Embryo viability associated with microassisted fertilization
19
10 Embryo viability associated with microassisted fertilization DIANNA PAYNE Handling oocytes and embryos on a daily basis tends to obscure the delicacy of the material with which we are dealing. Disenfranchised from their biological milieu, oocytes and embryos are subject to many non-physiological conditions that may be detrimental to their viability (Byatt-Smith et al, 1991; Rieger, 1992), and the developmental potential of cultured embryos is markedly reduced compared with that of embryos in vivo (Peek, 1991). In addition to non-optimal culture conditions, oocytes are subjected to invasive micromanipulative procedures designed to enhance fertilization rates and, while intervention takes place at the level of the oocyte, any damage incurred may not be apparent until after fertilization. What is the nature of this damage and does it affect viability? Is a 'pretty' embryo a viable embryo? Can embryo viability be estimated from routine morphological assessment, or are the factors that discriminate viable and non-viable embryos cryptic and therefore not amenable to observation? In this chapter, I will briefly address the question of how we measure embryo viability and then discuss embryo viability following microassisted fertilization. WHAT IS A VIABLE EMBRYO? A viable embryo is one that is capable of producing an ongoing pregnancy, so when estimating viability it is important to consider the way in which embryos are examined. Methods that destroy vitality, such as staining blastomere nuclei (Hardy et al, 1989) or electron microscopy (Sathananthan et al, 1982; Trounson and Sathananthan, 1984; Motta et al, 1988), produce valuable information but only give 'freeze-frame' pictures of the embryo at that moment in time and destroy any possibility of verifying true viability in the form of pregnancy potential. Another factor is that the embryos used are often abnormally fertilized or unsuitable for transfer or cryopreservation, and therefore they are probably not representative of truly viable embryos. Estimation of the viability of single human embryos is hampered by clinical constraints in which the identity of the successful embryo is obscured by its transfer with other embryos. Given the limitations of clinical in vitro fertilization (IVF), estimates of Baillibre' s Clinical Obstetrics and Gynaecology-- 157 Vol. 8, No. 1, March 1994 Copyright © 1994, by Bailli~re Tindall ISBN 0-7020-1844-9 All rights of reproduction in any form reserved
Transcript of Embryo viability associated with microassisted fertilization

10
Embryo viability associated with microassisted fertilization
D I A N N A P A Y N E
Handling oocytes and embryos on a daily basis tends to obscure the delicacy of the material with which we are dealing. Disenfranchised from their biological milieu, oocytes and embryos are subject to many non-physiological conditions that may be detrimental to their viability (Byatt-Smith et al, 1991; Rieger, 1992), and the developmental potential of cultured embryos is markedly reduced compared with that of embryos in vivo (Peek, 1991). In addition to non-optimal culture conditions, oocytes are subjected to invasive micromanipulative procedures designed to enhance fertilization rates and, while intervention takes place at the level of the oocyte, any damage incurred may not be apparent until after fertilization. What is the nature of this damage and does it affect viability? Is a 'pretty' embryo a viable embryo? Can embryo viability be estimated from routine morphological assessment, or are the factors that discriminate viable and non-viable embryos cryptic and therefore not amenable to observation? In this chapter, I will briefly address the question of how we measure embryo viability and then discuss embryo viability following microassisted fertilization.
WHAT IS A VIABLE EMBRYO?
A viable embryo is one that is capable of producing an ongoing pregnancy, so when estimating viability it is important to consider the way in which embryos are examined. Methods that destroy vitality, such as staining blastomere nuclei (Hardy et al, 1989) or electron microscopy (Sathananthan et al, 1982; Trounson and Sathananthan, 1984; Motta et al, 1988), produce valuable information but only give 'freeze-frame' pictures of the embryo at that moment in time and destroy any possibility of verifying true viability in the form of pregnancy potential. Another factor is that the embryos used are often abnormally fertilized or unsuitable for transfer or cryopreservation, and therefore they are probably not representative of truly viable embryos. Estimation of the viability of single human embryos is hampered by clinical constraints in which the identity of the successful embryo is obscured by its transfer with other embryos.
Given the limitations of clinical in vitro fertilization (IVF), estimates of
Baillibre' s Clinical Obstetrics and Gynaecology-- 157 Vol. 8, No. 1, March 1994 Copyright © 1994, by Bailli~re Tindall ISBN 0-7020-1844-9 All rights of reproduction in any form reserved

158 D. PAYNE
embryonic viability are usually based on the morphological appearance of living embryos and the results are correlated with pregnancy rates. The three most widely used measures of viability are: (1) continued cleavage in culture; (2) the shape and relative size of the blastomeres; and (3) the percentage of anucleate fragments. Embryo scores are usually based on a 3-5 step grading system. Good-quality embryos have regular blastomeres of a specific size for the stage of the embryo and no fragmentation, while poor-quality embryos have barely discernible blastomeres with more than 50% fragmentation (Bolton et al, 1989; Scott et al, 1991; Staessen et al, 1992; Steer et al, 1992).
In 200 natural cycles in which one embryo was transferred, Monks et al (1993) found that embryos with a good morphological appearance were more likely to implant, while Staessen et al (1992) reported that faster embryos with few fragments (< 20%) were more likely to implant than slow embryos with >20% fragmentation. In general, embryos with good morphology are associated with higher pregnancy rates, although embryos with very poor morphologies also give rise to significant numbers of pregnancies (Cummins et al, 1986; Scott et al, 1991; Staessen et al, 1992).
Development in vitro to fully expanded blastocyst may give a good indication of embryo viability. In a study of 317 spare embryos, Bolton et al (1989) found that approximately 20% of good-quality embryos developed to fully expanded blastocysts, but 5% of the poorest embryos also developed into fully expanded blastocysts. This confirms the correlation between morphology and viability but also shows that many embryos exhibiting good morphology are ultimately non-viable and some embryos with very poor morphology are viable.
While Bolton et al (1989) reported that the percentage of embryos developing to expanded blastocyst (17%) correlated closely with the implantation rate per embryo (13%), Fishel et al (1985) found that only 17.5% of fully expanded blastocysts hatched in vitro. Work in the mouse indicates that hatching rates correlate closely with implantation rates (Cui et al, 1993). Cohen et al (1991) showed a correlation between variations in zona pellucida thickness and implantation, which suggests that the blasto- cyst hatches through a thin or weaker area of the zona pellucida.
In vitro growth rates of embryos have provided valuable information regarding embryo viability. Fishel et al (1985) found that cell doubling times for routine IVF embryos ranged from 8.1 to 51.0 h compared with 16.6-23.3 h for embryos that eventually hatched. An analysis of 357 cycles in which one embryo was transferred revealed that 'fast' embryos which grow at 110% of the expected blastomere doubling rate (11.9 h in this study) were significantly more likely to produce a pregnancy, but only if associated with reasonable embryo quality (Cummins et al, 1986). As confirmation, Bolton et al (1989) found that cleavage rates did not predict blastocyst development in vitro before the four-cell stage whereas embryos with fewer fragments and regular blastomeres were more likely to develop to blastocysts. Interestingly, they also found that embryos which cleaved to eight cells at the appropriate time, thus making a successful transition through the activation of the embryonic genome (4-8-cell stage; Braude et al, 1988), were more likely to become

