Embrology - Quick Review for Otorhinolaryngology Postgraduates · o Internal Constrictor – (5th...
8
LARYNX • Emryology • Development • Situation • Functions • Anatomy • Ligaments and membranes of larynx Embrology : Develops from TRACHEOBRONCHIAL DIVERTICULUM in ventral wall of primitive pharynx during 4 th week just below hypobranchial eminence. Groove deepens (caudally to cranially) septum separates Tracheobronchial TUBE from pharynx and oesophagus forming oesophageotracheal septum. Airway epithelium develops from the ENDODERMAL lining of this tube. Caudally this tube only form 2 branches leading on to 2 main bronchii and also 2 lung buds develop Cranially Primitive larynx, (bounded by caudal part of Hypobrachial eminence {forms Epiglottis} and laterally by ventral folds of 6 th brachial arches) Arytenoid swellings develop on each side of tracheobroncheal groove, enlarge to come close to each other and to hypo brachial eminence (caudal portion). This converts the Vertical slit like cavity into a T shaped one Initially laryngeal cavity fully closed as cleft walls adhere, after 3 rd month dissolution of clump of cells 4 th and 6 th arch nerves Superior and recurrent laryngeal nerves Epiglottis originates by fusion of anterior extensions of 4 th arches (hypobrachial eminence) indicating paired origin. Laryngeal inlet midline epiglottic swelling, paired arytenoid swellings and lateral aryepiglottic folds Vocal cords form at 8 th – 10 th week (2 months) The epiglottis is last cartilaginous tissue to develop Hyoid bone 2 nd n 3 rd arches Each primary bronchus divided into 18 to 23 generations SO THYROID CARTILAGE, EPIGLOTTIS, CRICOTHYROID AND INFERIOR CONSTRICTOR BY 4th ARCH Sup laryngeal nerve ☺ ☺ Development :
Transcript of Embrology - Quick Review for Otorhinolaryngology Postgraduates · o Internal Constrictor – (5th...

LARYNX
• Emryology
• Development
• Situation
• Functions
• Anatomy
• Ligaments and membranes of larynx
Embrology :
Develops from TRACHEOBRONCHIAL DIVERTICULUM in ventral wall of
primitive pharynx during 4th
week just below hypobranchial eminence.
Groove deepens (caudally to cranially) � septum � separates Tracheobronchial
TUBE from pharynx and oesophagus forming oesophageotracheal septum.
Airway epithelium develops from the ENDODERMAL lining of this tube.
Caudally this tube only form 2 branches leading on to 2 main bronchii and also 2 lung
buds develop
Cranially � Primitive larynx, (bounded by caudal part of Hypobrachial eminence
{forms Epiglottis} and laterally by ventral folds of 6th
brachial arches)
Arytenoid swellings develop on each side of tracheobroncheal groove, enlarge to come
close to each other and to hypo brachial eminence (caudal portion).
This converts the Vertical slit like cavity into a T shaped one
Initially laryngeal cavity fully closed as cleft walls adhere, after 3rd
month dissolution
of clump of cells
4th
and 6th
arch nerves � Superior and recurrent laryngeal nerves
Epiglottis originates by fusion of anterior extensions of 4th
arches (hypobrachial
eminence) indicating paired origin.
Laryngeal inlet � midline epiglottic swelling, paired arytenoid swellings and lateral
aryepiglottic folds
Vocal cords form at 8th
– 10th
week (2 months)
The epiglottis is last cartilaginous tissue to develop
Hyoid bone � 2nd
n 3rd
arches
Each primary bronchus divided into 18 to 23 generations
SO THYROID CARTILAGE, EPIGLOTTIS, CRICOTHYROID AND
INFERIOR CONSTRICTOR BY 4th ARCH � Sup laryngeal nerve ☺ ☺
Development :

