
Emergency Surgery Framework
36
A framework for emergency surgery in Victorian public health services
-
Upload
halosunyrtimr6 -
Category
Documents
-
view
224 -
download
0
Transcript of Emergency Surgery Framework
7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 1/36
A framework for emergency
surgery in Victorian publichealth services

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 2/36
4 Clinical review of area mental health services 1997-2004
7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 3/36
A ramework or emergency
surgery in Victorian public
health services
7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 4/36
I you would like to receive this publication in an accessible ormat please phone 03 9096 1287
using the National Relay Service 13 36 77 i required, or email: [email protected]
This document is also available in PDF ormat on the internet at: www.health.vic.gov.au/surgery
© Copyright, State o Victoria, Department o Health 2012
This publication is copyright, no part may be reproduced by any process except in accordance with
the provisions o the Copyright Act 1968.
Authorised and published by the State Government o Victoria, 50 Lonsdale Street, Melbourne.
February 2012 (1201020)
Print managed by Finsbury Green. Printed on sustainable paper.
Acknowledgements
The ramework was developed in consultation with the Emergency Surgery Working Group.
Thanks to the ollowing working group members or their contribution:
Associate Proessor Daryl Williams – Melbourne Health
Ms Cath Cronin – Alred Health
Mr Martin Smith – Eastern Health
Associate Proessor Elton Edwards – Alred Health
Mr Frank Miller – Northeast Health Wangaratta
Ms Paula Foran – South West Health Care Warrnambool
Associate Proessor Melinda Truesdale – Melbourne Health
Associate Proessor Bob Spychal – Peninsula Health
Associate Proessor Nerina Harley – Melbourne Health
Proessor David Watters – Barwon Health
Proessor Russell Gruen – Alred Health
Mr Dhan Thiruchelvam – St Vincent’s Health and Eastern Health
Mr Denis O’Leary – Peninsula Health
Dr Martin Lum – Department o Health
Mr Mark Gill – Department o Health
Mr Terry Symonds – Department o Health
Ms Sue O’Sullivan – Department o Health
Ms Sandy Bell – Department o Health
Ms Lisa Clough – Department o Health

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 5/36
iii
Purpose 1
Dening emergency surgery 2
The Victorian context 4
Principles underpinning provision o emergency surgical services 5
Translating principles into practice 6
Appendices 19
Reerences 27
Contents

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 6/36
1
The availability o timely and high-quality emergency surgery is critical to the unctioning o the public
health system and is a high priority or the Victorian community.
The ramework has been developed by the department in collaboration with the Emergency Surgery
Working Group, a sub-group o the Ministerial Advisory Committee on Surgical Services and other
key stakeholders.
Implementing continuous improvements and innovation in health services is a priority area o the
Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan. The ramework contains
broad principles that underpin the delivery o sae, high-quality emergency surgical services. These
principles have been drawn rom published research, expert opinion and the advice o clinical
experts on the ESWG. The ramework aims to share this up-to-date inormation and identies a
number o key activities that will assist health services to optimise the quality o their emergency
surgery services.
The ramework will inorm the development o uture emergency surgery initiatives, particularly in
relation to access, health service capacity and capability and planning or emergency surgery demand.
Purpose

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 7/36
2
In Victoria, emergency surgery is generally dened as the provision o a surgical procedure which,
in the opinion o the treating clinician, is necessary and admission or which cannot be delayed.
Emergency surgery is oten about saving lives, organs and limbs. Examples o conditions that may
require emergency surgery include:
• trauma,includingbrokenbonesandbluntpenetratinghead,chestandabdominalinjuries
• gastrointestinalhaemorrhagecompromisingthepatient’sbloodsupply
• strangulatedhernia
• acuteappendicitis
• emergencycaesareansection.
Emergency surgery also encompasses other types o urgent surgery or which there are potential
threats and risks to quality o lie, such as ractured neck o emur.
Following a review o literature and consultations with expert stakeholders, the ollowing denition
was agreed or emergency surgery in Victoria:
Emergency surgery
‘Surgery where, in the opinion o the treating clinician, the admission or procedure cannot be
delayed. This is inscribed with varying degrees o urgency’
The denition o emergency surgery used or the purpose o the ramework has some crossover
with the denition o elective surgery. In Australia, elective surgery is commonly dened as surgerythat,inthejudgementofaspecialist,isnecessaryandadmissionforwhichcanbedelayedforat
least 24 hours.
An example o the intersection between emergency and elective surgical practice exists in instances
where patients arrive at the hospital in an unplanned manner and require surgery within the ollowing
week. Oten it may be sae or these patients to be sent home and return or admission via an
elective surgery pathway within the seven-day timerame. Another example can be ound in cases
where patients are admitted to hospital under a non-surgical specialty and are then ound to require
unplanned surgery.
The denition o emergency surgery used in this ramework deliberately includes these groups o
unplanned patients because the challenges o surgical scheduling or these groups are similar tomore urgent emergency patients. Moreover, these groups are oten accommodated via the same
processes and resources that are used or urgent emergency surgery patients.
Defning emergency surgery

