
eHealth Strategy Business Plan - University of Michiganioe481/ioe481_past_reports/w0009.pdf ·...
81
- - University of Michigan Health System eHealth Strategy Business Plan April 21, 2000 Univ eL’s it V of Michigan Iusiness SchooL Multidisciplinary Action Project Team Julie Brennan Sachin Kheterpal, M.D. Chekesha Kidd Jin-Kyoung Kim Tim Mohnke Ron Perry Faculty Advisor: Jane Dutton Company Liaisons: Deborah Biggs J.D., Paul Taheri M.D., M.B.A.
Transcript of eHealth Strategy Business Plan - University of Michiganioe481/ioe481_past_reports/w0009.pdf ·...

_
-
-
University of MichiganHealth System
eHealth Strategy Business Plan
April 21, 2000
Univ eL’s it V
of MichiganIusinessSchooL
Multidisciplinary Action Project TeamJulie BrennanSachin Kheterpal, M.D.Chekesha KiddJin-Kyoung KimTim MohnkeRon Perry
Faculty Advisor: Jane DuttonCompany Liaisons: Deborah Biggs J.D., Paul Taheri M.D., M.B.A.

University ofMichi2an Health System E-Health Stratev Business Plan
L UMHS BACKGROUND 1
A. CURRENT CHALLENGES 1
B. USE OF TECHNOLOGY AT UMHS 1
IL MARKET ANALYSIS .._.—.— .... .... -..
A. INDUSTRY ANALYSIS 2
B. TARGETMARKEI 3
C. COMPETmON 4
D. REGULATORY ISSUES 6
E. FUTURE TARGET MARKETS 6
III. PROPOSED PRODUCT AND SERVICE................................._.........__.. ........... .......7
A. PRODUCT OVERVIEW 7
B. PRODUCT ARCHITECTURE 7
C. CONSUMER USE 10
D. PRODUCT BENEFITS 11
E SECURITY AND CONFIDENTIALITY 12
F. COPYRIGHTS, PATENTS, AND TRADE SECRETS 13
0. PRODUCT LIABILITY 13
H. PRODUCT EXTENSIONS 13
H. EXIT STRATEGY 13
1V. COMPANY .. .................................13
A. NATUREOFTRE BUSINESS 13
B. DISTiNCTIVE COMPETENCIES AND UNIQUE RESOURCES 14
V. MARKETING AND SALES STRATEGY...... .. ........................... ..
A. POTENTIAL CUSTOMERS AND NEEDS IDENTIFICATION 15
B. MARKET SEGMENTS AN]) CUSTOMER PRI0RTnzATION 15
C. PRICING 15
D. DISTRIBUTION AND PROMOTION 17
VL ORGANIZATION, MANAGEMENT, O’.VNERSRIP, AND OPERATIONS. _..................................17
A. STRUCTURE 17
B. STAFFING — PRODUCT DEVELOPMENT 18
C. STAFFING - OPERATIONS 19
D. INCENTIVE STRUCTURE 19
E. PARThERSIIWS AND ALLIANCES 21
VIL FUTURE PRODUCTS.._................ ....._-.---.......
