EIU - Succeeding in a value-based environment: New business models to thrive in the future of...
30
A white paper from The Economist Intelligence Unit Healthcare Succeeding in a value-based environment New business models to thrive in the future of healthcare January 2014
description
EIU - Succeeding in a value-based environment: New business models to thrive in the future of healthcare - January 2014 Executive summary • Value-based health, or the maximising of health outcomes over cost, may hold the answer to streamlining of healthcare provision that will make the dual aims of good health and universal access possible. • Value is the emerging new currency within health markets. • The systems and structures needed to deliver value-based healthcare represent a radical departure from traditional approaches on purchasing and delivering care, typically starting with the way care is paid for or bought. • Value-based healthcare is enabled by a data-driven, evidence-based approach, which can significantly reduces inefficiencies in traditional health systems, by reallocating resources and streamlining operations according to their impact on outcomes. • Global rates of adoption for value-based practices differ significantly. Countries that have a large element of outcomes-based purchasing and reimbursement today include the UK, Germany and the US. • Nevertheless, emerging economies can get a head start in streamlining costs against outcome, by “baking in” the concepts of value-based healthcare as a central organising feature from day one. • This new dynamic of value-based health presents both opportunities and challenges for various segments in healthcare. • For hospital providers, we expect pressure on margins driven by lower prices and reduced volumes of activity and inpatient stays, in favour of activity in lower acuity settings, such as primary and preventative care. • Payors are faced with the need to restructure policies and commissioning schemes to reflect outcomes. Opportunities exist here to streamline costs associated with claims and coverage through proper health technology assessments and evidence-based protocols. • Suppliers must adapt operations from R&D through to commercialisation, to demonstrate value against directly and indirectly competing products and services. Winners will be characterised by the ability to strike innovative pricing deals, to collaborate with payors and to make the transition from selling products to delivering healthcare solutions. However, each market presents unique commerical, regulatory and competitive challenges. Robust clinical and commerical due diligence is essential. • Investors looking for returns will continue to find them in healthcare IT, data analytics, nontraditional modalities of care, preventative care and the emerging markets.
Transcript of EIU - Succeeding in a value-based environment: New business models to thrive in the future of...

A white paper from The
Economist Intelligence
Unit Healthcare
Succeeding in a value-based environmentNew business models to thrive in the future of healthcare
January 2014

© The Economist Intelligence Unit Limited 2013 1
Executive summary 2
Value-based health: the new normal in healthcare 4 Drivers and challenges 4
Definingvalueinhealth 5
Value-based health systems vis-à-vis traditional health markets 6
An evidence-driven approach 7
Global rates of adoption 8
A changing landscape for business 11 Providers: Pressure on margins force changes to business models 11
Payors:Expandedresponsibilitiestoensureaccountablecare 15
Suppliers: An opportunity to secure competitive advantage 17
Investors: Activity forecast and value-based due diligence 20
Conclusion 24
About EIU Healthcare 25 Our approach 26
Acknowledgements 27 Contact details 27
References 28
Contents
SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
2 © The Economist Intelligence Unit Limited 2013
Executive summary
SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
• Value-based health, or the maximising of health outcomes over cost, may hold the answer to streamlining of healthcare provision that will make the dual aims of good health and universal access possible.
• Value is the emerging new currency within health markets.
• The systems and structures needed to deliver value-based healthcare represent a radical departure from traditional approaches on purchasing and delivering care, typically starting with the way care is paid for or bought.
• Value-based healthcare is enabled by a data-driven, evidence-based approach,whichcansignificantlyreducesinefficienciesintraditionalhealth systems, by reallocating resources and streamlining operations according to their impact on outcomes.
•Globalratesofadoptionforvalue-basedpracticesdiffersignificantly.Countries that have a large element of outcomes-based purchasing and reimbursement today include the UK, Germany and the US.
• Nevertheless, emerging economies can get a head start in streamlining costs against outcome, by “baking in” the concepts of value-based healthcare as a central organising feature from day one.
• This new dynamic of value-based health presents both opportunities and challenges for various segments in healthcare.

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
© The Economist Intelligence Unit Limited 2013 3
• For hospital providers, we expect pressure on margins driven by lower prices and reduced volumes of activity and inpatient stays, in favour of activity in lower acuity settings, such as primary and preventative care.
• Payors are faced with the need to restructure policies and commissioningschemestoreflectoutcomes.Opportunitiesexisthereto streamline costs associated with claims and coverage through proper health technology assessments and evidence-based protocols.
• Suppliers must adapt operations from R&D through to commercialisation, to demonstrate value against directly and indirectly competing products and services. Winners will be characterised by the ability to strike innovative pricing deals, to collaborate with payors and to make the transition from selling products to delivering healthcare solutions. However, each market presents unique commerical, regulatory and competitive challenges. Robust clinical and commerical due diligence is essential.
•InvestorslookingforreturnswillcontinuetofindtheminhealthcareIT, data analytics, nontraditional modalities of care, preventative care and the emerging markets.

4 © The Economist Intelligence Unit Limited 2013
SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
Value-based health: The new normal in healthcare
Drivers and challengesThe need for greater value in healthcare has been a topic of much debate in recent years, driven by the widespread recognition that historical trends in costs of healthcare are unsustainable in developed economies and are what emerging economies can ill afford to replicate.
Primarilydrivenbymarketinefficiencies,thisphenomenoniscomplicatedby the multitude of stakeholders in traditional health systems, each with varyingobjectives,workflowsandagendas.Compoundingthat,amisalignmentof incentives and payment systems that focused on volume rather than value has contributed to the spiralling of healthcare costs. In the US, the Centres for Medicare and Medicaid Services (CMS) project that aggregate healthcare spendingwillgrowatanannualrateof5.8%from2012-22,outpacingGDPgrowth by as much as 1 percentage point annuallyi. With spending also rising in other developed and developing countries alike, The Economist Intelligence Unit expectsglobalhealthcarespendingtorisebyaround5%ayearonaverageoverthenextfiveyears,tonearlyUS$9trn.
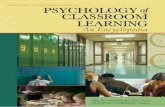
As healthcare costs spiral, constraints on budgets from lower global economic growth, and demand-side pressures from factors such as an ageing population, growingaffluence,ariseinchronicdiseasesandabetter-informedpatientpopulation has led to healthcare systems being stretched to their limit. It is estimated that without major healthcare redesign or intervention, healthcare costsindevelopedcountriessuchastheUScouldconstituteuptoone-fifthofGDPby2022,upfromits2011levelsof17.9%todayii. Although this is the highest percentage in the world, other countries will see comparable growth.
In addition, the politically and ideologically motivated aspirations of governments, involving the provision of universal healthcare for their