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 8/36
3
A set o denitions used in relation to emergency surgery has been developed and is outlined below
in Table 1.
Table 1: Denitions relating to emergency surgery
Term Denition
Emergency surgery Surgery where, in the opinion o the treating clinician, the admission
or procedure cannot be delayed. This is inscribed with varying degrees
o urgency.
Standard-hours surgery In most hospitals, the standard-hours operating period is between 8 am
and 5 pm Monday to Friday. There are minor variations in start or nish
times between hospitals.
Twilight sessions Some hospitals have extended operating hours to 8 pm or 10 pm. These
are oten reerred to as twilight sessions.
Ater-hours surgery In most hospitals, ater-hours surgery occurs between 5 pm and 12 am
Monday to Friday and all weekend.
Night-time hours In most hospitals, the hours between 12 am and 8 am Monday to Friday
are considered night-time hours.
Elective surgery The Australian Institute o Health and Welare National health data
dictionary (2008) denes elective surgery as ‘surgery that, in the opiniono the treating clinician, is necessary and admission or which can be
delayed or at least twenty-our hours’.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 9/36
4
Analysis o the data on emergency surgery in Victoria shows that:
• in2010–11,24percent(58,546separations)ofacutepublichospitalsurgicalseparations
were emergency surgery cases
• in2010–11,87percentofallemergencysurgerywasperformedinthepublicsector
• atsomelargemetropolitanhealthservices,theproportionofemergencysurgeryadmissions
has been as high as 38 per cent
• overthelastveyearshealthservicesinVictoriahaveexperiencedsteadygrowthinemergency
surgery demand
• growthisgreatestinmetropolitanhealthservices
• ataspecialtylevel,thegreatestgrowthhasbeeningeneralsurgery,neurosurgeryand
plastic surgery
• overthelastveyears,tertiaryhealthserviceshavetreatedmorecomplexemergency
surgery patients
• therehasbeenagradualdecreaseinlengthofstayforemergencysurgeryseparations
at most Victorian health services.
Some o the actors contributing to the increased demand or emergency surgery are:
• ariseinchronicandcomplexillnesses
• agrowingandageingpopulation
• ariseinratesoftrauma
• thedevelopmentofnewsurgicaltreatmentoptionsfromadvancesinmedicaltechnology.
More detailed descriptions o trends in the provision o emergency surgery are documented in
Appendix 1.
The work o surgical services in Victoria is underpinned by a suite o documents which set
directions or provision o clinical services more broadly. These documents include:
Victorian clinical governance policy ramework: a guidebook (Department o Health 2009b)
www.health.vic.gov.au/docs/doc/Victorian-clinical-governance-policy-ramework
Promoting eective communication among healthcare proessionals to improve patient saety and
quality o care (Department o Health 2010b)
www.health.vic.gov.au/qualitycouncil/downloads/communication_paper_120710.pd
Victorian Health Priorities Framework 2012–2022: Metropolitan Health Plan
(Department o Health 2011d) www.health.vic.gov.au/healthplan2022/
The emergency surgery ramework has been developed to complement these resources.
The Victorian context
7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 10/36
5
The department encourages health services to consider applying the ollowing nine principles to
the delivery o emergency surgical services in Victoria. The principles are relevant to all emergency
surgical services in Victorian public hospitals, including all surgical specialties. These principles have
been drawn rom published research, expert opinion and the advice o clinical experts on the ESWG.
1. Emergency surgery demand, access and perormance is routinely measured by health
services.
2. Balancing access to elective and emergency surgery is integral to optimal patient
care and health service perormance.
3. Emergency surgery capacity is matched to demand, and where demand necessitates,
elective and emergency surgery streams are separated.
4. Where clinically appropriate, emergency surgery is scheduled in standard hours.
5. Emergency surgical services are consultant-led.
6. Health service policies and processes or emergency surgery use a single statewide
system or urgency categorisation.
7. Health services have local escalation plans to support optimal team communication,
resource utilisation and confict resolution to support prompt access to surgery.
8. Health services use common emergency surgery measures or benchmarking and
continual service improvement.
9. Health services have local policies and processes or communication with patients
and amilies. This includes inormation about consent.
While applying these principles to the delivery o emergency surgery services, enough fexibility
needs to be maintained to respond to the needs o local communities, organisational arrangements
and priorities.
Positive leadership rom senior medical, nursing and management sta will be required to acilitate
the adoption o these principles. These sta will be important leaders o change to drive local
innovation and service-delivery improvements. Health services can also draw on a range o multi-
dimensional strategies available through redesign, service improvement and clinical saety resourcesto implement the above principles.
The department will work closely with health services to implement the ramework. The ESWG will
guide and oversee the implementation o key strategic elements o the ramework. In addition, the
department will engage with individual health services to support implementation o the key activities
required to urther enhance the quality o emergency surgery services.
Principles underpinning provision
o emergency surgical services
7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 11/36
6
Principle 1: Emergency surgery demand, access and
perormance is measured by health services routinely.
A number o studies in Australia have conrmed that emergency surgery demand is measurable,
and at a statewide and local health-service level the demand is predictable, with peaks and troughs
in activity occurring at similar times o the year, days o the week and times o the day. Additionally,
at a health-service level, emergency surgery demand shows less variability over consecutive years
when compared to elective surgery. The predictable nature o emergency surgery means that health
services can plan or emergency surgery demand and design models o care that eectively address
this demand.
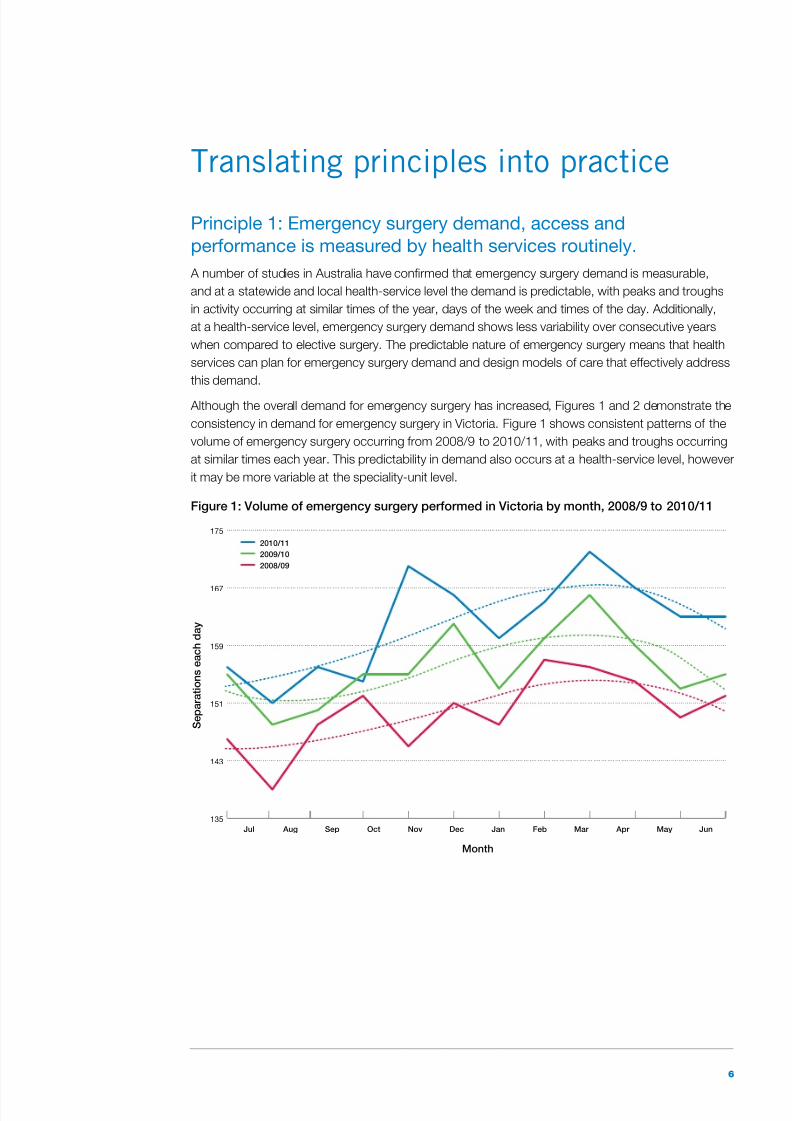
Although the overall demand or emergency surgery has increased, Figures 1 and 2 demonstrate the
consistency in demand or emergency surgery in Victoria. Figure 1 shows consistent patterns o the
volume o emergency surgery occurring rom 2008/9 to 2010/11, with peaks and troughs occurring
at similar times each year. This predictability in demand also occurs at a health-service level, however
it may be more variable at the speciality-unit level.
Figure 1: Volume o emergency surgery perormed in Victoria by month, 2008/9 to 2010/11
135
143
151
159
167
175
2010/11
2009/10
2008/09
JunMay Apr Mar FebJanDecNovOctSep AugJul
S e p a r a t i o n s
e a c h
d a y
Month
Translating principles into practice

