
EMBARGOED draft clinical options appraisal · 5 Transfer of designated high risk unscheduled...
52
1 STRICTLY EMBARGOED 00:01HRS FRIDAY 24 OCTOBER DRAFT DOCUMENT FOR DISCUSSION AND ENGAGEMENT Clinical options appraisal and potential way forward October 2014 Please note that everything detailed within this document is draft and has been developed with senior clinical staff in North Cumbria University Hospitals NHS Trust. Further, and more detailed, engagement is required with both clinical staff, partners and the public. The findings of which will help us to refine our plans which will then inform discussion with NHS Cumbria Clinical Commissioning Group.
Transcript of EMBARGOED draft clinical options appraisal · 5 Transfer of designated high risk unscheduled...

1
STRICTLY EMBARGOED 00:01HRS
FRIDAY 24 OCTOBER
DRAFT DOCUMENT FOR
DISCUSSION AND ENGAGEMENT
Clinical options appraisal and
potential way forward
October 2014
Please note that everything detailed within this document is draft and has
been developed with senior clinical staff in North Cumbria University Hospitals
NHS Trust. Further, and more detailed, engagement is required with both
clinical staff, partners and the public. The findings of which will help us to
refine our plans which will then inform discussion with NHS Cumbria Clinical
Commissioning Group.
2
Contents Page
Executive Summary 3 Purpose 8 Context 8 Approach - Whole System Working 9
Journey of improvement to date 10 Operational Challenges & Sustainability Issues 12
Sustainable Medical Workforce 12 Medical Workforce Considerations 12 NCUH Priority Issues 13
Clinical Dependencies and Site Determination 17 Service Strategic Direction & Clinical Principles 17
Options appraisal 19 Conclusions and next steps 20 Appendix one – clinical options appraisal 21
Unscheduled care at West Cumberland Hospital 21 Obstetrics and midwifery: Intrapartum care including neonatology 34 Paediatrics 40
Elective care 46 Transport 48 Clinical and System Outcome Measures 50

3
Executive Summary
North Cumbria University Hospitals NHS Trust (NCUH) and the health economy it
operates in are under significant pressure with Cumbria identified as one of 11
“distressed health economies” and the Trust is currently in ‘Special Measures’.
Whilst significant improvements have been made, the Trust remains in a fragile
position with some quality standards, operational standards and performance control
yet to be achieved. Services at both sites, but particularly at the West Cumberland
Hospital (WCH), fall short of the incoming seven day national standards, something
the Trust cannot ignore.
Small teams and low activity volumes compound the difficulties of two-site working
and directly impacts on clinical teams’ ability to maintain skills and on training
experiences for junior staff. This also impacts on the quality governance
arrangements and achievement of regulatory and emerging college standards.
These problems, alongside geographical and more recent reputational issues have
directly impacted on recruitment and have led to major difficulties in retaining and
recruiting staff, with local exacerbation of the national shortfall in general internal
medicine (GIM) accredited trainees, and resultant reliance on locums. Some 28% of
Trust consultant posts are currently covered by locums. As a result some services
are operationally extremely fragile; this is particularly true of acute medicine at WCH.
This has been highlighted by the Chief Inspector of Hospitals as of major concern
and importantly, identified as unsafe. Whilst there are clearly further financial
efficiencies to be made, a significant proportion of the current deficit reflects the
structural issues of distant 2-site working.
The Trust does not have any choice when it comes to urgently addressing its
regulatory compliance shortfalls, workforce challenges, inefficiencies and structural
issues in a way that is consistent with the strategy of the wider health and care
economy. It is imperative that these issues are addressed to secure the long term
clinical and financial future.
The Clinical Commissioning Group (GGG) North Cumbria Strategy 2014 – 2019
“Together for a Healthier Future” (TfHF) sets out common principles including right
care, at the right time, and in the right place. The outline proposals for hospital
services within TfHF have been further developed to create an ‘in-hospital’ clinical
strategy for North Cumbria and NCUH which envisages:-
1. An increase in the provision of specialist and high-risk emergency services at the Cumberland Infirmary Carlisle (CIC), consistent with the NHS Services, 7 days a week forum – clinical standards.
2. An increase in the number of people receiving services at WCH. 3. A wider use of clinical networks cross-site and with partner providers to
optimise the use of the limited amount of medical staffing resources.

4
The aim is to ensure, at all times, that patients can access the right services at the
right place and time. These services will be clinically safe and will save patient lives.
This may mean that a minority of patients may need to access services in either
Carlisle or Newcastle depending on their clinical needs, but will also mean that more
patients will access the care they need locally. This will allow systematic
standardisation of high quality care across the Trust and further quality
improvements to be made. It is without a doubt that some temporary
transformational changes to acute medical and surgical services have reduced
mortality rates.
Clinical staff involved in developing this draft have, to date, looked at a range of
potential options for change. These have been developed specifically to address the
challenges faced, and ensure the Trust meets all regulatory and other quality
standards. Options have been assessed and initially ranked against criteria that
include their ability to:
deliver safe pathways for patient care
meet all required quality and other regulatory standards
be practicably and sustainably implemented in workforce terms.
Given the significant financial deficit facing the Trust the impact on this is also noted,
although is not the priority issue. There are clearly other factors key to ensuring the
delivery of safe, high quality patient-centred services, these criteria are considered to
be of over-riding importance, and their successful delivery is a fundamental
necessity for the Trust to appropriately manage identified risk.
The Trust has initially assessed the potential options it believes are possible at this
early stage and based on the current evidence available. The Trust’s preferred
potential way forward is detailed in summary below as well as other core service
elements:
Maximisation of the opportunities offered by the new WCH redevelopment to
create a centre for excellence for lower risk care in West Cumbria, fully
integrated with community provision and with delivery of higher risk and more
specialised care at CIC and beyond (where appropriate i.e. Newcastle)
Inpatient & ambulatory/outpatient elective and speciality shift to WCH and
where appropriate, community hospitals, considerably increasing the total
volume of care that can be delivered locally to patients across all of North
Cumbria
Continuation long-term of the arrangements made on safety grounds in 2013
for transfer of high risk trauma and surgical patients to CIC, based on clear
evidence of improved clinical outcomes and reduced mortality rates

5
Transfer of designated high risk unscheduled medical pathways (as well as
above surgical pathways) from WCH to CIC, with detailed pathway
development and planning as soon as possible to enable better clinical
outcomes
With regards to maternity services, although the Trust has discussed
potential future solutions, particularly to help address critical safety
issues with regard to anaesthetic cover, no preferred option is stated
and all potential solutions are fully dependent on the outcome of the
independent maternity review which has been commissioned by NHS
Cumbria CCG.
A 24 hour Short Stay Paediatric Assessment Unit at WCH, supported by 24
hour paediatrician access, low acuity beds and a full In-patient Unit at CIC
working as part of a system-wide child health network
Please note the above preferred potential way forward is based on current
thinking and has been pulled together with senior clinical engagement,
although it still requires more comprehensive clinical and stakeholder
engagement and therefore may change over the coming months.
It is also noted that the planned Independent Review of Maternity services by
NHS Cumbria CCG, which must also closely examine issues concerning
anaesthetics, is yet to take place and more detailed modelling and analysis
would be required on all options. The Trust remains open-minded to
alternatives which can demonstrate that they better meet current challenges
(particularly in relation to anaesthetics). System leaders will wish to review
potential options in light of the Independent Maternity Review and further
detailed modelling and options appraisal is required.
The Trust’s preferred way forward in other areas seeks not only to secure
sustainable services for the long-term but also to maximise local service availability
wherever possible. The opening of the new West Cumberland Hospital in 2015
provides the ideal opportunity for newly configured services to be implemented.
The availability of appropriate transport to support preferred options presents a key
challenge to implementation: it is recommended that the CCG be requested to
commission an inter-hospital transport solution to support local communities and
address any concerns raised relating to the transport between Cumberland Infirmary
and West Cumberland Hospital.
The preferred way forward is expected to enhance clinical outcomes, not just on one
site but across the Trust as a whole through ensuring a sustainable model that
facilitates service development and quality improvements in the long term.

6
This draft clinical strategy, coupled with a comprehensive and innovative approach to
recruitment, allowing substantive net recruitment of 1 consultant & 1 specialty doctor
post every 3 months, anticipates the ability to secure a significantly more permanent
consultant workforce in 3 years as well as becoming a ‘trainer of choice’ for Health
Education North East (HENE), with increased fill rate and allocation of training
posts1. This strategy does not as yet take into account medical productivity changes
with the diagram below demonstrating the minimum expectation of shifts in
substantive posts as a proportion of the total establishment:
Ultimately the Chief Inspector of Hospitals will give final opinion on whether service
and workforce proposals can secure a safe and sustainable workforce, and will need
to have confidence in the Trust’s best judgment in relation to timescales for change,
and success in reducing risk through reduction in temporary staffing through our
workforce strategy.
This paper describes a clear strategic direction and provides credible and
transformational potential options which are implementable for the delivery of
1 Note: Whilst a simplification and not strictly accurate use of terminology, in this context and
throughout the document the term ‘Specialty Doctors’ is used to denote Specialty Trainees: ST Higher
(ST3 plus), ST3+ equivalent including SAS doctors; ‘Trainees’ denotes Lower Trainees, CMTs, F2s,
GPVTS, and ST(Lower).
Percentage Substantive Posts Against Establishment
As at September 2014 Post Change: April 2017
79%
72%
62%
52%
x%??
66%
Consultants
Middle Grade
Junior

7
safe, high quality and regulatory-compliant secondary care in North Cumbria.
Potential options are based on best available evidence to date and have been
designed to most successfully mitigate the significant risks within the existing
system, and to ensure that safe, service provision can be built upon and
sustained longer term.
Significant further cross-system work is needed to define out of hospital
initiatives and the anticipated impact on the Trust both in terms of new ways of
working and in expected reduced in-patient activity. This may require revision
of the current thinking which is based on existing activity levels.
The Trust remains open-minded to consideration of alternatives which can
demonstrate they better meet the current challenges. Additional Trust Board
consideration and on-going development of this high level strategy will be
required in conjunction with clinical teams, partners, regulators, and other
stakeholders over coming months. Robust governance arrangements will be
agreed internally and with external partners to further progress the work.
However and, to be clear, this document focuses on what the Trust, to date,
believes could be the potential way forward based on the evidence available.
The next steps are to engage further regarding these initially assessed and
ranked potential options, the outcomes of which will inform further
conversations with commissioners who will ultimately determine the services
commissioned within the local communities following a comprehensive
programme of engagement and public consultation.
Ann Farrar, Chief Executive
October 2014

8
Purpose
This paper sets out to date, the potential way forward for secondary care. It describes
the challenges in delivering this care, considering those core services faced with
critical issues, and explores options to make them clinically sustainable in the long
term. Consideration of specialist provision is beyond the remit of this paper and will be
taken forward through a separate mechanism. However, the common aim is to
maintain these services locally, ensuring they are delivered in accordance with NICE
guidance using systematic service reviews to consider the capacity requirements,
sustainable workforce solutions and best operating model for future service delivery.
Work has already started with radiotherapy and vascular services, with remaining
specialised services to follow.
The potential options detailed within this document confirm, to date, the Trust’s clinical
thinking relating to how it can practically meet both short and long term operational
and quality service requirements.
The Chief Inspector of Hospitals will re-visit the Trust shortly, and will review the
progress made to formulate a robust long term strategy which addresses the
sustainability issues in relation to medical workforce, particularly in acute medicine at
West Cumberland Hospital (WCH), and which has a clear and realistic plan for its
delivery. This will determine if sufficient improvement has been made, to remove the
“inadequate” rating for acute medicine at WCH and ultimately allow the Trust’s
removal from Special Measures.
This draft paper has been developed to support further discussion with staff
commissioners, partner providers and other stakeholders. Whilst options have been
identified, the Trust is open-minded to alternatives which can demonstrate that they
better meet current challenges, and will continue to work closely with its doctors and
nurses, the public, stakeholders and others to develop the very best possible
solutions.
Context
North Cumbria University Hospitals NHS Trust (NCUH) is the secondary care provider
in North Cumbria providing services to 340,000 people predominantly from its two
sites, the Cumberland Infirmary at Carlisle (CIC), and the West Cumberland Hospital
(WCH) in Whitehaven. The Trust also provides a midwifery-led service at Penrith
Birthing Centre.
The Trust, and the health economy it operates in, are under significant pressure, with
Cumbria identified as one of 11 “distressed health economies”. The Trust is in “Special
Measures”, by virtue of it currently failing to achieve on some aspects of quality
standards, operational performance and financial control. Services at both sites, but
particularly WCH, fall short of the incoming 7 day national standards.