EMBRYO VIABILITY 159
expanded blastocysts, suggesting that this step invites a high degree of embryonic mortality (Bolton et al, 1989).
Chromosomal normality is also essential for embryo viability but cannot be determined in living cells based on morphological criteria. Cytogenetic analyses of oocytes that failed to fertilize showed that about 30-60% were chromosomally abnormal (Macas et al, 1990; Tejada et al, 1991; Almeida and Bolton, 1993) and an additional 30% were cytoplasmically immature (Almeida and Bolton, 1993). In a study of 622 oocytes from 83 cycles with less than 50% fertilization, we demonstrated that 44% had abnormalities of the zona pellucida or cytoplasm (Payne et al, 1991a). Interestingly, Van Blerkom and Henry (1992) showed that up to 36% of uninseminated oocytes showing cytoplasmic dysmorphisms were aneuploid. Cytogenetic analysis of embryos derived from normally fertilized oocytes revealed that 40% were chromosomally abnormal (Papadopoulos et al, 1989), and in another study Bongso et al (1991) found that 32% of fragmented embryos had chromo- somal anomalies. Hence, non-viable embryos are derived in part from oocytes with chromosomal abnormalities, and these abnormalities may be reflected in the abnormal morphology of oocytes and embryos.
In summary, embryo viability correlates with embryo morphology and cleavage rates, although the relationships are not absolute. Chromosomal abnormalities impact greatly on embryo viability and, interestingly, appear to be reflected to some extent in the general morphological appearance of oocytes and embryos. It appears then that both morphology and cleavage rates are useful parameters for estimating embryo viability, so these indicators will be used in this study.
MICROASSISTED FERTILIZATION TECHNIQUES
Four micromanipulative methods have been used to enhance fertilization rates in couples with severe male-factor infertility: zona drilling (ZD), partial zona dissection (PZD), subzonal insemination (SUZI) and intra- cytoplasmic sperm injection (ICSI). Each of these techniques is progres- sively more invasive, and specific aspects of each influence the viability of oocytes and embryos.
To date, we have used ZD, PZD and SUZI in our own programme. The PZD trial was divided into three parts: PZD1 in which embryos were transferred on day 2 post-oocyte recovery; PZD2 in which sucrose was used to shrink oocytes prior to PZD, day 2 transfers were used and a short regimen of immunosuppression was instituted (Cohen et al, 1990b); and PZD3 in which embryos were transferred on day 3 post-oocyte recovery, sucrose was used and patients had immunosuppression.
Zona drilling
The term zona drilling (ZD) was first coined by Gordon and Talansky (1986) to describe the technique of chemically drilling a hole in the zona pellucida using acidified Tyrode's solution. Preliminary work in the mouse looked

160 D. PAYNE
Table 1. Comparison of embryo quality at transfer in five trials of micro- assisted fertilization techniques and routine IVF.
Procedure
Day of No, of embryos embryo transfer Grade 1 Grade 2 Grade 3 Total
ZD *a 2 4 (12.1) 26 (78.8) 3 (9.1) 33 PZD1 *a 2 2 (6.1) 30(90.9) 1 (3.0) 33 PZD2 b 2 16 (41.0) 22 (56.4) 1 (2.6) 39 PZD3 b 3 16 (39.0) 20 (48.8) 5 (12.2) 41 SUZI b 3 27 (26,2) 62 (60.2) 14 (13.6) 103 Routine IVF 3 35 (40.7) 39 (45.3) 12 (14.0) 86
Values in parentheses are percentages, * Payne et al (1991b). ×2 analysis: a, ns; b, ns; a,b, p<0 .05 .
(a) Z D , 4 0 H o u r s
Number
1 2 3 4 5 6 7
Cell Number
(d) P Z D 3 40 Hours
Number 25 . . . . . . . . . . . . . . . . . . . . . . . . . . . .
t 5
0 3 4 5 6 7 8 9-12
Cell Number
64 HOurS
~ Number
o 2 131 4 5 s 7 8 9-12
Cell Number
(b) P Z D 1 , 4 0 H o u r s
Number
oo 1 2 3 4 5 6 7 9 912
Celi Number
(C) P Z D 2 , 4 0 H o u r s
Number 30
2 0 4
1o
. . . . . . . . . . . .
3 4 5 6 7 8 9-12
Cell Number
(e) S U Z } 40 Hours
Number so
S9
29
10
O 1 2 3 4 5 6 7 8 9-12
Cell Number
(f) r l V F 40 Hours
Number 5O
C 121 1 2 3 4 5 6 7 8 9-12
Cell Number
64 Hours
Number
4 0
30
2O ....
1
Cell Number
64 Hours
Number
se°° t !-I r o~V] .
1 2 3 4 5 6 7 9-12
Cell Number
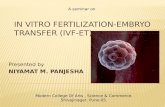
Figure 1. Comparison of growth rates for zona-drilled embryos (a) and embryos from the PZD 1 (b) and PZD2 (c) trials at 40 h following insemination; and for embryos from the PZD3 trial (d), subzonal insemination (e) and routine IVF (f) at 40 and 64 h postinsemination or injection. X 2 analysis: (a), (b)-(f) , p<0 .05 .

