Emergency Preparedness: Are Healthcare Systems Prepared ... · Yale New Haven Center for Emergency...
33
www.yalenewhavenhealth.org/emergency Presentation to: National Emergency Management Summit March 6, 2007 Yale New Haven Center for Emergency Preparedness and Disaster Response www.yalenewhavenhealth.org/emergency Emergency Preparedness: Are Healthcare Systems Prepared for the New Normal? James L. Paturas, CEM, EMTP, CHS-IV Deputy Director for Clinical Services
Transcript of Emergency Preparedness: Are Healthcare Systems Prepared ... · Yale New Haven Center for Emergency...

www.yalenewhavenhealth.org/emergency
Presentation to:
National Emergency Management Summit
March 6, 2007Yale New Haven Center for Emergency Preparedness and Disaster
Response
www.yalenewhavenhealth.org/emergency
Emergency Preparedness: Are Healthcare Systems Prepared for the New Normal?
James L. Paturas, CEM, EMTP, CHS-IVDeputy Director for Clinical Services

Identify the critical organizational elements that include management, clinical and technical expertise required to establish a regional resource center.
Outline the process involved in moving forward with the development of a regionally driven and fully integrated public health and healthcare delivery statewide plan for emergency preparedness
Identify the critical planning/research methods required to develop plans, polices and annexes that are replicable and transferable
OBJECTIVES

1950-2000
From 1951 through 2000 the number of disaster events increased by 1,100% from approximately 419 events from the years 1951-1960 to 5,512 from the years 1991-2000 according to the World Association for Disaster and Emergency Medicine (WADEM)
The number persons affected by disaster events increased by 18,000% from 11.5 million in the years from 1951-1960 to 2.1 billion for the years between 1991-2000 according to the World Association for Disaster and Emergency Medicine (WADEM)
And then came September 11, 2001
From 1951 through 2000 the number of disaster events increased by 1,100% from approximately 419 events from the years 1951-1960 to 5,512 from the years 1991-2000 according to the World Association for Disaster and Emergency Medicine (WADEM)
The number persons affected by disaster events increased by 18,000% from 11.5 million in the years from 1951-1960 to 2.1 billion for the years between 1991-2000 according to the World Association for Disaster and Emergency Medicine (WADEM)
And then came September 11, 2001

SEPTEMBER 2005
The nation was inadequately prepared to continue normal operations in the face of the enormity of the disaster caused byHurricanes Katrina and Rita, which destroyed or disabled hospital buildings, transportation and other vital infrastructure in addition to generating large numbers of patients to treat
Public safety individuals and organizations were not prepared tointegrate their normal functions with those of hospital systems and healthcare delivery organizations to manage the surge of patients.
Communities delegated preparedness responsibility to individual institutions but had not planned for the possibility of an event that would affect multiple institutions and support agencies simultaneously.
Counties and states did not have experience working together, had not planned together adequately and were not organized to respond to a major disruption of hospital services and medical surge event.
Resources were unavailable when needed or unable to be used as effectively as if they had been mobilized in a unified, integrated response.
The nation was inadequately prepared to continue normal operations in the face of the enormity of the disaster caused byHurricanes Katrina and Rita, which destroyed or disabled hospital buildings, transportation and other vital infrastructure in addition to generating large numbers of patients to treat
Public safety individuals and organizations were not prepared tointegrate their normal functions with those of hospital systems and healthcare delivery organizations to manage the surge of patients.
Communities delegated preparedness responsibility to individual institutions but had not planned for the possibility of an event that would affect multiple institutions and support agencies simultaneously.
Counties and states did not have experience working together, had not planned together adequately and were not organized to respond to a major disruption of hospital services and medical surge event.
Resources were unavailable when needed or unable to be used as effectively as if they had been mobilized in a unified, integrated response.

