Emergency Preparedness and Bioterrorism Region Training Presented by the Minnesota HomeCare...
103
Emergency Preparedness and Bioterrorism Region Training • Presented by the Minnesota HomeCare Association Staff and the MHCA Emergency Preparedness and Bioterrorism Task Force - 2002
-
Upload
bruce-hubbard -
Category
Documents
-
view
217 -
download
0
Transcript of Emergency Preparedness and Bioterrorism Region Training Presented by the Minnesota HomeCare...

Emergency Preparedness and Bioterrorism Region Training
• Presented by the Minnesota HomeCare Association Staff and the MHCA Emergency Preparedness and Bioterrorism Task Force - 2002

Center for Disease Control Info Page on Bioterrorism
• WHAT IS THE PUBLIC HEALTH PROBLEM?
• Bioterrorism is a significant public health threat

Center for Disease Control Info Page on Bioterrorism
• WHAT IS THE PUBLIC HEALTH PROBLEM
• Bioterrorism is a significant public health threat
• Response to a bioterrorism event will require rapid deployment of scarce public health resources

Center for Disease Control Info Page on Bioterrorism
• WHAT IS THE PUBLIC HEALTH PROBLEM• Bioterrorism is a significant public
health threat• Response to a bioterrorism event will
require rapid deployment of scarce public health resources
• The nation’s public health infrastructure currently is not adequate to detect and respond to a bioterrorist event

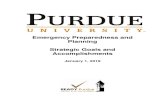
INTERIM RECOMMENDED NOTIFICATION PROCEDURES FOR LOCAL AND STATEPUBLIC HEALTH DEPARTMENT LEADERS IN THE EVENT OF A BIOTERRORIST
INCIDENT
Local Health Officer isinformed of abioterrorist incident orthreat
ORLocal Health Officersuspects that cases ofillness may be due to abioterrorist incident
FIRST:Notify FBINotify local lawenforcement
NEXT:Notify & involve StateHealth Dept. and otherresponse partners, per apre-established notificationlist
State Health Dept.notifies the CDC
FIRST: Inform and involveSate Health Dept. HealthDept. notifies CDC.Conduct investigation
Is Bioterrorismincidentconfirmed orthought to beprobable?
YES
Notify FBI. Notifyother pre-determinedresponse partners
NO
ContinueInvestigation

THE NEXT STEPS FOR CDC,STATE AND LOCAL HEALTH DEPARTMENTS ARE TO:
• Continue to enhance public infrastructure;– Surveillance– Epidemiology– Rapid lab diagnosis– Information systems

THE NEXT STEPS FOR CDC,STATE AND LOCAL HEALTH DEPARTMENTS ARE TO:
• Continue to enhance public health infrastructure
• Continue to develop response capacity;– Workforce– Communications– National Pharmaceutical deployment

THE NEXT STEPS FOR CDC, STATE AND LOCAL HEALTH DEPARTMENTS ARE TO:
• Continue to enhance public health infrastructure
• Continue to develop response capacity;
• Provide training in bioterrorism preparedness and response for the public health workforce

PREPAREDNESS PLANNING AND READINESS ASSESSMENT FOR HOME CARE ORGANIZATIONS
• First prepare for personal and staff protection



PREPAREDNESS PLANNING AND READINESS ASSESSMENT
• First Prepare for personal and staff protection
• Conduct an assessment of preparedness and response capacity– Review and evaluate current
emergency plan

PREPAREDNESS PLANNING
• First prepare for personal and staff protection
• Conduct an assessment of preparedness and response capacity
• Conduct coordinated planning with County Public Health and local health care providers

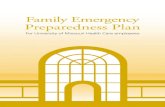
PLANNING MODEL
LocalPublicHealth
MinnesotaDepartment
OfHealth
Local:Law Enforcement, Fire,Emergency Management,
EMS, Local Chaptersof Red Cross,Salvation Army
LocalHealth CareProviders:- MD’s- Nurses- Clinics- HMOs- Home Care
-Hospitals- Nursing Homes- School- Others
Governor
Minnesota Departmentof Public Safety
National Guard
Local Elected Offi cials
EmergencyManagement
CDCField
Epidemiologistsand otherconsultants
FBI
STATE WI DEORGANI ZATI ONS


Implement planning strategies to include:
• A 24/7 activation• Redundancy of systems• Training of key individuals• System for identification of clients
needing essential services• System for identification of staff
availability