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 12/36
7
Patients requiring emergency surgery come rom many sources, such as transers rom other
hospitals, inpatient wards, transers rom specialist clinics, elective surgery cases with complications,
or presentations to the emergency department (ED). The most common pathway is presentation to
the ED.
The number o emergency surgery arrivals via the ED is airly consistent across all seven days o the
week, with emergency surgery patients consistently arriving in the ED at around midday on each day
o the week (Figure 2). One-third o all emergency surgery patients present to the ED between 10 am
and 2 pm, with nearly 60 per cent presenting between 8 am and 4 pm.
Figure 2: Volume o emergency surgery patient arrivals in the ED, by time o day and day
o the week
0
100
200
300
400
500
0 2 : 0 0
0 1 : 0 0
2 4 : 0 0
2 3 : 0 0
2 2 : 0 0
2 1 : 0 0
2 0 : 0 0
1 9 : 0 0
1 8 : 0 0
1 7 : 0 0
1 6 : 0 0
1 5 : 0 0
1 4 : 0 0
1 3 : 0 0
1 2 : 0 0
1 1 : 0 0
1 0 : 0 0
0 9 : 0 0
0 8 : 0 0
0 7 : 0 0
0 6 : 0 0
0 5 : 0 0
0 4 : 0 0
0 3 : 0 0
0 2 : 0 0
0 1 : 0 0
A r r i v a l s e a c h h o u
r o f e a c h d a y o f t h e w e e k
Arrival time in the ED
Monday
Tuesday
Wednesday
Thursday
Friday
Saturday
Sunday
Health services can use ED data to increase understanding o emergency surgery demand and planor this demand accordingly. However, the management o emergency surgical services requires
considerationofchallengesalongtheentirepatientjourney,frominitialpresentationathospital
through to transer o care.
Key activities and next steps:
• SystematicallycollectandanalyseEDdatainordertounderstandemergencysurgerydemand
and its impact on elective surgery and ED perormance.
• Planandallocatehealthserviceresourcestomeetanticipateddemand.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 13/36
8
Principle 2: Balancing access to elective and emergency surgery
is integral to optimal patient care and health service perormance.
Patient-centred surgery: strategic directions or surgical services in Victoria’s public hospitals
2010–15 (Department o Health 2009a) identies the issues in managing the oten competing
demands o emergency and elective surgery and the current constraints in delivering timely
emergencysurgery.Thedocumentreectsthewholesurgicaljourney,whichincludesthepatient
reerral, assessment, treatment and recovery processes, and outlines reorm directions or
emergency and elective surgical services.
It is important to note that emergency surgery demand has direct fow-on eects to other areaso a health service, such as elective surgery, the intensive care unit and the ED. Any service-delivery
model or emergency surgery needs to take into consideration these interrelated areas.
Perormance targets in interacing areas such as the ED and elective surgery can impact on
access to emergency surgery.
A key challenge encountered by health services is balancing elective and emergency surgery
demand while ensuring optimal patient care and health service perormance. I the allocation
o operating theatre time or emergency surgery does not correlate with demand or it, this may
have an unintended negative impact on elective surgery perormance due to postponements
and longer waiting times.
In many health services, both elective and emergency caseloads share the same operating theatres,
surgeons and teams. In these situations, elective and emergency surgery are inherently linked in
spite o the dierences between the patient caseloads. A balanced approach in the provision o
emergency and elective surgery can acilitate improved access, and result in improved patient
outcomes, decreased cancellations o elective and emergency surgery, shorter waiting times and
reduced rates o emergency surgery being undertaken ater-hours.
There is no one-size-ts-all approach to determining the appropriate model o care. Balancing the
two streams o surgery in a health service needs to be considered in light o local capacity, demand
and constraints. The department does not allocate specic unding or emergency surgery to health
services. Health services are responsible or allocating unds internally to procedures or clinical areas,
such as emergency surgery, in response to changing demands. This unding model allows clinical
decisions to be made at the local level.
Key activities and next steps:
• Improvetheutilisationofoperatingtheatresandotherhigh-costassetsandinfrastructure
by matching capacity with demand.
• Developtoolsforprioritisingelectiveandemergencysurgerypatientgroupswithinand
between clinical specialities.
• Minimisenon-operatingtimethroughefcientpatientturn-around.
• Designsurgicalrosterstotakeaccountofbothelectiveandemergencycommitments.
• Improveaccesstosupportservicessuchasradiologyandpathology.
• Minimisemultiplecancellationsofemergencysurgerycases.• Considertheinfrastructurerequiredforemergencyandelectivesurgerywhenredeveloping
existing acilities or developing new acilities.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 14/36
9
Principle 3: Emergency surgery capacity is matched to demand,
and where demand necessitates, elective and emergency surgery
streams are separated.
Increased demand and complexity mean managing emergency surgery poses a number o
challenges or the healthcare system. Emergency surgery models o care need to be fexible so that
services can respond to change over time.
One way o minimising the impact o emergency surgery on elective surgery is to separate the two
streams, either physically or administratively. This allows or a high volume o elective procedures
to be undertaken without cancellations or delays due to emergency surgery demand. Separatingelective and emergency surgery is accepted internationally as a way o improving access. Sta can
plan a more ecient program o surgery while providing greater certainty to patients.
The National Health and Hospitals Reorm Commission (2009) has reported that separating elective
rom emergency surgery in purpose-built centres is a way or public hospitals to gain eciencies in the
provision o surgical services. In a recent paper, Surgery utures: a plan or Greater Sydney , NSW Health
reported an ‘increase in both procedural and patient-fow eciencies o 10 to 20 per cent’ in sites that
separated elective and emergency surgery. Victorian health services have also shown improvement in
surgery perormance since quarantining elective and emergency surgery. This can be demonstrated by
reductions in postponements, length o stay and patients waiting longer than clinically recommended.
Victoria has unded two purpose-built, stand-alone elective surgery centres at Alred Health and
Austin Health. Alred Health established the Alred Centre in 2007, which is a separate theatre suite
used to treat elective surgery patients, connected to the main campus via a walkway. A slightly
dierent model operates at Austin Health, which has dedicated one o its two hospital campuses
to elective surgery only. By removing elective surgery rom the main campuses, Alred Health and
Austin Health have been better able to manage their respective emergency surgery loads. For
health services with high surgical demand, this can be an eective strategy or balancing elective
and emergency surgery streams. This approach may not be warranted at health services with lower
levels o emergency surgery demand, where administrative separation may be more appropriate.
It is important that administration procedures are complementary and not duplicated when elective
and emergency surgical streams are separated.
Where caseloads are high in particular specialties (such as orthopaedics, general surgery, obstetrics orplastic surgery) it may be appropriate or health services to allocate specic operating theatre times or
emergency cases in these specialties (based on the level o demand and available surgical capacity).
Key activities and next steps:
• Systematicallycollectandanalysesurgerydatatodetermineifdemandnecessitates
separating emergency surgery and elective surgery streams, either physically or
administratively.
• Identifyanddevelopgoodpracticeinthemanagementofelectiveandemergencysurgery,
including potential new models o care and workorce organisation or high-volume conditions
requiring surgery.
• Supportclinicianstoaccessandapplyevidenceaboutsurgicalproceduresandmodels
o care.
• Evaluatetheseparationofelectiveandemergencysurgerystreamsregularlytobuildan
evidence base or eective delivery o both elective and emergency surgery.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 15/36
10
Principle 4: Where clinically appropriate, emergency surgery
is scheduled in standard hours.
Health services may perorm emergency surgery out o hours in an eort to reduce the impact o
emergency surgery cases on scheduled elective cases, particularly where resources are ully utilised.
However, out-o-hours surgery is oten associated with higher risks to the acility.
There is evidence that prolonged hours o work and work at night carry a greater risk o undermining
surgical perormance and urther increase the risk o serious errors that can lead to death or serious
morbidity. In recognition o the potentially serious consequences o atigue, the Royal Australasian
College o Surgeons (2007) developed guidelines or sae working hours. These guidelines includeon-call and shit rostering, handover, and the responsible management o stress and atigue.
The Royal Australasian College o Surgeons Divisional Group o Rural Surgery (2005) identied
that continuous working periods greater than 14 hours, and a lack o sucient breaks during and
between work periods, will increase the risk o atigue and atigue-related errors.
In order to assist hospitals and sta to measure the risks associated with their work hours, the
Australian Medical Association (2005) published guidelines around sae working hours or doctors
working in hospitals. These guidelines incorporate a risk-assessment checklist or surgeons.
One o the key principles o the emergency surgery ramework is that where clinically appropriate,
emergency surgery should be scheduled in standard hours. Any re-alignment o operating theatre
templates should incorporate perorming as much emergency surgery within standard hours as
possible. Due to the nature o emergency surgery, there will always be a proportion o complex lie-,
limb- or organ-saving emergency surgery that must occur at night (Faiz et al. 2007). Emergency
surgical services need to recognise and incorporate this need. However, other emergency surgical
cases are best perormed during standard hours.
Evidence rom New South Wales and Western Australia indicates that the establishment o specic
emergency surgery models which incorporate dedicated in-hours surgeons and access to dedicated
in-hours operating theatre time has led to improved time to assessment in the ED, aster admission,
aster time to surgery, decreased number o elective surgery hospital-initiated postponements due
to emergency surgery, and decreased length o stay (Parasyn et al. 2009; Cox et al. 2010).
Evidencefromthesesamejurisdictionshasalsoshownthatbringingemergencysurgeryinto
standard hours is clinically sae, cost-neutral and may even save money or the organisation in the
long term (Parasyn et al. 2009; Cox et al. 2010). Necessary out-o-hours emergency surgery must
be balanced with sae working hours, and health services should instigate operational strategies
to manage this balance.
Key activities and next steps:
