This virus was doc-umented to have spread among soldiers at Fort Dix,New Jersey, and was similar to the virus known tohave been carried by swine since 1930, the year thatthe virus was first isolated. A similar virus is thoughtto be the agent of the great pandemic of 1918. It isvery difficult to review the description of the 1918pandemic and criticize the efforts in 1976 to immunizethe population of the United States against this poten-tial threat. Sufficient numbers of intensive care bedsdo not exist to treat a pandemic of adult respiratorydistress syndrome, and if they did exist, we wouldbankrupt the system with the effort. Over 280,000pneumonia deaths were reported in young adults, aged20-39 years, in 1918-1919. The mortality rate wasabout one per 100 in this young age group (21).
Epidemiol Rev Vol. 18, No. 1, 1996

Pandemic Influenza 67
Table 1 compares the excess mortality for the greatpandemic of 1918 with those that have followed sub-sequently, and summarizes the excess mortality for theinterpandemic periods (14, 20-22, 26-29, LoneSimonsen, CDC, Atlanta, Georgia, personal commu-nication, 1995). Crude rates were calculated for com-parison of the impact at different periods using theaverage annual number of excess deaths and the esti-mated population for the midpoint of the period. Forsome years more than one estimate of excess mortalitywas available, and for those years the highest numberwas chosen. Excess mortality remained high for theepidemics that occurred through the 1932-1933 sea-son; eight epidemics were observed during that 13year interpandemic period (1920-1933). It was esti-mated that 368,400 excess deaths occurred yielding anaverage annual rate of 23 per 100,000 persons, or28,338 excess deaths per year (14). The viruses thatcaused these epidemics were not identified; it is pos-sible that some were variants of the virus that causedthe 1918 pandemic and some were probably influenzaB viruses.
Virus identification was available for the next inter-pandemic period from 1933 until the 1957 pandemic.Nine influenza A(H1N1) epidemics and five influenzaB epidemics were recognized during the 24-year pe-riod (22). The most severe epidemics were the influ-enza B epidemic of 1935-1936 and the influenzaA(H1N1) epidemics of early 1937 and the winter of1943-1944 with excess deaths numbering 55,000,46,000, and 53,000, respectively (14, 22). With thesethree exceptions, the epidemics were relatively mildand occurred approximately every other year. Theaverage annual excess mortality rate dropped to 7.5per 100,000 persons during this 24-year period.
The next pandemic began in 1957 when influenzaA(H2N2) viruses appeared in the Far East. The preciseorigin is unknown, but the virus was isolated in Sin-gapore in February and in Hong Kong in April 1957(20). The prototype strain was designated as A/Japan/305/57(H2N2) and is commonly referred to as the
Asian influenza virus. Concurrently, the A(H1N1) vi-ruses known to have been prevalent in human popu-lations for at least 24 years no longer circulated inhumans. Detectable antibodies to A(H2N2) viruseswere rare in subjects less than 65 years of age, and thevirus was observed to spread rapidly in the Far East;therefore, a pandemic was predicted with spread to theSouthern Hemisphere in the summer of 1957 to befollowed by epidemics in the Northern Hemisphere(30). The predictions were accurate.
The first identifications of Asian influenza weremade in coastal cities on both coasts of the UnitedStates in June 1957. The virus seeded the populationduring the summer and became epidemic as soon asschools were back in session. The seasonal pattern ofexcess mortality was very similar to that observed withthe great pandemic of 1918. The first peak of excessdeaths occurred in late October 1957, followed by asecond peak in February 1958. A small peak of excessmortality caused by influenza A(H2N2) accompaniedby influenza B was interspersed before the next sub-stantial wave of Asian influenza in early 1960. Most ofthe excess deaths were detected in the first biphasicepidemic that covered the period from September1957 through March 1958; almost 70,000 of the totalof 115,700 excess deaths for the pandemic periodoccurred during that first year. Although some fulmi-nant deaths were reported in healthy young adults,particularly pregnant women, the mortality did notcompare with that observed in 1918-1919 (31-33).The age-specific rates returned to the traditional "U"-shaped pattern produced by highest rates in persons atthe extremes of the age spectrum. The overall impactwas only one-tenth of that observed in 1918-1919.
During the 10-year prevalence period for A(H2N2)viruses, new variants arose to produce major epidem-ics in early 1963 and in the winter of 1967-1968 (22).Moderate influenza B epidemics were observed in1961-1962 and in early 1966. The average annualexcess mortality rate for the 8-year interpandemic
TABLE 1. Excess deaths estimated for pandemic and interpandemic periods, 1918-1991
Period
PandemicInterpandemicInterpandemicPandemicInterpandemicPandemicInterpandemicInterpandemic*
Years
1918-19201920-19331933-19571957-19601960-19681968-19721972-19811981-1991
No. of excess deaths
675,000368,400242,600115,700114,900111,927198,800
200,000t
Annual average
225,00028,33810,10838,56714,36327,98222,08920,000
Crude rate per 100,000persons
218.423.0
7.522.0
7.513.910.310.0
' Preliminary estimates,t Approximation.
Epidemiol Rev Vol. 18, No. 1, 1996

68 Glezen
period (1960-1968) was the same as that seen in theperiod just before the Asian influenza pandemic.
The next pandemic occurred with the emergence ofinfluenza A(H3N2) viruses in 1968 (34). The proto-type virus was influenza A/Aichi/2/68(H3N2) and isusually referred to as A/Hong Kong influenza. Thiswas a "hybrid" pandemic strain because only one ofthe surface glycoproteins, the hemagglutinin (H3), wasunique for the population. The N2 neuraminidase waspresent also on the preceding H2N2 viruses (35). Asmentioned previously, viruses with the H3 hemagglu-tinin were thought to have caused the pandemic of1899 (16). Although the Hong Kong influenza viruswas detected in the United States as early as Septem-ber 1968, it did not become epidemic until December.Excess mortality peaked in December 1968 and Jan-uary 1969 (36). The same virus returned in early 1970and 1972 to produce epidemics with excess mortality(22). A total of 98,100 excess deaths were notedduring the 4-year period yielding an annual excessmortality rate of 12.2 per 100,000 for the pandemic.Most of the excess deaths occurred in persons aged 65years and older. It should also be noted that influenzaA(H2N2) viruses disappeared from human circulationwhen the influenza A(H3N2) viruses emerged, just asthe A(H1N1) viruses had ceased circulation in 1957with the emergence of A(H2N2).
