EHR System Selection - American Health Information...
36
© Copyright 2007 American Health Information Management Association. All rights reserved. EHR System Selection Practical Tools for Seminar Learning
Transcript of EHR System Selection - American Health Information...

© Copyright 2007 American Health Information Management Association. All rights reserved.
EHR System Selection
Practical Tools for Seminar Learning

Disclaimer
i
The American Health Information Management Association makes no representation or guarantee with respect to the contents herein and specifically disclaims any implied guarantee of suitability for any specific purpose. AHIMA has no liability or responsibility to any person or entity with respect to any loss or damage caused by the use of this audio seminar, including but not limited to any loss of revenue, interruption of service, loss of business, or indirect damages resulting from the use of this program. AHIMA makes no guarantee that the use of this program will prevent differences of opinion or disputes with Medicare or other third party payers as to the amount that will be paid to providers of service.
How to earn one (1) CEU for participation
To earn one (1) continuing education unit, each participant must do the following: Step 1: Listen to the seminar, via Webcast link, audio CD, or MP3. Step 2: Complete the assessment quiz contained in this resource book.
Use the included answer key. Do not return the quiz to AHIMA. Save it for your records.
Step 3: EACH LISTENER must visit
http://campus.ahima.org/audio/fastfactsresources.html and complete the sign-in form and the seminar evaluation.
Step 4: After you complete the evaluation, you will receive your CE certificate which
you should print for your records. The certificate must be retained by each participant as a record of their participation, along with a copy of their completed quiz.

Faculty
ii
Angela K. Dinh, MHA, RHIA Angela Dinh is Manager of Professional Practice Resources at the American Health Information Management Association (AHIMA). In her role Ms. Dinh provides professional expertise to develop AHIMA products and services aimed at furthering the art and science of health information management (HIM). Specifically, she is responsible for ongoing development in the areas of HIM in Physician Practice as well as HIPAA Security. Prior to joining AHIMA, Ms. Dinh was employed as an HIM consultant with a leading consulting service, Precyse Solutions, Inc., where she traveled nationwide to assist in many HIM functions from abstracting to EHR solutions to interim management from client site to client site. This included creating and implementing policies and procedures, analyzing and improving workflow, as wells as maintaining day to day operations. Before consulting, Ms. Dinh has worked in various HIM roles including management in a healthcare software company. Her expertise, however, lies in physician practice implementation. She has experience in physician practice, managing the implementation process of EHRs and has hands-on experience with multiple EHR systems. Ms. Dinh has also served as an adjunct instructor for St. Petersburg College (SPC) HIT program in St. Petersburg, FL and actively sits on the Advisory Board. She also serves on the committee at SPC actively in development of a Health Informatics program. Ms. Dinh is a member of a number of professional organizations including AHIMA, her state, and local organizations as well as the American College of Healthcare Executives. Ms. Dinh received her Master’s Degree in Health Administration from the University of South Florida and her Bachelor of Science degree in HIM from the University of Pittsburgh.

Table of Contents
Disclaimer ..................................................................................................................... i How to earn one (1) CEU for participation ......................................................................... i Faculty .........................................................................................................................ii Objectives ..................................................................................................................... 1 What is an EHR? ............................................................................................................ 1 The EHR Market............................................................................................................. 2 Benefits of an EHR ...................................................................................................... 2-3 Before You Begin ........................................................................................................... 3 Criteria and Functionality ............................................................................................. 4-5 Technical Requirements.................................................................................................. 5 Request for Proposal (RFP) ............................................................................................. 6 Vendor Contact ........................................................................................................... 6-8 Vendor Negotiation ..................................................................................................... 8-9 Certification Commission on Health Information Technology (CCHIT).................................10 Vendors .......................................................................................................................10 Summary......................................................................................................................11 Conclusion....................................................................................................................11 Resource/Reference List ...........................................................................................12-13 AHIMA Audio Seminars ..................................................................................................13 About assessment quiz ..................................................................................................14 Thank you for attending (with link for evaluation survey) .................................................14 Appendix ..................................................................................................................15 Articles Resources to Assist Physician Office EHR Selection and Implementation Using Test Vignettes to Assess EHR Capabilities Contracting for ASP Services Assessment Quiz CE Certificate and Sign-in Instructions Quiz Answer Key

EHR System Selection
1
Notes/Comments
Objectives
1. Identify system selection criteria and functionality to be included in a request for proposal (RFP)
2. Initiating Vendor contact
3. Learn about certification for ambulatory care systems through Certification Commission for Health Information Technology (CCHIT)
4. Recognize common vendors
1
What is an EHR?
• Core functions: • capture data• store data • retrieve data
• Integration/Interoperability
• Audit Trails
• Clinical Decision Making
2

EHR System Selection
2
Notes/Comments
The EHR Market
• World Wide Web
• Professional Organizations
• Certification Lists (CCHIT)
• Publications
• Consultant
• Peers
3
Benefits of an EHR
• Increase efficiency
• Ensure accuracy
• Reduce the risk of compliance audits.
• Increase revenues through capture of all charges and accurate and timely insurance billings.
4

EHR System Selection
3
Notes/Comments
More Benefits of an EHR
• Enhance the quality of patient care while allowing the provider to see more patients.
• Allow access to the patient record 24 hours a day and dependent upon set-up, access can be from anywhere an internet connection is available.
• Reduce administrative overhead costs such as inaccurate coding and billing, staff time associated with chart pulls, and storage.
5
Before You Begin…
1. Plan! Plan! Plan!
2. Support and Commitment a. Senior Management Supportb. EHR Task Force
3. Physician Champion(s)/Liaison(s)
4. Plan! Plan! Plan!
6

EHR System Selection
4
Notes/Comments
Criteria and Functionality
• Preventative medicine rules and alerts • Template based documentation (Modifiable
to suit your practice)• Medication Reconciliation• Drug-Drug Interactions• Reporting capabilities
Continued…
7
Criteria and Functionality
• Electronic signatures• Order Entry• Results Management• Coding Capabilities• Interoperability
Continued…
(Continued)
8

EHR System Selection
5
Notes/Comments
Criteria and Functionality (Continued)
• Institute of Medicine’s: Key Capabilities of an Electronic Health Record• http://books.nap.edu/html/ehr/NI000427.pdf
• HL7 EHR System Functional Model• http://www.ahima.org/infocenter/whitepapers/EHR_FM_
Readers_Guide_.rtf
• Certification Commission on Health Information Technology• http://www.cchit.org/
9
Technical Requirements (Continued)
• Network Infrastructure
• Database Server
• User Interfaces
• Hardware
• HIPAA Security Standards
10

