
Embriologi Gastro
50
DEVELOPMENT OF GASTROINTESTINAL TRACT Block: Gastro Dr Anggraini Barlian
Transcript of Embriologi Gastro
DEVELOPMENT OFGASTROINTESTINAL TRACT
Block: Gastro
Dr Anggraini Barlian
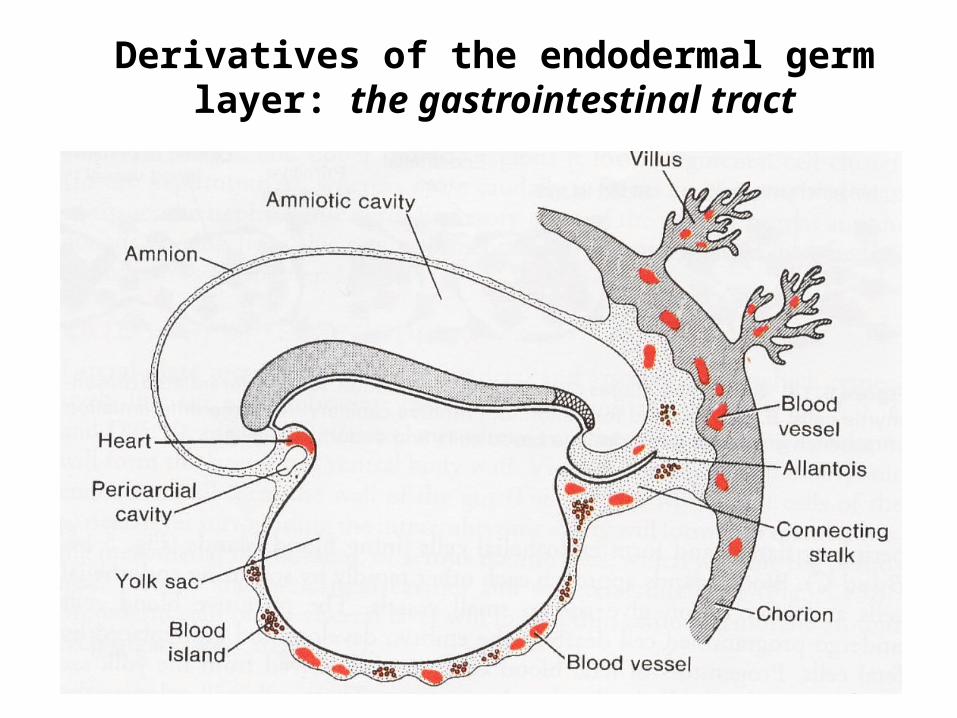
Derivatives of the endodermal germ layer: the gastrointestinal tract
Gastrointestinal tube and its derivatives
• Anterior-Posterior: pharynx, gastrointestinal tube (GI) esophagus, gut, small intestine & large intestine.
• Endoderm cells become epithelial lining digestive tube and glands.
• Mesenchyme/ mesodermal cells will surround the tube and become peristaltic muscles.
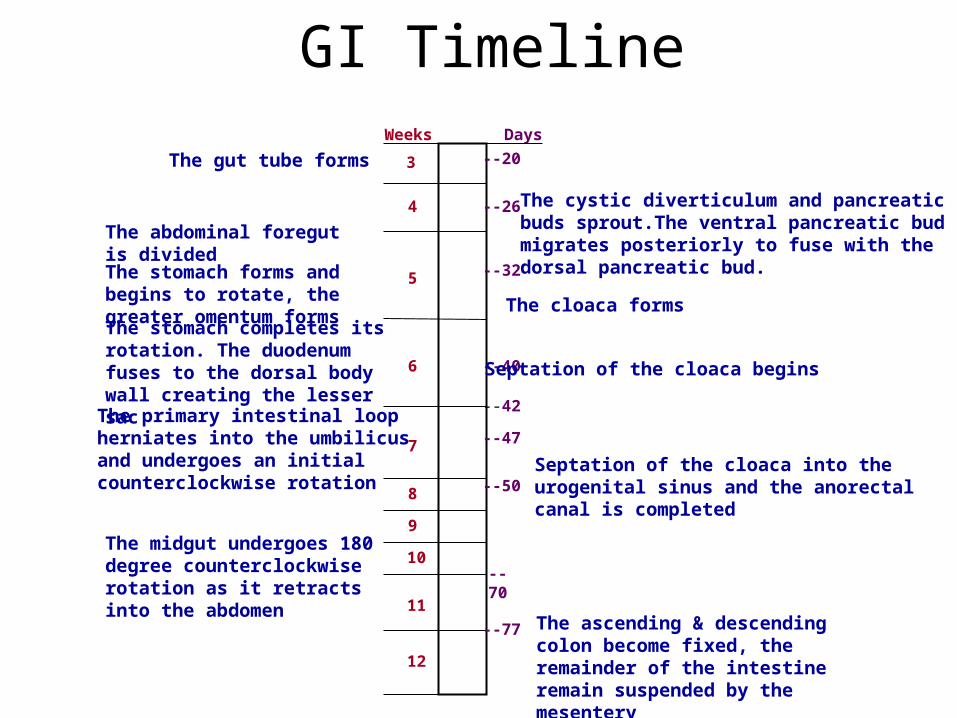
GI TimelineWeeks Days
3
4
5
6
7
8
9
10
11
12
--20
--26
--32
--40
--42
--47
--50
--70
--77
The gut tube forms
The stomach forms and begins to rotate, the greater omentum forms
The stomach completes its rotation. The duodenum fuses to the dorsal body wall creating the lesser sac
The primary intestinal loop herniates into the umbilicus and undergoes an initial counterclockwise rotation
The midgut undergoes 180 degree counterclockwise rotation as it retracts into the abdomen
The ascending & descending colon become fixed, the remainder of the intestine remain suspended by the mesentery