Several factors may have contributed to the rela-tively low mortality rate that accompanied the A/HongKong(H3N2) pandemic. The excess death rate wasabout half of that observed with the Asian (H2N2)influenza pandemic in 1957-1958. First, the N2 neur-aminidase common to the preceding virus (35) mayhave produced a cross immunity that modified theseverity of illnesses associated with the A(H3N2) vi-rus. Antibodies to the influenza neuraminidase do notprevent infection but may modify the extent of infec-tion by reducing the amount of virus released fromeach replication (37). Another factor was the timing ofthe epidemic; the first wave may have been altered bythe fact that schools recessed for the Christmas holi-days just as the epidemic was gaining momentum (38).Since school children are important for the dissemina-tion of the virus in the community, the recess mayhave dampened the progress of the first wave of theepidemic. Improved medical care, including more ef-fective antibiotics for secondary bacterial infections,could have resulted in a better outcome.
Although the pandemic produced by influenzaA/Hong Kong(H3N2) virus was relatively mild, thesubsequent H3N2 variants have continued to amassexcess mortality for over 20 years (1972-1991) (29,Lone Simonsen, CDC, Atlanta, Georgia, personalcommunication, 1995). Most of the excess mortality
for the current interpandemic period has occurred dur-ing these H3N2 epidemics. The annual average num-ber of excess deaths has remained above 20,000 peryear, and the average annual rate has remained abovethe excess mortality rates observed during the inter-pandemic periods since 1933. No good explanationexists for the continued toll of H3N2 viruses. Influ-enza A(H1N1) viruses that reappeared in 1977 havecontributed little to the excess mortality (29, LoneSimonsen, CDC, Atlanta, Georgia, personal commu-nication, 1995). It may be relevant that most of thepersons now at high risk for the complications ofinfluenza were born and attended school (the periodfor high risk of infection) during the H1N1 era prior to1957. This experience has served them well during therecent outbreaks of H1N1 viruses even though thesubsequent variants of the 1977 H1N1 prototype virushave been antigenically different compared with theH1N1 viruses that were prevalent before 1957 (39).(The prototype H1N1, A/USSR/77, that appeared in1977, was identical to a virus that circulated in theUnited States in 1950.) Influenza B epidemics haveresulted in measurable excess mortality on five occa-sions during the 20-year period compared with nineoccasions for influenza A(H3N2).
Critique of excess mortality as a measure ofseverity
Excess mortality as currently measured is a specificindication of the occurrence of epidemic influenza.When reported pneumonia-influenza deaths exceedthe threshold established by the mathematical modelused to predict the baseline mortality, an influenzaepidemic is in progress. Weekly reporting of deaths tothe CDC allows the development of timely informa-tion about the course of epidemics. The shortcomingof the system is that it may not be a sensitive measureof the impact of epidemics (40). The models used topredict the baseline have not been validated by deter-mining that the periods used to model the wintertimebaseline were free of influenza activity. They havetended to label years with epidemics due to influenzaB virus as nonepidemic years, and the epidemic weeksfor these years are incorporated into the baseline bycircular reasoning. This process assures that excessmortality will not be detected in young people who aresusceptible to influenza B viruses (41) and who havehigh morbidity proven by positive cultures duringthese epidemics (42,43). Furthermore, the detection ofexcess mortality is dependent upon the occurrence ofsynchronous epidemics throughout the country. Whenepidemics occur at different time periods in differentgeographic areas, the threshold may not be exceededfor 2 successive weeks; therefore, the pneumonia-
Epidemiol Rev Vol. 18, No. 1, 1996

Pandemic Influenza 69
influenza deaths that have occurred over a longerperiod of time in regional epidemics go undetected asexcess mortality. The solution is to validate the modelsfor predicting the baseline mortality with adequatevirologic surveillance to document that the baselineaccurately represents the occurrence of pneumonia-influenza deaths in the absence of significant influenzavirus activity. This would require systematic surveil-lance of influenza in representative geographic areasthroughout the country similar to that maintained inHouston, Texas, for the past 20 years (44). This wouldalso allow for adjusting the detection of excess mor-tality in each geographic area to the time that influenzais epidemic in that specific region.
Hospitalizations as an alternative measure ofseverity
Surveys of the occurrence of hospitalizations foracute respiratory conditions in Houston have producedpeaks that coincide with the peak of influenza virusactivity each winter (44, 46). The peak of hospitaliza-tions lags 1 week after the peak of influenza activity,defined by community surveillance of patients pre-senting for medically attended acute respiratory ill-ness. Several other investigators have used hospital-ization data to measure the impact of influenzaepidemics (47) and to determine the effectiveness ofinterventions (48-50). Hospital discharge records areretrievable by computers and have more complete andaccurate information than is available on death certif-icates. An illness resulting in hospitalization is themost important unit of measure for determining theimpact of an epidemic. Furthermore, 10-12 hospital-izations occur for each pneumonia-influenza death,thereby increasing the sensitivity of the measurementfor small populations. Analysis of data for personshospitalized during influenza epidemics provides amore complete description of the persons at risk forserious complications of influenza and will broadenthe indications for intervention. Excess mortality canalso be determined from hospital data. Deaths of pa-tients with hospital discharge diagnoses of acute re-spiratory illness during influenza epidemics are abouttwice as frequent as deaths from pneumonia-influenza,as determined from information collected from deathcertificates. Data from representative hospitals are cur-rently collected by the National Center for HealthStatistics. Timely analysis of hospitalizations duringinfluenza epidemics could provide useful informationfor planning interventions. In addition to data concern-ing hospitalizations, the current expansion of managedcare groups will allow retrieval of records of ambula-tory care and immunization status which should fur-
ther facilitate the assessment of both impact and inter-ventions (49).
