Emergency Nutrition Network - s3.ennonline.nets3.ennonline.net/attachments/1648/FEX-11.pdf ·...
28
December 2000 Issue 11 Field Exchange Emergency Nutrition Network How many Hok does a poor man have? Food assessment in south Sudan Kosovo evaluation Food Distribution in conflict
Transcript of Emergency Nutrition Network - s3.ennonline.nets3.ennonline.net/attachments/1648/FEX-11.pdf ·...

December 2000 Issue 11
Field ExchangeEmergency Nutrition Network
How many Hok does a poor man have?Food assessment in south Sudan
Kosovo evaluationFood Distribution in conflict

Editorial by Lola Gostelow
When I began working in the field of emergencynutrition in 1991, I think I took for granted the degreeof peer support, inter-agency sharing, scientific rigour
and constant probing through research that I experienced. Ienjoyed an incredible learning curve, stimulated by colleaguesand friends around the world, taking advantage of any meetingor conference to further explore the incredible power behind astrong partnership between research and action. I thoughtemergency nutrition was just like any other humanitariansubject, but how wrong I was. Emergency nutrition is a strongerdiscipline with a very close inter-agency ethos, and I think Ihave realised this more in the last year since moving into mynew role of general emergencies adviser. Communication innutrition is, in my opinion, more far-reaching in terms ofinternational reach; more voluminous; and more substantive innature than other humanitarian areas. Why?
I think there are several reasons, and one major one is evidencedhere in Field Exchange’s pages. The process that led to theestablishment of the Emergency Nutrition Network andthereafter the launch of Field Exchange, in my mind reflectsthree important, and rarely combined, principles: consensusamongst a group of technical practitioners about the needs; acall for concrete actions to address those needs; and acommitment from many organisations to support and facilitatethe work.
And so it was that three and a half years ago I was asked towrite the editorial for the first issue of Field Exchange, andgladly did so with Helen Young. We stressed the sharedownership of Field Exchange - i.e. that it belongs to all of uswho contribute to and use it - and it is that which has given itsuch strength. Although the geography might have shifted since1997, the conviction we outlined then holds as true today:“Whether we're sitting in Paris or London, Bukavu or Jhapa, weare all striving to continue to learn and develop our skills so thatwe can improve the effectiveness of the food and nutritioninterventions we are involved in.”
In some ways, we face problems on the ground that weshouldn't have to face, whether it be pellagra in Quito orincreasing malnutrition in Northern Kenya several months afteran international appeal. Nevertheless, I remain convinced that itis only through clear evidence and professional rigour that wecan hope to infiltrate the political bubbles within which life-or-death decisions are made. What should donors’ priorities be forthe last quarter of 2000 - a food security crisis unravellingbefore our very eyes in Zimbabwe; avoiding nutritionaldeterioration in Huambo by expanding the existing food aidprogramme; or relief for the Rajasthan/Thar drought?
The compound of research and practice makes for a powerfulconcoction and it is exactly this synergy that Field Exchangehas catalysed so powerfully: providing a forum for field practiceto be exchanged and explored while also sharing research andacademic insights that could influence future programming andpriority-setting. And the effort continues as we see in thisedition of Field Exchange.
I think this landmark edition permits a final note which I amcertain you would all wish me to indulge in: My heartycongratulations go to the editorial team of Fiona O'Reilly andJeremy Shoham without whose vision, hard work and doggedpersistence the Field Exchange would have crumpled. We owethem a lot, but most importantly we owe them continuedcommitment and support.
Thank you.
Field Articles8 How many Hok does a
poor man have?11 Challenges to implementing an
integrated emergency publichealth response
15 The application of minimumstandards during crisis
19 Lessons learnt from the 1998Bangladesh floods
21 A collaborative approach to anutritional crisis in an areaaccessible only by air
26 Huambo: an impending disaster?
3 Research• Effect of Breastfeeding and
Formula Feeding on Transmissionof HIV-1
• The impact of HIV on themanagement of severemalnutrition in Malawi
• Deaths among humanitarianworkers
• Local Production of Processedcomplementary food: World FoodProgramme experience
• Principles and Practice for FoodDistribution in Conflict
• A role for capital marketsin natural disasters
• Physical activity levels inemergency affected populations
10 News• Inter-Agency Standing Committee
endorses Sphere• Distance learning courses in
nutrition• New vacancies website• Capacity building in nutrition in
WFP• SCN reports on nutritional
assessments of adolescents andadults
7 Letters
24 EvaluationsKosovo evaluationSomali region Ethiopia
13 Agency ProfileOxfam Ireland - Interview withBrian Scott
22 Revised MSF nutritionguidelines - II
27 The Backpage
Contents

3
Research
Transmission of human immunodeficiency virustype 1 (HIV-1) is known to occur throughbreastfeeding, but the magnitude of risk has
not been precisely defined. Studies have led toestimates of transmission risk during acute maternalinfection of 29% (95% CI 16%-42%) and for womenwith established infection of 14% (95% CI 7%-22%).Whether breast milk HIV-1 transmission risk exceedsthe risk of formula feeding-associated diarrhoealmortality in developing countries is unknown.
A randomised clinical trial1 was conducted in Nairobito determine the frequency of breast milktransmission of HIV-1 and to compare mortality ratesand HIV-1–free survival in breastfed and formula-fedinfants. Over five and a half years 425 HIV-seropositive women were enrolled in the study.Women were eligible for inclusion if they wereNairobi residents and had access to municipal treatedwater. Participants did not use antiretroviral therapy.At about 32 weeks of pregnancy women wererandomised to breastfeed or formula feed. Theformula group were given free formula and shownhow to prepare it. They were told to boil water andfeed with a cup to minimise bacterial contamination.
Compliance with the assigned feeding method was:
i) 96% in the breastfeeding group (defined by any useof breast milk) 83% were exclusively breastfed at 6weeks, 62% at 3 months and 9% at 6 months.
ii) 70% in the formula feeding group (defined bycomplete avoidance of breast milk).
This comparatively low compliance in the formulagroup results from the fact that breastfeeding is thenorm in Kenya and women experienced pressurefrom family and community and were in some casesconcerned about maintaining confidentiality abouttheir HIV- status.
Of the 401 infants in the study analysis2 92 wereHIV-1 infected, 61 of these were in the breastfeedinggroup and 31 in the formula group. At 24 months thecumulative probability of HIV-1 infection wassignificantly higher for infants in the breastfeedinggroup than the formula feeding group. The estimatedrate of breast milk HIV-1 transmission was 16.2%
during the first 2 years of life. Breast milktransmission accounted for 44% in the group exposedto breast milk. The data suggest that substantialtransmission occurs early (by 6 months 75% of allbreast milk transmission had occurred). Anotherimportant finding was that the 2-year mortality ratesin the 2 groups were similar. However the HIV-1 freesurvival at 2 years was significantly lower in thebreastfeeding group than in the formula feedinggroup (58% vs 70% respectively; P = 0.02)
This important study throws some light on riskdifference between HIV-1 transmission and formulaeassociated diarrhoeal mortality. Though the studyshowed that in this setting the use of formulaprevented 44% of infant HIV-1 infections the authorscaution about generalisability of results. While HIV-1transmission via breast milk may be comparableacross populations given similar exposure, the risksassociated with formula are community specific. Inthis trial mortality in both groups was similar eventhough participants had access to clean water andextensive instruction on safe formula use. Indeveloping country situations (especially emergenciesinvolving refugee or displaced populations) whereclean water and formula feeding knowledge islimited, the balance of risks and benefits could beshifted. Furthermore, formula is unaffordable tomany (about $300 for 6 months in Kenya). Also, anintervention aimed at reducing HIV transmissionthrough promoting use of infant formula amongstHIV sero-positive women requires antenatal HIV-1testing and a healthcare infrastructure to provideeducation on formula feeding. The authors concludethat given the high sero-positive prevalence inpregnant women in sub-Saharan Africa the priority isto find ways to make a spectrum of preventativeinterventions widely accessible.
1 Nduati R, et al., Effect of Breastfeeding and Formula Feedingon Transmission of HIV-1: A Randomised Clinical Trial. JAMA,March, 2000-Vol 283, No. 9 p 1167.2 At time of delivery only 408 remained in the study. Afterexclusion of stillbirths and second born twins the number inthe study declined to 401.
Effect ofBreastfeeding andFormula Feedingon Transmission ofHIV-1Summary of published clinical trial
ETHIOPIA 2000. PIETERNELLA PIETERSE (CONCERN)

4
Research
Deaths amonghumanitarian workersSummary of published paper
Agroup of researchers recently collectedinformation from the records of aidagencies and other organisations on the
death of humanitarian aid workers between1985-981. Thirty two organisations provideddata on 392 fatalities. Deaths were categorisedby demography, occupational factors andcircumstances of death. The team had hoped tocalculate risk rates and ratios for nationals andexpatriate workers but information aboutstaffing levels that was needed to constructdenominators, was only available from a feworganisations.
Intentional violence was recorded as the causeof 68% of deaths, and unintentional violence in7% of cases. Motor vehicles accounted for 17%of cases and other causes for 8%. Death fromintentional violence was most common between1992-5. Fifty eight percent of deaths wereamong local staff and 42% amongst expatriates.Mean age at death was 38.2 for locals and 39.9for expatriates. Men accounted for 90% ofdeaths.
Information on types of occupation was onlyavailable for 227 workers who died:
Drivers 13%Guards 12%Office staff 21%Field staff 22%Medical staff 9%Peace keepers 19%Consultative staff 4%
Intentional violence was the cause of 76% ofdeaths among guards, 57% among medical staffand 56% among field staff. Occupations withthe highest proportion of deaths caused bymotor vehicle accidents were drivers,peacekeepers and office staff.
Deaths peaked in 1994 at the time of events inRwanda. Since 1994 reported deaths among UNstaff have decreased whereas deaths amongstNGO workers has continued to increase. TheGreat Lakes and Horn of Africa accounted fornearly half of all deaths.
While the number of deaths has increased, sohave the number of relief agencies and thenumber of humanitarian workers. Withoutdenominators for field staff the researcherscould not calculate risk or rates making itdifficult to ascribe the increased number ofdeaths to increased risks.
The large number of deaths due to intentionalviolence contrasts with death among PeaceCorps and development workers and emphasisesthe violent circumstances in which humanitarianworkers now operate. Descriptions of deathincluded victims being robbed and killed whileat an office, residence or roadblock or killedduring a carjacking. Unintentional deaths werein some cases related to carelessness likerunning into a spinning airplane propeller.Chronic and acute disease figured prominently
among death from other causes. Cerebralmalaria, a preventable cause of death, was notedfrequently. One third of deaths among NGOworkers were due to ‘other causes’ comparedwith 5% in workers from the UN. Thisrepresented a wide range of both acute andchronic medical conditions. One reason couldbe that health screening is less stringent forNGOs hiring temporary staff than it is for UNorganisations. Health screening for local staff islikely to be cursory in emergency situations.
The mean age at death of nearly 40 contradictsperceptions that deaths are mainly among youngpeople who are ill prepared. The ratio of deathsamong nationals to those among expatriates was4 to 3. Most relief organisations report usualstaff ratios in field operations of 7 to 1 or 8 to 1.Nearly a third of all deaths occurred in the firstthree months of duty with one of every sixdeaths occurring in the first month. This wasunrelated to extent of previous field experience.Even allowing for short term contracts, commonduring emergencies, new arrivals may not beprepared for the dangers present, includingdriving risks.
The authors of the study suggest that actions tolessen deaths can be taken. These includeaccurate understanding of risks, better briefingsand guidelines, providing helmets andprotective jackets where appropriate, improvingdriving skills, managing stress better, andhandling cash and protecting assets in otherways. Another action would be to limit aid inhigh risk situations, a decision manyhumanitarians find difficult to make.
The authors concluded that in order to fullyunderstand the risks of death and the potentialfor prevention a comprehensive prospectiveapproach to data collection and monitoring isneeded and that much could be learned fromsuch a database.
There has been remarkably little published onthe implications of HIV infection foremergency nutrition interventions.
HIV infection is common among children admittedfor nutritional rehabilitation in non-emergencysettings. Surveys of children admitted to malnutritionunits have found an HIV seroprevalence rangingfrom 14% in Rwanda in 1989 to 49% in Zimbabwein 1993/4 reflecting the increasing prevalence andburden of childhood HIV infection.
The findings of a recent study1 in Malawi suggestthat there may be important issues to be addressedregarding the treatment and management of HIVpositive severely malnourished children. Many ofthese issues may have even greater relevance toemergency settings.
The study was undertaken in a central nutritionalrehabilitation unit (NRU) in southern Malawi toassess the impact of HIV infection on clinicalpresentation and case fatality rates. HIVseroprevalence in 250 severely malnourished childrenover one year of age was 34.4% and overall mortalitywas 28%. A significantly higher proportion ofchildren with marasmus (62.2%)were HIV positivethan children with kwashiorkor(21.7%).
Breastfed children presenting with severemalnutrition were more likely to be HIV-seropositive. Clinical features were generally nothelpful in distinguishing HIV sero-positive from HIVsero-negative children. The case fatality rate wassignificantly higher for HIV seropositive children.Immunosuppression arising from HIV infectionincreases the risk of sepsis, already a common causeof death in malnourished children. Less direct effectswere through an impact on the management ofchildren, e.g. increased demands on limited nursingstaff and food supplies, the added risk of certaintypes of infection in overcrowded units, and thesense of hopelessness that undermines staff moraleand performance when faced with large numbers ofchildren with poor prognosis.
Many staff felt that HIV infected malnourishedchildren should be managed at home. Furthermore,in the general wards and outpatient clinics manymarasmic children were seen who were not admittedto the NRU and once admitted were only kept in forshort periods. Also, absence of HIV testing meantthat an unknown number of marasmic children(failing to thrive owing to maternal sickness or TB)who were not infected with HIV were labelledclinically as HIV infected and managed from theperspective of having a poor prognosis.
The authors of the article conclude by discussing theincreasing difficulties of managing the growingimpact of HIV infection on severely malnourishedchildren in Malawi in the context of reduced supportfor NRUs.
1 The impact of the human immunodeficiency virus type 1 onthe management of severe malnutrition in Malawi: Kessler.Let al: Annals of Tropical Paediatrics (2000) 20, pp 50-56
The impact of HIV onthe management ofsevere malnutritionin MalawiSummary of published paper
A news item in the BMJ2 reported thecessation of OLS flights in the wake ofbombing raids against relief facilities.Roger Winter of the US committee ofrefugees claimed that “these bombingsare clearly deliberate and that theSudanese government is targetingsouthern Sudanese civilians and reliefworkers”.
The air raids followed a series ofintemperate articles in the Sudanese pressalleging that aid agencies have beenhelping to arm and feed the rebel SPLA
1 Sheik et al (2000): Death among humanitarianworkers. BMJ volume 321, 15th July 20002 One Million threatened by suspension ofSudan’s relief lifeline. BMJ vol. 321 19-26thAugust page 470
5
Research
Pieter Dijkhuizen has been asenior programme adviser inpublic health and nutrition at
WFP headquarters in Rome for anumber of years. He has recentlypublished a review article1 on WFP’sinvolvement in the production ofcomplementary foods. A summary ofthe main findings of the reviewfollows.
WFP distributes approximately125,000 metric tons of processedcomplementary foods or blended foodsper year. This kind of food is used inmaternal and child health centres,school feeding, and in refugee andemergency projects. These foodsinclude corn soya blend as well aslocally produced brands such asUnimix, Indiamix and Lakuni Phala.Initially, the US agency forInternational Development (USAID)was the sole source of blended foods.Currently USAID provides half andlocal manufacturers provide the otherhalf of all the blended foods used inWFP programmes and projects. Localmanufacturers use local ingredientswith the exception of the vitamin andmineral pre-mixes which are purchasedfrom the international suppliers. WFPprovides these local manufacturerswith the product specifications and theprocessing instructions which are
consistent with those in the CodexAlimentarius. WFP allows localproducers a 10% profit.
Efforts to involve local manufacturersstarted with small-scale communitybased projects. But the resulting smallscale production was not large enoughto permit the necessary economies ofscale. There have also been problemsof quality control and finding andmaintaining qualified managers. Since1991, WFP has shifted its focus towork with private sector companies ina number of countries including,Bangladesh, Eritrea, Ethiopia, Indiaand Kenya. Each company produces inexcess of 2000 metric tons per year.WFP regulations require that foodsproduced locally be compatible andcomparable with substitutes such ascorn soya blend, which can beproduced in the US and imported intoa given country for less than 500dollars per metric ton. The approach taken in developinglocal processing capability starts byassessing potential processing capacity.Companies are selected through aprocess of public tender, whichincludes price agreements. WFPprovides training and technicalassistance to ensure that foods meet allproduct specifications. In instanceswhere it is determined that inadequate
processing capacity exists, WFP leasesthe necessary equipment to a privatesector company and provides trainingas well as technical assistance.Repayment for the leased equipment ismade as foods are produced and soldto WFP. This approach has provenfeasible in situations where no localcapacity exists since it requires noinvestment and risk-taking on the partof the producer and thus guaranteesthat WFP can negotiate a very lowprice for the food.
On average the foods cost US$360 permetric ton, with 70% of the cost goingtowards the purchase of raw materials.The remaining costs include interestand the profit margin allowed to localproducers. In this way WFP is able tosupport the production of processedcomplementary foods at costs around15-20 times less than those of brandson the commercial market.
WFP considers that it has had a verysuccessful experience working with theprivate sector.
1 Dijkhuizen. P (2000): Processedcomplementary foods in the World FoodProgramme. Food and Nutrition Bulletin, vol21, no 1 pp 62-64
Local Productionof Processed
complementaryfood: World Food
Programmeexperience
Summary of published review
Blended food is often used in supplementaryfeeding programmes. Fango, Ethiopia, 2000.
Pieternella Pieterse (Concern)

