
emergency in neurology in neurology.pdf · Emergency in Neurology • Emergency condition at ER...
13
1 Emergency in Neurology: Lesson from Experience Somsak Tiamkao http://epilepsy.kku.ac.th (my) How we learn ? • 10% of what we read • 30% of what we see • 50% of what we do • 70% of what we do,see and read • • Evidence base medicine • Emergency in Neurological Disease emergency ? Emergency ? case emergency? Emergency ? Emergency Emergency / Emergency Emergency interest (Dr.)
Transcript of emergency in neurology in neurology.pdf · Emergency in Neurology • Emergency condition at ER...

1
Emergency in Neurology:Lesson from Experience
Somsak Tiamkao
http://epilepsy.kku.ac.th
(my)
���������� ������������
How we learn ?
• 10% of what we read
• 30% of what we see
• 50% of what we do
• 70% of what we do,see and read
�����������• ������������ �������
• Evidence base medicine
• ������� ����
Emergency in Neurological Disease
� ��������� emergency �����?
� Emergency ����������?
� ��� case !"� emergency?
Emergency ?
� Emergency #�$%
� Emergency &������&'���()'!*��/,�&$
� Emergency &��-.���/0&12
� Emergency interest (Dr.)

2
Topic : true emergency � Stroke � Alteration of consciousness � Severe headache� Seizures � Motor weakness� Respiratory failure
Emergency in Neurology
• Emergency condition at ER
• Emergency condition at Ward
• Emergency investigation : CT-brain
��������������������/���� ������������� �!��"�#��� ���������"�� ���$%��& '!$���� '���(�(���) � ��� ?????
Emergency condition : ER
• Coma, alteration of consciousness
• Motor weakness
• Seizures
• Respiratory failure
• Vertigo
• Severe headache
Emergency condition: Ward
•Delirium
•Deterioration of stroke
•Status epilepticus
•Brain herniation
Emergency condition at ward
Status epilepticus
• ������������ ��� ��� ���!�!��"� 5 !�$�
• ���������� ����"�!$���%"�&'�(�)*���� imaging
• Valium 10 mg iv ���*�"�)+�����,-�*������!.���� ,�
• Dilantin 15-20 mg/kg, ������/�*�"���!50 mg/min (�,-�*�� 1 �� ,�)
• Phenobarbital 20 mg/kg, can repeat every seizures
• �)"��3����)� maintenance, TDM ,IV form
• Subtle SE/non-convulsive SE

3
Brain herniation
• Central herniation
• Uncal herniation
• On ET-tube, hyperventilation 24 hr
• Osmotic agent
• CT-brain ��%����+
• Early detection
Brain herniation
• Central herniation
• Uncal herniation
• On ET-tube, hyperventilation 24 hr
• Osmotic agent
• CT-brain ��%����+
• Early detection
Deterioration of stroke
• Intracranial cause•Recurrent, progressive
•Brain edema
•Hemorrhagic infarction
•Obstructive hydrocephalus
• Metabolic cause
• Drugs