Age-specific attack rates
The morbidity and clinical attack rates produced bypandemic influenza have received much less attentionthan has excess mortality. In other words, the attentionhas been focused on the groups of persons who aremost vulnerable to complications and death as a resultof influenza virus infection. For most pandemics,those at greatest risk are the elderly and the veryyoung. These same persons are, for the most part, atthe end of the transmission chain; they are not intro-ducers of influenza into the household (51). Therefore,immunization of these persons may reduce mortalityand serious illness but will have little effect on thecourse of the epidemic. The fires of the epidemic arefed by healthy susceptible school children, collegestudents, and employed persons who have many dailycontacts and who are more mobile. If the vaccineadministered to high risk persons is less than perfect,and provides only 70 percent protection, allowing theepidemic to proceed unimpeded will result in manyvaccine failures. An example of this scenario occurswhen personnel of nursing homes are unimmunized,become infected, and are allowed to expose vulnerableelderly persons to infection. Although influenza vac-cine reduces the risk of hospitalization for the elderly,the vaccine is far from perfect. A recent study reportedby Falsey et al. (52) found that 61 percent of over 200hospitalized elderly persons with proven influenza Avirus infection had been currently vaccinated. Gener-ally, the persons most at risk are the least likely tohave generated adequate protection in response to thecurrently available inactivated vaccines. This, then, ispart of the rationale for considering more carefully therole of persons who spread the virus in the community.
Wade Hampton Frost directed and reported largesurveys of influenza-like illness that were performedduring the 1918-1919 pandemic (53). The sampleconsisted of 146,203 persons who were representativeof the US population, which at that time numberedabout 103 million persons. Household representativeswere queried about acute respiratory illnesses that hadoccurred during the first 4 months of the epidemic.The illnesses sought were "influenza", "grippe", and"colds". A cold was significant if the person with thecondition was put to bed for at least 1 day. The numberof persons who developed pneumonia was also ascer-tained. A similar survey of 151,193 persons was car-ried out in 1929 by Selwyn D. Collins following anepidemic in the interpandemic period (21). (The1928-1929 epidemic was estimated to have causedabout 65,000 excess deaths.) The illness rate for the
Epidemiol Rev Vol. 18, No. 1, 1996

70 Glezen
1918 pandemic (first wave) was 29.4 per 100 persons,compared with 18.9 per 100 persons for the 1928 —1929 epidemic (table 2). The age distributions dif-fered, with the highest attack rates in children aged5-14 years in 1918-1919 and in children aged 1-9years in 1928-1929. Adult groups aged 55 years andolder had consistently higher rates in the later epi-demic. Children aged 5-9 years had the highest rate ofnearly 40 per 100 in 1918-1919, while the highest ratein 1928-1929 was just less than 25 per 100 for pre-school children. The curve for age-specific rates wasconsiderably flatter for the later interpandemic out-break (figure 2). It is obvious that the mortality curves(figure 1) for these epidemics did not mirror the mor-bidity curves. The school children and preschool chil-dren with the highest attack rates did not have thehighest mortality rates.
Subsequent surveys measuring influenza morbidityhave all involved households with children; therefore,they have consistently higher attack rates than theearlier community surveys performed by the US Pub-lic Health Service. The first community outbreak to beinvestigated in the 1957 Asian influenza pandemicoccurred in the summer in Tangipahoa Parish, Loui-siana, where schools opened on July 12 (54). Theattack rates were determined by polling the families ofchildren who attended the public schools. The out-break peaked in early August among families withchildren in the schools for low income (mostly black)children and almost a month later in the middle in-come (white) school. The overall attack rate was 41.5per 100 persons, with the highest rate (58.7) in chil-
TABLE 2. Age-specific influenza attack rates for pandemicand interpandemic periods 191&-1957
Age (years)
<11-45-910-1415-1920-2425-2930-3435-3940-4445-4950-5455-5960-6465-6970-74>75
Rate for total
1918Pandemic
20.733.739.138.134.532.333.732.629.623.620.717.516.214.313.511.18.8
29.4
Rates per 100 Persons
1928-1929Interpandemic
13.824.924.820.016.315.718.319.919.818.617.216.916.416.917.518.117.9
18.9
Age(years)
o
5-910-1415-19
20-34
35-3940-4445-4950-5455-59
>60
1957Pandemic
335254
27
2518171917
10
24
dren 10-14 years of age. Chin et al. (55) surveyed thefamilies of students attending a high school serving anupper middle income area of Kansas City, Missouri.The overall attack rate was 34 per 100 persons, and thehighest attack rates occurred in junior and senior highschool-aged students at 52 and 54 per 100, respec-tively (table 2). Jordan et al. (56) looked at the age-specific frequencies of significant antibody rises forpersons not receiving influenza vaccine in the Cleve-land (Ohio) Family Study (56). Over three-fourths ofstudents aged 10-14 years had an antibody rise to theA(H2N2) virus. Over 70 percent of high school- andcollege-aged students also were infected. The infec-tion rates for elementary and preschool children andadults were 67 percent, 50 percent, and 24 percent,respectively.