Hypobrachial eminence � epiglottis
4th
arch � Thyroid cartilage
6th
arch � all (corniculate (Santorini’s cartilage), cuneiform
(Wrisberg), cricoid, arytenoids & tracheal cartilages)
� Angiogenesis begins in the Mesenchyme which is localised in 2 planes i.e. �
o External Constrictor– (4th
arch) � analogous to Inf constrictor &
Cricothyroid.
o Internal Constrictor – (5th
and 6th
arches) � analogous to intrinsic muscles of
larynx.
� Thyroid, cricoid and most of arytenoid is are Hyaline cartilages whereas tip of arytenoid
and rest all are fibroelastic.
� RLN enters the sixth visceral arch on each side below 6th
aortic arch artery, on left side
arch artery retains its position as ductus arteriosus so the nerve is found below the
ligamentum arteriosum after birth.
� Rt side it lies below 4th
arch artery which becomes the subclavian artery.
Situation & Anatomy :
� 2nd
to 4th
cervical vertebrae in children and 3rd
to 6th
cervical vertebrae in adults from
laryngeal inlet to inferior border of cricoid cartilage
� Higher in women
� 9 cartilages � Cuneiform, corniculate and arytenoids (ACC Paired) and Thyroid,
cricoid and epiglottis (CET unpaired)
� Larynx starts high up under the tongue in early life and with age assumes an
increasingly lower position in neck.
� AP diameter : men 36mm & women : 26mm after puberty
� Supraglottis � Superiorly – Epiglottis & aryepiglottic folds that sweep down to the
arytenoids ;; Inferiorly – false vocal cords (ventricular bands)
� Glottis � below false cords i.e. includes true vocal cords and anterior and posterior
commissure.
� Subglottis starts at 5 to 10 mm below vocal cords (some say VC only). Subglottis
becomes trachea at lower border of Cricoid only.
Functions of Larynx :
Protection of lower airway
Provision of controlled airway
Phonation
Generation of High intrathorasic pressure for coughing and lifting

Framework of Larynx :
� Hyoid Bone � 2nd
and 3rd
arch
� Only bone in body not to be attached to any other bone. Body anteriorly, greater cornu
Posterolaterally, lesser cornu at junc. of both projecting superiorly.
� Thyroid Cartilage �LAMINA Angle 90 degree in men and 120 degree in women.
Lamina prolonged posteriorly upwards as superior cornua and
downwards as inferior cornua.
Superior � attaches lateral thyrohyoid ligament
Inferior � (shorter and thicker) has facet for attachment of
Cricoid Cartilage
• Oblique line on ext surface of Lamina from superior thyroid tubercle just infront of
root of superior horn to the inferior thyroid tubercle (lower border of lamina) and marks
attatchement of Sternothyroid, Inferior constrictor muscles and Thyrohyoid ( S I T )
• In midline just below thyroid notch on inner aspect attaches Thyroepiglottic ligament
and on each side below this attaches vestibular and vocal ligaments (i.e. Thyroarytenoid).
Both vocal ligaments meet to form anterior commisure
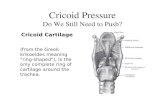
CRICOID CARTILAGE
� Deep broad lamina
posteriorly and narrow arch
anteriorly, attaches to
inferior cornu of thyroid
near junction of arch and
lamina
� Only complete
cartilaginous ring.
� Lamina has sloping
shoulders for attachment of
arytenoids
� Vertical ridge in midline of
lamina gives attachment to
longitudinal muscles of the
oesophagus
� Entire inner layer lined by
mucous membrane
*** Remember : Vocal folds aka vocal cords and vocal ligaments are inferior thyroarytenoids
enclosed within vocal folds. Vocalis muscle is the deeper and lower fibres of the
THYROARYTENOID (Vocal ligament) muscles which attatches to vocal process of Arytenoid
ARYTENOIDS