Consider:
• Staying alert – avoid complacency


Consider:
• Staying alert – avoid complacency• Utilizing community based
connections– Work with Parish Nurses– Explore working with neighborhood
groups


Consider:
• Staying alert- avoid complacency• Utilizing community based
connections– Work with Parish Nurses– Explore working with neighborhood
groups
• Getting on the HAN network


Consider:
• Staying alert – avoid complacency• Utilizing community based connections
– Work with Parish Nurses– Explore working with neighborhood groups
• Getting on the HAN network• Participating in Hospital or government
planning activities• Make a concerted effort to keep up to
date on current information• Educate staff and clients


BIOTERRORISMInfection Control
Planning and Response
Boyd Wilson, MS, CICSystem Director of Infection Control & EpidemiologyHealthEast Care System

Objectives
• Identify the most probable agents to be used in bioterrorism
• Describe how a bioterrorism act might express itself clinically
• State how these agents are transmitted & precautions necessary to prevent spread
• Discuss efforts that are underway to prepare for potential acts of bioterrorism and the implications for Home Care

Bioterrorism . . .
is the deliberate release of pathogenic microorganisms (bacteria, viruses, fungi or biological toxins) into a community to produce disease or intoxication in susceptible populations (humans, animals, plants) to meet terrorist needs.

Emergency Preparedness/Disaster Plan
• Policy• Definitions• - Natural Disasters• -Unnatural Disasters• Biological• Non-Biological

Natural Disasters and Unnatural Disasters
• Policy and Procedure• Notification- Calling Tree• Communication Failure• Reporting

Definition
• Disaster: is an occurrence that causes damage, ecological disruption, loss of human life, deterioration of health and human services on a scale sufficient to warrant an extraordinary response from outside the affected community area – World Health Organization

History
• Kaffa – plague – 1346• French and Indian - smallpox – 1746• Japan – Manchuria unit 731 – 1932• 1972 Biological Weapons Convention• Georgi Markov – 1978• Sverdlovsk – 1979 – at least 66 deaths

Recent Threats
• Iraq– 19,000 liters of botulinum toxin– 8.500 liters of concentrated anthrax
• Aum Shinrikyo Cult• Los Angeles, other scares• Former Soviet stockpiles• 15-20 nations have biological programs• Evolving states, fringe groups, individuals

Advantages of Bioweapons
• Easy to procure• Invisible• Detection difficult• Incubation period/escape period• Community preparation poor• Threat alone achieves goals

Agent Cost
• Inflict 50% casualties over 1 square kilometer
• Conventional $2000• Nuclear $800• Nerve Agent $600• Anthrax $1

Impact of a Biologic Incident
• Potential for widespread illness and death
110 pounds of anthrax spores sprayed along a 1.5 mile line source tract upwind from a city of 500,000 could kill 24,000 people
Profound pyschological stressLarge numbers of casualties

Environmental Constraints
• Sunlight – UV light kills many bacteria
• Wind – Disperses biological agents• Temperature – heat inactivates
many biological agents, most are resistant to freezing
• Desiccation – may inactivate or inhibit growth

If you hear these hoofbeats …
• Widened mediastinum on thoracic radiograph
• Influenza-like illness in summer months• Pneumonia death in otherwise healthy adult• Vesicular rash that starts on extremities• Hemorrhagic fever syndrome• Cluster of unusual, severe or unexplained
illnesses• Unexplained critical illness in otherwise
healthy young adult

……Consider these zebras
• Anthrax• Tularemia• Plague• Smallpox• Brucellosis• Viral hemorrhagic fever• Other potential bioterrorism agents

AAAHHHCHCHOOOOO!

DROPLET PRECAUTIONS(in addition to Standard Precautions)
PatientRoom
Masks
Room doors may be open or closed. No special ventilation required.
Surgical mask required when within 3 feet of patient (arms length).Not required for room entry.
See Infection Control Policies for further information.
VISITORS: Wear mask when within 3 feet of patient. Not required for room entry. Wash hands when leaving room.