The cystic diverticulum and pancreatic buds sprout.The ventral pancreatic bud migrates posteriorly to fuse with the dorsal pancreatic bud.
The cloaca forms
Septation of the cloaca begins
Septation of the cloaca into the urogenital sinus and the anorectal canal is completed
The abdominal foregut is divided
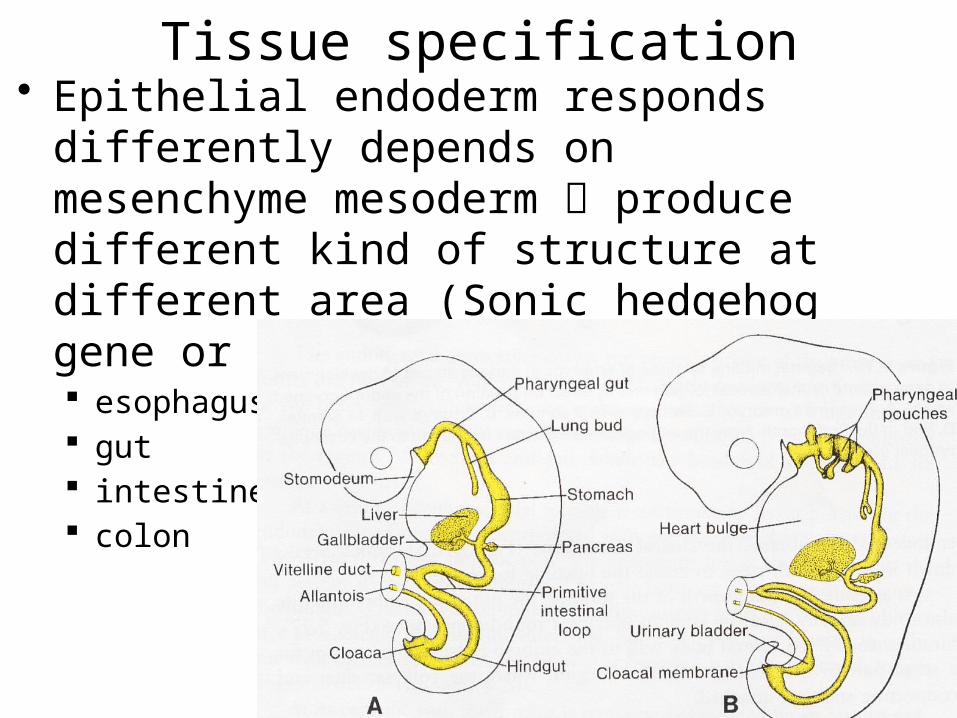
Tissue specification• Epithelial endoderm responds differently
depends on mesenchyme mesoderm produce different kind of structure at different area (Sonic hedgehog gene or Shh gene action): esophagus gut intestine colon
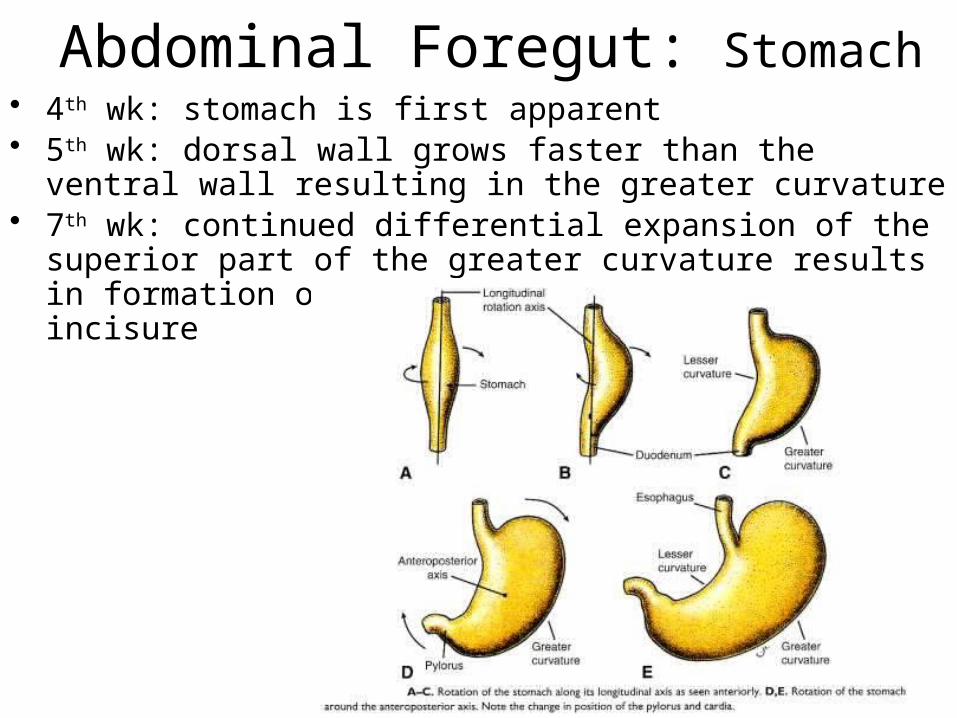
Abdominal Foregut: Stomach• 4th wk: stomach is first apparent• 5th wk: dorsal wall grows faster than the ventral wall resulting in
the greater curvature• 7th wk: continued differential expansion of the superior part of
the greater curvature results in formation of the fundus and the cardiac incisure
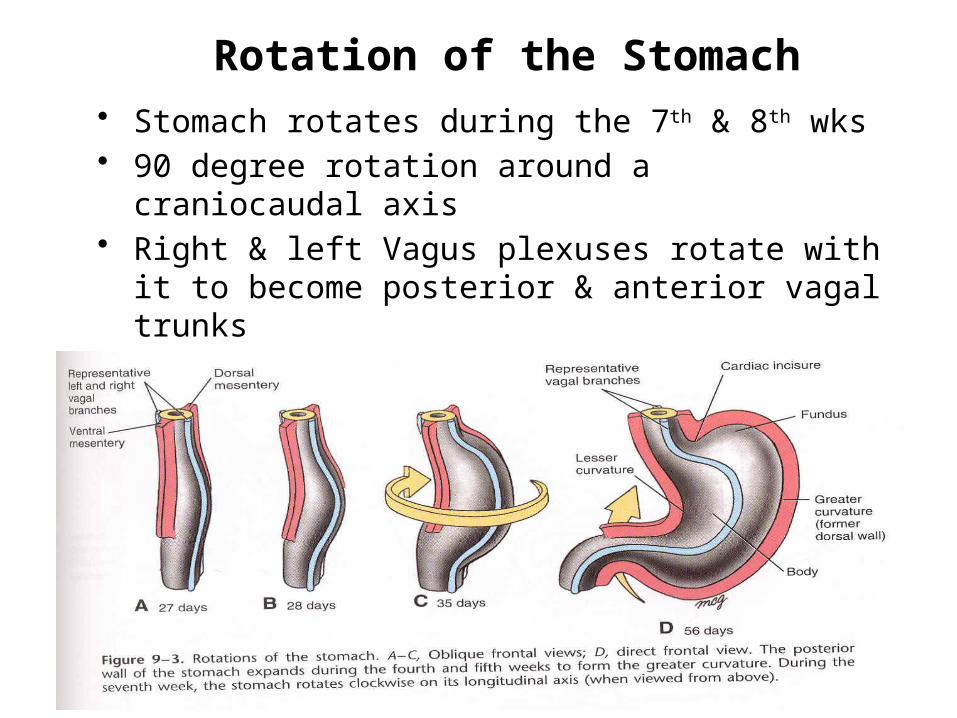
Rotation of the Stomach• Stomach rotates during the 7th & 8th wks• 90 degree rotation around a craniocaudal axis• Right & left Vagus plexuses rotate with it to become
posterior & anterior vagal trunks• The duodenum bends into a C shape from rotation of
the stomach
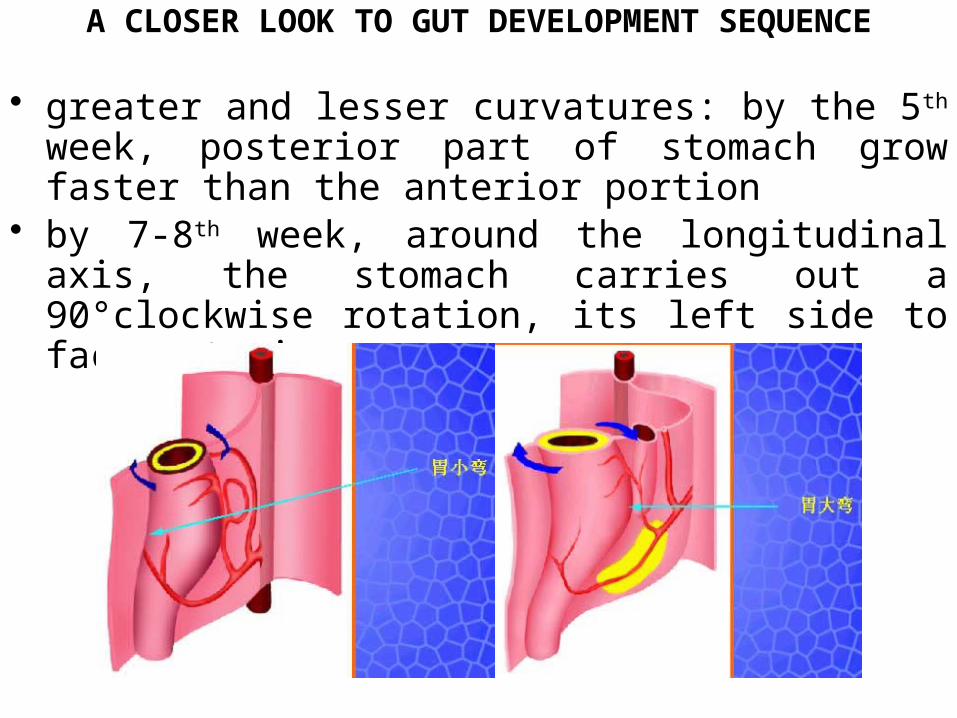
A CLOSER LOOK TO GUT DEVELOPMENT SEQUENCE