For the 1968 A/Hong Kong(H3N2) pandemic, an-other survey was carried out by Chin et al. (57) at thesame high school in Kansas City surveyed previously.The influenza A(H3N2) outbreak peaked in KansasCity during the third week of December 1968 justbefore the Christmas recess. The age-specific attackrates showed a remarkably different pattern than thecurve for age-specific attack rates for the first wave ofthe 1957 Asian pandemic (figure 3). In fact, the con-trast is similar to that comparing the age-specific ratesfor the pandemic of 1918-1919 with the interpan-demic outbreak of 1928-1929 (figure 2). The age-specific rates for 1968-1969 were fairly similar for allage groups with a slight excess in students aged 10-14years and a second peak for adults aged 35-39 years.The factors mentioned above that may have contrib-uted to the relatively low excess mortality associatedwith the 1968 pandemic may explain the flat attackrate in the first wave. The school holiday may haveinterrupted the transmission of the virus by dispersingthe school children who are important for spreadingthe infection. Cross protection provided by the N2surface glycoprotein shared with the A(H2N2) virusesthat circulated from 1957 through early 1968 mayhave reduced the attack rate for influenza-like illnessin the school children who were surveyed. A serologicsurvey showed that many of the students without ahistory of an influenza-like illness had antibodies tothe virus, indicating the frequent occurrence of mild orinapparent infections. Mild illnesses could have beenimportant for spread of the virus, because studentswith milder illnesses probably did not restrict theiractivity or contacts thereby increasing the opportuni-ties for spread of the infection. Senior and junior highschool students are the group most likely to have thepartial protection to infection mediated by antibodiesto neuraminidase, N2, because they would have expe-
Epidemiol Rev Vol. 18, No. 1, 1996

Pandemic Influenza 71
4 2 5 .
400 .
375.
TOTAL INCIDENCEALL SURVEYED LOCALITIES
-I 1 1 1 1 1 1 1 1-5 10 15 20 25 30 35 40 45 50 55
AGE
-i 1 1-70 75 80
FIGURE 2. Age-incidence of respiratory illnesses in surveyed groups during the epidemics of 1928-1929 and 1918-1919. (From Collins andLehmann (14).)
rienced the highest attack rates with the influenzaA(H2N2) viruses during the previous 8 years.
55
50
15
; 40
|35
j 30- 25j
• 20
LEGEND-
5 10 15 20 35 40 45 50 55 6OAGE LAST BIRTHDAY
FIGURE 3. Age-specific attack rates of influenza-like illness infamilies of students who attended a high school serving an uppermiddle income area of Kansas City, Missouri. (From Chin et al. (55).)
Two family studies have examined influenza virusattack rates in the period since the 1968 A/HongKong(H3N2) pandemic (13, 58). The studies differedin structure in that the Seattle, Washington, familieswere selected for presence of school-aged childrenwhile Houston families were selected because of birthof a newborn infant into the family. This difference inage distribution of the children may explain the dif-ferences in age-specific attack rates during the inter-pandemic period (table 3).
Implications of age-specific attack rates
Two features of the age-specific attack rates areevident. The first feature is that only a finite propor-tion of the population is infected with each annualepidemic (usually between 25 and 50 percent), andthis proportion does not vary between pandemic andinterpandemic outbreaks (13, 21, 53, 55-58). Evenpandemic viruses that are novel for the population donot reduce the pool of susceptibles by more than 50percent during the first wave. One explanation for this
Epidemiol Rev Vol. 18, No. 1, 1996

72 Glezen
TABLE 3. Influenza virus infection rates for persons followed in family studies in Seattle, Washington,1975-1979 and Houston, Texas, 1976-1984
Seattle* Houston
Age No. of Person-years No. infected irjopersons A 9 e No. of Person-years No. infected
<5 211
5-9 605
10-19 695
£20 1,222
Totals 2,733
52
200
269
145
666
25
33
39
12
24
<22-5
6-1011-1718-2425-34
>35
332474300149178651257
2.341 767
1182111436041
14054
35.544.547.740.323
21.521
32.8
• From Fox et al. (58).
may be that persons naive for the new virus have moresevere illnesses that put them to bed and limit thenumber of their contacts. On the other hand, duringinterpandemic outbreaks many persons with partialimmunity to the circulating virus have mild illnessesthat do not limit activity and reduce contacts. There-fore, the predominance of severe illnesses during pan-demics may serve to limit spread, while the mildillnesses observed in interpandemic outbreaks serve toencourage spread even when a portion of persons inthe population are immune. This could explain thesimilarity of attack rates for pandemic and interpan-demic periods.
The second important feature evident from the re-view of age-specific attack rates is that school childreninvariably have the highest attack rates during bothpandemic and interpandemic periods. Epidemiologicstudies during pandemics have demonstrated that chil-dren are important for spread of virus in the commu-nity (59). Observations made during the two majorpandemics of this century reinforce the thesis thatschool children are important in the spread of influ-enza. Even though the populations were universallysusceptible to the new influenza viruses that emergedin 1918 and 1957, and even though both viruses hadseeded the population in the preceding spring andsummer, the first major wave did not occur untilschools were in session. Peak activity of both pandem-ics occurred in late October after school had been insession for 6 -8 weeks.
For interpandemic periods, observations in Houstonhave demonstrated that school children predominateamong persons presenting for health care during theearly stage of influenza epidemics (60). The age dis-tribution of culture-positive patients changes duringthe course of the epidemic, with a shift to preschoolchildren and adults during the latter part of the epi-demic (table 4). School absenteeism occurs in the firstpart of the epidemic and employee absenteeism occurs
TABLE 4. Age distribution of patients with influenza virusinfections during epidemics occurring after school holidayscompared with those during epidemics interrupted byholidays, Houston, Texas, 1974-1981
Age(years)
<55-1920-24£45
<55-1920-44£45
% during epidemic stage
Early Peak
Epidemic after school holidays*
(n = 930)16.853.421.68.2
(n= 1,695) (n24.237.826.911.1
Epidemic interrupted by school holidays^
(n = 352)22.754.018.54.8
(n = 320) (n24.431.630.313.8
Late
= 750)25.931.630.012.5
= 261)20.745.625.78.0
* Early versus late stages, p <'t Early versus peak stages, p •
during the later part (61). Hospitalizations of personsaged 65 years and older tend to occur during the lasthalf of the epidemic, and pneumonia-influenza deathsare lagged at least 2 weeks after the peak of commu-nity morbidity (46). All of these observations supportthe thesis that school children are important dissemi-nators of the virus in the community for both pan-demic and interpandemic influenza. A series of familystudies also have demonstrated that children are themain introducers of influenza into the household (58,62, 63). Furthermore, statistical modeling based onlongitudinal community and family studies have con-firmed the role of children for introducing influenzainto the household (51), and have found that immuni-zation of school children would be effective for epi-demic control (64).