4
Delirium• Delirium is an acute, fluctuating transient disorder of consciousness and cognition with disorientation and memory impairment
• May be caused by a general medical condition, substances and/or multiples of both
• Also known as acute confusion, acute brain syndrome, metabolic encephalopathy, toxic psychosis and acute brain failure
Clinical features
• Disturbance of consciousness
• reduced ability to focus, sustain or shift attention
• Cognitive impairment• memory deficits, disorientation (for time, place and person),
language disturbances
• Perceptual disturbances
• misinterpretations, illusions and hallucinations (usually visual)
• Disturbance in sleep-wake cycle
• Altered psychomotor activity
• increased or decreased
• Disorganized thinking with incoherence and
delusions
Etiology
• Organic aetiology identified in 95%
• D I M T O P
• Multifactorial in origin•Organic factors
•Psychosocial stressors
•Unfamiliar surroundings
•Excessive or diminished sensory input
D I M T O P• D-Drugs
• Sedatives, hypnotics, hypoglycaemics, steroids, antihypertensives, alcohol, heavy metal and toxins
• I-Infection• UTI, bronchopneumonia
• M-Metabolic• Uraemia, hypo/hyperglycaemia, dehydration
• T-Trauma / Toxins• Head injury, post-operative, subdural haematoma
• O-Oxygen deficits• Cardiac and respiratory conditions
• P-Psychological/perceptual or post-ictal
Treatment• Specific measures
• Identify and treat the underlying condition
• Thorough medical history, physical and neurological examination, lab tests
• General measures• Ensure sleep
•Maintain fluid and nutritional state
• Provide support and nursing care
• Rest in a quiet, well-lit
• Maintain orientation
• Sedate the agitated, fearful patient
5
Severe headache at ER : organic cause
� SAH
� CNS infection
� Cerebellar hemorrhage
� SDH, ICH
� Vertigo
Emergency condition at ER
Severe headache• �� ,����, �+!���$��%+��! ����: SAH
• *��, ��� �, ����/�: meningitis
•Anticoagulant : hemorrhage
• %'���)+ : subdural hematoma
• �����.� :cluster, post-coital
•Weakness : ICH
Severe headache : ����� !�"�#��$ � Vital signs, BP, ��' � Eye ground � Visual field � Stiff neck � Motor weakness � Ocular movement, pupil � Long tract signs
Severe headache : CT-brain
� HIV patient � Heavy alcohol � Liver/renal failure � �S'�� anticoagulant � Neuro deficit � Severe injury
Severe headache: LP
� �$�$#U1�
� CNS infection� SAH �/0 CT-brain ��'(XXY

6
Respiratory failure
• Ventilatory failure
• Pa CO2 ���%'������ 40
• ��� ET-tube with respirator
• %����+�� �•NMJ
•Brain stem
•Brain herniation
Vertigo• Peripheral/central
• Neuro - defict• Cerebellar
– FTN nose to nose
– Heel – to - knee
• Nystagmus
• �3�!�
• Hearing,
• Risk factors(atherosclerosis)
• Symptomatic
• Imaging, CT, MRI-brain
Seizures
•First seizure
•Underlying epilepsy
• ����'����3,����!
• �)+� �/SE
• ��%����+
•Imaging, emergency?
Seizures � Acute seizures
� Cluster of seizures
� Status epilepticus ZGTC SE
ZNCSE
Acute seizures � ���\S1�]X'�^��� ER ^����X1�#�S1�_2`�
Z ���S1���12]��
Z !"�a��X�S1�
� S1�&12]&bY'�� ��.c ER �d�1S1�Z �1�e�]YY SE

7
���� ���$�� ER• *�"�-��8!�����%" ET tube $+���)
• *�"�-��8!������� valium $+���)
• *�"�-��8!���� load dilantin IV $+���)
• ��� �������) � �� ,� SE
Cluster of seizures
� S1��X����12&$\% �1�
� �1�e�]YY SE
Status epilepticus � �/Y��'�� ^�0���\S1���'�\' �d��/0-�\� Valium 10 mg ivx2 ��12��� 10 ���/� Phenytoin loading � Pb loading � !�� �$��������#��'\/� ��b#`� !"�&'�-b ET-tube ������� ����1�e���'�/Y !j\��1-��1��/
���&��# X�\�10��!
� CBC, BUN, Cr, electrolyte, Ca, Mg, PO4, LFT
� X��-b !"�Y����
� 98% !�&$
Motor weakness• Hemiparesis
•Brain
• Para, quadri•Spinal cord
•LMN
• Stroke, MG, GBS
• Investigation
Stroke ()'!*��--1� stroke q���� 72 S�.
Other diagnosis
�1��b&��# CT-brain &��# CT-brain ]X'�
Cerebral infarction
Cerebral infarction
ICH
!�c�e�s1X�����
Proper management Admission
Med

