
Emergence de new ALK mutations at relapse of neuroblastoma
15
Emergence of new ALK mutations at relapse of neuroblastoma Gudrun Schleiermacher MD PhD Institut Curie, Paris JCO, in press
-
Upload
siriccurie -
Category
Science
-
view
94 -
download
0
Transcript of Emergence de new ALK mutations at relapse of neuroblastoma

Emergence of new ALK mutations at relapse of neuroblastoma
Gudrun Schleiermacher MD PhD
Institut Curie, Paris
JCO, in press

Background
• Cancer : frequent secondary progression, resistance to conventional chemotherapy : therapeutic challenge
• Selection for genetic alterations during treatment• Subclonal driver mutations might play a role in tumor progression• Presence of driver mutation-harboring subclones at diagnosis, which
might expand at relapse, has been linked to adverse outcome in hematological malignancies (Landau et al, 2013)
• Different models of clonal evolution (Ding et al, 2011) : – Dominant clone evolves into relapse clone– A minor clone carrying the vast majority of primary tumor mutations
escapes and expands at relapse
Presented by: Gudrun Schleiermacher

Hallmark of neuroblastoma : clinical heterogeneity
Improvement of EFS in NB (all stages) over the last decadesBut : despite significant progress for lower stages, survival in stage 4 disease does still not exceed 40% (mortality linked to metastatic tumor progression)
Observation only Surgery Chemotherapy
ChemotherapyHigh dose chemotherapy with autologous stem cell rescueSurgeryRadiotherapyImmunotherapyMaintenance treatment
Moroz et al, 2011
Treatment of neuroblastoma :

ALK TRK plays a role in NB oncogenesis
Germline Mutations of ALK in neuroblastoma families
• Activating ALK mutations in 8 – 10% of all NB at diagnosis (Mosse et al, Janoueix-Lerosey et al, Chen et al, George et al 2008; De Brouwer et al, 2010)
• Report of a relapse-specific ALK mutation (Martinsson et al, 2011)
• Objectives of this study : Determine the frequency of ALK mutations at relapse and their role in clonal evolution of NB
Somatic Mutations of ALK
SigP
LBD
TM
Kinase domain
1
26
391
401
1031
10571116
1392
1620
Y1278S TAC>TCC
N
TIRS-1, SHC, RAS-MAPKPI3K, AKT, mTOR
ALK inhibitorsCrizotinib®
MYCNALK
MYCN ALK
Genomic amplification of ALK (<2%)

Methods
• 54 paired diagnosis – relapse NB tumor samples (France, Sweden, Belgium)• 2 cell lines with corresponding tumor sample from which cell lines were
established
• Sanger sequencing
• Deep sequencing (IonTorrent PGM®, LifeTechnologies) when an ALK mutation was seen in only one of the paired samples (7 cases)• Resequencing of hotspots exon 23 and exon 25• Depth of coverage : 100,000x• 4 control cell lines (CLB-Car, SKNDZ, SJNB12, SKNAS)
Presented by: Gudrun Schleiermacher
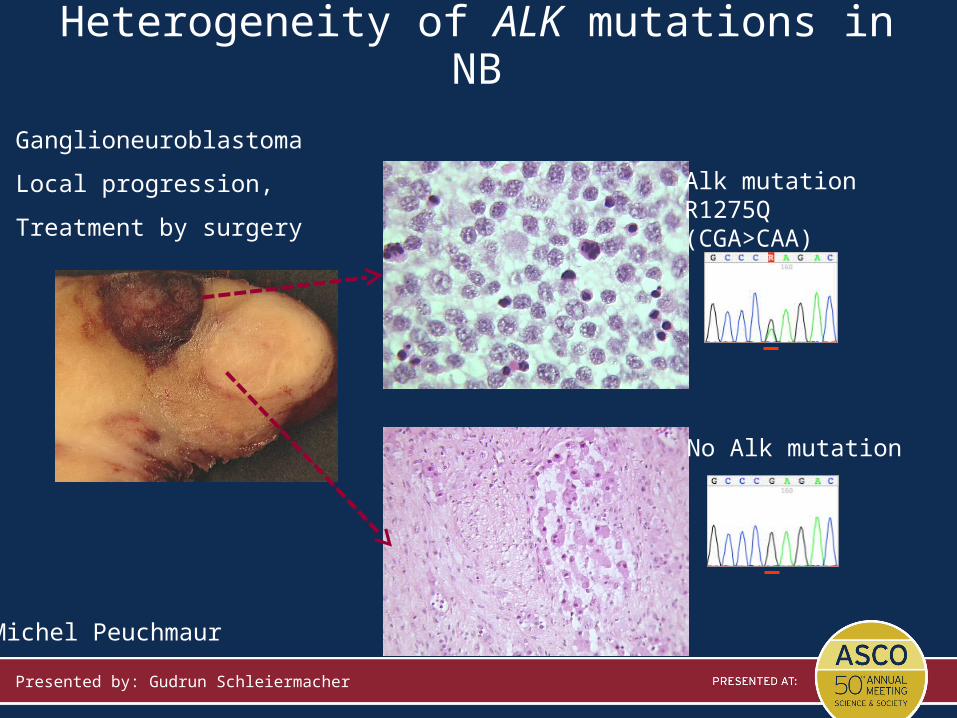
Alk mutationR1275Q(CGA>CAA)
No Alk mutation
Michel Peuchmaur
Heterogeneity of ALK mutations in NB
Ganglioneuroblastoma
Local progression,
Treatment by surgery
Presented by: Gudrun Schleiermacher

