Electrolyte Balance and SIADH
48
POSTGRADUATE OF BIOMEDICAL SCIENCE FACULTY OF MEDICINE UNIVERSITY SUMATERA UTARA IRA ASTUTI HASIBUAN
-
Upload
biomedikbiokimiausu2014 -
Category
Documents
-
view
223 -
download
1
Transcript of Electrolyte Balance and SIADH

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 1/48
POSTGRADUATE OF BIOMEDICAL SCIENCE
FACULTY OF MEDICINE
UNIVERSITY SUMATERA UTARA
IRA ASTUTI HASIBUAN

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 2/48
ELECTROLYTE
A substance whose components dissociate in solution intopositively (cation) and negatively (anion) charged ions. For
example, sodium chloride in solution (saline), dissociates intoNa and Cl. Other electrolytes of physiological importanceinclude Ca, PO42-, etc.
Glucose is not an electrolyte since it does not dissociate insolution. At all times the total number of positive chargesbalances the number of negative charges to achieve electricalneutrality.

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 3/48
Non Electrolyte
dextrose
ureum
kreatinin
Electrolyte
Cation : Na, K,Ca, Mg
Anion : HCO3,Cl, HPO4

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 4/48
ELECTROLYTE
Kation/anion Ekstra selular ( mEq/L ) Intraselular ( mEq/L )Na + 142 15
K + 5 150
Ca ++ 5 2
Mg ++ 1 27
Total 154 194
HCO3- 24 10
Cl - 105105 1
HPO4 = 2 100
SO4 = 1 20
Asam Org 6
Protein 16 63
Total 154 194
142
105
150
100

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 5/48
Water and electrolyte in the body
The total body water is divided functionally into theextracellular (20% of body weight) and the intracellular
fluid spaces (40 of body weight) separated by the cellmembrane with its active sodium pump which ensures
that sodium remains largely in the ECF
The cell contains large anions such protein and glycogen, whichcannot escape and therefore draw in K ions to maintain
electrical neutrality.
These mechanism ensure that Na and its balance anions Cl andHCO, are the mainstay of ECF osmolality, and K has
corresponding function in the ICF

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 6/48
SODIUM
Normal range: 136–145 mEq/L or 136–145 mmol/L
The total body sodium is 3000-4000 mmol, of which only 60%is exchangeable, the remainder being locked mainly in bone
The principal role of sodium is to regulate serum osmolality as well as fluid balance.
Changes in body water and plasma volume can directly or
indirectly affect the serum sodium concentration.

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 7/48
As a result of changes in effective circulating volume,baroreceptors and osmoreceptors will respondaccordingly in an attempt to restore an isovolemic state of
the body.
Baroreceptors are located in the carotid sinus, aorticarch, cardiac atria,hypothalamus, and the
juxtaglomerular apparatus in the kidney.
Stimulation of these receptors will promote urinary loss of water and sodium.
PHYSIOLOGY OF SODIUM

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 8/48
Osmoreceptors are presentprimarily in the hypothalamus.
The Resultant Renal EffectsFrom These Three DistinctPathways Will Alter thehomeostasis Of Water andsodium.
The three major mediatorsinvolved include vasopressin orantidiuretic hormone (ADH),The renin-angiotensin-aldosterone System (RAAS),
And Natriuretic peptides.
PHYSIOLOGY OF SODIUM
H i h i i l d i di i

8/19/2019 Electrolyte Balance and SIADH
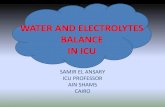
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 9/48
Homeostatic mechanisms involved in sodium, potassium,and water balance.

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 10/48
SIGN AND SYMPTOM OF HYPONATREMIA
AND HYPERNATREMIA
HYPONATREMIA HYPERNATREMIA
Abnormal sensor Agitation
Anorexia Apathy Cheyne-Stokes respirationDepressed deep-tendonreflexesDisorientation
HypothermiaLethargy Muscle crampsNauseaSeizures
ThirstRestlessness
Irritability Lethargy Muscle twitchingSeizuresHyperreflexia
ComaDeath

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 11/48
CAUSES OF HYPONATREMIA

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 12/48
SIADH
The syndrome of inappropriate antidiuretic hormone secretion(SIADH) is the most common cause of hyponatremia in
hospitalized patients
Normally, ADH is secreted from the posterior lobe of thepituitary gland in response to decrease in plasma volume or
increase in serum osmolality.
In SIADH, secretion of ADH is not caused by hemodynamicdisturbance and is mediated through nonosmotic receptors,
resulting in water retention and dilutional hyponatremia.

