
Emergency in neurology
90
Emergency in Neurology Narongrit Kasemsap, MD Neurology unit, Internal Medicine Department, Khonkaen University
-
Upload
narongrit-kasemsap -
Category
Health & Medicine
-
view
1.397 -
download
0
Transcript of Emergency in neurology
Emergency in Neurology
Narongrit Kasemsap, MD Neurology unit, Internal Medicine Department,
Khonkaen University
Objectives
Localization Patient with Coma.
Evaluation and Management TIA and Ischemic Stroke Patient.
Management Patient with Status Epilepticus.
Approach to Patient with Coma
Consciousness
Awareness (content of consciousness)
Arousal (level of consciousness )
“ State of awareness of self and the environment ”
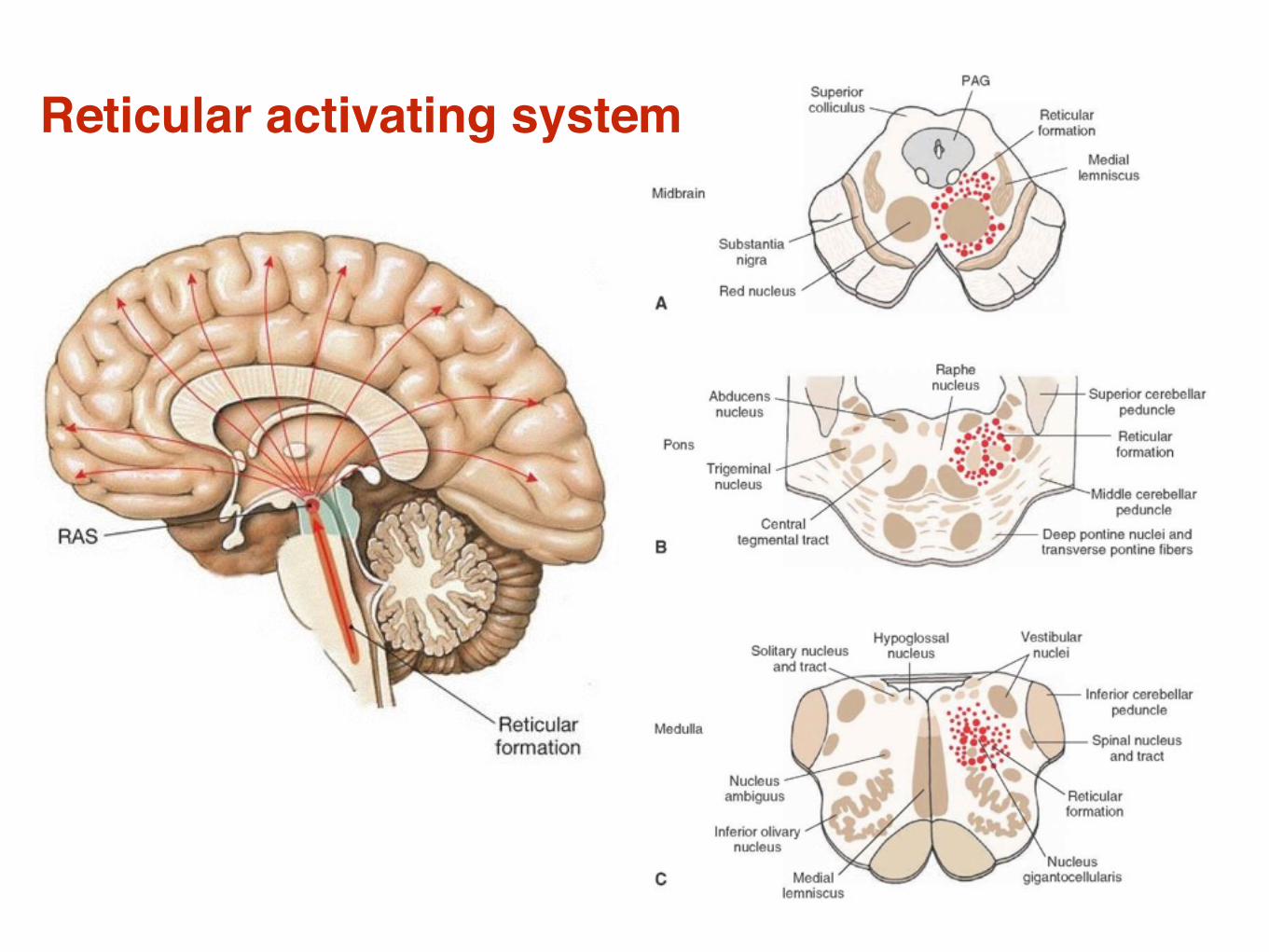
Reticular activating system
Neuroanatomical Basis of Coma
Diffuse
Extensive bilateral hemisphere
Bilateral thalamic lesion
Hypothalamus
Categorized Coma Coma without focal signs or meningism
Anoxic-ischemic, metabolic, toxic, drug-induced, infection, post-ictal state
Coma with meningism
SAH, meningitis, meningoencephalitis
Coma with focal signs
Intracranial hemorrhage, infarction, tumour, abscess

Multifocal Lesion Mimic toxic or metabolic causes
Venous sinus thrombosis
Bilateral subdural hematoma
Vasculitis
Meningitis

Causes of Alteration of Conscious
Structural causes
Metabolic causes
Assesment History
General examination
Neurological examination
Where is the lesion ?
What is the nature ?
History Difficult and sometime impossible.
Patient past health and illness.
seizure, diabetes, hypertension
substance abuse
depression, suicide attempts
etc..
Current medication.

Physical Examination General examination
General Neurological examination
Level of consciousness
Motor function
Brain stem function
Respiratory pattern
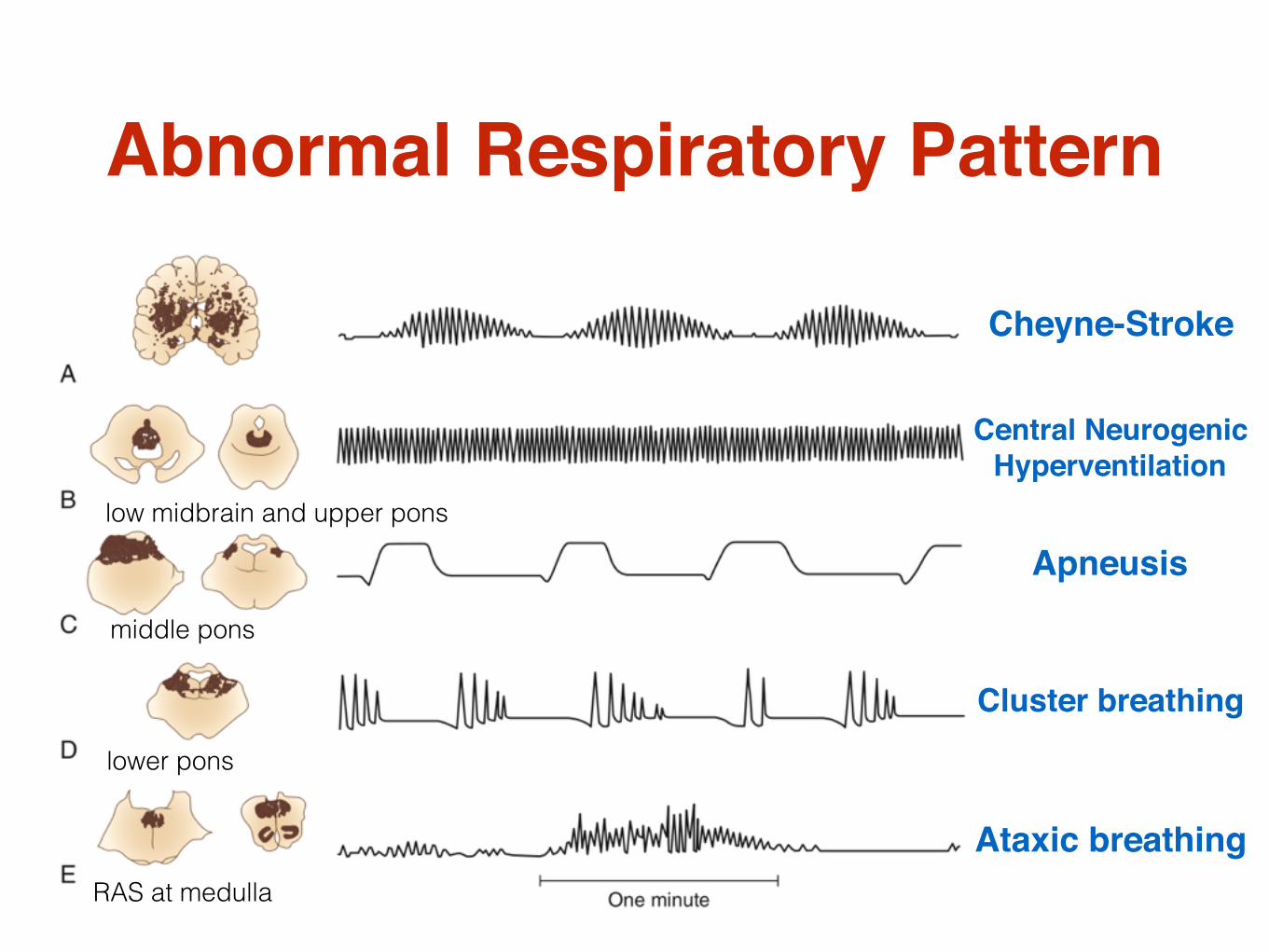
Abnormal Respiratory Pattern
Cheyne-Stroke
Central NeurogenicHyperventilation
Apneusis
Ataxic breathing
Cluster breathing
lower pons
middle pons
low midbrain and upper pons
RAS at medulla

Pupillary Finding in Comatose
Lesions above the thalamus and below the pons preserve pupillary reactions
Ocular motility Resting position.
Spontaneous eye movements.
If blinking is present : intact pontine reticular formation.
Bell’s phenomenon : intact pons and midbrain.
Reflex eye movements.
Eye deviation
Disconjugate eye movement : CN III, CN VI, brainstem lesion.
Upward deviation : poor localising value
Downward deviation : poor localising value
Skew deviation : posterior fossa lesion

Disconjugate eye
CN IIICN VI
Brainstem
Spontaneous Eye Movement
Purposeful eye movements : locked-in syndrome, catatonia, and pseudo-coma.
Roving eye movements : toxic, metabolic, bilateral hemisphere.
Contralateral conjugate eye deviation : epilepsy.

Normal / Metabolic encephalopathy
Bilateral CN VI palsy
Oculocephalic (Doll’s eye)
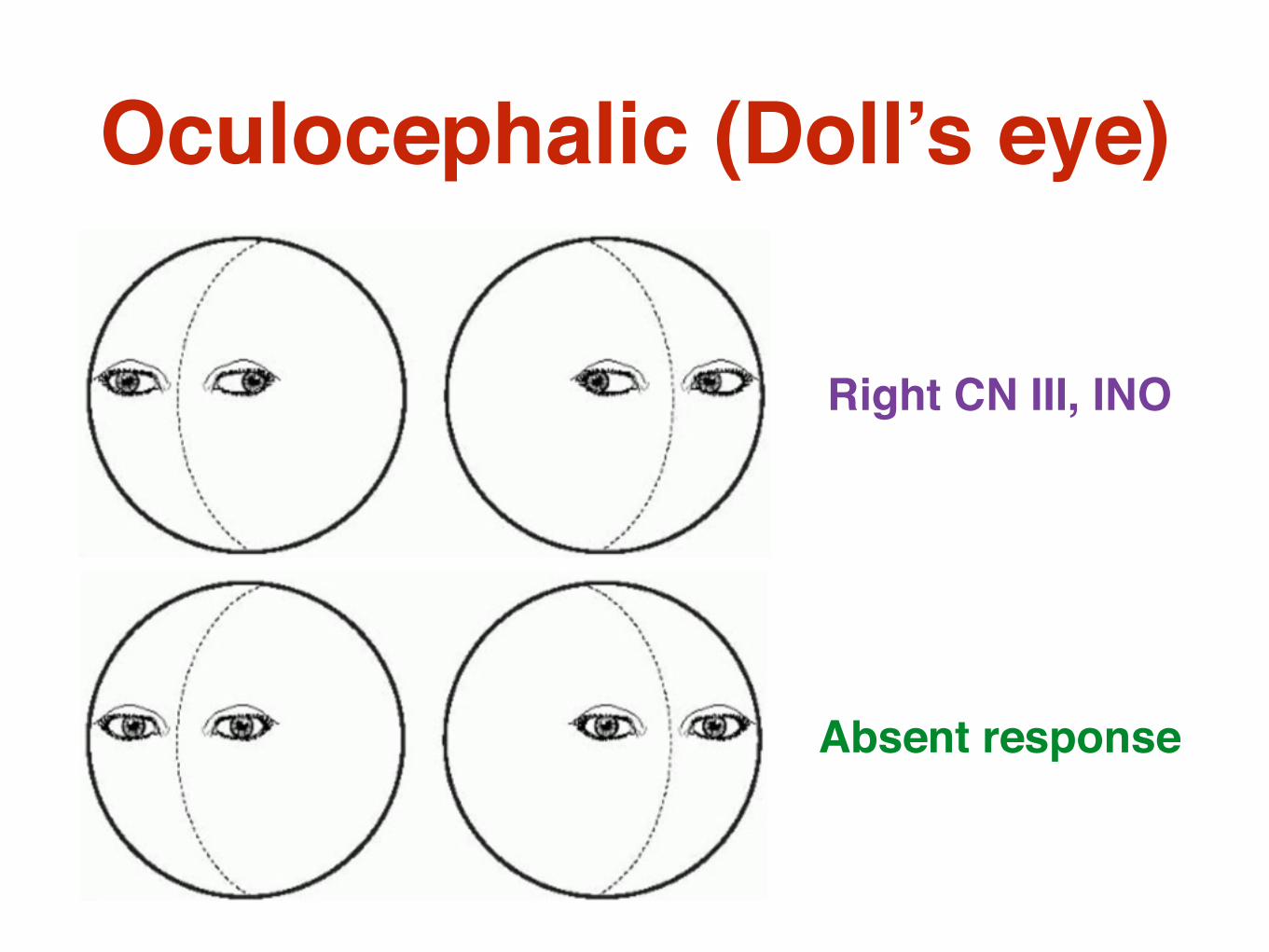
Right CN III, INO
Absent response
Oculocephalic (Doll’s eye)