• Redesignoperatingtheatretemplatestoscheduleasmuchemergencysurgeryaspossible
within standard hours.
• Monitortheatredatatoreviewpatternsoftheatreuseandtodemonstratereformstobring
surgery within standard hours.
• Supportclinicianstoaccessandapplyevidenceaboutemergencysurgerymanagement o patients and overall models o care to support more surgery being undertaken within
standard hours.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 16/36
11
Principle 5: Emergency surgical services are consultant-led.
Evidence suggests that eective emergency surgery models o care are contextually appropriate
and based on principles o consultant leadership.
The value o consultant-led emergency care is well recognised and supported by evidence
(Parasyn et al. 2009). The benets o consultant leadership include:
• moreaccurateandtimelydecisionmaking
• reductioninunnecessaryclinicalinvestigations
• greatertraineesupervisionandsharingofexpertise
• betteraccesstoday-timeemergencysurgery(wheredesignatedin-hoursoperatingtheatre time is available) and less night-time surgery
• apotentialformorecost-effectivedecisionmakingandnancialsavingswithinthehealthservice
• increasedstaffsatisfaction.
It is important to note that clinical leadership does not reer exclusively to surgical sta. Senior
medical sta and senior nursing sta are very important in the provision o eective emergency
surgical services. For example, a number o health services in Victoria use the leadership o senior
anaesthetists to determine the scheduling o emergency surgery cases when several patients o the
same clinical priority require surgery.
The Acute Surgery Unit is a model o consultant-led emergency surgery service delivery that has
been established in a number o health services in Australia. These health services have reported
benets such as those outlined above. Acute Surgery Unit models vary slightly according to local
requirements, however common eatures include:
• aconsultantrosteredonforaperiodofatleast24hours,includingbeingon-siteinstandard
hours to provide clinical support or all stages o patient care
• aformalisedhandoverprocesswithinformationbasedonastandardsetofkeyprinciples
• dedicatedemergencytheatresessionsinstandardhours
• aconsultantbeingpresentwhensurgeryisbeingperformedforteachingandsupervisionpurposes
• agreedclinicalguidelinesorprotocolsforcommonemergencysurgeryadmissions
• designatedAcuteSurgeryUnitbedsforassessmentandmanagement.
Contextual constraints o individual health services mean that dierent consultant-led models o care
will be appropriate at dierent health services. Strategies to improve emergency surgery services sit
alongside, and should be complemented by, a range o inrastructure initiatives and new operational
models o emergency care.
Key activities and next steps:
• Engageleadclinicianstoinvestigatethefeasibilityofestablishingaconsultant-ledemergency
surgery service.
• Whenconsideringaconsultant-ledmodelofcare,healthservicesshouldconsultwithhealth
services that have already established consultant-led models to learn rom their experience.
• Whereaconsultant-ledmodelistobeintroduced,healthservicesshould:
– support a reorganisation o both the model o care and the working arrangements
o medical sta
– establish health service agreement about theatre and bed access
– build clinical guidelines or common procedures over time.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 17/36
12
Principle 6: Health service policies and processes or emergency
surgery use a single statewide system or urgency categorisation.
The clinical urgency o a case underlies every decision about priority or emergency surgery. These
decisions take place in a high-pressure environment that involves non-negotiable time stress, with
potentialformajorpersonalconsequencesandadversepatientoutcomes(Fitzgerald,Lum&Dadich
2006). Each patient’s priority must be considered alongside that o others awaiting emergency
surgery, as cases oten require rescheduling to make way or those deemed more urgent.
Standardised categories o clinical urgency would acilitate consistent decision making and reconcile
differencesinprofessionalopinionsrelatingtopatientpriority(Fitzgerald,Lum&Dadich2006),thereby contributing to quality patient care.
A single statewide system or emergency surgery categorisation will improve the consistency o
decision making across the state, improve communication regarding the relative urgency o patients,
and improve the allocation o theatre resources within health services. Furthermore, a single system
enables benchmarking across similar health services in Victoria.
The six-level emergency surgery urgency categorisation system documented in Appendix 2 includes
indicative time rom booking to arrival in the operating suite. This system is based on the current
system used in a number o health services in Victoria and in New South Wales (NSW Health 2009).
Within this system, there is the opportunity or health services to include more detailed descriptions
as required. At health services where obstetric cases share operating theatre resources with other
surgical specialties, emergency surgery urgency categorisation should include obstetrics.
Key activities and next steps:
• Adoptthesix-levelemergencysurgeryurgencycategorisationsystemdocumentedin
Appendix 2.
• Monitorhealthserviceactivityagainsttheassignmentofurgencycategoriesandpatient
treatment times.
• Evaluatemodelsofcareinrelationtotheurgencycategorisationsystemandbuildanevidence
base or eective delivery o emergency surgery.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 18/36
13
Principle 7: Health services have local escalation plans to support
optimal team communication, resource utilisation and confict
resolution to support prompt access to surgery.
Emergency surgery patients oten have complex and challenging problems. These patients can
present at any time o the day or night, regardless o stang levels. The management o emergency
surgery must take into account unique threats to lie, limb and organ unction. In many cases, these
threats increase with the passage o minutes and hours.
A number o electronic tools exist or communicating about emergency surgery cases. The most
commonly used system in Victoria is the emergency theatre booking system, which allows real-timescheduling, increased transparency o patient bookings, better patient tracking systems and data
collection.
Clinical guidelines (also known as clinical protocols) provide a comprehensive care path or surgical
teamsandaimtoensureroutinemanagementforthemajorityofpatients.Clinicalguidelinesfacilitate
consistentmanagementofemergencysurgerypatientsbutdonotreplaceactiveclinicaljudgement,
which is required to determine when a clinical guideline is appropriate or when variation in care is
required. Clinical guidelines provide an eective and ecient system or monitoring and recording
variances in care or the purpose o reviewing and improving patient care (Earley et al. 2006;
Tallis&Balla1995).
Clinical handover is an essential component o all surgical care, including emergency surgery. The Victorian Surgical Consultative Council has developed guidelines or clinical handover (see
<www.health.vic.gov.au/vscc/practice-statements.htm> or details). Additionally, the Australian
Commission on Saety and Quality in Healthcare (2010) has developed the Organisational
leadership, simple solution development, stakeholder engagement, implementation and evaluation
and maintenance (OSSIE) guide to clinical handover improvement . This guide is designed to assist
organisations to implement a standardised process or handover that is customised to the local
context (see <www.saetyandquality.gov.au> or details). Clinical handover processes have been
incorporated into Acute Surgery Units and have been ound to aid inormal peer review and improve
communication between sta.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 19/36
14
The key eatures o an eective governance structure or emergency surgical services are:
• aclearstatementofrolesandresponsibilities
• cleardelegationsandlinemanagement
• participationinqualityassurancesystems.
Health services have a responsibility to ensure that all services provided to patients are sae,
appropriate and within the capability and role o the service (Department o Human Services 2009).
Credentialing and dening scope o practice is a mechanism by which the community can be
assured that a competent workorce is providing their care (Department o Human Services 2007).
A useul checklist to guide the delivery o sae surgical services has been developed by the WorldHealth Organisation and has been adapted or the local context by the Australian and New Zealand
surgical community. This checklist can be ound at: www.anzca.edu.au/resources/endorsed-guidelines
Key activities and next steps:
• Considertheuseofemergencysurgerytheatrebookingsystemstoidentifyandprioritise
emergency surgery patients.
• Useclinicalguidelinestofacilitateconsistentemergencysurgerypatientmanagement.
• Implementstandardisedclinicalhandoverprocesses.
• Developaneffectivegovernancestructureforemergencysurgerytosupportcliniciansto
make decisions about clinical prioritisation and to enable escalation where required.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 20/36
15
Principle 8: Health services use common emergency surgery
measures or benchmarking and continual service improvement.
The capacity to monitor and evaluate perormance is a critical building block or system-wide
improvement o healthcare delivery and improved patient outcomes. To inorm ongoing service
improvement and enable standardised measurement o emergency surgery perormance or
benchmarking across similar health services, a set o timestamps (Tables 3 and 4) and measures
has been developed. Denitions o timestamps are provided to ensure consistency in measurement.
These items are based on surveys o Victorian health services and similar work conducted interstate
and overseas.
The timestamps in Table 2 allow analysis o the time taken to achieve a denitive treatment decision
(using timestamp 1 and 2) and analysis o access to the operating theatre or patients once a
denitive plan or surgery is made (timestamps 2, 3 and 4). Timestamps specic to the operating
theatre and recovery period (Table 3) allow identication o times and time intervals related to the
procedure in theatre, rather than the process o accessing the required procedure (Table 2).
Table 2: Timestamps or measurement o emergency surgery access
Timestamp Denition
1. Patient arrival in
the emergency
department
Time the patient was rst registered or triaged (whichever comes rst) by
a clerical ocer, triage nurse or doctor in the ED. This is consistent with
the Victorian Emergency Minimum Dataset (VEMD) denition (Department
o Health 2011c), and is the closest reliable measure or when a patient
arrives in the ED.
2. Time o surgery
booking
Time that the booking or surgery is entered in the theatre booking
system.
This provides a proxy measure or the time that the decision or surgery
was made.
3. Patient arrival in
operating theatre
Time when the patient arrives in the anaesthetic bay, or i there is no
anaesthetic bay, the time when the patient arrives in the operating theatre
or procedure room.
4. Procedure start time Time when the procedure is begun (or example, incision or a surgical
procedure, insertion o scope or a diagnostic procedure). This is
consistent with the Victorian Admitted Episodes Dataset (VAED) denition
(Department o Health 2011b).