The high morbidity of children is not without se-quelae. Virus infections, particularly influenza, triggerasthma attacks that lead to hospitalization of predis-
Epidemiol Rev Vol. 18, No. 1, 1996

Pandemic Influenza 73
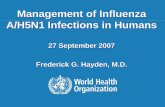
posed children. On average, more than 20 percent ofchildren less than 10 years of age have medicallyattended illnesses (65). The hospitalization rate (43 per10,000) for children less than 5 years of age duringinfluenza epidemics is second only to that for personsaged 65 years and older (figure 4). Surveys haveshown that less than 15 percent of young childrenhospitalized have any chronic condition; therefore,most hospitalized children are not in the group givenpriority for influenza immunization at this time (66).These hospital rates do not include children whoseprimary diagnoses were not acute respiratory condi-tions. Almost half of children hospitalized with proveninfluenza virus infections have major involvementwith another organ system (67, 68). Febrile convul-sions and encephalopathy were prominent (69-70);pericarditis and gastrointestinal problems also occur.
INFLUENZA-RELATED MORBIDITY AND MORTALITY
80
60
40
20
0
P-l Mortality
•
•
•
60
CO OUJ »"
I E40
20
ARD Hospltalizations
20
10
Medically Attended Illness
<5 5-9 10-14 15-19 20-24 25-34 35-44 45-54 55-64 £65
AGE (YEARS)
FIGURE 4. Age-specific rates for medically attended illness andmortality during influenza epidemics, Houston, Texas. (From Glezen(65).) P-l, pneumonia-influenza; ARD, acute respiratory disease.
Severe myositis is common with influenza B infec-tions (72). Suspected bacterial sepsis is a frequentdiagnosis for febrile infants under 3 months of age (67,73). Limiting consideration of serious morbidity toonly pulmonary conditions underestimates the role ofinfluenza virus infections as causes of hospitalizationof children. Therefore, children have serious morbiditythat justifies universal influenza immunization.
CONTROL OF EPIDEMICS
The use of licensed inactivated trivalent influenzavaccine is increasing, but even if all high risk personscurrently given priority for this vaccine should bevaccinated each year, influenza epidemics would con-tinue to occur. Healthy school children, preschoolchildren in day care, college students, and workingadults would continue to have high morbidity andwould continue to spread the virus in the community.Vulnerable high risk patients would be at risk becauseof repeated challenge to their immunity by contactwith infected persons.
Recent pandemics illustrate another problem thatmust be faced with an impending pandemic. The timebetween recognition of the emergence of a new pan-demic virus and the occurrence of the first wave maybe short. The lead time for the production and distri-bution of the currently licensed influenza vaccine,trivalent influenza vaccine, is 6 months. It is highlyunlikely that sufficient vaccine can be produced, dis-tributed, and administered to the entire populationbefore the first wave of the pandemic. In 1918 and1957, the first wave of the pandemic peaked in lateOctober allowing less time than usually occurs beforethe onset of interpandemic outbreaks, in the usualsequence of vaccine production starting in January.
Priorities for vaccine use have been established bythe Immunization Practices Advisory Committee(ACIP) of the US Public Health Service (74). Unfor-tunately, high risk patients are not easily accessible foradministration of vaccine within a short period oftime. Some alternatives for use of vaccine have beensuggested by mathematical models developed byLongini (75). Two models were presented, one basedon the first wave of the 1957 pandemic and the otheron the 1968 pandemic. The first model suggested thatif vaccine were available for only 30 percent of thepopulation, the most effective use would be for schoolchildren and 44 percent of preschool children (those inday care). The second model distributed the vaccine topreschool and school-aged children, and to youngadults. These models suggest rapid deployment of thefirst available vaccine to groups that will experiencethe highest attack rates. These are accessible groups,particularly if vaccine can be administered at school
Epidemiol Rev Vol. 18, No. 1, 1996

74 Glezen
and at the workplace. Prevention of the spread of virusin these groups would allow time to produce additionalinactivated vaccine and to distribute it to high riskpatients. Even if the vaccine is produced too late fordistribution before the first wave, it can be used toabort the second and third waves.
Priorities for the use of first available vaccine havebeen discussed, and cogent arguments can be made forimmunizing several different segments of the popula-tion. The resulting tension can be relieved by insertingthe use of a vaccine preparation other than inactivatedinfluenza vaccine. The live attenuated cold-adaptedinfluenza vaccine of Maassab (76), that is adminis-tered by nose drops or spray, could prove to be a moreeffective tool for epidemic control. The cold-adaptedvaccine has been studied for over 20 years and givento more than 7,000 persons of all ages (77, 78), but itis not yet licensed. Investigations have shown thisvaccine to be better than inactivated influenza vaccinefor young children, aged 3-9 years, and equivalent toinactivated influenza vaccine for older students andyoung adults (79-81). The cold-adapted vaccine hasnot been tested sufficiently in high-risk patients toallow its use in such patients, thereby reducing anytension that might accompany a directive to limit itsuse to certain groups specifically for epidemic control.The available inactivated influenza vaccine could bedistributed to high-risk patients and the priorities forits use would not be altered.
The cold-adapted vaccine has several advantages foruse in epidemic control. Not only does it providebetter protection for children aged 3-9 years whousually have the highest attack rates, but studies alsohave suggested that cold-adapted vaccine providesbroader and longer-lasting immunity against variantsof influenza A (79, 80). The cold-adapted vaccine iseasier to administer and is much more acceptable byyoung children.