RightLeft
MLF

Caloric response
COWS : Cold Opposite Warm Same
Check tympanic membrane before testing
Fast phase nystagmus
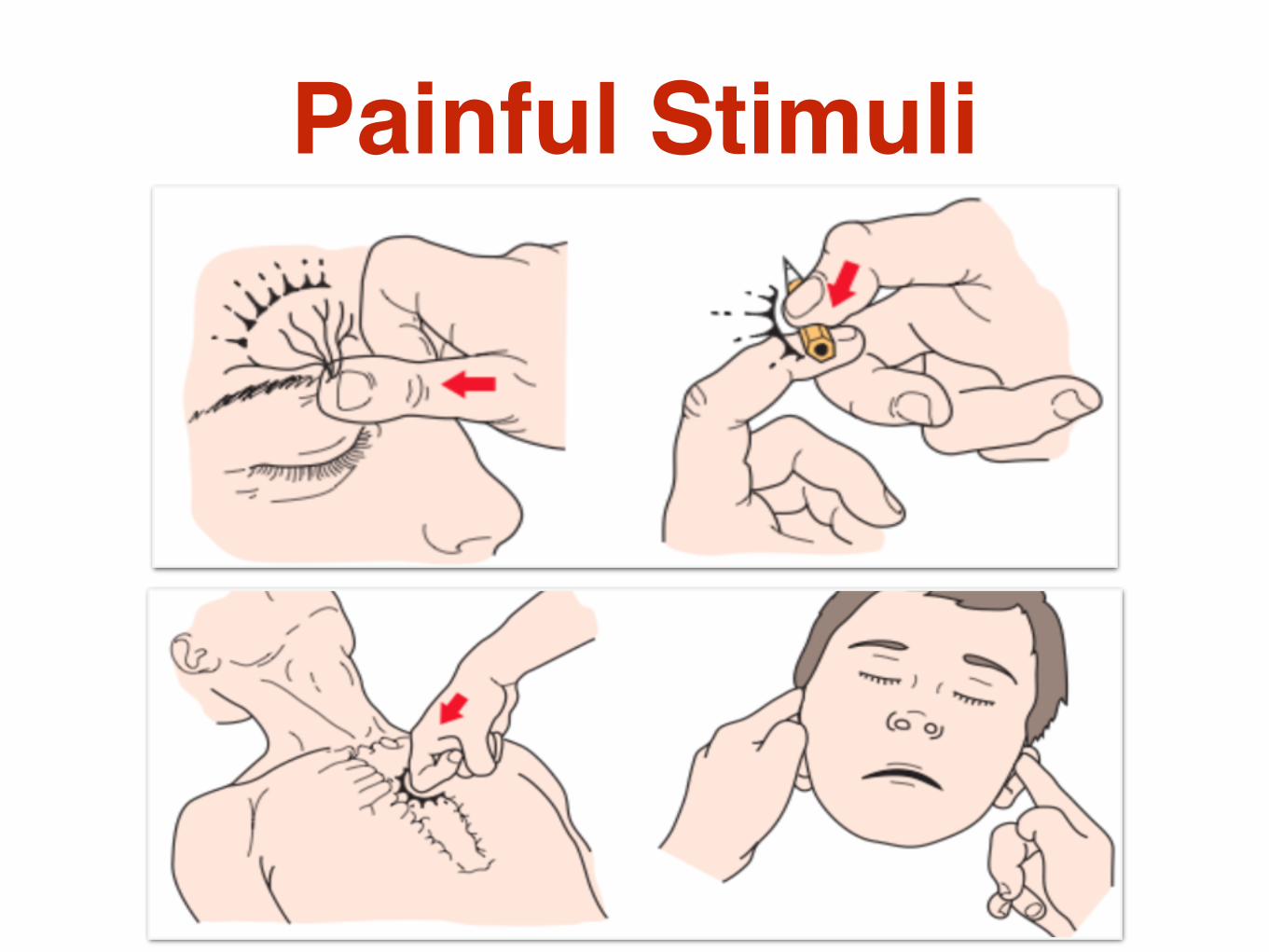
Painful Stimuli
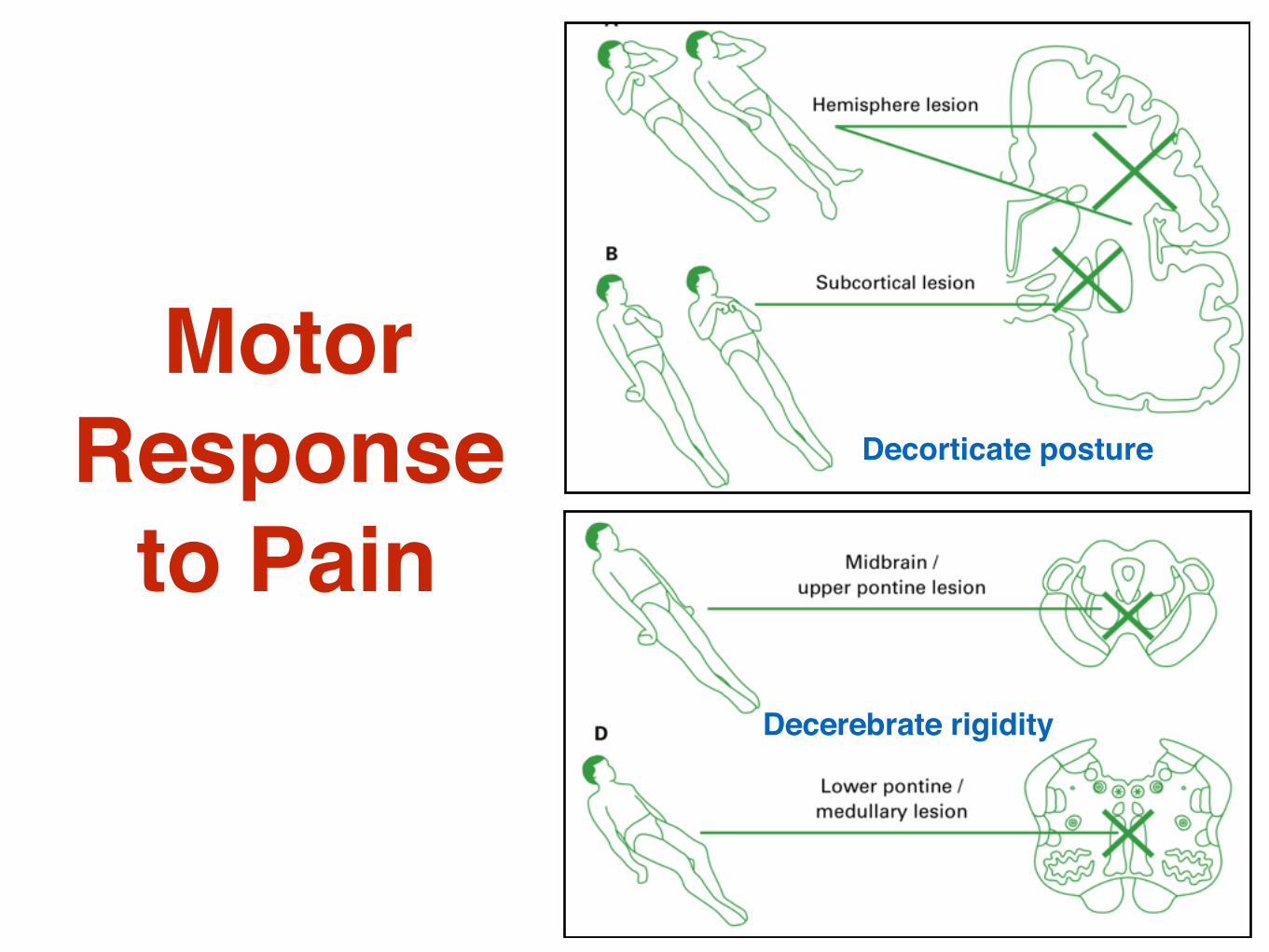
Motor Response
to PainDecerebrate rigidity
Decorticate posture
Clinico-Anatomical Correlation in Coma
Bilateral hemisphere damage/dysfunction
Symmetrical signs
May have fits or myoclonus
Normal brain stem reflexes
Normal oculocephalic and calorics response
Normal pupils
Supratentorial mass lesion with secondary brain stem compression
ipsilateral third nerve palsy
contralateral hemiplegia
Brain stem lesion Abnormal OCR, calorics
Asymmetrical motor responses
Toxic/metabolic Normal pupils: single most important criterion
(except opiate poisoning)
Ocular motility: rove randomly in mild coma and come to rest in primary position with deepening coma
Absent OCR and calorics
Decorticate and decerebrate rigidity or flaccidity, multifocal myoclonus
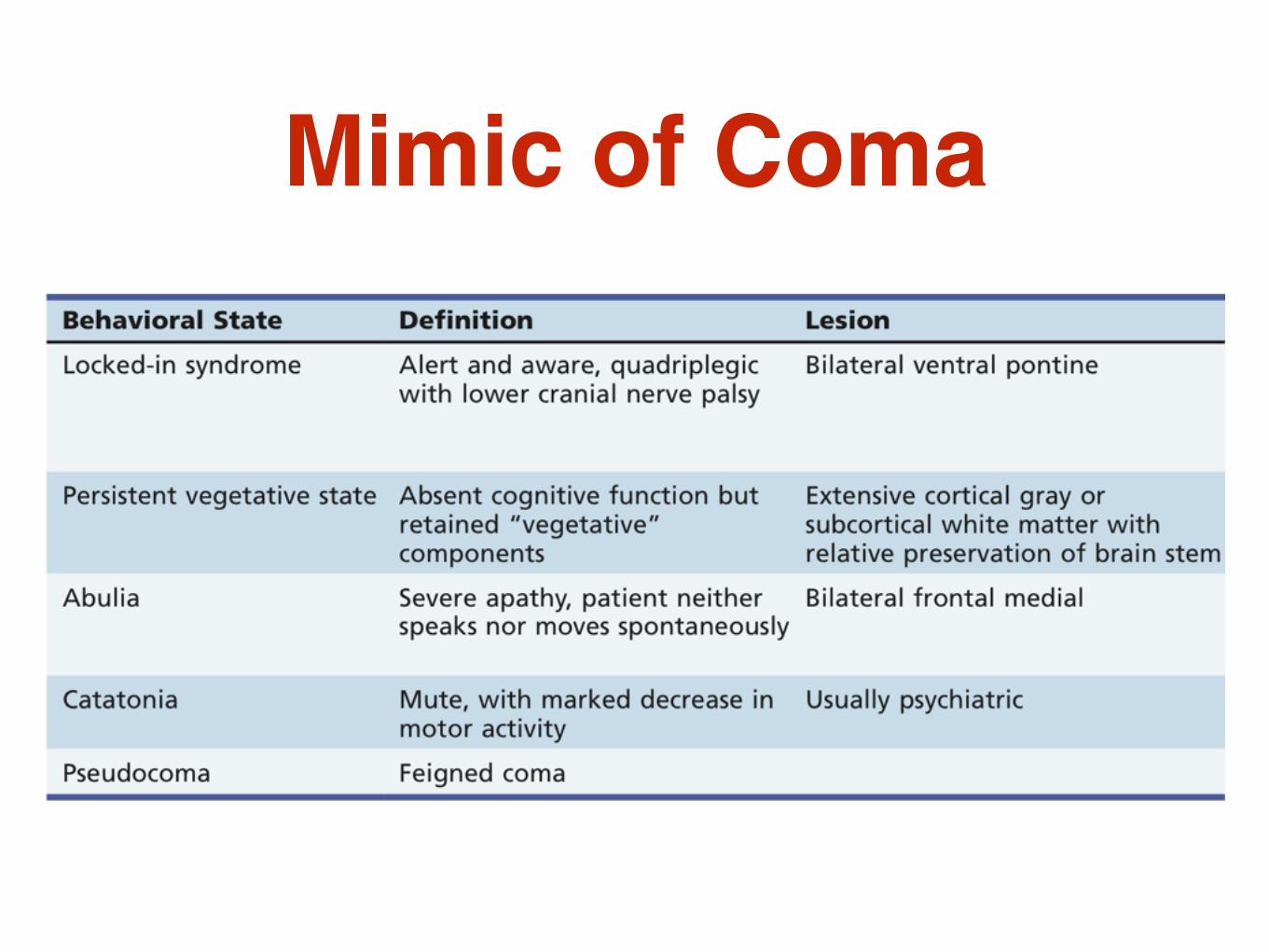
Mimic of Coma

Maintain airway, breathing, and circulation (ABC’s)
Urgently correct any hypothermia, if profound.
If trauma has occurred or is strongly suspected
Stability of the cervical spine before moving the head.
Initial Management of Coma
Initial Management of Coma
Rule out hypoglycemia esp DM.
Check basic blood work (blood count, E’lyte, BS, BUN, Cr, LFT, PT, PTT, ABG, possibly CO level if suspected) and urine drug screen.

Coma Cocktail
50 ml of 50%glucose IV
100 mg of thiamine IV
Naloxone or Flumazenil for opiate or BZP overdose.

Comatose patient with suspected SAH
Rule out SAH : brain CT scan without contrast.
Lumbar puncture if SAH is still strongly suspected but not seen on brain CT scan.
If SAH : neurosurgical consultation and urgent cerebral angiography.
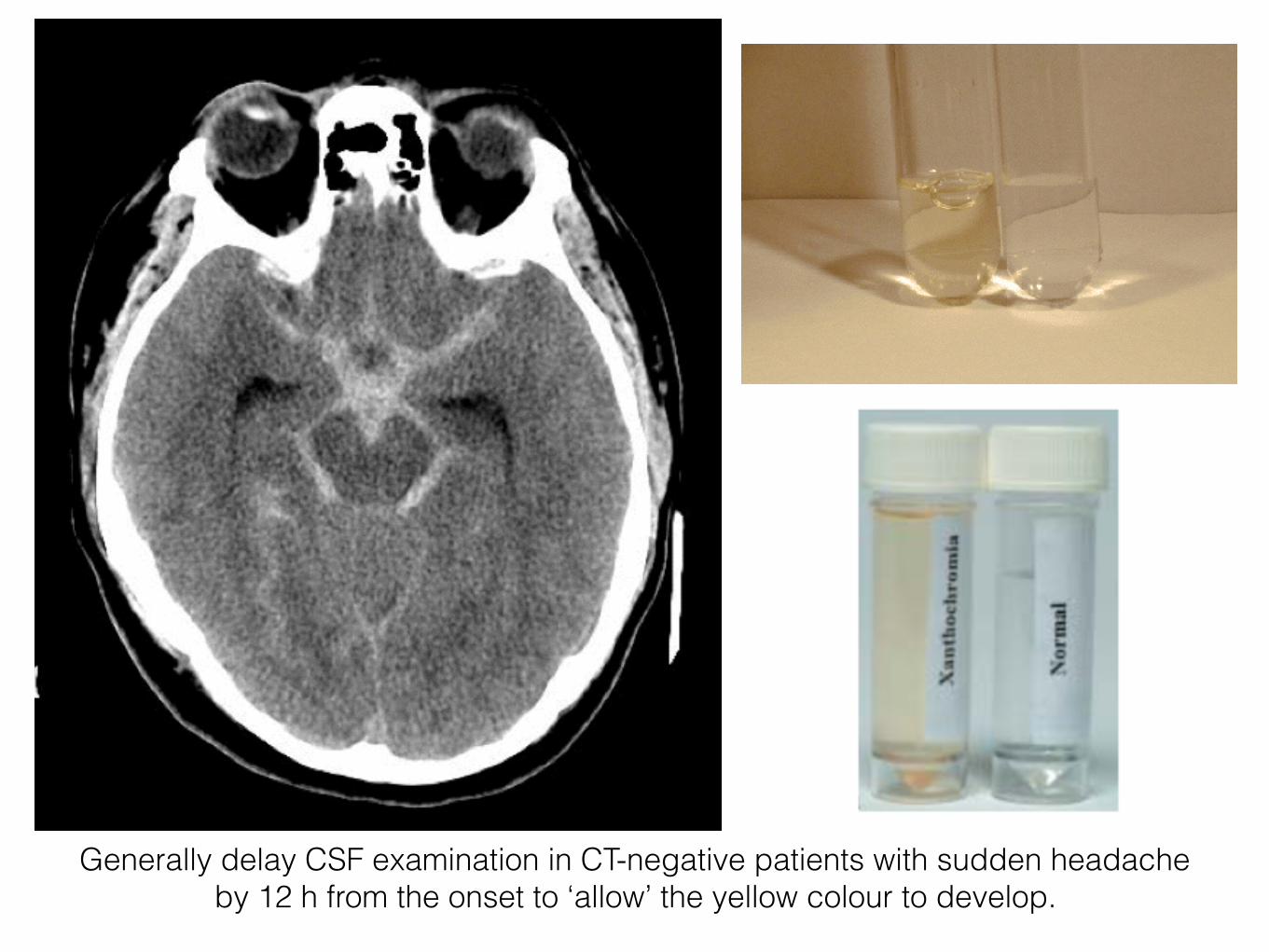
Generally delay CSF examination in CT-negative patients with sudden headache by 12 h from the onset to ‘allow’ the yellow colour to develop.