Are Healthcare Systems Prepared for the New Normal

Largest, most integrated healthcare system in Connecticut12,000 employees and 3,500 physicians78,000 patient discharges and 1,300,000 outpatient visits3 acute care hospitals, a children’s hospital and a psychiatric hospital− A Level 1 Burn Center and one Level 1 Trauma Centers
Primary teaching hospital of the Yale University School of Medicine (YSM)
-
Bridgeport Greenwich Yale-New Haven
Westerly YSM

Our Mission“To develop and deliver services around the nation and internationally that advance healthcare planning, preparedness and response for emergency events and disasters through collaborative partnerships and coordinated programs.”
Yale New Haven Center for Emergency Preparednessand Disaster Response
-

Yale New Haven Center for Emergency Preparedness and Disaster Response
Designated by the Commissioner of the Department of Public Health (DPH) in 2002 as a Center of Excellence (CoE) for Bioterrorism Preparedness and Response in Connecticut
At the request of the Connecticut Department of Public Health, Yale New Haven Health System (YNHHS) was charged with developing statewide emergency preparedness programs and education and training services for healthcare delivery organizations

Yale New Haven Center for Emergency Preparedness and Disaster Response
Provides leadership to:− 32 Acute Care Hospitals
− 90 Emergency Medical Services Agencies
− 41 Community Health Centers
− 66 Home Health Agencies
− 22 Urgent Care Centers
− 106 Skilled Nursing Facilities
− 7,000 Community Medical Practitioners
In addition, partnerships have been developed between the YNHHS CoE and the following organizations:− Mental Health Community
− Local Public Health/Public Safety
− Other Agencies (transportation, pharmacies, medical supply distributors, etc.)
Designated by the Centers for Disease Control and Prevention (CDC) as the Connecticut Center for Public Health Preparedness (CPHP) at YNHHS
The only hospital system in the country with a CDC CPHP designation

The Yale New Haven Health System Center of Excellence for Bioterrorism Preparedness and Response and the Yale University School of Medicine have developed a collaborative relationship in the following academic, clinical and support areas:− Emergency/Disaster Medicine− Public Health− Epidemiology− Infectious Disease− Toxicology− Burn/Trauma Surgery− Radiation Health/Nuclear Medicine− Pediatrics− Mental Health− Occupational/Environmental Health− Web Design and Development− Learning Management Systems− Emergency Response Resource Database
This academic/clinical relationship has fostered an environment that includes academic research, applied medicine and clinical education
The Yale New Haven Health System Center of Excellence for Bioterrorism Preparedness and Response and the Yale University School of Medicine have developed a collaborative relationship in the following academic, clinical and support areas:−− Emergency/Disaster Medicine− Public Health− Epidemiology− Infectious Disease− Toxicology− Burn/Trauma Surgery− Radiation Health/Nuclear Medicine− Pediatrics− Mental Health−− Occupational/Environmental Health− Web Design and Development− Learning Management Systems− Emergency Response Resource Database
This academic/clinical relationship has fostered an environment that includes academic research, applied medicine and clinical education
Academic/Clinical Delivery Partnership

Public Safety Organizations
Governmental Organizations
Public Health Organizations
Healthcare Delivery Organizations
TransportationOrganizations
Private Sector Organizations
Utility CompanyOrganizations
Statewide Response Organizations
Horizontal and Vertical Integration for Emergency Response
Local Response Organizations
Federal Response Organizations
Federal Organizations(HHS, DHS, FEMA, DoD)
Statewide Public Safety Organizations
Statewide Governmental Organizations
Statewide Healthcare
Organizations

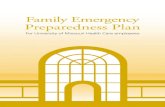
Integration of Response Systems
First PreparersGeneral PopulationPrivate IndustryCity PlannersDisaster PlannersNational PlannersPublic Health
First RespondersPoliceFireEMSCity and County Health OfficialsPublic Health
First ReceiversHospitalsClinicsHealth FacilitiesMedical Providers
Transportation, security, infrastructure,
crisis communications
FP
Healthcare delivery focused
Manmade/ natural events
Basic Disaster Life Support (BDLS)Advanced Disaster Life Support (ADLS)Pre-hospital Trauma Life Support (PHTLS)
FRd
FR

PersonnelBedsEquipmentPharmaceuticals/Medical SuppliesFacilities/SecurityCommunication Systems and Processes
Building a Healthcare Surge Capacity