EMBRYO VIABILITY 161
very promising; fertilization occurred at very reduced sperm concentrations and there was normal development of ZD embryos to live young (Gordon and Talansky, 1986; Depypere et al, 1988). As a result, ZD was imple- mented as a clinical procedure to treat severe male-factor infertility, but its application in the human was disappointing. While fertilization rates improved following ZD, oocyte and embryo morphology was severely impaired and no clinical pregnancies were achieved (Cohen et al, 1988; Gordon et al, 1988; Malter and Cohen, 1989a; Ng et al, 1989; Garrisi et al, 1990; Payne et al, 1991b; Jean et al, 1992). In our trial of ZD, 24% of ZD oocytes and embryos were degenerate after 48h in culture, a rate never encountered in routine IVF, and the morphology of cleaved embryos was significantly poorer (Table 1; Payne et al, 1991b). Analysis of growth rates of the fertilized ZD oocytes revealed that cleavage was significantly slower than in intact oocytes not exposed to acid Tyrode's solution (Figure 1).
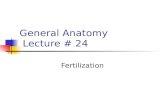
Human oocytes appear to be susceptible to low pH. The oocyte is usually covered with a fine lawn of short microvilli, but scanning electron microscopy (Santella et al, 1992) revealed that oocytes which had been exposed to acid Tyrode's solution had large patches of smooth plasma membrane divested of microvilli. A similar appearance was observed in aged oocytes. Figure 2 is a transmission electron micrograph of a ZD oocyte that has a reduced number of microvilli in the vicinity of the ZD hole (Payne et al, 1991b). This adverse effect could not have been anticipated from mouse studies, as electron microscopy demonstrated normal surface topography in ZD mouse oocytes (Depypere et al, 1988). Paradoxically, human embryos do not appear to be sensitive to low pH as zona drilling 4-8-cell human embryos with acid Tyrode's to assist hatching results in high implantation rates per embryo (Cohen et al, 1992a,b). A preliminary study of ZD using chymotrypsin as an
Figure 2. Transmission electron micrograph of a zona-drilled oocyte. Note the reduced number of mierovilli in the region of the hole (*) in the zona pel]ucida (ZP). Uranyl acetate and lead citrate staining. Bar = 2 Ixm. From Payne et al (1991b), With permission.

162 D. PAYNE
alternative to acid Tyrode's also resulted in poor embryo quality (Garrisi et al, 1990). Less aggressive drilling, however, using very low volumes (15 nl) of acid Tyrode's seems to result in improved embryo quality and three of five normally fertilized ZD oocytes developed to blastocysts (Edirisinghe et al, 1991).
In summary, ZD using acid Tyrode's has a detrimental effect on the oocyte as manifested by changes in surface topography, poor survival in vitro of ZD oocytes and embryos, and poor morphology and cleavage rates of fertilized ZD oocytes.
Partial zona dissection
Non-chemical methods of breaching the zona pellucida using a microneedle were adopted when it became apparent that ZD was detrimental to oocyte and embryo viability (Cohen et al, 1988). This is most commonly called partial zona dissection (PZD), although the terms zona cutting, zona opening and zona slitting have also been used. For convenience, PZD will be used to cover all forms of zona cutting and, although there are differences in the techniques, the final product of a cut in the zona is achieved in all. Fertilization rates generally improved following PZD, but pregnancy rates have been very variable between groups. A number of aspects of PZD affect embryo viability.
Shrinkage of oocytes in hypertonic sucrose
The perivitelline space of human oocytes is narrow compared with that of oocytes from the mouse for example, so oocytes have been shrunken to approximately 80% of their original volume in hypertonic sucrose prior to PZD (Malter and Cohen, 1989a). This enlarges the perivitelline space and allows freer passage of the needle without the risk of touching or piercing the oolemma. It also has an alarming, but apparently reversible and incon- sequential effect on the oocyte cytoplasm (Figure 3). Shrinking the oocyte may also reduce the amount of distortion and therefore mechanical damage to the oocyte during PZD,
PZD has been performed without sucrose shrinkage in some studies but the results are poor (Bourne et al, 1991; H. Bourne, personal communi- cation; Payne et al, 1991b; Simon et al, 1991). Simon et al (1991) reported a high proportion of fertilized PZD oocytes that failed to cleave (23 of 40), while 18 of 21 sibling oocytes fertilized with donor semen cleaved normally. In our PZDI trial, we found that the morphology of PZD embryos was significantly poorer than that of routine IVF embryos (Table 1; Payne et al, 1991b) although the cleavage rates were no different (Figure 1). In the subsequent PZD2 trial using sucrose shrinkage prior to PZD, embryo morphology was significantly improved and was no different from that in routine IVF (Table 1).
In some studies in which sucrose was employed, it was found that embryo morphology was poorer in the PZD group compared with routine IVF (Vanderzwalmen et al, 1992; Garrisi et al, 1993), and Garrisi et al (1990)

EMBRYO VIABILITY 163
Figure 3. (a) A PZD oocyte after 2 min in 0.1 i sucrose. Note the clear irregular area in the centre of the oocyte and the reduced cellular volume. This appearance was observed in all oocytes in sucrose. (b) The same oocyte 24 h later. The osmotic effect is temporary and does not affect viability. Eight transfers of 15 control intact oocytes subjected to 0,1 i sucrose resulted in three term, singleton pregnancies (pregnancy rate 38%). Nomarski optics; scale bar = 25 p.m.
reported a low cleavage rate of only 61% when sucrose was used. In contrast, Cohen et al (1989) reported that the degree of fragmentation and rate of cleavage in fertilized PZD oocytes was no different from those in sibling control oocytes. More significantly, pregnancies have been un- equivocally established after PZD using sucrose despite poor embryo quality (Cohen et al, 1989; Tucker et al, 1991; Vanderzwalmen et al, 1992; Levron et al, 1993), yet no pregnancies have been achieved when PZD has been performed without sucrose shrinkage. Hence, it appears that shrinking the oocyte in hypertonic sucrose is not detrimental to oocyte or embryo quality, and in fact may enhance PZD embryo viability by protecting the oocyte from mechanical distortion during PZD.
Immunosuppression PZD has been really successful in only a few groups in terms of a consistent pregnancy rate comparable with that following routine IVF (Cohen et al, 1989, 1990b; Tucker et al, 1991). Although embryo quality after PZD appears to be poorer than that in routine IVF embryos in the unsuccessful groups, it is well established that poor embryos can give rise to pregnancies. There is one very obvious difference between PZD embryos and routine IVF embryos: the cut in the zona pellucida. The length of the cut ranges from 20 Ixm (Malter and Cohen, 1989a) to up to 60-80 p.m (Figure 4; Payne et al, 1991b; Levron et al, 1993). It has been proposed that embryos with breached zonae are prone to immunological attack by leukocytes after transfer to the reproductive tract (Willadsen, 1982). This was based on a study of sheep morulae in zonae with large holes, which were embedded in defective agar coats and cultured temporarily in rabbit oviducts. On the basis of this work, Cohen et al (1990b) instituted a short regimen of