Field Exchange 10 highlighted a study underwayby the Humanitarian Policy Group andNutrition Works on the principles and practice
for food distribution in conflict. The objectives of thestudy were to assist humanitarian agencies to developa more principled approach to food distribution. Anumber of case studies were constructed to informthe study: ICRC operations in Somalia (1992 and1999-2000), CARE and WFP in Somalia (1999-2000), The Rwandan refugee crisis in Zaire (1994)and WFP and WVI in southern Sudan (1998-2000).The study1 has now been completed and a summarywith key recommendations is detailed below.
Key points
Fears of ‘fuelling conflict’ and ‘feeding killers’ haveled to a focus on ‘doing no harm’ by many agenciesand their donors. Food distributions will howeveralways benefit the warring parties to some extent.The most agencies can do is to try and minimise this.The main challenge for humanitarian agencies is howto ‘do good’ by finding ways of reaching the mostvulnerable in a political context where this directlyopposes the aims of the powerful. Thus a principledapproach requires active measures by relief agenciesin terms of assessment, analysis and action. Keyprinciples, are humanity, neutrality, impartiality,accountability and transparency. Explicit use of theseprinciples and what they mean for food distributioncan assist agencies in ethical decision-making.
The following steps are recommended for planning aprincipled distribution.
1. Situation analysis
A situation analysis should include the following:
• Risks to lives and livelihoods; to determine theneed to intervene and why.
• War strategies and the war economy; to determinethe degree of exploitation of certain groups andhow food aid can become part of this, e.g. risk ofdiversion.
• Political contracts; to determine the risk of taxation,theft and diversion of food aid, and who is likely tobe excluded. Also, to determine how to work withlocal institutions.
2. Agreement with authorities and co-ordination between agencies
Based on an analysis of accountability of localauthorities, develop an agreement outlining theprinciples of humanitarian action and the respectiveresponsibilities of each actor. Develop mechanismsfor co-ordination between agencies and consistencyin approach.
3. Identifying appropriate distributionmethods
Determine which distribution mechanism is mostlikely to succeed in reaching intended beneficiariesand whether this is feasible. Different distributionmethods have different risks and benefits associatedwith them. An essential question to be considered is:can beneficiary representatives or local institutions berelied on to distribute to the most vulnerable? If theanswer is no then the agency needs to consider
whether a registration is possible for directdistribution. Cooked food distribution may beconsidered in situations where the risk of theft offood aid from beneficiaries is high.
4. Identifying risks of abuse at each stage ofthe distribution process and developingstrategies to minimise them
Stages where there may be specific risks include:
• needs assessment (e.g. no access to certain areas orpopulations),
• engaging with local authorities (e.g. demands fortaxation),
• registration or identification of vulnerablehouseholds (e.g. clans compete for power leading toexclusion of marginalised clans),
• food transport and storage (e.g. taxation on arrivalat Extended Delivert Point (EDP),
• targeting and distribution (e.g. diversion by eldersand village committees) and
• post-distribution monitoring (e.g. taxation or theftafter distribution).
Strategies can be divided into those that maximisefood receipt by intended beneficiaries, and those thatincrease the possibility that they can keep theirrations once received. Examples include; registrationand information campaigns to inform all key actorsof the distribution process. Also, consider deliveryand distribution of small quantities of food on aregular basis, decentralisation of distribution,distribution of less desirable foods, distribution to thesmallest social unit or to the malnourished.
1 Jaspars S., Solidarity and Soup Kitchens: A review ofprinciples and practice for food distribution in Conflict.Humanitarian Policy Group Report 7. August 2000.
6
Research
Principles and Practice for FoodDistribution in ConflictSummary of Published Review
Distribution of cooked food toindividuals
Distribution direct to householdsbased on registration and rationcards
Distribution by communitybased relief committees
Distribution by local NGOs
Distribution by traditional elders
Distribution by local government
– Creates population concentration, Risk ofattack and military recruitment.
– Health risks associated with over-crowding.
– High cost because of high staff andmaterial needs.
– Food needs to be stored and cantherefore be stolen or looted.
– Local representatives are under pressureto favour relatives or the more powerfuland to divert to the military.
– Local representatives may excludeoutsiders, such as the displaced.Therefore agencies need to identify thepolitically vulnerable and ensure they arerepresented.
– Establishing truly representativecommittees is time consuming.
– In acute crisis, traditional leadership maytake over.
– Over-registration of more powerfulgroups, leading to unequal distribution.
– Difficult to register mobile populations;movement is increased at times ofinsecurity.
– Little beneficiary participation.
– May not be neutral or impartial, becauseof ethnicity and political affiliation.
– Under pressure to favour the powerfuland divert to the military.
– Outsiders (e.g. displaced) and sociallymarginalised may be excluded.
– Difficult to monitor.– Under pressure to collect tax and likely
to take part of food aid because of theirstatus.
– Unlikely to be neutral.– High cost if infrastructure needs to be
reinforced.– There is likely to be exclusion of certain
groups if a system of accountability doesnot exist.
– There may be taxation on food ifresources are scarce.
– Government may be responsible forcrisis, e.g. forced displacement.
– Only way of guaranteeing access to foodby the politically vulnerable.
– Reduces risk of theft and taxation.– No registration or ration cards needed.– Overcomes problems of lack of fuel,
utensils, water and physical weakness.
– Ensures that households receive food.– Initial control over beneficiary figures.– Less risk of diversion by elders and
taxation by military and administration.– Undermines abusive leadership.
– Helps strengthen civil society.– Reduces overhead costs.– Brings food to areas inaccessible to
international staff.– Contributes to local knowledge.– May encourage the creation of new
NGOs.
– Distribution according to social andcultural values.
– If this form of distribution is used thereis likely to be an independentmechanism for complaint or appeal.
– Reduces overhead costs.– Can be accountable if population unit is
small.
– Quick and efficient if local infrastructuresufficient.
– Fair distribution if a system ofaccountability exists.
– Builds local capacity.
Method Benefits Risks/Limitations
– Faster than distribution on the basis ofregistration.
– Empowers people and makes them moreresponsible.
– Creates social contracts by electingcommittee members.
– Reduces overhead costs.– Can specify gender balance.– Enhances agency understanding of local
society.

letter
s
7
Research
Guidelines for planning emergency general rationsstipulate that energy content should depend upon:• The age and sex structure of the population. • Health, nutritional and physiological status.• Physical activity levels (PAL). • Environmental temperature.
Accurate information is rarely available in the earlystages of an emergency so that an initial planningfigure, or initial reference value, of 2,100 kilocaloriesis used to calculate energy requirements forpopulations in developing countries (2,300kilocalories energy for industrialised countries). Theuse of a single planning figure makes the task ofcalculating food requirements more straightforwardat a time when decisions must be made quickly withlittle supporting information.
This reference value has been estimated by the WorldHealth Organisation as the mean per capita energyrequirement in emergency situations globally. Thefigure allows for light activity (majority of time spentsitting or standing with work limited to householdtasks and desirable social activity).
The mean per capita energy requirement may beadjusted once more is known about the following:• The age and sex structure of the population• Health, nutritional and physiological status and• Physical activity level (PAL).
Guidelines advocate that where the workload ofadults exceeds light activity the ration should beincreased by 100 kilocalories for moderate activity,150 kilocalories for moderate/heavy activity, and by250 kilocalories for heavy activity. Differences inworkloads by gender must also be considered.
Research1 recently conducted by a team in India maycall into question the validity of assuming thathousehold activities fall into the category of lightactivity. The research was undertaken due to the lackof information from India and other underdevelopedcountries on the actual energy costs of women’soccupational and household activities.
The study attempted to measure the energy cost ofactivities of women from the poor socio-economicgroups in India. Women between the ages of 18-40either working for incomes or classified ashomemakers were randomly selected. Timedeposition studies were conducted by a 24 hourobservation of their activities on a typical day.Predominant activities were identified from theactivity profiles and standardised for posture andduration. The BMR and energy cost of the activitieswere measured by indirect calorimetry (i.e.calculating energy consumption through measuringgas exchange). The tasks were divided into standardhousehold, childcare, occupational and otheractivities. Using WHO/FAO criteria attempts weremade to categorise the activities into light, moderateand heavy. It was significant that except for walkingthe standard activities and occupational work couldbe classified into the light category, (>2.2BMR)while most of the household and childcare activities,except cooking, were classified as moderate to heavyactivities (2.2->2.8 BMR). Mopping was the heaviestamong all the activities measured requiring around4.25 BMR. Walking holding the child was theheaviest among the child care activities (3.18 BMR).
1 Shatrugna T, Venkataramana Y, and Begum N (2000): EnergyExpenditure on household, child care and occupationalactivities of women from urban poor households. BritishJournal of Nutrition (2000) vol. 83, pp 497-503
Physical activitylevels in emergencyaffected populationsSummary of published paper
Market-based means of managing naturaldisaster risk are emerging according to arecent article in Food Policy.1 While
multiple peril crop insurance programmes indeveloping economies have in the past largelyfailed, it may now be possible to create an indexbased insurance contract for when there is a rainfallshortage. Furthermore, there may be a role forgovernment in developing the market for naturaldisaster risk-sharing.
The authors of the article argue that if farmers donot have the means to manage catastrophic riskfrom natural disaster bankers will be forced tointernalise the risks. When bankers recognise thatloan defaults are tied to natural disasters, they willeither ration credit or build in a credit premium tocover these risks. Yet, access to affordable credit isa key to development (and therefore reducedvulnerability to future disaster - Eds). The authorsstate that effective risk-sharing markets for naturaldisaster risks are largely lacking the world over andthat if such markets existed, one might expect, moreaccess to affordable credit, more rapid adoption ofnew technologies, more specialisation in productionand a more adaptive and flexible agricultural sector.
There are several reasons why private markets havenot developed for risk sharing. These include thefact that:
i) Government actions have crowded out suchmarket development by operating highly subsidisedpublic crop insurance programmes therebycompeting unfairly with private insurers and stiflingdevelopment of innovative insurance products.
ii) The costs of insuring farm level yields are highbecause the insurers have to invest in elaborateinformation collection in order to set appropriatepremiums and assess loss.
The authors recommend that what is needed is anindex-linked contract rather than insuring individualcrop yields, i.e. insurance that pays up when atrigger point is reached - like rainfall shortfall.
The authors suggest a number of different rainfallindex policies which may be taken out (zero-onecontract, layered contract and percentage contract).Each policy differs in the way payouts arecalculated in relation to rainfall deficit but have incommon the principle of ‘strikes’ when deviationfrom the rainfall norm triggers some form ofpayment.
The advantages and disadvantages of rainfallcontracts include the following:
Advantages
• lower administrative cost since no on-farminspections are needed and no individual lossadjustments required;
• the insurance can be sold to anyone who hasincome that is correlated to rainfall and can besold as a simple certificate in low denominations.
Disadvantages
• need to have reliable and secure rainfall measuresfor a large geographical area;
• the need to model inter-temporal weather eventssuch as El Niño;
• the possibility of mistakes in selection of criticalrainfall periods;
• the difficulty of potential purchasersunderstanding how to use the insurance contracts.
The authors suggest that some government help willdefinitely be needed in developing countries inorder to realise this type of insurance initiative e.g.:developing research to understand critical periodsof rainfall, investing in infrastructure for secure andreliable rainfall stations, educational efforts to helppotential users know how to evaluate insurancepurchase decisions.
1 Skees.J (2000). A role for capital markets in naturaldisasters; a piece of the food security puzzle. Food Policy,vol 25, (2000) pp 365-378
A role for capital marketsin natural disastersSummary of a published Paper
Dear Field Exchange,
I was interested to see the article in Issue 8 (onthe emergency livestock off-take programme inIsiolo district). ActionAid-Kenya works with theBoran people in Merti division and was one ofthe implementing NGOs mentioned in thearticle. We had already implemented a similaroff-take in 1996, and I went to review theprogramme in 1997. I found some goodexamples of how emergency responses cansometimes provide opportunities for increasedlivelihood security and changed social norms.
Some interesting unexpected impacts from theoff-take project related to gender issues. In thetrading centres, I noticed several ‘kiosks’ wherewomen were brewing tea for sale. Boran womenare not usually economically active outside thehome but it seems the drought provided a‘space’ in which to bend the rules. When crowdsgathered for the emergency livestock markets,these women had seen a trading opportunity.They started with zero capital, borrowing tea andsugar and paying it back at the end of the dayfrom their profits. A year later, these smallbusinesses had become going concerns: onewoman I interviewed was feeding and educatingher three children from the proceeds. This is agood reminder to us all that we need to assessthe impact of interventions through a broad lens,
not only against pre-set indicators and targets.
During a previous drought recovery period,women were included in the communitycommittees (at ActionAid-K’s request) whichwere set up to manage a livestock restockingprogramme. Their knowledge was particularlyuseful for accurate targeting. Several Boranelders (male) told me that only due to this didthey realise women had special knowledge andwere capable of working in committees andspeaking in meetings. A change which other‘development’ activities had failed to bringabout!
As a point of clarification to readers: the articledid not explain the reason for offering subsidiesto entice traders into the area. It was because ofthe 200 km journey, which pastoralists usuallyhave to make on foot in order to sell cattle in theIsiolo market. When cattle are already weak dueto drought, this results in animal loss on the way,and those who do arrive are in poor condition.Traders know they can buy at a knockdown price- no-one is going to trek the animals back homeagain - and the pastoralists make a loss. In 1997,the road was also very unsafe due to banditry.
Pippa Howell, Research & Programme LearningCoordinator, Emergencies Unit, ActionAide-mail: [email protected]