Contact Precautions
• Lice• Scabies• MRSA, VRE (resistant organisms)• Uncontained body fluids• VHF

CONTACT PRECAUTIONS(in addition to Standard Precautions)
PATIENTROOM
GLOVES
GOWN
HANDWASHING
Dedicate noncritical items.(Commode, stethoscope, BP cuff, thermometer, wheel chair, slide board etc.)Disinfect when removing from room and before use on another patient.Limit supplies in room.
Wear gloves when entering the room. Change gloves between tasks on same patient. Do not touch clean items/supplies with contaminated gloves.Remove gloves when leaving room.
Wear gown when entering room for any contact with patient or environmental surfaces. Remove gown when leaving patient’s room.
Wash hands after touching body fluids, contaminated items and after removing gloves upon leaving room. Resistant organisms: use Antimicrobial soap.
See Infection Control Policies for further information.
VISITORS: Follow guidelines above if providing direct care. Wash hands when leaving room.

Appropriate Selection and Use of PPE

Safe Handling of Sharps

Safe Disposal of Sharps

Labeling

Environmental Management
• Routine cleaning with usual products• Management of blood spills using an
approved disinfectant detergent• Routine management of soiled linen• Routine management of trash and
biohazardous waste materials• Gross decontamination of heavily
contaminated areas (i.e. bleach)

Decontamination
• Most often, not necessary for biological incidents
• Generally, no special equipment needed• Remove clothing and place in plastic bag• Shower with soap & water• Assure design allows for containment and
separation of zones (hot, warm, cold)• Appropriate protection of workers in the
zones based on level/type of contamination

Anthrax
Bacillus anthracis

Cutaneous Anthrax

Inhalational anthrax

Infection Control Precautions
• Anthrax is NOT transmissible person-to-person
• Standard Precautions with ALL patients ALL the time
• Routine cleaning of environmental surfaces, equipment & linen
• Disinfect heavily contaminated surfaces with bleach

Infection Control for Home Care
• Considerations - contamination of the environment and personnel
• Care: hygiene, wound care, antibiotic therapy
• Standard Precautions– Hand Hygiene– Routine use of PPE– Disposal of waste materials
• Usual Home Care Infection Control protocols for managing supplies and work surfaces
• Questions regarding suspicious mailings etc.

Smallpox
Variola major

Day 7
Day 4

Smallpox - Infection Control
• Home Care Precautions– Airborne and Contact Precautions– Private room – Doors must be kept closed – N95 mask to enter the room– Dedicate equipment to room as possible– Routine daily cleaning of environmental surfaces
and equipment– Special handling of soiled linen may be warranted– Continue precautions from onset of rash until
scabs separate from healed skin (3 weeks)

Full Barrier Protection

Smallpox - Infection Control
• Home isolation and care should be the objective for most patients
• To limit nosocomial infections, authorities should consider the possibility of designating a specific hospital or remote ancillary location for smallpox care


Isolation/Quarantine

Mass Care Facility


Exposures
• Vaccine administered up to 4 days after exposure may offer protection
• All persons who have had direct contact with a case or were exposed to smallpox aerosol release should remain in ‘quarantine’ for 17 days following exposure
• People should have temperature assessed daily. If Temp >101 F, smallpox may be developing and isolation must be initiated immediately.


Infection Control for Home Care
• Considerations - establish need and authority to enter isolation/quarantine zones; evaluate immune status of those caregivers
• Standard Precautions• Airborne Precautions - (N95, immunity)• Contact Precautions - (gloves, gown, shoe
covers, face protection)• Use only essential supplies (consider disposable)• Care when in contact with potentially
contaminated articles/surfaces• Remove discard PPE/waste items with household

Resources

Plague
Yersinia pestis

Pneumonic Plague - Infection Control
• Hospital/Health Care Facility Setting:– Droplet Precautions - Mask within 3 feet of
the patient– Private room preferred, doors can be open– Mask patient if patient must leave the room– Continue precautions until the patient has
been on antibiotics for 72 hours. No discharge until no longer infectious
– Routine cleaning of environmental surfaces, equipment & linen

Plague - Infection Control
• People will need to be encouraged to stay at home and not congregate
• Those on prophylaxis should wear a surgical mask until they have completed 72 hours of antibiotic prophylaxis
• No vaccine available

Infection Control for Home Care
• Considerations - establish need and authority to enter isolation/quarantine zones
• Standard Precautions• Droplet Precautions - (surgical mask within
3 ft)• Usual Home Care Infection Control protocols
for managing supplies and work surfaces• Care when in contact with potentially
contaminated articles/surfaces