164 D. PAYNE
I ©
a b Figure 4. (a) The diameter of an oocyte is 150 Ixm; therefore a PZD cut subtending an angle of 60 ° will be 70-80 Ixm in length. (b) The cut in the zona pellucida following SUZI is the width of the injection pipette, approximately 12 Ixm.
immunosuppression using prednisolone in the hope that it would prevent leukocytic attack of PZD embryos after transfer to the uterus. They reported a significant increase in the pregnancy rate and implantation rate per PZD embryo using immunosuppression. In spite of this result, the human zona pellucida, oocyte, fertilized oocyte and early embryo do not express HLA class I or class II molecules, and as such are probably 'invisible' to the maternal immune system. It is also unlikely that developing embryos from 8 cells to implantation express HLA antigens (Desoye et al, 1991). Hence, while it is unlikely that PZD embryos are disadvantaged immuno- logically by a cut in the zona pellucida as was previously believed, it is possible that prednisolone does improve the pregnancy rate. In addition, Polak de Fried et al (1993) reported a significantly increased implantation rate (3.4% compared with 42.3%) and pregnancy rate (11.1% compared with 42.3 %) after the administration of prednisolone to patients undergoing routine IVF.
Extrusion of blastomeres
Nichols and Gardner (1989) found that zona-manipulated mouse embryos often underwent anomalous development after transfer to the oviduct, and on occasions the embryo was missing from the zona pellucida after recovery from the tract. They proposed that compression of the embryo in the female tract was sufficient to extrude blastomeres through the cut in the zona pellucida. Compaction and the formation of tight junctions between blasto- meres does not begin in human embryos until the 6-8-cell stage (Dale et al, 1991). Prior to compaction, the blastomeres have only a loose association with one another and are easily removed, as evidenced by embryo biopsy. The diameter of blastomeres in the 4-cell human embryo is 50-60 Ixm, and we have observed that single blastomeres readily pass through a 70-80 ixm cut if any pressure is applied to the zona pellucida (Figure 5). In contrast, an

EMBRYO VIABILITY
°
9 165
©
b
Figure 5, (a) Pressure applied to a four-cell PZD embryo can result in extrusion of all the blastomeres through the large cut in the zona pellucida, (b) Pressure applied to an eight-cell PZD embryo in which compaction is occurring may result in the loss of only some blastomeres.
8-cell embryo in which tight junctions have formed may be more resistant to pressure from contractions of the reproductive tract or the trauma of transfer.
It was with this in mind that we altered the day of transfer from day 2 to day 3 in our PZD3 trial (Table 1). All other conditions of culture and handling of oocytes remained constant, and the quality of transferred embryos (Table 1) and their cleavage rates (Figure 1) were no different. Patients received a short course of immunosuppression (Cohen et al, 1990b), and luteal-phase tracking was undertaken with assays for 1713- oestradiol and progesterone on days 2, 5, 8, 11 and 15 post-oocyte recovery with an additional assay for human chorionic gonadotrophin (hCG) on day 15. The three luteal-phase tracking patterns are represented in Figure 6.
The transient rise phenomenon is observed in only 5% of routine IVF cycles, but 5 of 18 patients had transient steroid rises with a negative pregnancy test on day 15 after transfer of PZD embryos on day 3 post-oocyte recovery, and three patients had steroid rises on day 11 and returned positive pregnancy tests on day 15 (Table 2). Of the PZD embryos trans- ferred on day 3, it appears that some went on to produce hCG in the late luteal phase, thus accounting for the transient rise in steroids on day 11, but because some blastomeres (not all, due to the commencement of com- paction) were lost during or subsequent to embryo transfer, the 'critical mass' of embryonic tissue required for the establishment of a viable pregnancy was not present and the pregnancy test on day 15 was negative. In contrast, we believe that PZD embryos transferred on day 2 (before

166 D. PAYNE
compaction) in our PZD2 trial lost all or most of their blastomeres during (Cohen et al, 1992c) or after transfer.
Our SUZI results also support this view. The only obvious difference between our PZD3 and SUZI embryos was the size of the cut in the zona pellucida, 70-80 t~m versus 12 I~m respectively (Figure 4). Implantation and pregnancy rates were markedly higher with SUZI (Table 2), although there were no significant differences in embryo morphology (Table 1) or cleavage rate (Figure 1).
Hardy et at (1989) postulated that biochemical pregnancies result from low numbers of inner-cell mass cells due to abnormally high rates of cell death, and studies in the human (Tarin et al, 1992) and mouse (Van Steirteghem et al, 1991) have shown that the developmental competence
(a) Non-Pregnant
Oestradiol (ng/ml) Progesterone (ng/ml)
::r-o +,.c
~ 20o hCG <5 100
2 4 6 8 10 12 14 16 18 20
D=ty Post-OPU
(b) Pregnant
Oes~mcllol (ng/ml) Progestero~ {~ltmt)
10 500
. . . . . . . 1 ' o ° ° 0 2 4 6 8 10 12 14 16 18 20
Day POSt-OPU
(c) Transient Rise/Non-Pregnant
Oestradlol (ng/ml) Progesterone (ng/ml)
-q2 ':f 1:: , I ,,. / / \ \ 1 30°
0 2 4 6 8 10 "i2 14 16 18 20
Oay Post-OPU
Figure 6. The three luteal-phase steroid patterns observed in the PZD3 trial: (a) non-pregnant profile (hCG < 5); (b) pregnant profile (hCG = 113); (c) transient rise-non-pregnant profile (hCG < 5). The transient rise-non-pregnant profile, while uncommon in routine IVF, occurred in 5 of 15 non-pregnant PZD cycles, e, 17t3-oestradiol; +, progesterone. OPU, oocyte pick up.