8
Field Article
Acivil war has been raging in Sudan for over17 years since 1983 with fighting betweenthe Government of Sudan in the North and
various rebel factions in the South. Sudan has thepotential of being the “bread basket” of Africa.However, many areas remain food insecure due to acomplex set of intertwining factors. These range fromaerial and ground attacks in which grain stores areburnt, livestock looted and civilians killed as well aslarge-scale population displacement due to insecurity,to natural disasters such as drought and floods.Historically southern Sudan has also beenmarginalised in terms of access to social andeconomic infrastructure such as schools and healthfacilities, and roads and industries. WFP has beenproviding food aid to both the North and South ofSudan through “Operation Lifeline Sudan” since1989. The latest famine in Sudan was in 1998 whereit is thought that over 70,000 people died in the worstaffected region of Bahr el Ghazal.
In late September, as WFP’s Reports Officer forsouthern Sudan, I joined a WFP Annual NeedsAssessment (ANA) team visiting Keew village inZeraf Island, in Phou State of Upper Nile. The ANAteam were visiting Phou State, at around harvesttime, to assess the current food security situation andproject food needs for the state for the year to come.Such food needs assessments are carried out in allstates and counties of southern Sudan, and togetherdetermine how much food aid will be needed in2001. WFP teams apply Participatory Rural Appraisal(PRA) techniques to collect data used to project afood deficit, which is eventually translated into aWFP ration size and target population figure forindividual locations in a state or county.
Arrival
We landed with a bump on the soggy airstrip atKeew. Risper, Senait, Johnson and myself spilled outof the aircraft with our tents, mattresses, food trunksand water for one week. Risper Omondi (Kenyan),Senait Assefa (Ethiopian) and Johnson Thou Mon(Sudanese) are all WFP Assessment Officers who arein charge of projecting food needs in Phou State.Within an hour our tents were pitched in the nearbyNGO compound, and the heavens opened. When therain subsided, I discovered that the inside of my tenthad been flooded and that, arguably, there was moreto camping than meets the eye.
We first met with the local representatives of thehumanitarian wing (RASS) of the SPDF or SudanPeople’s Defence Forces, which is the militia groupcontrolling the area. They gave us a brief on thesecurity, socio-political and economic characteristicsof Zeraf Island, and together we agreed on aworkplan for the days to come. Meetings were alsoheld with the RASS Coordinators for the varioussectors such as health, education and livestock, to getan overview of the facilities in Zeraf Island in eachsector. As is often the case, limited data are collected
by the local officials and much of the information isbased on educated guesses. A meeting was held withthe chiefs, executive-chiefs and headmen of ZerafIsland, to again get an overview on the food securitysituation of the area. These traditional leaders wereasked to rank the various parishes in the threedistricts with regard to food security indicators suchas crop yields, livestock numbers, security, numbersof internally displaced persons (IDPs) and levels ofdisease.
Into the villages
The next few days were spent walking into thenearby villages: Risper was in charge of collectingdata on the “better off” and “internally displaced,”Senait on the “middle,” and Johnson on the “poor”and “very poor” socio-economic groups. We walkedthrough red acacia forests, waded through swampsthat were “puddles” according to our RASScounterparts but came up to our thighs, and afteranother twenty minutes’ walk we arrived in thevillage of Madjang. The counterparts had organisedahead of time, “key informant” groups of six to tenwomen and men from each of the socio-economicgroupings, whom we found already seated undervarious trees dotted around the village.
After a round of introductions and much handshakingand greetings we started with the “semi-structuredinterviews.” The first part of the session was spent on“wealth ranking” i.e. determining the socio-economicbreakdown of the community, the characteristics andthe proportion of people in each group, using a PRAtool called “proportional piling”. Johnson asked ayoung girl to pick 100 thou fruits (a popular andhighly calorific wild food eaten across southernSudan, known as lalop in Dinka and thou in Nuer)from a nearby tree. A woman in the group was thenasked to divide the pile representing the wholecommunity into the various socio-economicgroupings, and in turn sub-divide each group intoresident population versus IDPs, and married versuswidowed. As is often found in southern Sudan, theIDPs who had fled fighting in the oil-rich areas ofWestern Upper Nile and recently arrived in PhouState, as well as the widowed, were amongst the mostdestitute in the community.
Each socio-economic group was then asked about itsability to meet its food needs this year, and requestedto project the food security situation in the comingyear. Detailed questions were asked about each foodsource accessible by that particular socio-economicgroup, to build up a picture of the percentagecontribution of that food source to total food needs,as well as when during the year each food source isavailable. For an important food source for the“poor” and “very poor”, such as thou, questions needto be asked, like: “Is thou available in the area? If so,when do you start collecting the fruit, and when doyou stop? How many times do you collect thou inone week? Who collects it? How much do you
How many Hok does a poor man have?
Anna Shotton is the ReportsOfficer and Gender FocalPoint on the WFPSouthern Sudan Programme.
In the past year, she has produced arange of materials on gender issuesin food aid in southern Sudan thatare available at the WFP offices inNairobi. Anna wrote this article whilsttaking part in WFP's Annual NeedsAssessment exercise in southernSudan this year.
From top left tobottom right:Drying the firstcrops in Keew.Using propor-tional piling - aPRA tool.Johnson, Risperand Senaitcross theswamps. Girlcollecting Thou.Johnson briefsthe team on hisfindings
By Anna Shotton
9
Field Article
collect in one trip?” Information on crop growth andharvest size is also cross-checked by observing thecrops growing in the fields and looking at what is inpeople’s grain stores.
Field analysis
Back at the NGO compound, the ANA team briefedeach other on their individual findings and“triangulated” or cross-checked the data usingdifferent sources. For each food source, the teamcalculated its percentage contribution to the annual,kilocalorie (kcal) needs of a household of 6 persons,by season. The percentage of the total, annual foodneeds of a household that was not covered representsthe food deficit for the coming year faced by thissocio-economic group. This exercise is repeated forall socio-economic groups, and in 3-4 locations in astate/county. The average of the findings across thelocations now becomes the food deficit for that area.These data are then sent to WFP’s base inLokichoggio, northern Kenya for the next level ofanalysis by the Technical Support Unit (TSU) FoodSecurity Advisor and Officers.
Lokichoggio analysis
On receipt of the field data, WFP’s food economyexperts in Lokichoggio review the findings, vet themfor mathematical and other errors and cross-checkthem against other information available for aparticular state/county. The TSU scrutinises the fooddeficits by season and explores possible scenarios forthe food deficit being met by expanding on foodsources other than food aid. Food aid is thereforeonly recommended where the food deficit can’t bemet, causing under nutrition, or can only be met byexpanding on food sources that in the long-term willharm the household’s longer-term food security, suchas the slaughter of the household’s last remainingcow. Although factors such as the future securitysituation cannot be predicted with accuracy, generaltrends are taken into account before settling on a finalfood security scenario for a state/county for the yearahead as well as the total amount of food aidrecommended for that area.
The seasonality of the food deficit is important: onlyin extreme cases do people face food shortagesthroughout the entire year. For instance, if the food
deficit coincides only with the ‘hunger gap’ monthsof May, June and July, then WFP will divide up theannual food allocation for the area into three anddeliver it during those months. Depending on theranking of the food needs within the state/county,certain locations may receive more food aid thanothers. Emphasis is often placed on delivering foodaid during the cultivation season or just before toboost energy levels and therefore productivity, whichin turn should increase future crop yields.
After the TSU recommends ration sizes and targetedbeneficiary figures for all food deficit areas ofsouthern Sudan, a food delivery plan is drawn up.Whether the amount of food recommended isactually distributed on the ground as planned dependson a variety of factors. The most common challengesthat WFP faces when implementing its fooddistribution plans include insecurity, denial of flightclearance and poor weather conditions which preventaccess to beneficiaries as well as temporary shortagesof food aid in WFP’s stores depending on the timingand extent of donor contributions.
Departure
Johnson tuned the radio to the WFP frequency inLokichoggio to hear “Kilo Whiskey [the call-sign forKeew]...your pick up will be not be on figure 28 buton figure 29.” We looked up at the gathering cloudsoverhead: the rains might hold off for another day butcertainly not two. The possibility of getting stuck inKeew for an undefined length of time was staring usin the face. That night it rained but luckily for not toolong and the airstrip the next morning was declared“wet but landable.”
The Caravan flew low over the airstrip several timesto examine the surface, and declared “prepare forlanding.” The plane touched down, skidded thenslowed to a halt. We loaded our stuff onto the planeand got ready for take-off. The plane taxied up therunway and made to turn... that’s when the wheelsgot stuck in the mud. A boy was sent to get a ropeand a shovel, and two hours later, after much pullingand digging, the show was back on the road.Airborne at last and an iced, mango drink inLokichoggio in sight, I settled back into my seat andclosed my eyes.
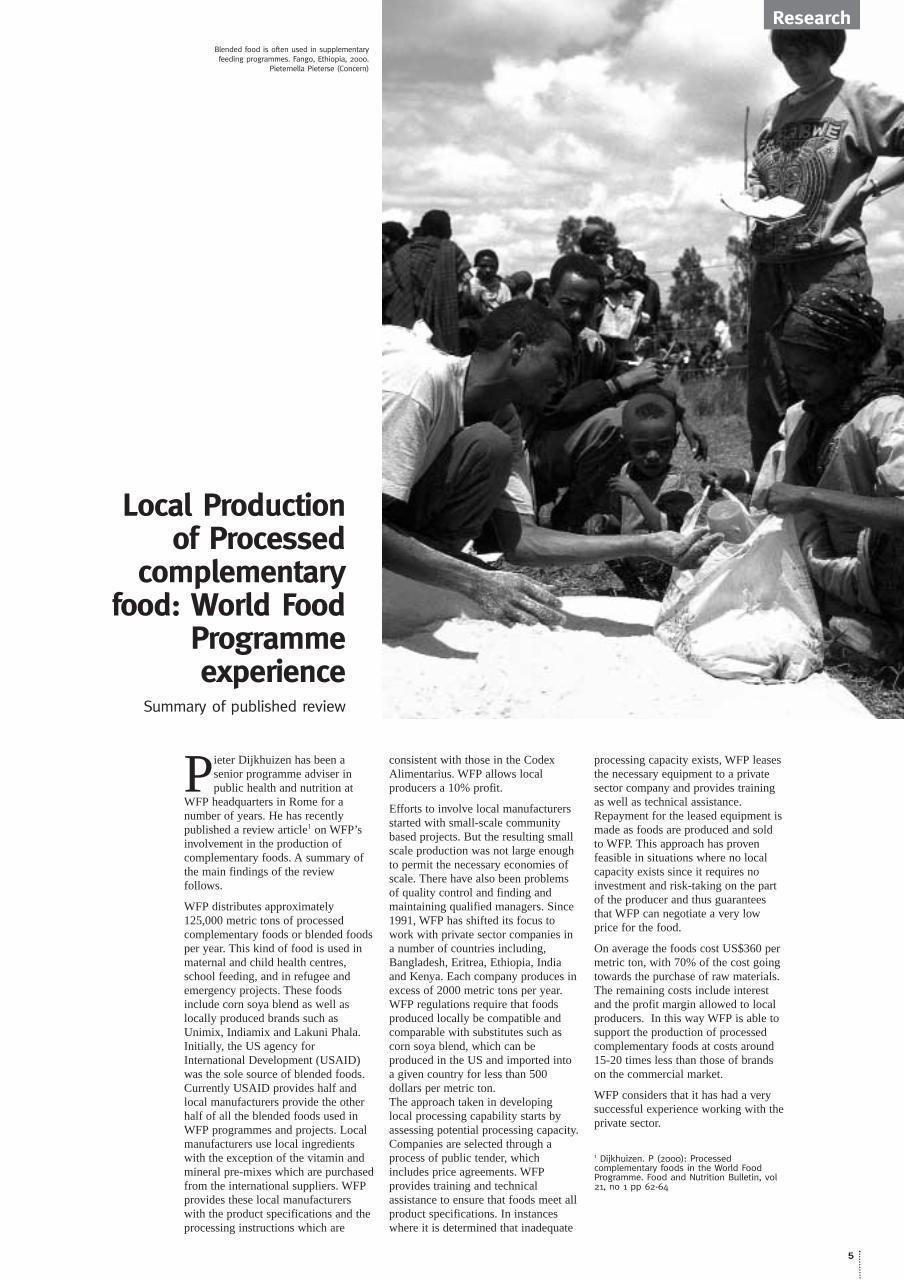
One middle-income household of 6 personsin Madjang village claimed to collect onesmall gau gau (a calabash measurement of 3kg) of thou kernels per week for five monthsof the year from December to April. Thismeans that the household collected 3 kg x4.3 weeks/month x 5 months/year = 64.5 kgof thou kernels per year. If 0.36 kg of thoukernels provides 2,100 kcal and there are2,190 ‘food days’ per year in a household of6 persons (6 persons x 365 days/year), thenthou kernels contribute 8% of a householdof 6 persons’ annual food needs in thissocio-economic group [(64.5 kg/0.36)/2,190) x100 = 8%].
% Population
Crops (grain)
Other crops
Livestock - Milk
Livestock - Meat
Fish
Wild Foods/honey
Barter
Labour
Kinship
Purchase
Total needs covered
Total needs deficit
Poorest
15-25%
0-10%
15-20%
0
0
15-25%
30-35%
0-10%
5-10%
0-10%
0-5%
90-100%
0-10%
Poor
35-35%
5-15%
15-25%
0-10%
0
15-25%
30-35%
0-10%
5-10%
0-10%
0-5%
105-110%
Middle
20-25%
10-15%
15-25%
5-15%
5-10%
20-30%
15-20%
0
0
0
5-15%
100-115%
Better off
15-20%
20-25%
15-20%
15-25%
5-15%
20-30%
5-15%
0
0
0
5-15%
110-120%
Table 1: Food deficit in Twic County, Bahr el Ghazal - ANA 1999
Keew is home to the Thiaang sub-clan of theLaak Nuer. Zeraf Island, has both high andlow-lands, and is encircled by the Zeraf riverto the east and the Nile to the west. Peoplein this area tend to survive on livestock,fishing, crops and wild foods. The island isswampy and is notorious for its malarialmosquitoes. Zeraf Island is subject to inter-clan fighting and raids from a Government ofSudan-backed militia working out of Phomtown north of the island.
WFP assessment teams use the HouseholdFood Economy Analysis (HFEA) approach,developed by Save the Children (UK), as aframework for understanding data collectedin the field. HFEA aims to identify andquantify a household’s means of access to allthe food sources available in an area. Theidea is that you need to understand howfamilies gain access to food in ‘normal’ times,before you can analyse the effects of externalshocks on access to food in a ‘bad’ year.When ‘shocks’ (crop failure, displacement,flooding etc.) occur, the focus of analysis isto determine the impact and consequencesof that shock on the various sources of food.Will traditional coping mechanisms meet thenew needs and at what cost? If a householdcannot meet the new needs created by such‘shocks’, then the analysis should show thesize and seasonality of the food deficit andwhich groups are most affected.
WFP has been using food economy analysisin southern Sudan since 1994 to determinefood needs, highlight potential emergenciesahead of time and prioritise food aidallocations between regions. The frameworkis particularly helpful in a complex and fluidenvironment such as southern Sudan, where‘official’ statistics are largely absent. Over 55WFP, NGO, humanitarian counterpart anddonor representatives are participating infield assessments in this year’s ANA (AnnualNeeds Assessment).

Inter-AgencyStandingCommitteeendorses Sphere
The UN’s Inter-Agency Standing Committee(IASC) Working Group met in New York inSeptember. During this meeting the IASC
endorsed Sphere.1 The IASC is one of the main inter-agency fora for the UN system. In September theIASC working group endorsed Sphere standards asan important tool for anyone working withpopulations affected by disaster. They also called onall IASC members to promote the use of theHumanitarian Charter and Minimum Standards inDisaster Response within their organisations,particularly in their field operations.
The Sphere project highlights this as an importantmilestone in the Sphere process, in particular withrespect to UN agencies that work with NGOs indisaster response.
Eighteen NGOs worldwide have been piloting theimplementation of the Humanitarian Charter andMinimum Standards over the past year. The Sphereimplementation staff are collating lessons learnedfrom this period and will be publishing a paper onthe website in November. Examples include usingSphere around the project cycle, in advocacy for therights of disaster-affected populations and in inter-agency coordination. For further information contact: The Sphere Project, 17 Ch.des Crêts Petit-Saconnex, P.O. Box 3721211 Geneva 19, Switzerland. E-mail: [email protected] Tel:(4122) 730 4501 Fax: (4122) 730 4905www.sphereproject.org
1 AROUND SPHERE IN 60 DAYS: Sphere Project Newsletter No.6, October 2000 www.sphereproject.org For further information, please contact the Project office inGeneva at 41-22-730-4501 or [email protected].
In July 1997, the Sphere Project waslaunched by a group of humanitarianagencies. This project sought to developa set of universal minimum standards incore areas of humanitarian assistance,water supply and sanitation, nutrition,food aid, shelter and site planning andhealth services.
The aim of the Project is to improve thequality of assistance provided to peopleaffected by disasters, and to enhancethe accountability of the humanitariansystem in disaster response.
New vacancies website
Save the Children UK would like to announcethe recent launch of its new vacancieswebsite. On these pages you will find all of
SC UK’s current global vacancies, details on howto apply and key information on working for SCUK. For more information, please visitwww.savethechildren.org.uk/vacancies. For more information contact: Claire Lawrence, ProjectOfficer - Emergencies Programmes Human Resources,Savethe Children Tel: 020 7716 2357 Fax: 020 7793 7614 e-mail: [email protected]
Capacity buildingin nutrition in WFP
The demand for basic technical informationis increasing in WFP especially as we moveto a cluster structure whereby more tasks
will become the responsibility of the field offices.
With the objective of strengthening and makingmore accessible, the organisation’s knowledgebase concerning essential food and nutritionissues, the World Food Programme, Food andNutrition Handbook was prepared.
Using the Food and Nutrition Handbook as aresource document, a set of training materials wasdesigned which cover the fundamental nutritionknowledge of use to WFP staff.
To assist with this undertaking and to ensurecontinuity in the future WFP are being assisted byDr. Helen Young of Feinstein Famine Centre inTufts University, Boston.
The training is a two-tier process. The first stageis to conduct training in 8 of WFP’s regionaloffices. The first training was successfully pilotedin Nairobi in April 2000, and was followed by onein Uganda in August. The second stage is to bringthe training to Country offices using the trainingpackages designed and using WFP Staff withnutrition expertise where available in country. Should you require further information on the subject,please feel free to contact Anne Callanan, Nutrition Unit inSPP, e-mail: [email protected]
SCN reports on nutritionalassessments ofadolescents and adults
The UN ACC/Sub-committee on Nutrition hasrecently published two reports (July 2000) on ‘theassessment of adult and adolescent nutritionalstatus in emergency-affected populations’. Thereport on adults describes simple techniquessuitable for the assessment of nutritional status ofadults aged 20-60 years old in emergency affectedpopulations. BMI, MUAC and clinical models areassessed for their usefulness in determining theprevalence of chronic under-nutrition in adults atthe population level and also for screeningseverely undernourished adults for entrance tofeeding clinics. The report on adolescents tacklesproblems with anthropometry in adolescents andpossible solutions. A number of ‘tentative andpreliminary’ recommendations are made in thisreport.
Summaries of the main findings of these reports willappear in the next issue of Field Exchange. Copies of bothreports are obtainable from:ACC/Sub-committee on Nutrition, 20 avenue Appia, 1211Geneva 27, Switzerland.
Distance learningcourses innutritionCompiled by Ann [email protected] October 2000
The following list was compiled from responsesto an email (sent to the email discussion groupNGONUT) in which information was
requested on distance learning courses in nutritionsuitable for low-income countries. We would bepleased to know of other distance learning courses innutrition that exist or are planned.
PG diploma / MmedSci in Human Nutrition,Sheffield University, UKThese qualifications are offered by distance learning.Information from Josie [email protected]
MSc in Human Nutrition at University ofBridgeport, Connecticut, USAInformation from Michael [email protected] or from theUniversity’s online campus at www.wcc-eun.com/ub.
‘Nutrition Rights’ course at University of Hawaiiat Mânoa, USAThe course syllabus is available athttp://www2.hawaii.edu/~kent/pols675cFall2000Syllabus.doc More information from George [email protected]
Nutrition courses in Masters of CommunityNutrition degree at University of Queensland,AustraliaFour subjects are available by distance learning. Formore information see http://www.acithn.uq.edu.au orcontact Jane [email protected].
MPH at Johns Hopkins University, USASome introductory human nutrition courses areavailable through the internet. Seehttp://distance.jhsph.edu/
Deakin University, AustraliaHuman Nutrition Programme, Deakin University,Australia.Graduate certificate, diploma and masters coursesopen to overseas students even if not on email.Contact Prof Gwyn Jones at [email protected] orSchool of Health Sciences, Deakin University,Geelong, 3217 Australia.
Thanks to Nice Macha in Tanzania who initiated thislist.
news10
news