Viral Hemorrhagic Fevers
• Marburg*• Ebola*• Lassa Fever*• Rift Valley Fever• Yellow Fever

VHF - Infection Control
• Hospital/Health Care Facility Setting:– Contact Precautions - (glove, gown to enter room)– Private room– Consider need to use full facial/barrier protection
or implement Droplet Precautions– Dedicate equipment to room as possible– Routine daily cleaning of environmental surfaces
and equipment; consider bleach for large areas with gross contamination
– Special handling of soiled linen may be warranted– Continue precautions until given further direction
by Public Health

Hemorrhagic Fever Viruses as Biological Weapons: Medical and Public Health Management
• JAMA, May 8, 2002 - Vol. 287, No.18• Protective Measures
– Excellent hand hygiene– Double gloves– Impermeable gowns– N-95 mask or PAPR + full face protection– Negative pressure isolation room– Leg and shoe covers– Restricted access/essential personnel– Dedicated equipment

Infection Control for Home Care
• Considerations - establish need and authority to enter isolation/quarantine zones
• Standard Precautions• Contact Precautions - (gloves, gown, shoe
covers, face protection)• Bring in and use only essential supplies
(consider disposable)• Care when in contact with potentially
contaminated articles/surfaces• Remove discard PPE/waste items with
household

Specimen Handling
• Following usual protocols for collection and transport of clinical specimens– labeling– packaging– Standard Precautions– Needle safety devices
• Verify in advance labs to be used for analysis and their requirements (BSL level, testing ability)
– Hospital Lab– Reference Lab– MDH Labs (link to CDC)

Planning and Response
• Preparedness and Prevention• Communication/Incident Command• Surveillance and Detection• Diagnosis/Clinical Characterization• Response Coordination

Preparedness
• Assessment of infrastructure to respond– Surveillance and detection systems– Healthcare facility capacities– Laboratory capabilities– Pharmaceutical supplies– Public Health, EMS, Healthcare, Military, Law Enforcement, Fire– Federal grants (PPE, Decontamination, etc)
• Education and Training– Public Health, EMS, Law Enforcement, Hospital/Clinic Healthcare
workers– Update disaster plans– Tabletop exercises
• Communication Networks/Incident Command

Communication
• Internal– Orange Alert/HEICS– Education, Guidance, Support, Reporting
• External– Partnerships/Collaborative Efforts– Health Alert Network– Lab Alert Network– State Emergency Broadcast System– Education, Guidance, Support, Reporting

State/Local/National Disaster Planning Network
MN Public Safety Task Force
MHHP Emergency
Preparedness Task Force
MDH Task Force on Terror
and Health
Hospital Preparedness
Subgroup
CDC
AHA
FEMA


Surveillance/Detection
• Strengthen national, state, local (hospital and clinic) surveillance and reporting mechanisms
• Develop criteria for investigating and evaluating suspicious cases or clusters
• Provide guidelines to healthcare workers
• Build on existing Infection Control procedures

Epidemiologic Indicators
A rapid increase (hours to days) in the number of previously healthy persons with similar symptoms seeking medical treatment (clinics, Emergency Rooms, ICU admissions).
A cluster of previously healthy persons with similar symptoms who live, work or recreate in common geographical areas.
An endemic disease rapidly emerging at an uncharacteristic time or in unusual patterns (i.e age groups).
An unusual clinical presentation. An increase in reports of dead animals. Lower incident rates in those persons who are protected (i.e.
confined to home; no exposure to large crowds) vs. those in large crowds or in the outdoors.
An increase in numbers of patients who expire within 72 hours after admission to the hospital

Diagnosis
• Clinical presentation• Laboratory identification
– Hospital-based (BSL 1 or 2)– MDH (BSL 3)– CDC or Military (BSL4)
• Epidemiologic presentation

Response
• Notification/Emergency Communication• Activate Plans/Mobilize Personnel• Triage for care
– Signs/symptoms upon presentation– Emergency Department, Clinics
• Decontamination– Prehospital (home, by EMS) or in the ED
• Implement Infection Control Precautions• Mass vaccination/prophylaxis plans