9
The geographical distribution of the population and two site working is challenging:
whilst as individual factors they are not unique, it is highly unusual to combine these
with the distance between the two sites, (and between the smaller site and the tertiary
centre) as well as the volume of activity at the smaller site, which serves a significant
and overall disadvantaged urban population. Current secondary care service
provision, with two hospitals receiving unselected “blue light” admissions, results in
duplication of emergency services across low volume sites; of only six medically led
obstetric units in England with less than 2,000 deliveries per year, two are within the
Trust. These characteristics combine to create major operational and workforce
challenges.
NCUH was visited in April 2014 by the Chief Inspectors of Hospital’s Team, receiving
an overall rating of “requires improvement”. Whilst all services received a “good” rating
for delivery of ‘caring’ services, two areas were rated as “inadequate” under the safety
domain: acute medicine at WCH and outpatients at both sites. Of major concern was
the operational fragility of the medical workforce and the lack of a long term strategy to
address this.
Events of the past 12 to 24 months including the Keogh Review and Chief Inspector’s
visit, the withdrawal of some junior doctors from WCH and ongoing recruitment issues
have combined to create a burning platform for transformational change in secondary
care services: it is now imperative that this is agreed and delivered at pace, and is
supported by the entire health and care system in North Cumbria and beyond.
Approach - Whole System Working
Whilst the long-term viability of some core secondary and local specialist services
have been highlighted as of concerns for many years, and there have been multiple
plans to reform health service provision for Cumbria, to date, these have failed to
address the underlying issues. More recently, with other partners in Cumbria
experiencing challenges, and recognising the interdependencies and common
themes, health and social care clinical and managerial leaders have committed to
work together to find shared solutions as a system-wide Cumbria Health & Care
Alliance.
The North Cumbria Programme Board (NCPB) was established in February 2014 to
develop and implement a joint strategy for North Cumbria health and social care which
would ensure clinically and financially sustainable high-quality services. Under the
banner “Together for a Healthier Future” (TfHF).
Clinically-led Care Design Groups considered options based on principles of “right
care, at the right time, and in the right place” which would:
radically increase the scale and integration of out of hospital services based
around primary care communities,
10
achieve sustainable high quality provision by delivering a programme of
hospital services consolidation, and
enable a modern model of integrated services and delivery of the Cumbria well-
being strategy.
The concepts of integration and consolidation are critical and wholly interdependent.
Their successful delivery is reliant on the success of joint working across the health
and social care environment. The ‘North Cumbria Strategy 2014 – 2019’ sets out
scenarios for hospital service configuration created across a continuum, which have
been used as the basis for initial modelling and analysis of TfHF service options which
are set out in the following sections. Work in parallel is considering the detail for ‘out of
hospital’ provision.
Journey of improvement to date
Since arriving in September 2012, the leadership team at North Cumbria have always
been very clear that the organisation is on a long journey of improvement which will
require continuing stability to move from being a failing trust, over many years, to a
high performing successful NHS trust.
Despite the on-going configuration and recruitment issues, significant improvements
have been made and there are now some very clear milestones in the Trust’s
improvement journey over past 18 months which should be recognised. Most notably,
is the reduction in the Trust’s mortality rate which was one of the highest in England
two years ago and is now within expected limits and has continued to decline on a
quarterly basis over the past year.
This is thanks to very difficult but vital changes made to improve patient safety and the
Trust now has very clear evidence that less people are dying in the Cumberland
Infirmary and West Cumberland Hospital, with more people surviving serious injury or
illness and going on to live longer lives with better outcomes following their stay in
hospital. It should be noted however, that WCH has historically had higher mortality
rates than the Cumberland Infirmary (CIC) and this continues to be the case (although
both are now within expected range).
In addition, staff should be rightly proud of the fantastic achievement of a ‘good’ caring
rating for all services and departments from the Chief Inspectors of Hospital’s visit in
July 2014
Throughout their visit, the CQC witnessed patients being treated with compassion,
dignity and respect at all times with staff clearly very committed to achieving the very
best for their patients. The Trust is immensely proud of the tireless efforts of each and
every member of staff who regularly go beyond the call of duty, in very challenging
circumstances, to provide compassionate care.

11
These positive changes in mortality and quality of care have not happened by
magic. They are the result of some specific service changes made on safety grounds
during 2013 and the momentous efforts by all staff who continue to put their patients
first and respond fantastically well embracing the challenges faced on a daily basis.
Despite these significant improvements, the Trust is extremely aware that the way
some services are currently delivered is still not as good as it should be, or to the
standards expected of the professional bodies and Royal Colleges of nurses,
midwives and doctors.
It is important to note that the CQC, following their latest inspection in April 2014, also
rated the safety element of care at West Cumberland Hospital as inadequate as a
result of the unstable position with regard to acute medical staffing.
The CQC also recognised that for North Cumbria in particular, the complex and
geographically challenged environment adds further difficulties in solving some of the
challenges faced, particularly around recruitment.
Although there have been previous attempts, as part of the ‘Care Closer to Home’
consultation in 2008, to address some of these issues by moving more care outside of
hospital, into the community and peoples’ homes, and to consolidate certain specialist
hospital based care – the hospital elements of these plans were ever brought to
fruition under previous system leaders.
The problems in North Cumbria have therefore never been solved or been allowed to
be truly addressed.
Whilst these problems are without doubt difficult, they are not impossible to solve,
however they have already, and will continue, to require change and challenge of the
status quo in order to provide the very best care for patients.
Work over the summer with the Trust’s senior clinical teams and in partnership with
NHS Cumbria CCG as part of the NCPB, has now started the conversation about the
potential way forward to address the challenges which remain.
To be clear, the Trust’s ambition for North Cumbria is to make hospitals in Carlisle and
Whitehaven as good as the best in the NHS and deliver the highest possible
standards of clinical care that each and every one of us would expect for our own
loved ones.
Change, by its very nature, is never easy but in order to deliver this ambition of high
quality, person centred healthcare, the challenges we face must be tackled once and
for all. This will require joint working with all health and social care partners to develop
pathways of care that will mean the best possible outcomes for each and every
patient.

12
Operational Challenges & Sustainability Issues
The following details further the operational and sustainability challenges the Trust is
facing now and into the future. The potential options assessment and ranking
considers these challenges. Our focus will always be to ensure the Trust delivers high
quality services without compromising on safe care. To do this, we must all recognise
the challenges staff are tackling day in day out.
Sustainable Medical Workforce
The issues facing the Trust are well rehearsed and commonly understood. As
previously outlined, running two isolated District General Hospital (DGH) sites
geographically distant from each other and from tertiary/specialist support, has
resulted in clinically unsustainable working practices and major difficulties in sustaining
medical staffing rotas. Small teams and low activity volumes have further compounded
difficulties, impacting on: skills maintenance; training experience for junior staff; quality
governance arrangements and achievement of regulatory and emerging college
standards. In addition, this is also financially unstable.
These problems directly impact on recruitment and have led to major difficulties in
retaining and recruiting staff, with a subsequent over reliance on locums which is
unsustainable in the long term. As a result, some services are operationally extremely
fragile; this is particularly true of acute medicine at WCH. Out of a total of 203
consultant posts Trustwide, 46 are currently covered by locums/agency staff; for
middle grades this is 66 out of 127 posts.
Medical Workforce Considerations
Current nationally agreed consultant contract on-call requirements mean that is highly
inefficient to run with an emergency/7-day rota of less than 5 consultants. More
importantly, in practical terms recruitment is, and will become increasingly, difficult with
fewer than 8 consultants in a rota. Seven day working requirements and other specific
Royal College requirements (for example, dedicated intensivists, 24/7 A&E Advanced
Trauma Life Support (trained medical staff presence), add significantly to the
challenge, although national contract changes may in part alleviate this
In addition, consultants increasingly wish (and should be encouraged) to sub-
specialise to enable improved outcomes for patients, with a range of skills provided
across a team (note in this instance services such as general surgery, gynaecology,
orthopaedics). Maintaining multiple sites with low levels of activity restricts this skills
development and maintenance, increases professional isolation and impacts on job
satisfaction. Whilst the Trust could seek to develop ‘buddying’ arrangements to
address this in part, it will not fully compensate and is likely to be an expensive model.
These issues, as well as impacting on quality and consultant productivity, have
significant impact both on the ability to train doctors and ultimately the attractiveness

13
of posts and ability to recruit and retain consultants, particularly in consultant
specialties where there are national shortages. As a consequence, whilst safety of
services has been maintained, they are not necessarily resilient, with over-reliance on
a few individuals and an ageing workforce, and where potentially a single resignation
may destabilise an already fragile service.
Significant use of locums is not an acceptable long-term solution either financially or
more importantly in terms of quality, continuity and service development. Differences
in mortality between sites are likely to be directly associated with the severe consultant
workforce difficulties at WCH. Services are also vulnerable due to short notice
contracts.
Resident specialty doctor recruitment is challenged by similar issues, with onerous on-
call requirements, inability to develop speciality skills and professional isolation.
Medical workforce problems are compounded by the system-wide lack of qualified and
unqualified nurses, with difficulties in recruitment across all providers; the Trust
remains reliant on a combination of additional hours, bank and agency nursing and the
sheer goodwill of staff, to maintain safe nursing levels in line with the Francis
recommendations.
Finally, an ability to recruit and retain sufficient specialist staff to retain training doctors
has had an impact on the allocation of trainees by HENE speak at and problems
recruiting to NCUH rotations. As a result of locum usage and subsequent inability to
provide an appropriate training experience, there will be no trainee doctors at WCH
from 2015, excepting those on the GP Vocational Training Scheme.
HENE colleagues confirm that due to national workforce issues, despite the significant
efforts made by the Trust, supported by buddy trust and acquisition partner
Northumbria Healthcare NHS Foundation Trust (NHFT) including dual appointments
and NHFT secondments, the situation is unlikely to significantly alter.
A reduction in the proportion of locum usage to acceptable levels will require not only
innovative and sustained approaches to recruitment and retention, but also
rationalisation of overall consultant numbers achieved through implementation of
integrated competency-based and multidisciplinary models of care which are
sustainable in the long term and are, ultimately, more likely to attract more candidates.
NCUH Priority Issues
Whilst the challenges above are relevant to all of The Trust’s services, three specific
high-risk issues must be resolved by the Trust as a matter of urgency ensuring an
appropriate balance of safety issues and patient-centred access at all times:
a. WCH Unscheduled Care
The Trust has struggled to recruit to consultant and middle grade medicine
posts over several years. As at September 2014, there were cross-Trust

14
vacancies in 21.5 out of 35 Acute Medicine & Care of the Elderly consultant
posts; five out of seven consultant on call positions are filled by locums at WCH
and four out of ten at CIC. Amongst resident medical doctors, vacancies are 15
out of 36 and all WCH posts are filled by locums. Vacancies in specialist posts
are significant cross-Trust, particularly for gastroenterology, respiratory, care of
the elderly and general cardiology; Acute Care Physician (ACP) cover is largely
dependent on secondees from Northumbria Healthcare. In A&E there is circa
50% reliance on locum consultant cover.
This over-reliance on locums in acute medicine at WCH has severely impacted
on the Trust’s ability to provide an appropriately supervised high quality
educational experience at WCH and junior trainees have been consequently
withdrawn. Unfilled middle grade posts from August 2014 put in jeopardy the
Trusts’ ability to maintain acute medicine in its current form, but following
strenuous efforts, the Trust successfully appointed locums to all nine posts
maintaining safe service provision in the short term. Additional rota and surgical
support changes have been implemented from August 2014, including the
planned use of nurse practitioners both day and night. The Trust and wider
system have developed robust contingency plans to manage potential rota
collapse in acute medicine including those for a ‘worst case scenario’, with
changes to emergency flows in West Cumbria and use of CIC overnight.
This, however, is an untenable position longer-term and a service configuration
which can be delivered by a largely substantive workforce is essential.
b. Obstetrics and Gynaecology
Current arrangements are the provision of the 2 site obstetrics, including
anaesthetic and paediatric cover and neonatology, as well as the Penrith
Birthing Centre. Neither district general hospital site operates a Midwifery Lead
Unit (MLU), nor does CIC currently offer an epidural service. Whilst the
maternity dashboard demonstrates an acceptable position in many (but not all)
areas, and CNST Level 1 achievement, arrangements are not compliant with all
current regulatory requirements. Specific regulatory, NICE, CNST2 and College
Guideline2 compliance issues that must be addressed include:
Lack of dedicated resident anaesthetic support across both sites
resulting in risks associated from management of multiple workstreams,
2Association of Anaesthetists of Great Britain & Ireland, Obstetric Anaesthetists’ Association OAA /AAGBI
Guidelines for Obstetric Anaesthetic Services, 2013 Clinical Negligence Scheme for Trusts, Maternity Clinical Risk Management Standards 2012/13, January 2012
RCOG, RCM, RCA& RCPCH. Safer Childbirth: Minimum Standards for the Organisation and Delivery of Care in
Labour, October 2007