EHR System Selection
6
Notes/Comments
Request for Proposal (RFP)
• What is it?
• Format Types
• Sample Template• http://library.ahima.org/xpedio/groups/public/document
s/ahima/bok1_034278.hcsp
11
Vendor Contact
• Identify Vendors• Consultant• Vendor Internet Sites• Websites of market research• Professional Organizations• User Groups• Peers
Continued…
12

EHR System Selection
7
Notes/Comments
Vendor Contact
• Traffic Control• Set rules• Identify key contact person• Set time limits• Evaluation/Elimination method
(Continued)
Continued…
13
Vendor Contact
• Step 1• 8 – 10 Vendors• General overview• Further research needed
• Step 2• Top 5 – 7 Vendors• Send the RFP• On-site Demos
(Continued)
Continued…
14
EHR System Selection
8
Notes/Comments
Vendor Contact
• Step 3• Top 1 – 2 (3 maximum)• Request additional information• Client references• Site visits
(Continued)
15
Vendor Negotiation
• Who?• Senior Management• The Task Force• Key members of task force• One person• Legal counsel
Continued…
16

EHR System Selection
9
Notes/Comments
Vendor Negotiation
• For Discussion • Pricing (What is included, what is not)• Support (Is this an extra cost post
implementation?)• Implementation (Is this a separate fee? How
much is included?• Hardware and software• Warranties
(Continued)
Continued…
17
Vendor Negotiation
• For Discussion • Licenses (Does one need to be purchased for
each individual user or is it a concurrent license for a certain number of users?)
• Maintenance and upgrades• Application Service Provider (ASP) option• HIPAA Business Associate Agreement
(Continued)
18

EHR System Selection
10
Notes/Comments
Certification Commission on Health Information Technology
• CCHIT is a voluntary, private organization providing certification of health information technology products in the industry.
• Launched by AHIMA, HIMSS, and the Alliance.
• Certification based on specific outlined criteria.
• http://www.cchit.org/
19
Vendors
• Cerner Coporation • http://www.cerner.com
• McKesson Coporation • http://www.mckesson.com
• Misys Healthcare Systems• http://www.misyshealthcare.com
• GE Healthcare – Centricity• http://www.gehealthcare.com
• Siemens Medical Solutions• http://www.medical.siemens.com
20

EHR System Selection
11
Notes/Comments
Summary
1. Plan! Plan! Plan!2. Research EHRs3. Determine Requirements4. Identify Vendors5. RFP Process6. Vendor Contact7. Vendor Selection8. Contact Negotiation
21
Conclusion
““EHRs are not the wave of the future, EHRs are not the wave of the future, they are a staple of today.they are a staple of today.””
22
EHR System Selection
12
Notes/Comments
Resource/Reference List
• Helpful Textbooks1. Amatayakul, Margret and Lazaurus, Steven S. Electronic
Health Records: Transforming Your Medical Practice. MGMA, 2005. ISBN: 1-56829-232-5. Click below for purchase.http://www5.mgma.com/ecom/Default.aspx?tabid=138&action=INVProductDetails&args=478
2. How to Evaluate Electronic Health Record (EHR) Systems By Patricia A. Trites, MPA, CHBC, CPC, EMS, CHCC, CHCO, CHP, CMP(H) and Reed D. Gelzer, MD, MPH, CHCChttps://imis.ahima.org//orders/productDetail.cfm?pc=AB213107&bURL=%2Forders%2FproductByCategory%2Ecfm%3Ft%3D6
23
Resource/Reference List
• Helpful Articles1. Resources to Assist Physician Office EHR
Selection and Implementation http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_030762.hcsp?dDocName=bok1_030762 (NOTE: this article is available to AHIMA members only, through the FORE Library HIM Body of Knowledge)
2. Small Practice, Big Decision: Selecting an EHR System for Small Physician Practices
http://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_031357.hcsp?dDocName=bok1_031357
24

EHR System Selection
13
Notes/Comments
Resource/Reference List
• Helpful Articles3. Using Test Vignettes to Assess EHR Capabilities
http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_031369.hcsp?dDocName=bok1_031369 (NOTE: this article is available to AHIMA members only, through the FORE Library HIM Body of Knowledge)
4. Contracting for ASP Services: When Signing on for the Benefits, Remember to Manage the Risks http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_031316.hcsp?dDocName=bok1_031316 (NOTE: this article is available to AHIMA members only, through the FORE Library HIM Body of Knowledge)
25
AHIMA Audio Seminars
Visit our Web site http://campus.AHIMA.orgfor updated information on the current seminar schedule. While online, you can also register for live seminars or order CDs and Webcasts of past seminars.
© 2007 American Health Information Management Association

EHR System Selection
14
Notes/Comments
Assessment
To access the assessment quiz that follows this seminar, download the seminar’s resource book at
http://campus.ahima.org/audio/fastfactsresources.html
Thank you for attending!
Please visit the AHIMA Audio Seminars Web site to sign-in and complete your evaluation form online at:
http://campus.ahima.org/audio/fastfactsresources.html
Each person seeking CE credit must complete the sign-in form and evaluation in order to view and print their CE certificate.
Certificates will be awarded for AHIMA CEUs and ANCC Contact Hours.