• greater and lesser curvatures: by the 5th week, posterior part of stomach grow faster than the anterior portion
• by 7-8th week, around the longitudinal axis, the stomach carries out a 90°clockwise rotation, its left side to face anterior
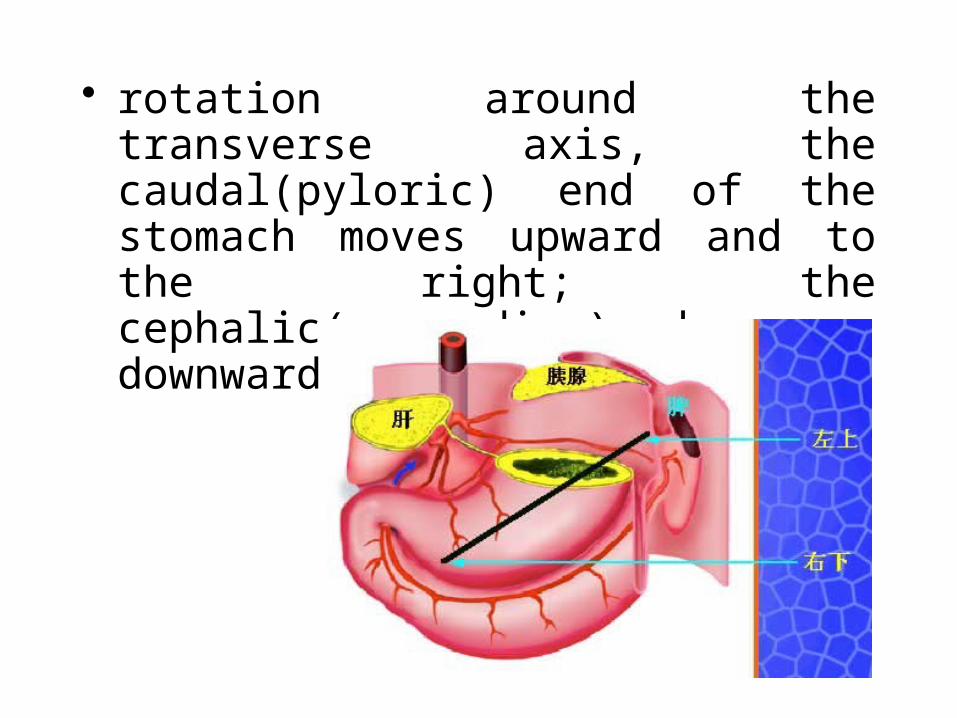
• rotation around the transverse axis, the caudal(pyloric) end of the stomach moves upward and to the right; the cephalic( cardiac)end moves downward and to the left
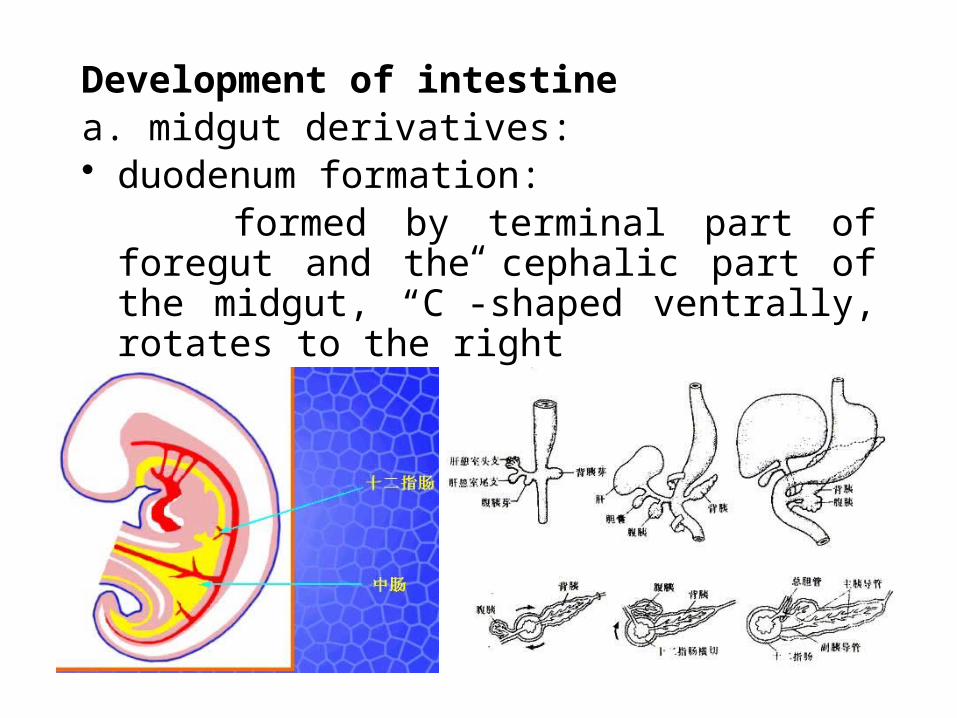
Development of intestinea. midgut derivatives:• duodenum formation: formed by terminal part of foregut and the
cephalic part of the midgut, “C”-shaped ventrally, rotates to the right
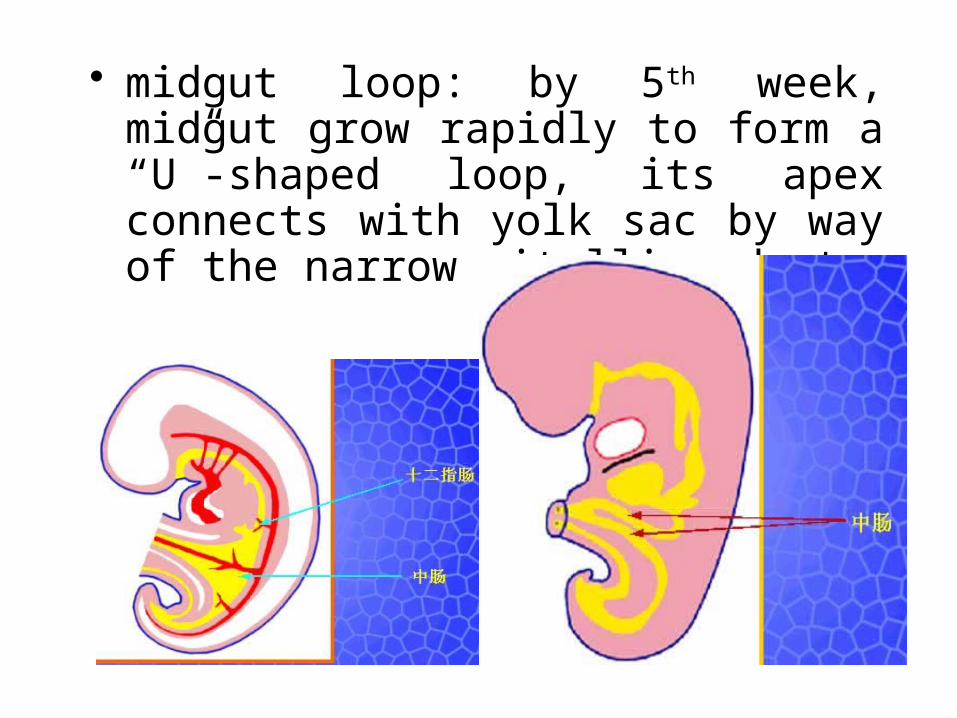
• midgut loop: by 5th week, midgut grow rapidly to form a “U”-shaped loop, its apex connects with yolk sac by way of the narrow vitelline duct
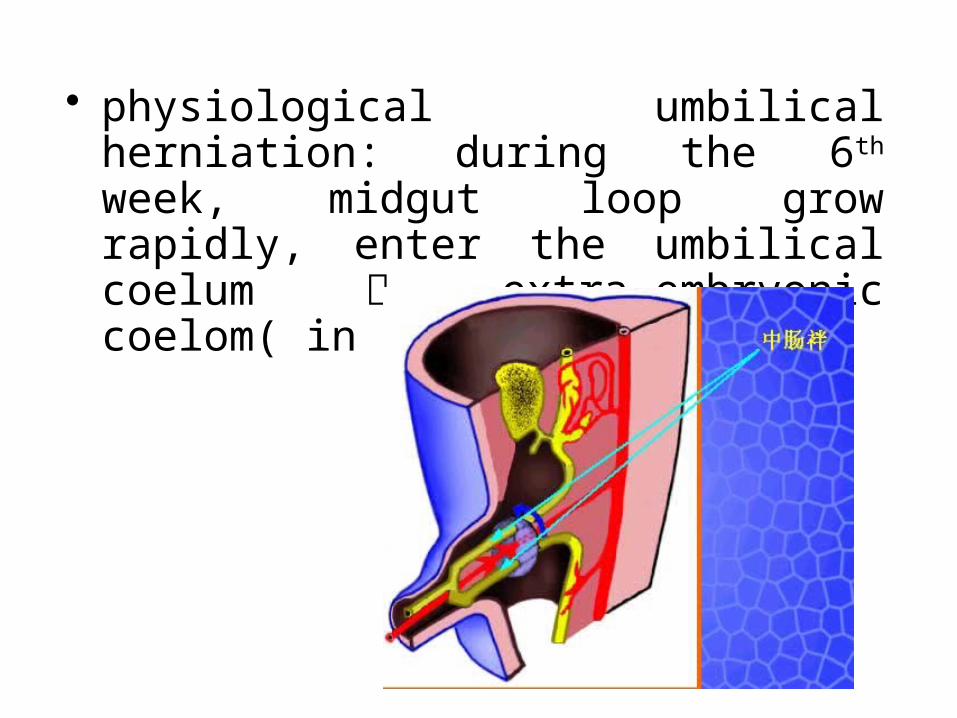
• physiological umbilical herniation: during the 6th week, midgut loop grow rapidly, enter the umbilical coelum extra-embryonic coelom( in umbilical cord)
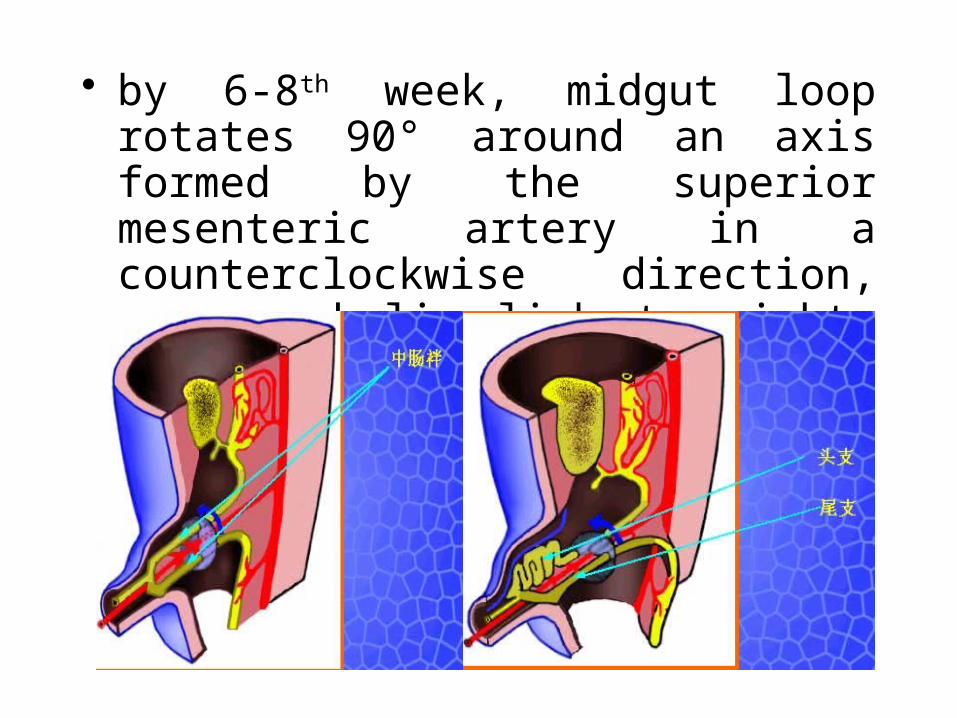
• by 6-8th week, midgut loop rotates 90° around an axis formed by the superior mesenteric artery in a counterclockwise direction, move cephalic limb to right, caudal limb left