15
in addition to insufficient dedicated daytime anaesthesia service at WCH
and lack of epidural service as a key option for pain relief at CIC
Lack of dedicated theatre team with immediately available anaesthetic
and theatre staff for emergencies at WCH
Lack of dedicated second theatre and theatre staff for caesarean
sections beyond two (WCH)/three (CIC) elective caesarean sections
(LSCS) lists per week
The critical issue, however, for obstetrics relates to the availability of
anaesthetic/intensivist support. Anaesthesia at WCH has not been able to
develop separate streams of anaesthetic cover for maternity and intensive care.
Units that rely on a shared anaesthesia/ITU on call generally have developed
separate 7/7 staffing for ITU and maternity, have greater resilience in total
anaesthetic numbers and have a busier caseload for other anaesthetic streams
of work to attract staff. The combined workstreams have been noted as factors
within recent anaesthetic (non obstetric) ‘never events’.
Even with existing sub-standard anaesthetic/ITU staffing levels, there are
numerous vacancies at both middle grade and consultant levels; WCH currently
has no anaesthetic trainees. Despite the doubling of CCTs in anaesthetics in
2011/12 only one successful appointment was made at WCH during this period.
There is major difficulty in recruiting middle grade obstetric staff at WCH with
the service run by three 12 PA (equivalent of 48hr clinical and non clinical paid
time) specialty doctors, and long-term locums generally used to cover night
duty. At CIC there are difficulties in maintaining the resident medical rota as it is
reliant on speciality trainees - however there is a national shortage: gaps have
had to be filled by locum consultants with resident on-call duties. Resident
anaesthetic trainees have variable levels of experience.
Risk mitigation plans in place include a third anaesthetic on-call rota 24/7 at
WCH to cover for simultaneous emergencies, and written escalation plans
including prioritisation of work guidelines. There is close monitoring of
outcomes through the maternity dashboard and patient experience feedback.
Arrangements are being made to ensure epidural can be provided at CIC as a
choice option to women in labour.
Business cases have been developed for a dedicated theatre team and
obstetric anaesthetist (not utilised in transfers) to replace current arrangements
which require disruption of elective lists. At CIC, where there is only one
resident anaesthetist out of hours covering all areas (obstetrics, theatre, ITU),
proposals include separate ICU consultant cover in addition to the 2 obstetric
consultant anaesthetists covering CEPOD (emergency lists) / obstetrics.
Following NCUH formally raising concerns in relation to service sustainability, it
was concluded that current operational and risk mitigation arrangements for

16
maternity were satisfactory, and that long-term configuration issues should be
dealt with as part of the local system planning process. NCPB commissioned
an Independent Review of Maternity service; this has been significantly delayed
to date but is expected to take place in November 2014 led by a past President
and current Deputy President of the Royal College of Obstetricians, with the
outcome made known by December 2014. It is noted that the Chief Inspectors
of Hospitals report also highlighted that maternity services at WCH were ‘not
sufficiently safe’ (largely due to medical cover – specifically anaesthetics)
c. Paediatrics
Due to the interrelationship and co-dependencies of paediatrics with intensivist,
A&E and obstetric services, it is vital that consideration is given to paediatric
provision in any discussion of other service changes. Consultant-led obstetric
services require 24/7 resident paediatric presence, as well as paediatric
consultant cover and paediatric services support A&E and in turn require
intensive care support. The interrelationship with community child health
provision is also key.
Present arrangements for both medical and nurse staffing in paediatrics do not
meet current college recommendations or Royal College of Paediatricians and
Child Health required standards34 , and concerns were raised by the Chief
Inspector of Hospitals in relation to the robustness of night-time paediatric
cover.
Currently paediatric and neonatal units at CIC and WCH deliver a traditional
provision for medical and nursing care; there are two consultant led in-patient
units with junior doctor support and some speciality doctor input, with the
exception of the neonatal unit at CIC site where senior nurses with expanded
skills initiate the care of the neonate supported by the Paediatric Consultant.
This area has no junior doctor input. Historically, CIC has tended to run without
recourse to appointing resident paediatric medical staff to cover gaps in trainee
rotas.
Adult high dependency unit (HDU) beds are used at WCH for the management
of critically ill children. HDU support is not explicitly commissioned at NCUH
with additional resource, but there are long-standing custom and practice
arrangements whereby the Trust manages HDU-level requirements. Both sites
successfully manage CPAP (Continuous Positive Airways Pressure) treatment
in children and it is noted that Newcastle Hospitals do not have a retrieval
service for non-ventilated children from the Trust thereby currently offering little
alternative to current practice.
3 Royal College of Paediatrics & Child Health; Facing the Future: Standards for Paediatric Services, April 2011
4 It is noted that consultation on revision to the 2011 standards closed on 15
th September 2014

17
The unattractive 3-tier out of hours arrangements at WCH, with a consultant
sleeping in to support paediatric emergencies, are not sustainable; at CIC
consultants are called in from home. Removal of specialty trainee doctors at
WCH has made recruitment to resident posts problematic, and whilst currently
managing to recruit there are expected to be increasing difficulties in securing
substantive consultant appointments which can meet the increasingly onerous
Royal College requirements. Whilst some investment has been made in
paediatric nurse practitioners (PNPs) which will assist, recruitment and training
of these staff is challenging and further investment needs to be made to deliver
paediatric care with an integrated PNP rota.
Clinical Dependencies and Site Determination
Where a service can only reasonably be safely maintained from one site, a
decision must be taken as to which: by virtue of geography and transport
to/distance from the nearest tertiary centre(s).
Understanding service co-dependencies is essential in determining site
configurations: A&E, intensive care and acute medicine are inter-reliant; to
function as a Trauma Unit as part of the regional trauma network (CIC has
designated trauma unit status) requires A&E, intensive care, general surgery,
trauma and orthopaedics, blood products, lab. and radiology support. Equally,
consultant obstetric provision requires support from anaesthetics, ITU, and
paediatrics (as detailed above) and there are limitations in operating without the
support of the range of other surgical specialties, creating interdependencies for
general surgery, gynaecology, T&O, ortho-geriatric and endoscopy.
Service Strategic Direction & Clinical Principles
As highlighted in Monitor’s April 2014 strategy,5 focus needs to be “on maintaining
services, not institutions”. Our patients do not distinguish between different provider
organisations and neither should we: our primary interest is in ensuring delivery of
seamless high quality and efficient care with our partners, across the health and social
care.
The Trust’s Integrated Business Plan and CCG 5-Year Strategy Together for a
Healthier Future both describe how the key changes we expect to be delivered in
conjunction with our partners, will shape the care experienced by patients and their
families:
5 Monitor strategy 2014 to 2017: Helping to redesign healthcare provision in England, April 2014

18
There will have been a reduction in reliance on in-patient care: more patients
will be treated in community or ambulatory care settings involving NCUH staff
directly supporting patients in their own homes, through support of primary and
community teams, through high quality outpatient and ambulatory care
services, and through integrated approaches to admission avoidance and early
discharge. Our focus will be on supporting patients and their families with the
“right care, at the right time, and in the right place”.
For those patients who do require hospital in-patient care, high quality, safe and
effective care with early senior assessment and rapid access to specialists and
diagnostic tests 7 days a week will be provided, with timely onward referral for
tertiary support where indicated.
Delivery will be through ‘integrated’ teams, both multi-disciplinary and inter-
provider/agency, which work to minimise duplication and maximise continuity
and efficiency of care: our focus will increasingly be on prevention (both primary
and secondary), and included within this as core practice will be patient
involvement in proactive care planning and an emphasis on enabling self-
management.
Delivery of care will not just be technically excellent, but will be caring,
responsive and compassionate, tailored to individual needs and wishes at all
times. This will enhance both patient and staff satisfaction: patients and families
will meet staff who are proud of their work, and who have time to continually
improve their services.
Patients and their families will be confident that where care has not been
delivered to the standards they would wish, this will be readily acknowledged,
fully explained and changes made speedily to rectify problems.
There will be continued delivery of care locally wherever possible, and
‘centrally’ where necessary to achieve best clinical outcomes; in this context
‘centrally’ may be any hospital site, a specific North Cumbria site or beyond: our
principle will be that care will be delivered as locally as it is possible to deliver
high quality, safe care making best use of finite Cumbria resource.
The Trust expectation is of secondary services working as a single entity in delivering
services across North Cumbria, with clinical networks supported by flexible working of
its staff. Wider clinical networks from outside the County will continue to be developed
both with buddy trust Northumbria Healthcare NHS Foundation Trust as acquisition
partner and with tertiary centres and other providers. The Trust principles
underpinning configuration of services are:
1. Safe, effective, patient-focused and compassionate care at all times and in all
places,
2. Compliance with all regulatory and quality standards
3. More patients than currently to receive services local to where they live
4. Specialist skills in WCH-based staff to be maintained and developed

19
5. Increasing provision of “one stop” services
6. Specialty support to in-patient activity at WCH to be secured through outpatient
and elective service providers
7. Specialty provision enabled through visiting consultants (whole days of activity)
and networked specialty services across Trust sites,
8. Access to secondary care services differing dependent on geography, as
happens with tertiary services
9. Clinical networks across the Trust providing the best balance between
centralised specialist care and outreached specialist care
10. Not all specialist services required to be on the ‘centralised site’
11. 24 hour and 7 day services to improve safety, quality and efficiency
Measurement of quality, operational and financial performance in all parts of the Trust
will drive improvement. Agreed performance indicators including compliance with
regulatory standards, college guidelines and local pathways and protocols will be
routinely monitored.
Options appraisal
The initial clinical options appraisal for key service areas has been considered in more
detail in appendix one and has been designed to address specific models of care
where there are clinical sustainability concerns. Options have been designed to
manage these risks and the potential implications and are assessed against criteria
that include their ability to:
deliver safe pathways for patient care,
meet all required quality and other regulatory standards,
be practicably and sustainably implemented in workforce terms.
Given the significant financial deficit facing the Trust the impact on this is also noted,
although is not the priority issue. Whilst there are clearly other factors key to ensuring
delivery of patient-centred services, these criteria are considered to be of over-riding
importance, and their successful delivery is a fundamental necessity for the Trust to
appropriately manage identified risk. Issues of access and patient experience must be
appropriately balanced by those of safety and clinical outcomes.
It should be noted that modelling is based on current activity levels; significant, further
cross-system work, is needed to define out of hospital initiatives and the anticipated
impact on the Trust both in terms of new ways of working and in expected reduced in-
patient activity. This work will continue to be led by the CCG through the NCPB/TfHF
arrangements and Health & Wellbeing Board leadership of the Better Care Fund
plans.
Appendix one shares in greater detail the options appraisal for each of these
areas

20
Conclusion and next steps
In conclusion, the Trust Board is clear of the opinion that to ensure the services it
provides are clinically safe and financially sustainable that change is not an option but
a necessity.
The evidence relating to the challenges articulated within this document continue to be
collated and will be further developed as the Trust progresses to more comprehensive
engagement with clinical staff. The findings of the Independent Maternity Review will
also add to a body of evidence that will support conversations with the local
commissioners of health services.
Over the coming weeks the Trust will engage in detail with clinical teams across the
organisation and with partners and has also commissioned independent public
engagement regarding the potential options detailed within this document.
The findings of this engagement will then be fed into final Trust recommendations
which will then be shared with the clinical commissioning group.
To be clear, this is NOT a consultation document, but a working draft clinical
strategy. This has been designed to support further clinical and public
engagement regarding the potential options detailed within this document.
It is the role of the commissioners of health services in Cumbria (NHS Cumbria CCG),
who are the leaders of the local NHS, to determine, based on the evidence available,
what they believe to be the options for the provision of health services. The final
options which they develop and refine, if there is a material change within a provided
service, will then be engaged and fully consulted on within the local community.