Appendix
Articles Resources to Assist Physician Office EHR Selection and Implementation http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_030762.hcsp Using Test Vignettes to Assess EHR Capabilities http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_031369.hcsp Contracting for ASP Services http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_031316.hcsp Assessment Quiz CE Certificate and Sign-in Instructions Quiz Answer Key
Resources to Assist Physician Office EHR Selection and Implementation by Mary H. Stanfill, RHIA, CCS, CCS-P
It is widely known that health IT adoption has lagged behind other industries. For more than a year, the federal government has encouraged strategic efforts to foster IT adoption.1 And it appears that momentum is picking up in physician practices. According to the Medical Group Management Association, one in five group physician practices in America has some sort of electronic record with a database containing patient medical and demographic information. In addition, the association reports a steady movement toward a paperless office and full use of electronic health records.2
That is good news when you consider that the vast majority of patient care is delivered in physician offices. Technology benefits applied in the physician office setting could significantly improve quality of care and patient safety within the healthcare industry.
However, many physician offices have trouble selecting an EHR. David Brailer, MD, PhD, national coordinator for healthcare IT, names vendor selection as one of the challenges that medical groups find daunting.3 And no wonder—a Google search for the terms “physician” and “electronic medical record” returns more than 200,000 links.
Looking for the Seal of Approval
Efforts are currently under way to certify electronic products for use in ambulatory care settings. Formed in July 2004, the Certification Commission for Healthcare Information Technology is working to create an efficient and credible method to certify healthcare IT products. This will help reduce the financial risk for providers when they invest in an expensive system. Not surprisingly, Brailer selected physician office EHRs as the first EHR product certification focus under the ambulatory care healthcare arena.4
However, Brailer made it clear that even when certification is available to assist physicians in EHR product selection, physician office staffs are generally not robust enough to take on the formidable task of EHR implementation. He asked the industry to recognize that challenge and assist with tools and resources to encourage adoption through operational changes.
HIM professionals have the knowledge and opportunity to assist physician office EHR selection and implementation. They can bring knowledge of health information processes and workflow into a new way of doing business, while ensuring quality information to support clinical database completeness and accuracy and pay-for-performance optimization.
This column outlines some of the numerous resources available to assist physician practices in identifying, evaluating, selecting, and implementing an EHR. The list offers HIM professionals resources to use in assisting physician practices with EHR selection and implementation. Following are the types of resources featured.
EHR public and private initiatives
Several government-sponsored and private initiatives are under way with an explicit purpose to equip physician practices with EHRs. These groups provide a wealth of information, typically well organized and available at no charge.
Page 1 of 5Practice Toolkit: Resources to Assist Physician Office EHR Selection and Implementation
8/16/2007http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_030762.hcsp?dDoc...

American Academy of Family Physician's Center for Health Information Technology-a major collaboration of physician organizations engaged in the effort to disseminate information to promote EHR adoption (http://www.centerforhit.org/).
California Health Care Foundation, in partnership with Community Clinics Initiative, is engaged in the California Community Clinics EHR Assessment and Readiness Project (http://www.chcf.org/documents/chronicdisease/ClinicsEHRAssessmentReadiness.pdf).
Certification Commission for Healthcare Information Technology-established to accelerate the adoption of robust, interoperable health IT throughout the US healthcare system, by creating an efficient, credible, sustainable mechanism for the certification of health IT products (http://www.cchit.org).
Doctor's Office Quality - Information Technology-a two-year special study demonstration that is designed to improve quality of care, patient safety, and efficiency for services provided to Medicare beneficiaries by promoting the adoption of EMRs and information technology in primary care physician offices (http://www.doqit.org/dcs/ContentServer?pagename=DOQIT/DOQITPage/PageTemplate).
eHealth Initiative is an independent, nonprofit organization whose mission is to drive improvement in the quality, safety, and efficiency of healthcare through information and information technology (http://www.ehealthinitiative.org).
EHR Collaborative-a group of organizations representing key stake holders, whose goal is to advance the adoption of information standards for healthcare (http://www.ehrcollaborative.org/index.htm).
Michigan Electronic Medical Record Initiative (http://www.memri.us/research.html)
Office of the National Coordinator for Health Information Technology-established by executive order to facilitate the effective use of information technology and collaborate with the various sectors in the healthcare industry to advance widespread use of interoperable EHRs (http://www.hhs.gov/healthit/)
Internet EMR/EHR resources
There is abundant information available on the Internet, including how-to articles, buyers guides, best practices, worksheets, and other tools. We’ve compiled some of the most reputable sources for you and encourage you to use these as a starting point as you assist physician practices. In many of these sites you’ll find additional links to other sites with valuable information. As with any Internet search, review information objectively and always consider the source. For example, look for advertisement labels and conflict-of-interest disclosures on all Web sites and articles.
American Academy of Family Practitioners articles and resources are available at http://www.centerforhit.org/x574.xml.
AHIMA articles and best practices available free to the public:
"Core Data Sets for the Physician Practice Electronic Health Record" (http://library.ahima.org/xpedio/groups/public/documents/ahima/pub_bok1_021607.html)"State of the EHR: The Vendor Perspective" (http://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_025338.pdf)
AHIMA e-HIM resources available at http://www.ahima.org/infocenter/ehim/.
California Healthcare Foundation publications:
"Electronic Medical Records: Lessons from Small Physician Practices" (http://www.chcf.org/documents/ihealth/EMRLessonsSmallPhyscianPractices.pdf) "Electronic Medical Records: A Buyer's Guide for Small Physician
Page 2 of 5Practice Toolkit: Resources to Assist Physician Office EHR Selection and Implementation
8/16/2007http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_030762.hcsp?dDoc...
Practices." (http://www.chcf.org/documents/ihealth/ForresterEMRBuyersGuideRevise.pdf)
"EMR Shopping? Finding Your Way in a Crowded Marketplace." SHANDS Healthcare. (http://www.shands.org/professional/ppd/practice_article.asp?ID=178#)
England's NHS information policy background which describes the purposes and characteristics of patient record systems and examines the question of migration towards paperless practice and the education and training needs of paperless practices (http://www.dh.gov.uk/assetRoot/04/06/97/65/04069765.pdf).
Health Information and Management Systems Society additional resources available at http://www.himss.org/ASP/topics_ehr.asp.
"Interested in EMR Software? Look Before You Leap." ACP Observer, October 2003. (http://www.acponline.org/journals/news/oct03/emr_software.htm)
Medical Group Management Association resources:
Research Connexion (http://www.mgma.com/research/emr.cfm) Electronic Medical Record (EMR) Checklist (ftp://ftp.mgma.com/pub/WEBMISC/Tools/EMR-checklist.pdf)
"Should I Buy an EMR Now? The Experts Weigh In" AMNews October 2004. (Open to AMA members and subscribers to AMNews) (http://www.ama-assn.org/amednews/2004/10/11/ bisa1011.htm)
Vendor resources and resources to identify and evaluate vendors
Many vendors have excellent materials; after all it is to their advantage to help you recommend the EHR that will be the best fit for a physician practice. A few vendor resources are included in our list. You’ll find many more as you begin to investigate specific software products. We encourage you to use vendors’ materials, but don’t let vendors, particularly any one vendor, be your sole source of information. Seek confirmatory information and other more objective sources as well.
Vendors resources
Misys white papers:
"Critical Success Factors for Practice-Wide EMR Implementations" (http://www.misyshealthcare.com/resources/whitepaper.pdf) "EMR Buyer's Guide: Considerations for Practices Evaluating EMR" (http://www.misyshealthcare.com/resources/emr+buyers+guide+white+paper+09041.pdf)
MedicaLogic (GE Medical Systems) peer advice on EMR implementation available at http://www.medicalogic.com/emr/peer_advice/.
Resources to Identify and Evaluate Vendors
AC Group reports evaluate leading electronic health and medical record applications (http://www.acgroup.org/pages/395598/index.htm)
EMR discussion forum available at http://www.emrupdate.com/forum/forum.asp?FORUM_ID=1
KLAS Specialty Reports-in-depth vendor performance reviews covering specific areas of interest to healthcare providers (http://www.healthcomputing.com/site/v2/aboutklas/whoweare.asp)
PhysiciansEHR.com vendor directory (http://www.physiciansehr.com)
Page 3 of 5Practice Toolkit: Resources to Assist Physician Office EHR Selection and Implementation
8/16/2007http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_030762.hcsp?dDoc...