Comatose patient with fever or septic syndrome Examine for any likely systemic focus (abscess,
peritonitis) of infection.
Panculture blood and urine, CXR.
Perform LP to exclude meningitis and begin initial broad-spectrum antibiotic coverage.
If LP is contraindicated : brain CT scan with and without contrast.
Brain MRI if suspect Herpes simplex encephalitis
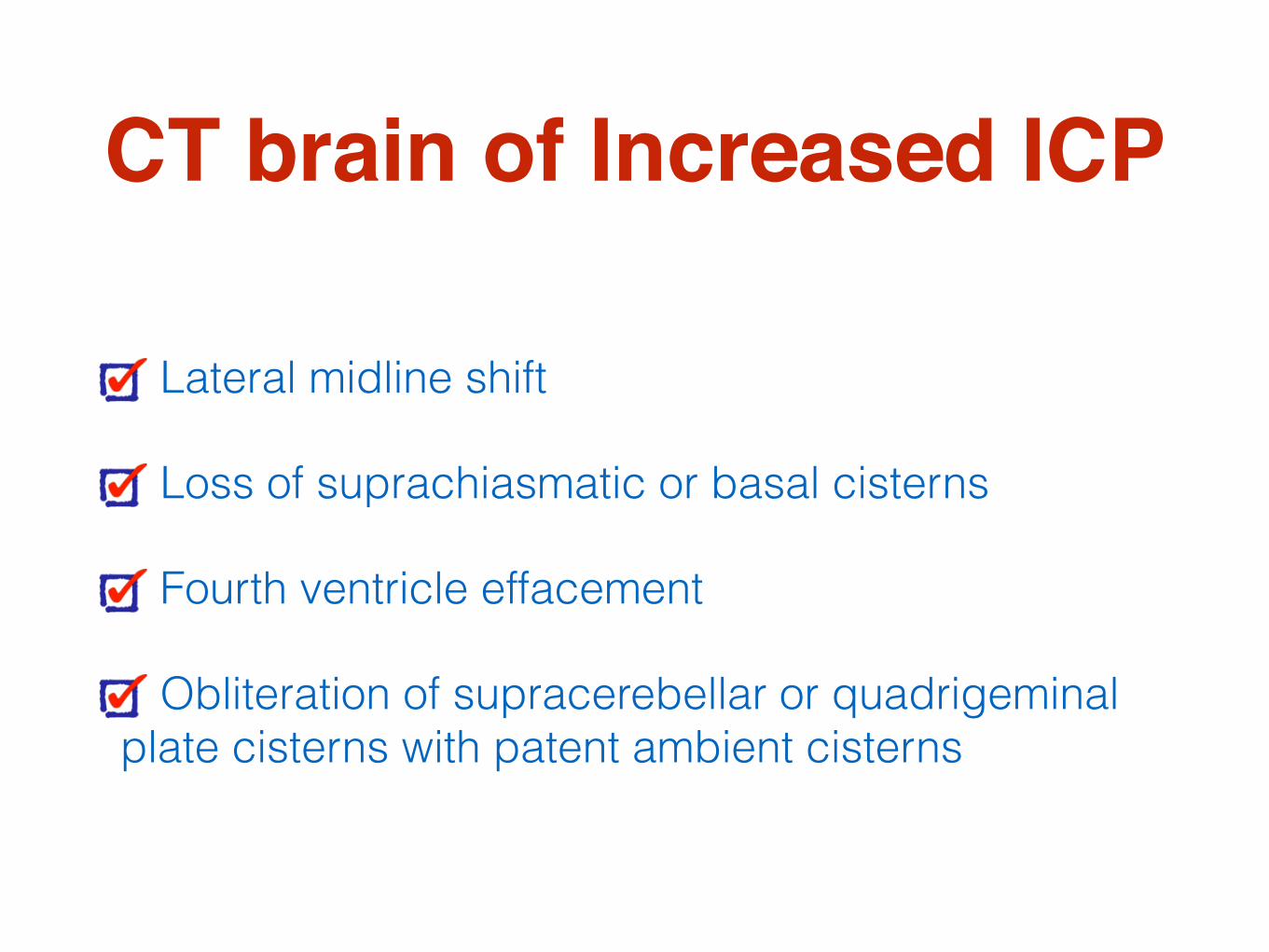
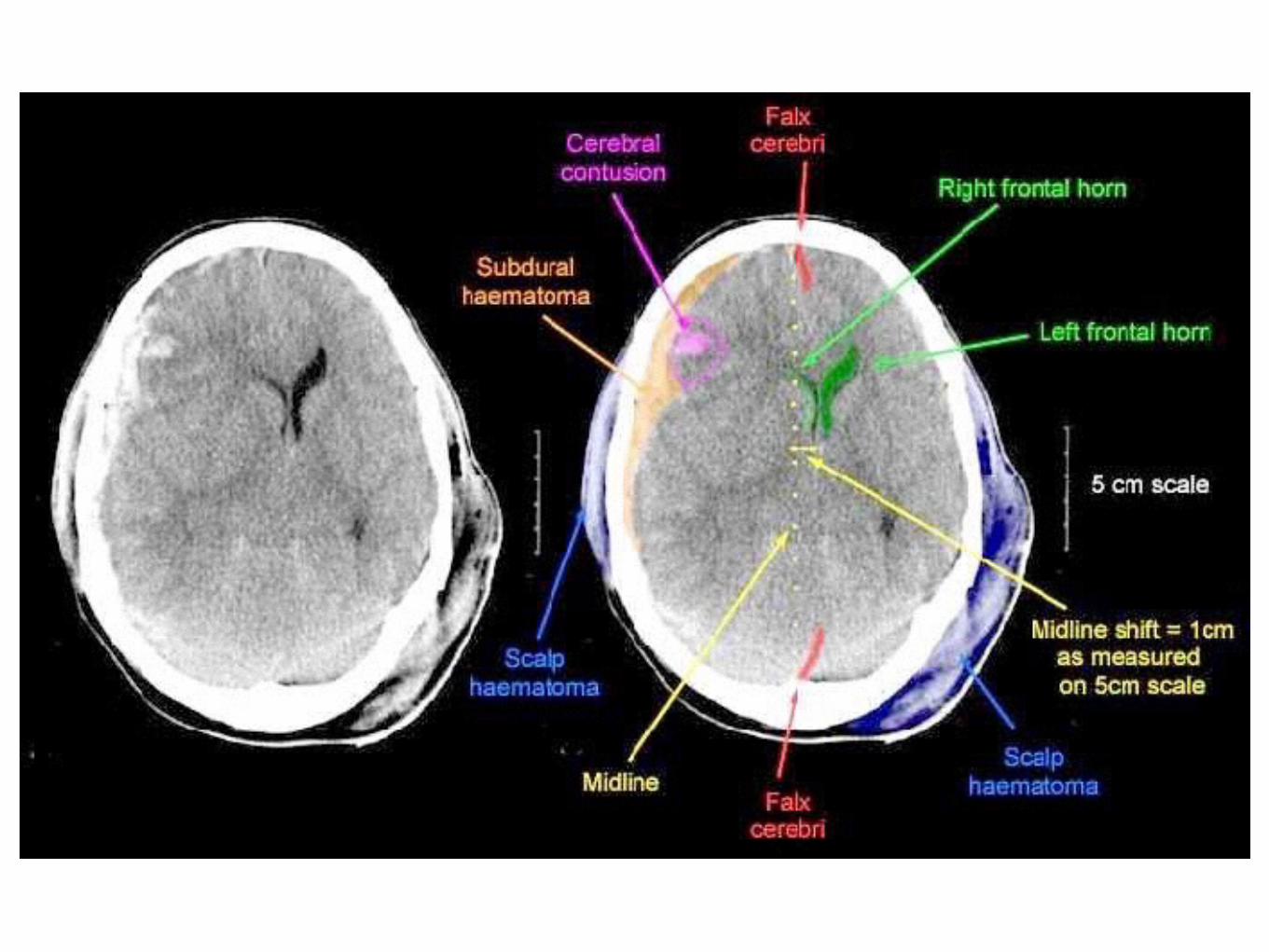
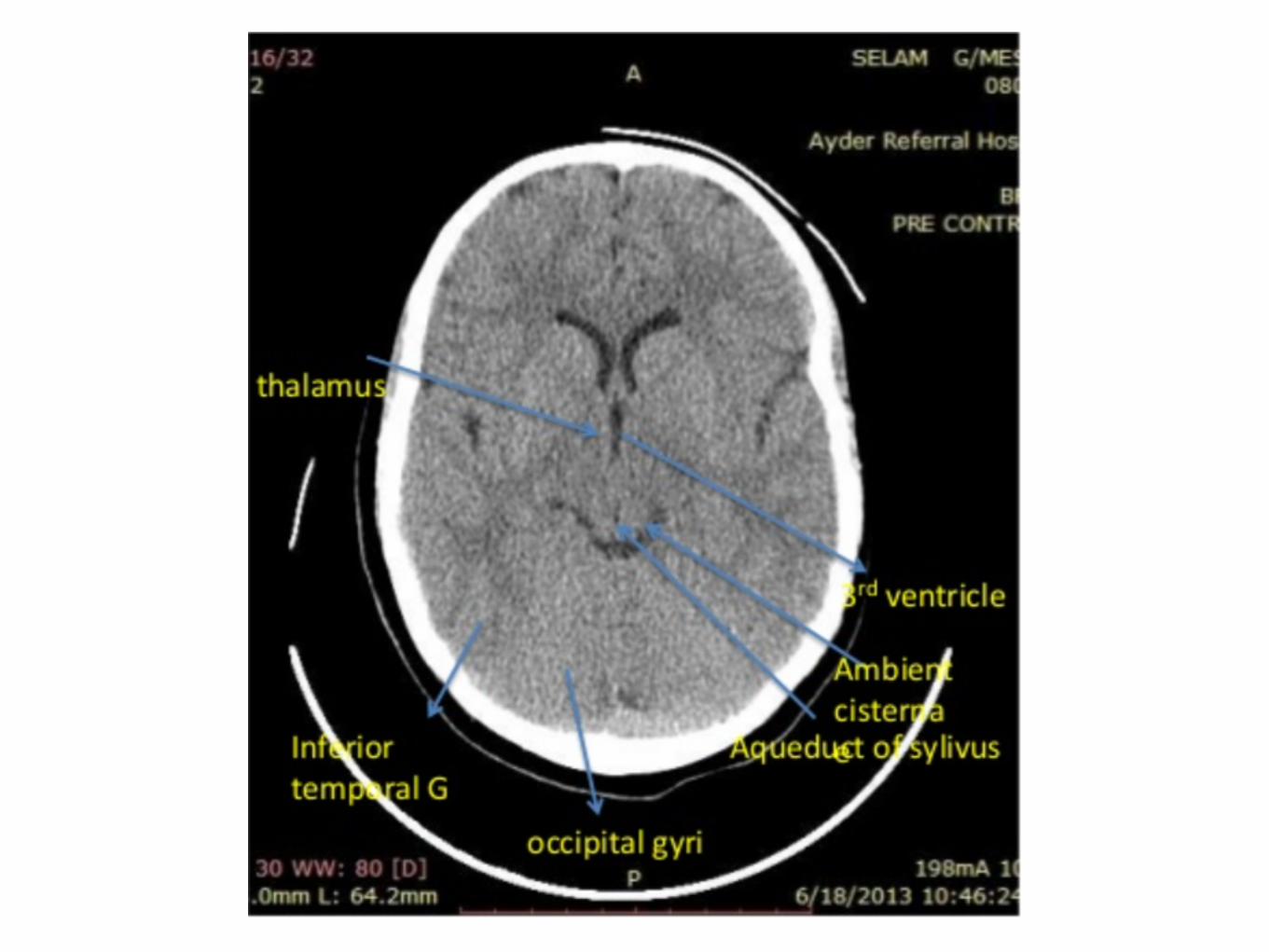
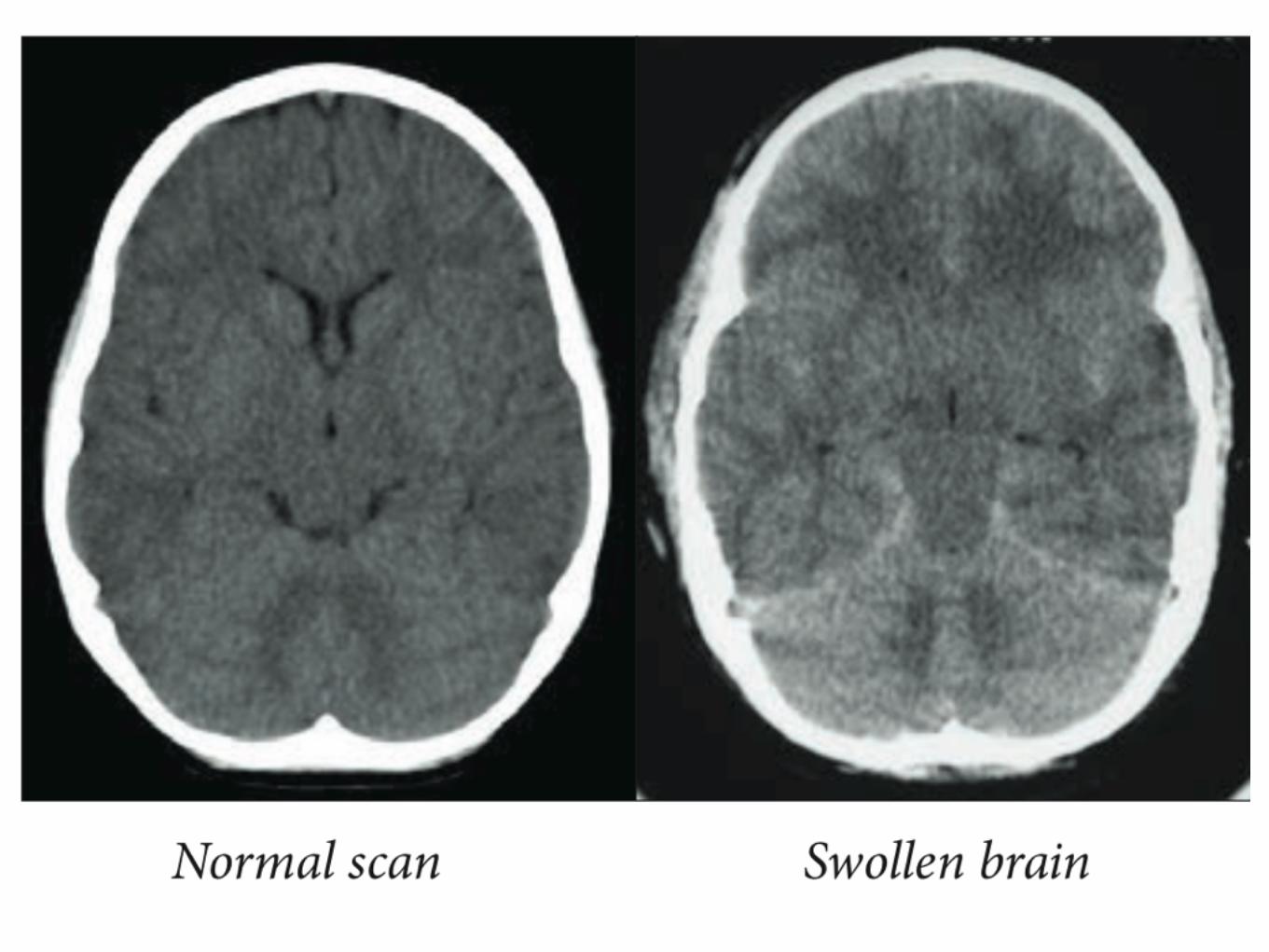
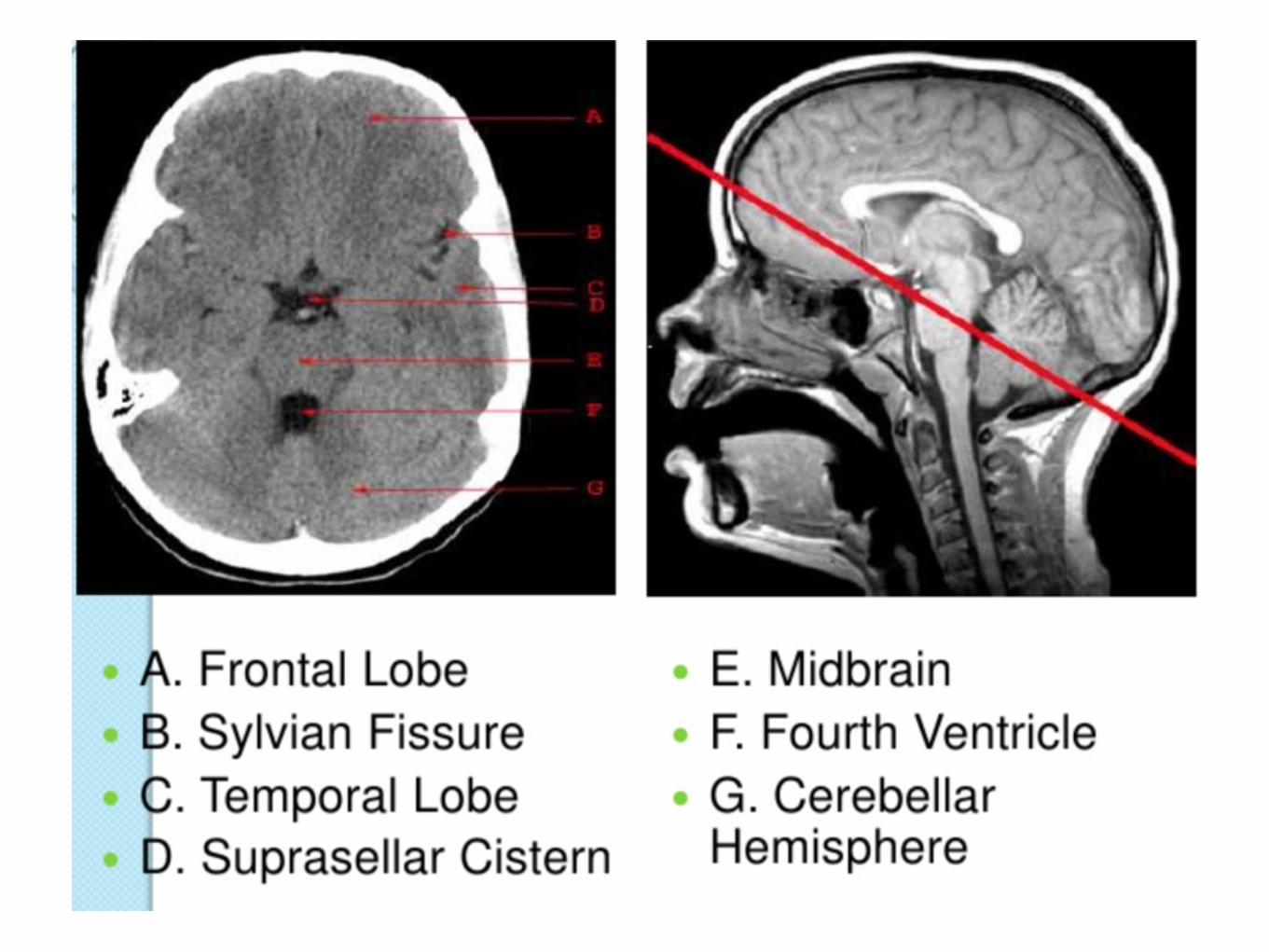
CT brain of Increased ICP
Lateral midline shift
Loss of suprachiasmatic or basal cisterns
Fourth ventricle effacement
Obliteration of supracerebellar or quadrigeminal plate cisterns with patent ambient cisterns