21
Appendix one – Clinical Options Appraisal
Unscheduled Care at West Cumberland Hospital
The hospital operates two distinct areas for medicine: ‘Front of House’ dealing with
acute admissions, and Back of House covering the medical wards for respiratory,
gastroenterology, general medicine and elderly. As from August 2014, night-time
medical cover has been provided by Hospital at Night (H@N) nurse practitioners
supported by resident middle grades, plus a consultant on-call (non-resident).
Non elective surgical care
In line with newly agreed arrangements, the management of non-elective/emergency
surgical assessment includes middle grade surgical presence only between 8am-8pm,
7 days a week. Moderate/high risk emergency surgical referrals are expected to be
made directly to CIC; low risk patients with surgical problems during the day time are
assessed in the ambulatory care unit; at night assessment is provided where possible
via the ambulatory care unit without admission (and return the following day), admitted
to WCH under the medical team if more appropriate, or transferred to CIC. This model
anticipates clinical assessment in A&E and subsequent pathway management without
rigid allocation to traditional medical & surgical ‘specialist’ streams: for example
patients with abdominal pain identified as not in need of surgery can be admitted at
night by the H@N Team pending surgical review in morning. This ensures that the
service provided responds flexibly to the needs of the patients rather than a reliance
on specialty support.
Continuation of these arrangements is assumed unless stated otherwise. It is noted
that some changes were made on safety grounds and will require formal public
consultation; some of the outcomes associated with these moves are evidenced under
‘clinical and system outcome measures’ section.
Proposed Clinical Pathway Changes
The preferred way forward focusses on managing the risks associated with
unscheduled care on the West Cumberland Site given the over-reliance on locums,
the extreme fragility of the medical workforce at WCH, the support that can be
provided to other WCH clinical services, and the currently evident site impact on
patient outcomes (mortality).
Current Model
The current arrangements for WCH takes all emergency admissions - “blue light” and
self-referrals as well as GP admissions, excepting some specific recent service
changes (see below) to manage certain high risk patients presenting in West Cumbria
at CIC:
Major trauma

22
Trauma requiring urgent/immediate operative procedure
Patients suitable for PCI or other CIC Heart Centre intervention
High Risk Emergency Surgery – i.e. requiring urgent/immediate operative
procedure
High risk vascular surgery (Tier 3)
Major GI bleeds out of hours
Patients not recognised by GPs/paramedics at presentation or self-referrals are
assessed, provided with immediate treatment as required and transferred to CIC (or
more distantly) for continuation of their care. Where possible, patients are ‘repatriated’
to WCH as soon as is clinically appropriate and practicable.
Option UC1 – Diversion/Transfer of High Risk Patients to CIC
Clinical Pathway
Option UC1 seeks to ‘de-risk’ the WCH site from its currently fragile state through
transfer or diversion of certain medical patients identified as at high risk, day and night
from WCH to CIC. It is proposed that these patients will benefit from the additional
resources, skills and expertise available on the CIC site, with lower risk patients
continuing to be safely managed at WCH.
Patients who can reasonably be identified in community settings can be immediately
transported to CIC either through discussion with their referring GPs or as a result of
paramedic triage. Those presenting at front of house are assessed, stabilised and if
meeting the criteria transferred to CIC. Patients are repatriated to WCH to complete
their care as soon as clinically appropriate; this includes patients stepped down from
critical care at CIC.
The implication of UC1 is that only selective ‘blue lights’ are taken to WCH, and with
the designation of the unit to be finally determined in line with national 'Urgent and
Emergency Care Review' definitions. This allows implementation of a model of care
delivered from an ‘emergency floor’, a concept previously agreed with commissioners
but not to date fully implemented. Front of house early assessment is provided from an
integrated team consisting of ED consultants, acute physicians, nurse practitioners
and critical care doctors. The whole system is supported by a Back of House team
including Critical Care and critical care outreach. Patients who require ventilation can
be safely managed on-site with over-night care and longer as necessary in advance of
transfer to CIC if clinically appropriate. The model is reliant on genuinely cooperative
working across the out of hours medical workforce working as a single team that sees,
assesses and “clerks” patients (see below).
Speciality support and advice is provided as required at night from CIC; the two sites
work increasingly together as a joint entity by day and night, with an expectation of
routine cross-cover, rotation of staff between sites, and maximisation of specialist
(direct or indirect) support of rotas.
23
Patients admitted to the WCH site will have access to intensivist support and facilities
with critical care/higher acuity beds including increased monitoring, inotrope support
and NIV, plus acute and post-acute care. Admission decisions options are based on
the following clinical pathway possibilities and are driven by the needs and best
interests of the patient:
Anticipated for home within 24 hours,
No specialist intervention is needed and patient is sufficiently stable to be transferred to ‘back of house’ medical ward +/- subsequent transfer to sub-acute ward,
Patient is high risk and would benefit from transferring to CIC for specialist treatment and intervention with repatriation when possible.
Clear admission and transfer criteria will be used with “Standard operating procedure”
for transfers, and with staff competency requirements defined by patient acuity.
Patients to be transferred from WCH front of house are stabilised, and managed until
they can be safely and appropriately transferred.
Proposed criteria for High Risk6:
Patients are identified as at high risk and suitable for CIC transfer on the basis of:
I. initial diagnosis (at front of house or by paramedic staff) of an agreed high risk
medical pathway,
II. High NEWS score.
High risk patients identified as suitable for transfer against the following criteria:
1. Medical admissions with NEWS score greater than or equal to 7 during their ED
admission AND/OR greater than or equal to 5 following appropriate ED
treatment (excluding respiratory failure patients suitable for NIV in WCH ICU).
2. High risk chest pain (determined by chest pain pathway) i.e. Acute Coronary
Syndrome/NSTEMI with NEWS below criteria 1.
3. Stroke (diagnosis as entered by ED clinician plus stroke chameleons) with
NEWS below criteria 1.
4. GI bleed (diagnosis as entered by ED clinician and not considered suitable for
discharge on G-B score) with NEWS below criteria 1.
Palliative patients or those with very poor pre-morbid function are excluded as they are
unlikely to benefit from the enhanced services at CIC. Clear evidence-based
Treatment Escalation Plans which take into account frailty will ensure standardisation
of care: these would be piloted in community settings to facilitate direct diversion of
patients where appropriate.
6 Detailed definitions and criteria to be developed

24
(It should be noted that further consideration could be given to those patients who may
well clinically benefit from CIC additional resource but who could not reasonably be
identified at first assessment; this may include some patients with lung cancer, liver
and other gastro-intestinal problems. These patients have not been modelled in at this
point.)
This option will shift some volume of activity between the sites, but more importantly
will allow those patients at greatest risk to be managed on a site where there is robust
(and more substantive) senior and specialised medical support as well as access to a
range of specialist support services. There is evidence that consolidated delivery
within larger specialised teams would enable greater standardisation and achievement
of high quality care. The options would require a shift in emergency beds and
associated resource from WCH to CIC. This would be offset by anticipated increase in
low risk elective activity and outpatient/ambulatory activity at WCH.
Operational Delivery of an Integrated Urgent Care System at Night
In the envisaged UC1 admissions system, and in keeping with the agreed concept of
an ‘Emergency Floor’, the H@N team at WCH works across all professional and
specialty boundaries. This would operate with a single consultant responsible across
ED/Medicine ‘front’ and ‘back of house’. Although during the day when the units are
busier there continues to be more traditional staffing, this way of working at night is
well suited to doctors with generalist skills i.e. trainees (before specialty formation),
GPs (CHOC7), A&E consultants, General Physicians, and ACPs. Staff are supported
by specialty pathways and opinion, either locally or from CIC. Led by Medicine, the
team’s role is to ensure that correct initial treatment is initiated, that patients are
triaged correctly into pathways based on risk and presentation and that their passage
through the system is expedited. Managing this front of house workload together
allows the team to share patients, develop and maintain skills and sustain work
interest. They will work within the newly built ED/EAU/Assessment Unit ‘emergency
floor’ at WCH and meet as a team at H@N shift change. It also allows for staff
undertaking similar roles to cross cover and reduce cost from the whole system. This
system is supported by nurse practitioners/F1s, and includes a consultant physician
on call from home.
Potential specialty doctor medical workforce associated with this model would only be
expected to only when the unit is at its quietest i.e. from 2200 to 0800.
Following a period of stabilisation and familiarisation, consultant out of hours cover
may potentially be provided cross-Trust by a single integrated rota plus 2nd consultant
‘back-up’.
7 CHOC – Cumbria Health On Call: GP out of hours provider

25
Options UC2 (a-e) – Managing Volume
Additional mechanisms could be used to further de-risk WCH by reducing volumes of
acute medical patients at the WCH site by transferring patients according to time of
day and/or home postcode in addition to changes as described in UC1:
Limited Hours for Receiving Emergency Admissions
A way to manage potentially high volumes of general medical patients requiring input
from relatively junior staff would be to restrict non-elective admissions to the site
during the day and/or at night. This could be either on the basis of purely a 999 “blue
light” divert, with the site continuing to accept GP referrals and walk-in patients
requiring admission, or could include all those requiring a front of house medical
assessment.
Diversion of Patients Based on Postcode
Whilst the Ambulance Service had historically taken patients to the nearest Accident &
Emergency Department, the introduction of clear guidelines empowered crews to
divert to a specialist centre, which may have a longer journey time but which is
expected to provide improved clinical outcomes. Similarly, local GPs generally make a
referral to their nearest hospital, although there are clear pathways for selection of a
particular site in some instances. This deliberate diversion is already built upon in
UC1.
When one site is experiencing high attendances or bed availability is limited, a ‘post
code divert’ system is currently used for a limited period of time to improve patient
flow. If UC1 was considered insufficient to fully address current challenges, this
approach could be used to manage volumes on an ‘as required’ (for example if current
locum medical staffing deteriorated) or even permanent basis. A number of patients
live in areas relatively equidistant between sites; a transfer of routine admitting site
from WCH to CIC (i.e. a marginal postcode shift) may make minimal differences to
patients, their visiting families and ambulance services, but considerably relieve
pressure on the WCH site (given current fragility of medical workforce).
There are various possible permutations, but for modelling purposes additional options
are identified as:
a. All blue lights transfer to CIC between 21.00 and 08.00
b. All acute admissions including GP and self-referrals transfer to CIC between
21.00 and 08.00
c. All acute admissions including GP referrals and self-referrals transfer to CIC
between 21.00 and 08.00 PLUS marginal postcode shifts during day
d. Marginal postcode shifts alone at night only
e. Marginal postcode shifts alone all times of day

26
Activity Changes & Bed Capacity
Assumptions & Modelling
The following high-level modelling undertaken on the high risk medical pathways has
been validated by Price Waterhouse Coopers; it has deliberately erred on the side of
caution in other words by other estimating where there is room for doubt. However
further more detailed modelling and scenario analysis will be required. For the
purposes of modelling it is assumed:
current NEL presenting activity and proportion of required admissions remain
in line with 2013/14 for WCH;
whilst the medical workforce changes in WCH surgical teams from August
2014 are factored into the baseline, other anticipated pathway changes
(potentially reducing surgical admissions) do not immediately occur.
Bed capacity work for Option UC1 & 2 assumes:
Repatriation to WCH after average 3 days LOS following transfer to CIC;
85% bed occupancy;
Some patients deteriorate on EAU/base wards at WCH and may need to be
transferred – a cautious over-estimate of ‘worst case’ is modelled
UC2 options all INCLUDE bed shifts relating to UC1.
Night time admissions defined as occurring between 21.00 and 08.00
UC2a based on admissions to WCH for majors arriving by ambulance
Postcode shifts based on ambulance and GP referred arrivals from specified
ward
The table below shows anticipated additional transfers/diversions from WCH to CIC for
UC1 patients over and above patients already transferring from WCH:
Additional CIC patient transfers :
Transfers/diversions per year
Transfers/diversions per week
Transfers/diversions per day
UC1:
High risk pathways
444 8.5 1.2
NEWS (including transfers from EAU/wards)
600 11.5 1.7
TOTAL 1044 20 3.0