Surge Capacity Determinants

Critical Capacity Evaluation Summary

Alternate Healthcare Delivery During a Pandemic Scenario
ICU
Acute Care Hospital
Critical Non-Critical
Triage
Alternate Care Sites–Traditional
Occupational Medical Services
Occupational Medical Services
Nursing HomesNursing Homes
Rehab HospitalsRehab Hospitals
Schools of Nursing/
Other Health Professions
Schools of Nursing/
Other Health Professions
Community Health Centers
Community Health Centers
Community Medical Practices
Community Medical Practices
Home Health Agencies
Home Health Agencies
School Based Health AgenciesSchool Based
Health Agencies
Mobile Medical Clinics
Mobile Medical Clinics
University Health Services
University Health Services
Urgent CareUrgent Care
Civic CentersCivic Centers HouseholdsHouseholds
HotelsHotels Senior CentersSenior Centers
Non-Traditional

Regional Healthcare Contingency Delivery Centers (RHCDC)
A National Model

RHCDC MISSION
To supplement the existing national health care infrastructure by dedicating surge resources for coordination of health care delivery, education, research and integrated community services.
Responsible for the coordinated development, implementation, evaluation of training, and capacities (such as administrative support, infrastructure including healthcare epidemiology, laboratories, information systems, leadership and expert personnel, research capability, equipment and supplies) for the healthcare delivery and response community within a defined geographic area
To supplement the existing national health care infrastructure by dedicating surge resources for coordination of health care delivery, education, research and integrated community services.
Responsible for the coordinated development, implementation, evaluation of training, and capacities (such as administrative support, infrastructure including healthcare epidemiology, laboratories, information systems, leadership and expert personnel, research capability, equipment and supplies) for the healthcare delivery and response community within a defined geographic area

First Responders
- Primary Care Providers
- Emergency Dept.Staff
- Public Health Professionals
- Local Laboratories
Public Health (PH) Depts.
Local EOCs
Military Installation PH Officers
State Health Depts.
Other State assets
State EOCs
National Guard
Emergency Coordinators in Regions
Federal Coordinating Officers
Disease investigation teams
Vaccination Teams
National Lab services
Data analysis support
Strategic National Stockpile
NDMS teams
- DMAT, NMRT, DMORT, DVAT
Other NDMS support
- Hospitalization (VA and DOD)
- DOD Advisory teams
- DOD augmentation teams
- DOD lab and technical support
- DOD general logistics (food, water, electricity, shelter)
- DOD transportation
DOD support to law enforcement
DOD general logistics (food, water, electricity, shelter)
- DOD transportation
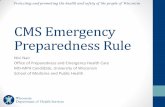
State Response
MMRS
Local Response, Municipal and County
Min
im
al
Low
Med
ium
Hig
h
Sev
ere
IInfluenza, foodborne
illnesses, endemic plague
Anthrax, plague with 1-2 cases Pandemic influenzaSmallpox Bioengineered agent
Severity
Time
Federal Response
Integrated Medical Capabilities: Red Wedge of Response

RHCDC COMPONENTS
RHCDC

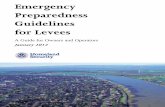
Regional Healthcare Contingency Delivery Center Organizational Model
Regional Healthcare Regional Healthcare Contingency Delivery Contingency Delivery
CenterCenter
FacilitiesFacilities Supplies / Supplies / PharmaceuticalsPharmaceuticals
PersonnelPersonnel EquipmentEquipment
Federal Medical Contingency Station
Military Assets (i.e. EMeds)
Strategic National Strategic National StockpileStockpile
State Assets (i.e. MaSH)
Local Assets (Hospitals)
Chempack Chempack
Regional Shared Regional Shared Cache StockpileCache Stockpile
Facility Cache Facility Cache StockpileStockpile
ESAR-VIP
State Emergency Credentialing
Programs
Military / Federal Personnel
Medical Reserve Corps (MRC)
Inpatient / Outpatient Beds
Ventilators, isolation units,
Decon Units
Regional Shared Regional Shared Equipment CacheEquipment Cache
Facility Equipment Facility Equipment Cache Cache

RHCDC PROGRAM DEFINITIONS
Facilities – Develop a model for facility surge capacity for the provision of medical care in response to a disaster
Consider alternative treatment sites and transport, access and security activities
Utilize non-traditional treatment/patient care areas
Predetermine triage locations (on-site or off-site) including primary and secondary triage locations
Define, identify and equip patient care capacity at off-site facilities
Establish policies on integration of Federal, State and non-government facility resources
Establish emergency (temporary) identification protocols
Enhance protection of critical infrastructure
Facilities – Develop a model for facility surge capacity for the provision of medical care in response to a disaster
Consider alternative treatment sites and transport, access and security activities
Utilize non-traditional treatment/patient care areas
Predetermine triage locations (on-site or off-site) including primary and secondary triage locations
Define, identify and equip patient care capacity at off-site facilities
Establish policies on integration of Federal, State and non-government facility resources
Establish emergency (temporary) identification protocols
Enhance protection of critical infrastructure