From the HealthEast
Bioterrorism Readiness Plan and
Guidelines for Infection Control
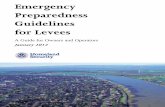
Response
XIII.A. General Patient Triage Guidelines
Patient presents following exposure tounknown agent possibly of biological origin
Exposure within past 8 hours? Consider abiologicalagent/
infectious diseaseexposure
Consider a chemical exposure.Refer to the chemical agentinformation in the ED2
Code Orange Plan.
Yes No
Sign/Symptoms? No
Contact MDH1 forinformation
Known pathogen orclinical syndrome?
Yes
No
Yes
Infection ControlPrecautions peragent identified.
See grid in this plan.Contact MDH1.Respiratory
Symptoms? Yes No
Airborne or DropletPrecautions.
Isolation Room.Surgical Mask on Patient.HCW3 wears N95 mask orPAPR (hood respirator).
Evaluate and contact MDH1.Contact Security.
Notify Infection Control.
Open wounds,bleeding, vomiting,
or diarrhea?
No
Standard Precautions.Contact MDH1.
Notify Infection Control. Yes
Contact Precautions.Evaluate and contact MDH1.
Notify Infection Control.
1 MDH MN Department of Health2 ED Emergency Department3 HCW Healthcare Worker4 PPE Personal Protective Equipment

Home Care Agency Role
• Coordinate response with local public health and/or regional hospital plans
• Support Phone Triage– Field questions (calls coming in)– Fever Watch/Quarantine Check (calls going
out)
• Home Visits• Support Ancillary Medical Facilities• Support Mass Vaccination Clinics• Protection/Education of employees/workers

Important Considerations for the Home Care Professional
• Assure you and your family are safe before attending to the needs of the patients
• Prioritize patients, attending to those with most serious conditions
• Coordinate response through your Agency Command Center (or Health System, PUBH)
• Be aware of any precautions for the areas in which you will travel and the impact– utility disruptions (water)– traffic flow (restricted access)– Public Health Alerts
• Have necessary Infection Control supports available

In Summary: Critical Issues
• Planning – Involvement in protocol/policy development
• Communication– Support systems in place and understood
• Education• Infection Prevention and Control
– Systematic, proactive Infection Control– Consistent application of standard measures
for infection prevention and control

Resources
• Web sites– MN Department of Health
• www.health.state.mn.us
– Centers for Disease Control & Prevention • www.bt.cdc.gov
– Center for Civilian Biodefense• www.hopkins-biodefense.org
– Medical Nuclear Biological Chemical Online• www.nbc-med.org
– Association for Professionals in Infection Control (APIC)• www. apic.org

QUESTIONS?
THANK YOU!

MVNA
• Emergency Preparedness/Disaster Plan

Introduction
• New realities after September 11, 2001
• Redefining disaster planning• What role home health agencies
can play?

Calling Tree

Staff Availability

Managing Excess Referrals Policy
• Acceptance• Prioritization• Acuity Level• Patient Transfer – Outside Home
Care Agencies• Patient Discharge

Staff Education and Training Policy
• Policy• Educational Tools• Overview, signs and symptoms of
disease thought to pose risk• Isolation procedures• Primary emphasis on Anthrax and
Smallpox

Prioritization Procedure Implementation
• Designation of High Priority Patients• Notification of Patients to be
Transferred, Discharged or Delayed• Notification of Patient ER Contacts • Nurse Availability to Accept New
Referrals

Ongoing Communication
• Daily Briefings• Managing Panic and Related Stress• Entering and leaving restricted
areas

Family Disaster Plan
• Terrorism – Preparing for the Unexpected
• Create an Emergency Communication Plan
• Establish a Meeting Place• Assemble a Disaster Supplies Kit• Check on the School ER Plan if you
have school age children

Mass Immunizations
• Routine Public Vaccination should not be encouraged
• More people died from vaccination than smallpox in 1947 NYC efforts to immunize 6.7 million people
• Using 2000 census, 4200 would have a serious enough reaction to warrant vaccinia immune globulin and 153 people would die

What if it were necessary to Immunize Everyone?
• Need to accept a moderate number of vaccine-related deaths and permanent neurological impairment
• Permanent neurological impairment• Vaccine is fully licensed• Intense public education needed• Adequate stores of Vaccinia immune globulin
available• Informed consent at public health sites with
screening for known and suspected medical conditions that would predispose to complications and mortality

Why Should Home Care Agencies be involved in Public Health Bioterrorism Response Programs
• Excellent relationship with the public and their communities
• Respected and trusted• Training and Expertise• Located in almost every zip code

Next Steps
• Table Top Exercise