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
© The Economist Intelligence Unit Limited 2013 5
populations, have led to an overwhelming recognition that something has to give. Unless we start thinking differently about the provision and focus of care, and what it means to be in the business of healthcare, the current trajectory is dangerously unsustainable.
DefiningvalueinhealthThe concept and pursuit of "value-based healthcare"iii,atermfirstcoinedbyMichaelPorterandElizabethTeisberganddefinedsimplyasthemaximisingof outcomes over cost, may hold the answer to the streamlining of healthcare provision that will make the dual aims of good health and universal access possible.
This route, however, is rejected by some, as it may appear to make subjective trade offs or champion “cut-price” healthcare. Questions that revolve around how much to pay for new medical advances, the value of a life-year and for whom, are often contentious. It is critical to bear in mind the eight tenets presented by Porter and Teisberg, which centre on patient quality (see Figure 2).
“The concept of quality has itself become a source of confusion,” Mr Porter remarks, quality tends to be driven by health guidelines and only measured for care processes. For there to be any real improvement in care, however, trueoutcomes,notprocesses,needtobemeasured(tenetfive).Thiswillgiveproviders accurate feedback on how to ensure better value care.
Figure 1: Healthcare spending as % of GDP
Source: The Economist Intelligence Unit Healthcare.
0
2
4
6
8
10
12
14
16
18
20
IndonesiaThailandChinaSouth KoreaUKGermanySwedenUSA

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
6 © The Economist Intelligence Unit Limited 2013
Outcomes should include those that are the most meaningful to a population of patients. Top-tier outcomes include survival and the degree of health or recovery. Lower-tier outcomes are dependent on success at the top tier. Examples of tier-two outcomes are "time to recovery" and "health complications". Tier-three outcomes look at the sustainability of health and wellbeing, and include long-term consequences of treatment. Tier-three outcomes may include "disease recurrence" or "disease-free survival"v. Often an improvement on one outcome willbringknock-onbenefitstoothers,suchastimelytreatmentimprovingsurvival.
Systematic and robust outcome measurement is still uncommon, but awareness ofitsfeasibilityandbenefitsisgrowingvi. Measurement is essential for innovation and providing the highest value care. In order to be competitive and sustainable in the long term, organisations must improve value or risk losing out to those that dovii.
Value-based health systems vis-à-vis traditional health marketsPractically speaking, the systems and structures needed to deliver value-based healthcare represent a radical departure from traditional approaches to purchasing and delivering care. Some of the main differences are highlighted in the table below.
Figure 2: Porter and teisberg’s eight tenets
1.Redefinethebusinessaroundmedicalconditions
2. Choose the range and types of services provided
3. Organise around medically integrated practice units
4. Create a distinctive strategy in each practice unit
5.Measureresults,experience,methods,patientattributesbypracticeunit
6. Move to single bills and new approaches to pricing
7. Market services based on excellence, uniqueness and results
8. Grow locally and geographically in areas of strength

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
© The Economist Intelligence Unit Limited 2013 7
An evidence-driven approachMuchofwhatisdoneinhealthcaretodayisnotdeliveringahealthbenefit.Of3,000interventionsinuseandevaluatedinasystematicway,only11%wereofprovenbenefitandaround50%werecategorisedasunknowneffectivenessviii. In some situations healthcare can do more harm than good, such as screening for a disease when the absolute risk of having the disease is low (causing unnecessaryworry),whenthereisnobenefitfromearlydetection,orwhentheoutlook (prognosis) is good.
For instance, prostate cancer screening is not offered in the English National Health Service because it leads to over-treatment which itself carries risks. To save one life, 48 additional cases need to be treated, and for every three men who have a high screening blood test and a biopsy, two will not have cancerix.
Figure 3
traditional health systems value-based health systemReimbursement By volume of healthcare
activity or product
By patient outcome compared
with alternatives
Regulatory approval
requirements and process
Demonstrate high quality
manufacturing standards,
clinical safety and clinical
effectiveness, but only against
a placebo
Formal systems in US and
EU now require clinical
effectiveness to be proven
against comparative therapies
for best outcome over cost
Pricing of supplies By volume purchased Relative pricing correlated
withhealthbenefitdelivered
per unit of input
Data and records Lack of measurement of
health outcomes, leading to
an inability to purchase or
performance manage against
this metric
Transparency of input (activity
and product volumes) and
outcomes
Health system planning Lack of planning against
present and future need
Integrated and collaborative
care, budgeted and planned
for in accordance with
population health needs,
access and universal coverage
of essential services
Moving towards a data-driven, evidence-based approach can significantly reduce inefficiencies in traditional health systems