Cerebrovascular disease
Transient Ischemic Attack
(TIA)
“A transient episode of neurological dysfunction caused by focal brain, spinal cord, or retinal
ischemia, without acute infarction”
Stroke. 2009;40:2276-2293.
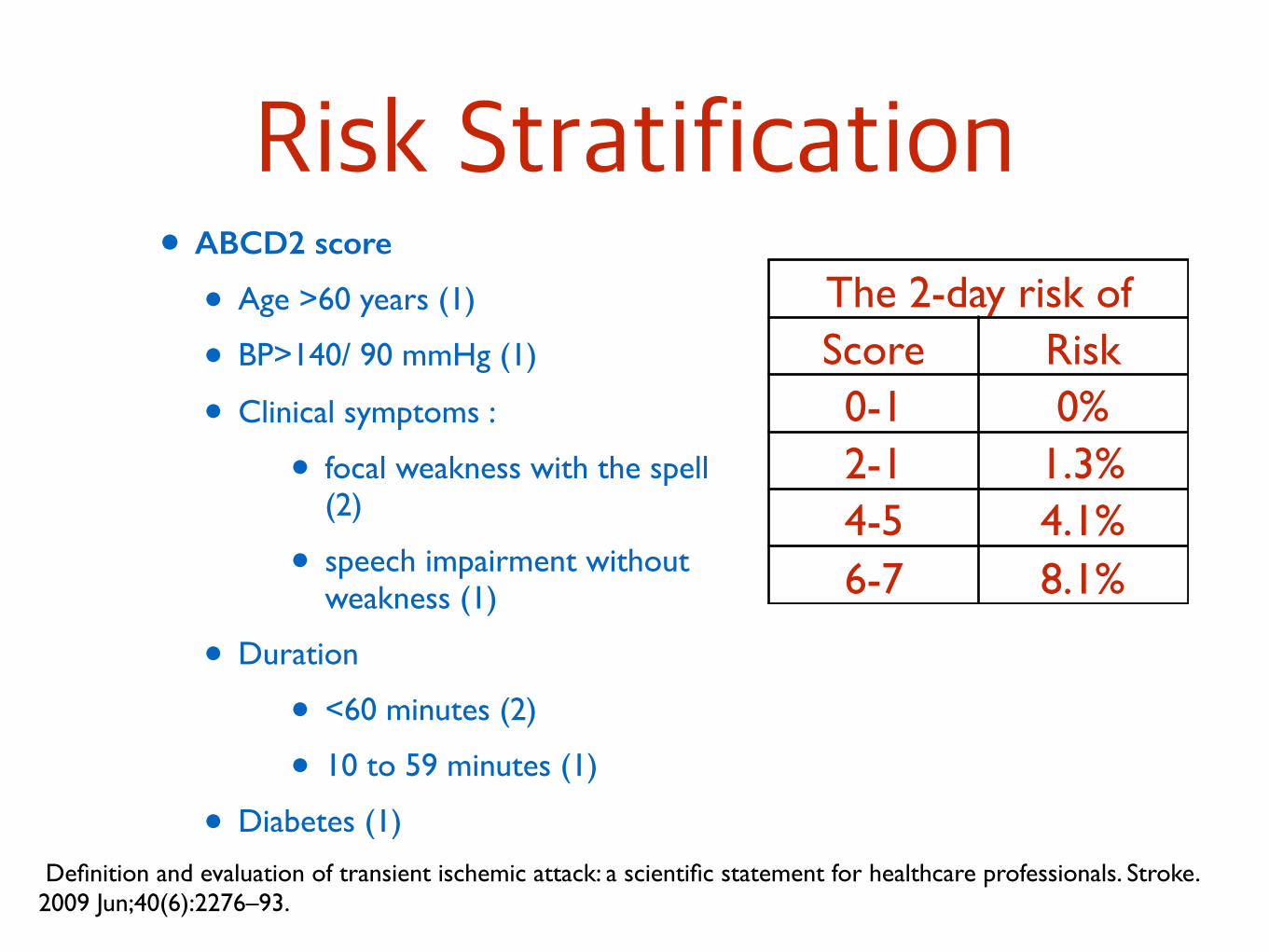
Risk Stratification• ABCD2 score
• Age >60 years (1)
• BP>140/ 90 mmHg (1)
• Clinical symptoms :
• focal weakness with the spell (2)
• speech impairment without weakness (1)
• Duration
• <60 minutes (2)
• 10 to 59 minutes (1)
• Diabetes (1)
The 2-day risk of stroke Score Risk
0-1 0%2-1 1.3%4-5 4.1%6-7 8.1%
Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals. Stroke. 2009 Jun;40(6):2276–93.
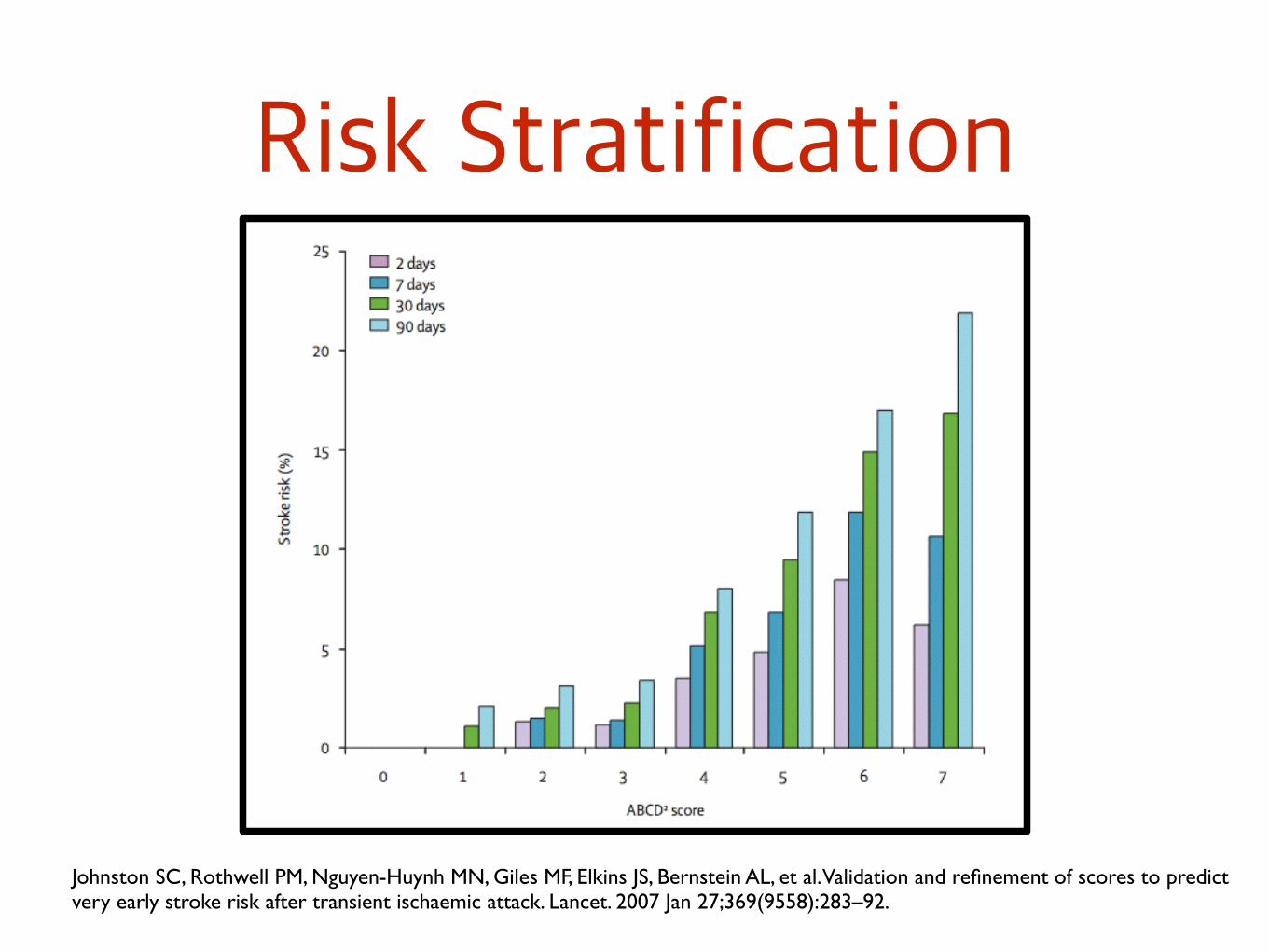
Risk Stratification
Johnston SC, Rothwell PM, Nguyen-Huynh MN, Giles MF, Elkins JS, Bernstein AL, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet. 2007 Jan 27;369(9558):283–92.
Stroke
“Sudden loss of blood circulation to an area of the brain, resulting in a corresponding
loss of neurologic function”