11
Field Article
Analysis of the underlying causes ofmalnutrition have shown it to be a complexprocess, thus interventions in non-emergency
situations have attempted integrated responses byfocusing on health, food, agriculture, water,economics, religion, traditional beliefs, socialpractice and welfare systems. The ‘Conceptual Modelof the Causes of Malnutrition in Emergencies’ (TheSphere Project, 2000:76) extends this acknowledgedcomplexity into the emergency arena and has becomethe basis for action. Oxfam and other agencies seekto provide an integrated approach during assessment,implementation, monitoring and evaluation.
Despite their best intentions agencies cannot alwaysprovide the interventions they would like, or deliverto the minimum standards they set themselves. Thispaper reflects upon some of the challengesencountered whilst delivering an integrated responsein Gode Zone, Somali Region in Ethiopia.
Background
The Somali Region in Ethiopia has had failure ofboth short and long rains over the past three years.The region is semi-arid and predominantly inhabitedby pastoralists and some agro-pastoralists, who, inthe main, are dependent upon rain-fed pasture andagriculture for their survival. As the drought periodlengthened, their ability to sell or exchange livestockor produce and sell crops became severely affected,and livestock losses increased. The region is one ofthe poorest in Ethiopia with limited access to basicservices and infrastructure such as health, education,water supply, roads and communication. The socialaspects of life in the Somali region are complex and,in common with many predominantly pastoralistareas of Africa, have often become associated withinter clan rivalry and political tension. This continuesto create conditions of poor security in large parts ofthe region, and conflict over control of scarceresources.
Oxfam (GB) agreed with the Ethiopian governmentin early 2000 to provide support in the SomaliRegion, and this paper will report on their emergencyinterventions in Gode Zone. It was suggested thatOxfam (GB) meet the needs in Adadle district ofGode Zone (plus one village in Afder Zone) and alsoprovide expert support to the Water Bureau tomaintain the water supply over a wider area.
Oxfam (GB) began their interventions in late April,when the most critical obstacles to survival were lackof water and food, high rates of acute globalmalnutrition, low immunisation coverage, limitedaccess to health care, increased prevalence of disease,and inadequate shelter, cooking utensils and watercontainers. Extremely high rates of acute globalmalnutrition were identified by several agencies, anda quick house-to-house mid-upper-arm circumference(MUAC) screening by Oxfam (GB) at the end of
May in Bulhagary village indicated an acute globalmalnutrition rate of over 40%.
Consequently, Oxfam (GB) initially planned to:
• Set up supplementary feeding programmes (SFPs)serving up to 2000 moderately malnourishedchildren and 500 vulnerable adults at any one time;
• Set up a therapeutic feeding programme (TFP) forup to 200 severely malnourished, with referralfacilities to Gode Hospital;
• Strengthen the existing facilities at Gode hospital,particularly for the treatment of malnutrition-relatedmedical conditions;
• Support the Zonal Health Department’s (ZHD)measles vaccination and vitamin A campaign;
• Strengthen existing local capacity through trainingof community hygiene promoters;
• Provide treated water to the Oxfam (GB) TFP,villages where the Oxfam (GB) SFPs were sited,Gode hospital and other agencies assisting theaffected population;
• Integrate hygiene promotion activities into allaspects of the water and sanitation activities, and inthe feeding centres themselves;
• Introduce appropriate sanitation measures (latrines,waste disposal, construction) for the feeding centresand the villages in which these were operating; and
• Carry out community mobilisation activities insupport of the interventions.
The decision to conduct these interventions reflectedan assessment of need, and the programmes of otheragencies and government.
Challenges encountered
SFPs were opened in Bulhagary, Busarado, Derihayoand Liban to serve these four villages andsurrounding areas. A fifth was intended in Tordob,but for security reasons was not started. Dry, ratherthan wet feeding was undertaken, as families hadaccess to fuel, and attendance once a week allowedfor the resumption of normal social and economiclife. An Oxfam (GB) TFP was opened in Bulhagary.However, the difficulties setting up and operating inGode Zone were many, some are mentioned below.
Timing of the integrated response
Integrated programmes need to operate atapproximately the same time for the greatest impact.Unfortunately this did not always happen in Adadle.Oxfam (GB) decided to deliver feeding programmesin areas where they believed the general populationwas receiving adequate relief food or had their ownresources. In practice the intended 12.5kg of cerealper person per month from the DDP/WFP wasprobably not delivered. This prompted ICRC toprovide a complementary ration of oil and Unimix (afortified blended food) or sorghum. However, thepopulation in Gode Zone was increasing continuallyand, as both rations were distributed once per month,people would often arrive in villages where thedistribution was not due for several weeks.Consequently many people went hungry or, if theywere lucky, shared the meagre resources of others.When there is insufficient food entering the houseany SFP food is more likely to be shared by thefamily rather than consumed by the malnourishedindividual alone.
As soon as Oxfam (GB) arrived in Gode toimplement the programmes they became aware thathealth care facilities in Adadle were in need of
Challenges to implementing an integratedemergency public health responseBy Dr. Jean Galdwin
Dr Jean Gladwin is a publichealth nutritionist andresearcher with severalyears work experience in
low income countries in emergencyand stable settings. She has recentlytaken up a long-term post in Ethiopiaworking for the World FoodProgramme.
Dry supplementary feeding programme distribution by Oxfam.Gode, Ethiopia. July 2000 (Jean Gladwin)
strengthening, particularly where SFPs were located. Minormedical care was available to the malnourished in the SFP,but the general population needed to travel for days to accesshealth care. Two villages had temporary Zonal HealthDepartment (ZHD) health units, but these were inadequatelystaffed and resourced. No other agency was available to takeon the support of the health centres, therefore Oxfam (GB)agreed to support five health centres in villages where theSFPs were located. Unfortunately, this support was notimmediately available, and the SFPs operated for manyweeks before the general population had improved access tohealth care.
The provision of treated water to villages where the SFPswere operating went well usually due to the efforts ofOxfam (GB), the Water Bureau, SCF (US) and UNICEF.However, there were times when water was not available andthe integrated programme was interrupted. The water wasbeing tankered over great distances to higher than normalconcentrations of population. This was quite a logistical featand there were many occasions when the water tankersbroke down or the water supply from Gode town wasunavailable.
Oxfam (GB)’s intended integrated programme had a hygieneand health promotion component. Bulhagary and BusaradoSFPs began at the same time as the Public Health Specialistwas setting up hygiene promotion activities, including thetraining of community-based health promoters.Unfortunately, the same did not happen in Derihayo andLiban, which interrupted the integrated response. It isparticularly important to ensure good hygiene practices invillages where the concentrations of people are high and yetthis part of the programme proved very difficult toimplement. Moreover, despite the existence of EPI teams atthe zonal level the measles immunisation and vitamin Acapsule distribution coverage was low until the June/Julycampaign. Although that campaign did reach over 6000children under five years old it would have been better if hadbeen initiated earlier as several measles-related deaths werereported in June.
Working with the local community
Providing emergency support to nomadic populations in anarea of weak infrastructure is very difficult. Frequentdiscussions were held with community representatives (men
and women) to decide where SFPs should be sited, and thecommunity’s needs. However, clan rivalries had to be takeninto account when implementing the programme andinsecurity curtailed the activities at times.
Balancing community needs and wishes against theresources available and technical knowledge meant that notevery one could be catered for. Targeting, rather than equalsharing of resources was difficult for many people to accept.All the villages wanted to have a TFP which led to tension attimes, and although the people of Derihayo and Liban werewilling to take the severely malnourished children to theexisting TFPs none of the severely malnourished childrenfrom Busarado were taken. This may have been because thecommunities were different sub-clans (although analternative TFP was available) or for other reasons. Thewomen from Busarado said that it would be difficult forthem to leave other family members or their temporaryshelters. Oxfam (GB) offered to support siblings, but it didappear that there was a lack of a community supportnetwork. Without an in-depth investigation it is difficult toknow why the children did not go to the TFP, but whateverthe reasons the integrated emergency response was againinterrupted.
Lack of staff and local implementing partners
Usually Oxfam (GB) prefers not to become fully operationalin emergency situations but to work with local implementingpartners. If circumstances do not allow this, perhaps due tolack of capacity or conflicting political agendas orinsecurity, it is necessary to set up programmes staffed byOxfam personnel and introduce Oxfam procedures. In GodeOxfam (GB) became fully operational, and although most ofthe two hundred staff members employed were from GodeZone, most of the senior people were not. They included asmall number of expatriates and Ethiopians from other partsof the country, who did not have the same culturalbackground or have extensive knowledge of the area. This isan issue in any programme, but particularly so in SomaliRegion where the clan system dominates all aspects ofsocial, economic and political life.
Oxfam (GB) arrived in Somali Region at a time when nottoo many other agencies were setting up programmes.Consequently government employed nursing staff weretemporarily seconded, which greatly eased the operation and
12
Field Article
Oxfam water treatment plant.Gode, Ethiopia. August 2000 (Crispin Hughes/Oxfam)

13
Brian Scott, executive director of OxfamIreland led me to his office on the top floor ofthe Oxfam Ireland building on the banks of
the River Liffey and just a stone’s throw fromO’Connell Street bridge in the heart of Dublin city.The office has a great view of downtown Dublin.
The director, who is from and lives in NorthernIreland, explained that up until May 1st 1998, OxfamUK & Ireland were a single entity (a British charity)which had a branch in Dublin. Oxfam’s establisheditself in Northern Ireland and “spread by osmosis viaits shops through Northern Ireland and the Republicin the 60s and 70s”. Two and a half years agohowever, Oxfam UK & Ireland ceased to be and re-established as two separate charities, Oxfam GB andOxfam Ireland. This arrangement allows betterrepresentation of the views and priorities of Irishpeople in both the north and south.
For legal reasons Oxfam Ireland consists of OxfamNorthern Ireland and Oxfam Republic of Irelandwhich are registered as 2 separate charities. OxfamIreland became the 11th member of OXFAMInternational (see box) “However in operational
terms we run as one organisation, and to all intentsand purposes are one OXFAM. This means thatwhoever you are on this Island, whatever yourreligious or political persuasion there is no barrier toyour support of Oxfam. We have departments whichcover the whole island for example, retail, marketingand fundraising. Some of the department managerssit in the Belfast office and some in the Dublinoffice.” Understandably there are difficulties withrunning an organisation which straddles bothNorthern Ireland and the Republic. For examplemaintaining parity of salaries taking into accountexchange rates and differential taxes and costs ofliving is not easy. However there are also advantages.Finance and administration are based in Belfastwhere it is easier to find staff.
The energetic and enthusiastic executive directorworked in the private sector prior to starting withOxfam 3 years ago, “Until this I had no involvementwith the NGO world at all. I’ve always beeninterested in development - economic development inone shape or form.” Brian started out as aschoolteacher in Zambia back in the sixties. “I feltpowerless, I saw things I would like to change butfelt no sense of ability to do so as this little cog inthis national education machine. So I naively thoughtto myself the private sector was the place to be, Ijoined a publishing house in Tanzania.” Here makingan English textbook appropriate to Tanzanian cultureand available for each child and teacher was one ofBrian’s greatest achievements at that time. Aftermoving to Mexico to set up a subsidiary publishinghouse producing textbooks for schools for a numberof years, Brian went to Business school andundertook an MBA DBA. Pursuing his interest in therole of the private sector in development hisdissertation looked at the role of the private sector inproviding technical and management services foragribusiness development. As he is now executive
Agency Profile
meant that Oxfam could train such staff to respond tofuture emergencies. Experienced nutritionists wererecruited which no doubt improved the quality of theprogrammes, especially in comparison to othernutrition programmes in the region that were beingoperated without nutritionists. However, senior localstaff and international staff were very difficult to findand now that many agencies are implementingemergency programmes in other parts of Ethiopia itwill become harder to recruit and retain such staff.
Incidence of disease and environmentalconditions
Somali Region is a very tough environment in whichto work, particularly so after the short rains and dueto the constant wind that began in June. Theincidence of communicable disease is very high, andOxfam (GB) staff suffered much illness. MSF (B)estimated the prevalence of TB in parts of SomaliRegion could be as high as 250:100,000, but thetreatment requires a long-term commitment, which isnot always possible during an emergency and whenfunding is precarious. The TB treatment programme,supported by MSF (B) and the ZHD, was confined toGode town, and did not cover Adadle district unlessthe person concerned agreed to live in Gode.Consequently few cases were treated, and no doubtthe inability to deal with TB and poor environmentalconditions reduced the impact of other programmes.
Logistics and bureaucracy
Logistical and bureaucratic problems encountered inattempting an integrated response proved to be verytime-consuming. Poor infrastructure, made worse bysecurity problems, rendered parts of Somali Regionextremely isolated geographically. During the rainyseason (for ten days in late April and early May 2000Gode Zone received a very heavy rainfall, although itdelivered less than normal for the time of year),many villages are inaccessible because most roadsare simply dirt tracks. Even the maintained roads inAdadle have broken bridges that are impassable inthe rain. The lack of good quality tankers meantthere was a constant need for spare parts that had tocome from Addis Ababa, often resulting in breaks inwater supply. Some of these problems could beovercome by increased funding, but many neededlonger-term solutions, or long periods of waiting.
Conclusion
An integrated emergency response is unlikely to beprovided by a single agency and consequently a co-ordinated response is necessary, spearheaded bygovernment. In Gode Zone governmentaldepartments did not have the capacity to co-ordinatean appropriate response, although some departments(such as the ZHD) were better equipped with seniorstaff than others. Consequently the UN and NGOssupported the Government Task Force and itssubcommittees.
Oxfam (GB) is conducting very good programmes inGode Zone. Lives have been saved and the quality oflife improved. This review is intended as a reflectionupon the achievements and problems, not as acriticism. The Oxfam (GB) staff are extremely hardworking and dedicated. Their programmes are oftenrecommended as role models for other agencies.However, their efforts alone cannot provide all thenecessary support for the people in Adadle district.
ReferencesThe Sphere Project Humanitarian Charter and MinimumStandards in Disaster Response, published by The SphereProject, Geneva.
Emergency relief project for the drought affected people inSomali Region, Ethiopia, Oxfam (GB), Addis Ababa April 2000.
General report of Assessment Mission conducted in Shinnileand Jijiga Zones of Somali Region, Ethiopia July 10th - 15th2000 Oxfam (GB), Addis Ababa, Ethiopia.
Dr Jean Gladwin is currently working in Ethiopia and wouldwelcome visits by other nutritionists. She can be contactedby e-mail: [email protected]
Oxfam IrelandInterview with Brian ScottBy Fiona O’Reilly
Name Oxfam Ireland
Address 9 Burgh Quay, Dublin 2, Ireland
Telephone +353 (0)1 672 7662
Fax +353 (0)1 672 7680
Email [email protected]
Internet http://www.oxfamireland.org
Year formed 1998
Director Brian Scott
Overseas staff 0
HQ staff 30
Annual Budget IR£ 2,674,920
Residents in Mutete, Rwanda developingterraces for crop planting.
Courtesy of Oxfam Ireland

Being Part of Oxfam International
Major emergencies have sadly become part of the fabric of OxfamInternational’s (OI) work in recent years. Where civilians are caughtup in conflict or natural disasters in the poorest countries of the world,that’s where Oxfam International often has to marshal its resources toprovide help and expertise.
Oxfam International is a group of eleven national organisations, whoseconsiderable experience in this field over many years can lend the kindof help that people really need in times of crisis. So, Oxfam Irelandworks with colleagues in Washington, Ottawa, Berlin, The Hague,Oxford, Hong Kong, Melbourne and other key centres to make abigger impact on the lives and future of the people Oxfam seeks tohelp.
Sometimes this means lobbying national governments or internationalinstitutions like the United Nations to take urgent action inhumanitarian situations. On other occasions, it means providingequipment and personnel at speed in places struck by a major disaster.Or, it can mean supporting partner organisations in the field, helpingthem to prepare for or tackle humanitarian problems in their owncountry.
Oxfam Ireland has been part of all of these. Kosovo, East Timor,Mozambique, Angola, Sudan and Ethiopia are recipients of OxfamIreland’s humanitarian programme.
In one of the biggest emergencies to challenge aid agencies last year,Oxfam Ireland supported Oxfam GB’s work with vulnerable groups inboth Serbia and Kosovo where saving lives, protection, rehabilitationand rebuilding education were all part of OI’s efforts.
In East Timor last year, advocacy played a key part in gettinginternational peacekeeping troops into Dili to halt the destruction ofthe newly independent country by Indonesian militias. Oxfam Irelandwas one of several Oxfams working tirelessly to make sure the UN didnot renege on commitments to the East Timorese. Financial supportamounting to 30,000 US$ has gone to OI’s programme in Timor,where our work still continues.
And in Mozambique, Oxfam Ireland is part of a programme ofrehabilitation in Inhambane province in the centre of the country.Some 115,000 US$ has been earmarked for work organised byOxfam’s Spanish affiliate, Intermon, to provide housing, clean waterand sanitation facilities, seeds and tools.
Mozambique faces the possibility of renewed flooding in the closingmonths of this year and Oxfam Ireland’s invaluable work helpsmillions of people whose livelihoods have been totally destroyed.
Emergencies aside, Oxfam Ireland works with its OI colleagues on araft of other issues - education, debt relief, fair trade and globalisation- that enable Oxfam International to have an impact in putting rightsome of the world’s inequities. Oxfam Ireland’s contribution plays avital part in making a difference on the long road ahead.
Rachel Stabb – Oxfam International Media Officer for Emergencies23rd October 2000
14
Agency Profile
Director of an NGO. I wondered if Brian hadchanged his mind about the contribution of theprivate sector to development. “No I haven’t, itcomes back to what we are trying to do in thefirst place, - alleviate poverty and suffering. Howare the poor going to become less poor andbetter off? By earning a living. They are notgoing to do so by receiving more handouts.”
Oxfam Ireland is interested in enterprisedevelopment to enable people to be independentand self-sufficient. I asked what do charities likeOxfam know about enterprise development andwhether this is not more appropriately an areafor the private sector. Brian explains that Oxfamin particular have much experience in this area“I as Executive Director have responsibility for achain of retail shops - it’s a business and believeme the competition is pretty tough out there. It istrue that without the dedicated selfless work ofvolunteers who run the shops we could notoperate but similarly if we didn’t run them like abusiness they’d close.”
Oxfam Ireland is small so it focuses on a fewAfrican countries: Ethiopia, Kenya, MozambiqueAngola, Zambia, Sudan, Rwanda and Tanzania,working through other Oxfams and indigenousorganisations. “In emergency operations webecome part of the Oxfam Internationalapparatus. Historically, Oxfam GB usually tookthe lead using their long experience inemergency response, with other Oxfamsproviding support. This model isn’t universalhowever, for example in East Timor OxfamAustralia took the lead and everyone elsesupported them. In terms of developmentprojects we have much stricter controls indefining in advance what it is we want,determining specifically what projects and partswe will fund.”
One of the advocacy issues Oxfam Ireland islooking at is global food trade. Brian sees theunderlying causes of poor nutrition and health aspoverty. “A huge amount of which is in ruralareas among subsistence and semi-subsistencefarmers.” He believes that “one of the ways ofincreasing their income is through producingcash crops of one sort or another and getting abetter price for it. And how can we do that?” heasks rhetorically “well maybe getting faireraccess to markets. Oxfam Ireland has beencampaigning in Ireland for fair food trade and isalso engaged in advocacy for access for all tobasic education. Oxfam Ireland works in anumber of thematic areas: food, education, HIVand AIDS, fair trade and enterprise development.Brian gave examples of how themes andprogrammes feed into one another. “Oxfamshops are there to raise money, but they are alsoused to sell fair trade products, and we areengaged overseas in developing small enterprisesin one way or another e.g. farmer co-operativesthat are engaged in the production of fair tradeproducts.”
For the future Brian would like to see OxfamIreland becoming as efficient as possible andcontinuing with the Oxfam tradition ofinnovation. He would like, as an organisation, tohave the capacity to know which kind of activityis most cost effective.
Brian says: “ I am deeply unhappy with ourfailure to raise sufficiently the indignation ofmore people about the obscenities of worldpoverty.” He would like to see a mass movementof people imposing taxes on themselves in theform of taking out direct debits and supportingwhichever group or NGO they choose to addresspoverty in the world today.
Rwanda - Oxfam Ireland