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
8 © The Economist Intelligence Unit Limited 2013
Inthiscase,itisnotclearthatascreeningprogrammebringsmorebenefitthan harm. Chronic and debilitating rare diseases are at the opposite end of the spectrum from mass screened conditions, where the effective management of these diseases may require extremely high cost, so called “ultra-orphan” drugs. Appropriate international benchmarks and best practices research, protocols and guidelines can help to optimise the clinical value proposition of these drugsx.
Improvingvalueinhealthcarethereforerequirestheidentificationofwhatworks, what does not and what treatments are harmful. Moving towards a more data-driven, evidence-based approach towards healthcare management can significantlyreducetheinefficienciespresentintraditionalhealthsystems.Itis this recognition that has led to the establishment of organisations such as the National Institute for Health and Care Excellence (NICE) in the UK, and the InstituteforQualityandEfficiencyinHealthcare(IQWiG)inGermany.
In order to optimise care pathways, these organisations increasingly rely on independently-gathered evidence summaries from existing trial data, research involving patient surveys, or communication with clinical experts to benchmark cost and set the appropriate standards and best practices for the provision of care.
NICEusesquality-adjustedlifeyears(QALYs)toestimatethebenefitthatcan be conferred by a new drug or treatment. NICE assigns a value of £20,000 (US$31,800)to£30,000peryearofperfecthealth,soifatreatmentisableto extend or improve quality of life without exceeding this cost, it can be considered cost effectivexi.
Global rates of adoptionImplementation and adoption rates of value-based practices vary widely across geographies. The level of development in healthcare systems differs substantially across regions, impacting a location’s readiness to roll out a value-based health environment.
We see the adoption of value-based health as closely tied to health coverage in a country. As health insurance coverage for the masses increases, so does the healthcare bill to payors, which drives the need for greater value-based practicestoensurefiscalsustainability.
Figure 4: Healthcare coverage evolution and value-based practices
Out of pocket paymentsGovernment insurancefunded health systemthrough contribution
Value-basedpurchasing andcommissioning
Shift from fee forservice healthcareprovision towardoutcome basedreimbursement

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
© The Economist Intelligence Unit Limited 2013 9
Leading the way as early adopters of value-based health are high-income developedcountries.Countriesthathaveasignificantelementofoutcomes-basedpurchasing and reimbursement today include the UK, Germany and the US.
In the US for example, the Patient Protection and Affordable Care Act (PPACA), commonly known as Obamacare, brought into effect elements of outcomes-based reimbursement, which exist alongside other funding mechanisms. In Germany, under the Act for the Restructuring of the Pharmaceutical Market in Statutory Health Insurance (AMNOG), passed in January 2011, companies can only set their ownpricesforanewproductforthefirstyearafteritislaunched.Duringthistimetheyhavetocollectevidenceonthecost/benefitsuperiorityoftheirnewmedicine over previous treatments. This information is then used to negotiate future prices with the public health system.
Emerging business models: The German ExperienceLike many developed countries, Germany has seen healthcare spending rise as a result of population ageing and the increasing complexity of treatments. In 2010 it therefore abandoned its policy of free pricing for pharmaceuticals and introducedacost-benefitsystemoverseenbytheInstituteforQualityandEfficiencyinHealthCare(IQWiG).
Under the Act for the Restructuring of the Pharmaceutical Market in Statutory Health Insurance (AMNOG), passed in January2011,companiescanonlysettheirownpricesforanewproductforthefirstyearafteritislaunched.Duringthistimetheyhavetocollectevidenceonthecost/benefitsuperiorityoftheirnewmedicineoverprevioustreatments.This information is then used to negotiate future prices with the public health system.
Ifnegotiatorscannotagreeaprice,thenthedrugischannelledthroughafixed-priceschemethatcomparesitspriceto that of similar patented and generic drugs, as well as to a basket of prices across several European countries. Orphan drugs are exempt from this process.
Thepolicyformedpartofawiderausteritypackagethataimedtosavearound€4bn(US$5bn)in2011alone.Togetherwith the additional pricing measures contained in AMNOG, the health system is now expected to save €2.2bn a year in pharmaceutical spending. Given the prevalence of international reference pricing systems, savings are also being made outside of Germany.
The system has been strongly criticised by the European Federation of Pharmaceuticals Industries and Associations, however. It says the price controls are too harsh, and the process of proving “cost-effectiveness” too onerous. It also argues that, because Germany’s lowered prices feed through into international reference pricing systems elsewhere, companies are now reluctant to launch new products in Germany. For example, Boehringer Ingelheim held back its new type II diabetes treatment Trajenta (linagliptin) in Germany.
Emerging markets are faced with a unique opportunity to “bake in” the concept of value-based health as a central organising feature from day one

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
10 © The Economist Intelligence Unit Limited 2013
Emerging business models: Towards technology assessmentIn their efforts to get value for money from the expansion of their healthcare systems, several middle-income countries—including Argentina, Brazil, China, Israel, Mexico, South Korea, Philippines, Taiwan and Thailand—have set up health technology agencies. Often based on agencies in developed countries, their role is to assess the evidence on different treatments and issue recommendations on pricing and reimbursement.
In Thailand, for example, the Health Intervention and Technology Assessment Program (HITAP) was set up in 2007, when the country abolished co-payments for its Universal Coverage Health Scheme. Since then, the HITAP has played a key role in evaluating treatments and interventions, such as HIV counselling or cervical cancer screening for cost-effectiveness. These are judged partly on gross national income per QALY gained.
In2009theHITAPusedthismeasuretohelpdrawupanationalbenefitbasket,overseenbyasubcommitteethatjudges spending priorities based on six criteria:
1. Size of the population affected
2. Severity of the disease in terms of quality of life
3. Effectiveness of the treatment
4. Variations in clinical practice
5.Impactonhouseholdlivelihood
6. Equity and ethics
Some measures were controversial, however. For example, Thailand tried to combat overuse of drugs by drawing up a negative list of non-essential treatments and gathering hospital data on how they were being used. The project worked and drug expenditure dropped. But when that was followed by a move to ban reimbursement of four particularly overused drugs, the authorities had to back down in the face of public opposition. HITAP still faces challenges when it comes to reconciling the needs of patient groups with the country’s economic constraints.
Nevertheless, as emerging economies such as Indonesia, Thailand and Philippines look to roll out various forms of universal healthcare, they are faced with a unique opportunity. In building their health systems from the ground up, they can get a head start in streamlining costs against outcome, by "baking in" the concept of value-based healthcare as a central organising feature from day one.