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 21/36
16
Table 3. Additional operating theatre timestamps
Timestamp Denition
Anaesthetic start Time when anaesthetist begins preparing the patient or an anaesthetic.
Position or prep start Time when the nursing or surgical team begins positioning or prepping
the patient or the procedure.
Procedure or surgery
stop
Time when all the instruments and sponge counts are completed and
veried as correct; all postoperative radiological studies to be done in the
operating or procedural room are completed; all dressings and drains are
secured and the surgeons or physicians have completed all procedure-
related activities on the patient.
Anaesthetic stop
(anaesthetic handover)
Time when anaesthetist hands over care o the patient to a post-
anaesthesia care team.
Patient leaves recovery Time patient leaves recovery.
Time that ‘time out’
was commenced
Timeoutisadeliberatepauseinactivityjustbeforesurgerycommences.
All members o the surgical team veriy the ollowing details:
• presenceofthecorrectpatient
• typeofproceduretobeperformed
• correctproceduresitemarked• anticipatedcriticalevents
• availabilityofrequiredequipment.
Health services are encouraged to review current timestamps and denitions being used, and to
consider incorporation o those outlined in Tables 2 and 3 into local systems. Measurement o
the time periods between timestamps may allow identication o particular points o delay in the
emergencysurgerypatientjourney.
In addition to the timestamps outlined above, collection and analysis o the ollowing measures o
emergency surgery perormance is suggested:
• lengthofhospitalstayforindexprocedures(forexample,emergencycholecystectomy,fractured
neck o emur, acute appendicitis)
• measurementofafter-hourssurgicalactivity(forexample,percentageofnon-life-,limb-or
organ-saving emergency surgery that is perormed between 12 am and 7 am)
• percentageofpostponementsofbookedemergencysurgerycasesthatarenotduetoclinical
reasons. This will include cancellations or reasons such as lack o theatre, surgeon, equipment or
post-operative bed
• pre-operativewaitingtimeforindexconditions(measuredfromtimeofarrivalintheEDtosurgery
start time).
It is important to note that these measures should be considered as base measures only, and health
services may opt to collect additional measures i they have a specic element o care they wish
to monitor. A guide to surgical services redesign measures or improvement (Department o Health2011a) provides an extensive list o possible emergency surgery measures.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 22/36
17
Use o consistent timestamps, denitions and measures to monitor trends and perormance will
allow targeted actions to be undertaken to achieve high standards o emergency surgery care within
each health service. Ongoing measurement will allow monitoring o changes in perormance over
time. Monitoring will also allow health services to benchmark emergency surgery perormance with
similar health services and to share innovations in service delivery. Consistency in measurement will
help ensure that standards o patient saety are uniormly applied across the state.
The Victorian Audit o Surgical Mortality annual report 2009 (Royal Australasian College o Surgeons
2009) reported that o the audited deaths, delays in reerral to a surgical unit were requently
commentedon.Themajorityofsurgicaldeathsinthisauditedseriesoccurredinelderlypatientswith
underlying health problems, admitted as an emergency with an acute lie-threatening condition otenrequiring surgery.
The most common issues reported were delay in transer to a surgical unit, inappropriateness
o the decision to operate and unsatisactory pre- or post-operative assessment. It should be
acknowledged that a number o these were ‘areas o consideration’ and were thereore relatively
minor criticisms. These ndings indicate an opportunity to improve the timeliness o reerrals to
surgical units. Evidence suggests that consultant-led models, such as Acute Surgical Units, are
another possible strategy to address this.
The benets o sharing innovations in emergency surgery service delivery, models o care and
benchmarking perormance across health services was identied in the literature review which
inormed the development o this ramework. The Good practice in management o emergency
surgery: a literature review (Department o Health 2010a) can be downloaded rom: www.health.vic.
gov.au/docs/doc/good-practice-in-management-o-emergency-surgery:-a-literature-review
Key activities and next steps:
• Reviewcurrenttimestampsanddenitionsanddecideonappropriatemeasuresofemergency
surgery perormance.
• Systematicallycollectdatatomonitorperformanceandtrendstoidentifyareasrequiring
improvement.
• Evaluatemodelsofcaretobuildtheevidencebasefortheeffectivedeliveryofemergency
surgery and target actions to address areas requiring improvement.
• Benchmarkemergencysurgeryperformancewithsimilarhealthservicestoshareinnovations
in service delivery.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 23/36
18
Principle 9: Health services have local polices and processes
or communication with patients and amilies. This includes
inormation about consent.
Health services with eective emergency surgical services demonstrate good communication, which
is acilitated through organisational support, systems, resources, polices and processes and regular
sta education. Receiving timely and adequate inormation ensures consent is inormed, and assists
in preparation o patients or surgery by reducing patient and carer anxiety and providing a more
positive experience or patients and carers.
Prior to surgery, patients and their carers should receive inormation about:
• thesurgicaltreatmentandcarerequired
• pre-surgeryfastingrequirements
• thewaitingprocessforsurgery
• thepossibilityofsurgerytimebeingchangedifmoreurgentcasesarise.
Inormation to patients should be provided both verbally and in writing. Written inormation should be
supported with translated material and training or sta and delivered in a culturally sensitive manner.
To improve communication with patients and carers, one health service in Victoria has established an
Emergency Surgery Coordinator. The role o the Emergency Surgery Coordinator is to:
• facilitatetimelyaccesstoemergencysurgerybymaximisingin-hoursemergencysurgerywithoutnegatively impacting on elective surgery throughput
• actasaresourceforsurgicalteamstoexplorealloptionsavailabletoenablesurgeryintheright
setting as quickly as possible
• actasaconduitbetweenpatients,carers,surgeons,anaesthetistsandnursingstafftomanage
patient care
• minimisecancellationsofelectivesurgerypatientsonthedayofsurgeryduetoemergency
surgery demand
• investigatepatientcomplaintsassociatedwithemergencysurgicalservices
• coordinatetheintroductionoftheemergencytheatrebookingsystem.
Key activities and next steps:
• Supportpatientstobeactivepartnersintheircareandprovidehighqualityandaccessible
inormation about their emergency surgery.
• Reviewpracticesforcommunicatingwithpatientsandcarers.
• Provideinformationbothverballyandinwriting,includingtranslatedmaterialforpatientsand
carers rom culturally and linguistically diverse backgrounds.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 24/36
19
Appendix 1: Analysis o emergency surgery in Victoria
Victoria’s emergency surgical services
In 2010–11, 24 per cent o acute hospital1 surgical separations were emergency surgery cases,
which equates to 58,546 emergency surgery procedures according to Victorian Admitted Episodes
Dataset (VAED) data. At some large metropolitan health services the proportion o emergency
surgery admissions can be as high as 38 per cent. Figure 1 shows the proportion o emergency
surgery separations in acute public hospitals in Victoria and shows a gradual increase in demand
or emergency surgery. In 2010–11, 87 per cent o all emergency surgery procedures perormed in
Victoria were provided in the public sector.
Figure 1: Proportion o emergency surgery in acute hospitals in Victoria
S e p a r a t i o n s
P e r c e n t t h a t i s e m
e r g e n c y
Emergency surgery separations
Percent of surgery that is emergency
45,000
47,000
49,000
51,000
53,000
55,000
57,000
2006-072005-06 2007-08 2008-09 2009-10 2010-11
20%
21%
22%
23%
24%
25%
26%
Years
Twomajorfactorsthathaveledtothegrowthindemandforemergencysurgeryhavebeenan
ageing Australian population and increasing rates o trauma.
1 An acute hospital is a hospital with an emergency department.
Appendices