EMBRYO VIABILITY 167
Table 2. Comparison of pregnancy and implantation rates in five trials of microassisted fertilization techniques and routine IVF.
No. of Mean no of embryo No. of embryos per No. Implantation
Procedure transfers embryos embryo transfer pregnant rate (%)
ZD* 21 44 2.1 0 0 PZDI* 15 33 2.2 0 0 PZD2 19 39 2.0 1 (5.3) 2.6 PZD3 18 41 2.3 3 (16.7) 7,3 SUZI 52 103 2.0 16 (30.8)t 18,4 Routine IVF 32 86 2.7 7 (21.9)$ 9.3
Values in parentheses are percentages. * Payne et al (1991b). t Includes one set of twins and one set of triplets; $ Includes one set of twins.
and viability of embryos is compromised if too many blastomeres are removed or lost. It is our contention that the PZD embryos in our PZD2 and PZD3 trials were intrinsically viable and the frustratingly poor results were due to loss of blastomeres through an overly large cut (70-80 txm) in the zona pellucida during transfer or in the uterus. In this context, it is worth noting that the group that has achieved the most success with PZD (Cohen et al, 1989, 1990b) uses a much smaller cut (20 Ixm). Evidence in support of this hypothesis also comes from Cohen et al (1992c), who reported a similarly poor implantation rate of 7% after the transfer of human embryos that were subjected to PZD for assisted hatching, but once the embryo transfer catheter was changed to one that did not collect cervical mucus the implanta- tion rate increased to present levels (J. Cohen, personal communication).
In summary, shrinkage of oocytes in hypertonic sucrose prior to PZD enhances embryo viability to a level comparable with that in routine IVF embryos as measured by morphology, cleavage rates and pregnancy potential. However, PZD embryos are more fragile, owing to the cut in the zona pellucida, and need to be protected from mechanical distortion during or subsequent to embryo transfer.
Subzonal insemination
The most successful microassisted fertilization technique in terms of pregnancy rate and reproducibility of results has been subzonal injection of sperm into the perivitelline space. Since the first report of a pregnancy using this technique (Ng et al, 1988), a plethora of reports has appeared in the literature. The development of this technique has enabled clinics to treat patients with heretofore intractable semen defects.
Overall, SUZI pregnancy rates and implantation rates have been equivalent to those achieved with routine IVF in most centres, although published pregnancy rates vary from 8.6% to 50% and implantation rates per embryo from 5.9% to 44.4% (Table 3). The limited available data on the quality of SUZI embryos suggest that the cleavage rate and degree of

oo
Tab
le 3
, S
umm
ary
of n
ine
publ
ishe
d st
udie
s on
sub
zona
l in
sem
inat
ion,
No.
of
No,
of
No.
N
o, o
f N
o, o
f N
o,
No.
of
embr
yos
Stu
dy
cycl
es
SU
ZI
oocy
tes
fert
iliz
ed (
2 P
N)
tran
sfer
s em
bryo
s tr
ansf
erre
d pr
egna
nt
impl
anti
ng
Fis
hel e
t al
(19
90)
85
369
55 (
14.9
) 31
51
3
(9.7
) 4
(7.8
) al
l cli
nica
l C
ohen
et
al (
1991
)*
9 63
10
(15
.9)
6 9
3 (5
0.0)
4
(44,
4)
Fis
hel
et a
l (1
991)
13
0 53
9 69
(12
.8)
39
61
6 (1
5.4)
9
(14.
8)
all c
lini
cal
Ng
et a
l (1
991)
13
1 77
1 12
8 (1
6.6)
58
--
5
(8.6
) --
1
bioc
hem
F
ishe
l et
al
(199
2)
225
1003
15
8 (1
5.8)
82
13
9 12
(14
.6)
17 (
12.2
) al
l cl
inic
al
Pal
erm
o et
al
(199
2)
44
433
91 (
2t ,0
) 34
74
7
(20,
6)
9 (1
2,2)
3
earl
y lo
sses
S
akka
s et
al
(199
2)
150
942
115
(12.
2)
58
102
6 (1
0.3)
6
(5,9
) 3
bioc
hem
W
olf
et a
l (1
992)
46
36
3 66
(18
.2)
28
46
7 (2
5.0)
7
(15,
2)
3 ea
rly
loss
es
Imoe
dem
he a
nd S
igue
(19
93)
39
276
72 (
26.1
) 26
66
6
(23.
1)
6 (9
,1)
3 ea
rly
loss
es
Val
ues
in p
aren
thes
es a
re p
erce
ntag
es,
* D
ata
have
bee
n se
lect
ed s
o th
at o
nly
tran
sfer
s of
SU
ZI
embr
yos
are
show
n.
PN
, pr
onuc
lei.
r~

EMBRYO VIABILITY 169
fragmentat ion of S U Z I embryos is the same as for routine IVF embryos (Cohen et al, 1991; Fishel et al, 1991; Palermo et al, 1992). Da ta f rom our own series of SUZI patients suggests that the morphology of S U Z I embryos (Table 1; Figure 7) and their cleavage rates (Figure 1) are not significantly different f rom those of routine IVF embryos, and this is reflected in the high pregnancy and implantation rates (Table 2).
Intracytoplasmic sperm injection
Intracytoplasmic sperm injection (ICSI) is the newest and most exciting rnicroassisted fertilization technique developed thus far. A single spermato- zoon, chosen by the embryologist , is injected directly into the ooplasm. To
Figure 7. Micrographs of human embryos after SUZI. (a) Fertilized oocyte showing normal pronuclear development, sperm in the perivitelline space (arrow) and the small cut in the zona pellucida (small arrow) from the injection pipette. (b) A four-cell embryo 42h after SUZI, showing regular nucleated blastomeres and a few anucleate fragments (arrows). (c) A seven- cell human embryo 64 h after SUZI, with slightly irregular blastomeres for the stage of cleavage and a few anucleate fragments. (d) A poor quality five-cell embryo 64 h after SUZI, with irregular blastomeres and considerable fragmentation (arrows). This embryo produced an ongoing pregnancy. Nomarski optics; scale bar = 25 txm.

170 D. PAYNE
date, the only reports on the clinical application of ICSI have come from one group (Palermo et al, 1993; Van Steirteghem et al, 1993a,b). Fertilization rates average 65%, even with severely defective semen, and there is no polyspermy, which can be a significant problem in SUZI (Wolf et al, 1992). Clinical pregnancy rates of 39% (53 of 135) and a total implantation rate of 27% per embryo have been reported, with 90% of patients who started treatment receiving an embryo transfer (Van Steirteghem et al, 1993b). These studies suggest that embryo viability is similar to spontaneously pregnant cycles in the normal fertile population.
Other factors affecting embryo viability
A number of other factors that are common to ZD, PZD, SUZI and ICSI influence embryo viability and pregnancy potential.
Hyaluronidase
Hyaluronidase is used in most centres to disperse the cumulus oophorus, and this step is often followed by fine pipetting to strip the remaining coronal cells from the zona pellucida. The zona pellucida is a very porous structure which is permeable to molecules up to 900 kD (Hastings et al, 1972; Sellens and Jenkinson, 1975). Hyaluronidase is a molecule of only 60-90 kD, so it is probably able to penetrate the zona pellucida and, while the effect of hyaluronidase on the oocyte is unclear, Fishel et al (1992) speculated that it might be responsible for parthenogenetic activation of oocytes (one pro- nucleus and two polar bodies). Parthenogenetically activated oocytes can cleave but a high proportion exhibit more than 20% fragmentation (Staessen et al, 1993). Interestingly, Van Steirteghem et al (1993a,b) reported that reductions in the specific activity of hyaluronidase and the incubation time in hyaluronidase resulted in fewer one-pronuclear oocytes.
Discontinuity of the zona pellucida
Apart from the problem of blastomere extrusion in 4-8-cell embryos, there has been significant concern that a cut in the zona pellucida causes premature and abnormal hatching of expanded human and mouse blasto- cysts (Malter and Cohen, 1989a; Cohen, 1991). initial work with mouse embryos established that hatching occurred significantly earlier in ZD embryos, whereas PZD embryos hatched at the same time as controls (Depypere et al, 1988). In contrast, Malter and Cohen (1989b) observed that hatching of mouse embryos commenced 24 h earlier following PZD and ZD, and also observed abnormal hatching in PZD mouse embryos and in three human PZD embryos. Later work indicates that mouse PZD embryos with cuts in the zona pellucida of up to 25 p~m in size had a significantly reduced proportion of blastocysts hatching normally (30%) compared with control embryos or those with cuts of less than 1 txm (88%) (Cohen and Feldberg, 199l). Extrapolating these data to human embryos with cuts in the zona pellucida compatible in size with cuts from PZD, SUZI and ICSI, a