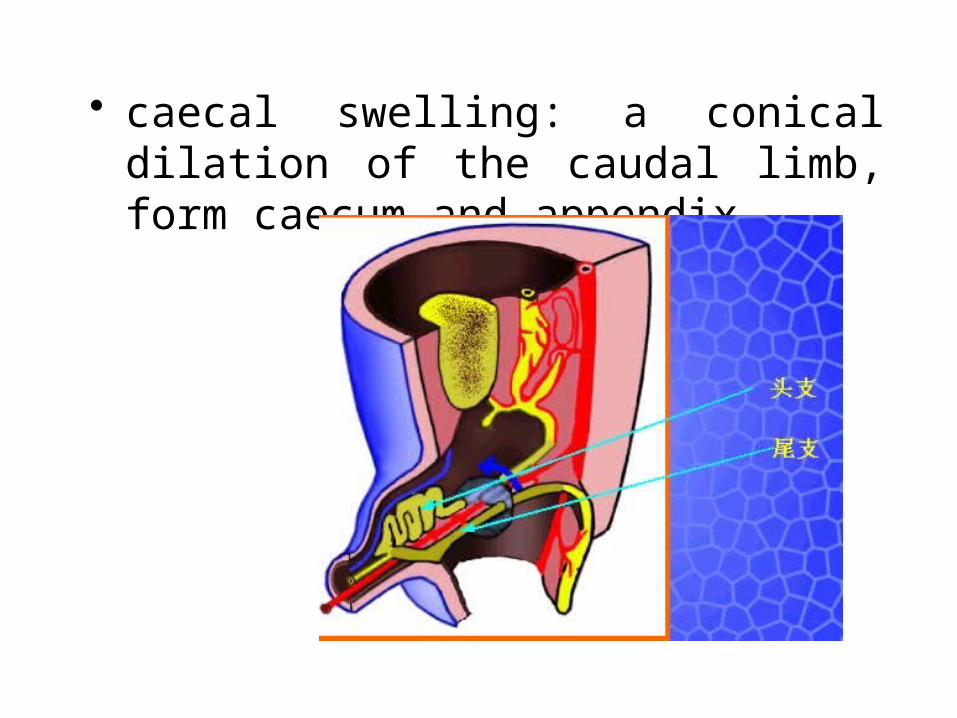
• caecal swelling: a conical dilation of the caudal limb, form caecum and appendix
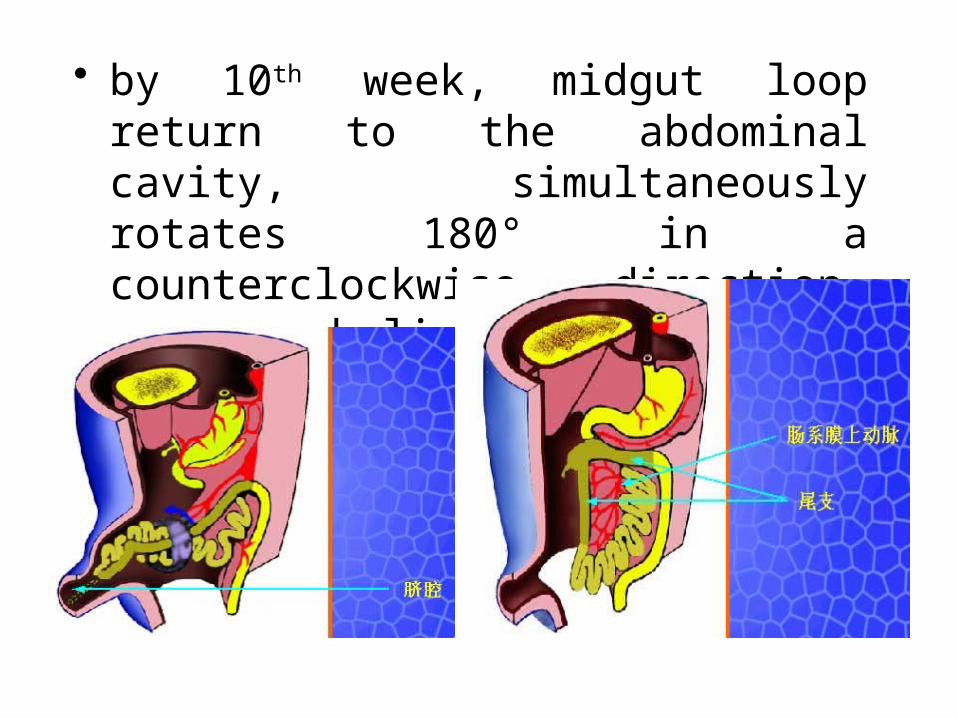
• by 10th week, midgut loop return to the abdominal cavity, simultaneously rotates 180° in a counterclockwise direction, move cephalic limb to left, caudal limb right
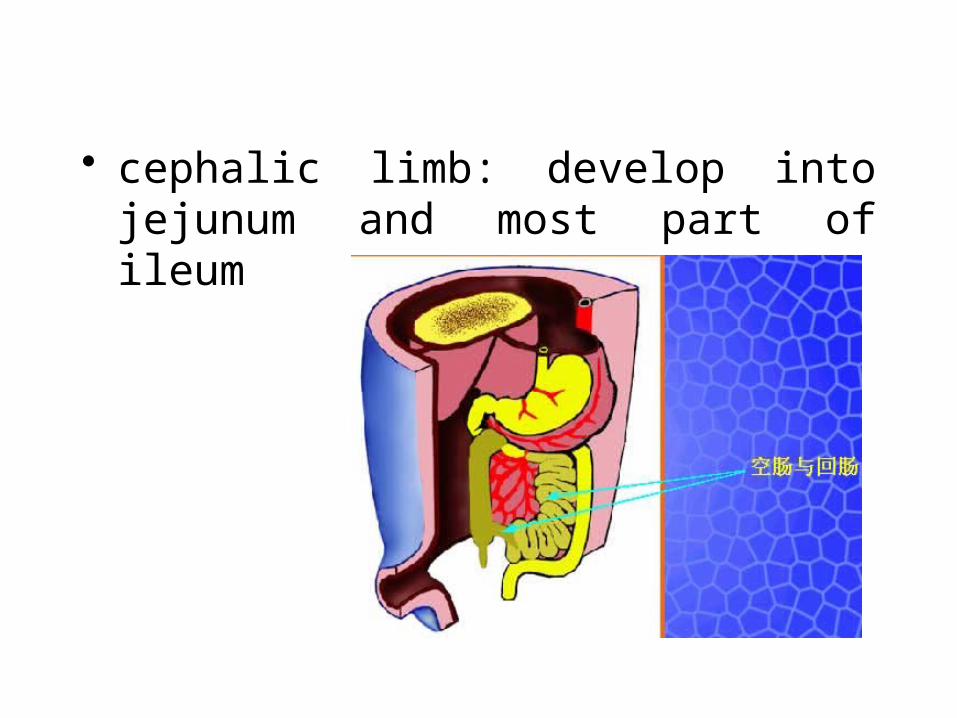
• cephalic limb: develop into jejunum and most part of ileum
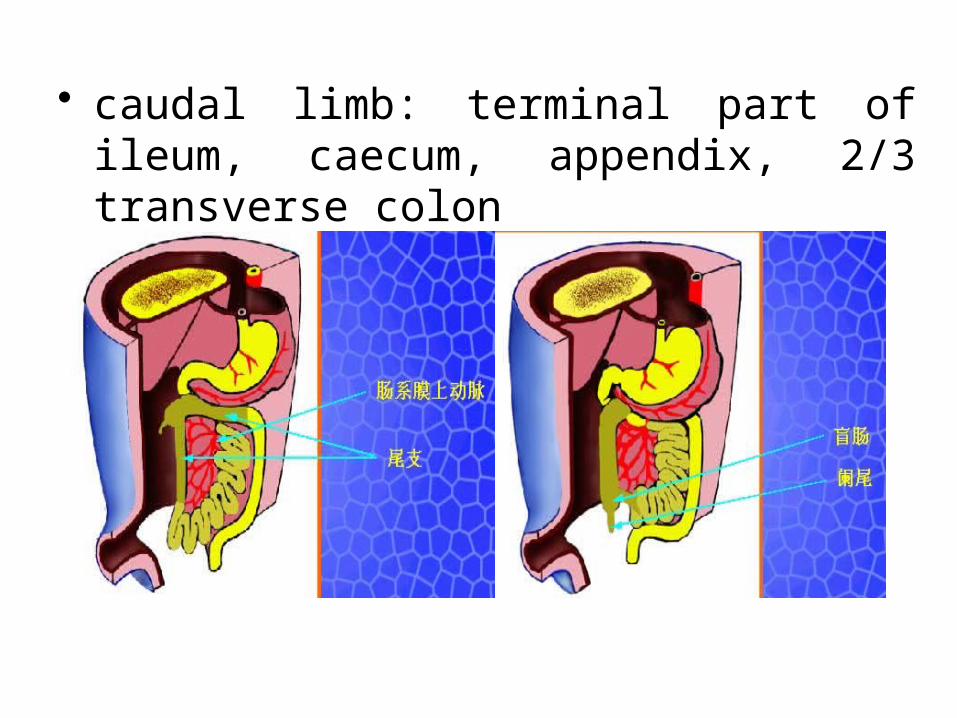
• caudal limb: terminal part of ileum, caecum, appendix, 2/3 transverse colon
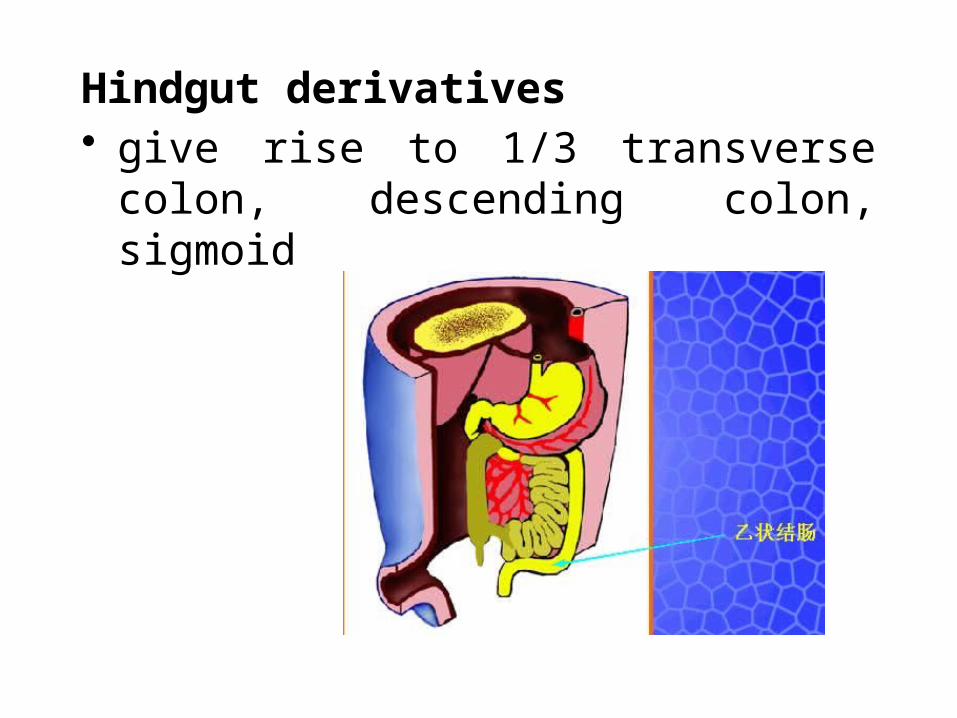
Hindgut derivatives• give rise to 1/3 transverse colon,
descending colon, sigmoid
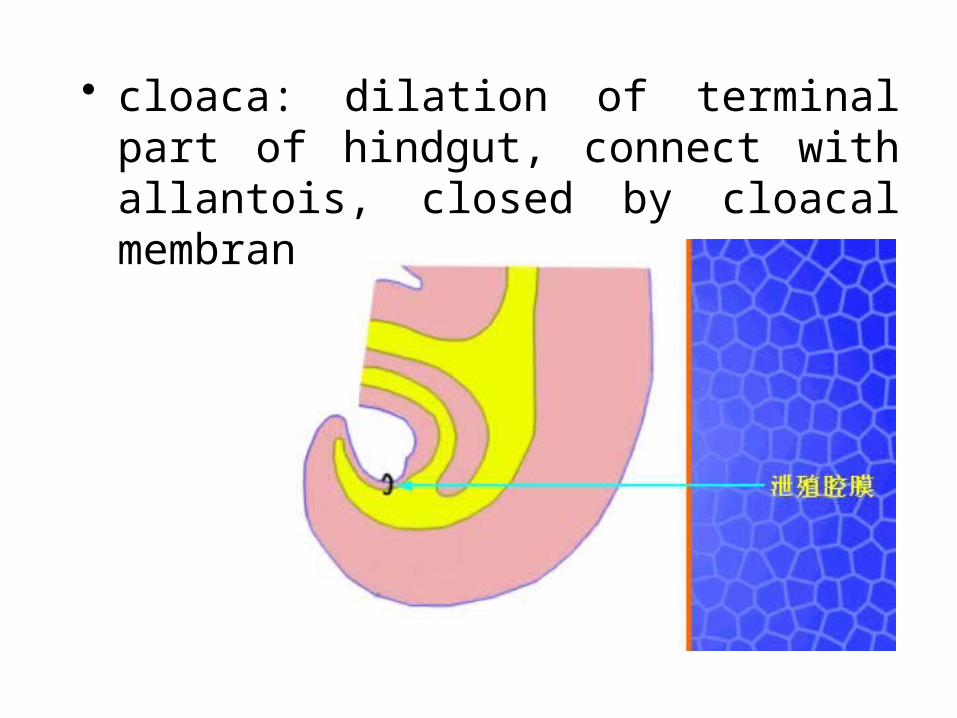
• cloaca: dilation of terminal part of hindgut, connect with allantois, closed by cloacal membrane
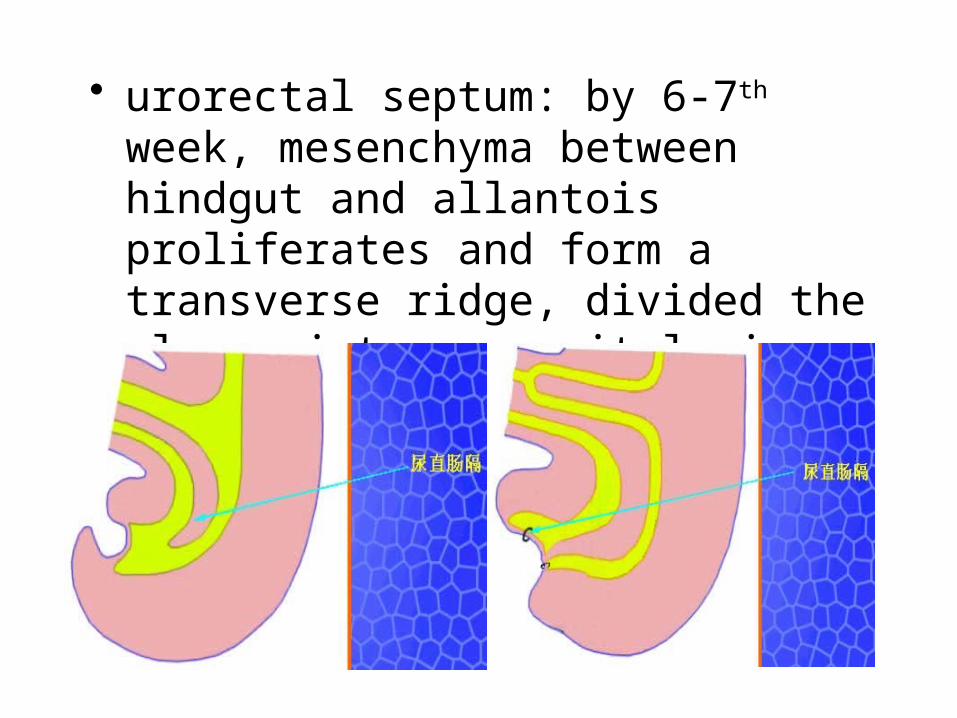
• urorectal septum: by 6-7th week, mesenchyma between hindgut and allantois proliferates and form a transverse ridge, divided the cloaca into urogenital sinus and anorectal canal
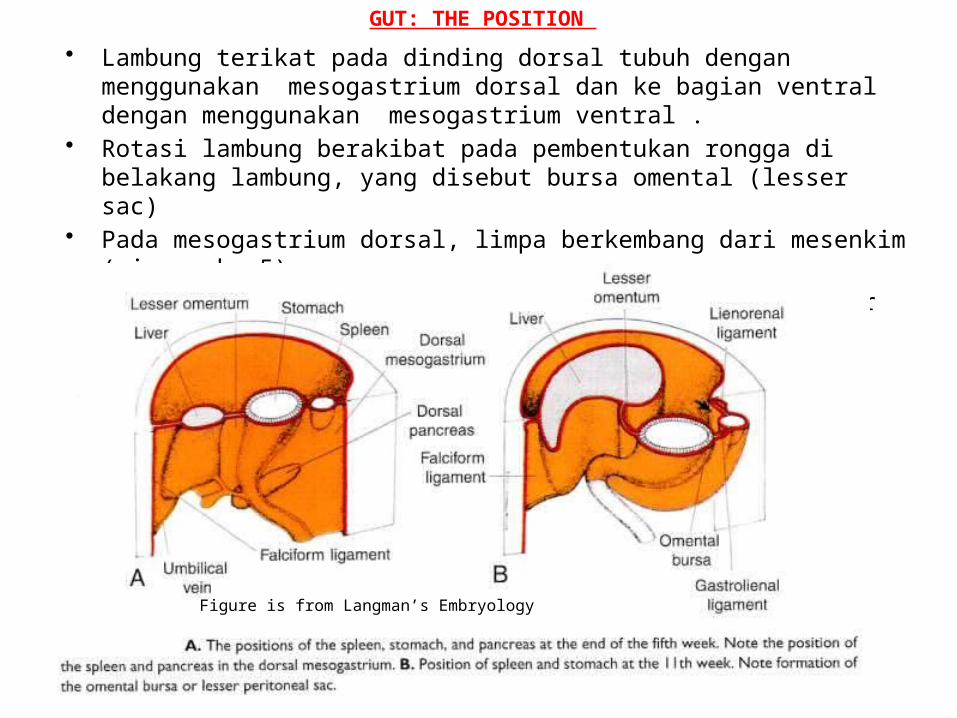
GUT: THE POSITION
• Lambung terikat pada dinding dorsal tubuh dengan menggunakan mesogastrium dorsal dan ke bagian ventral dengan menggunakan mesogastrium ventral .