15
Field Article
The application ofminimum standardsduring crisisA practitioner’s perspective, southern Sudan 1998/9
Stephanie Maxwell worked as themedical co-ordinator for MedicinesSans Frontiers Holland (MSFH)between May ‘97 and March ‘99,and as programme manager duringthe crisis period in southern Sudan.
Between mid 1999 to early 2000 she was workingas a nutrition consultant for Unicef in theOperation Lifeline Sudan Programme (OLS) for thesouthern sector. Part of the Unicef assignmentincluded a review of some of the targeted feedingprogrammes being implemented in southernSudan.
The Sphere Project was launched in 1997 todevelop a set of universal minimum standardsin core areas of humanitarian assistance. The
aim of the project is to improve the quality ofassistance provided to people affected by disasters,and to enhance the accountability of thehumanitarian system in disaster response. The projectwas however never intended to provide acomprehensive guide for assessing interventions orcover the complete range of potential humanitarianresponses. This sometimes gets forgotten in thedebate over the application of minimum standardsduring a crisis.
The Minimum Standards specify the minimumacceptable levels to be attained in sectors ofhumanitarian response. Each standard has a set ofkey indicators which signal whether the standard hasbeen attained. They provide a way of measuring andcommunicating both the impact, or result of theprogrammes as well as the process, or methods used.
This article examines aspects of the influence, useand impact, of the nutrition ‘Minimum Standards’during the response to the 1998/9 humanitarian crisisin southern Sudan. The discussion is largely basedupon consideration of Standard 2 for TargetedNutritional Support for Severe Malnutrition, andsome of the key indicators used in the context of theemergency in southern Sudan in 1998/1999. Therelevant standard and indicators read as follows:
The 1998 food crisis in southern Sudan
The multiple factors that brought about thehumanitarian crisis, and shaped the humanitarianresponse are well documented.* The principalconstraints that characterised the 1998 humanitariancrisis and response in southern Sudan aresummarised as follows:
• Humanitarian agencies were initially denied accessto the affected population by the Government inKhartoum.
• Limited infra-structure and poor communicationsystems.
• Logistical constraints, especially when airstripswere wet and/or too short, making it impossible forvital cargo planes to land.
• Working in flat, flooded and swampy conditions.• Lack of experienced international and national
professionals.• The overwhelming scale of the problem.• Inadequate co-ordination of the humanitarian
response.
Furthermore, one of the key prerequisites for anefficient and effective emergency nutritionintervention was not fulfilled during the early stages
Standard 2
Targeted nutritional support standard 2:severe malnutrition
Mortality, morbidity and suffering associated withsevere malnutrition are reduced.
Examples of Key indicators
• Proportion of exits from a therapeutic feedingprogramme who have died is <10%.
• Proportion of exits from therapeutic feedingprogramme recovered is >75%.
• Proportion of exits from therapeutic feedingprogramme defaulted <15%.
• There is a mean weight gain of >8g per kg perperson per day.
• Nutrition worker to patient ratio is at least 1:10.
Airdrop site, South Sudan ‘99(UNICEF)
* Co-ordinating a Humanitarian Response in Sudanby Murphy et al, Field Exchange Issue 6
By Stephanie Maxwell

of the crisis. An adequate general food ration was notprovided for all in need.
Awareness of the Sphere Project and theMinimum Standards
There was limited awareness among field staff of theexistence of internationally established minimumstandards for humanitarian assistance. Generally, it wasagency head office staff rather than ‘front-line’ staff whowere aware of the project. In some instances, MinimumStandards were invoked as a basis for assessing theperformance of agency interventions. In retrospect, anumber of critical observations about the role andapplication of the minimum standards can be made.
When standards can not be attained
The two following boxes describe aspects of thetherapeutic feeding programmes implemented by anMSF section in 1998 and my personal experience ofadapting guidelines when faced with a complex andoverwhelming situation. This highlights potentialconflict with Sphere project minimum standards and thekey indicators used to measure attainment of thosestandards. The standard in question is ‘standard 2’ (seebox on previous page) for targeted nutritional supportfor severe malnutrition while the relevant key indicatorsare “There is a mean weight gain of > 8g per kg perperson per day” and “Nutritional and medical care isprovided to people who are severely malnourished,according to clinically proven therapeutic careprotocols”.
16
Field Article
Standard 1
General Nutritional Support Standard 1:Nutrient Supply.
The nutritional needs of the population are met.
After appraising the situation in one site which hada limited number of locally available qualifiedstaff, a high level of insecurity for internationalstaff, and resolute mothers who were reluctant tosit in a centre all day - I recommended that asimplified TFC regime be put in place.
I recommended a two tier TFC. The two tiers werefor children who did or did not have an appetitebased on the assumption that those without appetiterequired more supervision. Malnourished childrenwith an appetite would either come in the morningor the afternoon for approximately four hoursdepending on the allocated shift. Children withoutan appetite would be encouraged to spend morethan half a day at the centre. All children received atake home ration of made up milk and BP5biscuits. If necessary, and with time and sufficienttraining, I assumed that it would be possible tobuild on the simplified model so that it wouldeventually have the characteristics of aconventional TFC. The rationale for such a designwas:
• to free up time for mothers thereby reducing thelikelihood of other children being admitted;
• due to the limited number of qualified nationalstaff available such a system meant that therewere less children at the centre at any given timeso that the TFC could more easily adhere toanother of the key SPHERE indicators “Nutritionworker to patient ratio is at least 1:10”;
• to enable national staff to run the programme ifinternational staff were evacuated for securityreasons.
Adapting the guidelines - Example 1
Cattle Camp, South Sudan ‘99.(UNICEF)
This deliberately simplified TFC regime deviatedfrom certain aspects of standard therapeutic careprotocols/guidelines e.g. a three-phase system with12-24 hour supervision. Understandably, this receivedcritical attention from certain experienced MSF teammembers. Their concerns were real and justifiable,MSF had years of experience and who was I to adaptinternationally recognised MSF nutrition guidelines.“Minimum standards for therapeutic feeding were notbeing met.”
Eventually, the team agreed to implement thesuggested design. During the course of theprogramme children successfully gained weight (butat a slower rate than 8gms/kg/day) and the approachwas replicated in other sites later on in the crisis. It isdifficult to establish scientifically the merits of thisparticular intervention (after several weeks theprogramme was closed due to insecurity and some ofthe relevant data were lost). However, in Panthouduring the later stages of the crisis the above designwas implemented and the recovery rates were 75%. Ibelieve such an approach was appropriate andeffective for the given context.
A number of critical observations about the role andapplication of minimum standards can be drawn fromthese experiences:
a) Assessing standards in a particular context.While the Sphere Project offers a set of standards andindicators, neither these standards nor otherinternationally recognised nutritional guidelines wereable to prepare or offer solutions for “front lineworkers” for the array of constraints and challengesfaced by humanitarian agency staff during the 1998food crisis.
b) Distinguishing between innovative and poorlymanaged programmes.
During the crisis, there appeared to be inadequaciesin the capacity of some commentators to distinguishbetween organisations which had adopted ‘innovativeapproaches’ to deal with the overwhelming situation(which in some cases meant deviating fromguidelines), and organisations which wereimplementing poorly managed targeted feedingprogrammes (which also sometimes occurred). Theuse of the Sphere Project as a tool did little tostrengthen (and may even have undermined) thecapacity to make such distinctions. In somesituations, optimal programme design (as advocatedin guidelines) had to be modified in order tomaximise the achievement of the minimum standard.
There were certainly instances where this apparentdeviation from standard protocols/guidelines wasperceived as a failure to meet standards as suggestedby Sphere (e.g. the key indicator suggested as ameans of assessing attainment of the minimumstandard is adherence to standard protocols). Theoverall situation was not helped by the fact thatprofessionals did not appear to agree readily on themost appropriate strategy for nutrition interventions,given the complex and challenging circumstances.
c) The application of MinimumStandards and their respectiveindicators
Where programme design ismodified in order to maximise
attainment of standards the relevant key indicators forany given standard may not be appropriate orattainable, and if applied, may indicate poorprogramme performance.
d) The misleading nature of the term ‘MinimumStandards.’
Some professionals argue the standards, and theirrespective indicators, are appropriate for accessibleand relatively safe refugee settings while in complexemergencies, they may be the ideal, but not reallyachievable. For example, water supply standards werenot achievable throughout most of southern Sudanduring the ‘98 crisis. But the term ‘MinimumStandards’ suggests they should be achievable. Incertain situations, when standards and their indicatorsare unrealistic, the Sphere Project is considerablyweakened as a tool to challenge poor practice.Perhaps a more appropriate and less confusing termmay be ‘international references’ or ‘internationalstandards’.
e) Using the Minimum Standards as a measure forgreater accountability.
Though well intentioned, the attempts to makeagencies more accountable by promoting theadoption of the Minimum Standards in southernSudan, did not always achieve this objective. Onereason appears to be that criticism was being receiveddefensively. In addition, due to the strainsexperienced by the main co-ordination body (in thiscase, the UN) and the lack of capacity found in localauthority structures, some professionals assumed anad hoc watchdog role. As there was no agreedmandate for such a role, this had, at times, theinadvertent effect of making agencies less willing tobe transparent and did little toimprove accountability.
17
Field Article
During the crisis some MSF programmesreduced the admission criteria for the TFC from<70% wt-for-ht to <60% wt-for-ht in order to beable to cope with the overwhelming numbers. Itcould be argued that the Minimum Standardsfor targeted support to reduce mortality,morbidity and suffering associated with severemalnutrition were being met as far as possible,given the difficult circumstances encountered(including an inadequate and erratic generalfood ration). However, some of the relevantindicators for the minimum standard such as the“proportion of exits from a therapeutic feedingprogramme who have died is <10%” and the“proportion of exits from therapeutic feedingprogramme recovered is > 75%” could nolonger be reasonably applied as children < 60%wt-for-ht are likely to suffer higher mortality. Ifsuch indicators were applied withoutconsideration of the context one would conclude(unfairly) that the programme was of poorquality and ineffective.
Limitations of minimum standards inprogramme assessment - Example 2
Supplementary FeedingCentre in South Sudan ‘99.(UNICEF)

18
Field Article
f) The ‘right’ to commentAt the onset of the crisis, MSF was among a numberof agencies who publicly voiced their concern overthe World Food Programme’s capacity to meet thescale of needs facing the vulnerable population.However, a number of MSF workers questionedwhether it was appropriate for MSF to continue tocomment on the capacity of WFP to respond to thesituation when MSF could also be criticised for notadhering to Minimum Standards. This was one of thereasons why MSF reduced efforts to high-light thedifficulties facing WFP.
g) The impact of the Sphere Project in shaping theresponse to the crisis.Even with greater awareness of the project, it isunlikely that the project would have greatly helped toimprove the quality and efficiency of the response,for the following reasons:
• The Sphere Project would not have offered practicalsolutions to the constraints being faced bypractitioners
• Many of the Sphere Project standards would haveappeared unrealistic, and it is possible that the‘baby would have been thrown out with the bathwater’.
• Where programmes had adapted their interventionsand therefore appeared not to attain the MinimumStandards, indicators could no longer beappropriately applied in order to determine thequality and effectiveness of the intervention.
One factor which would have significantly helped toimprove the effectiveness and quality of the overallnutrition response, would have been a wider use ofinternationally recognised operational nutritionguidelines (even though I have later recommendedthat these need to be revised to providerecommendations on ‘optimal’ practice in the face of
overwhelming circumstances). This is particularlytrue for agencies that had large numbers ofinexperienced professional staff, and/or agencies withlimited institutional experience of selective feedingprogrammes. Several agencies I visited which wereimplementing feeding programmes, struggled withpractical issues like maintaining adequate registrationbooks. Such difficulties could have easily been solvedby the greater use of recognised nutrition operationalguidelines.
Suggestions for strengthening the Sphereproject
The Sphere Project should be commended andsupported for aiming to improve practice within thehumanitarian arena. However, the Project hasweaknesses. Below are some suggestions to helpminimise these weaknesses and maximise the valueof Sphere.
a) Reconsider the term ‘minimum’The term ‘minimum’ is misleading and confusing andshould be replaced by the term ‘internationalstandards’ or ‘international references’. The fact that Minimum Standards in certain contextsare unrealistic needs to be addressed.Criteria could be established to determine under whatcircumstances and how, minimum standards can beadapted to specific contexts: but always with theeventual aim of achieving international Standards. Anadditional chapter could be devoted to this. Thisprocess should also be supported by revising existingguidelines to include recommendations for situationswhere standard protocols cannot be adhered to, andcompromise measures might need to be introduced.These measures may go some way towards reducingthe intimidating aspects of the standards and preventinnovative ideas being stifled for fear of falling shortof the standards.
b) Promote the use of operational guidelinesThe Sphere Project should more actively promote theuse of recognised agency operational guidelines inorder to compliment the Sphere Project document.
c) Create the necessary environment to promoteaccountability and transparency
It is a matter of urgency to improve existingaccountability systems and to ensure the correctenvironment is created to encourage agencies to beaccountable and transparent. The current Ombudsmanproject (instigated at the World Disasters Forum in1997) seeks to encourage agencies to adhere to themain codes and standards in humanitarian work. Theproject, co-ordinated by the British Red Cross, isinvestigating the feasibility of creating anaccountability mechanism for humanitarianassistance. The Ombudsman will provide amechanism to “help bridge the accountability gapbetween agencies and the claimants” of humanitarianassistance by having an independent office toinvestigate complaints or problems.
d) Strengthen the link between the policy makerand the practitioner
The link between the policy maker, researcher andpractitioner needs to be strengthened. Practitionersneed to be better informed of latest research findingsand their link to policy development while policymakers need to be better appraised of the realities onthe ground. The Sphere Project has taken theinitiative to raise awareness of appropriateintervention standards around the world. This isundoubtedly a positive step and should be applauded.However, the project can only have limited impactunless there is a corresponding commitment by theagencies to institutionalise the principles, policies andvalues of the Project while assisting practitioners toapply these in a flexible and appropriate manner.
Humanitarian practitioners arebecoming more technicallyproficient, and the above article
is an excellent exploration of thedilemmas of operating in a difficultsituation, while maintaining loyalty toas scientific and ethical an approach aspossible. The author raises validquestions about the application of theMinimum Standards and KeyIndicators.
The Sphere Minimum Standards weredeveloped to reflect a qualitative levelof disaster provision applicable acrossall operating environments. Thestandards define the requirements forlife with dignity in relatively generalterms, while the indicators attach eitherqualitative or quantitative values toassociated standards. It would be adisservice to the rights of populationsaffected by disasters to call the levelsreflected in the current Spherehandbook international - hopefullyinternational levels would be higher!
It might be argued that agencies andstaff were effective given thelimitations of Sudan in 1998. TheHumanitarian Charter and MinimumStandards make a line in the sand (theright to dignity, quantified in the fivebasic sectors) from which we canmeasure our programmes, describe a
particular context, and justify resultsand the indicators we use to measurethose results. Perhaps one way to lookat the Key Indicators in the Spherehandbook is to insist that they bemaintained as written. They areminimal after all, and what NGOs needto do better is describe in morecredible detail what the reality is in thefield. With this line in the sand thatfixed indicators would help define,humanitarians can describe needs andreport on their results with reference tosomething concrete. (Thus there is abig difference between inappropriateindicators and unattainable ones).Obviously in Sudan in 1998 there wasa pretty big gap between the line andthe reality on the ground. That gap canbe explained in terms of time toimplement an operation, resources andother contextual factors like securityand access.
The Sphere handbook does not containoperational guidelines because it is abook of Minimum Standards andindicators. How agencies and their staffwill respond in a particular situationwill depend on their mandate, capacityand experience. One might argue that‘front line workers’ could better lobbyfor resources and support by explainingtheir operating context with referenceto that “line in the sand”. Whether
agencies have time to do this analysis,reporting and advocacy is anothermatter, and a problem that we all face.
Distinguishing between innovative andpoorly managed programmes iscompromised when one applies only atechnocratic application of thequantitative indicators. The differencebetween innovation and shoddyprogramming is in the ability toarticulate the analysis done and theassumptions made about the cause-effect relationship between actions andthe impact on people’s ability to livewith dignity.
Accountability requires some sort ofstandard, and so the creation of theMinimum Standards is an importantstep in improving accountability. TheSphere Project is in fact a process, andthat process is continuing to evolve andimprove. A revised edition of thehandbook will be published in the year2003, based on the suggestions, adviceand feedback from practitioners in thefield, and lessons learned from theapplication of the handbook inpractice. Those comments should bedirected to the Project Office using thefollowing email: [email protected] .
Let us remember that a situation inwhich entrance criteria must bereduced, or indeed, in which a TFC is
needed at all, is a horrible injusticefacing people in the developing world.The fact that most humanitarianworkers must make decisions when ina dilemma, based on minimalinformation, with inadequate resourcesand access is one of the most difficultthings about field work. It is also oneof the things that humanitarianagencies don’t speak about enough.The essence of accountability in thisparticular context would not be to saywhether a standard is being met or not,but to measure the gap between whatwas possible and what is aspired, andto explain why that gap exists. Thisarticle explains why the MinimumStandards were not met, and any donorwould understand. Any recipient wouldalso understand, but the fundamentalquestion remains, why does thishappen in the year 2000? Thehumanitarian system needs to blow thewhistle on injustices, and having acommon language to work from willonly strengthen our unique andindependent actions toward thiscommon purpose.
Post ScriptBy Sean Lowrie, Training Manager, Sphere Project
[email protected] or [email protected] Tel: (44)20-7379-5247 ext. 255 Fax: (44)20-7379-0543 Mailing address: c/o CARE International in UK Tower House, 8-14 Southampton Street,London WC2E 7HA, UK http://www.sphereproject.org