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 13/48

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 14/48
The key points in diagnosing SIADH are the serumsodium concentration, tonicity of plasma and urine,
urine sodium concentration and clinical volumestatus.
Finding of hyponatremia ( serum sodiumconcentration < 135 mEq/L ), hypotonicity plasma
osmolality ( <280 mOsm/kg) inappropriateconcentrated urine ( > 100 mOsm/kg ), elevated
urine sodium concentration (>20mEq/L) areconstant with SIADH
SIADH is a diagnosis of exclusion, and adrenal,cardiac, liver, kidney, and thyroid dysfunction
must be ruled out.

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 15/48

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 16/48
CAUSES OF HYPERNATREMIA
HYPERNATREMIA
Na > 145 mmol/L
EUVOLEMIA
Diabetic incipidus increasedinsensible water loss
fever,
extensive burns,
mechanical ventilation
HYPOVOLEMIA
profuse sweatingdiarrhea
HYPERVOLEMIA
Primaryhyperaldosteronism
Cushing disease
Sea water, neardrowning
Resuscitative effortsusing hypertonic
sodium bicarbonate

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 17/48
The total body K lies between 3000 and 3500 mmol and iscontained in the intracellular space at a concentrastion of 120-145 mmol/L
Only a very small proportion is in the ECF, where itsconcentration lies crucially in the narrow range 3.5-5.2mmol/L.
The major physiological role of potassium is in theregulation of muscle and nerve excitability. It also playimportant roles in control intracellular volume, protein
synthesis, enzymatic reaction, and carbohydrate metabolism
POTASSIUM

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 18/48
Na-K-ATPase pump is principally responsible for regulatingpotassium entry into cell. Potassium is primarily excreted by
the kidneys
Potassium homeostasis is altered by insulin, aldosterone,changes in acid-base balance, renal function, orgastrointestinal and skin loses
Although potassium may affect different body functions,its effect on cardiac muscle is the most important due to
the potential life threatening effect of arrhytmia as a resultof either high or low serum potassium concentration

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 19/48
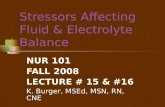
The acute homeostatic sequence of events in the body to
maintain serum potassium within a narrow concentration range.
HYPOKALEMIA

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 20/48
HYPOKALEMIA
Hypokalemia is defined as a serum potassium concentration less
than 3.5 mEq/L (<3.5 mmol/L).ETIOLOGY : clinicians should determine whether hypokalemia isdue to intracellular shifting of potassium (apparent deficit) orincreased loss from the body (true deficit)
AlkalosisΒ2-
adrenergicstimulationinsulin
Decreased intake :Tea and toast diet, alcoholism,
indigence, potassium-free IV fluids,anorexia nervosa, bulimia
Increased output :Extrarenal : vomiting, diarrhea, laxative
abuse, intestinal fistulesRenal : corticosteroids, amphotericin B,diuretics, hyperaldosteronism, cushing’s
syndrome, licorice abuse
Apparentdeficit
Truedeficit

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 21/48
HYPERKALEMIA

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 22/48
HYPERKALEMIA
Hyperkalemia is defined as serum potassium concentrationgreater then 5.0 mEq/L (> 5.0 mmol/L )
Hypokalemia may indicate a true or apparent potassiumimbalance
Renal failure is the most common causes of hyperkalemia

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 23/48
ETIOLOGIES OF HYPERKALEMIA
Apparentexcess
( extracellularshifting )
True excess
Metabolicacidosis
INCREASED INTAKE
Endogenous causes :HemolysisRhabdomyolysisMuscle crush injuries
Burns
Exogenous causes :Salt subtitutesDrugs ( e.g. penicillinpotassium )
DECREASED OUTPUT
Chronic or acute renalfailureDrugs : potassium-sparing diuretics, ACE-
inhibitors, NSAID, Angiotensin II receptorantagonist, heparin,trimethoprimDeficiency of adrenalsteroids Addison’s disease
SIGN AND SYMPTOM OF HYPERKALEMIA

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 24/48
SIGN AND SYMPTOM OF HYPERKALEMIA
Symptom of hyperkalemia usually do not developed untilserum potassium concentration reach 5.5 mEq/L.
Symptoms are caused by changes in neuromuscular andcardiac function and include muscle twitching, cramping,
weakness and paralysis.
The most concerning symptoms are cardiac abnormalities :peaked T waves, widened QRS complexes, prolonged PRinterval, shortened QT interval, this can lead to cardiac
arrhytmias.