27
UC2 modelling includes the transfers associated with UC1 i.e. it sets out the
cumulative impact of the options. Modelling has adjusted to remove potential double
counting with UC1:
Additional CIC patient transfers :
Transfers/diversions per year
Transfers/diversions per week
Transfers/diversions per day
UC2a - All blue lights at night
1,486 28,5 4.1
UC2b - All acute admissions at night
3,306 63,4 9.1
UC2c All acute admissions at night plus postcode shifts all times
4,083 78.3 11.2
UC2d - Postcode shifts at night
1,450 27.8 4.0
UC2e - Postcode shifts all times
2,228 42.7 6.1
For the transfers/diversions modelled at UC1 it is likely that circa 35% of these would
take place between the hours of 21.00 and 08.00.
The table below summarises the anticipated associated bed requirement changes:
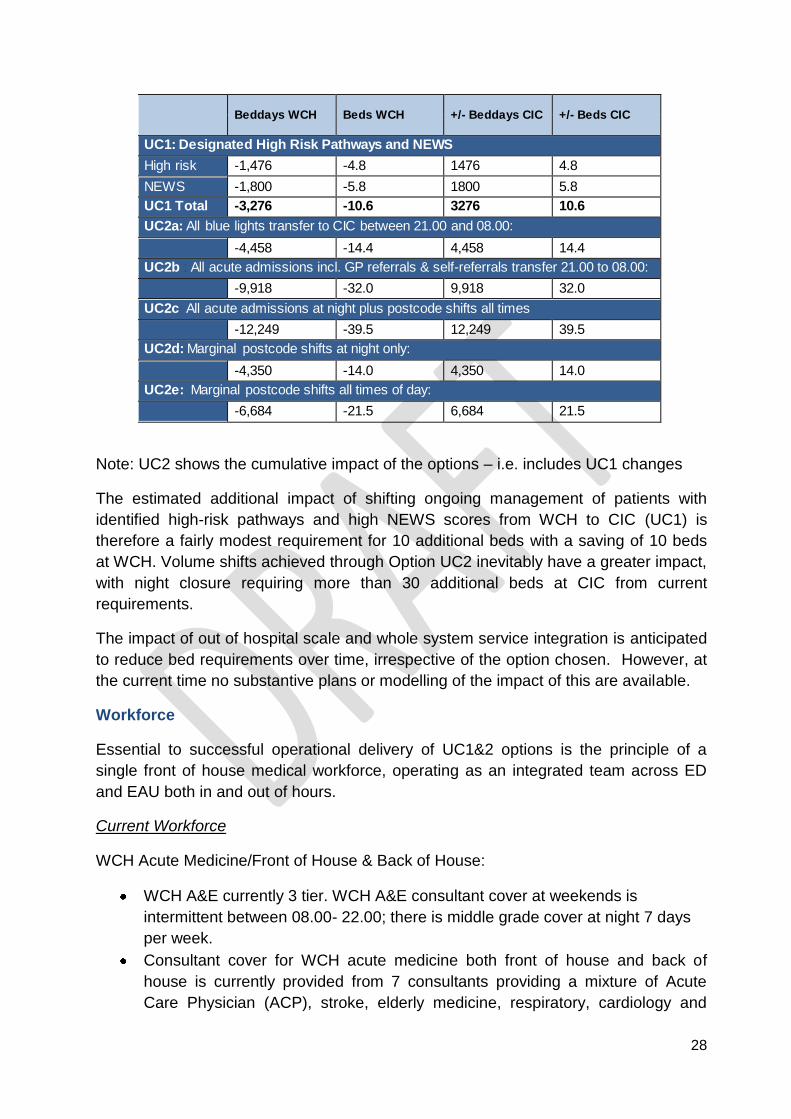
28
Note: UC2 shows the cumulative impact of the options – i.e. includes UC1 changes
The estimated additional impact of shifting ongoing management of patients with
identified high-risk pathways and high NEWS scores from WCH to CIC (UC1) is
therefore a fairly modest requirement for 10 additional beds with a saving of 10 beds
at WCH. Volume shifts achieved through Option UC2 inevitably have a greater impact,
with night closure requiring more than 30 additional beds at CIC from current
requirements.
The impact of out of hospital scale and whole system service integration is anticipated
to reduce bed requirements over time, irrespective of the option chosen. However, at
the current time no substantive plans or modelling of the impact of this are available.
Workforce
Essential to successful operational delivery of UC1&2 options is the principle of a
single front of house medical workforce, operating as an integrated team across ED
and EAU both in and out of hours.
Current Workforce
WCH Acute Medicine/Front of House & Back of House:
WCH A&E currently 3 tier. WCH A&E consultant cover at weekends is
intermittent between 08.00- 22.00; there is middle grade cover at night 7 days
per week.
Consultant cover for WCH acute medicine both front of house and back of
house is currently provided from 7 consultants providing a mixture of Acute
Care Physician (ACP), stroke, elderly medicine, respiratory, cardiology and
Beddays WCH Beds WCH +/- Beddays CIC +/- Beds CIC
UC1: Designated High Risk Pathways and NEWS
High risk -1,476 -4.8 1476 4.8
NEWS -1,800 -5.8 1800 5.8
UC1 Total -3,276 -10.6 3276 10.6
UC2a: All blue lights transfer to CIC between 21.00 and 08.00:
-4,458 -14.4 4,458 14.4
UC2b : All acute admissions incl. GP referrals & self-referrals transfer 21.00 to 08.00:
-9,918 -32.0 9,918 32.0
UC2c All acute admissions at night plus postcode shifts all times
-12,249 -39.5 12,249 39.5
UC2d: Marginal postcode shifts at night only:
-4,350 -14.0 4,350 14.0
UC2e: Marginal postcode shifts all times of day:
-6,684 -21.5 6,684 21.5

29
general medicine on call: 5 ACPs work 8am-6pm on weekdays, with physician
of the day presence until 10pm.
There is consultant presence at weekends covered by Locum Physician of the
Day from 0800-22.00; overnight cover is provided 6 nights out of 7 and all
weekends by Locums.
4 middle grade doctors in medicine at WCH provide 24 hour cover over 7 days
a week; CTs/GPVTS cover acute medicine working to a 1 in 9 rota.
F1 Acute Medicine doctors covering the Back of House rota have been
replaced (August 2014) by Nurse Practitioners supported by Consultants.
Nurse Practitioners also provide back of house 24/7 support to medical and
surgical wards with a further 7 working in ambulatory care.
7 F1 Doctors continue to cover Front of House during the daytime where they
receive training and supervision from a Consultant. From August 2015 the F1
Front of House role is covered by Nurse Practitioners supported by the GPVTS
grade of Doctors and ACP
Emergency General Surgery:
Consultant presence 8am to 6pm and 9am -12pm at weekends
Middle grade cover 8am-8pm 7 days per week
After 8pm, Hospital @Night Team cover to wards, with specialty surgical
emergency assessment support/provision from CIC
1 consultant for anaesthetics/ITU on-call for all streams, plus 1 resident middle
grade (all streams), plus 3rd tier consultant provision for contingency cover
CIC:
CIC acute medicine includes ACPs between 8am and 10pm, resident middle
grade medical cover and a consultant on-call from home.
2 consultant anaesthetists on-call – 1 for ICU, 1 for theatres/maternity. 1
resident middle grade OOH plus ICU consultant on-call from home and only as
required at weekends; A&E anaesthetics cover until 22.00.
Option UC1
It is proposed that implementing a transfer process for High Risk Patients to CIC and
reducing the acuity of non-elective admissions at WCH, coupled with the right
combination of Consultants, ACPs, GPVTS and Trust Doctors and Nurse Practitioners
covering Front and Back of House will ultimately allow removal of locums whilst
maintaining acute medical services
Single medical workforce at night operating as an integrated team with staff
generalist competencies that undertakes triage assessment and immediate
management for surgery and medicine across an integrated front of house.
Work is already progressing to develop attractive joint posts with primary care
colleagues to provide stability and a substantive tier at CT/GPVTS level.

30
After a period of stabilisation arrangements could move from 2 separate
consultant rotas for each site, to a single consultant physician on-call rota from
home with a second on-call back-up in operation. This change could have a
major positive impact on sustainability.
Movement over time towards an integrated model for ED consultant workforce
cross-trust.
Assumes additional front of house workload of 3 patients per day at CIC can be
absorbed within current medical staffing levels.
Over time, high acuity/ICU beds and outreach service are managed by a
Critical Care Nurse Practitioner supported by a resident middle grade
intensivist/anaesthetist including transfer/retrieval team and consultant on call.
(In the event of no on-site ventilated patients and no obstetrics, there may be
potential for remodelled utilisation of medical and nursing roles to manage the
high acuity and HDU beds 24/7)
Option UC2
If WCH were to accept no overnight admissions (UC2b) it is assumed that this would
allow further consolidation of the ED/Front of House medical workforce at WCH, and
of ED on-call at CIC with reduction in consultant on-call requirements cross-trust: there
would then be an expectation over time of integrated Front of House consultant on-call
rotas cross-site, and flexible use of available substantive consultant staff based on
competencies, changing over time to dual trained recruitment where possible.
Other UC2 variations would not make any additional substantive change to the
medical workforce model (aside from that required to support back of house beds).
Clinical Support, Estates & Facility & Issues
Clinical Support
It is assumed that there would be no net impact on pathology and radiology services
across the Trust; it will however be critical for early involvement of clinical support
colleagues in any detailed plan development. The siting of major surgery (and
obstetrics) has implications for blood transfusion service and delivery. This will also be
relevant if major GI bleeds are consistently to be transferred from WCH to CIC.
Depending on what else is required at the WCH site, there may be a need to modify
stocked levels of O negative blood for stabilisation pre transfer purposes.
The vision for critical care anticipates a journey over time, making optimal use of
available WCH and CIC resources to support changes, with anticipated gradual
reduction (but continued as necessary) Level 3 activity at WCH, increase in Level 2
provision and with converse changes at CIC. This includes long-term
capacity/capability to stabilise, ventilate and manage Level 3 patients until such time
as care is appropriately transferred. Care will be designed to ensure Intensive Care

31
Standards8 can be fully met, and key to this is safe transfer between sites, and an
increase in CIC capacity:
Critical Care beds at WCH would operate as a continuum with higher acuity
beds used (a) as support for unstable/ deteriorating medical patient (or surgical
with medical complications); (b) for care for sicker patients from front of house
who are not transferred including severe sepsis; (c) for patients repatriated from
CIC ICU once stepped-down from organ support; and (d) for potentially small
numbers of new elective patients: for example, revision hip arthroplasty. All
local patients requiring NIV would be managed in ICU facilities.
CIC activity has already increased as a result of transfer of high risk surgical
pathways and elective demand. The 4 designated high risk medical pathways
are unlikely to significantly impact on critical care demand although those with
high NEWS scores will: it is estimated that UC1 would result in an additional
100 patients with a CIC critical care stay. These patients are likely to be at the
higher acuity end with an estimated average LOS of 4.5 days. This represents
450 bed days or 1-2 additional beds.
Whilst this additional demand on top of existing increased pressures will
necessitate facility expansion at CIC it is currently assumed that there is no
overall net increase in critical care bed requirements across the Trust.
Containment is expected to be achieved through a combination of reduced
Level 3 demand at WCH with more flexible and integrated use of high
acuity/HDU & CCU beds within the new facility, including different management
of overdose patients, transfer of stroke patients and changes to paediatrics. It is
not anticipated that increased elective activity at WCH would significantly
impact on critical care demand given the need to ensure a casemix where there
is minimal risk of requiring return to theatre.
Consideration needs to be given to appropriate staffing for patient retrieval.
Estates & Facilities
It is proposed that high risk medical patients transferred to CIC at UC1 will be
managed on the second floor with all patients initially managed through Larch A/B
prior to transfer to specialty wards:
Acute stroke – Elm A
ACS – Willow C/CCU
GI Bleed – Beech A
NEWS 5> - Larch A/B
To achieve the optimal clinical outcomes being sought will require careful
consideration of speciality requirements and configurations to ensure we can place
patients in the ‘right bed’. In advance of longer-term re-configuration of the CIC estate,
8 The Faculty of Intensive Care Medicine/Intensive Care Society, Core Standards for Intensive Care Units, 2013