The important putative advantage of cold-adaptedvaccine has yet to be demonstrated, i.e., its use forepidemic control. The concept of immunization ofschool children to reduce community morbidity is notnew. Monto et al. (82) immunized school children inTecumseh, Michigan, with inactivated influenza vac-cine in 1968 and found lower total morbidity than thatexperienced by a matching community during the firstwave of the influenza A(H3N2) pandemic (82). Montosuggested at that time that the use of an intranasalvaccine (cold-adapted) might be accomplished readilyand at a lower cost. In addition to the Tecumseh study,Warburton et al. (84) used a subunit vaccine toA(H3N2) in communities of the Northern Territory ofAustralia in 1968 to demonstrate "herd" immunity.The people in the "vaccinated" communities had im-
munization rates ranging from 5 to 50 percent (mean29 percent) and had significantly lower attack rates(5-28 per 100, mean 15 per 100) compared with thepeople in the "unvaccinated" communities who hadhigher attack rates (6-100 per 100, mean 65 per 100).
Several resources now available should facilitate theevaluation of the cold-adapted vaccine for epidemiccontrol. The advantages of the vaccine are listedabove. The ready availability of clinical informationfrom computerized sources, such as hospitalizations,clinic visits, and school attendance, will allow anassessment of the effect of the vaccine. The epidemicscan be defined for the community by virologic sur-veillance, and the coincident effect on the rates forhealth care visits and hospitalizations can be used tomeasure the effect. Similar surveillance systems canbe established in matching communities to determinethe net benefit of the immunization program. If theseinvestigations can document a significant benefit, thisapproach to epidemic control could be used currentlyto control interpandemic influenza and could providean effective method for confronting the next pan-demic. Even if vaccine should not be available for thefirst wave of the next pandemic, immunization ofschool children could dampen the second and thirdwaves.
Epidemic influenza has been shown to significantlydisrupt and adversely effect the delivery of health care.Control of yearly epidemics would not only reducepain, suffering, and death, but would facilitate plan-ning for efficient delivery of care by reducing theannual stress imposed by the influx of patients duringannual influenza epidemics and provide an effectivemeans of combating the threat of the next pandemic.
ACKNOWLEDGMENTS
This study was supported by contract no. AI-15103 fromthe National Institute for Allergy and Infectious Diseases.
REFERENCES
1. Lederberg J, Shope RE, Oaks SC Jr, eds. Emerging infections:microbial threats to health in the United States. WashingtonDC: National Academy Press, 1992.
2. Marine WM, Thomas JE. Antigenic memory to influenza Aviruses in man determined by monovalent vaccines. PostgradMed J 1979;55:98-104.
3. Schoenbaum SC, Coleman MT, Dowdle WR, et al. Epidemi-ology of influenza in the elderly: evidence of virus recycling.Am J Epidemiol 1976;103:166-73.
4. Webster RG, Wright SM, Castrucci MR, et al. Influenza—amodel of an emerging virus disease. Intervirology 1993;35:16-25.
5. Reichelderfer PS, Kendal AP, Shortridge KF, et al. Influenzasurveillance in the Pacific basin. In: Current Topics in Medical
Epidemiol Rev Vol. 18, No. 1, 1996

Pandemic Influenza 75
Virology. Singapore: World Scientific, 1989:412-44.6. Influenza and pneumococcal vaccination coverage levels
among persons aged s 6 5 years—United States, 1973-1993.MMWR Morb Mortal Wkly Rep 1995,44:506-7, 513-15.
7. Dolin R, Reichman RC, Madore HP, et al. A controlled trial ofamantadine and rimantadine in the prophylaxis of influenza Ainfection. N Engl J Med 1982;307:580-4.
8. Clover RD, Crawford SA, Abell TD, et al. Effectiveness ofrimantadine prophylaxis of children within families. Am J DisChild 1986; 140:706-9.
9. Crawford SA, Clover RD, Abell TD, et al. Rimantadine pro-phylaxis in children: a follow-up study. Pediatr Infect Dis J1988;7:379-83.
10. Oker-Blom N, Hovi T, Leinikki P, et al. Protection of manfrom natural infection with influenza A2 Hong Kong virus byamantadine: a controlled field trial. Br Med J 1970;3:676-8.
11. Pettersson RF, Hellstrom P-E, Penttinen K, et al. Evaluation ofamantadine in the prophylaxis of influenza A (H1N1) virusinfection: a controlled field trial among young adults andhigh-risk patients. J Infect Dis 1980;142:377-83.
12. Monto AS, Gunn RA, Bandyk MG, et al. Prevention ofRussian influenza by amantadine. JAMA 1979;241:1003-7.
13. Glezen WP, Couch RB. Influenza viruses. In: Evans AS, ed.Viral infections in humans—epidemiology and control. 3rded. New York, NY: Plenum Medical Book Company, 1989:419-49.
14. Collins SD, Lehmann J. Trends and epidemics of influenzaand pneumonia, 1918-1951. Public Health Rep 1951;66:1487-507.
15. Patterson KD. Pandemic influenza, 1700-1900: a study inhistorical epidemiology. Totowa, NJ: Rowman and Littlefield,1986.
16. Masurel N, Marine WM. Recycling of Asian and Hong Konginfluenza A virus hemagglutinins in man. Am J Epidemiol1973;97:44-9.
17. DauerCC, Serfling RE. Mortality from influenza, 1957-1958and 1959-1960. Am Rev Respir Dis 1961;83(2 Suppl):15-26.
18. Crosby AW. America's forgotten pandemic: the influenza of1918. Cambridge, England: Cambridge University Press,1989.
19. Frost WH. The epidemiology of influenza. J Am Med Assoc1919;73:313-18.
20. Eickhoff TC, Sherman IL, Serfling RE. Observations on ex-cess mortality associated with epidemic influenza. JAMA1961;176:776-82.