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 25/48
Normal range : 96-106 mEq/L or 96-106 mmol/L
Chloride is passively absorbed from the upper small intestine. In thedistal ileum and large intestine., its absorbtion is coupled withbicarbonate ion secretion
Chloride is influenced by the extracellular fluid balance and acid-base
balance.
The physiological role of chloride is primarily passive. It balances outpositive charges in the extracellular f luid and, by passively following
sodium, helps to maintain extracellular osmolality

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 26/48

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 27/48
Causes : A patient is on acid-suppressive therapy (e.g., high-doseH2-blockers or proton pump inhibitors)Patient who is receiving continuous or frequentnasogastric suction Person whose has profuse vomiting, a greater loss ofchloride than sodium can occur because gastric fluid
contains 1.5–3 times more chloride than sodium.Gastric outlet obstruction, protracted vomiting and self-induced vomitingMetabolic alkalosis
HYPOCHLOREMIA

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 28/48
The most causes : saline infusion in hospitalized patientparenteral nutrition solutions with high chlorideconcentrationsDrug : acetazolamideMetabolic and respiratoric acidosis
HYPERCHLOREMIA

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 29/48
CALCIUM
Ninety-nine percent of total body calcium resides inbone. Less than 1 % exist in the extracellular fluid.
Normal serum calcium concentration in the extracellularbetween 8.6 and 10.2 mg/dL. Nearly 50 % of serum calcium
is protein bound, primarily to albumin.
Calcium is essential to many body function, including bonemetabolism, neuromuscular activity, electrical conductionin the heart and smooth muscle, coagulation, and exocrine
and endocrine functions.
CALCIUM

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 30/48
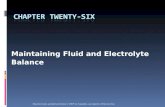
HOMEOSTASIS
Calcium homeostasis is regulated by parathyroid hormone,calcitonin and vitamin D.
For every 1 g/dL decrease in serum albumin concentrationbelow 4 g/dl serum calcium concentration will decrease by
0,8 mg/dl, therefore serum calcium concentration should becorrected in patient with hypoalbuminemia
Corrected calcium = ( 0,8 ( 4 – albumin )) + serum calcium

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 31/48
source : https://quizlet.com/31186621/endocrine-06-bone-mineral-homeostasis-flash-cards/

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 32/48
HYPOCALCEMIA
Diminished intakeMedications : calcitonin
Ethylenediaminetetraacetic acid ( EDTA )GlucocorticoidLoop diuretics
Phosphate saltsPicamycin
HyperphosphatemiaHypoalbuminemiaHypomagnesemia
HypopharatiroidismPancreatitisRenal failureSecondary hyperpharathyroidism Vitamin D deficiency
CAUSES

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 33/48
HYPERCALCEMIA
CAUSESThe most causes is malignancy and primarilyhyperparathyroidism
Hypercalcemia can also result from:Excessive administrationOf IVcalcium saltsCalcium supplements
Chronic immobilizationPaget’sdiseaseSarcoidosisHyperthyroidism Acute adrenal insufficiency Somer espiratory diseases
Lithium-inducedrenalcalciumreabsorptionExcessivevitaminD,vitaminA,orthyroidhormone,which increasesintestinal absorptionTamoxifen AndrogenichormonesEstrogenProgesterone
SIGNS AND SYMPTOMS

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 34/48
HYPOCALCEMIA
Tetany → characteristic symptom
Neuromuscular disfunctionCardiovascular disfunctionCentral nervous system dysfunctionChronic hypocalcemia : hair loss,dermatitis, eczema, grooved nails
HYPERCALCEMIA
FatigueConfusionBradycardia
Arrhytmiachronic hypercalcemia :nephrolithiasis, metastatic calcification,renal failure

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 35/48
MAGNESIUM
Magnesium is found primarily in the bone,muscle and soft tissue. Approximately 1 % of total
body stores present in extracellular fluid
The normal serum magnesium concentration is1.5 to 2.4 mg/dl.
Magnesium is utilized throughout the body as acofactor for enzyme and is required in reaction
involving adenosine triphosphatase ( ATP )

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 36/48
REGULATION
Largely regulated by the kidney Other factors including :gastrointestinal function,parathyroid hormone activity,
patient condition
HYPOMAGNESEMIA

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 37/48
HYPOMAGNESEMIA
Defined as serum magnesium concentration less than 1.5mg/dl and is severe when the serum concentration is
below 1 mg/dl
CAUSES ExcessivegastrointestinallosesRenal losses
Surgery Trauma
BurnsSepsisPancreatitisMalnutrition
alcoholism
symptoms Arrhytmias, torsades de pointes, seizures,
coma and death
HYPERMAGNESEMIA

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 38/48
Defined as serum magnesium concentration greater than 2.4mg/dl. Most patients remain asymptomatic until serum
magnesium concentration exceed 4 mg/dl.
CAUSESRenal insufficiency
iatrogenic