A. PHYSICIAN INFORMATION WEB PAGE (P1W) 24
B. DECISION SUPPORT SYSTEM 24
C. CONTINUING MEDICAL EDUCATION 24
D. JUST -IN-TIME EDUCATION 24
VIII. PERFORMANCE METRICS .. .................. ....... ......._ .. ......
IX. FUNDING REQUIREMENTS........................... ............- .. ._.....
A. CURRENT FUNDING REQUIREMENTS 27
B. FUNDING REQUIREMENTS THROUGH 2005 28
C. LONG RANGE FINANcLL SFRATEGY 28
X. FINANCIAL PROJECTIONS .. ...... .. ......... ..
A. ASSUMPTIONS 29
B. 5-YEAR PROJECTIONS 30
University’ ofMichigan Business School Map Team 19
University ofMichi2an Health System E-Health Stratev Business Plan
LIST OF APPENDICES
APPENDIX A: MARKET ANALYSIS 31
APPENDIX A-i: Technical Demands of Health-Related Applications of the Internet 32APPENDIX A-2: Competitive Analysis - Players 32APPENDIX A-3: Competitive Analysis — Tier 4 Competitors 33APPENDIX A-4: Competitive Analysis — Tier 3 Competitors 35APPENDIX A-5: Future Target Markets 37
APPENDIX B: PROPOSED PRODUCT AND SERVICE 38
APPENDIX B-i: Overview of CPW 39APPENDIX B-2: Detailed Product Map 40APPENDIX B-3: Technical Architecture 41APPENDIX B-4: Education Delivery Process 42APPENDIX B-5: Product Termination Timeline 43
APPENDIX C: SLAES AND’MARKETJNG 44
APPENDIX C-i: Target Customers of CPW 45APPENDIX C-2: Potential Customer Analysis 46APPENDIX C-3: Market Segmentation 47APPENDIX C-4: Segment Prioritization Template 48APPENDIX C-5: Customer Prioritization Template 49APPENDIX C-6: EVA Analysis 50
APPENDIX D: ORGAMZATION AND PARTNERSHIP 51
APPENDIX D-i: Organization Chart of NEWCO 52APPENDIX D-2: Staffing and Salaries - Product Development Phase 53APPENDIX D-3: Staffing and Salaries - Operations Phase 54APPENDIX D-4: Competitive Analysis 56APPENDIX D-5: Potential Partners Company Description 57APPENDIX D-6: Required Capabilities of Potential Partners 59
APPENDIX E: FUTURE PRODUCTS 60
APPENDIX E- 1: Product Synergies 61
APPENDIX F: FINANCIAL PROJECTIONS 63
APPENDIX F-i: Development Phase Financial Projection Assumptions 64APPENDIX F-2: Product Development Cost Summary 65APPENDIX F-3: Detailed Product Development Costs 66APPENDIX F-4: Detailed General & Administrative Costs - Operations 67APPENDIX F-5: Proforma Income Statement and Statement of Cash Flows 68APPENDIX F-6: Sensitivity Analysis 69
APPENDIX G: LIST OF INTERVIEWS 70
BIBLIOGRAPHY 73
University ofMichigan Business School Map Team 19

Universifl’ ofMichigan Health System E-Health Siraiev Business Plan
Executive Summary
University of Michigan Health System BackgroundWith an annual expense budget of $1 billion dollars and 15,663 employees and faculty, theUniversity of Michigan (UMHS) rivals many prominent US firms in temis of size while facingunique regulatory and legislative challenges as a public institution. Due to increasing fmancialpressures placed upon health systems, and academic medical centers in particular, UMHS isfaced with the task of fmding innovative profitable endeavors that leverage its significantintellectual capital, technical knowledge, clinical experience, and prestige.
Market AnalysisAs superior clinical outcomes become more commonplace among providers, consumers of the$1.2 trillion health care industry are increasingly demanding a superior service experience todifferentiate health systems and providers. At the same time, health systems must increase thepatient base in order to maintain revenues in the face of decreasing reimbursement rates andutilization. Patient education and information have been identified as two of the most importantmodifiers of overall patient satisfaction. Surveys indicate that patients want more educationalinformation from their physician. Furthermore, data indicate that 52 million individuals will visitWeb health care sites in the year 2000. The case to satisfy the health care consumer’s unmet needfor reputable, individualized, timely, and usable health care education materials is extremelycompelling.
,-, Proposed Product‘..J NEWCO will develop a software engine that links existing patient information databases with
appropriate educational content to create a customized patient web page (CPW) accessed bypatients using a unique patient ID and password. The web page will contain information aboutthe patient’s current conditions, treatments, medications, and procedures in addition to basichealth maintenance activity educational materials. Once developed and proven using the UMHSpatient set, the web engine will be sold to other health systems, payors, and self-insuredcorporations.