5/54 new ALK mutations at relapse
All pts with ALK mutations at diagnosis also had ALK mutations at relapse
Results (Sanger sequencing): 14/54 Alk mutationsClinical information ALK mutation
ALKDetection by Sanger
Patient N°Age at diag
(months)stage (INSS)
Interval diagnosis-relapse (months)
relapse typeFU
(months from diagnosis)
Outcome Genomic profile AA change Diagnosis Relapse
NBG03 50 4 23 loc 29 DOD MNA F1174L pos pos
NBG14 90 4 10 loc 55+ NED S F1174L pos pos
NBG21 41 2b 11 met 17 DOD MNA F1174L pos pos
NB0175 101 2b 93 loc +meta 150 DOD S Y1278S pos pos
NB0399 0.2 4s 6 meta 136 DOD N R1275Q pos pos
NB0824 3 4 3 meta 16 DOD N F1174L pos pos
NB1269 14 4 10 loc 11 DOD S L1196M pos pos
NB1224 24 2b 4 loc 14 NED S R1275Q pos pos
NB0073 3 4s 7 meta 272 NED N T1151R pos pos
NBG05 37 4 45 loc +meta 50 DOD MNA R1275Q neg pos
NBG12 12 4 9 meta 9 DOD S F1174S neg pos
NBG17 29 4 13 meta 24 DOD MNA F1174L neg pos
NB1382 4 4 51 loc +meta 63 DOD S Y1278S neg pos
NB0308 3 2b 21 loc 93 NED N F1174L neg pos
Presented by: Gudrun Schleiermacher

Methods• 54 paired diagnosis – relapse NB tumor samples
• 2 cell lines and tumor sample from which cell lines were established
• Sanger sequencing • Deep sequencing (IonTorrent PGM®) when an ALK mutation was seen in only
one of the paired samples (7 cases)• Resequencing of hotspots exon 23 (hotspot F1174) and exon 25 (hotspot
R1275)• Depth of coverage : 100,000x• 4 control cell lines (CLB-Car, SKNDZ, SJNB12, SKNAS)
Exon 25 Exon 23
Presented by: Gudrun Schleiermacher

Analysis of noise (control cell lines):
Y1278 R1275
F1174
Exon 25
Exon 23
Presented by: Gudrun Schleiermacher

Chr position /patient n°
# reads A C G T
chr2:29432655 (A) Y1278S # reads % p-value % p-value % p-value % p-valueNB1382_D 226371 99.954 1.00E+00 0.011 1.00E+00 0.031 1.00E+000 0.004 1.00E+00NB1382_R 179938 66.326 <1E-016 33.613 <1E-016 0.032 1.00E+000 0.029 1.82E-015Controls (n=4) SD SD SD SDTotal of all reads 701987 99.941 NA 0.012 NA 0.043 NA 0.004 NA Mean 99.942 2.49E-003 0.012 4.67E-003 0.043 3.07E-003 0.004 2.51E-003chr2:29432664 (A) R1275Q # reads % p-value % p-value % p-value % p-value NB1224_D 258308 14.164 <1E-016 0.064 <1E-016 85.755 <1E-016 0.016 1.00E+000NB1224_R2 302176 0.035 1.00E+000 0.001 1.00E+000 99.952 1.00E+000 0.012 1.00E+000NB1224_R4 318313 0.053 1.00E+000 0.002 1.00E+000 99.935 1.00E+000 0.011 1.00E+000NB1224_R5 302918 28.536 <1E-016 0.121 <1E-016 71.329 <1E-016 0.013 1.00E+000Controls (n=4) SD SD SD SDTotal of all reads 703934 0.038 NA 0.001 NA 99.952 NA 0.009 NAMean 0.032 2.49E-003 0.012 4.67E-003 99.921 3.07E-003 0.004 2.51E-003
PGM® analysis : cases with discordant Sanger results
Cases studied by PGM®in case of discrepancies of Sanger sequencing in different samples5 patients : 13 samples2 established cell lines : 4 samples
Analysis: comparison of base frequencies observed in a given sample, at a given position, to that observed in controls (Fisher exact test)
In some cases: no evidence of ALK mutated subclones
Presented by: Gudrun Schleiermacher