© The Economist Intelligence Unit Limited 2013 11
SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
A changing landscape for business
Value-based health changes the land-scape fundamentally from a business perspective. For traditional health systems that have been characterised and remunerated by volume and activity with little-to-no regard for measurement of performance againsthealthoutcomes,value-basedhealthrepresentsasignificantdeparturefrom routine. Provider utilisation metrics such as inpatient days and bed occupancyrates,typicallyconsideredindicatorsofaprovider’slikelyfinancialsuccessandprofitability,arenowinconflictwiththegoalof“value.”
Indeed, declining inpatient use rates in the US have been viewed by some as representative of aggregate best practices for overall levels of medical service utilisation. In a value-based environment, inpatient care is almost viewed as a last resort, favouring instead a care mix that involves lower-intensity primary care settings: care centres and clinics, health management and preventative care.
PROVIDERS: Pressure on margins force changes to business modelsUnlesspaymentmethodsandbusinessmodelschangesignificantly,providerrevenue will come under pressure as volumes decline through value-based initiatives. Revenue will also face greater downward price pressure from payors, whileprofitsbecomeexposedtocostsassociatedwithregulationsaimedatencouraging equity of access to services. In some markets, traditional healthcare

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
12 © The Economist Intelligence Unit Limited 2013
activity, such as clinic visits for disease management, is actively disincentivised infavourofdiseaseprevention,drivinggreaterefficacyandcost-effectivenessinternationallyxii.
Integrated practice designed with entire care pathway in mindA mitigation solution would be to restructure operations to bring down costs through careful benchmarking of care pathways and provision, ensuring that clinical evidence and outcomes research are employed to set adequate standardisation protocols and inform the reorganisation of care delivery. Through the elimination of unwarranted clinical practice variation, costs can be reduced.
To take it a step further, providers should also consider the entire pathway of care, recalibrate the business around certain conditions and organise the practice around integrated unitsxiii. Effective procurement, provision and assessment of healthcare cannot happen without detailed knowledge and consideration of the entire pathway of care—the chain of clinical steps and events linked together along a timeline that structures patient management from initial presentation in primary care, through to secondary and tertiary care. To deliver an integrated andefficienthealthcareservice,itisvitaltomapoutanidealpathwayofcare,preferably led by patient outcomes data.
Harvest patient data through electronic medical recordsElectronic medical record systems provide at least basic demographic data and patient history, which can be aggregated and analysed to see what works and what does not. The effectiveness of this would, of course, depend on the electronic medical record system being versatile and easy to integrate into clinical practice. Integration into practice units, also called service designation or integrated care, can be supported by evidence to create a picture of the ideal service model.
Opportunities in lower acuity, primary and preventative careOpportunities exist for providers to leverage the shift towards lower acuity settings (i.e. GP commissioning) to expand into non-traditional areas of business including primary and community care, and preventative services.

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
© The Economist Intelligence Unit Limited 2013 13
Case in point: Evidence-based design of care pathways
An information provider to the National Health Service in the UK needed to create care pathways based on the best available evidence. It needed a clinically robust way to standardise its processes. Most importantly, it needed to communicate complex health information in a simple and transparent way delineating the source, quality and currency of the evidence.
The Economist Intelligence Unit Healthcare developed an innovative methodology to create each care pathway. Clinicians undertook a review of the scope to decide the breadth and depth of each pathway. Each pathway was based on a particular disease or health condition such as ‘suspected breast cancer.’ Trained information specialists conducted systematic searches of international biomedicaldatabasesandfilteredhundreds of research papers according to relevance and quality. Trained evidence reviewers graded the research according to explicit criteria.
A multidisciplinary team drafted and edited each care pathway. This included creatingan‘evidencecertificate’whichappraised and tagged each step of the pathway with an evidence level. This wasfollowedbyafinaleditbyclinicians.Generalists and specialist clinicians conducted peer reviews of each topic.
More than 400 pathways were delivered over a two-year period. We also developed four comprehensive pathways and built systems to help the provider develop further protocols for themselves.
These care pathways have met exacting international quality standards. The protocols have been used to help standardiseandbenchmarkcareprocessesandcarequality,leadingtoimprovedclinicalefficiencyandcostsavings.
Source: bazian, the Economist Intelligence Unit Healthcare

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
14 © The Economist Intelligence Unit Limited 2013
Case in point: Designing the ideal service modelxv
A regional healthcare payor needed support to decide the optimal and rational way to select providers for cleft lip and palateservicesinadefinedlocalpopulation.
Empirical treatment evidence from systematic reviews or randomised controlled trials for certain conditions like cleft lip and palate can be limited. A robust search of unpublished (‘grey’) literature and consultation with specialists and third party sources was a useful way of building the evidence base.
A collaborative team from The Economist Intelligence Unit Healthcare undertook a multipart analysis to generate a picture of the ideal service model. A background search and an appraisal of all evidence types, both published and unpublished, was conducted by a trained information specialist. The project scope was multifaceted to include numerous questions about the disease epidemiology, regional demographic data, current service data, effectiveness and cost-effectiveness of different service models, current standards of care and evidence for outcomes measured. A health needs assessment, epidemiological review and modelling exercise was undertaken to estimate the current and future demand for these services in the region.
ThefinalServiceDesignationGuidefacilitatedthecollaborativediscussionbetweencommissionersandproviderswith the shared aim of delivering a clinically optimal, practical and continuously improving service appropriate for the population served, across the entire pathway of care.
Outputsincludedevidence-basedqualityindicators,servicespecification&standardsrecommendationsforinformationreporting.
Findings included:-Identificationofgapsincurrentserviceprovision(patientpathway,servicemodel);-Needforstakeholderconsensusandbuyinonqualityindicatorsandstandards;-Needtotestdraftstandardsforreliability,validity,sensitivitytochange;-Assessmentofcurrentprovidersagainstagreedstandards;-Needforbetterdatacollectionspecifictocleftlipandpalatesurgeons,sothatactivityandcostscanbebettertracked.
Source: bazian, the Economist Intelligence Unit Healthcare