19
Field Article
Lessons learnt from the 1998 Bangladesh floods
Bangladesh experienced the worst flood of thecentury between July - October 1998. Some30 million persons were affected by the crisis.
The people of Bangladesh have extraordinary copingmechanisms for dealing with floods, but the scale andduration of the 1998 flood placed these underconsiderable strain, and there were serious concernsabout the possibility of a large-scale famine.
The government and aid agencies responded in avariety of ways. Flood shelters were built; medicalcare was provided in treatment centres and by mobileteams; damaged homes were repaired; agriculturalproducts were supplied; cash for work programmeswere initiated as well as grants and interest freeloans. Food assistance was targeted at those in urgentneed and the poorest members of the community. Inthe areas where the study was carried out, pooresthouseholds were identified on the basis of incomestatements provided by each household. In otherareas where SCF and NGOs were working thepoorest were identified through discussions with thecommunity. Nutrition interventions includedsupplementary feeding for households with amalnourished child, and the provision of Vitamin Acapsules where night blindness was detected.Questions have been asked as to the effectiveness ofthe targeting and the extent to which interventionsinfluenced the nutritional status. A study of theresults of a Save the Children UK survey indicatessome answers to these questions.
The nutrition survey
Save the Children UK conducted a survey in sixseverely flood affected districts in August 1998 tolook at the nutrition situation, coping mechanismsand community priorities for suitable rehabilitation.The survey was repeated in the same areas inDecember 1998. Multiple stage cluster sampling wasdone for each round of survey following WHOguidelines (WHO 1983). Villages were selectedrandomly as Primary Sampling Units by probabilityproportionate to size. Villages were then divided intoclusters of 30-40 households and one of theseclusters was chosen randomly for sampling. A totalof 60 clusters in 6 areas were surveyed during thefirst round, and 56 clusters were surveyed during thesecond round. Children aged between 9-59 monthswere measured to assess their nutritional status; 1597children were measured during the first round and1451 in the second. The children were weighed andmeasured and their weight for age, weight for heightand height for age were calculated. In the study,wasting (weight for height) was mostly used as themost appropriate indicator for acute malnutrition, andit avoided difficulties in assessing the age of thechild. Data were analysed using statistical packageprogrammes (SPSSPC 9.0 and EPI Info 6.0).Anthropometric measurements were compared withNCHS median and z scores were calculated usingEPINUT.
In an attempt to assess the extent to which the
interventions during the flood influenced the nutritionstatus of children, a secondary analysis was carriedout on the situation of 180 children who wereincluded in both the first and second surveys. Theanalysis identified factors which influenced therecovery pattern of the children, and which mayassist in the development of policy guidelinespromoting more effective interventions.
The analysis found that while moving from crisis(flood period) to rehabilitation (post-flood) phasethere was clear evidence of a cross-over phenomenonin the recovery pattern of nutrition status. Of the 180children, 17% were acutely malnourished duringAugust whereas by December the proportion hadreduced to 12%. Although this represents animprovement of 5% in the malnutrition prevalence,the recovery pattern was not straightforward. Aninternal shift had occurred which reduced the neteffect. 90% of the malnourished children in Augustimproved by December, with 82% returning to anormal nutritional status. In contrast, half of thechildren who were well in August saw theirnutritional status worsen so that in December 9% ofthem had fallen into the malnourished category. InDecember, 14 out of 23 malnourished (64%) were“new” cases or previously normal children. We canthus observe an important cross-over phenomenon.
Implications for targeting
An interesting finding of this study was that thecriteria for targeting assistance were not alwaysappropriate especially during the rehabilitation phase.Results of the study showed that those who werepoor and in need during the flood period werehelped, and those who had a malnourished childduring the crisis were also more likely to receiveassistance. These observations fit with the statementsof agencies involved in the flood response. In arehabilitation or recovery phase, however, thesituation becomes different. The flood affected allpeople regardless of their socio-economic condition.A family that coped and survived well during theflood might have exhausted all their assets. Theywould therefore be more vulnerable in therehabilitation phase in comparison to a poorer andmore vulnerable family that was assisted during theflood by local or external agencies. People who havelost most of their assets are considered to be too greata risk for “normal” and “soft” loans and are forced tofind money at very high interest rates. A highproportion of asset loss was significantly associatedwith deterioration from normal nutritional status tomalnutrition.
This study suggested that criteria for targetingassistance should be established for both the crisisand recovery phase right at the start of any reliefprogramme to ensure that the impact of interventionsis sustained.
Another interesting observation was made regardingthe assistance and membership of NGOs. The study
This article is based on research conducted by Dr. Moazzem Hossain who was working as aProgramme Manager in Health and Nutrition of Save the Children Fund UK at the time of thestudy. Elizabeth Stevens, Policy Officer at Save the Children UK, wrote the following articlebased on the research.
From the top: This was a busy market place in Shariatpur, it took the rivera few hours to engulf. Middle Upper Arm Circumference (MUAC) measuring.It is done carefully and at the right place to ensure accuracy. Weighing ababy. Fixed places may not be always available. Alternate method includedholding the instrument by two assistants through a beam. Measuring thelength of a baby below 2 years. For children of more than 2 years height(standing) has been measured.All photographs courtesy of Save the Children UK

20
Field Article
found that although criteria for targetingassistance were used, there was a greaterproportion of NGO members among thebeneficiaries. This implies that the very poorestdid not necessarily receive assistance. Anevaluation of the DEC-funded response to thefloods also noted that NGO members might havebenefited disproportionately: “There is somecriticism that NGOs in general targeted their owngroup members disproportionately. The mostdisadvantaged members of a community may notalways have benefited from some NGOs disasterresponse.” It would appear that agencies need tobe aware of this potential problem when targetingaid.
Factors affecting recovery
A number of variables - loan burden, loss ofassets, illness, source of food - were analysed fortheir impact on nutritional status. The loanburden had a strong association with the recoverypattern. The proportion of assets lost, episodes ofdiarrhoea and source of food during the weekpreceding the survey in December were alsofound to have a significant relationship with thecross-over phenomenon.
Access to loans
Almost all people had to take some form of loanduring or after the flood. Mohajons are money-lenders who lend money at very high rates (sometimes 200% a year) at the moment of crisis. Poorpeople with minimum reserve or collateral areforced to take loans from these mohajons.Inability to pay back the money usually ends inlosing the remaining assets or else provide freelabour for any amount of days decided by themoney-lenders. A loan from a mohajon wasnegatively correlated with the progress innutritional status. On the other hand, havingaccess or ability to take loans from other sources(banks, neighbours etc.) with a long-termrepayment schedule at a very low or no interestwas positively correlated with the improvementof nutrition status. This suggests that flood-affected families need to be assisted before theyexhaust their resources and are forced to takeloans from a mohajon, or that their accessibilityto other loans should be widened.
Access to food assistance
The children of families who had access to avariety of sources of food (e.g. loan fromrelatives or donation from aid agencies) had agreater chance of improving than declining innutritional status. The survey in Decembershowed a significant association between childrendeclining to become malnourished and whetherthey had access to additional sources of food.78% of those who deteriorated to becomemalnourished depended only on their own stockfor food while only 36% in the group whichmoved from malnourished to normal did so.
Those 78% had a more limited access to foodeither through a loan from relatives or donationfrom local or external agencies.
Prevention of diarrhoea
The other factor that seemed to have someinfluence on the recovery pattern was therepeated attacks of diarrhoea. Although there wasassociation between an attack during flood(August) and deteriorating from normal tomalnutrition, it was absent when checked with anepisode of diarrhoea during December. But theassociation was stronger for those who hadrepeated episode of diarrhoea i.e., during flood(August) and post-flood period (December). Thissuggests that likelihood of deterioration fromnormal to malnutrition could be reduced if therepeated episode of diarrhoea could be preventedby taking adequate care of those who become illduring the initial flood period.
Conclusions
This study led to an observation of a cross-overphenomenon in which some children’s nutritionalstatus declined from normal to malnourished overthe period of four months. This is obviously acause for concern. Certain factors - type and sizeof loan, proportion of assets lost, episodes ofillness, and sources of food - showed anassociation with the cross-over of children fromnormal to malnourished states and the reverse.These findings have implications for the choiceof intervention made by aid agencies andgovernment.
The findings also raise the question of therelevance of targeting malnutrition during anemergency of such a large scale in whicheveryone is affected. Furthermore, it may not beappropriate to use the same criteria for targetingassistance during both the crisis and rehabilitationphases. Appropriate criteria should be establishedduring the design of the project so that the effectsof interventions are not lost in the recoveryphase.
This research was not of a longitudinal designand the numbers of subjects are small. However,the findings do merit further consideration. Itwould be useful for well-designed longitudinalstudies in flood prone areas to be undertaken, tolook at these issues more carefully and developappropriate policy recommendations.
Note: Dr Hossain would like to acknowledge thecontribution of Save the Children Fund UK who fundedthe initial surveys. He is grateful to Lola Gostelow,Emergency Advisor and Anna Taylor, Nutrition Advisor,SCF-UK, Martine Billanou, Programme Director of SCF-UKBangladesh, and to Muhammod Shuaib and Abdullah-Al-Harun of SURCH for their support and encouragement.Thanks is also extended to the children and their parentswho were affected during the flood but always co-operated during the data collection.Correspondence: Dr. Moazzem Hossain, Save the ChildrenFund, House 28, Road 16 (New), Dhanmondi R/A, Dhaka-1205, Bangladesh. Email: [email protected]
From top right: Dr. Hossain discussing with mothers at Fuluarchar; themeeting was held standing in the water as there was no dry place in thewhole island. Flooded household on the verge of collapse. A family isfloating with all its movable assets on a platform made of bamboos. Theroad on the embankment supposed to protect Naria (Shariatpur) is nowdestroyed; the neighbouring household did not last long. A child iscrossing the river on a bamboo raft.All photographs courtesy of Save the Children UK

Merlin started working in Sierra Leone in1996 in response to health and nutritionalcrises caused by the civil war and is
currently supporting programmes in both KenemaDistrict in the East of the country and in Freetown.Merlin is providing emergency health care services toboth resident and displaced populations and re-establishing essential health care services at primaryand secondary levels in both these areas.Additionally, Merlin operates a nutritionalprogramme in Kenema District, including therapeuticand supplementary feeding and implementation ofregular nutritional surveys.
GOAL commenced operations in Sierra Leone inMarch 1999 initially in the Freetown peninsular withemergency shelter and health care for InternallyDisplaced Persons and a community based approachto working with Street Children. In response to theneed for increased capacity in nutrition and healthcare, GOAL started a Supplementary FeedingProgramme in Kenema District and supportedPrimary Health Units.
Merlin and Goal have worked in close collaborationin the district since September 1999 when, inresponse to the need to increase nutritionalinterventions, Merlin decentralised its SFP andhanded over district wide management to Goal inorder to concentrate its inputs into the TFC andremaining central SFC.
Context in which the assessment wasundertaken
Sierra Leone has been in the grip of a civil war forthe past 10 years. Following the signing of the LomePeace Accord in July 1999, there have been periods
of relative stability and improving security andaccess. However the situation deteriorateddramatically in May 2000 with increased rebelactivity throughout the country and hostage taking ofUNAMSIL personnel. Following UNAMSILoperations in July large movements of people cameinto both Kenema Town (approx. 20,000) from theNorthern areas of the district and into Daru Town(approx. 7,000), in Kailahun district. Whilst most ofthese were absorbed into the host population itselfthere was an increase in number of the alreadyovercrowded internally displaced camps in KenemaDistrict.
Due to the established nutritional programme inKenema district, Merlin, GOAL and the other localand international agencies were able to respondquickly to the health and nutritional needs as a resultof the crisis. Daru, however, was more complicated.
Daru Town, is situated in Kailahun District in theEastern Province of Sierra Leone. It is an isolated,UNAMSIL controlled enclave surrounded by rebelforces. Road access from Kenema Town and itsmarkets had been intermittent. Following the Julyoperations, vehicles have been attacked by rebelforces and the road now remains closed to even localtraffic. Not only has access to markets been cut offfor the local population but also for the rebels. As aresult there have been an increasing number ofreports of harassment and looting of remaining foodstores in the surrounding villages by the rebels.
Access is currently by air only, weekly through WFP,by arrangement through the INGO helicopter orthrough UNAMSIL. Oxfam, IMC, WFP (schoolfeeding programme) and SCF are currently the onlyagencies who are operational in Daru. Their
21
Field Article
A collaborativeapproach to anutritionalcrisis in anarea accessibleonly by airBy Nicola Cadge and Lynne Russell
Nicola Cadge has a background innursing and a Masters Degree inPublic Health. Nicola has workedfor Merlin for more than twoyears both in West DRC andpresently in Sierra Leone as
Medical Co-ordinator.
Lynne Russell is a nurse who hasbeen working with GOAL sinceSeptember 1999 (her firstoverseas medical appointment).Lynne is the Medical Coordinatorfor GOAL’s projects in Kenema
and Freetown, in Sierra Leone.
SIE
RR
A L
EO
NE
- (
C)
JEN
NY
MAT
TH
EW
S,
ME
RLI
N P
HO
TO L
IBR
AR
Y