Other resources and use cases
Lastly, seek out those who have paved the way and learn from their experiences. Take advantage of listserves to network with others working with physician practices and take the time to read case studies.
Searching for an EHR can be very time consuming. An individual physician practice may need to spend many weeks, even months, becoming familiar with the systems that are available and analyzing the group practice’s needs and goals. Brailer has asked the industry to assist physician practices in this process, and HIM professionals are well suited to that role.
2004 Centricity Healthcare User Group Presentations available at http://www.emr.msu.edu/2004_chug_presentations_intro.htm.
Adler, Kenneth G. "Why It's Time to Purchase an Electronic Health Record System." Family Practice Management, November/December 2004. Available online at http://www.aafp.org/fpm/20041100/43whyi.pdf.
Hanson, Susan P. and Roy E. Schutzengel. "Pioneers and Perseverance." Journal of AHIMA 75, no. 1 (2004): 38-43. Available online in the FORE Library: HIM Body of Knowledge at http://www.ahima.org.
Moore, Pamela. "We Bought the Wrong EMR! Make the Right Choice the First Time." SHANDS Healthcare. Available online at http://www.shands.org/professional/ppd/practice_article.asp?ID=239.
Sittig, DF, Kuperman GJ, Fiskio J. "Evaluating Physician Satisfaction Regarding User Interactions with an Electronic Medical Record System." Proceedings from the 1999 AMIA Annual symposium: 400-4. Available online at http://www.amia.org/pubs/symposia/D005736.PDF.
Smith, David, and Lucy Mancini Newell. "A Physician's Perspective: Deploying the EMR." Journal of Healthcare Information Management 16, no.2 (Spring 2002): 71-79. Available online at http://www.himss.org/asp/ContentRedirector.asp?ContentID=15735.
"Your Guide to Implementing the EHR: AHIMA Work Groups Deliver Best Practices." Journal of AHIMA 75, no. 1 (2004): 26-31. Available online in the FORE Library: HIM Body of Knowledge at http://www.ahima.org.
Notes
1. Brailer, David, and Tommy Thompson. “The Decade of Health Information Technology: Delivering Consumer-centric and Information-rich Health Care.” July 21, 2004. Available online at www.hhs.gov/healthit/documents/hitframework.pdf.
2. Versel, Neil. “One in Five Group Practices Now Uses EHRs.” Health IT World, January 25, 2005. Available online at www.health-itworld.com/enews/01-25-2005_508.html.
3. Ibid.
4. For more information on the Certification Commission for Health Information Technology, including target dates for EHR certification, go to www.cchit.org.
Mary Stanfill ([email protected]) is a practice manager at AHIMA.
Article citation: Stanfill, Mary. "Practice Toolkit: Resources to Assist Physician Office EHR Selection and Implementation." Journal of AHIMA 77, no.2 (February 2006): 63,65 [extended online
Page 4 of 5Practice Toolkit: Resources to Assist Physician Office EHR Selection and Implementation
8/16/2007http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_030762.hcsp?dDoc...

version].
Copyright ©2006 American Health Information Management Association. All rights reserved. All contents, including images and graphics, on this Web site are copyrighted by AHIMA unless otherwise noted. You must obtain permission to reproduce any information, graphics, or images from this site. You do not need to obtain permission to cite, reference, or briefly quote this material as long as proper citation of the source of the information is made. Please contact Publications at [email protected] to obtain permission. Please include the title and URL of the content you wish to reprint in your request.
Page 5 of 5Practice Toolkit: Resources to Assist Physician Office EHR Selection and Implementation
8/16/2007http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_030762.hcsp?dDoc...

Using Test Vignettes to Assess EHR Capabilities by Reed D. Gelzer, MD, MPH, CHCC, and Patricia Trites, MPA, CHBC, CPC, CHCC, CHCO
Test vignettes help evaluate how EHR products handle common documentation needs.
For those who are braving the EHR selection process, there is a great deal of guidance available on how to organize this difficult process. The steady advance of technical standards, functional standards, and product certification contributes much-needed help in compiling functional requirements. (These resources are also helpful to those who are looking to evaluate their current systems.) Organizations can also receive help in evaluating EHR systems through the use of testing protocols that apply established, professionally and legally accepted standards in the form of test vignettes.
Test vignettes, as used in this article, are scripts representing common documentation events, processes, and procedures that occur during an encounter. They seek to illustrate the performance and output of a software system in a fair and reproducible manner. Typically, a knowledgeable system user follows the script and performs the information entry while evaluators observe. The resulting documentation is judged according to professional documentation principles.
In addition to highlighting important software features and functions, test vignettes also assist HIM staff and organization leadership in comparing how various EHR products handle key HIM functions. Vignettes also help illustrate how a provider’s documentation policies and procedures may be reflected in an EHR it currently uses or is considering for purchase.
About This Vignette
Test vignettes can be applied to any health record function. The vignette presented here tests an EHR system’s ability to maintain a legal health record. The script focuses on evaluating functions pertaining to amendments, attestation, authorship, and nonrepudiation, as well as the auditing functions that support their integrity. Constructing the vignette began with a review of the core requirements of medical records as legal business records in a computerized environment.1
No one encounter will include the many functional challenges that this vignette contains. The vignette is not intended to be a typical encounter; instead it presents a test environment that includes a number of common challenges to the documentation workflows that occur in normal practice environments. The vignette does not include all variants that a testing protocol should measure in the course of an HIM-focused, due-diligence process. It is intended as a presentation of one type of testing for one set of critical functions. It is most appropriate as a script for a live or remote demonstration, but it could possibly serve as part of a request for information.
The scenario starts with a review of the context and the system functions being examined. It includes possible requirements regarding general assurances necessary for a system’s evaluation, especially when testing a system for possible purchase. These assurances should
Page 1 of 6Using Test Vignettes to Assess EHR Capabilities
8/16/2007http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_031369.hcsp?dDoc...