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
© The Economist Intelligence Unit Limited 2013 15
PAYORS: Expanded responsibilities to ensure accountable careWithconstrainedbudgets,insurersandpayorswillneedtodefinelevelsofcoverageinwaysthatarefinanciallysustainableandyieldaffordablepremiums.The payor function and responsibilities increase from that of contracting and reimbursement—to being gatekeepers of accountable care. There is also an increasing need to intervene directly in the insurer-payor-provider transaction in detailed and clinically-articulate ways that can demonstrate value to the regulator, the government sponsor and the patient.
A private health insurer recognised excessive rising claims around knee arthroscopy procedures. It also noted significantvariationinclaimsacrossdifferentapprovedproviders.Thechallengewastomanagethevolumeofthoseclaims in a way that was clinically robust.
The Economist Intelligence Unit Healthcare conducted a systematic review examining the evidence on effectiveness oftheprocedureindifferentpatientgroups.Arobust,analysisoftheevidence,stratifiedbypatientgroupandspecificclinical criteria followed.
Based on this analysis, the insurer designed pre-authorisation processes and tools that were implemented with clinicians and their governing bodies. The analyses also fed into the development of communications with the insurer’s members (patients), to assist with shared decision making and informed choices about their options for the relevant orthopaedic conditions (which include physiotherapy or MRI, rather than arthroscopy).
The analyses and resulting tools have helped the insurer and payor to standardise care and optimise value. It has done so by eliminating inappropriate claims, by educating patients about less invasive and more clinically appropriate options. The client has also reduced unwarranted variation among providers, and there has been a broader effect: the providers now know that the payor is managing performance from a clinical perspective, with resultingindirectbenefitsonthevariabilityandclinicalappropriatenessofclaims.
Source: bazian, the Economist Intelligence Unit Healthcare
Case in point: managing insurance claims variation through evidence-based protocolsxvi

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
16 © The Economist Intelligence Unit Limited 2013
Case in point: Engaging patients in their own health and care
Media hype about health stories often leads to an increased burden on health resources. Over-sensationalisation or misrepresentation can increase demand on primary care as worried patients seek advice, and on occasion can lead to “social panic” that has dramatic detrimental effects on health and on health resources.
The Economist Intelligence Unit Healthcare works closely with the National Health Service (NHS) in England to create a public health site called “Behind the Headlines”. Together with the NHS, we identify two stories from the media each morning and utilise the quick turnaround time of our analysts to publish an unbiased critique and review of clinical evidence and research on the NHS Choices website by mid-afternoon.
By picking apart the story and providing the evidence and limitations to the science and reporting, a much more objective view of the research results is achieved. To date we have critiqued around 4,000 stories. The service is used by journalists and the public directly, and has led to more moderate and balanced reporting in the lay media. It is also used by doctors and nurses, to help explain and counter the fears of their patients. The site as a whole is used to engage with patients, empower them to self-manage aspects of their care and exercise informed choices when making health decisions.
Source: bazian, the Economist Intelligence Unit Healthcare
Through the design of policies and insurance contracts, payors keep providers and doctors accountable by setting coverage, procurement, and reimbursements based on value and outcomeratherthanactivity.Thereisalsoscopetoinfluencevaluethroughtheprocurementandreimbursement of pathways of care rather than individual activities. To be effective, payors and insurers need to develop and maintain value-based performance metrics and manage provision based on clinical performance against these metrics.
We see this trend gaining pace with the likes of United Healthcare, a leading insurer and provider,announcinginJuly2013thatitwill,inthenextfiveyears,increasethevalueofcontractswithproviderscontainingacomponentofqualityandcostefficiencytoUS$50bn(nearlydoublethepreviousfigure)xvii.

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
© The Economist Intelligence Unit Limited 2013 17
New business models in development include the formation of payor-provider partnerships, also known as accountable care organisations (ACO). The number of ACOs in the US has risen dramatically from fewer than 30 in April 2012 to over 100 in January 2013. However, while such collaborations can improve the quality of care and reduce healthcare spending, they may also lead to antitrust activity, reducing competition and driving up prices, leading to just the opposite result.
The good news is, with investment into evidence research and data likely to occur from a shift towards value-based health, payors will increasingly have access to the tools and intelligence that will enable them to make better choices on their expenditure.
SUPPLIERS: An opportunity to secure competitive advantageFor industry suppliers the concept of value-based health manifests itself in both opportunities and threats. Increasing regulation, demands for demonstration of value, and price pressures from generics and payors will mean that the traditional business models will apply in a diminishing number of areas.
"Blockbusters" (or drug breakthroughs that demonstrably deliver to the mass market an unequivocal step change in outcomes), may become a thing of the past as we move towards a value-based environment. Here, it is comparative effectiveness against alternatives that counts.
Already, initiatives such as the AllTrials campaign, which supports the open availability of clinical trial results and study reports—whether positive or negative—have gained popular backing. Many health information groups, including The Cochrane Collaboration, as well as charities have shown support, with the recent addition of GlaxoSmithKline (GSK), a multinational pharmaceutical company. Registers such as ClinicalTrials.gov and International Standard Randomised Controlled Trial Number (ISRCTN) encourage registration of research protocols and allow open access to trials and their results before they are published as journal articles. This increasing transparency will raise the bar for future research, but it will not aid in its translation into clinical practice or industry. There is still a key role for the analysis and interpretation of research evidence.
R&D to improve outcomesWith the refocus of customers on value, marketing strategies should also adapt accordingly. Whether it is the pricing structure, product portfolio or promotions mechanism,theyallhavetobeconfiguredtodemonstratevalue.