22
Field Article
This is the second in a series of piecespublished in Field Exchange* whichsummarises key sections of the newly revised
MSF nutrition guidelines for use in emergencies. Thefirst article highlighted the importance of locating thefood security situation on the continuum from foodinsecurity to famine and the implications forintervention. This second article summarises thesection of the guidelines1 which deals with choice ofnutritional interventions and programme design inrelation to severity of food crisis and other factors.
Decision tree
An overall contextual analysis is critical for guidingappropriate decisions on intervention type anddesign. Each situation requires a coherent nutritionalstrategy as well as ensuring that all target groups arecatered for by the different programmes.
Based upon the stage of the food insecuritysituation*, MSF have developed a decision treewhich helps to interpret the seriousness of a situationthrough an analysis of indicators. Quantitative andqualitative information on these indicators can thenbe used to inform decisions about nutritionalstrategies.
Although analysis of the indicators is an importantcomponent of decision-making there are otherconsiderations as well. The capacities and copingstrategies of the community must not beunderestimated or undermined by the intervention.Unnecessary feeding programmes can have anadverse impact on the community by creatingdependency and disrupting market mechanisms.
Additionally, factors such as population movements,epidemics, poor health care, inadequate watersupplies (quantity, quality), extreme temperaturesand security problems should all be taken intoaccount when deciding to implement a programmeand what form it should take.
An optimal nutritional strategy takes into accountconstraints in order to arrive at a realistic response.The constraints most commonly encountered are:limited access to the population, lack of skilledpersonnel, insufficient financial resources andinsecurity.
Revised MSFNutritionGuidelines IIBy Saskia van der Kam, MSF Holland,Senior Nutritionist
* see Field Exchange 101 The MSF nutrition guidelines are still in draft; consequentlydetails may differ from the final book
activities are greatly restricted because of thelogistical constraints and lack of access routes.Only one clinic is operational and until recentlydid not have the necessary equipment to undertakegrowth monitoring and report on nutritional status.
There are no accurate population data for DaruTown. Population estimates vary from 12, 000(7,000 resident and 5,000 IDPs) reported byUNAMSIL to 8,000 (5,000 resident and 3,000IDPs) estimated by the agencies on the ground.
The assessment
Increasing concern amongst the internationalagencies over the deteriorating food security andnutritional status of the vulnerable populations inDaru Town led WFP to request that Merlin andGOAL undertake an assessment of the nutritionalstatus of children aged 6 to 59 months. It wasclear from the outset that this would not constitutea commitment to expand MERLIN or GOALprogramme activities but was an attempt by all theagencies involved to utilise their relative expertise,skills, human resources and logistical support in acollaborative effort to gain an insight into thecurrent nutritional status of the population.Appropriate interventions would be planned incollaboration with all the key agencies involvedfollowing the assessment.
Planning the assessment was complicated. Theco-ordination was undertaken at three separatesites, Freetown, Kenema and Daru by radio.There were delays as a result of the WFPhelicopter needing servicing. There had beenclose liaison with UNAMSIL to ensure co-operation and security of the assessmentpersonnel. Two weeks after the initial request, onthe 15th August the WFP Helicopter left Freetownand collected 6 Merlin, 6 GOAL and 2 IMC stafffrom Kenema and then flew onto Daru Town,arriving at 10:00. They were accompanied by theGOAL expatriate Medical Co-ordinator. Transportwas arranged by Oxfam and sensitisation of thepopulation performed by Oxfam volunteers.
Three locations had been identified and the staffwere divided into four teams, with Oxfamvolunteers undertaking crowd control. There werestrict time constraints with time on the groundlimited to a mere 3 hours, including travel to andfrom the sites. However, a total of 590 childrenaged 6 to 59 months were screened using weightfor height indicators. Two WFP staffsimultaneously conducted a quick commodityprice survey and assessed food availability in themarket. They also visited the outskirts of the townto assess the degree of home garden production.Following analysis of the nutritional results,calculated as a percentage of the median usingNCHS/CDC/WHO sex combined reference tablesthe global malnutrition rate in the populationscreened (n = 544) was found to be 7.6%. Themoderate malnutrition rate 3.9% and the severeacute rate was 3.7%.
It is not possible to extrapolate these findings tothe general population as it was not a randomisedassessment. It is clear that the ideal would havebeen to undertake a full randomised nutritionalsurvey. However, in the absence of accurate (oreven estimated) population data this was notpossible. This was a key constraint in our abilityto obtain meaningful data and data that could beused in the planning of appropriate interventions.Additional constraints were the limited number ofplaces on the helicopter, time restrictions in DaruTown and limited logistical support once on theground which resulted in time lost waiting for
vehicles to transport the staff. The helipad was twomiles from the centre of town and it wasimpossible to carry weighing and measuringequipment on foot. Despite this, there was a highlevel of collaboration amongst a number ofagencies, which made it possible to undertake thescreening exercise.
There were a number of recommendations madebased on these results. First and foremost was theneed to secure unrestricted and safe road accessbetween Kenema and Daru Towns. This wouldincrease access to markets and food, allow theteams in to undertake a mapping exercise toestimate the population in the town and verify thenumber of IDPs and consequently undertake arandomised nutritional survey. Such a surveywould help better establish whether there was aneed for TFC and SFP interventions. However, itwas acknowledged that the only type ofinformation collection that can currently take placegiven the existing constraints are food securitymonitoring (involving commodity price tracking)and initiation of nutritional surveillance at thehealth centre.
Post-Assessment meeting and Action Plan
An inter-agency meeting (including Merlin,GOAL, WFP, UNICEF, MoH, IMC and SCF)held following the helicopter survey concludedthat due to the security and logistical constraints itwould not be possible to undertake a randomisednutritional survey. Despite the limitations of thedata obtained it was decided to initiate a SFPprogramme on the basis that malnutrition rateswere above 5% in conjunction with aggravatingfactors, e.g. poor food security, lack of access tomarkets and increased population numbers due tothe displacement. Furthermore, access to foodwas unlikely to improve in the near future. Thereis currently insufficient logistical support andhuman resources to establish a TFC in Daru Townitself or undertake a Vulnerable Group Feedingdistribution. It was therefore proposed thatseverely malnourished children could betransported to the Kenema TFC for treatment.SCF and WFP will undertake food securitymonitoring while UNICEF donated equipment tothe clinic to undertake growth monitoring. Merlinand GOAL do not have the capacity to operate inDaru Town at the present and introducing newagencies into the area would only increase thepressure on already stretched helicopter services.An agency currently operating on the ground hasthe capacity and experience to establish an SFPand is currently searching for funding. Merlin andGOAL have offered training of their staff.
The process of assessment and establishing aprogramme in Daru has been slow and laborious.Progress has been obstructed because of thenumerous constraints. Many dilemmas still needto be resolved. Yet the collaborative approach tothis situation has remained a strength. Agencieshave shared resources and experience in trying tomeet each challenge. Daru Town is by no meansthe only such enclave in Sierra Leone, there areBunbuna and Kabala also. One of the lessons tocome out of this experience was that there has tobe a high degree of detailed planning for thistype of assessment as time on the ground is solimited. Any delays can have a large opportunitycost. The experience gained here can be used toassess, plan and implement future programmes ina more efficient way - hopefully with the samelevel of collaboration between agencies on theground.
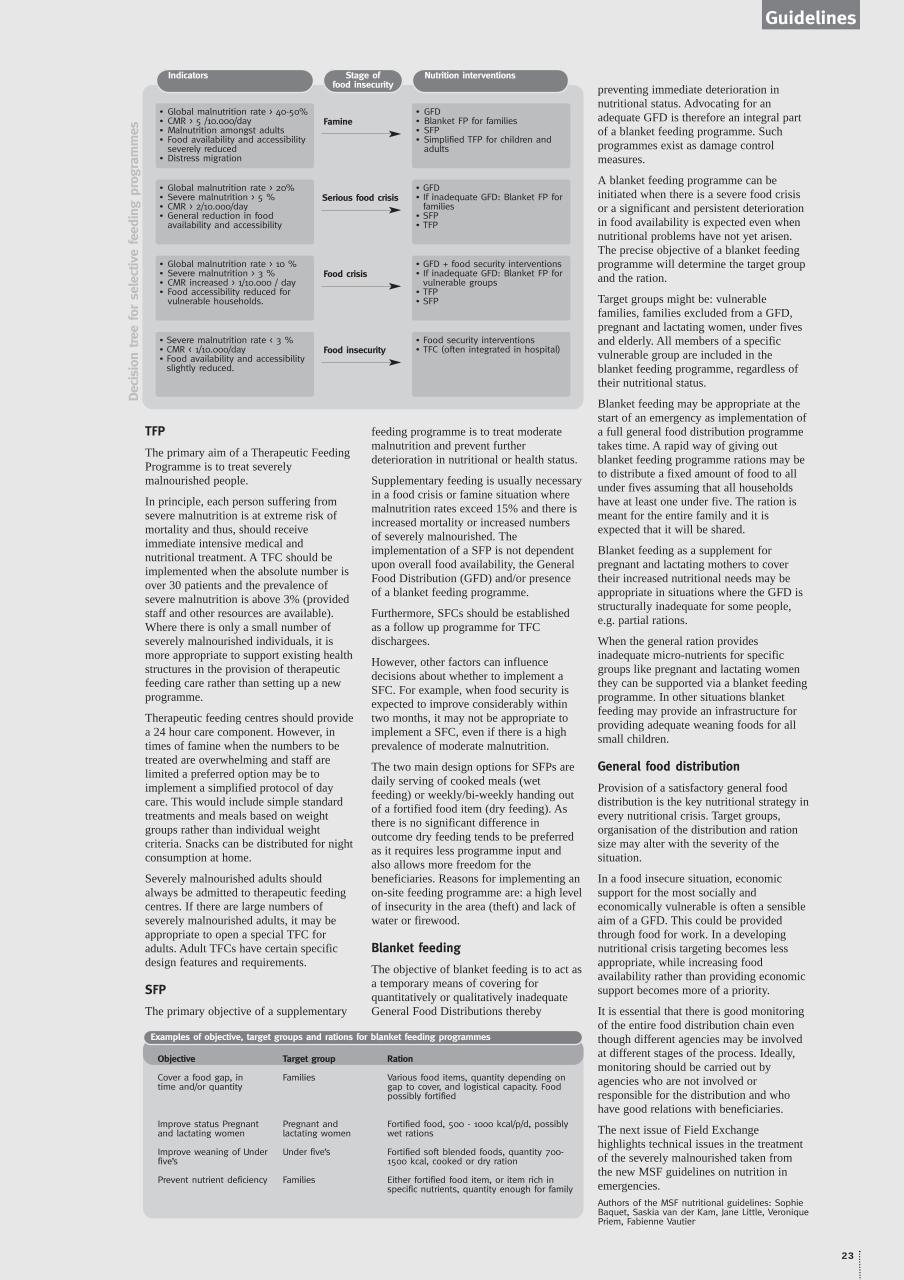
TFP
The primary aim of a Therapeutic FeedingProgramme is to treat severelymalnourished people.
In principle, each person suffering fromsevere malnutrition is at extreme risk ofmortality and thus, should receiveimmediate intensive medical andnutritional treatment. A TFC should beimplemented when the absolute number isover 30 patients and the prevalence ofsevere malnutrition is above 3% (providedstaff and other resources are available).Where there is only a small number ofseverely malnourished individuals, it ismore appropriate to support existing healthstructures in the provision of therapeuticfeeding care rather than setting up a newprogramme.
Therapeutic feeding centres should providea 24 hour care component. However, intimes of famine when the numbers to betreated are overwhelming and staff arelimited a preferred option may be toimplement a simplified protocol of daycare. This would include simple standardtreatments and meals based on weightgroups rather than individual weightcriteria. Snacks can be distributed for nightconsumption at home.
Severely malnourished adults shouldalways be admitted to therapeutic feedingcentres. If there are large numbers ofseverely malnourished adults, it may beappropriate to open a special TFC foradults. Adult TFCs have certain specificdesign features and requirements.
SFP
The primary objective of a supplementary
feeding programme is to treat moderatemalnutrition and prevent furtherdeterioration in nutritional or health status.
Supplementary feeding is usually necessaryin a food crisis or famine situation wheremalnutrition rates exceed 15% and there isincreased mortality or increased numbersof severely malnourished. Theimplementation of a SFP is not dependentupon overall food availability, the GeneralFood Distribution (GFD) and/or presenceof a blanket feeding programme.
Furthermore, SFCs should be establishedas a follow up programme for TFCdischargees.
However, other factors can influencedecisions about whether to implement aSFC. For example, when food security isexpected to improve considerably withintwo months, it may not be appropriate toimplement a SFC, even if there is a highprevalence of moderate malnutrition.
The two main design options for SFPs aredaily serving of cooked meals (wetfeeding) or weekly/bi-weekly handing outof a fortified food item (dry feeding). Asthere is no significant difference inoutcome dry feeding tends to be preferredas it requires less programme input andalso allows more freedom for thebeneficiaries. Reasons for implementing anon-site feeding programme are: a high levelof insecurity in the area (theft) and lack ofwater or firewood.
Blanket feeding
The objective of blanket feeding is to act asa temporary means of covering forquantitatively or qualitatively inadequateGeneral Food Distributions thereby
preventing immediate deterioration innutritional status. Advocating for anadequate GFD is therefore an integral partof a blanket feeding programme. Suchprogrammes exist as damage controlmeasures.
A blanket feeding programme can beinitiated when there is a severe food crisisor a significant and persistent deteriorationin food availability is expected even whennutritional problems have not yet arisen.The precise objective of a blanket feedingprogramme will determine the target groupand the ration.
Target groups might be: vulnerablefamilies, families excluded from a GFD,pregnant and lactating women, under fivesand elderly. All members of a specificvulnerable group are included in theblanket feeding programme, regardless oftheir nutritional status.
Blanket feeding may be appropriate at thestart of an emergency as implementation ofa full general food distribution programmetakes time. A rapid way of giving outblanket feeding programme rations may beto distribute a fixed amount of food to allunder fives assuming that all householdshave at least one under five. The ration ismeant for the entire family and it isexpected that it will be shared.
Blanket feeding as a supplement forpregnant and lactating mothers to covertheir increased nutritional needs may beappropriate in situations where the GFD isstructurally inadequate for some people,e.g. partial rations.
When the general ration providesinadequate micro-nutrients for specificgroups like pregnant and lactating womenthey can be supported via a blanket feedingprogramme. In other situations blanketfeeding may provide an infrastructure forproviding adequate weaning foods for allsmall children.
General food distribution
Provision of a satisfactory general fooddistribution is the key nutritional strategy inevery nutritional crisis. Target groups,organisation of the distribution and rationsize may alter with the severity of thesituation.
In a food insecure situation, economicsupport for the most socially andeconomically vulnerable is often a sensibleaim of a GFD. This could be providedthrough food for work. In a developingnutritional crisis targeting becomes lessappropriate, while increasing foodavailability rather than providing economicsupport becomes more of a priority.
It is essential that there is good monitoringof the entire food distribution chain eventhough different agencies may be involvedat different stages of the process. Ideally,monitoring should be carried out byagencies who are not involved orresponsible for the distribution and whohave good relations with beneficiaries.
The next issue of Field Exchangehighlights technical issues in the treatmentof the severely malnourished taken fromthe new MSF guidelines on nutrition inemergencies.Authors of the MSF nutritional guidelines: SophieBaquet, Saskia van der Kam, Jane Little, VeroniquePriem, Fabienne Vautier.
23
Guidelines
Indicators Stage offood insecurity
Nutrition interventions
• Global malnutrition rate > 40-50% • CMR > 5 /10.000/day• Malnutrition amongst adults• Food availability and accessibility
severely reduced• Distress migration
• GFD• Blanket FP for families • SFP• Simplified TFP for children and
adults
Famine
• Global malnutrition rate > 20%• Severe malnutrition > 5 % • CMR > 2/10.000/day• General reduction in food
availability and accessibility
• GFD• If inadequate GFD: Blanket FP for
families • SFP• TFP
Serious food crisis
• Global malnutrition rate > 10 %• Severe malnutrition > 3 %• CMR increased > 1/10.000 / day• Food accessibility reduced for
vulnerable households.
• GFD + food security interventions• If inadequate GFD: Blanket FP for
vulnerable groups• TFP• SFP
Food crisis
• Severe malnutrition rate < 3 % • CMR < 1/10.000/day• Food availability and accessibility
slightly reduced.
• Food security interventions• TFC (often integrated in hospital) Food insecurity
Dec
isio
n tree
for
sel
ectiv
e fe
edin
g p
rogra
mm
es
Examples of objective, target groups and rations for blanket feeding programmes
Objective
Cover a food gap, in time and/or quantity
Improve status Pregnantand lactating women
Improve weaning of Underfive’s
Prevent nutrient deficiency
Target group
Families
Pregnant andlactating women
Under five’s
Families
Ration
Various food items, quantity depending ongap to cover, and logistical capacity. Foodpossibly fortified
Fortified food, 500 - 1000 kcal/p/d, possiblywet rations
Fortified soft blended foods, quantity 700-1500 kcal, cooked or dry ration
Either fortified food item, or item rich inspecific nutrients, quantity enough for family

During 1998 and early 1999 the FederalRepublic of Yugoslavia (Serbian)forces increased their efforts to
‘ethnically cleanse’ Kosovo. They justified thison the basis that they were ‘cleaning out’Kosovar Liberation Army (KLA) bases. Inresponse, NATO forces launched air strikesagainst the Federal Yugoslavia Republic (FYR)in March 1999. The war between FYR andNATO forced displacement from Kosovo andprecipitated a major humanitarian emergencyinvolving the largest and fastest movement ofpeople in Europe since World War II.
The Disaster Executive Committee (DEC)launched its Kosovo appeal on 6th April 1999.This appeal raised over 50 million poundssterling, which was shared out between 12British agencies; the largest share going toOxfam (about 30% of the total raised). TheDEC subsequently commissioned anindependent evaluation1 of phase 1 and 2 ofexpenditure of the appeal funds covering theperiod from 6th April 1999 to 31st January2000.This time period covered the massiveoutflow of Albanians from Kosovo to Albania,Macedonia, Montenegro and Bosnia, theirreturn to Kosovo and the resulting outflow ofSerbs and Roma from Kosovo. The evaluationtook place between January and June 2000with the evaluation team visiting Albania,Macedonia, Kosovo, Montenegro, Bosnia-Herzegovina and Serbia. The evaluation wasmulti-sectoral. It examined preparedness andinitial response, appropriateness of response,coverage, protection, effectiveness and impact,efficiency/cost-effectiveness, connectednessand performance standards. The food andnutrition component of the DEC response wastherefore only a small component of theevaluation but nevertheless reported interestingand important findings.
Relative to the large food aid programmesimplemented by agencies such as WFP andCRS during the crisis, the DEC agencies spentvery little on food and nutrition programmes.The evaluation conclusions are, therefore, notgeneralisable to the overall food and nutritionresponse but only apply to the response ofDEC agencies. The main conclusions aboutthe provision of food and nutritional supportby DEC agencies during the crisis were asfollows:
• Only 17 percent of DEC fundswere spent on food aid inphase 1 and less than 3percent in
phase 2. It was appropriate for DEC agenciesto concentrate on areas other than food aid,(especially in phase 2 when the priorities wereto ensure security and weatherproofed shelterfor returnees to Kosovo) given thatmalnutrition was not an imminent problem,that there was a glut of food aid and that DECfunds could be used flexibly. Localcommunities also provided support toKosovars, especially in Albania, where localfamilies hosted the refugees, and mosques andrestaurants provided free meals.
Among the DEC agencies, the church agenciesspent the highest proportion of their budgetson food. This may partly reflect the churchestraditional role as a provider of food andshelter to those in need and the existence ofgrass roots networks for distribution.
• At the early stages of the emergency foodaid was given for nutritional reasons, howeverlater on in the emergency it appears to havebeen given as a supplement or short-termincome transfer. Therefore, cost-effectivenessof food aid, i.e. the cost of supplying food aidin relation to its value to the beneficiarythough an important impact indicator, was notmonitored or evaluated during the programme.
• There was very little assessment or analysisof the food situation of the refugees in theperiod March-June 1999. This meant thatdecisions on quantity and quality of foodrations were largely supply rather than needsdriven.
• UNHCR was responsible for providingguidelines on the provision of complementaryfoods additional to the basic ration. Certainprovisos were stipulated by UNHCRincluding; not distributing fresh meat, babyfoods, infant formula or chocolate. However,many NGOs did not stick to these provisosand instead designed their own complementaryfood parcels. This meant that there wasenormous variation in rations in terms of thenumber of items included, calorific values, thecost and value to the beneficiary. For example,one NGO food parcel contained 18 itemsincluding Turkish delight and chocolate.Consistency of supply is more difficult toattain with complementary food items and canlead to heightenedbeneficiary
expectations, which cannot always be met.
• High cost parcels (around £10 per parcel)containing luxury items of limited nutritionalvalue were distributed using DEC funds.Money could have been better spentelsewhere.
• The majority of DEC funded food aidprogrammes were targeted at the morevulnerable groups both in terms of the type ofbeneficiary and the countries covered.
• There were problems in targeting. Althoughthere were few reports of refugees/IDPs totallymissing out on food aid rations, there waspotential for duplication and thus wastage, i.e.families getting more than one lot ofdistributions. Duplication was not likely to bean extensive problem as food aid needs werenot great.
• Where the needy in the local population (i.e.host populations in Albania and Macedonia)were included in the distribution, incidences ofill feeling among the local population arose.These were mostly manifested through socialpressure on local partners to support onefamily rather than another or to share aidequally between all citizens.
• Poor monitoring and reporting of food aiddistribution increased the potential for a lackof uniformity in approach.
• Local purchase of food was not necessarilycheaper than international purchase. However,positive aspects of local purchase couldsometimes be speed, with less likelihood oftransport and importation delays as well assupport to the local economy.
• Well-established nutritional guidelines wereignored in some instances, e.g. failure to meetSphere minimum standards of assessment andanalysis; items included in complementaryfood rations, inclusion of milk powder inrations. This raises the issue of lack ofawareness of guidelines and the need foradequate technical support in the field,especially to local partners who may havelimited experience of emergencies.
The impact of the crisis on the food security ofhost populations in Albania and Macedoniaappears to have been minimal.1 Independent Evaluation of Expenditure of DECKosovo Appeal Funds - Phase 1 and 11, April 1999 -January 2000. Volumes 1-3. ODI in Association withVALID International: August 2000
Kosovo Evaluation
24
Evaluations
Bread distribution in Albania.(Tearfund)