RHCDC PROGRAM DEFINITIONS
Personnel – Establish regional and national medical healthcare personnel response capability integrated with state and federal response programs
Integrate Federal and State government resources (e.g. DMATs, Public Health Service, VA System, National Guard)
Mutual aid agreements with surrounding area hospitals.
Use emergency credentialing systems that include a process for verification of credentials
Investigate each states licensing/certification verification systems for all relevant staff types.
Investigate the existence of agreements between neighboring states for waiving license verification in a disaster situation.
Personnel – Establish regional and national medical healthcare personnel response capability integrated with state and federal response programs
Integrate Federal and State government resources (e.g. DMATs, Public Health Service, VA System, National Guard)
Mutual aid agreements with surrounding area hospitals.
Use emergency credentialing systems that include a process for verification of credentials
Investigate each states licensing/certification verification systems for all relevant staff types.
Investigate the existence of agreements between neighboring states for waiving license verification in a disaster situation.

Education, Research and Evaluation – Provide coordinated and consistent education and training programs that support state and federal mandates Train and exercise clinical, operations and facility personnel to fulfill their disaster medicine response roles
Education and training courses centered on mass casualty disaster response and will include continued refinement of:
– Clinical and operating policies and procedures– Hospital Incident Command System (HICS)– Transporting, deploying and restaging the facility– Communication– Maintenance and use of equipment
Education and training programs will combine clinical mentoring, programs and procedures and printed resources along with hands-on equipment training and facility preparations.
Education, Research and Evaluation – Provide coordinated and consistent education and training programs that support state and federal mandates Train and exercise clinical, operations and facility personnel to fulfill their disaster medicine response roles
Education and training courses centered on mass casualty disaster response and will include continued refinement of:
– Clinical and operating policies and procedures– Hospital Incident Command System (HICS)– Transporting, deploying and restaging the facility– Communication– Maintenance and use of equipment
Education and training programs will combine clinical mentoring, programs and procedures and printed resources along with hands-on equipment training and facility preparations.
RHCDC PROGRAM DEFINITIONS

Supplies/Pharmaceuticals – Provide a consistent approach to availability of regional supply stockpiling for up to 72 hours prior to arrival of the SNS
Identify and inventory existing caches of pharmaceuticals, equipment and medical supplies that are available locally, regionally and at the state level.
Develop comprehensive plans that establish integration and coordination with any other state, regional or federal assets that may become available.
Collaborate with local and regional partners to establish caches of equipment and the development of coordinated supply and pharmaceutical stockpile agreements
Establish appropriate communication and requisition processes that ensure ongoing supplies and pharmaceuticals access and support
Supplies/Pharmaceuticals – Provide a consistent approach to availability of regional supply stockpiling for up to 72 hours prior to arrival of the SNS
Identify and inventory existing caches of pharmaceuticals, equipment and medical supplies that are available locally, regionally and at the state level.
Develop comprehensive plans that establish integration and coordination with any other state, regional or federal assets that may become available.
Collaborate with local and regional partners to establish caches of equipment and the development of coordinated supply and pharmaceutical stockpile agreements
Establish appropriate communication and requisition processes that ensure ongoing supplies and pharmaceuticals access and support
RHCDC PROGRAM DEFINITIONS

Equipment – develop a standard approach and process for available equipment to meet medical surge capacity of patients in a given region and a model for equipment stockpiling across the nation
Employ an all hazards / multi-use approach to determine equipment stockpile plans based on most likely threats/events
Identify medical equipment from state, local and federal agencies that include environmental, engineering and biomedical equipment
Determine financing of equipment acquisition, outsourcing needs and identify partnering companies.
Conduct evaluation of total par level recommendations and general availability at each RHCDC
Integrate RHCDC facility specific plans with local, regional and statewide initiatives
Equipment – develop a standard approach and process for available equipment to meet medical surge capacity of patients in a given region and a model for equipment stockpiling across the nation
Employ an all hazards / multi-use approach to determine equipment stockpile plans based on most likely threats/events
Identify medical equipment from state, local and federal agencies that include environmental, engineering and biomedical equipment
Determine financing of equipment acquisition, outsourcing needs and identify partnering companies.
Conduct evaluation of total par level recommendations and general availability at each RHCDC
Integrate RHCDC facility specific plans with local, regional and statewide initiatives
RHCDC PROGRAM DEFINITIONS