� Three sided pyramids with forward projection (vocal process) attaches to vocal folds and
lateral projection (muscular process) to which is attached posterior and lateral
cricoarytenoid
� Btw these two processes upper triangular area gives attachment to Vestibular ligament
and lower gives attachment to Lateral cricoarytenoid muscles and also vocalis.
� Apex articulates with corniculate cartilage.
� Medial surface covered with mucous membrane forms lateral boundary of posterior
glottis and posterior surface is covered by transverse arytenoid muscles
� Articulates with corniculate (elastic fibro cartilage) with synovial joint, situated in
posterior part of aryepiglottic fold
� Base attaches to cricoid lamina with both rotatory movements and side to side gliding
movements
� Posterior cricoarytenoid ligament prevents forward movement of arytenoid cartilages
� Cuneiform are 2 small elongated flakes of fibro cartilages one in each margin of
aryepiglottic fold
EPIGLOTTIS
� Attached to thyroid cartilage just below thyroid notch in midline by
THYROEPIGLOTTIC ligament and to hyoid by hyoepiglottic ligament and projects
upwards behind the tongue and body of hyoid bone.
� Preepiglottic space is space between these two (hyoepiglottic and thyroepiglottic
ligaments)
� Valleculae is space between tongue and Epiglottis. So epiglottis forms posterior wall of
valleculae
� Glossoepiglottic folds medial and lateral and aryepiglottic folds
EXTRINSIC LIGAMENTS
� Thyrohyoid � thyrohyoid membrane (fibrocartilagenous) reinforced by fibrous cartilage
as median thyrohyoid ligament and posteriorly as Lateral thyrohyoid ligament
� These may contain cartilage i.e. cartilage triticea
� Memb. pierced by superior laryngeal nerve’s internal branch and sup laryngeal vessels
� Cricotracheal ligament � is between cricoid and 1st tracheal ring
INTRINSIC LIGAMENTS
Quadrangular membrane arises from the lateral border of Epiglottis and arytenoid
cartilages. Upper memb forms framework of aryepiglottic folds and lower margin is
thickened to form the vestibular ligament underlying vestibular fold (false vocal cord)
Cricovocal Ligament / Cricothyroid Ligament Or Conus Elasticus – Lower part of
Quadrangular membrane is thickened & has elastic fibres.
Upper Border of this membrane forms true vocal cords
Anteriorly thickening of memb. called cricothyroid ligament.
Fibroelastic membrane divided into upper and lower part by the laryngeal ventricle.

MUSCLES OF LARYNX
� Intrinsic muscles of larynx are all paired
1. Posterior cricoarytenoid � opens glottis
2. Lateral cricoarytenoids � Adducts vocal cords
3. Transverse arytenoids (unpaired) � Adducts vocal cords
4. Oblique arytenoids � (posterior aspect of muscular process
of arytenoids only but superficial to
transverse arytenoids)
5. Vocalis / Thyroarytenoid � lies above n lateral to cricovocal
ligament/conus elasticus. relaxer
6. Cricothyroid � Only intrinsic muscle which lies
outside cartilaginous framework of
thyroid. Cricothyroid muscle dysfunction
may be implicated in vocal fold collapse
(lengthens the vocal folds i.e. tensor)
7. Aryepiglotticus � continuation of oblique arytenoid
(weak sphincter of laryngeal inlet)
8. Thyroepiglotticus � Widens inlet of larynx by pulling
aryepiglottic folds slightly apart
� Infrahyoid muscles � Thyrohyoid, Sternothyroid, Sternohyoid
� Suprahyoid group � GSM D SPS , Geniohyoid, Stylohyoid, Mylohyoid,
Digastric, Stylopharyngeus, Palatopharyngeus and Salpingopharyngeus
� Both stylopharyngeus and salpingo elevate larynx whereas palato. Tilts larynx
forwards
� Vocal folds overlie Conus Elasticus.
� Closers of laryngeal inlet are aryepiglotticus and Interarytenoid.
� PRIMARY ELEVATORS � Stylopharyngeus, Salpingopharyngeus, Palatopharyngeus,
thyrohyoid.
� SECONDARY ELEVATORS � GSM D
� VOCAL FOLDS are layered structures � superficial nonkeratinised stratified squamous
epithelium, underlies lamina propria � 3 layers � Rienkes space (Gelatin like),
Intermediate (Elastin fibre rich) and deep (Collagen rich layer) forms vocal ligament.