32
this will require the transfer of bed space for 10 patients from the second floor
environment into alternative accommodation.
Longer term a business case is being developed (value circa £30m) to create a new
fifth Pavilion at CIC to house A&E, EAU, ambulatory care, cardiology services
(including CCU the Cath Lab) with reconfiguration of other services to improve clinical
adjacencies, infection control and patient experience. These proposals could be
developed to ensure capacity for UC2 requirements.
The acute bed reductions in UC1 &UC2 at WCH would be netted off against the 30
acute and sub-acute medical bed base modelled into the WCH Redevelopment
Business Case, noting that the staffing requirements are not identical. This would
ensure flexibility to manage planned increases in elective workload over time. Any
further (probably sub-acute) changes to bed requirements would need to be modelled
once anticipated increased primary/community care capacity takes effect.
Option Appraisal and Discussion
As highlighted in local Risk Summits and in the Chief Inspectors of Hospital’s report,
there are significant and unacceptable risks in continued delivery of services operating
to the current model due to the ability to recruit and retain sufficient substantive
medical staff. Services at night following changes to junior and non-medical staff from
August 2014 have been secured through a Nurse Practitioner H@N model but whilst
currently safe, arrangements are very fragile given their reliance on locums, posing a
risk in maintaining safe management of unselected medical admissions (both in terms
of complexity and volume) in the longer term. Without change to the casemix and
volume of current non-elective medical activity, the middle grade tier at WCH (which is
currently fully made up of locum staff) will continue to be required with little prospect of
substantive recruitment. This creates a cost pressure in excess of £1.0m per annum,
in addition to the quality impact on patient care.
Introducing a system for transfer/diversion of high risk patients as in Option UC1 safely
manages the current WCH workforce risks by day and night with reduced locum
reliance. This would be the clinically preferred option as it explicitly seeks to improve
clinical outcomes for high risk patients as opposed to a pathway decision based on
service necessity. The model continues to retain resident anaesthetic/intensivist
support for front and back of house necessary to safely run an unselected A&E. (Note
the obstetric/neonatal issues in relation to running multiple anaesthetic streams).
Unnecessary patient journeys can be avoided by maximising the patients who can be
identified prior to arrival at hospital in community settings and directly diverted to CIC,
although clearly there is still impact on relatives’ journeys. The initially anticipated (and
modelled) additional length of stay for patients transferred/diverted can be mitigated by
access to better diagnostics and other resources at CIC and increasing integrated
working with community providers both facilitating swifter discharge.
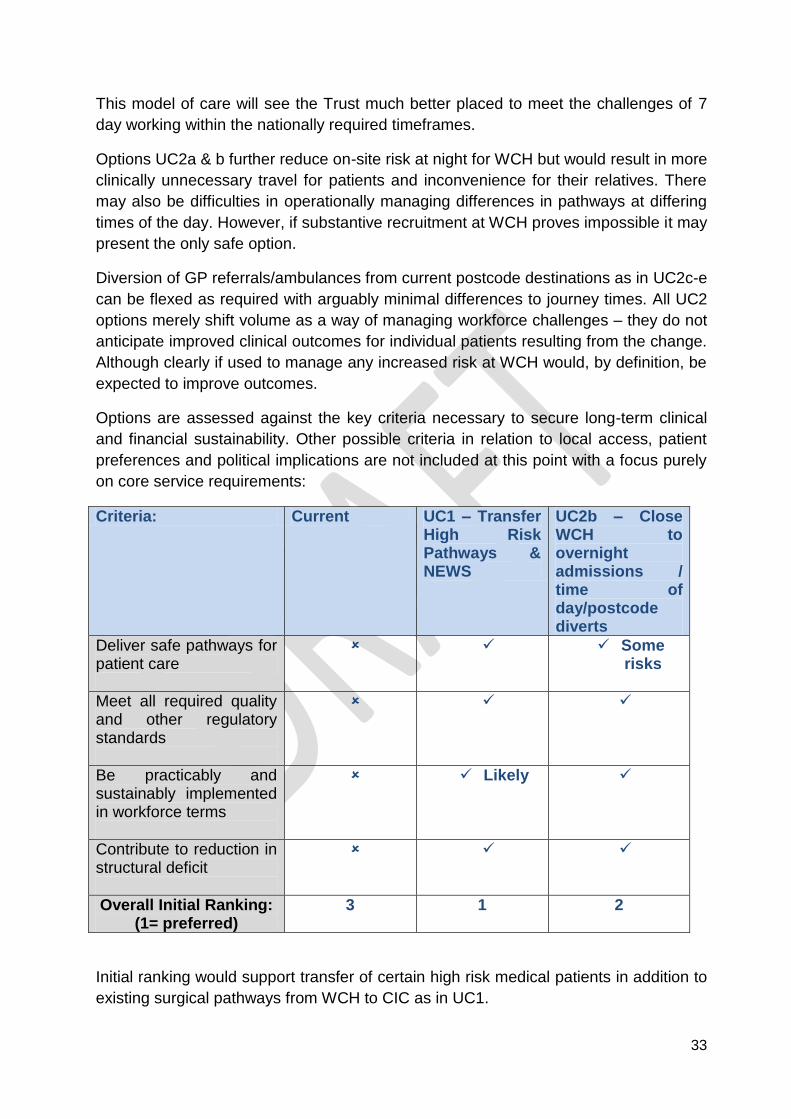
33
This model of care will see the Trust much better placed to meet the challenges of 7
day working within the nationally required timeframes.
Options UC2a & b further reduce on-site risk at night for WCH but would result in more
clinically unnecessary travel for patients and inconvenience for their relatives. There
may also be difficulties in operationally managing differences in pathways at differing
times of the day. However, if substantive recruitment at WCH proves impossible it may
present the only safe option.
Diversion of GP referrals/ambulances from current postcode destinations as in UC2c-e
can be flexed as required with arguably minimal differences to journey times. All UC2
options merely shift volume as a way of managing workforce challenges – they do not
anticipate improved clinical outcomes for individual patients resulting from the change.
Although clearly if used to manage any increased risk at WCH would, by definition, be
expected to improve outcomes.
Options are assessed against the key criteria necessary to secure long-term clinical
and financial sustainability. Other possible criteria in relation to local access, patient
preferences and political implications are not included at this point with a focus purely
on core service requirements:
Criteria: Current UC1 – Transfer High Risk Pathways & NEWS
UC2b – Close WCH to overnight admissions / time of day/postcode diverts
Deliver safe pathways for patient care
Some risks
Meet all required quality and other regulatory standards
Be practicably and sustainably implemented in workforce terms
Likely
Contribute to reduction in structural deficit
Overall Initial Ranking: (1= preferred)
3 1 2
Initial ranking would support transfer of certain high risk medical patients in addition to
existing surgical pathways from WCH to CIC as in UC1.
34
Obstetrics & Midwifery: Intrapartum Care including
Neonatology
Current Service
Obstetric care is provided at both Trust sites with 1686 births at CIC in 2013 and 1313
at WCH. Each service has dedicated staff and there is no cross-over for emergencies.
Day assessment unit services are provided on both sites. Additional midwifery led care
is provided at the Penrith Birth Centre and throughout the community including choice
of home births. A review of midwifery services in 2012 has enhanced provision with
the creation of specialist midwifery and supernumerary posts and a robust
preceptorship programme.
Five consultants contribute to obstetrics and gynaecology services on both sites, the
clinical director working across both. This allows 40 hours per week dedicated
prospective presence and a 1 in 5 delivery suite rota with 1 post currently covered by a
locum consultant to backfill the Gynaecology/Oncology Lead Consultant. A further
consultant is covering a middle grade vacancy at CIC.
Proposed Clinical Pathway Options
It is assumed that whatever the outcome of the planned Independent Maternity
Review, changes will be needed in line with one of the potential options outlined
below. All options are expected to operate as part of a Cumbria-wide maternity
network including community-based provision. Community midwifery care, plus
antenatal and postnatal clinics would continue to be delivered at all existing sites, with
expansion where at all possible to improve access to local services. Option appraisal
relates only to the delivery/birth (Intrapartum) element of care.
The option of a single obstetric unit at WCH and no intrapartum provision at CIC is not
modelled: this is not a feasible option given (i) previously consulted-upon decisions to
centralise high risk pathways at CIC and (ii) distance from specialist emergency
support. Both these factors would prevent safe intrapartum management of higher risk
patients in Cumbria in this model, as well as denying the greatest number of patients
local access.
Option OB1 – Enhanced 2 Site Consultant-led Intrapartum Care
In this Option the current regulatory compliance and quality issues have been
addressed through the enhanced provision of anaesthetic support and through a
dedicated obstetric theatre. An MLU would operate immediately adjacent to the
consultant unit, with a degree of shared resource and ability to manage primigravida
patients due to its co-location.

35
Option OB2a – CIC Consultant-led Intra-partum Care plus WCH MLU
All women identified as at higher risk and potentially requiring intrapartum consultant
input, including all primigravida patients, are managed at CIC. An MLU is provided at
WCH for low risk multiparous patients9. Women requiring/requesting epidural would
need ante- or intrapartum transfer to CIC. This option would require transfer of some
women/babies in labour and post-natally to the Obstetric Unit. There would be no
Special Care Baby Unit (SCBU) on site, with care for neonates provided by an
appropriately trained midwife at all times. WCH would provide antenatal care and,
subject to further clinical discussion, potentially planned (low risk) caesarean sections.
Option OB2b – CIC Consultant-led Intra-partum Care plus standalone Allerdale
MLU
All women identified as at higher risk and potentially requiring intrapartum consultant
input, including all primigravida patients, are managed at CIC. A standalone MLU is
provided in Allerdale for low risk multiparous patients. Women requiring/requesting
epidural would need ante- or intrapartum transfer to CIC. This option would require
transfer of some women/babies in labour and post-natally to the Obstetric Unit. There
will be no Special Care Baby Unit (SCBU) on site at WCH, with care for neonates
provided by an appropriately trained midwife at all times.
WCH would continue to provide antenatal care as well as the Allerdale Unit.
Activity Changes
The intrapartum activity anticipated from the different models is shown based on best
practice criteria and national percentages for women suitable for MLU delivery10:
Current Model OB1 OB2a OB2b
WCH
CIC Other
WCH
CIC Other
WCH
CIC Other
Aller
CIC Other
Births11
1278
1698
41 1278
1698
41 336 2640
41 336 2640
41
This activity assumes no loss of market share and no increase in home/birthing centre
births.
9 Royal College of Midwives, Freestanding Midwifery Units, Local high quality maternity care: Busting the Myths,
2014 10
Royal College of Obstetricians’ & Gynaecologists, Reconfiguration of Women Services in the UK, Good Practice No. 15, December 2013 11
Total births assumed are based on trend not 2013 figures
36
Workforce
Workforce modelling will be based on Birth Rate Plus, RCM Guidance Paper 2009 and
Safer Childbirth, 2007. Assumptions for the models include:
Option OB1 - Enhanced 2 Site Consultant-led Intra-partum Care
24/7 dedicated anaesthetic cover both sites.
2nd maternity theatre both sites
Epidural provision both sites (an EWTD compliant rota for a full obstetric
service including epidural requires a minimum of 8 staff).
Staffing for 2 elective LSCS lists adequately covered at WCH.
Option OB2a & OB2b - CIC Consultant-led Intra-partum Care plus WCH MLU/
standalone MLU
24/7 dedicated anaesthetic cover at CIC.
Midwives 24/7 across the MLU/CLU at CIC, and standalone MLUs
It is noted that MLU staffing is dependent on exact model chosen.
Proposed changes at OB2a & 2b anticipate the ability to secure a more permanent
consultant workforce in 3 years.
Medical Staffing Special Care Baby Unit (SCBU)
The overall provision of SCBU is inextricably linked to the medical staffing of the
paediatric department, and the overall paediatric medical staffing requirements will be
dependent on obstetric options. Workforce implications for the chosen model largely
(but not wholly) relate to nursing requirements, with deployment of neonatal nurses to
the obstetrics centre(s) in line with the chosen model.
Facility & Clinical Support Issues
It is assumed that an enhanced model with co-located MLUs would require revision of
current facilities to create an appropriate and separate MLU environment.
Single site obstetrics as at OB2a and OB2b would require significant re-configuration
of space at CIC to accommodate the anticipated additional 942 births, including an
MLU facility.
An MLU at WCH as in OB2a could be relatively easily accommodated within plans for
WCH redevelopment; a standalone MLU as in OB2b would require significant capital
investment, as well as ongoing revenue commitment.
It is assumed that there would be no net impact Trustwide on clinical support
requirements arising from implementation of OB1 or OB2a. There would however be
clinical support implications for a standalone facility as at OB2b which would need to
37
be appropriately modelled; these would include imaging, pathology and pharmacy
support as well as ancillary support services. The siting of obstetrics has implications
for blood transfusion service and delivery.
Option Appraisal & Discussion – Consultant-led Intrapartum Services
Whilst a 2-site consultant service would be preferable in terms of local access for
patients it is with reluctance that the Board’s initial opinion is that this is likely not a
realistic option for the medium-long term future. The principal issue relates to
anaesthetics: to secure a regulatory compliant and safe 2-site service in the longer
term as described at OB1 requires significant recruitment of Trust obstetrically
competent anaesthetists. To provide dedicated resident anaesthetic cover for
obstetrics out of hours on both sites, plus 12 consultant PAs per week for emergency
work on delivery suite as well as elective LSCS cover would require potentially up to
16 more anaesthetists (consultant and middle grade – estimated at 12 at WCH and 4
at CIC).Irrespective of any additional funding opportunities, success in recruiting to
such a number of additional medical posts is highly unlikely – even if posts were made
more attractive by separation of maternity/ITU cover. The Trust has repeatedly been
unsuccessful in recruitment of Trust grade doctors, likely due in part to the
unattractiveness of out of hours responsibilities, alongside the other local factors of
professional isolation and low volumes to maintain skills and develop specialist
interests.
Despite sustained efforts driven by a common desire to maintain 2-site provision, no
model for ITU/Anaesthetics has been identified to date that is both sufficiently safe
and can be practically implemented. The challenge is inextricably linked with future
arrangements for acute medicine – whilst it is envisaged that a resident anaesthetist is
maintained at WCH they would only be able to run one stream of care, not two – this
then points to a judgement call in relation to the preferred stream to maintain.
For obstetrics, this situation is further compounded by difficulties in recruitment to
middle grade and consultant obstetricians. The position is highly unlikely to change in
the foreseeable future.
The Board has considered at length how consultant led intra-partum services might
conceivably be maintained on 2 sites. The challenges of this have been much debated
both internally and externally with commissioning partners and others, with the Board
very keen that the Independent Review should take place as soon as possible, and
also cognisant of its responsibilities to ensure appropriate risk mitigation plans are in
place. However, and in advance of this Review and further work, the challenges are
considered by the Board at this early stage to be such that a 2 site model appears
impossible to deliver against current regulatory guidelines and NICE guidance.
If consolidation of obstetric intra-partum services onto 1 site were to be ultimately
agreed it is considered that due to availability of other services, in particular dedicated

38
anaesthetic/intensivist streams and surgical services, plus distance to the tertiary
centre, single–site consolidation would necessarily be at CIC.
Consideration has been given to how access for our expectant mothers living in West
Cumbria could be additionally enhanced if obstetrics were consolidated at CIC. The
option for an MLU at WCH whilst attractive, is considered by some senior clinicians to
pose a small but unacceptably high risk given its distance from the consultant-led unit,
as well as poor patient experience for women and babies requiring intrapartum or
post-partum transfer. This is an opinion which greatly concerns the Trust Board. On
the basis of peer reviewed research, these risks may be reduced to more acceptable
levels by siting the MLU in Allerdale far closer to the consultant-led facility.
However, to support this option still requires additional consideration of how the
possible impact on perinatal mortality from longer travel times can be mitigated
against, noting that distance from mother’s homes as well as from the MLU is relevant
in this context. The Trust would expect to learn from the experience and solutions in
other countries such as Scotland; this would include excellence in antenatal/postnatal
care and risk assessment, and enhanced travel and possible hotel arrangements as
key, with choice maximised where at all possible for lower risk deliveries.
Our aims at all times will be to minimise risk, deliver care locally wherever possible
and maximize women’s choices
Assessment of the possible options is shown below against the key criteria necessary
to secure long-term clinical and financial sustainability. As before, other possible
criteria in relation to local access, patient preferences and political implications are not
included at this point with a focus purely on core service requirements.
Criteria:
Current OB1- Enhanced 2 Site Obstetrics
OB2a – CIC CLU/MLU & WCH MLU
OB2b – CIC CLU/MLU & Allerdale MLU
Deliver safe pathways for patient care
?
Meet all required quality and other regulatory standards
Partially met
Be practicably and sustainably implemented in workforce terms

39
Contribute to reduction in structural deficit
Not formally ranked given awaited independent maternity review
- - - -
To make a fully informed and final judgement on obstetric challenges requires an
understanding of the findings of the Independent Maternity Review and further
detailed work with clinicians to consider all possible options and their implications, with
any decisions founded upon a firm evidence base. However, and notwithstanding the
outcome of the Independent Review, based on evidence available to date (and
acknowledging that the model may still be relatively expensive) OB2b is believed to be
the safest sustainably implementable option at this current time. Such a consolidated
consultant-led intra-partum delivery unit configured as part of a Cumbria Maternity
network would require rigorous mitigation of issues/risks caused by increased travel
for delivery, excellence of care throughout the perinatal period, with choice to enable
local provision for lower risk mothers wherever possible through home births and an
MLU.
As a service of significant patient/public interest, any proposed changes would require
comprehensive user engagement and public consultation led by commissioners;
temporary changes could potentially be required in advance of this in order to maintain
patient safety but would be avoided if at all possible.
It must be stressed that this opinion has been formed in necessary response to
the challenges posed and will be re-visited in light of the expert Review findings.
The Trust remains open-minded to consideration of alternatives which can
demonstrate they better meet the current challenges of consultant-led
provision.