be solicited from the vendor prior to the demonstration.
The script of the scenario appears in the table that follows. The organization provides the vendor with the identification and system permissions of the users featured in the script. The analytic questions shown in the "observation" column help guide the evaluator’s queries. (They are not intended as instructions for the user working directly with the software or as questions for the vendor.) These questions address authorship, attestation, nonrepudiation, and auditing, seeking to identify the system’s ability to:
Track exactly who did what tasks and when Support changes in, and additions to, documentation that occurred during the course of an encounter by changing of authors Support changes in, and additions to, an encounter that occurred after the encounter was attested (signed) Re-attest a re-opened encounter, including supporting documentation for the changes as an extraordinary event
Throughout the review, the utility of audit functions should also be noted--where the audit supports differentiation and where it may not, specific to the targeted areas for authorship, attestation, integrity, and amendments. The vendor should be asked to provide a printed copy of the audit report or audit views that substantiate the scenario events that require auditability. Evaluators should also note the required skill set and system security access level.
The objective here is documentation veracity, not speed. The vignette is one example of how testing protocols can be used to compare the ability of different systems to perform common HIM functions.
Scenario: Testing Legal Functionality
Scenario Context
An established patient presents with a scheduled appointment for an annual physical. The patient already has PFSH, medications, labs, and radiology information in the system.
The visit is in a primary care practice where staff trust is high, intake staff members have the discretion--in line with practice policies and procedures--to do common tests when deemed highly likely to be needed or as specifically established as standard operating procedure (e.g., U/A on a first-trimester pregnancy).
Purposes
1. Demonstrate system capabilities to support authorship and to demonstrate timeliness, attestation, and nonrepudiation
2. Demonstrate system business rules for building information using common convenience tools and the ability to differentiate the employment of these tools
3. Demonstrate amendment functions 4. Demonstrate appropriately detailed documentation audit features and functions 5. Highlight how each product handles key documentation events and supports authenticity with the
assistance of the system’s audit functions
Demonstration Requirements
1. System must be substantially the same as that generally installed at a client site. 2. A similar test run on a randomly chosen user site must yield substantially the same results. 3. The system must support multiple user identifications within the same encounter. [Note:
demonstration versions may not offer this routinely, so it must be requested to ensure a useful test.] 4. If the tested system has features or functions the vendor would like to emphasize for special notice or
clarification, the vendor may include this information in a separate document, referring back to the test protocol to indicate the context of its relevance.
5. If an opportunity for a verbal explanation is requested from or by the vendor, the point of contact and
Page 2 of 6Using Test Vignettes to Assess EHR Capabilities
8/16/2007http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_031369.hcsp?dDoc...