� Anterior 3/5th
of the vocal cord is within vocal folds and called intermembranous part
of the vocal cord posterior 2/5th
is called intercartilaginous
� Mucous membrane lining larynx is CLOSELY attached over posterior surface of
epiglottis, corniculate, cuneiform and vocal ligaments, elsewhere it is loosely attached
and prone to oedema.
� Most larynx lined by pseudostratified ciliated columnar respiratory type of
epithelium.
� Mucous glands numerous at posterior surface of epiglottis, lower aryepiglottic folds,
saccules.
� Vocal folds are lubricated not by own but mucous glands of saccules (OIL TANKS OF
LARYNX)
SPACES WITHIN LARYNX
Preepiglottic space – wedge shaped –
Anterior � thyrohyoid ligament and hyoid bone
Posteriorly � Epiglottis
Superiorly � hyoepiglottic ligament (continues laterally with paraepiglottic space)
Inferiorly � thyroepiglottic ligament
Paraglottic space � laterally thyroid cartilage ;;;; medially conus elasticus and quadrangular
membrane ;;;; posteriorly piriform fossa mucosa ::::: it encompasses laryngeal ventricles and
saccules
Nerve supply of larynx
� ** Some fibres of Vagus originate in Medulla in Nucleus Ambiguus and some at higher level.
Fibres from upper section of NUCLEUS AMBIGUUS Join 9th nerve i.e. glossopharyngeal nerve
and fibres from inferior portion of nucleus join ACCESORY NERVE i.e. XI nerve.
� 9 10 11 are intricately related nerves in medulla.
� Vagus has superior and inferior ganglion
� The vagus nerve leaves the skull base via the jugular foramen anterior to the jugular vein. The
vagus then assumes a more posterior position medial to the jugular vein.
� The vagus nerve has an inferior ganglion also known as the Nodose ganglion immediately below
the jugular foramen.
� The course taken by the vagus nerve differs between the right and the left sides. The left vagus
nerve follows the carotid artery into the mediastinum crossing anterior to the aortic arch.
� The anterior bronchoesophageal artery supplies the left vagus nerve.
� The approximate length of the left recurrent laryangeal nerve is 12 cms, whereas the right
nerve measures about 6 cms only.

� The blood supply to the recurrent laryngeal nerve comes from the inferior thyroid artery.
� SLN arises from inf ganglion of vagus (nodose ganglion) below level of jugular foramen and
receives branch from Superior cervical sympathetic ganglion � goes behind ICA to sides of
pharynx at level of greater horn of hyoid bone divides into small ext and large int branch
� External br. Supplies Cricothyroid (motor)
� Internal pierces thyrohyoid and divides further into sensory and secretomotor.
� Laryngeal inlet has max sensory innervation
� Vocal folds have lower sensory innervation
� 3 branches from Internal Laryngeal nerve supply valleculae, epiglottis and pyriform fossa.
� Also carries afferents for neuromuscular spindles and other stretch receptors in the larynx.
� SLN ends by piercing inferior constrictor and joining asc. b/o recurrent laryngeal nerve (Galen’s
anaestomosis and is purely sensory)
� Recurrent Laryngeal Nerves �
� As the vagus nerve exits the medulla, the fibres of the recurrent laryngeal nerve are anteriorly
situated in it.
� As the vagus traverses inferiorly, the fibres of the recurrent laryngeal nerve starts to rotate
medially until they are ultimately separated from the vagus nerve.
� Rt originates from main trunk of vagus in front of subclavian and lt in front of Arch of Aorta. Lt
more liable to injury.
� Both run in the groove between trachea and oesophagus and divided into anterior and posterior
branches before entering the larynx.
� RLN pass deep to lower border of inferior constrictor muscles and enters larynx behind
cricothyroid ligament. � divides into motor and sensory � sensory supplies below level of vocal
folds and all muscles of larynx by motor.
Arterial Supply
� Laryngeal artery � b/o Superior and inferior thyroid arteries
� Cricothyroid � b/o superior thyroid artery
� VENOUS � Above vocal fold and below vocal fold drainage.
� Superior thyroid drains in internal jugular
� INFERIOR THYROID VEIN drain into brachiocephalic vein








![v ] o v Àsinoemedicalassociation.org/anatomyphysiology/cranialnerves.pdf · Retina Superior/ middle/inferior rectus, i nferior oblique, levator palpebrae. Pupillary constrictor,](https://static.fdocuments.in/doc/165x107/5e3fa1668870a77ea0333b64/v-o-v-sin-retina-superior-middleinferior-rectus-i-nferior-oblique-levator.jpg)