EMBRYO VIABILITY 171
reduced pregnancy rate may be expected (Cohen et al, 1990a), if only 30% of the 17% of embryos that develop to blastocyst after IVF hatch (BoRon et al, 1989). In fact, in those units that have been successful with microassisted fertilization techniques, the implantation rate has been equivalent to or higher than that achieved with routine IVF and, since the quality of embryos produced after microassisted fertilization is the same as that in routine IVF embryos, a small cut in the zona pellucida may in fact be beneficial to implantation by aiding the hatching process (Cohen et al, 1989).
Sperm selection
One of the major concerns with regard to microassisted fertilization has been that the normal process whereby a single spermatozoon is able to pass through the zona pellucida and fuse with the oocyte has been bypassed, and progressively more so as the invasiveness of the techniques increase. With the advent of ICSI, and to some extent SUZI, the selection of sperm is solely at the discretion of the embryologist, so the question of sperm 'normality' becomes important. During microinjection, it is possible only to distinguish the grossly abnormal sperm with misshapen heads and to some extent tail abnormalities, and the fine nuances of morphological normality outlined by Kruger et al (1986) cannot be differentiated. In SUZI, the fertilizing sperm must at least complete the acrosome reaction prior to fusing with the oolemma, but this is probably the only normal function the sperm is required to retain, as all further events leading to the formation of pronuclei are dictated and performed by the ooplasm (Tesarik and Kopecny, 1989).
Preliminary work by Kola et al (1990) showed that SUZI embryos have the same incidence of chromosomal abnormalities as conventionally fertilized ones. However, recent studies have indicated that there may be a relationship between severe teratozoospermia and reduced embryo viability. Cohen et al (1991) found that PZD embryos derived from severely teratozoospermic sperm had a very poor implantation rate, but that SUZI embryos from the same quality sperm had better rates of implantation. In contrast, Palermo et al (1993) found that embryos from severely teratozoospermic sperm had a significantly impaired implantation rate with both SUZI and ICSI. It is difficult to know what to make of these reports until further data have accrued, but the indication is that fertilization with morphologically abnormal sperm may produce less viable embryos. Preliminary studies suggest that there is no relationship between chromosomal abnormalities and sperm morphology (Martin and Rademaker, 1988), so other factors that might explain the poor embryo viability may need to be addressed.
SUMMARY
Embryo morphology and cleavage rates represent useful, but not absolute, measures of embryo viability. Oocyte and embryo chromosomal abnor- malities affect embryo viability and are reflected to some degree in the morphology of oocytes and embryos. Microassisted fertilization techniques

172 D. PAYNE
have been successfully used to treat severe male-factor infertility. Zona drilling using acidified Tyrode's solution is detrimental to oocyte and embryo viability and should not be used. Partial zona dissection (PZD) produces viable embryos that have developmental competence no different from that of routine IVF embryos, but the oocytes should be shrunken in hypertonic sucrose prior to PZD to avoid distortion and mechanical damage. The size of the cut in the zona pellucida is also critical and should be kept to a minimum to avoid loss of blastomeres during transfer. It appears from data on embryo quality, pregnancy rates and implantation rates that SUZI embryos have viability comparable to that of routine IVF embryos. Astonishingly, the passage of an injection needle directly into the ooplasm during ICSI has no effect on fertilization or developmental competence, as demonstrated by the excellent clinical pregnancy rates.
Acknowledgements
I would like to thank Dr Sean Flaherty for assistance with preparation of the manuscript, Nicholas Swann for preparation of the diagrams, and the staff of the 1VF laboratory. I also appreciate the assistance of Professor Colin Matthews and the staff of the Reproductive Medicine Unit at The Queen Elizabeth Hospital and Wakefield Clinic.
REFERENCES
Almeida PA & Bolton VN (1993) Immaturity and chromosomal abnormalities in oocytes that fail to develop pronuclei following insemination in vitro. Human Reproduction 8: 229-232.
Bolton VN, Hawes SM, Taylor CT & Parsons JH (1989) Development of spare human preimplantation embryos in vitro: an analysis of the correlations among gross morphology, cleavage rates, and development to the blastocyst. Journal of In Vitro Fertilization and Embryo Transfer 6: 30-35.
Bongso A, Ng SC, Lim Je t al (1991) Preimplantation genetics: chromosomes of fragmented human embryos. Fertility and Sterility 56: 66-70.
Bourne H, Hale L, Vassiliadis A et al (1991) The effect of zona opening prior to insemination on human embryo viability. Abstracts of the 7th Annual Meeting of the ESHRE, 105, p 105.
Braude P, Bolton V & Moore S (1988) Human gene expression first occurs between the four- and eight-cell stages of preimplantation development. Nature 332: 459--461.
Byatt-Smith JG, Leese HJ & Gosden RG (1991) An investigation by mathematical modelling of whether mouse and human preimplantation embryos in static culture can satisfy their demands for oxygen by diffusion. Human Reproduction 6: 52-57.
Cohen J (1991) Assisted hatching of human embryos. Journal of In Vitro Fertilization and Embryo Transfer 8: 179-190.
Cohen J & Feldberg D (1991) Effects of the size and number of zona pellucida openings on hatching and trophoblast outgrowth in the mouse embryo. Molecular Reproduction and Development 30: 70-78.
Cohen J, Malter H, Fehilly C et al (1988) Implantation of embryos after partial opening of oocyte zona pellucida to facilitate sperm penetration. Lancet ii: 162.
Cohen J, Malter H, Wright Get al (1989) Partial zona dissection of human oocytes when failure of zona pellucida penetration is anticipated. Human Reproduction 4: 435442.
Cohen J, Eisner C, Kort H et al (1990a) Impairment of the hatching process following IVF in the human and improvement of implantation by assisting hatching using micro- manipulation. Human Reproduction 5: 7-13.
Cohen J, Malter H, Eisner C et al (1990b) Immunosuppression supports implantation of zona pellucida dissected human embryos. Fertility and Sterility 53: 662-665.