Etiology Diagnosis
Baseline laboratory
FBS, CBC, Lipid, BUN, Cr, Electrolytes,
Coagulogram ,Urine exam
Cardiac work up : CXR, EKG
Non-contrast CT brain
Work up for Etiology of Stroke

Cardio-embolic stroke
Echocardiogram : TTE, TEE
Holter monitoring : paroxysmal AF
Work up for Etiology of Stroke
Stroke in the young <45 yr No evidence of Cardio-embolism or
atherosclerosis risk factor
ESR, ANA, anti-HIV, VDRL, LFT.
Protein C, Protein S, Antithrombin III, factor V laiden, prothrombin gene, Homocysteine.
Antiphospholipid syndrome : anticardiolipin, Lupus anticoagulant
Suspected of intra or extra-cranial artery stenosis
Carotid bruit, Amouroxis fugax
Lacunar infarction with mRS>2
Vascular Work up

Carotid duplex ultrasonography
Transcranial Doppler ultrasonography
Vascular Work up
Magnetic resonance angiography
Computerized angiography
Vascular Work up
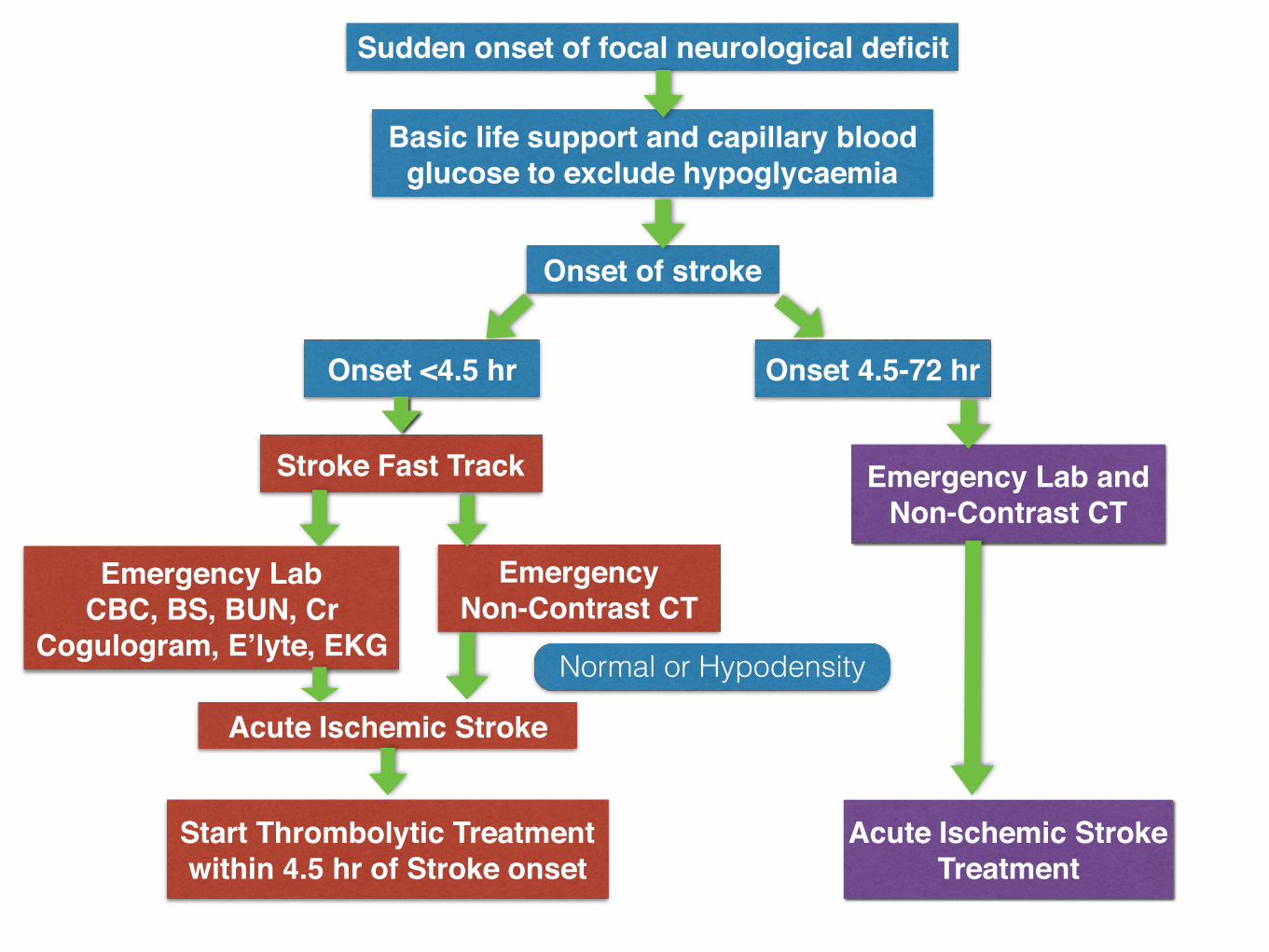
Onset of stroke
Sudden onset of focal neurological deficit
Basic life support and capillary blood glucose to exclude hypoglycaemia
Onset <4.5 hr
Stroke Fast Track
Emergency LabCBC, BS, BUN, Cr
Cogulogram, E’lyte, EKG
Emergency Non-Contrast CT
Acute Ischemic Stroke
Start Thrombolytic Treatment within 4.5 hr of Stroke onset
Normal or Hypodensity
Onset 4.5-72 hr
Emergency Lab and Non-Contrast CT
Acute Ischemic Stroke Treatment
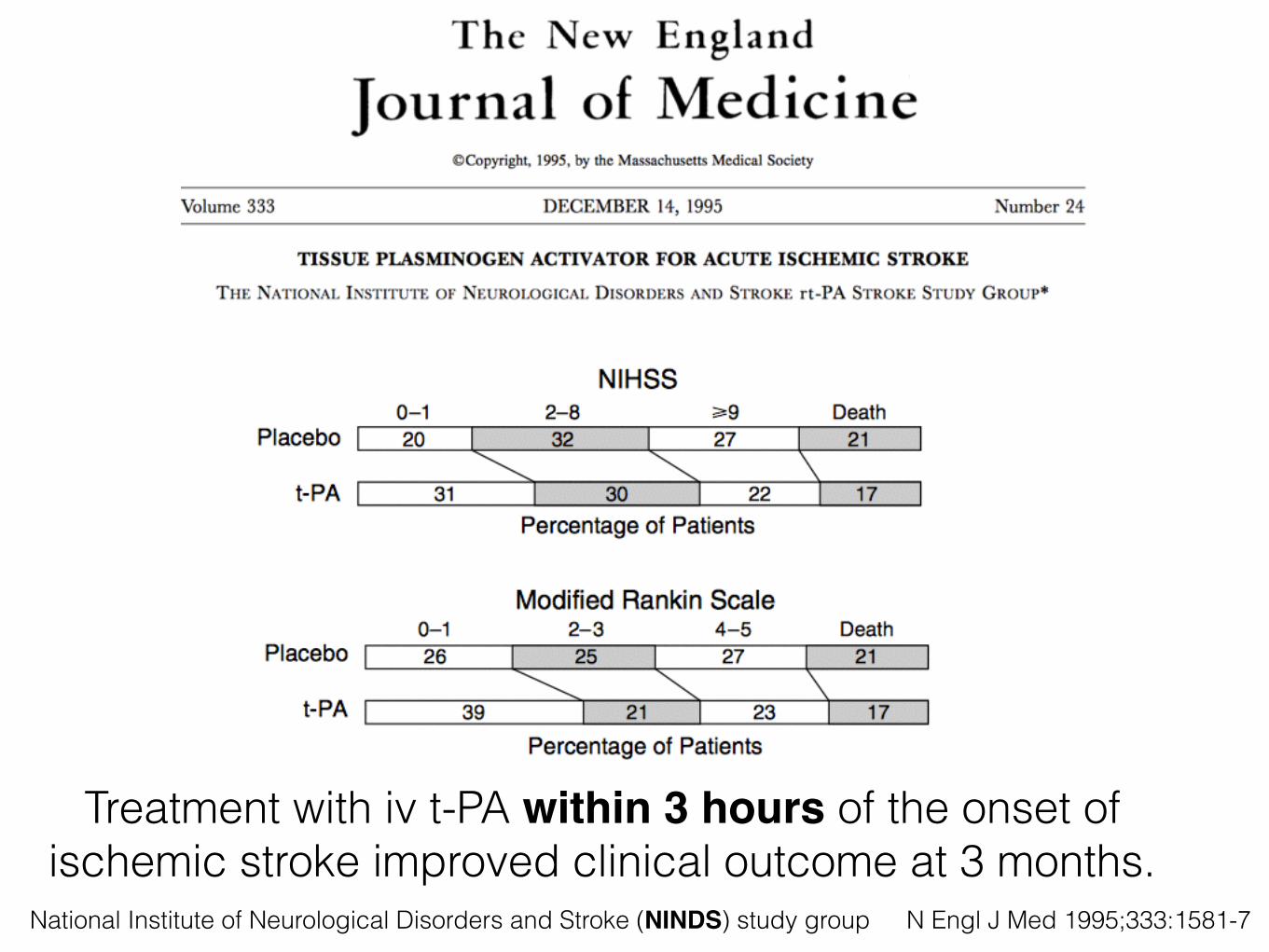
N Engl J Med 1995;333:1581-7
Treatment with iv t-PA within 3 hours of the onset of ischemic stroke improved clinical outcome at 3 months.
National Institute of Neurological Disorders and Stroke (NINDS) study group
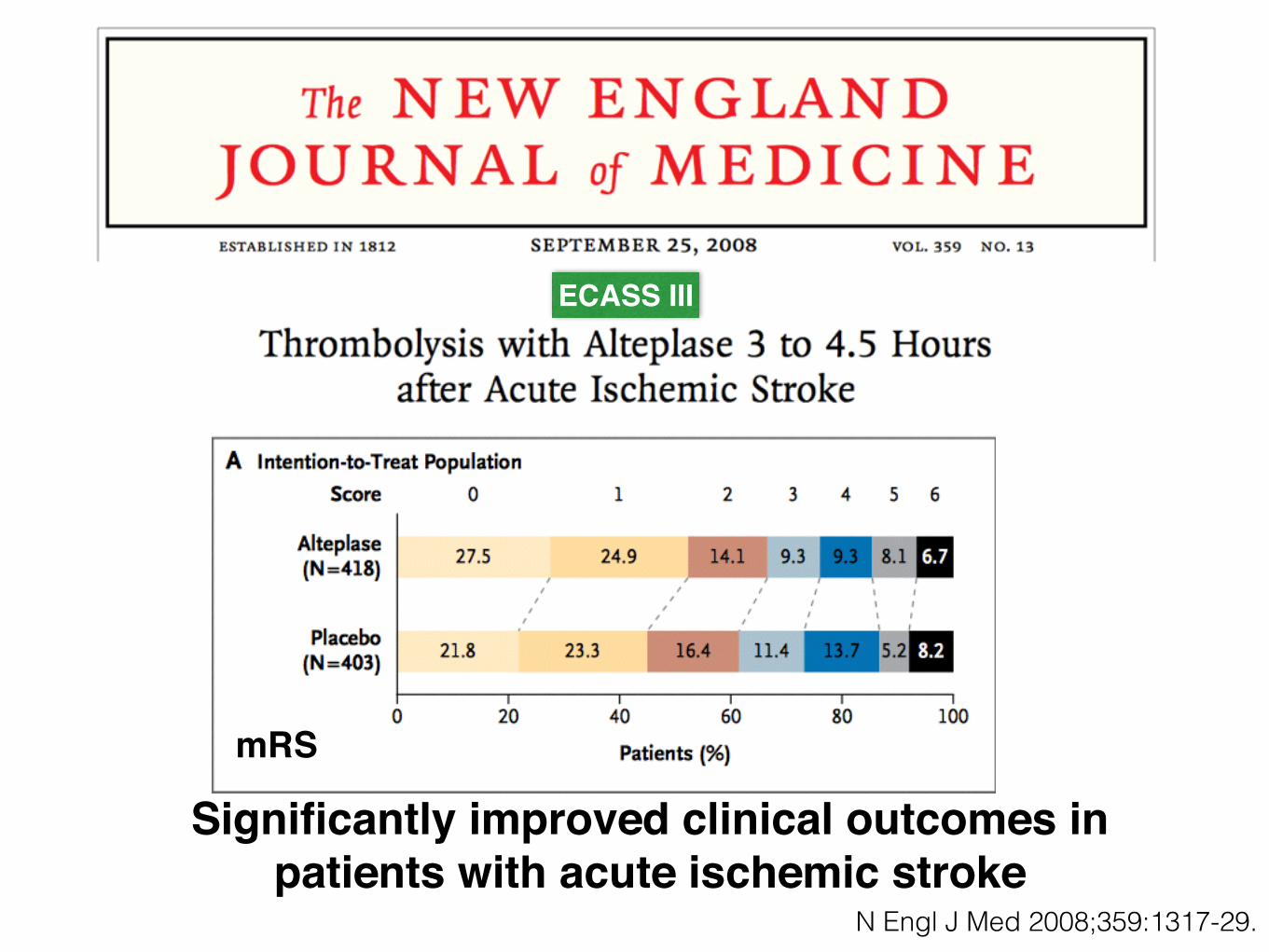
Significantly improved clinical outcomes in patients with acute ischemic stroke
N Engl J Med 2008;359:1317-29.
ECASS III
mRS

Inclusion Criteria
&Exclusion
Criteria (0-3 hr)
Inclusion Criteria
Exclusion Criteria
Stroke 2013