Marketing StrategyNEWCO has identified that current industry trends are forcing health care institutions to seekcredible clinical content providers and tools to increase patient base. Utilizing UMHS’significant national brand awareness, its patient base as a showcase for the product, and strategicrelationships, NEWCO will successfully segment and target entities responsible for ensuringpatient satisfaction, outcomes, and cost reduction: 3600 hospitals, 4000 payors, and Fortune 100self-insured companies.
Competitive AnalysisThough over 15,000 health care web sites currently offer static web content that must be filteredand interpreted by the patient, only a handful of competitors such as Cemer Corporation andLDX / ChannelHealth hope to deliver customized patient web content. None of these potentialcompetitors has ownership of the crucial patient data necessary to develop, deploy, or refme theproduct. Furthermore, they do not possess the credible and evidence-based clinical contentoffered by UMHS.
University ofMichigan Business School Map Team 19 ui
University ofMichi2an Health System E-Health Strate’v Business Plan
Company Description, Organizational Structure, and ManagementNEWCO will be a Michigan for-profit taxable subsidiary of the Michigan Health Corporation(MHC). MHC was established by the Regents of the University as a vehicle to participate in,coordinate, and develop health care related activities to maintain and enhance the educational,research and service missions of the University. Technical staff will be full-time employees andstockholders of NEWCO. UMHS clinical staff will be motivated to develop clinical contentthrough market-competitive cash reimbursement and stock ownership.
Revenues and ProfitabilityNEWCO requests an initial investment of $1.6 million from UMHS over an eight-month productdevelopment period to realize revenues of $11 million in 2003, resulting in an NPV of $4.9million and payback period of three years on a cumulative cash flow basis. These projections arebased upon conservative estimates of staffing requirements, development costs, and marketshare. Equity relationships with strategic technical, content, and distribution partners will beinvestigated to decrease the UIvIHS capital investment.
Value to U1fflSThe CPW product line will be used as a launching pad to future strategic health care productofferings such as a Customized Physician Information Web Page, Decision Support System, andInteractive Continuing Medical Education and Just-In-Time Education.
The formation of NEWCO and successful launch of the CPW will add needed non-clinicalrevenue to the UMHS bottom line while furthering its educational mission. In addition, it willencourage UMHS faculty to leverage their intellectual capital through internal UMHS ventures.
University ofMichigan Business School Map Team 19 iv

University ofMichiean Health System E-Health Stratevv Business Plan
L IJMHS Background
The University of Michigan Health System (UMHS) is comprised of the Medical School and itsFaculty Group Practice, 7 hospitals, 30 health centers, 120 outpatient clinics, M-CARE HMOand Michigan Health Corporation. In order to retain its non-profit fmancial status, decisions andbusiness endeavors must directly affect the three pronged mission of excellence in patient care,education, and research.
Recognized by US News and World Report as a top 10 medical center and medical school,UMHS has earned an excellent reputation. In FY 1999, UMHS received 36,713 admissions and1,231,216 outpatient visits. UMHS has been fortunate to maintain a profitable operation in pastyears. As health care industry pressures increase, however, the health system must continue togenerate revenue while decreasing costs and providing high quality patient care. UMHS mustsimultaneously build upon its existing educational and research activities.
A. Current Challenges
The majority of academic medical center revenue is generated through clinical care. With themovement to managed care and discounted fee-for-service, hospital margins have been declining(Spanier, 2000). UMHS, like other academic medical centers, has traditionally relied on cross-subsidization of funding from clinical services to support research and educational missions.This is becoming more difficult as reimbursement declines and pressures to reduce costs
“—- continue. To thrive in the future, UMHS must leverage its strengths and develop innovativemethods of generating revenue. eBusiness has the potential to serve as a significant source ofrevenue for early-to-market organizations. UMHS should take advantage of this opportunity.