Scenario
a brief indication for the need is required. This added information will not be considered part of the evaluation, testing, and verification process.
6. The report must include a printed copy of the documentation output, representing what would be sent in response to a request from another medical office or from a third-party payer.
7. The audit report must include a printed copy of the output of the audit and the steps necessary to produce the report.
8. If any portion of the vignette is omitted, explanations must be provided.
Action Observation
I. Intake--user 1 A. Checks patient into the clinical workspace
B. Updates allergies by adding a mild urticarial reaction to penicillin, treated at Hospital X’s ED January 1, 2006
Can the system identify new general patient information that is added by user 1 in the encounter? [Note: some systems do not identify the user when changes are made to general patient information fields that are separate from the encounter functionality and workflow. Some systems will not indicate the state of the data prior to the change, instead noting only that information within that functional area was changed.]
Can the added allergy be identified in the system as associated with the encounter by date and user ID?
C. Documents vital signs: T/BP/P/R and weight
Does the system associate each data field input with user 1? Alternatively, are vital signs recorded in a table and is each new table a unique event that can be associated with a different user?
D. Documents presenting problem or chief complaint: annual physical
Does the system associate the information with the user 1 ID?
E. Documents basic HPI/ROS using the standard tools and functions within the system including those generally used by providers. (Please note separately if the system does not permit, under any setup options, a subset of intake users to employ the provider HPI and ROS tools). Within HPI/ROS:
Does the system associate the information with the user 1 ID?
1. Identifies episodic fatigue and malaise or similar
Does the system associate the information with the user 1 ID?
2. Identifies episodic visual blurring Does the system associate the information with the user 1 ID?
3. Identifies "no cardiac symptoms" as the patient reported item
Does the system associate the information with the user 1 ID?
4. Cues global "all other ROS items negative" function, if available
Does the system separately identify or otherwise support the differentiation of information recorded by a "global" statement from uniquely selected individual information elements? [Note: "global" cues or "aggregate documentation events" are those documentation tools that support either cueing a series of documentation insertions or outputs as a result of one user action, keystroke, or click, including those that insert boilerplate text or defined norms or normals.]
Does a global or aggregate event generate detailed documentation text? If so, is it distinguishable in the output from uniquely selected, typed, or voice-recognition documentation? Is it distinguishable using user-accessible audit functions?
Does any coding accumulation in the background calculate the same codes whether from global or aggregate documentation
Page 3 of 6Using Test Vignettes to Assess EHR Capabilities
8/16/2007http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_031369.hcsp?dDoc...
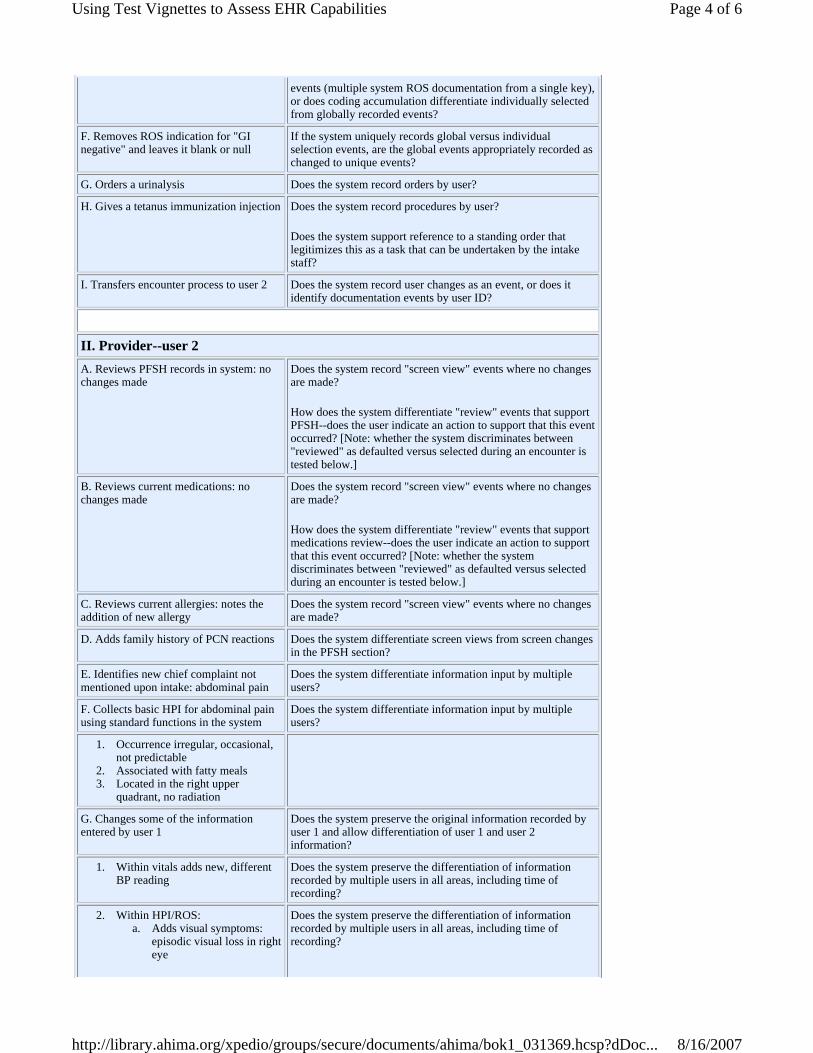
events (multiple system ROS documentation from a single key), or does coding accumulation differentiate individually selected from globally recorded events?
F. Removes ROS indication for "GI negative" and leaves it blank or null
If the system uniquely records global versus individual selection events, are the global events appropriately recorded as changed to unique events?
G. Orders a urinalysis Does the system record orders by user?
H. Gives a tetanus immunization injection Does the system record procedures by user?
Does the system support reference to a standing order that legitimizes this as a task that can be undertaken by the intake staff?
I. Transfers encounter process to user 2 Does the system record user changes as an event, or does it identify documentation events by user ID?
II. Provider--user 2 A. Reviews PFSH records in system: no changes made
Does the system record "screen view" events where no changes are made?
How does the system differentiate "review" events that support PFSH--does the user indicate an action to support that this event occurred? [Note: whether the system discriminates between "reviewed" as defaulted versus selected during an encounter is tested below.]
B. Reviews current medications: no changes made
Does the system record "screen view" events where no changes are made?
How does the system differentiate "review" events that support medications review--does the user indicate an action to support that this event occurred? [Note: whether the system discriminates between "reviewed" as defaulted versus selected during an encounter is tested below.]
C. Reviews current allergies: notes the addition of new allergy
Does the system record "screen view" events where no changes are made?
D. Adds family history of PCN reactions Does the system differentiate screen views from screen changes in the PFSH section?
E. Identifies new chief complaint not mentioned upon intake: abdominal pain
Does the system differentiate information input by multiple users?
F. Collects basic HPI for abdominal pain using standard functions in the system
Does the system differentiate information input by multiple users?
1. Occurrence irregular, occasional, not predictable
2. Associated with fatty meals 3. Located in the right upper
quadrant, no radiation
G. Changes some of the information entered by user 1
Does the system preserve the original information recorded by user 1 and allow differentiation of user 1 and user 2 information?
1. Within vitals adds new, different BP reading
Does the system preserve the differentiation of information recorded by multiple users in all areas, including time of recording?
2. Within HPI/ROS: a. Adds visual symptoms:
episodic visual loss in right eye
Does the system preserve the differentiation of information recorded by multiple users in all areas, including time of recording?
Page 4 of 6Using Test Vignettes to Assess EHR Capabilities
8/16/2007http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_031369.hcsp?dDoc...

b. Changes urinary from intake to indicate nocturia, twice per night
c. Leaves the rest blank or unchanged
H. Within physical exam, indicates positive and negative findings in at least five system exam areas including neurological, cardiovascular, and abdominal/GI using a mixture of positives and negatives. Do not mention murmurs in cardiovascular examination.
I. Within physical exam, indicates skin/dermatological findings are all normal by a global key, if available
Does the system differentiate user input and, if global key documentation events are supported, how are they differentiated from unique selection?
J. Reviews the U/A result Does the system differentiate user activities? How is clinical information review captured?
K. Completes the assessment or impression section
1. Diagnosis: abdominal pain, possible cholelithiasis
2. Diagnosis: UTI
L. Completes the plan section 1. Diagnostic ultrasound of abdomen 2. Refer to general surgery 3. Patient instructed to call provider
if fever, vomiting, worsening pain
M. Completes the documentation tasks and executes closing tasks and signature equivalents
How are closing events and signature events recorded? Identify in the accompanying report the steps undertaken by a user to execute a signature event. (Use screenshots if appropriate or helpful.)
N. If available, show how nursing or checkout staff can document any printed patient instructions after the encounter has been closed
How are additional information events recorded? How are they identified as components of the encounter?
O. Recalls additional exam findings not documented; re-opens encounter to document ophthalmic exam and add to cardiac exam
How does the system record and differentiate the inputs from different authors made at different times?
How are amendments supported and differentiated from the original, signed record? How are amendments connected to the original documentation? How are additions to documentation and to processes such as tests and referrals identified and preserved?
1. Adds PERRL, extra-ocular movements, inability to maintain lateral gaze, vision blurs
2. Adds funduscopic negative 3. Adds new cardiac finding: new
systolic murmur, 3/6 4. Adds new diagnosis: cardiac
murmur, NOS 5. Adds new referral: cardiology 6. Adds new scheduled test: cardiac
ultrasound
P. Resigns encounter How does the system handle resignature events and differentiate them from the original closing events?
If the EHR system is to be integrated or interfaced with a billing system, how does the documentation function interact with the
Page 5 of 6Using Test Vignettes to Assess EHR Capabilities
8/16/2007http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_031369.hcsp?dDoc...