21. Collins SD. Age and sex incidence of influenza and pneumo-nia morbidity and mortality in the epidemic of 1928-29 withcomparative data for the epidemic of 1918-19. Public HealthRep 1931:46:1909-37.
22. Noble GR. Epidemiological and clinical aspects of influenza.In: Beare AS, ed. Basic and applied Influenza research. BocaRaton FL: CRC Press, 1982:11-50.
23. Harris JW. Influenza occurring in pregnant women: a statis-tical study of thirteen hundred and fifty cases. J Am MedAssoc 1919:72:978-80.
24. Woolston WJ, Conley DO. Epidemic pneumonia (Spanishinfluenza) in pregnancy: effect in one hundred and one cases.J Am Med Assoc 1918;71:1898-9.
25. Parkman PD, Hopps HE, Rastogi SC, et al. Summary ofclinical trials of influenza virus vaccines in adults. J Infect Dis1977;136(suppl):S722-30.
26. Serfling RE, Sherman IL, Houseworth WJ. Excess pneumo-nia-influenza mortality by age and sex in three major influenzaA2 epidemics, United States, 1957-58, 1960 and 1963. Am JEpidemiol 1967;86:433-41.
27. Choi K, Thacker SB. Mortality during influenza epidemics inthe United States, 1967-1978. Am J Public Health 1982;72:1280-3.
28. Ailing DW, Blackwelder WC, Stuart-Harris CH. A study ofexcess mortality during influenza epidemics in the UnitedStates, 1968-1976. Am J Epidemiol 1981:113:30-43.
29. Lui KJ, Kendal AP. Impact of influenza epidemics on mor-
tality in the United States from October 1972 to May 1985.Am J Public Health 1987;77:712-16.
30. Langmuir AD. Epidemiology of Asian influenza: with specialemphasis on the United States. Am Rev Respir Dis 1961;83(2Suppl):2-10.
31. Freeman DW, Bamo A. Deaths from Asian influenza associ-ated with pregnancy. Am J Obstet Gynecol 1959;78:1172-5.
32. Robinson JC, Hulka JF. Influenza in pregnancy. Clin ObstetGynecol 1959:2:649-57.
33. Widelock D, Csizmas L, Klein S. Influenza, pregnancy, andfetal outcome. Public Health Rep 1963;78:1-11.
34. Cockburn WC, Delon PJ, Ferreira W. Origin and progress ofthe 1968-69 Hong Kong influenza epidemic. Bull WorldHealth Organ 1969;41:345-8.
35. Schulman JL, Kilboume ED. The antigenic relationship of theneuraminidase of Hong Kong virus to that of other humanstrains of influenza A virus. Bull World Health Organ 1969;41:425-8.
36. Sharrar RG. National influenza experience in the USA,1968-69. Bull World Health Organ 1969;41:361-6.
37. Couch RB, Kasel JA, Gerin JL, et al. Induction of partialimmunity to influenza by a neuraminidase-specific vaccine.J Infect Dis 1974; 129:411-20.
38. Glezen WP, Loda FA, Denny FW. A field evaluation ofinactivated, zonal-centrifuged influenza vaccines in childrenin Chapel Hill, North Carolina, 1968-69. Bull World HealthOrgan 1969;41:566-9.
39. Glezen WP, Keitel WA, Taber LH, et al. Age distribution ofpatients with medically-attended illnesses caused by sequen-tial variants of influenza A/H1N1: comparison to age-specificinfection rates, 1978-1989. Am J Epidemiol 1991;133:296-304.
40. Glezen WP, Payne AA, Snyder DN, et al. Mortality andinfluenza. J Infect Dis 1982;146:313-21.
41. Troendle JF, Demmler GJ, Glezen WP, et al. Fatal influenzaB virus pneumonia in pediatric patients. Pediatr Infect Dis J1992
42. Glezen WP, Couch RB, Taber LH, et al. Epidemiologic ob-servations of influenza B virus infections in Houston, Texas,1976-1977. Am J Epidemiol 1980;l 11:13-22.
43. Frank AL, Taber LH, Glezen WP, et al. Influenza B virusinfections in the community and the family: the epidemics of1976-1977 and 1979-1980 in Houston, Texas. Am J Epide-miol 1983; 118:313-25.
44. Couch RB, Kasel JA, Glezen WP, et al. Influenza: its controlin persons and populations. J Infect Dis 1986; 153:431-40.
45. Perrotta DM, Decker M, Glezen WP. Acute respiratory dis-ease hospitalizations as a measure of impact of epidemicinfluenza. Am J Epidemiol 1985;122:468-76.
46. Glezen WP, Decker M, Joseph SW, et al. Acute respiratorydisease associated with influenza epidemics in Houston,1981-1983. J Infect Dis 1987;155:1119-26.
47. McBean AM, Babish JD, Warren JL. The impact and cost ofinfluenza in the elderly. Arch Intern Med 1993;153:2105-ll.
48. Foster DA, Talsma A, Furumoto-Dawson A, et al. Influenzavaccine effectiveness in preventing hospitalization for pneu-monia in the elderly. Am J Epidemiol 1992,136:296-307.
49. Fedson DS, Wajda A, Nicol JP, et al. Clinical effectiveness ofinfluenza vaccination in Manitoba. JAMA 1993;270:1956-61.
50. Nichol KL, Margolis KL, Wuorenma J, et al. The efficacy andcost effectiveness of vaccination against influenza amongelderly persons living in the community. N Engl J Med 1994;331:778-84.
51. Longini IM Jr, Koopman JS, Monto AS, et al. Estimatinghousehold and community transmission parameters for influ-enza. Am J Epidemiol 1982;115:736-51.
52. Falsey AR, Cunningham CK, Barker WH, et al. Respiratorysyncytial virus and influenza A infections in the hospitalizedelderly. J Infect Dis 1995;172:389-94.