Currently, massive amounts of clinical, research, and educational information reside withinUMHS’s databases, Internet sites, individual departments, and faculty minds. However, UMHSis not fully leveraging its intellectual capital. Members of the faculty are selling their clinicalknowledge to Internet content providers such as Oncology.com. To curb this “brain drain,” thehealth system has the opportunity to develop an innovative business and incentive structure toencourage faculty to participate in activities that will benefit patients, the health system, thefaculty members themselves.
B. Use of Technology at UMHS
One of UMHS’s greatest strengths is its advanced research and application of technology.Throughout the University campus, UMHS participates in development and use of cutting-edgetechnology. Some of the existing projects include:
Visible Human Project Medical Readiness TrainereMail for clinical care enhancement (CHOICES) Web-based health risk appraisal and educationClinical telemedicine and tele-education Remote patient wound managementSurgical Simulation Center
University ofMichigan Business School Map Team 19 1

University ofMichk’an Health System E-iIealth Strateav Business Plan
UMHS is also a leader in the development of the Intemet2 project based in Ann Arbor. Intemet2is an initiative led by over 170 universities working with industry and government to developand deploy advanced network applications and technology. These activities uniquely positionUMHS to serve as a leader in developing an eHealth strategy to better serve patients, families,and communities.
IL Market Analysis
A. Industry Analysis
The health care services industiy is comprised of a complex network of private for-profitcorporations, non-profit organizations, federal agencies, and state bodies. Academic medicalcenters are affected by all of the changes in the health care industry in general. Some of thesechallenges include, but are not limited to:
• Rapid increase in the age of the population• Continued transition to ambulatory care from inpatient care• Declining funding and reimbursement• Increasing consumer power and knowledge• Large uninsured population - approximately 40 million Americans remain uninsured• Patient rights initiatives - improving patient rights to choice, information, and privacy• Internet and technology changes affecting the delivery of care• Increasing utilization of homeopathic therapies by patients and allopathic clinicians
A major trend affecting all types of medical care is the increasingly important role of technology.The Internet is being used by patients to gather information about their own, their families’, andfriends’ diseases or health status. Health care providers use the Internet to collect clinical data,track patient records, and communicate within their own institutions.
The chart below illustrates the evolution of health care and the impact of technology.
Today Time
a,
Cu>a,
Cu0,
RemoteCare
RemoteTreatment
(::(fradjtjon\mea
- Telecare- DistantMonitoring
- Medscape-WebMD
- Magazine- Brochure
- Telemedicine- Remote prescription
- Customized patient info- Personalized healtheducation
Source: Goldman Sachs, MAP Team analysis
University ofMichigan Business School Map Team 19 2
University ofMichiL’an Health System E-Health Stratev Business Plan
Currently, consumers and providers have the opportunity to retrieve static and limited interactive
information from Web sites. Due to current reimbursement guidelines and changes to operations
that are necessary to accommodate new technology, remote care is not immediately feasible for
most institutions. However, as technology and infrastructures advance, remote care will becomemore ubiquitous. In the future, the Internet and private networks will be utilized for extensiveresearch, training and education opportunities. Today, educational opportunities are the most
promising because they require limited technology infrastructure and are not capital intensive fororganizations with mature IT infrastructure.
The table in Appendix A-l page 32 provides a relative scale of the importance of varioustechnological capabilities in the delivery of education, research and clinical care.
Within the health care field, the Internet provides a variety of media for providers and other
organizations to communicate with consumers. According to a study published by the ComputerScience and Telecommunications Board and the National Research Council (2000),
“Ongoing trends in health care are likely to reinforce the trend toward consumer-oriented health information. . . Patients have been encouraged to take a more active
role in their own health care, and care providers have recognized the value ofengaging patients to participate more meaningfully in their own care. Attempts bycare providers and managed care plans to streamline services and cut costs have
shortened hospital stays, increasing the need for patients and their families tounderstand how to provide care for themselves. Greater emphasis is being placedon preventive care, which requires consumers to understand health risks and theeffects of different behaviors on health. These trends heighten the need forconsumers to have access to reliable health information and open channels ofcommunication to care providers and other health professionals.”