• Rotasi lambung berakibat pada pembentukan rongga di belakang lambung, yang disebut bursa omental (lesser sac)
• Pada mesogastrium dorsal, limpa berkembang dari mesenkim (minggu ke-5). – dari mesogastrium dorsal-berkembang ligamen greater omentum,
lienorenal dan gastrosplenic.
Figure is from Langman’s Embryology
Arterial Supply of the Gut Tube• Celiac trunk supplies the abdominal
foregut• Superior mesenteric trunk supplies the
midgut• Inferior mesenteric artery supplies the
hindgut
the paired vitelline veins and umbilical vein form hepatic sinusoids
at about 6th week, blood stem cell immigrate into liver from yolk sac, hemopoiesis begin
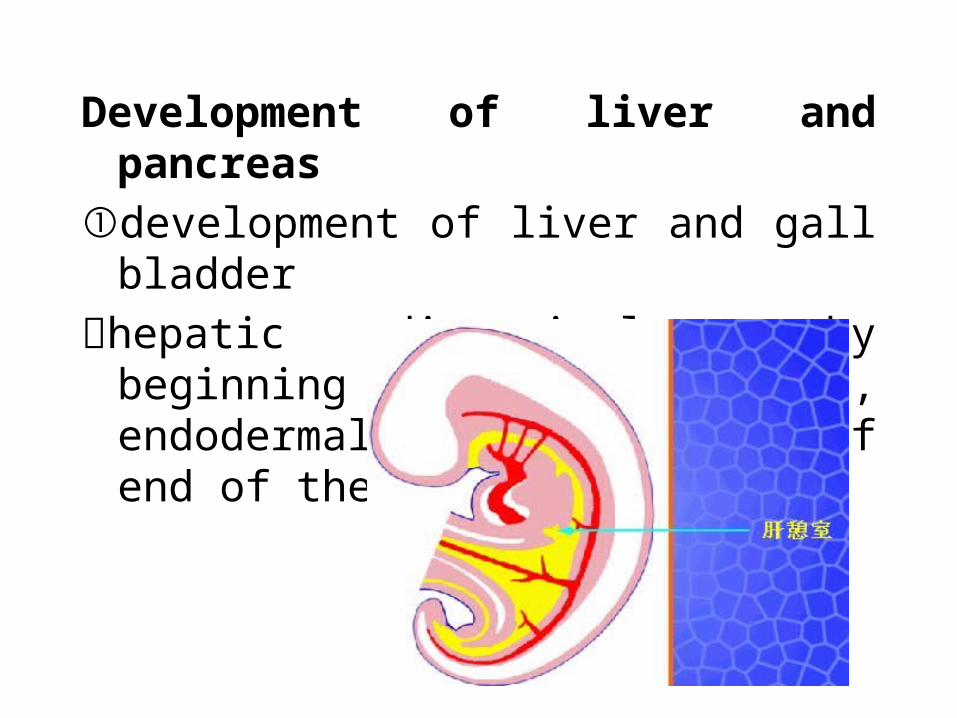
Development of liver and pancreas
①development of liver and gall bladder
hepatic diverticulum: by beginning of 4th week, endodermal proliferation of end of the foregut
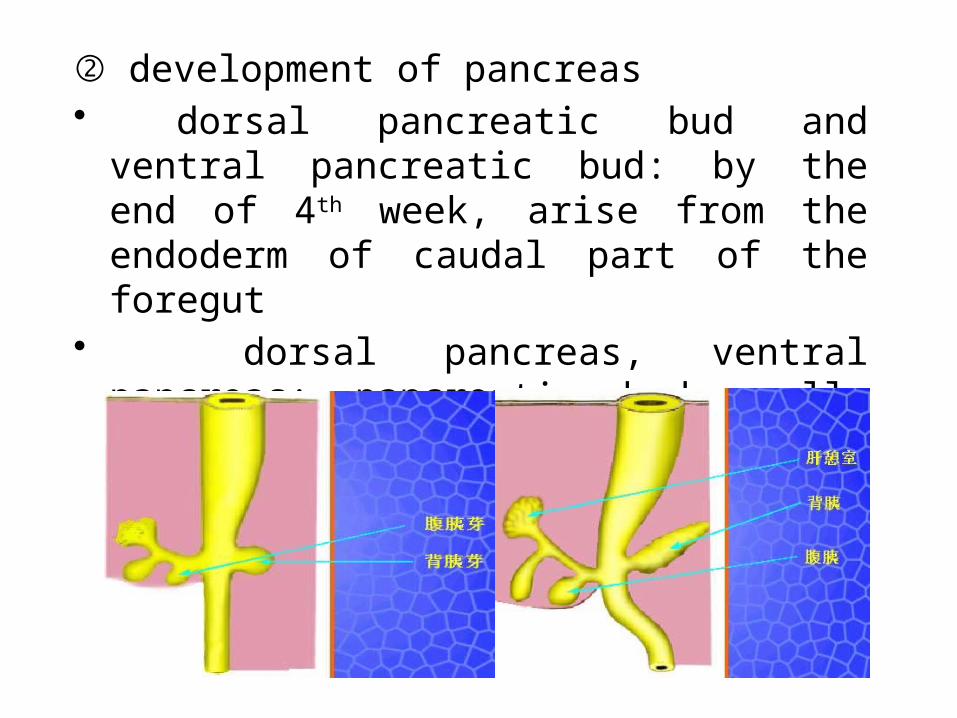
② development of pancreas• dorsal pancreatic bud and ventral pancreatic
bud: by the end of 4th week, arise from the endoderm of caudal part of the foregut
• dorsal pancreas, ventral pancreas: pancreatic buds cells proliferate to give rise to acinus and ducts
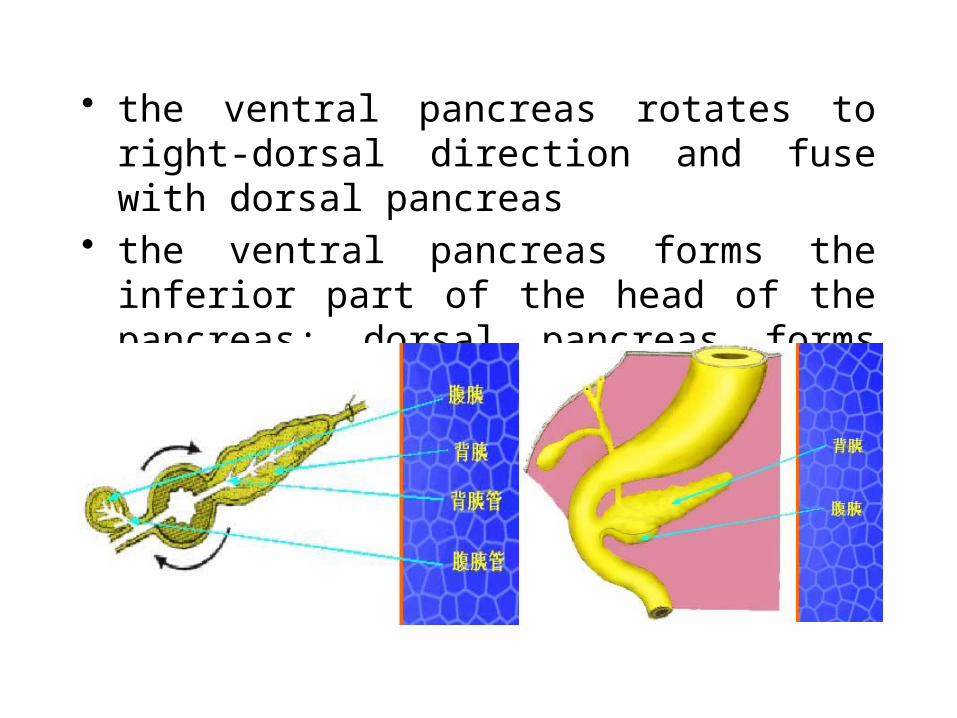
• the ventral pancreas rotates to right-dorsal direction and fuse with dorsal pancreas
• the ventral pancreas forms the inferior part of the head of the pancreas; dorsal pancreas forms other part of pancreas
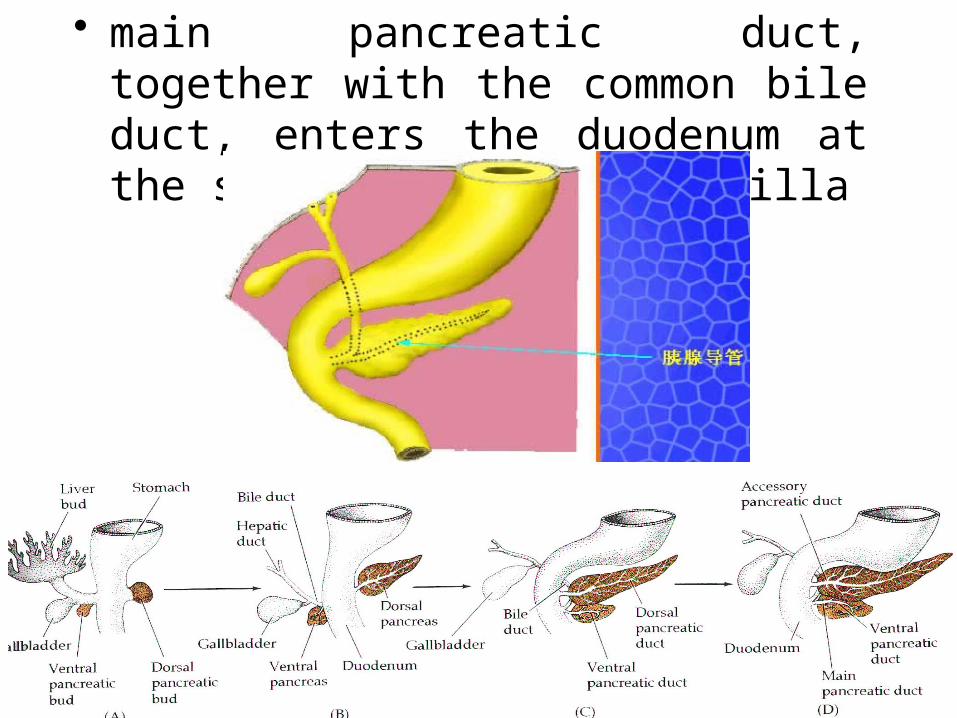
• main pancreatic duct, together with the common bile duct, enters the duodenum at the site of the major papilla
Clinical Applications
Anomalies of Gastrointestinal Development
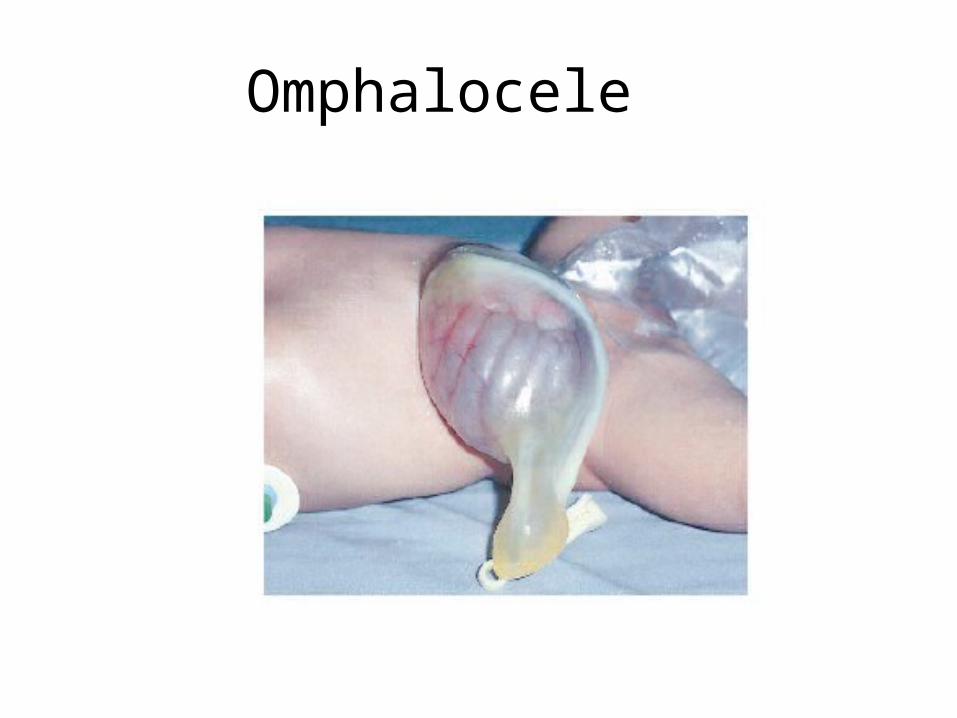
Omphalocele
• Occurs in 1 in 6,000 births• GI structures protrude through an
unclosed umbilical ring, covered in membranes– Herniated organs may not have fully
retracted in the 10th wk (likely if amnion covered only)