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
18 © The Economist Intelligence Unit Limited 2013
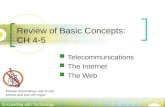
Case in point: Health technology assessments (Hta) for a new drugxviii
In the UK paying for healthcare is not simple. Commissioners are responsible for purchasing the right mix of drugs and services to meet the needs of their population. There is a need to assess the clinical and cost impact of drugs vis-à-vis the needs of the local population, in order to allocate resources for the services commissioned effectively. HTAs & impact assessments demonstrate value to payors.
The Economist Intelligence Unit Healthcare rapidly delivers HTAs in as little as 2-3 weeks and impact assessment, fromscopetofinalreport.Thesereportssummarisecostdata,epidemiologicaldata,clinicalpathwayflowmodels&population cost & clinial impact.
Belowisatypicaldatavisualisationshowingpathwayflow&clinicalimpactanalysisforaparticulardrug.
Source: bazian, the Economist Intelligence Unit Healthcare
Estimating need for treatment, breast cancer patients
Total BC cases
Non invasive
InvasiveAdvanced
disease
Early andlocally advanced Survivors
No diseaseprogression
Diseaseprogresses
Die beforedisease progresses
90%
10%30%
70%
35%
65%
95%
5%
Investmentintounderstandingandengagingpayorsandpatientstodefinevalue will pay dividends when managing a product portfolio and a long-term research and development (R&D) strategy. Companies should consider non-traditional approaches to R&D that will enhance value, for example by improving drug adherence or enhancing bio-availability.
Frugal innovation taking place in the emerging markets for drugs and devices may also hold some hints to competing in a value-based environment. For example, a pocket-sized ultrasound device could not only replace the stethoscope, but also, because of its added imaging abilities, reduce the

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
© The Economist Intelligence Unit Limited 2013 19
number of unnecessary referrals and thus confer cost savings. The barriers to adoption include the initial cost of purchasing such a device, as well as the inherent conservatism of doctors, which makes them generally prefer tried and tested technologiesxix.
Flexible pricing dealsPartnerships with ACOs or providers to increase adherence levels could be one way to improve recorded outcomes. Using data to demonstrate how a therapy will lead to lower total overall costs, for instance through lower hospitalisation rates, demonstrate relative value.
Flexible pricing strategies include, for instance, rebates and refunds for patients who do not respond to certain drugs. These are just some of the tactics that can help branded pharmaceutical companies retain a share of the market in a value-based environment. GSK, for example, has negotiated various pricing strategies for Tyverb/Tykerb (lapatinib), its treatment for advanced breast cancer, which we discuss in the section below.
Again customising these approaches to different emerging markets is key. Our experience has been that sustained success by suppliers in the high growth regions requires in depth local knowledge, in order to develop effective and relevant strategies.
Emerging business models: Getting personal
One way to improve the cost-effectiveness of treatments—particularly expensive cancer drugs—is to target them better. This not only ensures less money is spent on ineffectual treatment, but also minimises the number of patients suffering from side-effects. For that reason, an increasing number of drugs are now being approved along with companion diagnostics,whichidentifythosepatientswiththerightbiomarkerstobenefit.Thetrendtowardspersonalisedmedicines has the potential to dovetail neatly with the trend towards value-based health.
There are now several drugs that are widely used along with diagnostic tests. Roche’s Herceptin (trastuzum), a breast cancer treatment, is usually used after a positive test for the protein marker HER-2. For Roche’s Avastin (bevacizumab), the test has to be negative. This has helped to persuade some health payers to fund these drugs, even though they cost anestimatedUS$50-100,000forayear’streatmentperpatient.Glivec/Gleevec(imatinib),aNovartistreatmentforchronic myloid leukemia, relies on companion tests for the Philadelphia chromosome and proto-oncogene c-Kit.
Switzerland’s Roche, which has a huge cancer portfolio, is so convinced that such tests will be crucial to prove cost-effectiveness that it has inked diagnostic deals with several companies, including Clovis, Transgene and most recently Pac Bio. AstraZeneca UK is one of several companies to have struck up alliances with Denmark’s Dako to develop companion diagnostic tests.

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
20 © The Economist Intelligence Unit Limited 2013
INVESTORS: Activity forecast and value-based due diligenceSegments likely to see greater demand in the near future include healthcare IT systems, patient health records and data analytics providers. Communications and IT systems that help coordinate patient records across the continuum of care will also be required at a magnitude not previously encountered in hospital-centric models. Still in its early days, value-based health strategy and execution relies heavily on the availability of the right data and records, without which it is not possible to implement fully.
Existing players, such as Bupa Health Dialog, offer analytical products and services that help commissioning bodies improve patient care and achieve cost savings. These will see high demand going forward, as more such bodies will look to streamline their operations out of necessity. Finally, the move towards lower
Emerging business models: Flexible pricing dealsThe cost-effectiveness criteria applied to cancer drugs is a source of particular debate, given that such drugs are often extremely expensive and may only be effective in limited population groups or may extend life by only a few months. Yet for the patients involved, and their families, the hope they offer may be vital.
Somecompanieshavetriedtogetaroundthisproblembyofferingflexiblepricingdeals.GlaxoSmithKline,forexample,has had a lengthy struggle over Tyverb/Tykerb (lapatinib), its treatment for advanced breast cancer. In 2008, it offered the UK’s National Institute for Health and Care Excellence (NICE) an annual price-cap on the cost of reimbursing the drug.In2009,ittriedanotheroffer,ofacost-sharingdealthatwouldhaveseenthecompanyfundthefirst12weeksoftreatment. The advantage of such deals for GSK is that they would have kept the formal price of the drug high, avoiding knock-on effects in reference pricing systems.
NICE has consistently rejected these offers, saying that GSK had not yet proved Tykerb’s cost-effectiveness in comparison with rival treatments, notably Roche’s Herceptin. It was also worried that the drug often has to be used in combination with other treatments, hiking the effective price. GSK is continuing to conduct trials on Tykerb, often in combination with other treatments, or for extended uses, including as a treatment for gastric cancer.
ThedrughasalsobenefitedfromtheUK’sdecisiontoallocatespecificfundingof£200m(US$312m)ayeartocancertreatments that might otherwise have failed cost-effectiveness tests. That fund was supposed to end next year, when the UK introduces a new value-based pricing system to be overseen by NICE, but it has recently been extended to 2016. Sales ofTykerbroseby6%in2012,to£239m,althoughtheycontinuetofallshortofinitialhopes.