EMBRYO VIABILITY 173
Cohen J, Alikani M, Malter HE et al (1991) Partial zona dissection or subzonal sperm insertion: microsurgical fertilization alternatives based on evaluation of sperm and embryo morphology. Fertility and Sterility 56: 696-706.
Cohen J, Alikani M, Trowbridge J & Rosenwaks Z (1992a) Implantation enhancement by selective assisted hatching using zona drilling of human embryos with poor prognosis. Human Reproduction 7: 685-691.
Cohen J, Alikani M, Reing AM et al (1992b) Selective assisted hatching of human embryos. Annals of the Academy of Medicine 21: 565-570.
Cohen J, Malter HE & Talansky BE (1992c) Microsurgical fertilization. In Brinsden PR & Rainsbury PA (eds) A Textbook of In Vitro Fertilization and Assisted Reproduction, pp 205-226. Carnforth: Parthenon.
Cui K-H, Verma PJ & Matthews CD (1993) Hatching rate: an optimal discriminator for the assessment of single blastomere biopsy. Journal of Assisted Reproduction and Genetics 10: 157-162.
Cummins JM, Breen TM, Harrison KL et al (1986) A formula for scoring human embryo growth rates in in vitro fertilization: its value in predicting pregnancy and in comparison with visual estimates of embryo quality. Journal of In Vitro Fertilization and Embryo Transfer 3: 284-295.
Dale B, Gualtieri R, Talevi R et al (1991) Intercellular communication in the early human embryo. Molecular Reproduction and Development 29: 22-28.
Depypere HT, McLaughlin K J, Seamark RF et al (1988) Comparison of zona cutting and zona drilling as techniques for assisted fertilization in the mouse. Journal of Reproduction and Fertility 84: 205-211.
Desoye G, Dohr GA & Ziegler A (1991) Expression of human major histocompatibility antigens on germ cells and early preimplantation embryos. Laboratory Investigation 64: 306-312.
Edifisinghe WR, Wales RG, Chapman HM & Yovich JL (t991) Assisted fertilization of mouse oocytes and preliminary results for human oocytes using zona drilling. Journal ofln Vitro Fertilization and Embryo Transfer 8: 48-55.
Fishel SB, Cohen J, FehiUy C et al (1985) Factors influencing human embryonic development in vitro. Annals of the New York Academy of Sciences 442: 342-356.
Fishel S, Jackson P, Antinori S et at (1990) Subzonal insemination for the alleviation of infertility. Fertility and Sterility 54: 828--835.
Fishel S, Antinori S, Jackson P e t al (1991) Presentation of six pregnancies established by sub-zonal insemination (SUZI). Human Reproduction 6: 124-130.
Fishel S, Timson J, Lisi F & Rinaldi L (1992) Evaluation of 225 patients undergoing subzonal insemination for the procurement of fertilization in vitro. Fertility and Sterility 57: 840-849.
Garrisi GJ, Talansky BE, Grunfeld L e t al (1990) Clinical evaluation of three approaches to micromanipulation-assisted fertilization. Fertility and Sterility 54: 671-677.
Garrisi G J, Chin AJ, Dolan PM et at (1993) Analysis of factors contributing to success in a program of micromanipulation-assisted fertilization. Fertility and Sterility 59: 366-374.
Gordon JW & Talansky BE (1986) Assisted fertilization by zona drilling: a mouse model for correction of oligospermia. Journal of Experimental Zoology 239: 347-354.
Gordon JW, Grunfeld L, Garrisi GJ et al (1988) Fertilization of human oocytes by sperm from infertile males after zona pellucida drilling. Fertility and Sterility 50: 68-73.
Hardy K, Handyside AH & Winston RML (1989) The human blastocyst: cell number, death and allocation during late preimplantation development in vitro. Development 107: 597- 604.
Hastings RA, Enders AC & Schalfke S (1972) Permeability of the zona pellucida to protein tracers. Biology of Reproduction 7: 288-296.
Imoedemhe DAG & Sigue AB (1993) Subzonal multiple sperm injection in the treatment of previous failed human in vitro fertilization. Fertility and Sterility 59: 172-176.
Jean M, Barriere P, Sagot P e t al (1992) Utility of zona pellucida drilling in cases of severe semen alterations in man. Fertility and Sterility 57: 591-596.
Kola I, Lacham O, Jansen RPS et al (1990) Chromosomal analysis of human oocytes fertilized by microinjection of spermatozoa into the perivitelline space. Human Reproduction 5: 575-577.
Kruger TF, Menkveld R, Stander FSH et at (1986) Sperm morphologic features as a prognostic factor in in vitro fertilization. Fertility and Sterility 46: 1118-1123.