8
Stroke � ()'!*�����������&'&��# CT-brain �1��/
� .'���b�\'&��# CT-brain ��'�̀� SSS
� Admit ������.'��/ &/�
� Close observation
� Control blood sugar: BP
Antiplatelet
� ()'!*�� cerebral thrombosis
� ASA ���\ 160 ��. �c2��!
� ��b&'�X1� hemorrhagic infarction
� Antiplatelet S�$\�0��1��b�/���sc�e��� acute stroke
Anticoagulant � ()'!*�� cardiogenic cerebral embolism
� AF valvular heart disease
� S10�2`���1�����b��'\//�' -/�
� �'\/��!v�1� recurrent stroke
� �' -/��� hemorrhagic infarction
���. /.01. �12345678�
� SBP 220 ��.!��
� DBP 120 ��.!��
� �� �'� AMI, CHF, hypertensive encephalopathy, other
Coma
• Intracranial causes
• Extracranial causes
• Neuro - deficit?
• � �����3,����! ABC
• �����)��$ ,� 2 %����+
• CT-brain �!��:�$��*�"� �!���"��� intracranial?
Alteration of conscious
� �Y���!���1&$a��!��#`�&1� Z Liver/renal failure, DM, epilepsy
� !���1&$����S'-�� -^&$\, �� (anticoagulant) � \)�b��/a��-����S'-��^$e� Heavy alcohol/alcoholic dependent?� Head injury � Sepsis

9
Management
• Essential history
• Physical examination
• Pupil size and react to light
• Ocular movement
• Nystagmus
• Eye ground
• Spontaneous movement
• Long tract signs
Alteration of conscious � &��#\)�b��/ neuro deficit? � \)��� �X�0���� ]����� \) pupil size, react tolight? � \) ocular movement � \) BBK, clonus� \) stiff neck
Alteration of conscious : CT-brain
� Liver/renal failure
� HIV patient
� Anticoagulant, PT prolong
� Neurological deficit
� Metabolic causes ��bx$Y��
Alteration of conscious : LP
� Meningitis, encephalitis
� Septic encephalopathy
� ��b#̀� !"�&' CT-brain �b�������
Alteration of conscious : EEG
� Non-convulsive status epilepticus: NCSE
� !���1&$a��X�S1�
� �/!���1&$S1��`����b��/0#���\-&$��12�/2
� \)&��b��/ nystagmus, tonic deviation?
CT-brain : emergency
• Stroke
• Seizures
• Meningitis
• Encephalitis
• Coma
• Severe headache
• Alteration of consciousness