25
Evaluations
Two consultants from UNICEF and WHO carriedout an assessment of the emergency response inthe Somali region of Ethiopia in August this
year.1 The objectives of the assessment were:
i) to provide an overview of the humanitarian responseto date, and
ii) to outline the major problems hindering an effectiveresponse.
The methodology for the assessment consisted first ofthe collation of various survey reports and assessmentreports of non-government organisations (NGOs), theDisaster Preparedness and Prevention Committee(DPPC) and United Nations (UN) agencies. This wasfollowed by interviews with key informants such asagency directors, medical co-ordinators andnutritionists and finally, field visits to Gode zone,Jijiga zone and Shinile zone.
The Somali region in Eastern Ethiopia comprises 9zones and has a population of approximately 3.76million, the majority of whom are pastoralists andagro-pastoralists. The area is remote and isolated fromthe highlands. Three consecutive years of poor rainfallhad adversely affected agricultural yields and thecondition of pastures. This led to a gradual depletion infood stores, livestock and other household assets andsevere deterioration in household food security. As aresult, the prevalence of acute wasting in thepopulation under 5 years of age reached critical levelsin many parts of the Somali region in early 2000 andremained of serious concern in some areas. There wasalso evidence that crude and under-5 mortality rateshad increased and passed the thresholds used to definean emergency.
Findings of the Assessment
Nutritional Surveillance
There is no formal nutritional surveillance systemcovering the Somali region. In many other regions ofEthiopia, the early warning department of the DPPC inconjunction with SCF-UK monitor the nutrition andfood security situation through the NutritionSurveillance Programme (NSP). The NSP is alongitudinal monitoring system that utilises a standardset of food security, agricultural and anthropometricindicators to track changes over time. Theanthropometric indicator that has been used by theNSP is mean weight for length (MWL) of thepopulation. A cut-off point of 90% MWL has beenused by the DPPC to define population nutritionalvulnerability and the need for external food aid. Eventhough the NSP has not been formally operating in theSomali region, the MWL indicator had been used by anumber of non-government organisations (NGOs) andby the DPPC itself as an indicator of nutritionalvulnerability. Because MWL reflects the populationmean and not the proportion of children falling belowinternationally recognised cut-offs for the definition ofwasting, the MWL alone is an inadequate indicator ofnutritional vulnerability in an emergency situation.
In addition to the MWL and standard anthropometricindicators such as weight for height Z-score andpercentage of the median, other anthropometricindicators used in the region include Mid Upper ArmCircumference (MUAC) and MUAC for height(QUACK stick). The different indicators used madecomparison from zone to zone or region to regiondifficult and international comparisons or longitudinalmonitoring over time virtually impossible.
Sampling methods for nutritional surveys had alsovaried considerably; the minority of surveys had beenformal 30 clusters surveys employing the standard EPImethodology. Rapid assessments usually reportingMUAC, results from the screening of beneficiaries ofsupplementary feeding programmes, or conveniencesamples of children less than 5 years of age measured
at a central village location were frequently employed.Survey methods that do not employ random samplingare prone to selection bias and the interpretation ofresults is extremely problematic.
The majority of anthropometric information had beencollected by NGOs operating in the southern zones ofthe Somali region.
Few surveys attempted to identify underlying causes ofmalnutrition. There was however, evidence suggestingthat high morbidity due to diarrhoeal disease,exacerbated by unusual population concentrations andpoor water and sanitation conditions, had negativelyimpacted on the overall nutrition situation.
Selective Feeding Programmes
In response to the high prevalence of malnutrition,international and national NGOs commenced selectivefeeding programmes throughout the Somali regionfrom April to July 2000. The coverage and type ofprogrammes varied widely within and between zones.Disparity in coverage can be partly attributed tosecurity constraints and partly to differences inpopulation size between these zones. However, giventhat malnutrition prevalence rates in all five zones hadbeen extremely high, it appears that Gode zone andGode woreda in particular were over-targeted whileother zones were relatively under-served.
In the absence of current guidelines from DPPC or theMOH for therapeutic feeding and insufficientinstitutional support, NGOs used their own criteria andguidelines. Not surprisingly the quality of careprovided by less experienced NGOs did not alwaysmeet minimum standards; some of the problemsobserved in TFCs included:
• Admission criteria were variable and ofteninconsistent (for example, MUAC and weight forheight criteria were intermingled, children wereadmitted who had another illness such astuberculosis but were not severely malnourishedetc.).
• Routine medical treatment was sometimesinadequate and not in line with standard protocols inrespect of measles vaccination, micronutrientsupplementation, treatment of intestinal parasitosis,systematic treatment of infections with oralantibiotics.
• Feeding protocols varied and types of food providedwere frequently not in line with Sphere/WHOrecommendations. Of particular concern was themisuse of BP-5 biscuits which have aninappropriately high protein content for the earlyphases of therapeutic feeding and should not begiven as a take-home ration overnight because of thehigh probability of them being shared or sold.
Supplementary Feeding Programmes (SFPs) were alsodisproportionately represented in Gode zone,particularly Gode woreda, when compared with otherzones. Again in the absence of guidelines andcoordination, admission and discharge criteria andtarget groups varied widely. In addition, althoughlevels of global malnutrition and the inadequateGeneral Food Ration (GFR) would have justified (atleast temporarily) blanket distribution of drysupplementary feeding to all children less than fiveyears of age and pregnant and lactating women inmany zones. Only two agencies engaged in suchprogrammes. Problems with the supplementaryfeeding programmes included the following:
• Provision of health care (routine immunisation, ORT,vitamin A supplementation) did not always meetminimum standards.
• In Gode in particular, catchment areas of SFPoverlapped and because distributions were not on thesame days, an unknown but perhaps substantialnumber of beneficiaries registered in more than onefeeding programme.
Food Security
Many assessments addressing differing facets of foodsecurity had been carried out since the first reports ofthe deteriorating situation in the Somali region.However, because the Somali region is not covered bythe NSP there is a lack of base-line food security datathat makes this information difficult to interpret.
NGOs included aspects of food security in nutritionsurveys but this information could not substitute for acomprehensive food security monitoring system in aregion where geographic variability is so pronounced.
General Food Distribution
A variety of constraints resulted in an uneven andsometimes insufficient distribution. Verification wasdifficult in the absence of accurate statistics onpopulations (and movements) or on food allocationsand distribution. A system of post distributionmonitoring at the distribution point and/or householdlevel had not been implemented.
Initially, the zonal DPPC used official populationstatistics to identify affected numbers and eligiblebeneficiaries. Although in theory certain groups didnot qualify for food distribution, in practice food wasdistributed to all people counted on the day before adistribution.
New food allocations were based on head-counts fromprevious distributions. As populations were attracted toareas with a reliable GFR, the amount of foodallocated did not always match the eligible number ofbeneficiaries present during the new round ofdistribution.
Reliable figures on the amount of food distributedwere difficult to obtain. Due to a complicated andfragmented information system with most data onlyavailable at the central levels of DPPC and WFP,allocation, dispatch and distribution figures could onlybe compared months after actual distribution tookplace. Furthermore, WFP and implementing partner onsite monitoring during head-counts and distributionswas extremely limited due to security restrictions,insufficient (air) transport and insufficient logistic orhuman resource capacity. Also, despite attempts toimprove information sharing and co-ordination, neitherDPPC/B nor WFP managed to incorporate in itsdistribution figures, food distributed by otherorganisations.
Summary Problem Analysis
The overall problems with the humanitarian responsein the Somali region relate to the lack of acomprehensive surveillance system and the lack of asuitable coordination mechanism and therefore thelack of an integrated response. The DPPC/B whosemandate was to co-ordinate the response lackedsufficient technical and human resource capacity tofulfil this role.
While some therapeutic and supplementary feedingprogrammes are of excellent quality, many also do notmeet minimum standards. The fact that the quality ofthese programmes remains poor reflects the overalllack of nutrition co-ordination and monitoring.
The lack of a comprehensive nutrition surveillancesystem has resulted in a failure in targeting of food aidto the most vulnerable geographic areas and adjustingpriorities according to needs. It has allowed some areassuch as Gode to attract a relative surplus of food items,selective feeding programmes and support in the healthsector, while other areas such as Shinile and Jijigazones have remained with grossly inadequateassistance in these sectors and an ongoing nutritionalemergency.
Finally, a major problem in assessing the foodsituation has been the absence of accurate statistics onpopulations (including the displaced) and fooddistributions. 1 Peter Salama, UNICEF/ IEHRB(CDC) , Albertien van der Veen,WHO/ORHC, Report on the Food and Nutrition Situation inGode, Fik, Korahe, Jijiga and Shinile zones of the,SomaliRegion, Ethiopia, August 11, 2000
Somali Region EthiopiaSummary of situation report

26
Field Article
Update on the current situation
The last edition of Field Exchange included anaccount of discussions on how food aid should betargeted in the siege town of Huambo situated in thePlan Alto region of Angola1. The article illustratedthat 6 months of discussions took place beforeconsensus could be reached that there were noadvantages to targeting food aid as the entirepopulation experienced a very similar degree of foodinsecurity. Between November 1999 and May 2000 full monthlyrations were given four times in a general distribution(excluding only those living in the concrete city) inthe areas covered by WFP. ICRC allocated moreregular half rations in their areas of responsibility. InMay the ration stopped following a WFP/FAO Cropassessment which concluded that the recent harvestwould meet the peoples’ food need for two months.ICRC continued however to distribute seed and foodfor seed protection.
In May 2000 malnutrition rates reached their lowestlevels since the fighting resumed in December 1998(see graph) but were still high (10% global, 4%severe) relative to baseline levels (global 4%). Thereduced levels of malnutrition are likely to be aconsequence of high quantities of relief fooddistributed in the preceding period and themaintenance of a low price of maize (in real terms).Low prices were probably due to the food aid and theincrease in the amount of trade taking place betweenthe city and its broader hinterland.
Future prospects - Food aid policy
In June 2000, WFP published a strategy paper2 fordistribution of relief food in Angola. The strategy
states “Now is an appropriate transition time for WFPto replace large scale free food distributions with amore targeted approach, based on strict registrationcriteria and self targeted safety nets.”
The recommended beneficiary groups were asfollows:
1. Current WFP case load to continue to receive afree food ration until May 2001.
2. From May 2001:• Newly displaced (travelling more than 50kmfrom their home) will receive a full ration for 3months and if they become involved in anagricultural programme will be eligible for a fullration for 18 months and a half ration for a further6-12 months.• Malnourished children and adults will be eligible(as under the current system) for supplementary(for moderately malnourished) or therapeutic (forseverely malnourished) feeding until they havereached recovery criteria.• Families of individuals registered for therapeuticor supplementary feeding will be eligible for a halffamily ration for 3 months.• Children under five at risk of moderatemalnutrition (low MUAC) will be eligible toreceive a meal from a communal kitchen for 6weeks.• Returnees / Resettlers will be eligible for a fullration for 8 months and a half ration for a further12 months.• School children will receive a meal at school incommunities at risk of malnutrition.• Food for work for certain beneficiaries.
While the strategy paper clearly states that thetargeting will not begin until May 2001, there areindications that these strategies are already beingimplemented. In Casseque 3, the only IDP camp inHuambo and which accommodates many of the mostrecently displaced the general ration was stopped,rations were targeted to specific vulnerable groups,and food for work implemented. It is unclear whetherWFP are being forced to revert to targeting byreduced donor commitments and resulting scarcity offood aid resources or whether the strategy is basedupon some other rationale.
Potential consequences for the emergencyaffected population
Huambo is a city with an estimated 250,000 peopleliving in the biarros. In order to feed itself over thenext four months (until February when the nextharvest begins) the population will needapproximately 17,000MT maize3. There are a limited number of sources of maize inHuambo:
1. Maize grown within the city itself. An assessmentconducted by Save the Children in August indicatedthat maize produced by households with access toland (and therefore not including any of the
displaced) amounted to approximately 5% of theirannual food needs.2. Maize brought into the city through trade. Inrecent months, security has allowed maize from thecountryside to be traded in the city. This supply mayhowever start to decline as the rains are about tobegin and security often deteriorates in the wetseason.3. Maize brought into the city by the humanitariancommunity. ICRC intend to continue to distributefood over the coming months. WFP however, whosefood distribution has covered the greater part of thecity in the past appear to be on the verge of changingover to a safety net targeted general ration asoutlined above.
If 17,000MT maize does not come into the city fromthese sources over the next four months, theconsequences for nutritional status are likely to besevere and cases of malnutrition are likely to increasedramatically.4 An estimated 80% of householdswould not be able to meet food needs if there were asmall increase in the price of maize because they relyalmost entirely on purchasing their food. If the WFP strategy is implemented as outlinedabove then it is possible that a situation will bereached whereby the population has to wait tobecome malnourished or at clinical risk ofmalnutrition before they receive food assistancethrough the targeted supplementary feeding centres.
Emergency preparedness in nutritionprogramming
SCF are closely monitoring the following:
1. Nutritional status. - through nutritional surveys. 2. Admission rates in feeding centres.3. Readmission rates in feeding centres. 4. Duration of stay and weight gain of registered
children 5. Proportion of admissions over five years of age
Conclusions
The prospects in the short term for the population ofHuambo are bleak. Lack of donor commitment andinappropriate strategies risk placing the lives of manyin jeopardy. The international community will beforced to respond when malnutrition rates reachextreme levels, but seem reluctant to act to preventthis occurring. The immediate restoration of thegeneral food distribution appears to be the onlypractical way of supplying the city with adequatequantities of food in the time frame required.
1 Gostelow, L., Reflections on food and nutrition interventionsin Huambo. Field exchange July 2000 Issue 102 Report of the mission to review distribution strategies inAngola. Conclusions and Recommendations. June 2000.3 Based on needing an average of 0.5kg maize per day4 The best available estimate of the quantity of food requiredfrom the humanitarian community for the period October2000 - March 2001 is that provided in 1999/ 2000. The relieffood supplied in that period (9,000 -10,000 tons) wassufficient to hold prices roughly constant.
Huambo: animpending disaster?By Anna Taylor SCF-UK
0
5
10
15
20
oedema
severe (<-3 z score or oedema)
global (<-2z score or oedema)
May-00Nov-99May-99Jan-99
Trends in malnutrition - Huambo
% P
reva
lenc
e m
alnu
trtio
n
IRN
AS
TR
APA
S,
HU
AM
BO

27
The Emergency Nutrition Network (ENN) grew outof a series of inter-agency meetings focusing on food andnutritional aspects of emergencies. The meetings were hostedby UNHCR and attended by a number of UN agencies, NGOs,donors and academics. The Network is the result of a sharedcommitment to improve knowledge, stimulate learning andprovide vital support and encouragement to food and nutri-tion workers involved in emergencies. The ENN officiallybegan operations in November 1996 and has widespread sup-port from UN agencies, NGOs, and donor governments. Thenetwork aims to improve emergency food and nutrition pro-gramme effectiveness by:
• providing a forum for the exchange of field level experi-ences
• strengthening humanitarian agency institutional memory • keeping field staff up to date with current research and
evaluation findings• helping to identify subjects in the emergency food and
nutrition sector which need more research
The main output of the ENN is a quarterly newsletter, FieldExchange, which is devoted primarily to publishing field levelarticles and current research and evaluation findings relevantto the emergency food and nutrition sector.
The main target audience of the Newsletter are food andnutrition workers involved in emergencies and those research-ing this area. The reporting and exchange of field level expe-riences is central to ENN activities.
The ENN is located in the Department of Community Healthand General Practice, Trinity College, Dublin, Ireland.
The TeamFiona O’Reilly is the ENN Co–ordinator, and FieldExchange co–editor. Fiona has been involved inthe area of nutrition, health and development forthe past 10 years, half of which has been spentworking in emergency situations.
Jeremy Shoham is co–editor for Field Exchangeand the ENN technical consultant. Jeremy hasbeen working in the area of emergency food andnutrition for the past 15 years.
Kornelius Elstner works part time with the ENN.
The Backpage
Field Exchange
UNHCR
The
supported by:
GENEVA FOUNDATIONto protect health in war
EditorsFiona O’ReillyJeremy Shoham
Layout & WebsiteKornelius Elstner
Contributors for this issueNicola CadgeSaskia van der KamJean GladwinLola GostelowStephanie MaxwellLynne RussellAnna ShottonElizabeth StevensAnna TaylorSean Lowrie
Thanks for the Photographs to:Jean GladwinMerlinOxfam IrelandOxfam UKPieternella PieterseSave the Children UKAnna ShottonAnna TaylorTearfundUNICEF
On the coverResidents of Mutete developingterraces to grow crops, such aspotatoes, that can be consumed andsold in nearby makets. Rwanda,courtesy of Oxfam Ireland.
As always thanks for the Cartoon to:Jon Berkeley, who can be contactedthrough www.holytrousers.com
Special thanks to Professor JohnKevany, Jean Long and Deirdre Handyfrom Trinity College for assistance andsupport for the ENN.
Pandamonium by Jon Berkeley

Emergency Nutrition NetworkDepartment of Community Health & General PracticeUnit 2.5, Trinity Enterprise Centre,Pearse Street, Dublin 2, Ireland
Tel: +353 1 675 2390 / 843 5328Fax: +353 1 675 2391e–mail: [email protected]/enn