ExclusionCriteria (0-3 hr)
Relative Exclusion Criteria
Stroke 2013

Additional Exclusion Criteria for IV rtPA Within 3 to 4.5 Hours
Stroke 2013
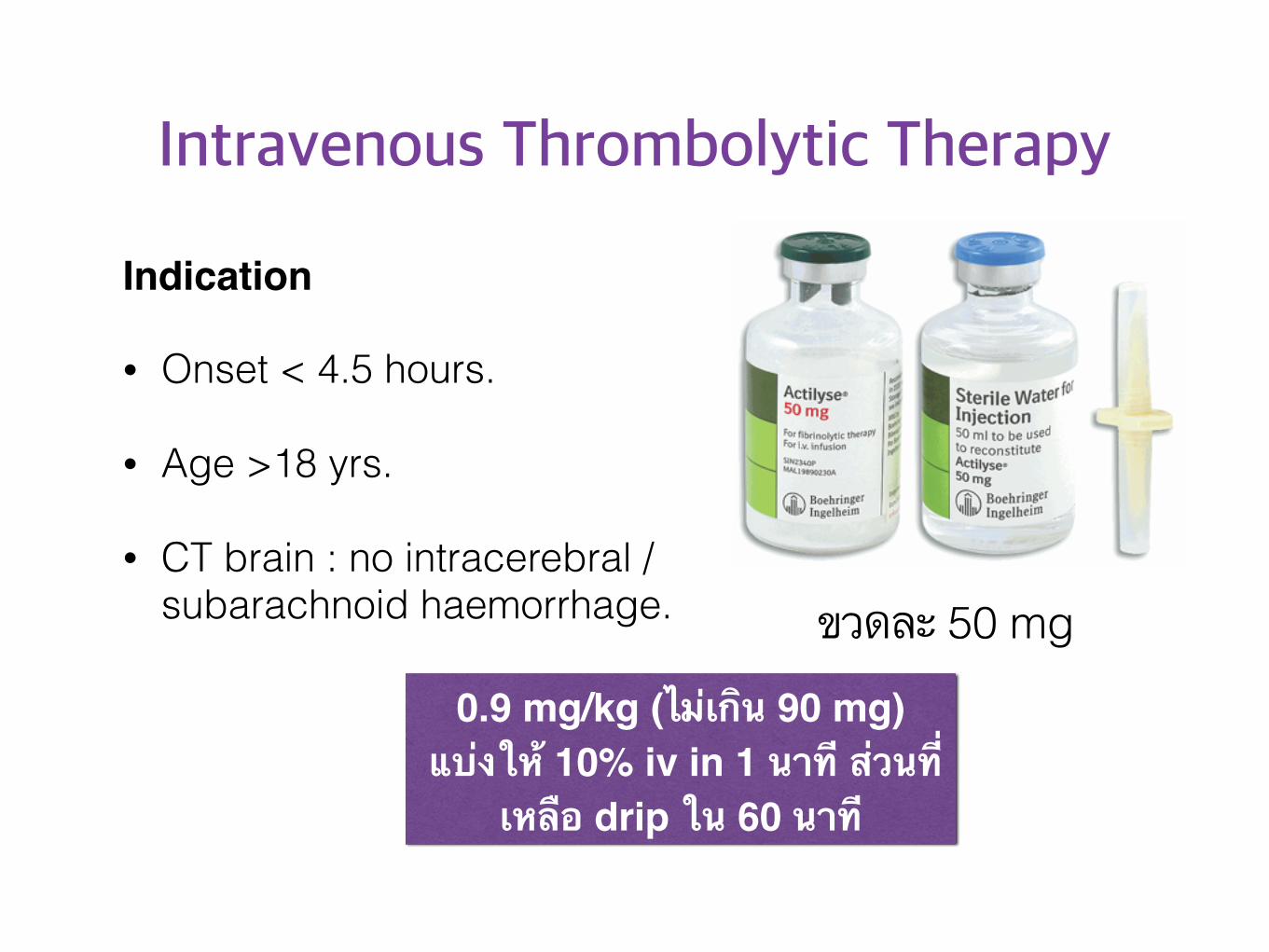
Intravenous Thrombolytic Therapy
Indication
• Onset < 4.5 hours.
• Age >18 yrs.
• CT brain : no intracerebral / subarachnoid haemorrhage.
0.9 mg/kg (ไม่เกิน 90 mg) แบ่งให้ 10% iv in 1 นาที ส่วนที่
เหลือ drip ใน 60 นาที
ขวดละ 50 mg
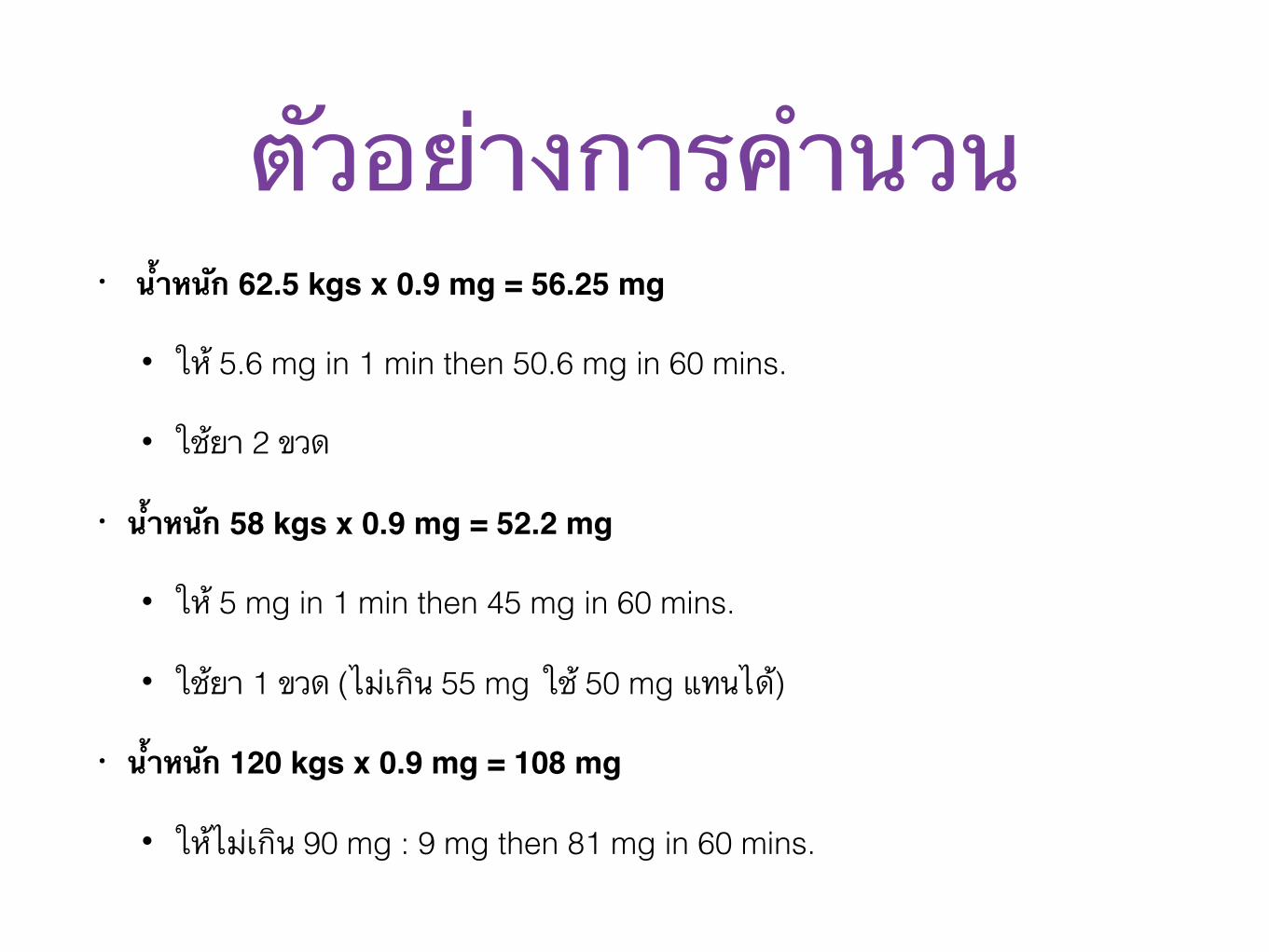
ตัวอย่างการคำนวน• น้ำหนัก 62.5 kgs x 0.9 mg = 56.25 mg
• ให้ 5.6 mg in 1 min then 50.6 mg in 60 mins.
• ใช้ยา 2 ขวด
• น้ำหนัก 58 kgs x 0.9 mg = 52.2 mg
• ให้ 5 mg in 1 min then 45 mg in 60 mins.
• ใช้ยา 1 ขวด (ไม่เกิน 55 mg ใช้ 50 mg แทนได้)
• น้ำหนัก 120 kgs x 0.9 mg = 108 mg
• ให้ไม่เกิน 90 mg : 9 mg then 81 mg in 60 mins.

Acute Treatment
Anti-platelets
• Aspirin 160-325 mg/d ภายใน 48 ชั่วโมง
• กรณีที่ได้รับ thrombolytic therapy ห้ามให้ anti-platelets ภายใน 24 ชั่วโมง

Acute TreatmentAnticoagulants
แนะนำให้ใน Cardio-embolic stroke ยกเว้นมีข้อห้าม ได้แก่
Large infarction size, Brain edema.
กรณีอื่นๆ ยังมีหลักฐานไม่เพียงพอ เช่น crescendo TIA, extracranial arterial dissection, basilar artery thrombosis
INR 2-3, 2.5-3.5 (mechanical prosthetic heart valve)
AF, AMI with LV thrombus, Cardiomyopathy,
Rheumatic MV diseaseMechanical Prosthetic heart valve
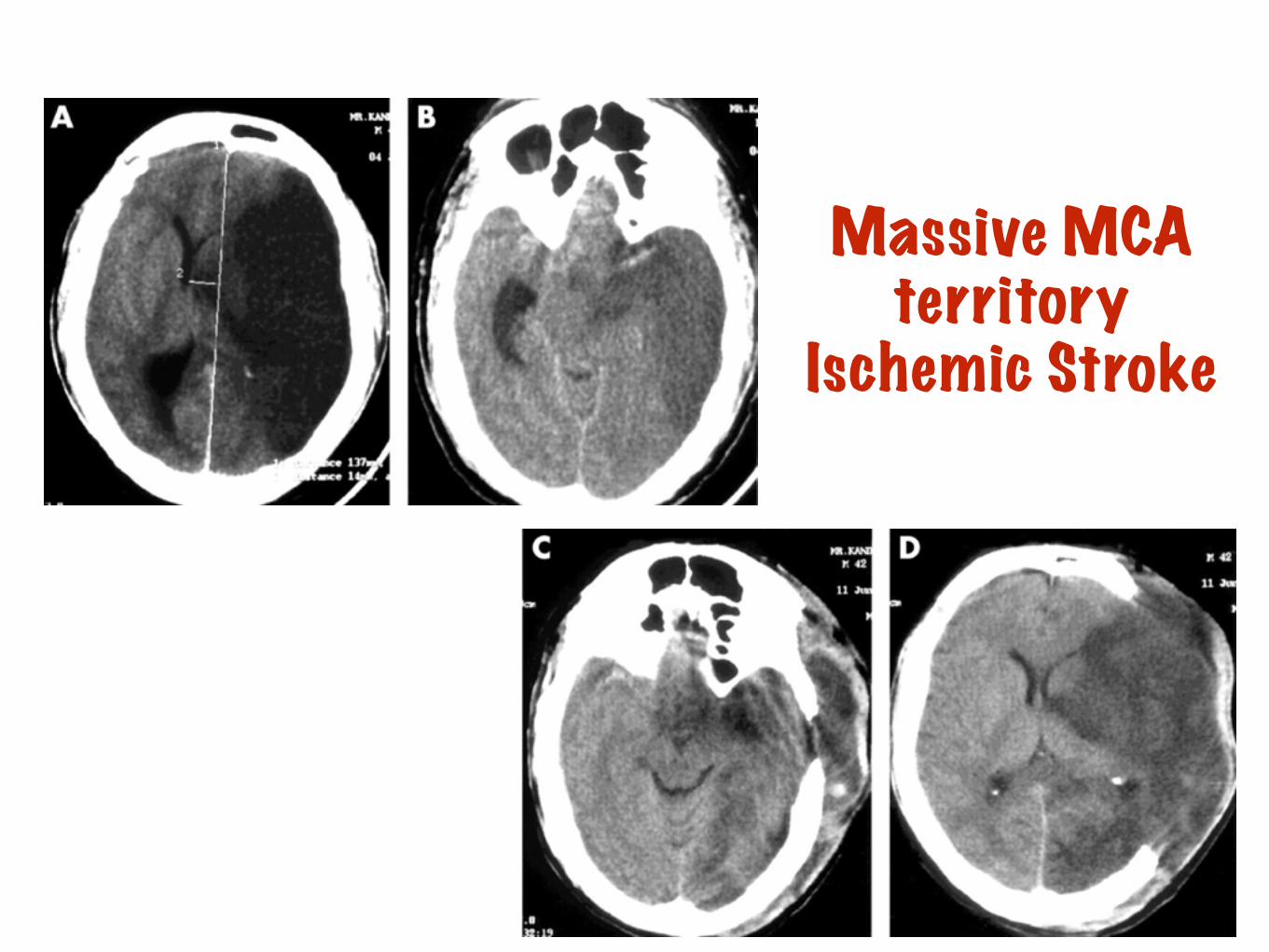
Massive MCA territory
Ischemic Stroke
Anticoagulant in AIS
Early administration of UFH or LMWH does not lower the risk of early recurrent stroke including among people with cardioembolic sources.
Not recommended for treatment of patients with acute ischemic stroke (Class III; Level of Evidence A).

General ManagementNPO : drowsiness, large infarction
Swallowing evaluation
Early mobilization
General Management1. ควรให้ยาลดความดันโลหิตเมื่อ
• SBP>220 หรือ DBP>120 mmHg
• SBP <220 หรือ DBP <120 mmHg ร่วมกับ
• SBP>180 หรือ DBP>105 (thrombolytic treatment)
2. Anti-hypertensive
• Captropril, Nicardipine, Nitroglycerine, Nitroprusside
3. ในกรณีที่ความดันโลหิต <100/70 mmHg ให้หาสาเหตุและแก้ไข
Congestive heart failureAortic dissectionAcute Myocardial InfarctionAcute renal failure
Don’t Use Nifedipine sublingual or oral
ป้องกันภาวะ hypoxemia (keep O2sat>92%)
ควบคุมระดับน้ำตาลในเลือดที่ 80-140 mg/dl และ 140-180 mg/dl ในรายที่เป็นเบาหวาน
ควรให้สารน้ำเป็น 0.9%NaCl, หลีกเลี่ยงการใช้ free water หรือสารน้ำที่มีน้ำตาล
ควบคุมอุณหภูมิร่างกายให้ปกติ ถ้ามีไข้ให้หาสาเหตุและรักษา
ให้ยากันชักเมื่อมีอาการ ไม่ควรให้เพื่อป้องกัน
General Management
Management of Stroke Complication
ICH after Thrombolytic treatment
Suspect : acute neurological deterioration, acute headache, severe hypertension, nausea/vomiting
Stop thrombolytic + CT brain Emergency.
Check PT, aPTT, platelet count.
Cross match for FFP 10 mg/kg
Management of Stroke Complication
Increased Intracranial Pressure
Intubation and Hyperventilation if alteration of consciousness.
Avoid hypervolemia, hypotonic solution, dextrose in iv fluid.
Osmotherapy
20% mannitol
10% glycerol
Consult Neurosurgeon : decompressive craniectomy.