T 0,048 0,101 0,039A 8,15 0,019 0,049G 0,003 19,125 0,001C 91,799 80,754 99,912
T 0,025 0,083 0,111 0,039A 0,798 26,113 30,921 0,049G 0,003 0,008 0,005 0,001C 99,175 73,796 68,963 99,912
%%
p<10-16 p<10-16
PGM (%)
NBG17_D NBG17_R1 NBG17_R2NB0308-RNB0308-D
NB0308
0
0,1
0,2
0,3
0,45
25
45
65
85
100
0
0,25
0,5
0,75
15
25
45
65
85
100
NB0308-D NB0308-R ControlNBG17-D NBG17-R1 NBG17-R2 Control
NBG17
PGM® analysis : evidence of subclonal events
NBG17 : Presence of an ALK mutated subclone (TTC> TTA; 0.798%) at diagnosis
NB0308 : ALK mutation switch (TTC> TTA/TTG) leading to the same AA change at D and R

G 0,003 0,003 0,010A 0,046 0,4 0,006C 6,609 32,378 0,015T 93,342 67,22 99,970
0
0,1
0,53
83
100
0,2
0,3
0,4
63
43
23
Ba(PT_BM) CLB-BA Control%
p<10-16
Ba(PT_BM) CLB-BA
Cell lineAge at diag
(months)
stage (INSS)
Primary sample
Cell line established
from
FU (months)
OutcomeGenomic
profileAA change
Primary sample
Cell line
CLB_Ma 9 4Abdominal
tumorbone marrow 16 DOD MNA F1174L neg
F1174L
CLB_Ba 27 4bone
marrowbone marrow 117 NED MNA F1174L neg
F1174L
Results (NB cell lines)
Presence of an ALK mutated subclone (6.6%) in the Sample from which the cell line was established

Discussion
• Sensitivity of the PGM® deep sequencing technique:• Mean overall coverage (control cell lines): >175,000X
• Errors in PGM: • vary strongly according to the genome structure : homopolymers; • possible link to sequencing errors due to polymerase slippage, errors in the chemistry
• Mean overall background variability : 0·034%+/-0·035% for each base
• Number of reads would be considered statistically different from the background (Bonferroni correction) : a variation supported by 296 reads, or observed with a frequency of 0·17%, would result in a statistically significant difference from the controls (two-sided Fisher’s exact test)
• Sensitivity 0.17% (100 fold that of Sanger sequencing , 20%)
• Limits in sensitivity : quantity of analyzed material• PCR of exon 23/25 amplicons : 50 ng of genomic DNA
• ~ 5000 (diploid) cells
• Limit of detection : 1/5000 cells; 1/10 000 haploid genomes
Presented by: Gudrun Schleiermacher

ALK in tumor progression
Clinical implicationsEncourage new biopsy at relapse!
Search for subclones:
Evaluation of frequency of ALK mutated subclones at diagnosis
ALK targeted treatment for cases with subclonal ALK mutations? further investigations in vitro and in vivo
• In NB, ALK mutations might occur as subclones at diagnosis with secondary expansion
• selective advantage during tumor progression• ALK-mutated and non-mutated cells might co-exist in an equilibrium• expansion of an ALK-mutated clone upon treatment : preferential cytotoxic
effect on ALK non-mutated clones?
NB at diagnosis
NB at relapse
When considering biomarker based ALK
targeted therapy:
Search for genetic alteration
of ALK
Presented by: Gudrun Schleiermacher

Acknowledgements
Unité INSERM 830Translational Research in Pediatric Oncology Team
Olivier DelattreJulie Cappo
Angela BelliniIsabelle Janoueix-Lerosey
Centre Léon Bérard, LyonValérie Combaret
Unité de Génétique Somatique
Gaelle PierronNathalie Clement
Eve Lapouble
Département de Pédiatrie
Jean MichonIsabelle Aerts
Clinicians and pathologists of the SFCE
Michel Peuchmaur
Plateforme de SéquençageThomas Rio FrioQuentin LeroyVirginie Bénard
Leo Colmet Daage
Department of Medical Genetics, Gotheburg, SwedenTommy MartinssonNiloufar Javanmardi
Collaborators in Sweden:Anna DjosIngrid Øra
Fredrik Hedborg*Catarina Träger
Britt-Marie HolmqvistJonas Abrahamsson
Per KognerGhent UniversityFrank Speleman Bram de Wilde









![Neuroblastoma: Biology and Therapy · neuroblastoma tumors and is the most consistently reported abnormality.[1,2] Cytogenetic analysis of near-diploid neuroblastoma tumors and cell](https://static.fdocuments.in/doc/165x107/5d4ce04a88c9930e558b554a/neuroblastoma-biology-and-therapy-neuroblastoma-tumors-and-is-the-most-consistently.jpg)