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 25/36
20
Ageing and population growth
An important impact o an ageing population is the increase in the number o older patients with
higher acuity and multiple comorbidities undergoing emergency surgery. Figure 2 shows that in
Victoria, older patients require proportionally more emergency surgery than younger patients.
Figure 2: Emergency surgery separations by age and gender, with comparison to
Victorian population
C o n t r i b u t i o n
o f e a c h c o h o r t
Male surgery Female surgery Male population Female population
0%
1%
2%
3%
4%
00-04 05-09 85+10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84
Age
Trauma
Since the Victorian State Trauma Registry (VSTR) has had ull statewide coverage, the rate o trauma
hasincreased(DepartmentofHealth2010c).TheVSTRrecorded2,646hospitalisedmajortrauma
patientsin2008–09comparedto2,379in2007–08.Theoverallannualrateofhospitalisedmajor
trauma in Victoria was 49 per 100,000 population, compared to 44 in 2007–08, 46 in 2006–07, and
42 in 2005–06. Since 2001–02, there has been an average annual increase in the rate o hospitalised
majortraumaof8.0percent.Whilethemajorityofmajortraumacasesaretypicallyyoungpeople,
there has been a substantial increase in cases involving people aged 75 years and over, rom 10.3
per cent in 2001–02 to 19.1 per cent in 2008–09. This change could be explained by improved
coverage o the VSTR, improvements in case identication, changes in approaches to diagnosis
and management in the elderly, and the ageing population (Department o Health 2010c). This is
demonstratedbytheriseinpercentageofhospitalisedmajortraumapatientsrelatedtolowfallsof
24.6 per cent in 2008–09 compared to 19.6 per cent in 2005–06.
7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 26/36
21
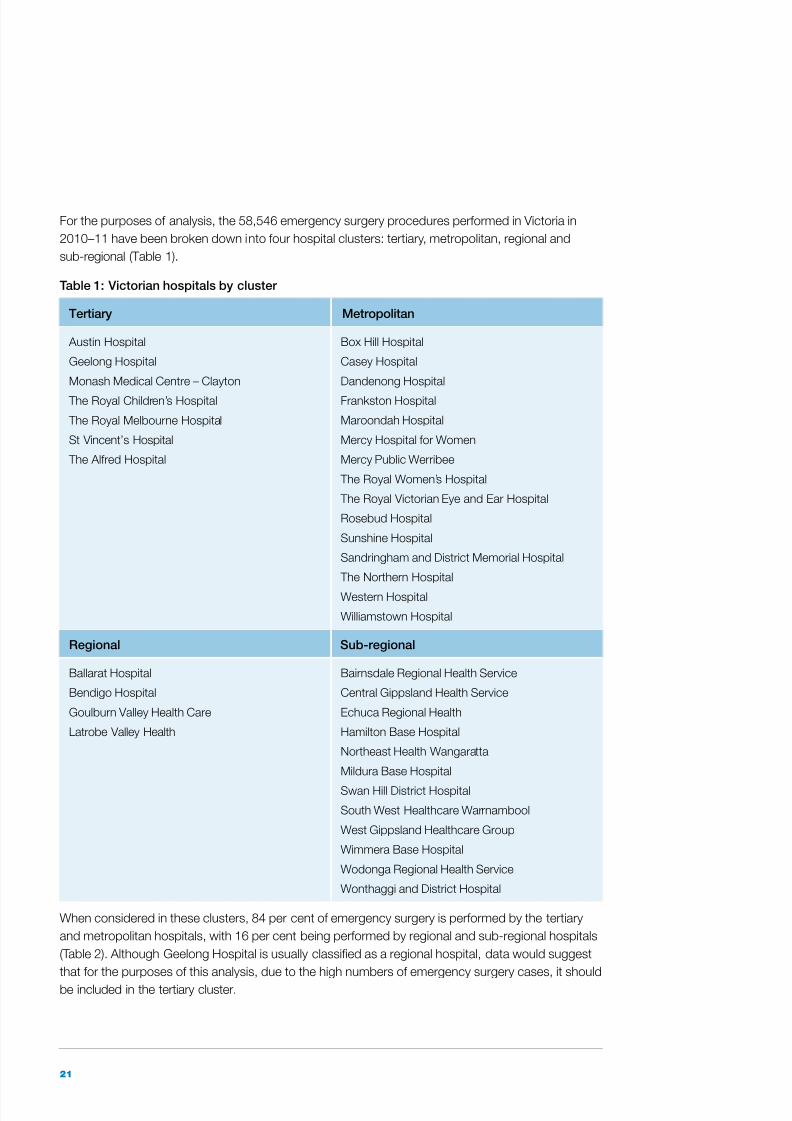
For the purposes o analysis, the 58,546 emergency surgery procedures perormed in Victoria in
2010–11 have been broken down into our hospital clusters: tertiary, metropolitan, regional and
sub-regional (Table 1).
Table 1: Victorian hospitals by cluster
Tertiary Metropolitan
Austin Hospital
Geelong Hospital
Monash Medical Centre – Clayton
The Royal Children’s Hospital
The Royal Melbourne Hospital
St Vincent’s Hospital
The Alred Hospital
Box Hill Hospital
Casey Hospital
Dandenong Hospital
Frankston Hospital
Maroondah Hospital
Mercy Hospital or Women
Mercy Public Werribee
The Royal Women’s Hospital
The Royal Victorian Eye and Ear Hospital
Rosebud Hospital
Sunshine Hospital
Sandringham and District Memorial Hospital
The Northern Hospital
Western Hospital
Williamstown Hospital
Regional Sub-regional
Ballarat Hospital
Bendigo Hospital
Goulburn Valley Health Care
Latrobe Valley Health
Bairnsdale Regional Health Service
Central Gippsland Health Service
Echuca Regional Health
Hamilton Base Hospital
Northeast Health Wangaratta
Mildura Base Hospital
Swan Hill District Hospital
South West Healthcare Warrnambool
West Gippsland Healthcare Group
Wimmera Base Hospital
Wodonga Regional Health Service
Wonthaggi and District Hospital
When considered in these clusters, 84 per cent o emergency surgery is perormed by the tertiary
and metropolitan hospitals, with 16 per cent being perormed by regional and sub-regional hospitals
(Table 2). Although Geelong Hospital is usually classied as a regional hospital, data would suggest
that or the purposes o this analysis, due to the high numbers o emergency surgery cases, it should
be included in the tertiary cluster.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 27/36
22
Table 2: Emergency surgery separations by hospital cluster, 2010–11
Hospital cluster Total emergency surgery
separations
Contribution to state total
Tertiary 24,154 41.3%
Metropolitan 24,844 42.4%
Regional 5,517 9.4%
Sub-regional 4,031 6.9%
(Peter MacCallum Cancer Centre and Albury Hospital not included).
Growth in emergency surgery
The greatest volume o emergency surgery is in the specialties o general surgery, orthopaedics
and plastic surgery (Figure 3). The greatest growth in emergency surgery over the last ve years is
demonstrated in the specialties o general surgery, neurosurgery and plastic surgery.
Figure 3: Surgical specialties with highest volume o emergency surgery activity in Victoria,
2006–07 to 2010–11
A n n u a l s e p a r a t i o n s
General surgery
Orthopaedics
Plastic surgery
Cardiac surgery
ObstetricsNeuro surgery
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
2004-05 2005-06 2006-07 2007-08 2008-09 2009-10 2010-11
Year