Secondary Stroke Prevention
Drugs DosageAspirin 60-325 mg/d
Clopidogrel 75 mg/d
Cilostazol 200 mg/d
Aspirin + dipyridamole 25+200 mg/d
Antiplatelet drugs

Secondary Stroke PreventionAnticoagulant : use in cardio-embolic stroke.
Warfarin
New oral anticoagulant :
Dabigatran
Apixaban
Rivaroxaban
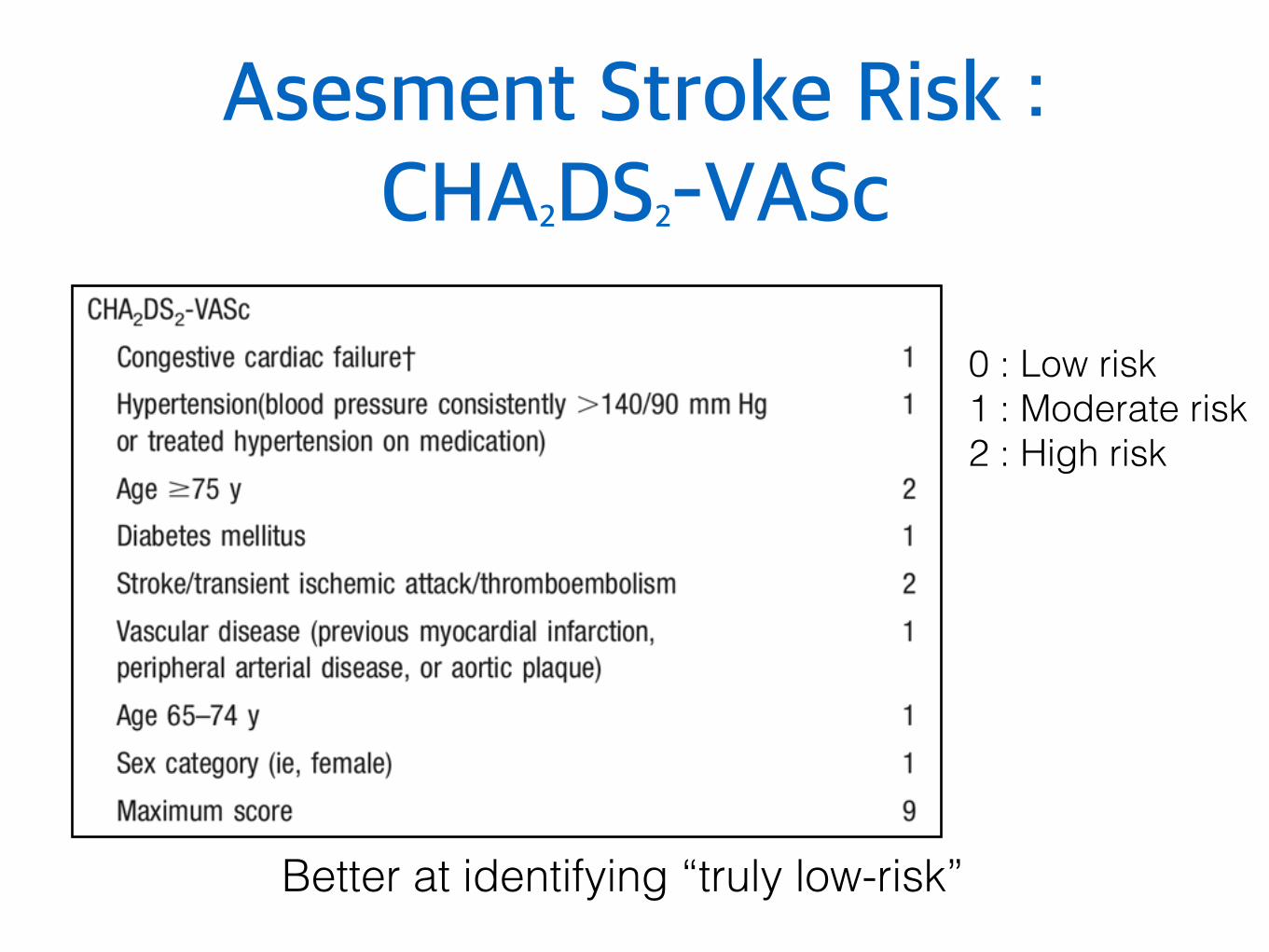
Asesment Stroke Risk : CHA2DS2-VASc
0 : Low risk 1 : Moderate risk 2 : High risk
Better at identifying “truly low-risk”

Assessing Bleeding Risk : HAS-BLED 0-2 : Low risk
>3 : High risk
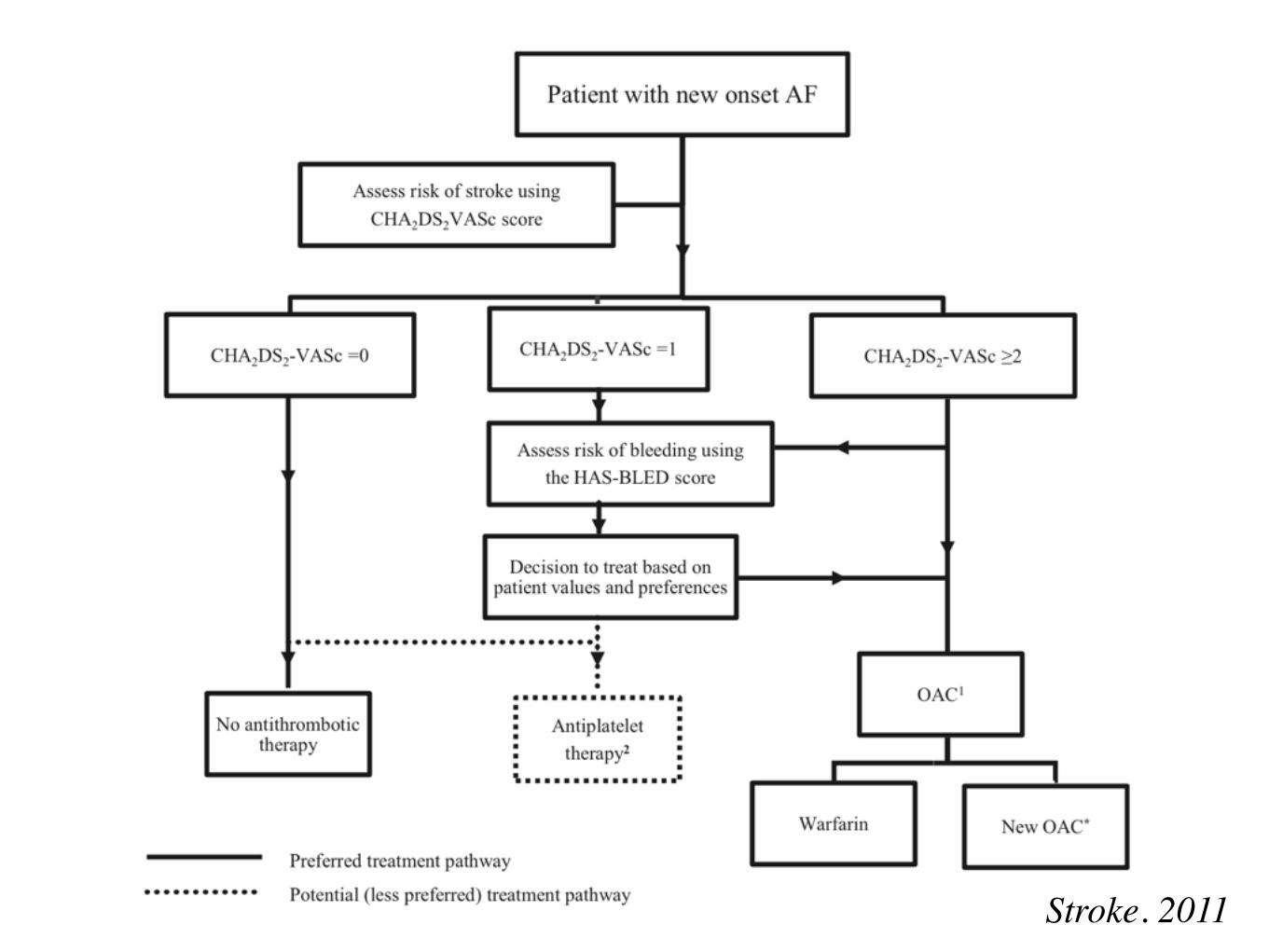
Stroke. 2011

Secondary Stroke PreventionCarotid endarterectomy
Carotid stenosis 70-99% ในรายที่มีอาการไม่มาก
ควรทำภายใน 2 สัปดาห์ หรือกรณีที่อาการคงที่อาจพิจารณาผ่าตัดภายในระยะเวลาไม่เกิน 6 เดือน
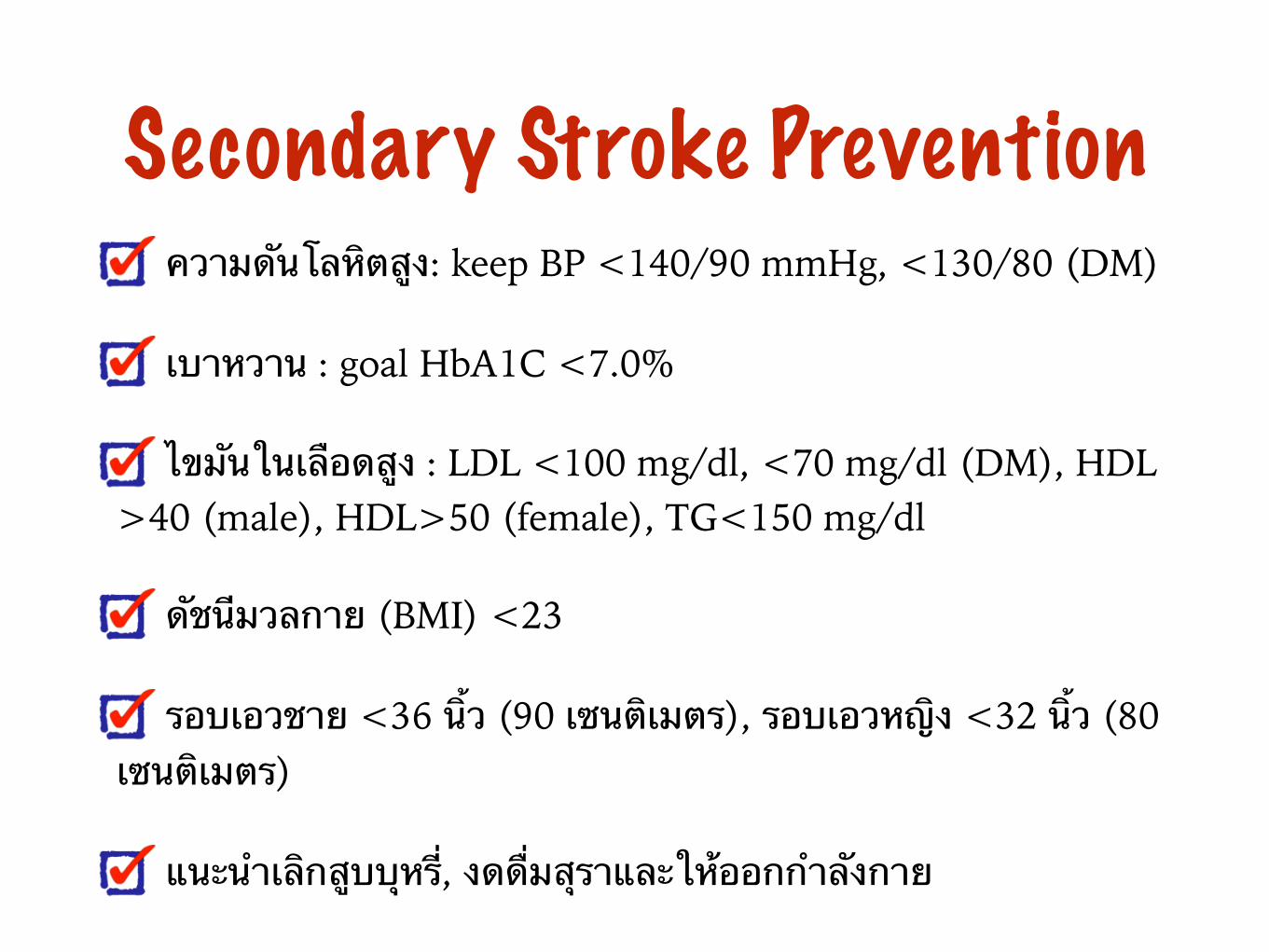
Secondary Stroke Prevention ความดันโลหิตสูง: keep BP <140/90 mmHg, <130/80 (DM)
เบาหวาน : goal HbA1C <7.0%
ไขมันในเลือดสูง : LDL <100 mg/dl, <70 mg/dl (DM), HDL >40 (male), HDL>50 (female), TG<150 mg/dl
ดัชนีมวลกาย (BMI) <23
รอบเอวชาย <36 นิ้ว (90 เซนติเมตร), รอบเอวหญิง <32 นิ้ว (80 เซนติเมตร)
แนะนำเลิกสูบบุหรี่, งดดื่มสุราและให้ออกกำลังกาย