As technology and health care continue to merge, full-service health sites will emerge in the
consumer market. According to research by Forrester (2000), “health systems will need topublish their own materials and participate in direct-to-consumer marketing as educated,
empowered consumers shop for health services with increasing discernment.”
B. Target Market
The patient education market offers the greatest opportunity for web-based products and is our
initial target market. Currently, patient education over the Internet consists of Web sitesproviding healthcare information for health information seekers. The sites typically include basichealth information, community interaction (via chat rooms/news groups), and access to moreadvanced information through search and message boards. Information posted on the Internet isnot monitored for quality or accuracy, yet consumers continue to demand more.
Medical information is the second most sought after topic on Internet, and 40% of all US Internet
users are somewhat active health info seekers (Goldman, 1999). In 1998, 34 million peopleaccessed health information on the Web. In 1999, 45 million people sought health information onthe Web, and in 2000, 52 million people will seek health information on the Web. 53% of online
Universitr ofMichigan Business School Map Team 19 3

/
University ofMichi’an Health System E-Health Strate’ Business Plan
health information seekers are female, and 60% of online health information seekers are over theage of 40 (Goldman, 1999). The market segment continues to grow.
Over the past decade, the patient has become more of a partner in physician-patient encounter.Education is a key component of this encounter, but the majority of patients do not feel that theirphysician provides adequate information during encounters. Consequently, many individualsturn to the Internet for additional information. The younger the patient, the more likely they areto use the Internet for health information. However, the fastest growing online population isindividuals over the age of fifty. 84% of patients surveyed during a MEDSTAT study indicatedthat they want better access to health care information (Picker, 1999). 77% of patientsinterviewed in a recent survey stated they would like to receive on-line information from theirphysician (Healtheon, 2000).
Many providers rely on patient satisfaction measures to determine how well they are meetingconsumer needs. The Picker Survey allows providers to evaluate how well they are addressingthe educational needs of patients. The primary factors that correlate best with overall patientsatisfaction are emotional support and informationleducation. A customized web site that allowsproviders to better educate their patients will increase overall satisfaction leading to higher levelsof patient retention and referrals.
Although patients are actively seeking information on the web, physicians do not believe thatmedical information on Internet has helped to better educate patients (Picker, 1999). According
C to interviews conducted by the UMHS MAP Team, most physicians do not refer patients toparticular health/medical sites, mainly because they are not able to identify credible and safesites. Consumers, including patients and clinicians, feel the sites lack credibility of content(Physician, 2000). “A recent study found that 6% of the 400 sites containing information on aform of cancer called Ewing’s sarcoma contained erroneous information, and many more were
There is an unmet need in the patient education market for a credible, accurate and easy-to-navigate patient information site. “Consumers need effective searching and filtering tools thatcan identify and rank information according to their needs and capabilities and present theinformation in a form that they can understand. . . Consumers also need a way to judge the quality,authoritativeness, and provenance of the information.”(Goldman, 1999) Better educated patientswill be able to work with their physicians to produce better health outcomes. Physicianscurrently spend valuable time “uneducating’ patients concerning information they received onthe Internet. A site that proactively directs high-quality information to patients and links patientsto other credible sites will reduce these problems and fulfill an unmet patient need.
C. Competition
Market estimates indicate that there are 15,000 consumer health information web sites, but thereis a clear lack of differentiation among most sites. Some sites are sponsored by credible medicalorganizations such as the American Cancer Society or the American Medical Association; otherscontain postings by any individual. Unfortunately, many people are unable to discern betweenaccurate and inaccurate information, and this is a major concern of health care professionals.
University ofMichigan Business School Map Team 19 4
University ofMichii’an Health System E-Health Stratei’v Business Plan
Out of the 15,000 health information web sites, there is a handful of established players, such asMedscape and WebMD, who have distinguished themselves through content, credibility orinfrastructure. New players such as Medem, created by a consortium of seven medicalassociations, are emerging and hope to provide credible information for patients and providers.Other companies are focusing solely on providing content; ADAM, a major commercial medicalcontent provider with 10,000 pages on 1,500 topics, is an example. Similarly, PubmedJMedlineis a search engine providing 9.2 million medical citations.