Communications – Develop integrated and consistent approaches to communication processes and equipment for the delivery of medical care locally, regionally and nationally and through horizontal and vertical integration
Develop consensus across the various partners that coordinates state intergovernmental communications response activities
Public health emergency communication plans linked with local government, private healthcare agencies, professional associations and private industry
Public health and healthcare partners develop specific tactical emergency communications plans to support a public health response for detection, surveillance, diagnostic and clinical management, emergency notification, voice communication and supporting technologies
Establish and prioritize cost effective emergency communications and information technology standards for the purchase of hardware and software that supports interoperability and redundancy
Communications – Develop integrated and consistent approaches to communication processes and equipment for the delivery of medical care locally, regionally and nationally and through horizontal and vertical integration
Develop consensus across the various partners that coordinates state intergovernmental communications response activities
Public health emergency communication plans linked with local government, private healthcare agencies, professional associations and private industry
Public health and healthcare partners develop specific tactical emergency communications plans to support a public health response for detection, surveillance, diagnostic and clinical management, emergency notification, voice communication and supporting technologies
Establish and prioritize cost effective emergency communications and information technology standards for the purchase of hardware and software that supports interoperability and redundancy
RHCDC PROGRAM DEFINITIONS

INTEGRATION

PRE-EVENT INTEGRATION
RHCDC will provide for an integrated and comprehensive program and response components within a defined geographic area and representing an effected or at-risk population and shall:
During the pre-event phase, develop, test (through exercises), and have in place plans for clinical services delivery
During the pre-event phase, prepare, test, and have in place plans to develop new, and to maintain existing, collaborations with members of the healthcare delivery and response community
RHCDC will provide for an integrated and comprehensive program and response components within a defined geographic area and representing an effected or at-risk population and shall:
During the pre-event phase, develop, test (through exercises), and have in place plans for clinical services delivery
During the pre-event phase, prepare, test, and have in place plans to develop new, and to maintain existing, collaborations with members of the healthcare delivery and response community

EVENT INTEGRATION
During the event phase, deliver clinical services to affected and at risk populations and provide medical management and treatment of adverse events arising from utilization of clinical services developed in response to an emer-gency situation
During the event phase, communicate preliminary findings regarding the delivery and efficacy of clinical services to appropriate Federal, State, and local public health authorities
During the event phase, deliver clinical services to affected and at risk populations and provide medical management and treatment of adverse events arising from utilization of clinical services developed in response to an emer-gency situation
During the event phase, communicate preliminary findings regarding the delivery and efficacy of clinical services to appropriate Federal, State, and local public health authorities

POST EVENT INTEGRATION
During the post event phase, have in place a validated process of metrics and measures for eval-uating the effectiveness of clinical services through clinical research, including external evalua-tion, quality assurance and mitigation, and an eval-uation of the clinical services delivery center’s capability to respond to the needs of populations at risk and address potential hazard vulnerabilities
During the post-even phase, share information about the effectiveness of services and the capability of the RHCDC delivery centers to respond to the event to appropriate Federal, State, military and local public health authorities
During the post event phase, have in place a validated process of metrics and measures for eval-uating the effectiveness of clinical services through clinical research, including external evalua-tion, quality assurance and mitigation, and an eval-uation of the clinical services delivery center’s capability to respond to the needs of populations at risk and address potential hazard vulnerabilities
During the post-even phase, share information about the effectiveness of services and the capability of the RHCDC delivery centers to respond to the event to appropriate Federal, State, military and local public health authorities

SUMMARY

James L. PaturasDeputy Director, YNH-CEPDR
One Church Street, New Haven, CT 06510www.yalenewhavenhealth.org/emergency
James L. PaturasDeputy Director, YNH-CEPDR
One Church Street, New Haven, CT 06510www.yalenewhavenhealth.org/emergency
Contact Information