10
CT-brain in stroke
• $-�$+���)�! acute stroke
• Siriraj Stroke Score
• $-�$+���)�!��:�*�"� �!���"��8! stroke?
• &'�(�)*�� anticoagulant ������ new neurodeficit, ��� ����
• *�"�-��8!����;�� contrast $+���)
• ������ impression/where is lesion
CT-brain in seizures presenting at ER• Status epilepticus �� ��������+�*������
• Seizures with head injury
• Seizures $��%�% )��� encephalitis
• Seizures in HIV , CRF, liver patients
• Seizures �!&'�%'���)+���� post-ictal paralysis
CT-brain in encephalitis
• $-�$+���)�"�! LP
• �<3���'���������� LP
• �<3�������!��; )�)�=���3�!�
• �<3�����%����+��� encephalitis
•JE
•HSE
CT-brain in meningitis
• *�"�-��8!����$-�$+���)�"�! LP
• ���$-��! renal, liver failure
• ����$-��! HIV, anticoagulant, neuro deficit, conscious seizures within 1 week
CT-brain in Severe Headache
• Sudden severe headache
• Neck stiffness without fever
• Severe headache with alteration of
conscious, seizures
• Severe headache with neuro-deficit
CT-brain in Coma/Alteration of conscious
• *�"*���� ���!" �
• Acute onset, neuro-deficit
• HIV,anticoagulant,renal,liver failure
• ��%����+��� metabolic *�"<�
• ����� LP?
11
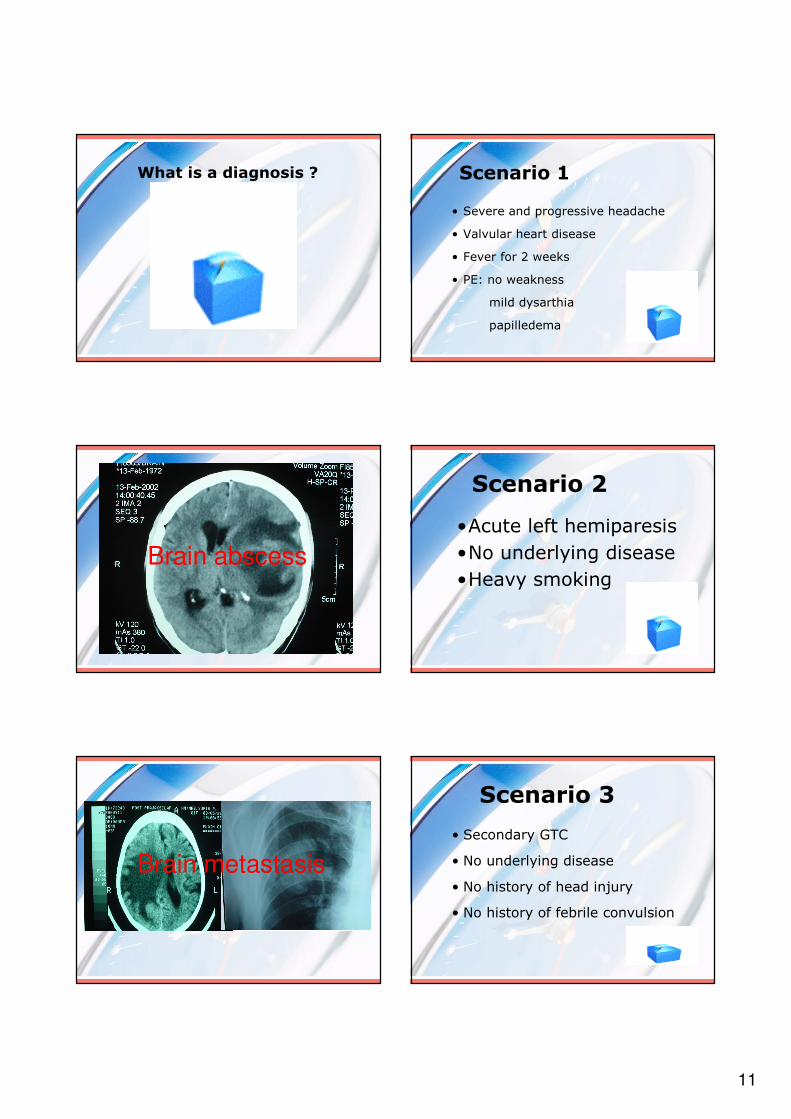
What is a diagnosis ? Scenario 1
• Severe and progressive headache
• Valvular heart disease
• Fever for 2 weeks
• PE: no weakness
mild dysarthia
papilledema
Brain abscess
Scenario 2
•Acute left hemiparesis
•No underlying disease
•Heavy smoking
Brain metastasis
• Secondary GTC
• No underlying disease
• No history of head injury
• No history of febrile convulsion
Scenario 3

12
Meningioma
• Young lady
• Acute left hemiparesis
• Previous history of blurred vision
• History of intractable hiccup
Scenario 4
Multiple sclerosis•First seizure
•Post partum
•Swelling of left leg
Scenario 5
Venous sinus thrombosis
•Progressive paraparesis
•Difficult to void
•Frequent blood transfusion
Scenario 6

13
Thalassemia
:�0;
1. ���&'�$\.cq����/0���]���'�b� -�
2. &'��'�����-b�#!y,���()'!*��
3. Y1��c�!���1&$]X�����1�e���'\/ ����-��1Y �&����{|
4. .'���b�10��#����/�`�.������/Y!�c�e���b���/0 �/0���'�1��/
Thank you for your interest


