40
Paediatrics
Current Service
The Trust provides paediatric assessment and inpatient services on both sites from a
total capacity of 39 beds. CIC has 24 acute paediatric beds, which operate as 8
assessment beds and 16 inpatient beds from 08:00 hrs – 20:00 hrs, and overnight
with 16 inpatient beds only. WCH has 15 acute paediatric beds, which operate as 8
assessment beds and 7 inpatient beds from 08:00 hrs – 21:00hrs; overnight it
functions as a 15 bedded area. The WCH new development is planned to provide 7
assessment beds and 7 inpatient beds as a 24/7 service.
The current medical rotas at WCH provide a three tier approach six days per week,
currently working with an SHO, speciality doctor, PNP and consultant resident on call.
At CIC consultants are called in from home in an emergency, with very limited middle
grade support.
There are approximately 44 children per day attending NCUH A&E departments12 of
which 40% (18) are at WCH. 25% of these are for medical conditions as opposed to
injuries, and of these 50% are admitted. 50% of unplanned paediatric admissions are
from GP referral. In 2012, 16% of WCH paediatric patients stayed more than 48 hours,
equivalent to 9 per week - these numbers will be lower now as some young patients
with trauma or with surgical needs are already being directed to CIC as a result of
changes of the trauma and surgical pathways.
Proposed Clinical Pathway Options
The Trust paediatric services represent a small but key part of overall child health
provision in North Cumbria – community, tertiary and intensive care elements are and
will remain integral to Trust arrangements. Care Closer to Home previously supported
the development of short term paediatric and assessment services on the WCH site
with the main paediatric inpatient unit to be provided at CIC. The model is one of
‘assess & treat’ with an expectation of increased outreach and community support.
Most elements of future acute service provision are clear but the hours of functioning
of an assessment unit at WCH have remained outstanding and are the partial focus of
the options set out. (It is noted however that there is a clinical argument for acuity
rather than length of stay influencing best management and this issue also requires
consideration.)
A 48-hour Unit option has not been modelled separately: this would require the same
staffing levels as current with additional enhancement in order to comply with College
Guidelines. Given that the vast majority of children are discharged within 48 hours, the
option would require transfer of a maximum of six children per week. (This is likely to
have been over-estimated given (a) that most of these children would not necessarily
be expected to stay more than 48 hours at the point of admission but may end up
12
Note – this is based on 2010 data

41
doing, and (b) impact of a different SSPAU model of working, for instance mental
health patients and children needing IV antibiotics.)
It is noted that paediatric, CCG and CPFT colleagues are currently working closely to
develop an ‘integrated’ model that seeks to meet standards sustainably through
flexible workforce use across organisational boundaries, and anticipates far greater
support for children outside of hospital. Assessment of children would take place in a
variety of settings and not be confined to 2 designated assessment units. High level
modelling of this option is awaited; in the meantime it is accepted that the Trust must
form a view on the options available to address the challenges within the system.
Once further detailed proposals are received it will be possible to review the options
appraisal.
Two potential options are therefore considered in more detail:
Option P1 - 24 hour WCH Short Stay Paediatric Assessment Unit and
paediatrician access plus low acuity beds
14 assessment beds and low acuity beds integrated with enhanced community
provision and CIC support
The unit would be open for assessment of patients 24 hours per day with local
Consultant cover out of hours.
All urgent/emergency for higher acuity needs will be referred/transferred to the
preferred tertiary care centre or the inpatient unit at CIC for further management
Paediatric day surgery would continue and where possible be expanded
subject to clinician agreement
The proposed changes in P1 anticipate the ability to secure more permanent
consultant workforce.
Option P2 – 14 hour WCH Short Stay Paediatric Assessment Unit (SSPAU) plus
24/7 paediatrician cover
Unit open from 08.00hrs to 22.00hrs 7 days per week – 14 assessment beds
integrated with enhanced community provision and CIC support.
08.00 start accommodates day case activity.
Children requiring longer stays would be referred/transferred to CIC which
would therefore require additional bed capacity.
All emergency care out of these hours would default to A&E/intensivists and
Cumbria Health on Call (CHOC) for immediate management and/or transfer to
CIC. This arrangement would be additionally supported by local 24 hour
paediatrician access.
Given the presence of paediatricians on site at WCH during the day time,
paediatric day surgery could continue and where possible be expanded subject
to clinician agreement

42
In either model the WCH SSPAU would be staffed by experience Nurse practitioners
and day time consultant presence with no reliance on junior/middle grade staff.
Additional nurse support would be required to escort patient transfers to CIC, plus
staffing for overnight beds re-designated from assessment. At CIC there will be
continued requirement for either a resident paediatrian or, if feasible in terms of
investment and training PNPs, as well as 2-site consultant on-call. Higher acuity
patients at CIC will require the right level of medical support with an experienced
‘middle grade’ tier of nurse pratitioners and specility doctors. Both options would take
into account additional staffing requirements in order to meet college guidelines:
Additional paediatric consultant cover to ensure on site present from
10.00-22.00 Monday to Friday, plus 09.00-12.00 and 18.00-22.00 at
weekends
Junior doctor at CIC 08.00-22.00
Additional play specialists
Additional nurse practitioners
Additional nightime qualified and unqualified nursing.
Activity Changes
Current Activity at WCH: There has been no significant increase in admissions over
the last 12 months, but a higher percentage of children discharged within 12 hrs:
LOS Fairfield ward 0 <6 Hrs 6 <12 Hrs
12 to 24 hrs
>24 hrs Total % <12hrs
12/13 E&NEL admission 401 257 708 777 2143 30%
13/14 E&NEL admission 524 289 726 618 2157 37%
Using the above table and similar assessment models from other areas assumptions
have been made regarding the possible impact of the SSPAU model on transfer and
occupancy at CIC. Clinical decision-making regarding need for admission is currently
made on the model of acute care available. A change of model will influence the
management of children’s admission and discharge requirements, with anticipated
fewer children requiring admission and consequently fewer transfers. These numbers
therefore reflect likely upper limits:
Option P1 – 24 hour SSPAU plus Low Acuity Beds – Based on the work of our
buddy trust, NHFT, experience of Gateshead Health NHS Foundation Trust and the
43
above 13/14 activity patients it is likely that 80% of current activity could be managed
locally circa – equating to 431 transfers per year, 8.3 per week, or 1.2 per day.
Option P2 – 14 hour SSPAU - 19% of paediatric admissions of less than 12 hours
were admitted at night13. Including these, a total of c1500 patients (1344 +156) would
need transfer to CIC: approximately 4 children per day (29 per week). This estimate
has been adjusted to take into account need to have completed safe transfer prior to
unit night closure.
Facility & Clinical Support Issues
With current midnight occupancy at CIC based on 16 overnight beds at 60%, and an
assessment unit model with rapid assessment and ‘discharge’, it is considered unlikely
that the physical number of beds in CIC will need to increase at P1 or P2 (although
some current assessment beds would be re-designated as inpatient beds).
It is assumed there would be no net impact on clinical support requirements; however
consideration is needed in relation to appropriate stabilisation and management of
children requiring HDU/ICU care, CIC HDU capacity, and safe transfer to Newcastle,
where this is a more suitable destination than CIC.
Option Appraisal & Discussion
A 24/7 full inpatient service on 2 sites is not considered viable long-term on the basis
of the medical staffing requirements including need for paediatric critical care support,
given difficulties in recruiting both anaesthetists and to a lesser extent paediatricians.
Most importantly, consolidation of in-patient services onto one site is expected to
create a more robust service including appropriate management of ward-based
dependent children. This approach including centralised care for critically ill children,
coupled with local access to high quality assessment provision is in line with the
general direction of travel nationally for delivery of high quality acute children’s
services.
A more robust paediatrician rota could be sustained if the two current rotas combined
and provided cross site medical staffing rotas with just one 24/7 site providing out of
hours on call. However, there is a genuine concern in relation to the management of
very acutely ill-children self-presenting to A&E outwith of SSPAU opening hours as in
P2. These numbers would likely be very small (the vast majority of patients can be
diverted out of hours –see below) and the risk could be mitigated through access to a
local consultant paediatrician at night. Assuming successful recruitment to nurse
practitioner posts, P2 offers the greatest likelihood of the Trust compliance in the long-
13
2011/12 data

44
term with College standards in respect of workforce requirements, although current
paediatric workforce can support P1.
P1 and P2’s success is in part dependent on increased high quality community
support, and this is particularly true for P2 out of hours. However, only 2-3 patients per
day requiring admission present via A&E at WCH and 85% of these are between 9am
and 10pm14 . For those who do present, the integrated front of house workforce
including critical care support would be anticipated in P2 to be able to safely provide
immediate management prior to transfer and/or where appropriate assistance from a
local paediatrician.
For P2 and to a lesser extent P1 safe transfer of children, with appropriate clinical
support and timely response is a key issue particularly for very sick children. The
additional numbers of children requiring transfer in P2 as opposed to P1 are
approximately 2 per day (17 per week). 68% of unplanned admissions are GP
referrals, and 21% arrive by ambulance at A&E with only 11% self-presenting via the
A&E department15; therefore referrals may potentially be immediately diverted to CIC
where it is clear that a longer admission is required as well as outside of SSPAU
hours. Seasonal issues impacting on transfer rates (e.g. children with bronchiolitis),
and the need for early - and potentially unnecessary - transfers must be considered,
as must be the impact on families of long travel times.
Consideration must also be given to length of stay versus acuity requirements and the
justification for transferring children with low acuity needs. In a model with 24hour
paediatric assessment service there is a good argument for provision of low acuity in-
patient beds for those children not requiring continual nursing/medical input – the
precise criteria for ‘low acuity’ admissions would require detailed clinical work.
Other issues which would need to be addressed for P1 or P2 to be successfully
implemented include:
Development and investment in current paediatric staff nurses to achieve
Paediatric Nurse Practitioner status (requirements reduced in P2) to deliver this
new model of care. Whichever option in relation to hours of operation is chosen,
implementation will require considerable lead in time for required nurse
practitioner training.
Need for additional resources to enable increased rapid access clinics or
outreach community nursing support to facilitate earlier discharge. Successful
achievement of this would further reduce tariff income.
Integration of child health provision across North Cumbria. This offers
significant opportunities for both quality and efficiency improvements and would
be expected to reduce admissions over time.
14
Based on 2010 data 15
Based on 2013 A&E HED data

45
Trust wide management of children with HDU-level requirements. Anaesthetic
issues have been explored in the previous section; arrangements to manage
safe airways and to meet standards for children requiring HDU must be re-
visited irrespective of the option chosen.
Whilst not of primary importance in the context of this work, it should be noted that the
volume of activity is insufficient to financially support two in-patient units under current
funding arrangements - a situation which would be further exacerbated by successful
introduction of both the hospital assessment model and out of hospital child health
care. Conversely, staffing requirements may reduce as a result of both swifter
assessment in hospital and reduced numbers requiring hospital assessment.
Options are assessed against the key criteria necessary to secure long-term clinical
and financial sustainability. As previously, other possible criteria in relation to local
access, patient preferences and political implications are not included at this point with
a focus purely on core service requirements:
Criteria: Current P1 - 24 hour SSPAU plus low acuity beds
P2 - 14 hour SSPAU including 24/7 paed. cover
Deliver safe pathways for patient care
Meet all required quality and other regulatory standards
Be practicably and sustainably implemented in workforce terms
Possible
Contribute to reduction in structural deficit
Overall Ranking: (1= preferred)
3 1 2
In summary there is a clear strategic direction for secondary care paediatric services
to form part of a system-wide integrated model of care with increased levels of safe,