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 39/48
SIGNS AND SYMPTOMS OF HYPERMAGNESEMIA
• Bradycardia, flushing, sweating,sensation of warmth, nausea, vomitting,decreased serum calcium and decreasedclotting mechanism
2-5 mEq/L
• Drowsiness and decreased deep tendonreflexes6 mEq/L
• Flaccid paralysis and increased PR andQRS intervals10-15mEq/L
> 15
mEq/LRespiratory distress and asystole
PHOSPHATE

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 40/48
PHOSPHATE
Normal range serum phosphate concentration : 2.6–4.5mg/dL or 0.84–1.45 mmol/L for adults
It is important for intracellular metabolism of proteins,
lipids, and carbohydrates and it is a major component inphospholipid membranes, RNAs, nicotinamide diphosphate(an enzyme cofactor), cyclic adenine and guanine nucleotides(second messengers), and phosphoproteins.
Phosphate absorption is diminished when a large amount ofcalcium or aluminum is present in the intestine due to the
formation of insoluble phosphate compounds.
PHOSPHATE REGULATION

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 41/48
Serum phosphate and calcium concentrations as well as PTH
and vitamin D levels are intimately related with each other.
Serum phosphate indirectly controls PTH secretion via anegative feedback mechanism. With a decrease in the serumphosphate concentration, the conversion of vitamin D to 1,25-DHCC increases (which increases serum concentrations of bothphosphate and calcium). Both the intestinal absorption andrenal reabsorption of phosphate is increased.
The concomitant increase in serum calcium then directlydecreases PTH secretion. This decrease in serum PTHconcentration permits a further increase in renal phosphate
reabsorption.
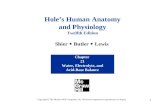
HOMEOSTASIS REGULATION OF CALCIUM ANDPHOSPHATE BY PTH VITAMIN D DAN FGF23

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 42/48
From the following article:The skeleton as an endocrine organ
Douglas J. DiGirolamo, Thomas L. Clemens & Stavroula Kousteni .Nature Reviews
Rheumatology 8, 674-683 (November 2012) doi:10.1038/nrrheum.2012.157
PHOSPHATE BY PTH, VITAMIN D DAN FGF23
HYPOPHOSPHATEMIA

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 43/48
Hypophosphatemia indicates a serum phosphate
concentrationless than 2.6 mg/dL (<0.84 mmol/L).
Common causes of decreased serum phosphate
concentrations:1. Increased renal excretion2. Intracellular shifting3. Decreased phosphate or vitamin D intake
Infusion of concentrated glucose solutions, especially whenaccompanied by insulin, can produce hypophosphatemiathrough intracellular phosphate shifting → refeeding
syndrome
SIGNS AND SYMPTOMS OF

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 44/48
Patients with moderate reduction in serum phosphate(2–2.5 mg/dL or 0.64–0.81 mmol/L) are often asymptomatic.Neurological irritability may occur as the serum phosphateconcentrationDrops below 2 mg/dL(<0.64 mmol/L )
Severe hypophosphatemia is often associated with muscle
weakness, rhabdomyolysis, paresthesia, hemolysis, plateletdysfunction, and cardiac and respiratory failure. CNS effectsoften include encephalopathy, confusion, obtundation,seizures, and ultimately, coma
HYPOPHOSPHATEMIA
HYPERPHOSPHATEMIA

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 45/48
Hyperphosphatemia indicates a serum phosphateconcentrationgreaterThan 4.5 mg/Dl (>1.45 mmol/L).There are three basic causes for elevated serumphosphate concentrations:
1.Decreased renal phosphate excretion2. Shift of phosphate from intracellular to extracellularfluid3. Increased intake of vitamin D or phosphate-containing
products (orally, rectally, or intravenously )
THE MOST CAUSERENAL
DYSFUNCTION
SIGNS AND SYMPTOMS

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 46/48
Signs and symptoms of hyperphosphatemia commonlyresult from the accompanying hypocalcemia andhyperparathyroidism
Renal function may diminish if hyperphosphatemia isleft untreated.
In the presence of renal dysfunction, phosphateexcretion is further reduced to cause an even greater
increase of serum phosphate concentration and a furtherdecline in serum calcium concentration
REFFERENCES

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 47/48
REFFERENCES
Lau A., Chan L., Electrolyte, Other minerals, andTrace Elements
Lobo D., Lewington A., Allison S., Basic Concepts of
Fluid and Electrolyte Therapy
Bartel B., Gau E., Fluid and Electrolyte Management
Balasubramanian A., Flareau B., Sourbeer J.,2007.,Syndrome of Inappropriate Antidiuretic Hormone
Secretion

8/19/2019 Electrolyte Balance and SIADH
http://slidepdf.com/reader/full/electrolyte-balance-and-siadh 48/48