– Or, if there is peritoneum in the sac, the organs retracted but herniated again secondarily when the ventral abdominal wall failed to close
Omphalocele• ½ to 1/3 have other anomalies or
chromosomal defects– Pentology of Cantrell (failure of migration and
fusion of the lateral and cephalic folds): omphalocele, diaphragmatic hernia, sternal cleft, ectopia cordis (evagination of the heart), & intracardiac anomaly
– Beckwith-Wiedeman Syndrome: omphalocele, macroglossia, macrosomia, hemihypertrophy, hypoglycemia related to pancreatic hyperplasia
– Associated with Trisomy 13, 18, &21
Omphalocele
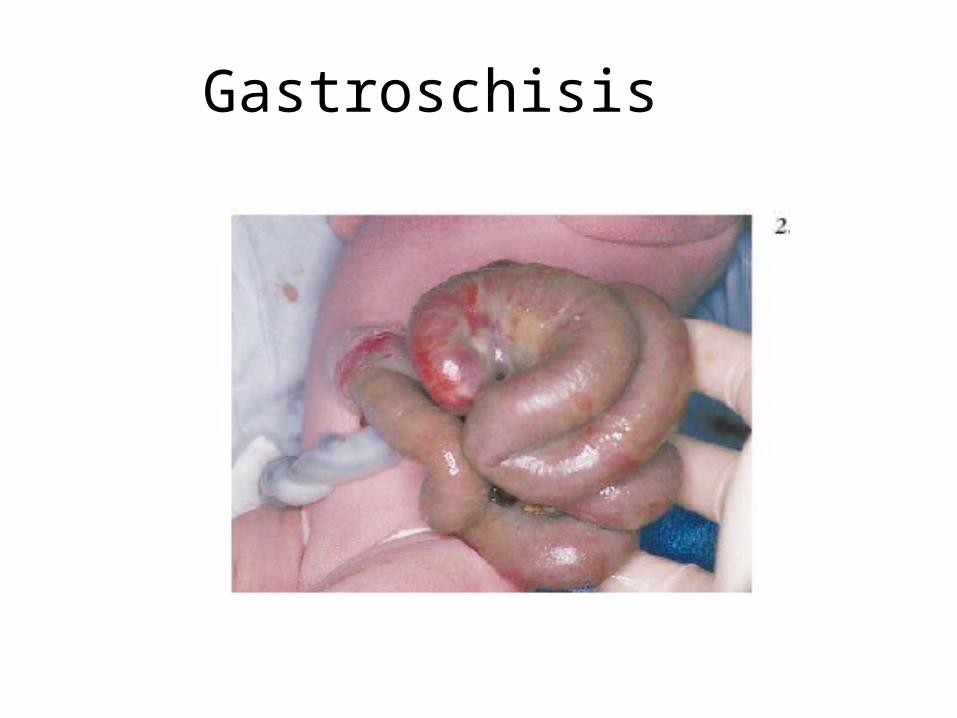
Gastroschisis
• Occurs in 1 in 10,000 births• Defect of the ventral abdominal wall
between the rectus muscles lateral to the umbilicus
• Occurs on the right side– Arises through an abnormality in the
involution of the right umbilical vein during the 5th & 6th wks causing a maldevelopment of associated mesodermal elements in that region of the body wall
Gastroschisis
• Not covered by a membrane– Herniated intestine is often edematous,
and can be ischemic- especially if the defect is small
– Increased risk of sepsis– Increased fluid and heat losses
• Not associated with other abnormalities
Gastroschisis
Nonrotation of the Gut
• The primary gut loop fail to rotate the 180 degree counterclockwise rotation as it enters the abdominal cavity
• The earlier 90 degree rotation may happen normally
• The jejunum and ileum end up on the right side of the body and the colon ends up on the left side- Left-sided colon
Reversed Rotation of the Gut
• The initial 90 degree rotation occurs normally, but the 180 degree rotation occurs clockwise instead of counterclockwise (so net is 90 degree clockwise)
• Everything is in normal spatial relationship except the duodenum is anterior to the transverse colon and it does not become secondarily retroperitoneal, but the transverse colon does!