46
high quality community based provision, supported by secondary care, a single
inpatient unit, and with a common and localised approach to paediatric assessment.
The SSPAU model forms a key part of this, and for WCH will be delivered by
consultants and nurse practitioners working at a senior level with no reliance on junior
doctors. WCH will continue to have 24-hour access to a consultant paediatrician.
A key issue relates to hours of SSPAU operation. Whilst P2 is most likely to be most
sustainable long-term in workforce terms, there are concerns in relation to
unnecessary transfers of small numbers of sick children at night, as well as
consideration of acuity versus length of stay issues.
P1 if therefore considered the most appropriate option at this time – but noting that
workforce and activity issues may require this model to be re-visited in the future.
Further work and clinical discussion is needed to define and fully model the low acuity
local care provision and to progress a whole system integrated solution for child
health.
Elective Care
Inpatient & Day Case
A core element of the clinical strategy is increase to the non-complex elective and day
case activity taking place at WCH. The aim of this is to:
Maximise the total volume of care that can be provided locally to West
Cumberland patients
Enable successful and sustainable delivery of A&E, Cancer and 18 week
standards through the most efficient use of available elective care capacity
Take advantage of the new facilities and staff skills at WCH to create a positive
choice for elective care for all North Cumbria patients - and potentially from a
wider catchment - with WCH becoming an Elective ‘Centre of Excellence’
Work undertaken to consider day case and elective in-patient activity across both CIC
and WCH has included clinical review of procedures that could be undertaken safely
at WCH, as well as current in-patient activity that could be converted to day case
procedures based upon BADS 25 information. Consideration has been given to
theatre utilisation improvements and theatre/bed capacity requirements. Work is well
advanced for general surgery and urology:
Specialty Theatre Utilisation
Annual In patient cases to move from CIC to WCH (beddays)
Additional monthly Theatre lists required at WCH at 80% utilisation
Annual Day Cases to move from CIC to WCH
Additional monthly Theatre lists required at WCH at 80% utilisation
Current% Proposed%

47
General Surgery
56 80 480 (765) 5 372 8
Urology
52 80 312 (405) 2 396 5
The additional theatre capacity for 8 lists per month (proposed inpatient lists) can be
created from current facilities using Trust-wide staffing resource. Additional capacity
would however be required to cover the day case activity in advance of the new
hospital, but after April 2015 can be absorbed within this facility. Staffing potentially
freed up at CIC may be unavailable if reallocated to manage 18 week backlog
pressures, requiring some additional interim support; this is a particular risk in relation
to anaesthetic staff. Other considerations include the need for radiology support for
pre-operative guide wire insertions and other in-theatre requirements.
Proposed shifts in in-patient activity corresponds to freeing up 4 beds at CIC and
which could be absorbed in the current surgical business unit bed base on Overwater
Ward at WCH. Additional day case theatre lists will require some realignment and
maximised utilisation of the day case and bed facilities. Longer term reconfiguration
can be agreed for when the new hospital opens in April 2015 and which takes into
account changes agreed as described for unscheduled pathways.
Indications are that shift of in-patient activity for general surgery and urology can begin
within the next few months, with day care following once the new hospital facility is
open. Plans are advanced for a shift in (initially non-wire) breast surgery including
reconstructions with a WCH-based symptomatic outpatient clinic for new patients.
Further work needs to be undertaken to scope potential for a shift in gynaecological
work and in orthopaedics, in combination with work to determine sustainable 18 week
delivery post April 2015.
All these anticipated shifts are subject to active patient choice. Other factors and their
costs will need to be fully modelled, although it is assumed that there is no need for
additional HDU support at WCH with the possible exception of care for hip revision
patients.
Outpatients
A significant proportion of outpatients are seen at CIC from Eden, Copeland and
Allerdale localities. Considering only those specialties where more than 1000 patients
are seen from non-Carlisle localities, the table below shows potential volumes for
‘repatriation’ to WCH. Assuming that patient choice already influences location to
some degree a modest potential 50% repatriation is shown. It is however anticipated
that the new build at WCH will provide both additional facility opportunities and likely
influence patient choice to make this shift even greater.

48
Specialty Annual Copeland Patients
Potential Estimated 50% Repatriation
Ophthalmology 1172 586
Orthopaedics 1034 517
Orthodontics 1581 791
ENT 428 214
Breast Surgery 1105 553
Gynaecology 305 153
Rheumatology 325 163
Oral Surgery 489 245
Cardiology 109 55
Radiotherapy 420 210
Dermatology 548 274
Gastroenterology 194 97
Urology 97 49
Dermatology Nurse 401 201
TOTAL 8,208 4,108
It is noted that there will be other possible venues in West Cumberland, including
Cleator Moor, and GP surgeries, although these will not necessarily always be suitable
depending on patient volumes and clinical, facility and/or equipment restrictions. The
objective however is to secure available local access to services for West Cumberland
residents, not to increase WCH site activity per se, so this potential will continue to be
explored as part of clinical strategy. The greater use of community facilities will
ensure sufficient physical capacity remains in WCH outpatients.
Increasingly the Trust expects to see a new model of outpatient delivery, with
specialist provision much more closely integrated with primary and community health
care, working as extended multidisciplinary teams, particularly for patients with long
term conditions. Whilst a different model will change the overall activity in the long
term, this would still be provided locally (whether by the primary health care team or
specialist) and illustrates the significant potential available to partners.
Transport
A new transfer protocol for adults is now in place which has been developed with
NWAS colleagues. A refreshed transfer policy for children is in development. The
need for cross-system work to enable maximal identification of patients prior to
presentation at hospital, and minimise additional hand-offs, poor patient experience
and other inefficiencies is noted.
Discussions continue to progress with North West Ambulance Service (NWAS) in
relation to increased capacity requirements to support potential patient transfers.
Short-term cross-system contingency arrangements already developed with NWAS
colleagues include St John’s Ambulance to provide additional capacity for transfers;

49
however, longer term arrangements would require recruitment of additional staff and
procurement of ambulance vehicles.
The following identifies possible transfer/diversion activity and associated costs:
Unscheduled Care
Current protocols require some transfers/diversions every day. Concentrating high risk
medical services on the CIC site as in UC1 will require additional average
transfers/diversions of around 3 per day; recognising that diversion may be possible
for many. Additional transfers/diversions resulting from overnight closure are in the
order of a further 8.
Consideration also needs to be given to repatriation requirements, including potentially
those patients stepped down from CIC intensive care, as well as onward transfers to
the North East
Obstetrics
With very careful selection of patients antenatally, (i.e. those women who are deemed
low risk and able to safely deliver in an MLU – approx. modelling figure = 336) those
women requiring intrapartum transfer could be in the order of 5-9% (17- 30 patients
per year) – some 1-3 per month. These patients would however require immediate
attention to minimise adverse patient experience and ensure both maternal and
fetal/neonatal safety.
It is estimated that, with appropriate identification of low risk patients, babies needing
post-delivery transfer from a standalone MLU to SCBU would be in the order of 1% -
perhaps only 3-4 patients per year.
Paediatrics
P2 would require a maximum of 26 transfers per week and P1, 12 per week. However,
it is likely that a proportion of these could be diverted at point of GP referral (and
others assessed at WCH may prefer and be suitable to use own transport options).
Consideration will need to be given as to the seasonal nature of transfers, in particular
babies and young children with respiratory difficulties.
Children requiring transfer for in-patient care will need robust pathway management,
with criteria determined by the anaesthetist team, NWAS and Retrieval Team – a new
transfer protocol for children is being developed. In particular arrangements for
increased numbers of very sick children requiring transfer to CIC or Newcastle must
be considered. Consideration needs to be given to the impact of any newly required
transfers to either CIC or the tertiary centre on safety and nurse escort requirements
as well as ambulance transportation.
50
Anticipated transport impact
High-level transport analysis has been undertaken based on work undertaken in South
Cumbria however a number of assumptions have been used which all need to be
validated and is therefore not included yet.
Further detailed discussions with NWAS and modelling will therefore be required to
understand the full impact of potential solutions identified. Discussion is also required
with clinicians in relation to potential for direct diverts to CIC through use of paramedic
assessment and agreed pathways with primary care.
Careful consideration will need to be given with commissioners and transport
providers regarding options and alternatives for:
transfer and diversion of non-elective patients from WCH to CIC
repatriation of patients from CIC to WCH to complete their care
relatives in particular older people and those with young children visiting in-
patients
staff from integrated workforce arrangements and altered service
configurations
any onward transfers required to the specialist centre in Newcastle
The readily available capacity of appropriate transport to support preferred options
presents a key challenge to implementation: it is recommended that the CCG be
requested to commission a discrete inter-hospital transport solution with the
specification developed based on work with the Trust and with NWAS colleagues, and
informed by external scrutiny of proposals by the Chief Executive of South West
Cornwall (where there is a similar rural footprint).
Clinical & System Outcome Measures
The potential way forward for transformational change detailed within this paper would
require close monitoring if implemented to provide assurance to the commissioners,
regulators and the public that they have resulted in the anticipated service
improvement. A number of system measures would be used to track overall
improvement in line with Chief Inspector/CQC, commissioner, NHS TDA and other
requirements. Any chosen service options will need to demonstrate their ability to
meet expected targets and standards and this will form a key part of further options,
discussion and appraisal.
Importantly, it is expected that a reduction in the variation in mortality between the
sites (with necessary casemix adjustment) and potentially further overall relative
mortality reduction will be achieved through agreed changes. This is in line with the
mortality improvements seen to date which are considered due in part to recent
pathway changes for cardiac, trauma and surgical patients:

51
At an individual pathway level the Trust has seen what can be achieved through
consolidation into larger teams, working in more systematic structured ways – there
have been improvements in clinical outcomes for both trauma and cardiology patients.
For example, for patients with fractured neck of femur the average time to operation
from admissions has significantly improved at the same times as a sustained and
continuing reduction in mortality.
Key Performance Indicators (KPIs) to measure outcomes of any potential further
changes described would include:-
1) Mortality rate improvements: with a decreased difference between sites and at weekends
2) Transfer between sites: monitoring of all transfers against agreed standards and criteria; impact on care continuity including LOS
3) WCH Activity: overall increase across all emergency/elective in and outpatient care
4) Medical Workforce: reduction in proportion of locum/agency doctors
Year
Quarter Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Observed 297 288 274 295 303 297 275 321 322 261 249 257
Expected 254.97 249.76 216.62 253.55 259.06 246.25 253.21 277.92 305.21 274.96 264.69 295.23
Key to Step Changes
Oct-12
Dec-12
Dec-12
Mar-13
Mar-13
Jun-13
Jun-13
Start of Primary PCI Service Jul-13
Oct-13
Dec-13Start of Care Bundles
2011 2012 2013
Mortality Review 2011/12
Change to the Production of Discharge Letters
Beginning of Surgical Transfers from WCH to CIC
Opening of PCI Unit
Commencement of NEWS / Deteriorating Patient Group & Harm Group
Implementation of 5/7 ACP both Sites
Beginning of Orthopaedic Transfers from WCH to CIC
Commencement of Patient Safety Panels (Review of Serious Incidents)
0
50
100
150
200
250
300
350
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
2011 2012 2013
Observed & Expected Deaths - 2011 to 2013
Observed Expected
B
A
C
A D F
E G IH
B
C
D
E
F
G
H
I
A
B
C
D
E
F
G
H
I
A
B
C
D
E
F
G
H
I
A
B
C
D
E
F
G
H
I
A
B
C
D
E
F
G
H
I
A
B
C
D
E
F
G
H
I
J
J

52
5) NHS Forum 7 day Services: compliance with national clinical standards 6) Regulatory standards: CQC Compliance
Other specific specialty level measurable expectations will include:
Compliance with Royal College Guidelines and Outcome Measures;
Compliance with NICE standards;
Compliance with HENE requirements for junior support and supervision;
Availability of staff with required competencies/skills e.g. APLS (Advanced
Paediatric Life Support).
Specialties will develop a small number of clinical and other indicators that can be
measured and reported on internally and externally to provide service level assurance.
Indicators will be accepted measures of safety, quality, operational performance and
financial delivery, used in other parts of the NHS and amenable to benchmarking, and
draw on readily available information. This will include care bundles and specialty
performance indicators in use within Northumbria Healthcare NHS Foundation Trust.
These indicators will be routinely monitored as part of Strategy implementation.
Example indicators for Stroke and GI Bleeds may include:
Stroke: Overall SSNAP16 score – aiming for both overall improvement and differential reduction between sites
Door to needle time
Best Practice Tariff attainment
Thrombolysis rate
GI Bleeds: Percentage with upper GI bleeding receiving a risk assessment using validated risk score
Percentage with severe acute upper GI bleeding (unstable) receiving endoscopy within 2 hrs optimal resuscitation
Percentage admitted with acute upper GI bleeding (stable) receiving endoscopy within 24 hrs optimal admission
Clear pathways and systematised protocols for patient management including transfer
will be developed and agreed by the Trust and commissioners. Adherence to
pathways and protocols will be routinely audited.
October 2014
16
Sentinel Stroke National Audit Programme


