53. Frost WH. Statistics of influenza morbidity: with special ref-erence to certain factors in case incidence. Public Health Rep
Epidemiol Rev Vol. 18, No. 1, 1996

76 Glezen
1920;35:584-97.54. Dunn FL, Carey DE, Cohen A, et al. Epidemiologic studies of
Asian influenza in a Louisiana parish. Am J Hyg 1959;70:351-71.
55. Chin TDY, Foley JF, Doto IL, et al. Morbidity and mortalitycharacteristics of Asian strain influenza. Public Health Rep1960;75:149-58.
56. Jordan WS Jr, Denny FW Jr, Badger GF, et al. A study ofillness in a group of Cleveland families. XVII. The occurrenceof Asian influenza. Am J Hyg 1958;68:190-212.
57. Davis LE, Caldwell GG, Lynch RE, et al. Hong Konginfluenza: the epidemiologic features of a high school familystudy analyzed and compared with a similar study during the1957 Asian influenza epidemic. Am J Epidemiol 1970;92:240-7.
58. Fox JP, Hall CE, Cooney MK, et al. Influenzavirus infectionsin Seattle families, 1975-1979. I. Study design, methods andthe occurrence of infections by time and age. Am J Epidemiol1982;116:212-27.
59. Jordan WS Jr. The mechanism of spread of Asian influenza.Am Rev Respir Dis 1961;83(2 Suppl):29-35.
60. Glezen WP. Serious morbidity and mortality associated withinfluenza epidemics. Epidemiol Rev 1982;4:25-44.
61. Glezen WP, Couch RB. Interpandemic influenza in the Hous-ton area, 1974-76. N Engl J Med 1978;298:587-92.
62. Jennings LC, Miles JAR. A study of acute respiratory diseasein the community of Port Chalmers. II. Influenza A/PortChalmers/1/73 intrafamilial spread and the effect of antibodiesto the surface antigens. J Hyg (Lond) 1978;81:67-75.
63. Taber LH, Paredes A, Glezen WP, et al. Infection with influ-enza A/Victoria virus in Houston families, 1976. J Hyg (Lond)1981;86:303-13.
64. Elveback LR, Fox JP, Ackerman E, et al. An influenza sim-ulation model for immunization studies. Am J Epidemiol1976,103:152-65.
65. Glezen WP. Influenza surveillance in an urban area. CanJ Infect Dis 1993;4:272-4.
66. Glezen WP, Decker M, Perrotta DM. Survey of underlyingconditions of persons hospitalized with acute respiratory dis-ease during influenza epidemics in Houston, 1978-1981. AmRev Respir Dis 1987;136:550-5.
67. Glezen WP, Paredes A, Taber LH. Influenza in children:relationship of other respiratory agents. JAMA 1980;243:1345-9.
68. Glezen WP. Considerations of the risk of influenza in childrenand indications for prophylaxis. Rev Infect Dis 1980;2:408-20.
69. Edelen JS, Bender TR, Chin TDY. Encephalopathy and peri-carditis during an outbreak of influenza. Am J Epidemiol1974;100:79-84.
70. Price DA, Postlethwaite, RJ, Longson M. Influenzavirus A2infections presenting with febrile convulsions and gastrointes-tinal symptoms in young children. Clin Pediatr (Phila) 1976;15:361-7.
71. Delorme L, Middleton PJ. Influenza A virus associated withacute encephalopathy. Am J Dis Child 1979;133:822-4.
72. Middleton PJ, Alexander RM, Szymanski MT. Severe myo-sitis during recovery from influenza. Lancet 1970;2:533-5.
73. Dagan R, Hall CB. Influenza A virus infection imitatingbacterial sepsis in early infancy. Pediatr Infect Dis 1984;3:218-21.
74. Prevention and control of influenza recommendations of theAdvisory Committee on Immunization Practices (ACIP): Cen-ters for Disease Control and Prevention. MMWR Morb MortalWkly Rep 1995;44(RR3):l-22.
75. Longini IM. Modeling influenza epidemics. In: Kendal AP,Patriarca PA, eds. Options for the control of influenza: pro-ceedings of a Viratek-UCLA Symposium, Keystone, Colo-rado, April 20-25, 1985. New York, NY: Alan R. Liss,1986:89-105.
76. Maassab HF, Francis T Jr, Davenport FM, et al. Laboratoryand clinical characteristics of attenuated strains of influenzavirus. Bull World Health Organ 1969;41:589-94.
77. Couch RB, Quarles JM, Cate TR, et al. Clinical trials with livecold-reassortrant influenza virus vaccines. In: Kendal AP,Patriarca PA, eds. Options for the control of influenza: pro-ceedings of a Viratek-UCLA Symposium, Keystone, Colo-rado, April 20-25, 1985. New York, NY: Alan R. Liss,1986:223-41.
78. Edwards KM, Dupont WD, Westrich MK, et al. A randomizedcontrolled trial of cold-adapted and inactivated vaccines forthe prevention of influenza A disease. J Infect Dis 1994;169:68-76.
79. Clover RD, Crawford S, Glezen WP, et al. Comparison ofheterotypic protection against influenza A/Taiwan/86 (H1N1)by attenuated and inactivated vaccines to A/Chile/83-like vi-ruses. J Infect Dis 1991;163:300-4.
80. Piedra PA, Glezen WP. Influenza in children: epidemiology,immunity, and vaccines. Semin Pediatr Infect Dis 1991 ;2:140-6.
81. Clements ML, Betts RF, Murphy BR. Advantage of liveattenuated cold-adapted influenza A virus over inactivatedvaccine for A/Washington/80 (H3N2) wild-type virus infec-tion. Lancet 1984;l:705-8.
82. Monto AS, Davenport FM, Napier JA, et al. Modification ofan outbreak of influenza in Tecumseh, Michigan by vaccina-tion of schoolchildren. J Infect Dis 1970;122:16-25.
83. Warburton MF, Jacobs DS, Langford WA, et al. Herd immu-nity following subunit influenza vaccine administration. MedJ Aust 1972;2:67-70.
Epidemiol Rev Vol. 18, No. 1, 1996