174 D. PAYNE
Levron J, Stein DW, Brandes JM & Itskovitz-Elder J (1993) Presence of sperm in the periviteltine space predicts fertilization rate after partial zona dissection. Fertih'ty and Sterility 59: 820-825.
Macas E, Floersheim Y, Hotz E et al (1990) Abnormal chromosomal arrangements in human oocytes. Human Reproduction 5: 703-707.
Malter HE & Cohen J (1989a) Partial zona dissection of the human oocyte: a nontraumatic method using micromanipulation to assist zona pellucida penetration. Fertility and Sterility 51: 139-148.
Malter HE & Cohen J (1989b) Blastocyst formation and hatching in vitro following zona drilling of mouse and human embryos. Gamete Research 24: 67-80.
Martin RH & Rademaker A (1988) The relationship between sperm chromosomal abnor- malities and sperm morphology in humans. Mutation Research 207: 15%164.
Monks NJ, Turner K, Hooper MAK et al (1993) Development of embryos from natural cycle in-vitro fertilization: impact of medium type and female infertility factors, ttuman Repro- duction 8: 266-271.
Motta PM, Nottola SA, Micara G & Familiari G (1988) Ultrastructure of human unfertilized oocytes and polyspermic embryos in an IVF-ET program. Annals of the New York Academy of Sciences 541: 367-383.
Ng SC, Bongso A, Ratnam SS et al (1988) Pregnancy after transfer of sperm under zona. Lancet ii: 790.
Ng SC, Bongso A, Chang S-I et al (1989) Transfer of human sperm into the perivitelline space of human oocytes after zona-drilling or zona-puncture. Fertility and Sterility 52: 73-78.
Ng SC, Bongso A & Ratnam SS (1991) Microinjection of human oocytes: a technique for severe oligoasthenoteratozoospermia. Fertility and Sterility 56:1117-1123.
Nichols J & Gardner RL (1989) Effect of damage to the zona pellucida on development of preimplantation embryos in the mouse. Human Reproduction 4: 180-187.
Palermo G, Joris H, Devroey P & Van Steirteghem AC (1992) Induction of acrosome reaction in human spermatozoa used for subzonal insemination. Human Reproduction 7: 248-254.
Palermo G, Joris H, Derde M-P et al (1993) Sperm characteristics and outcome of human assisted fertilization by subzonal insemination and intracytoplasmic sperm injection. Fertility and Sterility 54: 826-835.
Papadopoulos G, Templeton AA, Fisk N & Randall J (1989) The frequency of chromosome anomalies in human preimplantation embryos after in vitro fertilization. Human Repro- duction 4: 91-98.
Payne D, Barry M, Warnes GM & Matthews CD (1991a) Oocyte abnormality as a factor contributing to fertilization failure in vitro. Proceedings of Xth Annual Scientific Meeting of The Fertility Society of Australia, p 113.
Payne D, McLaughlin KJ, Depypere HT et al (1991b) Experience with zona drilling and zona cutting to improve fertilization rates of human oocytes in vitro. Human Reproduction 6: 423-431.
Peek J (1991) Assessment of embryos from in vitro fertilization. Reproduction, Fertility, and Development 3: 113-117.
Polak de Fried EP, Btanco L, Lancuba S & Asch RH (1993) Improvement of clinical pregnancy rate and implantation rate of in-vitro fertilization-embryo transfer patients by using methylprednisone. Human Reproduction 8: 393-395.
Rieger D (1992) Relationships between energy metabolism and development of early mammalian embryos. Theriogenology 37, 75-91.
Sakkas D, Lacham O, Gianaroli L & Trounson A (1992) Subzonal sperm microinjection in cases of severe male factor infertility and repeated in vitro fertilization failure. Fertility and Sterility 57: 1279-1288.
Santella L, Alikani M, Talansky BE et al (1992) Is the human oocyte plasma membrane polarized? Human Reproduction 7: 99%1003.
Sathananthan AH, Wood C & Leeton JF (1982) Ultrastructural evaluation of 8-16 cell human embryos cultured in vitro. Micron 13: 193-203.
Scott RT, Hofmann GE, Veeck LL et al (1991) Embryo quality and pregnancy rates in patients attempting pregnancy through in vitro fertilization. Fertility and Sterility 55: 426-428.
Sellens MH & Jenkinson EJ (1975) Permeability of the mouse zona pellucida to immuno- globulin. Journal of Reproduction and Fertility 42: 153-157.
Simon A, Younis J, Lewin A et al (1991) The correlation between sperm cell morphology and

EMBRYO VIABILITY 175
fertilization after zona pellucida slitting in subfertile males. Fertility and Sterility 56: 325-331.
Staessen C, Camus M, Bollen N et al (t992) The relationship between embryo quality and the occurrence of multiple pregnancies. Fertility and Sterility 57: 626-631.
Staessen C, Janssenswillen C, Devroey P & Van Steirteghem AC (1993) Cytogenetic and morphological observations of single pronucleated human oocytes after in vitro ferti- lization. Human Reproduction 8: 221-223.
Steer CV, Mills CL, Tan SL et al (1992) The cumulative embryo score: a predictive embryo scoring technique to select the optimal number of embryos to transfer in an in vitro fertilization and embryo transfer programme, Human Reproduction 7: 117-119.
Tarin JJ, Conaghan J, Winston RML & Handyside AH (1992) ttuman embryo biopsy on the 2nd day after insemination for preimplantation diagnosis: removal of a quarter of embryo retards cleavage. Fertility and Sterility 58: 970-976.
Tejada MI, Mendoza R, Corcostegui B & Benito JA (1991) Chromosome studies in human unfertilized oocytes and uncleaved zygotes after treatment with gonadotropin-releasing hormone analogs. Fert:Tity and Sterility 56: 874-880.
Tesarik J & Kopecny V (1989) Developmental control of the human male pronueleus by ooplasmic factors. Human Reproduction 4: 962-968.
Trounson A & Sathananthan AH (1984) The application of electron microscopy in the evaluation of two- to four-cell human embryos cultured in vitro for embryo transfer. Journal of ln Vitro Fertilization and Embryo Transfer 1: 153-165.
Tucker M J, Bishop FM, Cohen Je t al (1991) Routine application of partial zona dissection for male factor infertility. Human Reproduction 6: 676-681.
Van Blerkom J & Henry G (1992) Oocyte dysmorphism and aneuploidy in meiotically mature human oocytes after ovarian stimulation. Human Reproduction 7: 379-390.
Vanderzwalmen P, Barlow P & Nijs M et al (1992) Usefulness of partial dissection of the zona pellucida in a human in vitro fertilization programme. Human Reproduction 7: 537-544.
Van Steirteghem A, Liu J, Van Den Abbeel E et al (1991) In vitro fertilization and pre- implantation diagnosis. In Verlinsky Y e t al (eds) Preimplantation Genetics. Plenum Publishing Corporation. As sighted in Liabaers I, Sermon K, Lissens W e t al (1992) Preimplantation diagnosis. Human Reproduction 7: 107-110.
Van Steirteghem AC, Liu J, Joris HH et al (1993a) Higher success rate by intercytoplasmic sperm injection than by subzonal insemination. A report of a second series of 300 consecutive treatment cycles. Ituman Reproduction 8: 1055-1060.
Van Steirteghem AC, Nagy Z, Joris H et at (1993b) High fertilization and implantation rates after intracytoplasmic sperm injection. Human Reproduction 8: 1061-1066.
Willadsen SM (1982) Micromanipulation of embryos of the large domestic species. In Adams CE (ed,) Mammalian Egg Transfer, pp 185-210. Boca Raton, Florida: CRC Press.
Wolf JPh, Ducot B, Kunstmann JM et al (1992) Influence of sperm parameters on outcome of subzonal insemination in the case of previous IVF failure. Human Reproduction 7: 1407-1413.