Status Epilepticus
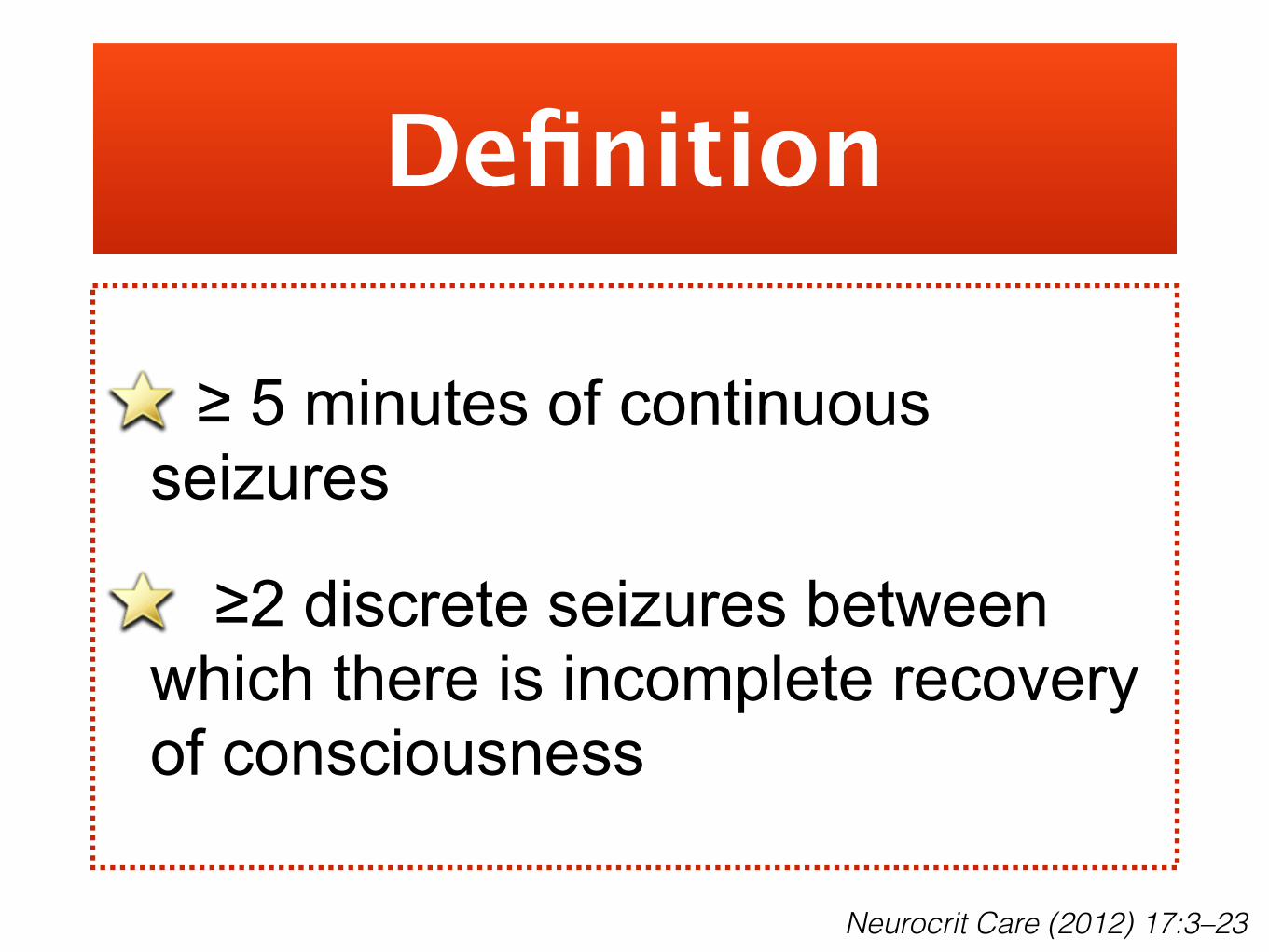
≥ 5 minutes of continuous seizures
≥2 discrete seizures between which there is incomplete recovery of consciousness
Definition
Neurocrit Care (2012) 17:3–23
Convulsive Status Epilepticus
Focal motor SE and EPC not included in these definition
Non-Convulsive Status Epilepticus (NCSE)
Electrographic seizure without clinical GCSE
Two distinct phenotype : “Wandering confused”, “Subtle status”
Classified by Semiology
Neurocrit Care (2012) 17:3–23

Cause of SE : Acute Process
Neurocrit Care (2012) 17:3–23
Metabolic disturbances: E’lyte, hypoglycemia, renal failure
Sepsis
CNS infection: meningitis, encephalitis, abscess
Stroke: ischemic stroke, ICH,SAH, CVST
Head trauma with or without epidural or subdural hematoma
Drug : toxicity, withdrawal (opioid, BZP, barbiturate, alcohol), Non-compliance with AEDs
Hypoxia, cardiac arrest
Hypertensive encephalopathy, PRES
Autoimmune encephalitis : anti-NMDA, anti-VGKC, paraneoplastic syndrome
Cause of SE : Chronic Process
Neurocrit Care (2012) 17:3–23
Preexisting epilepsy: breakthrough seizures or discontinuation of AEDs
Chronic ethanol abuse in setting of ethanol intoxication or withdrawal
CNS tumors
Remote CNS pathology (stroke, abscess, TBI, cortical dysplasia)

Diagnostic Work up
Neurocrit Care (2012) 17:3–23
Monitor vital signs.
CT scan of brain.
DTx, BS, CBC, basic metabolic panel, Ca, Mg, AED levels.
Continuous EEG monitoring
Consider : Brain MRI, CSF study, toxicology (INH, TCA, CsA, theophylline, cocaine, sympathomimetics, alcohol, organophosphates)
Complication of Status Epilepticus
Metabolic acidosis
Brain edema
Hypoglycemia
Others : arrhythmia, hyperthermia/hypothermia, hyperkalemia, DIC, rhabdomyolysis, myoglobinuria, renal failure

Stage of Status Epilepticus
Current Opinion in Neurology 2011, 24:165–170
Rapid action, Parenteral, Lipid soluble
Early 0 - 30 min Lorazepam, Diazepam
Establish 30 - 60 min Phenytoin, Phenobarbital, Valproate, Levetiracetam
Refractory > 60 min Propofol, Thiopental, Midazolam
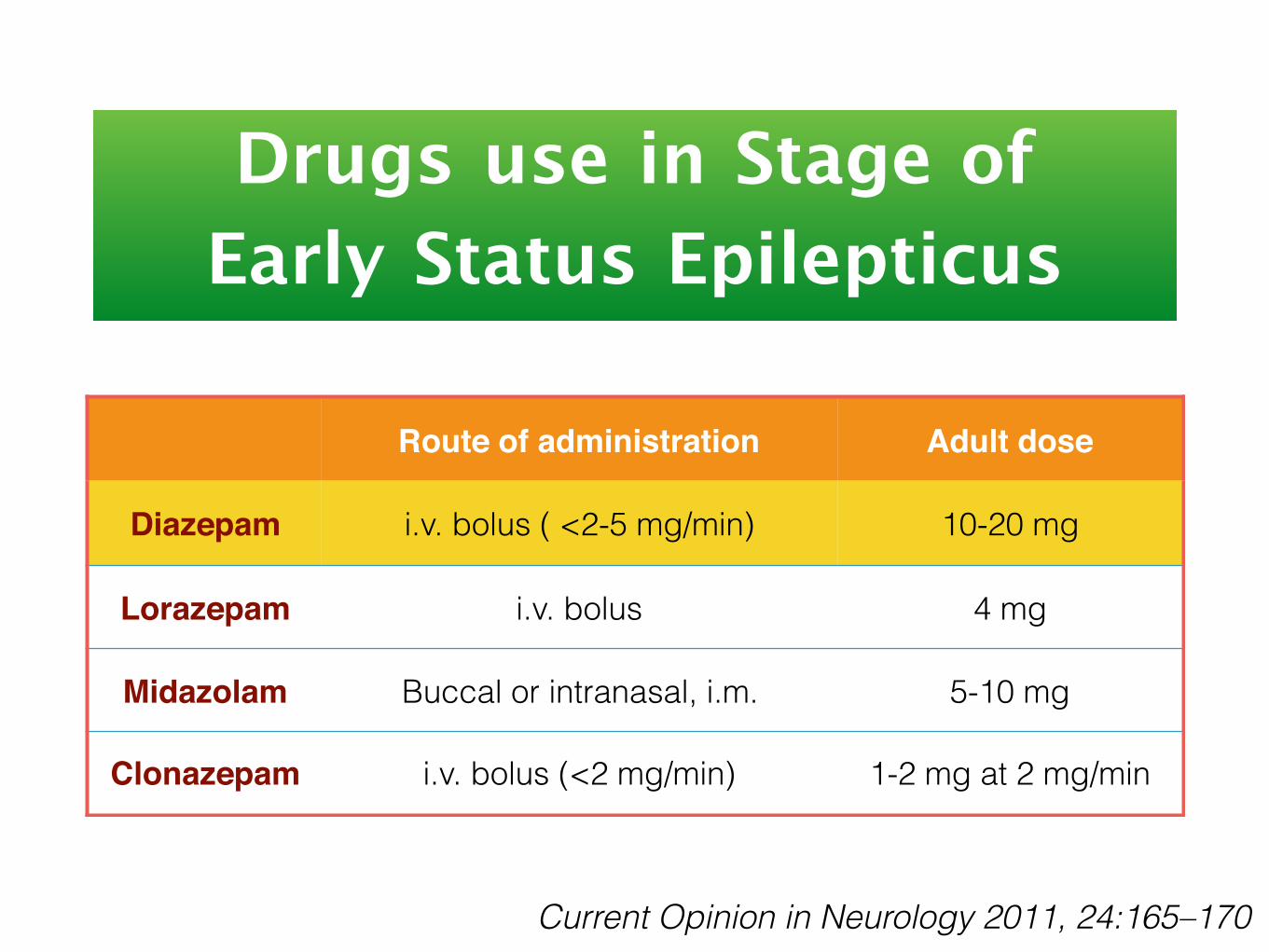
Drugs use in Stage of Early Status Epilepticus
Route of administration Adult dose
Diazepam i.v. bolus ( <2-5 mg/min) 10-20 mg
Lorazepam i.v. bolus 4 mg
Midazolam Buccal or intranasal, i.m. 5-10 mg
Clonazepam i.v. bolus (<2 mg/min) 1-2 mg at 2 mg/min
Current Opinion in Neurology 2011, 24:165–170

Drugs use in Stage of Established Status Epilepticus
Route of administration Loading Dose Continuous dose
Phenytoin i.v. bolus (<50 mg/min) 15-20 mg/kg after 8 hr 300-500
mg/d q8h
Fosphenytoin i.v. bolus (<100 mg PE/min) 15-20 mg PE/kg after 8 hr 300-500
mg/d q8 h
Phenobarbital i.v. bolus (<100 mg/min) 10-20 mg/kg after 8 hr 180-240
mg/d q12h
Valproate i.v. bolus (<50mg/min) 15-30 mg/kg 1-2 mg/kg/hr
Levetiracetam i.v. bolus in 15 min
Optimal dose not known, often use 2000-4000 mg 10-30 mg/kg q12h
Topiramate * naso / orogastric 500 mg q 12h x 2days150-750 q 12h usual effective
300-1600
Current Opinion in Neurology 2011, 24:165–170 แนวทางรักษาโรคลมชัก* small report
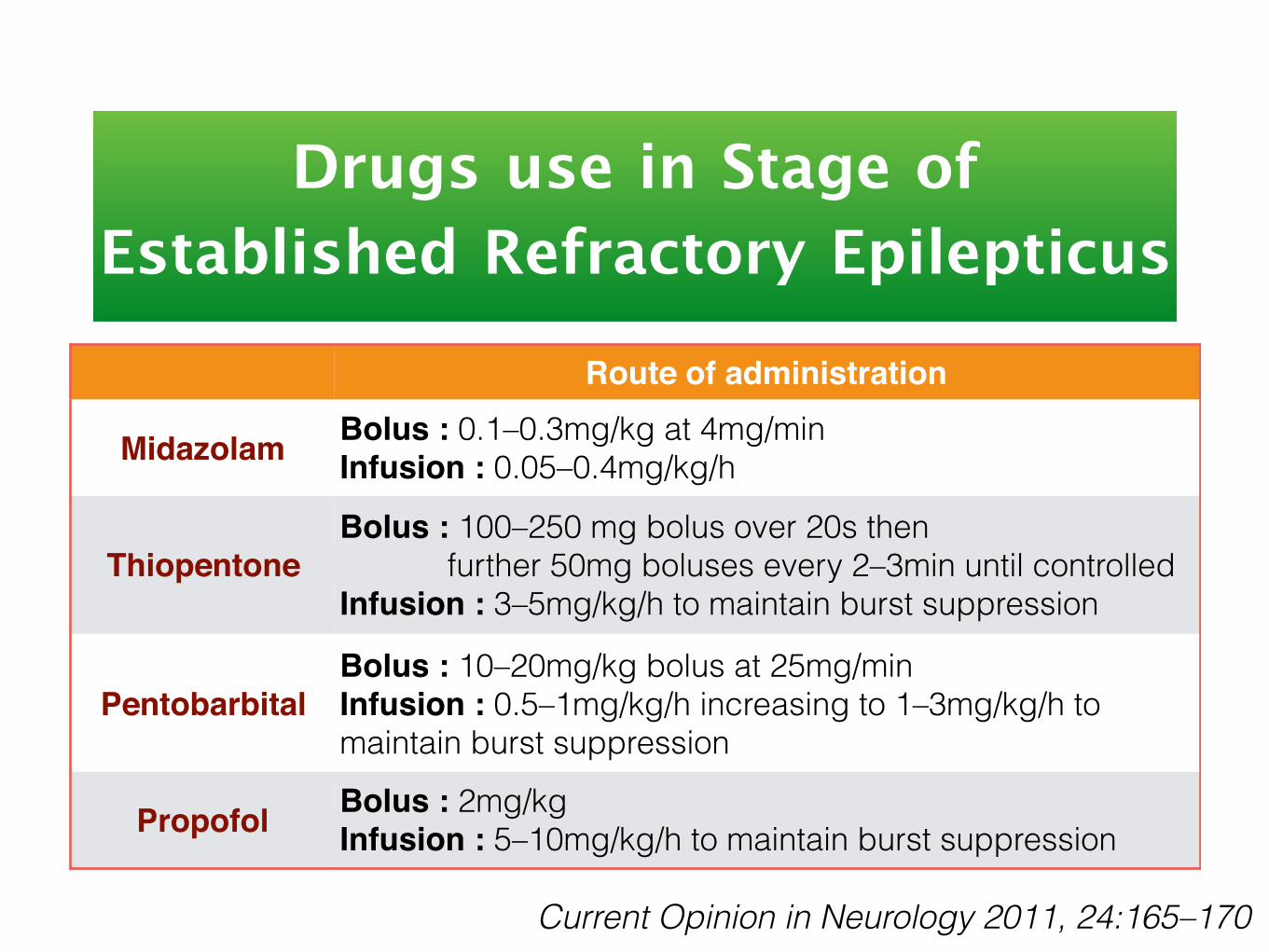
Drugs use in Stage of Established Refractory Epilepticus
Route of administration
Midazolam Bolus : 0.1–0.3mg/kg at 4mg/min Infusion : 0.05–0.4mg/kg/h
ThiopentoneBolus : 100–250 mg bolus over 20s then further 50mg boluses every 2–3min until controlled Infusion : 3–5mg/kg/h to maintain burst suppression
PentobarbitalBolus : 10–20mg/kg bolus at 25mg/min Infusion : 0.5–1mg/kg/h increasing to 1–3mg/kg/h to maintain burst suppression
Propofol Bolus : 2mg/kg Infusion : 5–10mg/kg/h to maintain burst suppression
Current Opinion in Neurology 2011, 24:165–170
Suggest reading
The End


