Note
1. AHIMA. "Update: Maintaining a Legally Sound Health Record--Paper and Electronic." Journal of AHIMA 76, no. 10 (2005): 64A-L. Available online in the FORE Library: HIM Body of Knowledge at www.ahima.org.
billing system to avoid duplicate billing for the same event and to provide coding edits or corrections?
Reed D. Gelzer ([email protected]) and Patricia Trites ([email protected]) are cofounders of Advocates for Documentation Integrity and Compliance, an educational, advocacy, and consulting organization. The authors thank members of the AHIMA e-HIM® Work Group on Maintaining the Legal EHR for feedback and comment on the test vignette presented in this article.
Article citation: Gelzer, Reed D., Trites, Patricia. "Using Test Vignettes to Assess EHR Capabilities." Journal of AHIMA 77, no.5 (May 2006): 56-59.
Copyright ©2006 American Health Information Management Association. All rights reserved. All contents, including images and graphics, on this Web site are copyrighted by AHIMA unless otherwise noted. You must obtain permission to reproduce any information, graphics, or images from this site. You do not need to obtain permission to cite, reference, or briefly quote this material as long as proper citation of the source of the information is made. Please contact Publications at [email protected] to obtain permission. Please include the title and URL of the content you wish to reprint in your request.
Page 6 of 6Using Test Vignettes to Assess EHR Capabilities
8/16/2007http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_031369.hcsp?dDoc...

Contracting for ASP Services: When Signing on for the Benefits, Remember to Manage the Risks by Thomas G. Dolan
By sweating the IT, ASPs offer providers an easier way to go digital. But providers should ensure they can get their data back when and how they want.
Say you've outsourced mission-critical applications to an application service provider (ASP). Everything goes well, but then something happens. Your ASP goes out of business, or maybe it loses interest in pursuing the particular type of business it sold you, or maybe you get into a dispute over a payment or other issue. The cause doesn't matter as much as the result. For suddenly the friendly customer service and IT maintenance that was once there evaporates. You're left with a dump of data in a proprietary format that you cannot use. Or maybe you're left trying to get your data back at all, in any form. What should you have done differently?
Providers can spare themselves such worst-case scenarios by ensuring that the contracts they sign establish their ownership of the data and spell out an orderly transition of data back from the ASP should events ever require it.
With Benefits Come Risks
ASPs offer an easier entry into electronic practice, especially for smaller providers. Contracting with an ASP is usually less expensive than purchasing, implementing, and maintaining IT systems. Often the ASP stores its software and the customer's data on its own hardware, and the customer logs on through a high-speed Internet connection. In other arrangements, the data or even the hardware reside with the healthcare provider.
However, the relationship requires careful attention. After all, you're putting your data in someone else's hands. "Most healthcare customers tend to be impressed by great ASP software," says Marilyn Lamar, a partner at McDermott Will & Emery, Chicago, IL. "But it's important they bring a critical risk analysis component to the table as well."
"I would start by doing due diligence on the background of the ASP itself," Lamar advises. "Some of them are very large and stable, and some are not." Start by researching the ASP's financial data, which you can do if it's a publicly traded company. If it's a privately held company, Lamar says, "it may be unwilling to disclose its records. Perhaps it's never been audited and doesn't want to make that information public. If it doesn't, I wouldn't recommend doing business with it."
Lamar also suggests making sure that you are dealing with the right corporate entity. Ask questions, because you may find that the large corporate parent company isn't the entity that actually contracted with you. Instead you may be dealing with a small subsidiary with little capital, maybe even a shell company set up for tax purposes. "We see this happen fairly often," says Lamar. "You should make sure you contract with the parent company that has the assets."
Page 1 of 3Contracting for ASP Services: When Signing on for the Benefits, Remember to Manage t...
8/16/2007http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_031316.hcsp?dDoc...

Whose Data Is It, Anyway?
Providers often overlook the critical issue of data ownership, says Lamar. "You have to have a statement in the contract that the data is the sole property of the customer," she advises, noting that contracts frequently fail to mention the issue at all. Ownership is critical should the provider and the ASP part ways. In the worst-case scenario, Lamar says, you want this statement if you need to go to court or, even more importantly, if you need to threaten to go to court. If the ASP knows this statement is in the contract, it is more likely to back down before incurring court expenses.
Contracts should also specify that the data are backed up at specified intervals. It's silly to outsource data tasks and then ask to receive backups every day, Lamar says, but weekly or monthly backups will guard against major data loss if something goes wrong at the ASP. Lamar also suggests specifying audit rights in the contract, so that you can check on the data at any particular time and verify its current status and integrity.
Providers need to guarantee the integrity and availability of their data for compliance reasons as well as quality of care. If you get tangled up in a dispute with your ASP, "your real disaster can start under the HIPAA regulations, which require the confidentiality, integrity, and accessibility of your patient records," says Barry Herrin, a partner at Smith Moore, LLP, in Atlanta, GA. "If you've created a situation in which you can't get at these records, you're in big trouble. Since we've seen the dot-com bubble burst, there's no excuse in thinking that an ASP vendor will be in business forever."
Negotiating contracts to guard against exposure can be complex, admits Herrin, but providers should keep focused on managing their risks. They should also recognize that they have opportunities to vary the noneconomic terms of the contract. "If you focus on your protective rights at the start," Herrin says, "most times, if the price is right, you can get the concessions you want in the contract."
Arranging an Orderly Out
A provider who has established rights to its data still has another important contract item to negotiate: the right to get its data back in a reasonable manner. It’s vital to have an orderly transition in place so that you can move from the old ASP to a new one with up-to-date data and minimal disruption, says Herrin. “My recommendation is to never sign a contract unless an orderly transition period is negotiated,” he says.
Most ASP vendors understand their customers' needs in this respect, Herrin says, and whatever their possible initial resistance are likely to agree. The real problems result when an ASP goes through unexpected financial difficulties and is headed toward bankruptcy, he explains. "In this case the ASP has fewer personnel for maintenance and fulfilling obligations, and it is really only focused on its own troubles. Sometimes they will say, 'Go ahead and sue me. I don't have any money.'"
To mitigate this risk, Herrin says, providers can have a source code escrow agreement built into the contract. Just as in real-estate dealings, the escrow agreement is in the hands of a third party such as a bank. If the ASP goes bankrupt or otherwise breaches the contract and cannot provide the orderly transition promised, the third party is under instructions to provide the code to the client. With the source code--the programming language behind the ASP's software--the provider is assured their data can be converted out of the ASP's proprietary format and into a standard industry format.
Getting Back Data You Can Use
There are two potential complications in negotiating to receive source code. The first is that
Page 2 of 3Contracting for ASP Services: When Signing on for the Benefits, Remember to Manage t...
8/16/2007http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_031316.hcsp?dDoc...