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 28/36
23
In Victoria, there has been a steady increase in demand or emergency surgery since 2006–07
(Figures 4 and 5). Data indicates that this growth has been greatest at metropolitan hospitals. Figure
5 shows the growth over ve years at the our metropolitan hospitals that had the most number o
emergency surgery separations in 2010–11.
Figure 4: Emergency surgery activity by hospital cluster, 2006–07 to 2010–11
A n n u a l s e p a r a t i o n s
Tertiaryhospitals
Metropolitanhospitals
Regionalhospitals
Sub-regionalhospitals
2006-07 2007-08 2008-09 2009-10 2010-110
5,000
10,000
15,000
20,000
25,000
Year
Figure 5: Emergency surgery activity in selected health services, 2006–07 to 2010–11
E m e r g e n c y s u r g e r y s e p a r a t i o n
s
0
5,00
1,000
1,500
2,000
2,500
3,000
3,500
4,000
Geelong Hospital Dandenong Hospital Frankston Hospital The Northern Hospital
2006-07
2007-08
2008-09
2009-10
2010-11
Health service

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 29/36
24
Trends in acuity
Data shows that higher Weighted Inlier Equivalent Separation (WIES) weight is distributed to tertiary
health services, refecting the higher complexity o their emergency surgery patients (Figure 6).
Figure 6: Emergency surgery average WIES by hospital cluster, 2006–07 to 2010–11
A v e r a g e W I E S
Tertiaryhospitals
Metropolitanhospitals
Regionalhospitals
Sub-regionalhospitals
2006-07 2007-08 2008-09 2009-10 2010-11
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
Year