Malrotation• The cephalic limb of the primary intestinal loop
undergoes the initial 90 degree rotation only• The caudal limb undergoes only the later 180 degree
rotation• So the distal end of the duodenum becomes fixed on
the right side of the abdominal cavity and the cecum is fixed near midline just inferior to the pyloris
• The abnormal position of the cecum may cause the duodenum to be enclosed by a band of peritoneum (Ladd’s bands)
• Diagnose with UGI to visualize duodenum
Volvulus• Abnormal rotation or fixation can lead to this life
threatening condition• Midgut lies free with only duodenum and proximal
colon attached to the posterior abdominal wall• Volvulus can occur as suspended regions of the gut
twist around themselves constricting the intestine and compromising the blood supply– Surgical emergency
• 80% present in the first month• Symptoms include bilious vomiting (95%), abdominal
pain (varies), bloody stools (28%)
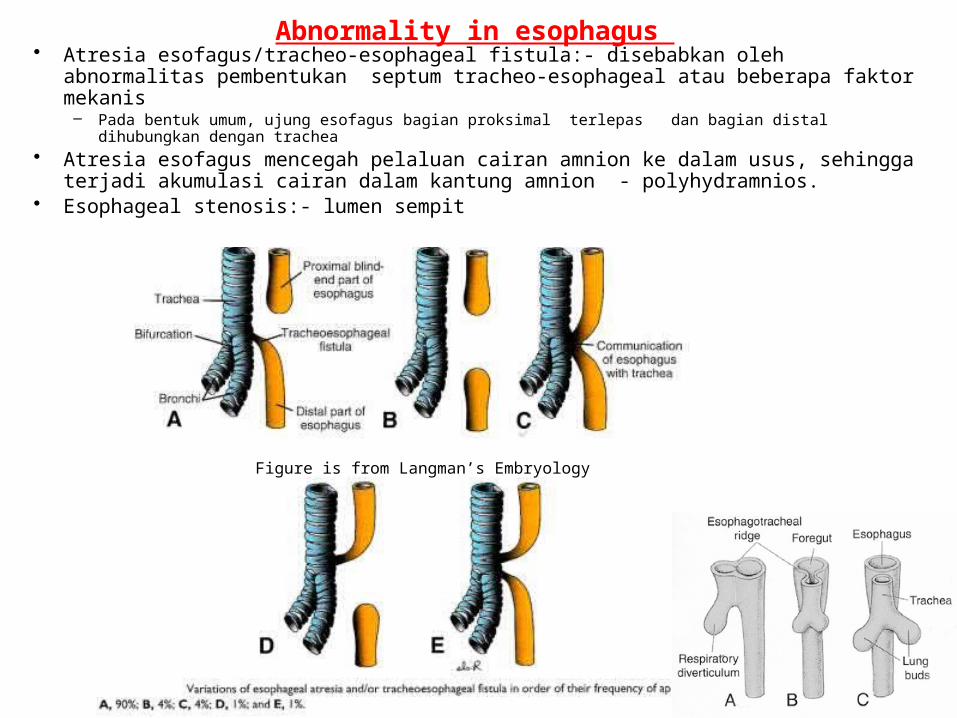
Abnormality in esophagus • Atresia esofagus/tracheo-esophageal fistula:- disebabkan oleh abnormalitas
pembentukan septum tracheo-esophageal atau beberapa faktor mekanis – Pada bentuk umum, ujung esofagus bagian proksimal terlepas dan bagian distal dihubungkan
dengan trachea • Atresia esofagus mencegah pelaluan cairan amnion ke dalam usus, sehingga
terjadi akumulasi cairan dalam kantung amnion - polyhydramnios.• Esophageal stenosis:- lumen sempit
Figure is from Langman’s Embryology
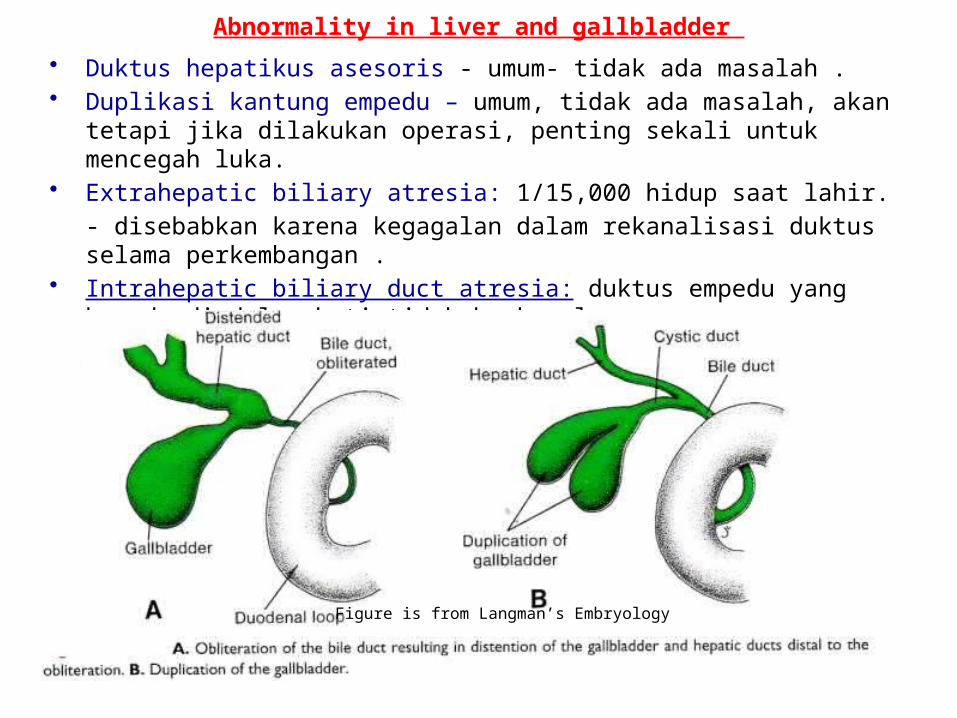
Abnormality in liver and gallbladder
• Duktus hepatikus asesoris - umum- tidak ada masalah .• Duplikasi kantung empedu – umum, tidak ada masalah, akan tetapi jika
dilakukan operasi, penting sekali untuk mencegah luka.• Extrahepatic biliary atresia: 1/15,000 hidup saat lahir.
- disebabkan karena kegagalan dalam rekanalisasi duktus selama perkembangan .
• Intrahepatic biliary duct atresia: duktus empedu yang berada di dalam hati tidak berkanal
Figure is from Langman’s Embryology
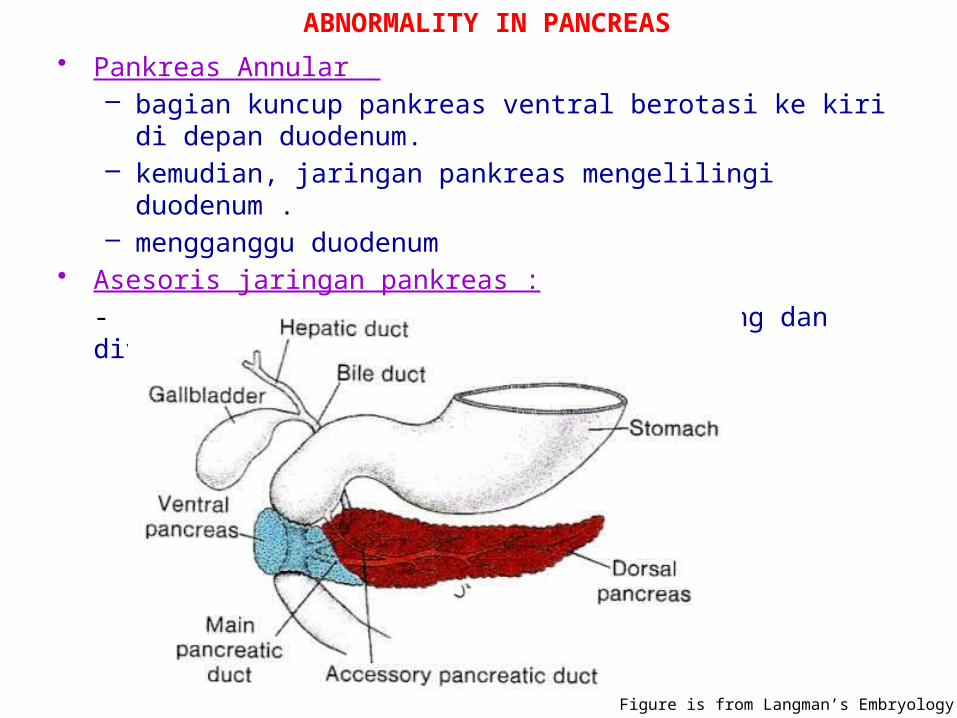
ABNORMALITY IN PANCREAS
• Pankreas Annular – bagian kuncup pankreas ventral berotasi ke kiri di depan
duodenum.– kemudian, jaringan pankreas mengelilingi duodenum .– mengganggu duodenum
• Asesoris jaringan pankreas :
- seringkali terletak dalam mukosa lambung dan divertikulum Meckel
Figure is from Langman’s Embryology
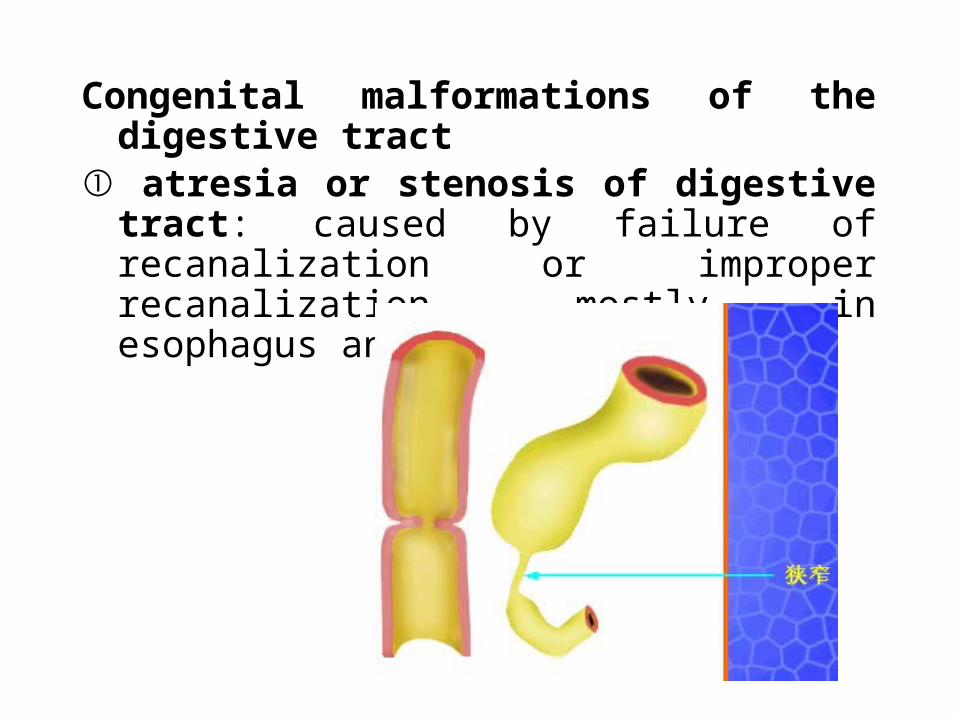
Congenital malformations of the digestive tract ① atresia or stenosis of digestive tract: caused by failure of recanalization or improper recanalization, mostly in esophagus and duodenum