the ASP may not want to share it--it may be reluctant to give up its software license, notes Lamar. The second is that only computer programmers understand it. A provider who receives the ASP's source code still faces the expense and delay of having it processed.
"Source codes are very complicated," warns Stanley Crane, chief technology officer of ASP vendor Allscripts in Chicago, IL. "There might be one to two million lines of code. We have a development team of about 100. If you have to deal with source code at a period of critical transition, you're in for a lot of complications."
Clients are better served ensuring that their data are made available to them in industry standard formats, whenever they request, Crane says. That's the right thing for vendors to do, he says, and he recommends doing business with vendors who agree to that condition.
Terry Daly, RN, agrees that translating source code is not ideal, but given that it is not insurmountable she thinks clients are well served by an escrow agreement. Daly, vice president of marketing for InteGreat Concepts of Scottsdale, AZ, notes that the database behind their program, for example, runs off a standard Microsoft platform. "You should be able to have or hire one database administrator who understands this source code," she says.
Daly also points out that the risks differ depending on the ASP model. Some ASPs install and maintain their systems on site, so the data reside at the customer's facility. If the ASP should go out of business, the provider would no longer receive upgrades or maintenance, but it could still function with what it had on hand until it got a new vendor. (In situations where data reside in the provider's facility, Crane reminds providers to be certain the contract addresses who is responsible for backing up and storing the data.)
The bottom line, advises Lamar, is to ensure the continuity of your business, that "at the end of your term, your data will be presented to you in a format that is generally readable by other systems."
Herrin agrees. "After [Hurricane] Katrina, people are thinking more in terms of disaster planning," he says. "But this is a disaster that can occur without a hurricane. The worst-case nightmare is if you sit down with a new ASP vendor and have no usable data for your financials or patient records and have to start all over."
Thomas G. Dolan is a healthcare and business writer based in the Pacific Northwest.
Article citation: Dolan, Thomas G.. "Contracting for ASP Services: When Signing on for the Benefits, Remember to Manage the Risks." Journal of AHIMA 77, no.5 (May 2006): 48-50.
Copyright ©2006 American Health Information Management Association. All rights reserved. All contents, including images and graphics, on this Web site are copyrighted by AHIMA unless otherwise noted. You must obtain permission to reproduce any information, graphics, or images from this site. You do not need to obtain permission to cite, reference, or briefly quote this material as long as proper citation of the source of the information is made. Please contact Publications at [email protected] to obtain permission. Please include the title and URL of the content you wish to reprint in your request.
Page 3 of 3Contracting for ASP Services: When Signing on for the Benefits, Remember to Manage t...
8/16/2007http://library.ahima.org/xpedio/groups/secure/documents/ahima/bok1_031316.hcsp?dDoc...

Assessment Quiz – EHR System Selection
ANSWERS to this quiz are found on the last page of the seminar resource book, Practical Tools for Seminar Learning.
To earn continuing education credit of one (1) AHIMA CEU, Fast Facts Audio Seminar listeners must also complete this 10-question quiz. This CE credit is for attending the audio seminar AND completing this quiz. Please keep a copy of the completed quiz with your certificate of attendance. Do not send a copy to AHIMA.
1. If an EHR can exchange information with a pharmacy system, what is the correct term for the exchange of information between the two systems? a. Interface b. Health Information Exchange c. Interoperability d. Data transmission
2. The overall key functions of a __________ are basically to be able to capture data or enter data and retrieve it easily. a. Medical Record b. Electronic Health Record c. Computer Network d. Interface
3. True or false? CCHIT certifies ambulatory care systems only.
a. True b. False
4. One way to assist in identifying vendors in the market is a. Phonebook b. Newspaper c. Consultant d. Billboards
5. A _________ invites vendors to provide their EHR’s specifications, company history, answer the needs and questions, and provide costs. a. Vendor Selection b. Request for Product Information c. Request for Product & Pricing d. Request for Proposal
6. True or false? In step 1 of vendor contact, RFPs have not been sent out.
a. True b. False
7. This method of EHR application use is similar to paying rent. The user accesses the EHR housed on computers managed by the vendor. a. Vendor Negotiation b. Private Network c. Application Service Provider (ASP) d. None of the above
8. Step 3 of vendor contact should include __________. a. Off-site visits b. Demonstrations c. Food and treats d. On-site visits
9. True or false? Step 2 of vendor contact recommends that the vendors be narrowed down to 5-7 vendors.
a. True b. False
10. CCHIT was launched by a. American Health Information Management
Association b. Healthcare Information and Management
Systems Society c. The National Alliance for Health Information
Technology d. All of the above
Do not send a copy of completed quizzes to AHIMA. Please keep them with your certificate of attendance, for your records. Be sure to sign-in and complete your evaluation form, to receive your certificate, at
http://campus.ahima.org/audio/fastfactsresources.html.
To receive your
CE Certificate
visit http://campus.ahima.org/audio/fastfactsresources.html
click on the link to
“Sign In and Complete Online Evaluation” listed for this seminar.
You will be automatically linked to the
CE certificate for this seminar after completing the evaluation.
Each participant expecting to receive continuing education credit must complete the online evaluation and sign-in information,
in order to view and print the CE certificate.

Quiz Answer Key Fast Facts Audio Seminar: EHR System Selection 1: c; 2: b; 3: false; 4: c; 5: d; 6: true; 7: c; 8: a; 9: true; 10: d Do not send a copy of your completed Fast Facts Audio Seminar quiz to AHIMA. Please keep it with your certificate of attendance, for your records.