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 30/36
25
Trends in length o stay
Figure 7 demonstrates that or all hospital clusters there has been a reduction in length o stay
or emergency surgery since 2006–07.
Figure 7: Emergency surgery length o stay by hospital cluster, 2006–07 to 2010–11
A v e r a g e l e n g t h o f s t a y ( d a y s )
Tertiaryhospitals
MetropolitanhospitalsRegionalhospitalsSub-regionalhospitals
2006-07 2007-08 2008-09 2009-10 2010-11
4
5
6
7
8
9
10
11
Year
Table 3: Emergency surgery separations, average length o stay and acuity or surgical
specialties with the largest volume o separations, 2010–11
Specialty
Emergency surgery
separations
Average length o
stay (days)
Acuity
(average WIES)
General surgery 16,740 7.35 2.53
Orthopaedics 11,436 7.86 2.85
Plastic surgery 10,313 4.31 1.55
Cardiology 3,485 5.39 3.39
Obstetrics 2,750 1.48 0.62
Neurosurgery 2,448 10.57 5.03
Table 3 demonstrates that general surgery accounted or the greatest volume o emergency surgery
separations in 2010–11 (16,740 separations). O the six surgical specialties with the greatest
volumes o emergency surgery separations, neurosurgery cases had the longest average length o
stay and acuity.
7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 31/36
26
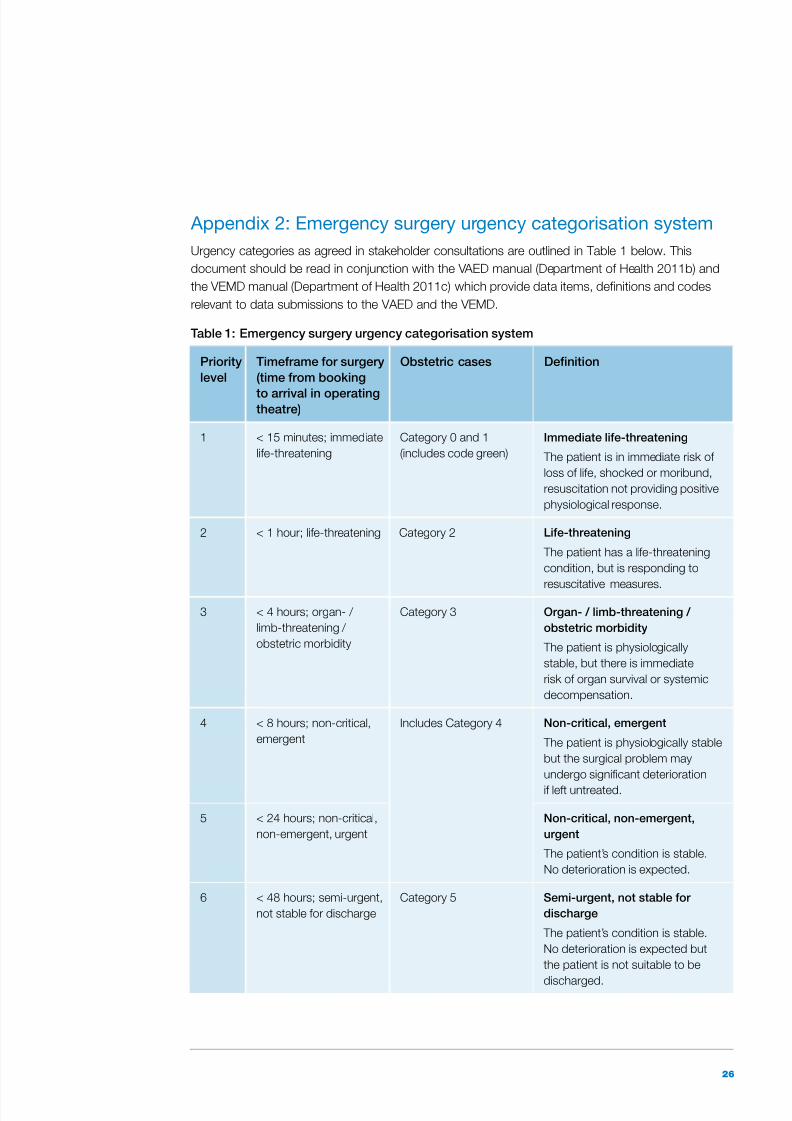
Appendix 2: Emergency surgery urgency categorisation system
Urgency categories as agreed in stakeholder consultations are outlined in Table 1 below. This
documentshouldbereadinconjunctionwiththeVAEDmanual(DepartmentofHealth2011b)and
the VEMD manual (Department o Health 2011c) which provide data items, denitions and codes
relevant to data submissions to the VAED and the VEMD.
Table 1: Emergency surgery urgency categorisation system
Priority
level
Timerame or surgery
(time rom booking
to arrival in operatingtheatre)
Obstetric cases Denition
1 < 15 minutes; immediate
lie-threatening
Category 0 and 1
(includes code green)
Immediate lie-threatening
The patient is in immediate risk o
loss o lie, shocked or moribund,
resuscitation not providing positive
physiological response.
2 < 1 hour; lie-threatening Category 2 Lie-threatening
The patient has a lie-threatening
condition, but is responding to
resuscitative measures.
3 < 4 hours; organ- /
limb-threatening /
obstetric morbidity
Category 3 Organ- / limb-threatening /
obstetric morbidity
The patient is physiologically
stable, but there is immediate
risk o organ survival or systemic
decompensation.
4 < 8 hours; non-critical,
emergent
Includes Category 4 Non-critical, emergent
The patient is physiologically stable
but the surgical problem may
undergo signicant deterioration
i let untreated.
5 < 24 hours; non-critical,
non-emergent, urgent
Non-critical, non-emergent,
urgent
The patient’s condition is stable.
No deterioration is expected.
6 < 48 hours; semi-urgent,
not stable or discharge
Category 5 Semi-urgent, not stable or
discharge
The patient’s condition is stable.
No deterioration is expected but
the patient is not suitable to be
discharged.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 32/36
27
Australian Commission on Saety and Quality in Health Care 2010, The OSSIE guide to clinical
handover improvement , Australian Commission on Saety and Quality in Health Care, Sydney.
Australian Institute o Health and Welare 2008, National health data dictionary , Version 14,
Canberra.
Australian Medical Association 2005, National code o practice: hours o work, shitwork and
rostering or hospital doctors, Australia.
Cox MR, Cook L, Dobson J, Lambrakis P, Ganesh S and Cregan P 2010, ‘Acute surgical unit:
a new model o care’, ANZ Journal o Surgery , vol. 80, no. 6, pp. 419–424.
Department o Health 2009a, Patient-centred surgery: strategic directions or surgical services in Victoria’s public hospitals 2010–15, State Government o Victoria, Melbourne.
Department o Health 2009b, Victorian clinical governance policy ramework: a guidebook ,
State Government o Victoria, Melbourne.
Department o Health 2010a, Good practice in management o emergency surgery: a l iterature
review . State Government o Victoria, Melbourne.
Department o Health 2010b, Promoting eective communication among healthcare proessionals
to improve patient saety and quality o care, State Government o Victoria, Melbourne.
Department o Health 2010c, Victorian State Trauma Registry 2008–09 summary report , State
Government o Victoria, Melbourne.
Department o Health 2011a, A guide to surgical services redesign measures or improvement ,
State Government o Victoria, Melbourne.
Department o Health 2011b, Victorian Admitted Episodes Data Set manual: 21st edition 2011–12,
State Government o Victoria, Melbourne.
Department o Health 2011c, Victorian Emergency Minimum Dataset user manual: 16th edition
2011–12, State Government o Victoria, Melbourne.
Department o Health 2011d, Victorian Health Priorities Framework 2012–2022: Metropolitan Health
Plan, State Government o Victoria, Melbourne.
Department o Human Services 2007, Rural procedures services: planning ramework , StateGovernment o Victoria, Melbourne.
Department o Human Services 2009, Credentialing and defning the scope o clinical practice or
medical practitioners in Victorian health services: a policy handbook , State Government o Victoria,
Melbourne.
Earley AS, Pryor JP, Kim PK, Hedrick JH, Kurichi JE, Minogue AC, Sonnad SS, Reilly PM and
Schwab CW 2006, ‘An acute care surgery model improves outcomes in patients with appendicitis’,
Annals o Surgery , vol. 244, no. 4, pp. 498–504.
FaizO,BanerjeeS,TekkisP,PapagrigoriadisS,RennieJandLeatherA2007,‘Westillneedto
operate at night!’ World Journal o Emergency Surgery , vol. 2, no. 29.
Fitzgerald J, Lum M, and Dadich A 2006, ‘Scheduling unplanned surgery: a tool or improving
dialogue about queue position on emergency theatre lists’, Australian Health Review , vol. 30, no. 2,
pp. 219–231.
Reerences

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 33/36
28
National Health and Hospitals Reorm Commission 2009, A healthier uture or all Australians: fnal
report June 2009, Commonwealth o Australia, Canberra.
NSW Health Surgical Services Taskorce 2009, Emergency surgery guidelines, NSW Department o
Health, Sydney.
NSW Health Surgical Services Taskorce 2011, Surgery utures: a plan or Greater Sydney , NSW
Department o Health, Sydney.
Parasyn AD, Truskett PG, Bennett M, Lum S, Berry J, Haghighi K and Crowe P 2009, ‘Acute-care
surgical service: a change in culture’, ANZ Journal o Surgery , vol. 79, pp. 12–18.
Royal Australasian College o Surgeons Divisional Group o Rural Surgery 2005, Standards or rural surgeons’ working hours and recommendations or stafng and practice in rural departments o
surgery , Australia.
Royal Australasian College o Surgeons 2007, Standards or sae working hours and conditions or
ellows, surgical trainees and international medical graduates, Australia.
Royal Australasian College o Surgeons 2009, Victorian Audit o Surgical Mortality annual report
2009, Australia.
Tallis G and Balla J 1995, ‘Critical path analysis or the management o ractured neck o emur’,
Australian Journal o Public Health, vol. 19, no. 2, pp. 155–159.

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 34/36
29

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 35/36
4 Clinical review of area mental health services 1997-2004

7/28/2019 Emergency Surgery Framework
http://slidepdf.com/reader/full/emergency-surgery-framework 36/36


