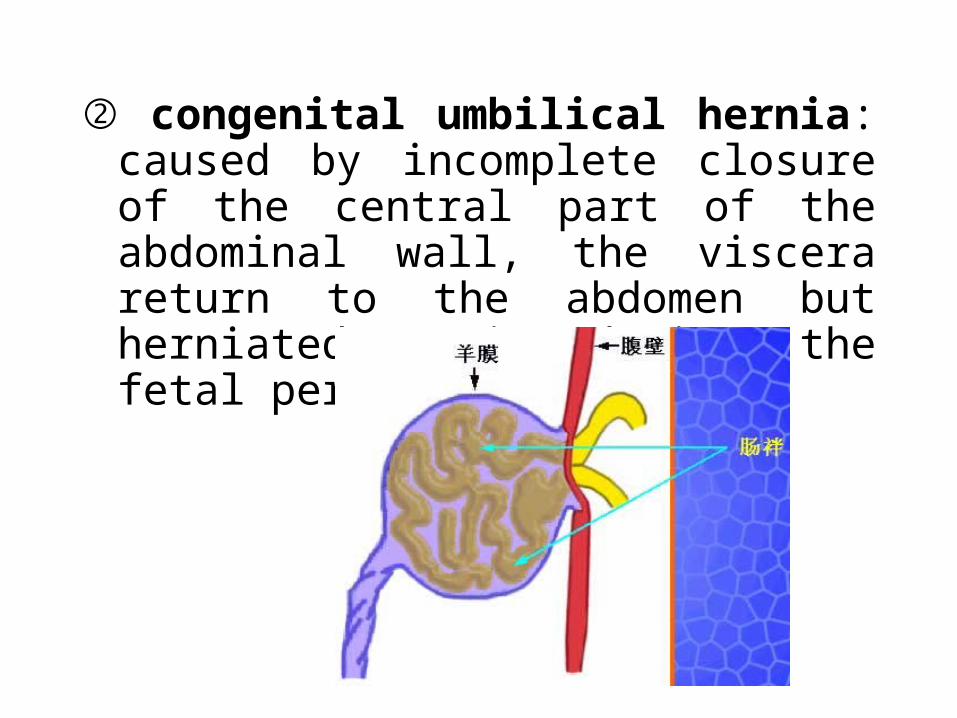
② congenital umbilical hernia: caused by incomplete closure of the central part of the abdominal wall, the viscera return to the abdomen but herniated again during the fetal period
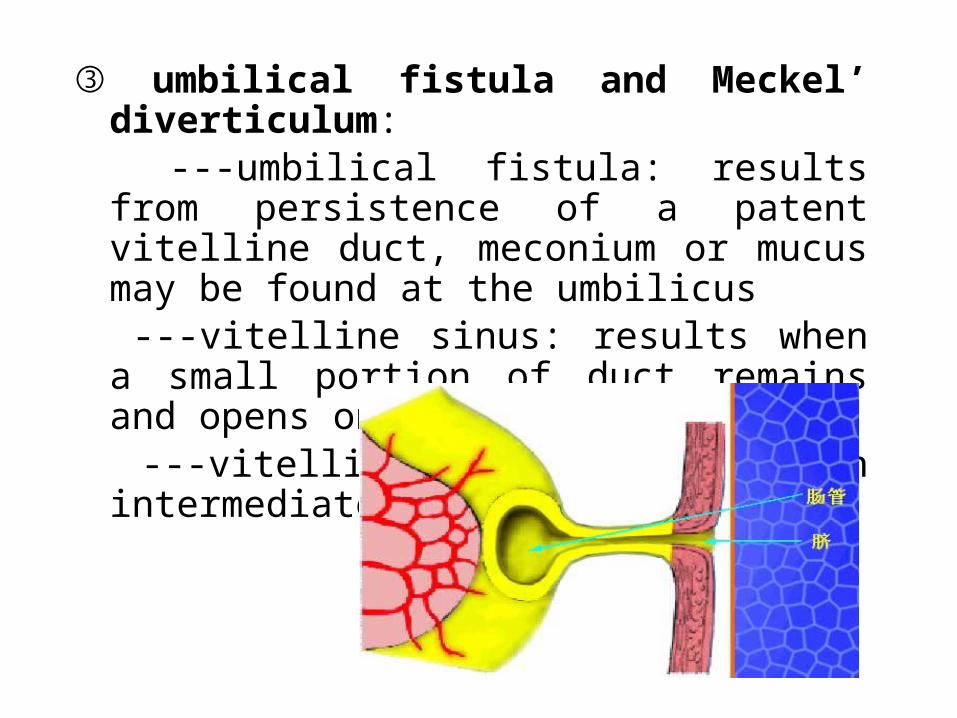
③ umbilical fistula and Meckel’ diverticulum: ---umbilical fistula: results from persistence of
a patent vitelline duct, meconium or mucus may be found at the umbilicus
---vitelline sinus: results when a small portion of duct remains and opens onto the skin
---vitelline cyst: results when intermediate patent leaves
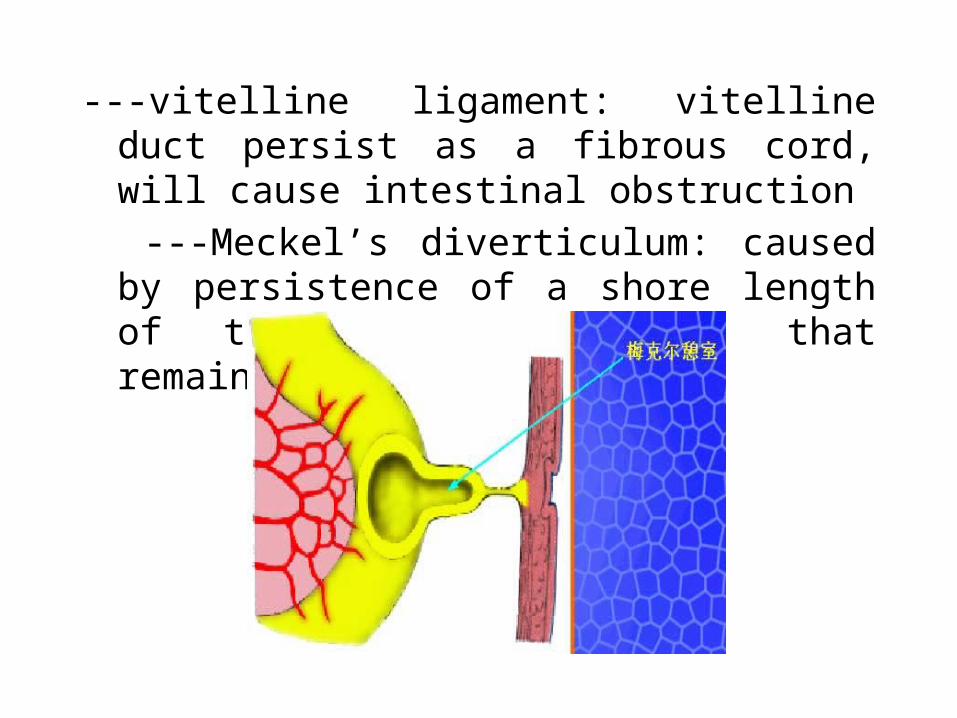
---vitelline ligament: vitelline duct persist as a fibrous cord, will cause intestinal obstruction
---Meckel’s diverticulum: caused by persistence of a shore length of the vitelline duct, that remains attached to ileum
Meckel’s Diverticulum• May be attached to the umbilicus by a
fibrous cord, omphalomesenteric cyst or fistula
• 1/5 of cases have ectopic pancreatic or gastric tissue– Commonly present as painless rectal
bleeding in a toddler from ulceration of ectopic gastric mucosa
• Meckel’s scan (technetium-99m pertechnetate isotope) identifies the gastric mucosa
④ congenital aganglionic megacolon: results from the absence of ganglion cell of the parasympathetic ganglia, which cause failure of the distal segment to move the intestinal contents onward HIRSCHPRUNG
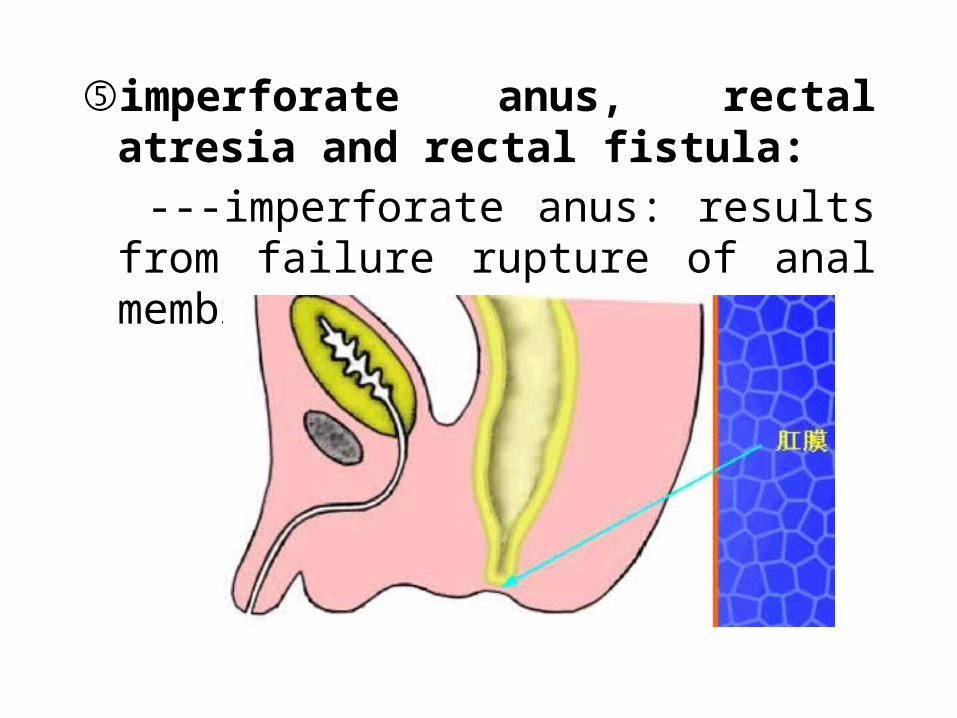
⑤imperforate anus, rectal atresia and rectal fistula:
---imperforate anus: results from failure rupture of anal membrane
---rectal atresia: due to a failure of the anal pit to develop or deviation of the urorectal septum in dorsal direction
---rectal fistula: associate with an imperforate anus, between the rectum and the vagina or urinary bladder or urethra
⑥ abnormal rotation of the intestinal loop: nonrotation or reversed rotation of the midgut
⑦ atresia of the gall bladder and bile ducts: results from failure of vacuolization of the epithelial cords or reopen
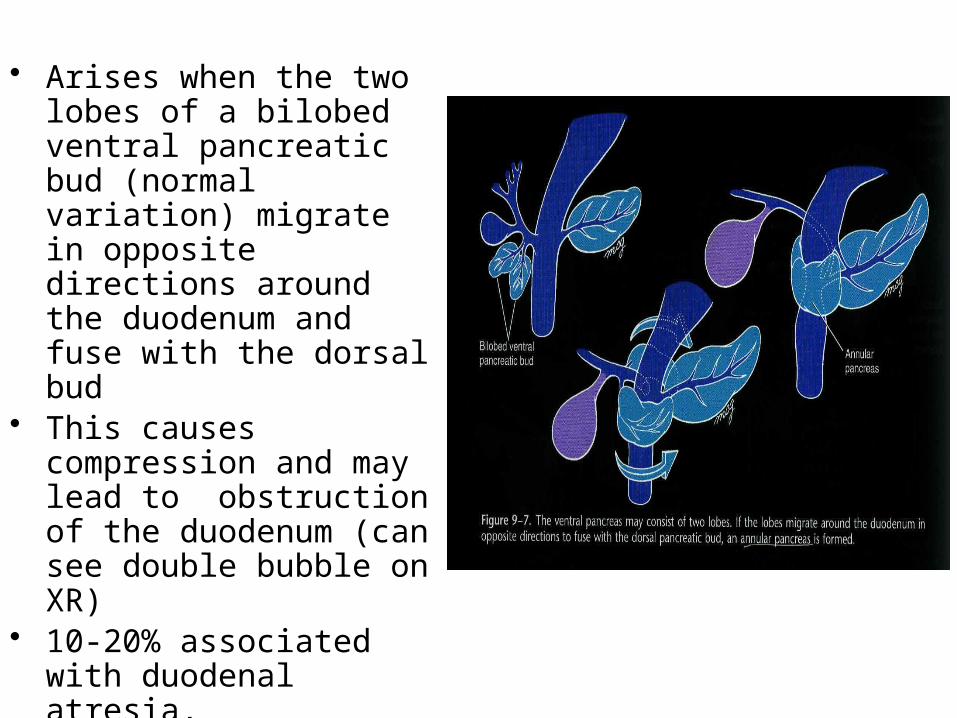
• Arises when the two lobes of a bilobed ventral pancreatic bud (normal variation) migrate in opposite directions around the duodenum and fuse with the dorsal bud
• This causes compression and may lead to obstruction of the duodenum (can see double bubble on XR)
• 10-20% associated with duodenal atresia, malrotation, & Trisomy 21


