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
© The Economist Intelligence Unit Limited 2013 21
intensity primary care may present opportunities for investors and providers alike to diversify and vertically assimilate for a more relevant service offering for the future.
Barringanysignificantinnovation,consolidationisalsolikelyaspricepressures increase, with the industry unable to support its current complexity of players and margins. Expect to see both vertical and horizontal consolidation with middlemen and unnecessary margins eliminated.
Case in point: Price vs value-add trade off analysis for new product launch
A medical device supplier looking to introduce a new handheld imaging device to GPs in Indonesia commissioned a conjoint analysis and customer insight study. The aim was to understand the optimal trade-off between price and value-added features.
The Economist Intelligence Unit Healthcare designed research that drew on both primary research and existing expertise in order to generate customer feedback and assess affordability. The research involved focus group discussions with GPs, as well as quantitative surveys with 300 GPs.
The resulting analysis yielded insights on the features that added the most value and outcomes, while understanding the range of acceptable prices for the device among their target customers. Armed with information about price elasticity of demand, the medical device supplier was able to tailor its product and route to market to meet market needs.
Source: Clearstate, the Economist Intelligence Unit Healthcare
Source: The Economist Intelligence Unit Healthcare.
0
10
20
30
40
50
60
75706560555045403530252015
IDR m
�
��
�
��
� �
�
��
��
Pote
ntia
l dem
and
(%)
58
52
47
41
35 3128
26
19
118
42
Demand highest atprices IDR15 m
The demand is less elastic for the price range IDR35 m - IDR50 m
The demand is very elastic for theprice range IDR50 m - IDR60 m
Demand loss of 15%
Demand is lowestat prices
IDR65 m - IDR75 m

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
22 © The Economist Intelligence Unit Limited 2013
Clinical expertise in commercial due diligenceIn the midst of this transaction activity, investors will need to account for value-based health as part of their commercial due diligence process. With value-based purchasing and reimbursement becoming the norm, outcomes in healthcare will eventually be entirely interlinked with an entity’s commercial success.
In particular, investors need to understand the extent to which value-based health affects the target’s markets and operating environment, and its impact on current and future achievable market size and share. This includes an analysis of the regulatory environment, market access and pricing, procurement and reimbursement practices, the value potential of its product pipeline (for pharmaceuticals and medical technology) in the new environment.
It is also imperative for investors to understand the target’s competitive positioning and performance in value terms, as historical performance alone may lead to nebulous conclusions, given the step change toward value-based health. An analysis of demand and forecasts of changes to the care pathway through a systematic review of evidence will help to evaluate the future commercial strength of the target, given its current product or service portfolio.
Failing to look into this aspect in healthcare transactions put investors at risk of arriving at wrong strategic and tactical decisions.

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
© The Economist Intelligence Unit Limited 2013 23
Case in point: Investment due diligence for a private equity investor
A leading private equity fund was exploring a hospital investment opportunity and wanted comprehensive commercial due diligence on the market and the asset to make an informed go/no go decision.
The Economist Intelligence Unit Healthcare were able to provide fast turnaround time, with a team of six full-time consultants with specialist skills and local Indonesian knowledge to be stationed exclusively at the client site to validate the investment thesis as the deal went live. Through a detailed analysis of the hospital group’s operational data, and our expertise on drivers of hospital revenue, we were able to build a demand forecasting model using both statistical and primary data to assess the market potential, actual market size and market share of the hospital. This enabled us to assess the achievability of the target’s business case and quantify the extent of the opportunities on offer.
We also conducted management and insurance partner evaluations, assessed clinical standards, and looked into the viabilityoftheirfuturecashflows.Throughcustomerinterviewswealsoidentifiedriskfactorstotheinvestmentofthetarget’s plans to enter the medical tourism business.
The client was presented with a true, unbiased depiction of the commercial circumstances in which the target operates. They were able to make the investment decision with a clear picture, backed up by credible data and tested assumptions.
Source: Clearstate, the Economist Intelligence Unit Healthcare
Analysis framework
Financial Projections(Profitability, Breakeven Analysis)
Healthcare LandscapeAssessment
Business ModelEvaluation
OperationsAssessment
Develop deatailed hospitalstrategy and implementation plan
Conduct feasibility assessment to evaluate potential candidatePhase 2Phase 1
Proposed future business model:Detailed proposal on targetcustomers, service offerings,pricing levels etc.
Clinical operations changes:Suggestions to improve clinicalefficacy, quality standards etc.
Risk mitigation:Assessment of major risks andappropriate ways to manage
Resources and investment:Outline detailed resources interms of finances, people etc.
Detailed financial projections:Develop financial projections forfirst five years of operations
Execution plan:Outline key tasks and milestones
Macro healthcaremarket trends andreform
Regulatory scan ofrelevant policies
Competitor analysisof private/publichealthcare providers
Socio-economic profileof key target segments
Primary and secondary marketsfor private healthcare
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
Target customer analysis
Service offerings
Competitive positioning(including pricing)
Reputation and quality(e.g. accreditationstatus, etc.)
Strategic partnerships(e.g. governmentteaching universities,insurance firms)
Marketing andbrand strategy
Management team
Clinical team(expertise level)
Patient Service
Human Resources(recruiting costs, mix)
IT
Back office operations,efficiency (finance, purchasing)
Risk identificationand mitigation
Provideconclusionsto supportgo/no godecisions

24 © The Economist Intelligence Unit Limited 2013
SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
Conclusion
Value-based health is here to stay. It will have profound and enduring implications for the way health markets operate, both on the supply and demand side.
Implementing value-based health requires a refocus, a mind-set shift that begins with an acknowledgement that better patient outcomes should be the end goal for any action or decision in healthcare. This means understanding how evidencecansupportcarepathwaystoprovidegreaterefficacy,efficiencyand,ultimately, better quality healthcare for the patient.
For the supply side, business models will need to change radically to accommodate the downward pressure on margins and move towards outcome-driven purchasing. On the demand side, purchasing, regulation and the operation of health markets will alter dramatically, as will health infrastructure requirementsandhealthfinancingmechanisms.
Emphasis on value and cost will lead to industry consolidation, but where excesses are destroyed, innovation in business models will continue to push the industry forward. This will provide opportunities for growth and return for those adaptable enough to be proactive and embrace this trend for the step-change opportunities it provides.
SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare

About The Economist Intelligence Unit Healthcare
The Economist Intelligence Unit Healthcare helps organisations operating across the healthcare sector to build successful and sustainable businesses through independent commercial research and clinical expertise.
Clinical evidence-based practice
An innovative pioneer of evidence based research, helping clients to optimise clinical outcomes and deliver better value health products and services
Commercial practice
Specialist emerging market healthcare research consulting helping clients solve tough strategic and commercial challenges with detailed market intelligence
© The Economist Intelligence Unit Limited 2013 25

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
26 © The Economist Intelligence Unit Limited 2013
Our approachOur unique approach combines an inherent knowledge of macroeconomic and regulatory environments with specialised healthcare market research consulting and a detailed clinical perspective, to help clients support their strategic decisions, improve outcomes and achieve competitive advantage in an increasingly complex healthcare marketplace.
Where are the drivers of growth and opportunities globally?Country, regulatory, demographic and economic conditions affecting the risks and opportunities in healthcare
Global macro & forecasting
What are some important clinical developmentsand trends, and their implications for my business?
Care pathways, clinical evidence, outcomes research,health technology assessments
Clinical evidenceWhat market dynamics am I facing, how should I
plan my business and marketing strategy?
Strategic and tactical insights, go-to-market strategyand commercial due dilligence
Commercial strategy

AcknowledgementsThedevelopmentofthiswhitepaperbenefitedsignificantlyfromtheinputandsupport provided by the expert team including:
robert Cook, Clinical Director at bazian
Danielle Worster, Senior Information Specialist at bazian
Ana Nicholls, Managing Editor, Industry Briefing at EIU healthcare
Contact detailsFor more information on how Economist Intelligence Unit Healthcare can support your organisation’s transition toward achieving better value in healthcare, please contact:
address:
The Economist Intelligence Unit
20 Cabot Square
London E14 4QW
United Kingdom
Website:
www.bazian.com
www.clearstate.com
www.eiu.com
michelle Chan
Marketing Director, EIU Healthcare
Tel:+44(0)2075768059
Daniel morris
Commercial Director, EIU Healthcare
Tel:+44(0)2075768000
Dr vivek muthu
Managing Director, EIU Healthcare
Tel:+44(0)2075768000
© The Economist Intelligence Unit Limited 2013 27

SUCCEEDING IN a valUE-baSED ENvIroNmENtNew business models to thrive in the future of healthcare
28 © The Economist Intelligence Unit Limited 2013
ReferencesiOfficeofActuaryCentreforMedicareandMedicaidServices(CMS)
iiOfficeofActuaryCentreforMedicareandMedicaidServices(CMS)
iiiPorterME,TeisbergEO.Redefininghealthcare.Boston,MA:HarvardBusinessSchoolPress,2006.
ivPorterME,TeisbergEO.Redefininghealthcare.Boston,MA:HarvardBusinessSchoolPress,2006.
vhttp://www.nejm.org/doi/full/10.1056/NEJMp1011024
vihttp://www.nejm.org/doi/full/10.1056/NEJMp1011024
viihttp://hbr.org/2013/10/the-strategy-that-will-fix-health-care/ar/2
viiihttp://clinicalevidence.bmj.com/x/set/static/cms/efficacy-categorisations.html
ix http://www.cancerscreening.nhs.uk/prostate/faq07.html
x http://www.bazian.com/case_studies/NCGUltraOrphanDrugs
xi http://www.nice.org.uk/newsroom/features/measuringeffectivenessandcosteffectivenesstheqaly.jsp
xii http://www.healthengland.org/health_england_publications.htm
xiiiPorterME,TeisbergEO.Redefininghealthcare.Boston,MA:HarvardBusinessSchoolPress,2006.
xivhttp://hbr.org/2013/10/the-strategy-that-will-fix-health-care/ar/2
xv http://www.bazian.com/case_studies/Cleft_Lip_and_Palate
xvi http://www.bazian.com/case_studies/Bupa
xviihttp://www.forbes.com/sites/brucejapsen/2013/07/10/unitedhealthcare-makes-50-billion-wager-on-accountable-care-as-obamacare-looms/
xviii http://www.bazian.com/case_studies/CSAS
xix http://www.technologyreview.com/news/426336/medicine-needs-frugal-innovation

© The Economist Intelligence Unit Limited 2013 2
LONDON
20 Cabot Square
London
E14 4QW
United Kingdom
Tel: (44.20) 7576 8000
Fax: (44.20) 7576 8500
E-mail: [email protected]
NEW YORK
750 Third Avenue
5th Floor
New York, NY 10017
United States
Tel: (1.212) 554 0600
Fax: (1.212) 586 1181/2
E-mail: [email protected]
HONG KONG
6001, Central Plaza
18 Harbour Road
Wanchai
Hong Kong
Tel: (852) 2585 3888
Fax: (852) 2802 7638
E-mail: [email protected]
GENEVA
Rue de l’Athénée 32
1206 Geneva
Switzerland
Tel: (41) 22 566 2470
Fax: (41) 22 346 93 47
E-mail: [email protected]
The Economist Intelligence Unit The Economist Intelligence Unit is a specialist publisher serving companies establishing and managing operations across national borders. For 60 years it has been a source of information on business developments, economic and political trends, government regulations and corporate practice worldwide.The Economist Intelligence Unit delivers its information in four ways: through its digital portfolio, where the latest analysis is updated daily; through printed subscription products ranging from newsletters to annual reference works; through research reports; and by organising seminars and presentations. The firm is a member of The Economist Group.
While every effort has been taken to verify the accuracy of this information, The Economist Intelligence Unit Ltd. cannot accept any responsibility or liability for reliance by any person on this report or any of the information, opinions or conclusions set out in this report.
Copyright © 2013 The Economist Intelligence Unit Limited. All rights reserved. Neither this publication nor any part of it may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, by photocopy, recording or otherwise, without the prior permission of The Economist Intelligence Unit Limited.
Cover image - nui7711/Shutterstock