Recently developed sites allow users to type in personal information in order to receive updatesand information specific to their disease state. WebMD is an example of such a site. These sitesare not connected to personal medical records that allow the site to proactively “push”appropriate information to consumers.
A few companies offer products that allow patients to receive individualized health information.Individual patients can then access a personal web page and obtain relevant health information.Medivation is marketing its product to small physician practices and individual offices. IDX /ChannelHealth and Cemer have also establishid individual web sites; these are being marketedto physician groups, hospitals, and health systems.
Academic medical centers have access to patient records and credible medical education contentthat would enable them to create individualized web products. IT-savvy centers such as JohnsHopkins and Mayo Clinic have developed consumer Web sites and possess internal publishingcapabilities. Intellihealth is a site that was initially developed and co-branded by Hopkins andAetna. This partnership has since ended (Advisory, 2000), but Hopkins retains the experience tolaunch new products. Mayohealth is a similar site sponsored by the Mayo Clinic. Duke also hasthe potential to develop advanced applications from its current web site.
Although academic medical centers are uniquely positioned to create individualized medicalcontent web sites, the MAP Team was unable to identify any AMCs developing or offering aproduct with individualized health content linked to medical records. The market for this productis attractive, and it is likely that other AMCs may attempt to develop a product in the near future.
Please review Appendices A2, A3, and A4 on pages 32-35 for a schematic representation of thiscompetitor analysis.
Although the market for individualized patient education is large, barriers to entry haveprevented many companies from launching products to meet truly consumer needs. The greatestbarriers to entry include:
• Access to patient data: The producer of an individualized patient web site must haveaccess to patient data in order to link appropriate content to an individual’s site. Onlymedical providers and payors have direct access to this data.
• Credibility of clinical content: Successful players must provide general and high-level
care information. Those that hold the content internally have a significant advantage overthose that have to purchase it from others.
Universig’ ofMichigan Business School Map Team 19 5

University ofMichwan Health System E-Health Sfratev Business Plan
• Breadth and depth of clinical content: Content must be specific enough to address theindividual needs and concerns of a wide variety of patients.
• Technology resources: Organizations must have the technical capability to develop andcustomize patient-specific sites.
• Costs of development and maintenance: Costs to develop software and technologyinfrastructure are high and often prohibitive for many organizations
D. Regulatory Issues
Legislation and government play a major role in the health care industry. Recent legislation hasfocused on decreasing costs within the health care industry, increasing consumer rights andaccess to care, and ensuring security of information. The most relevant pieces of legislation arebriefly discussed below.
a) Balanced Budget Act (BBA)The 1997 Balanced Budget Act reduced the Medicare budget significantly over five years,which continues to greatly affect provider reimbursement.
b) Health Insurance Portability and Accountability Act (HIPAA)’The proposed enactment of HIPAA will force sweeping changes to strengthen healthinformation access, security, and privacy.
c) Patients’ Bill ofRightsThe Patients’ Bill of Rights is intended to provide increased access to health care services andenforce legal liability for payor clinical recommendations.
d) Other LegislationThe Medical Information Protection Act of 1999, Health Care Personal InformationNondisclosure Act of 1999, and the Medical Information Privacy and Security Act 2 are threelaws that require specified health entities in possession of protected health information toallow the subjects of the information to inspect, copy and amend it.
E. Future Target Markets
Patients will be our initial target in the education market. The product will be marketed tohospitals, physicians, health systems, payors and self-insured corporations; the information willbe transmitted to patients through these parties. Future target markets for educational materialswill include practicing physicians, medical schools, students, other medical institutions, andother health professionals. Information concerning the sizes of these various markets can befound in Appendix A-5, page 37.
‘For further details on HIPAA, visit the Department of Health and Human Services at www. hhs.gov.2 Information concerning the three bills related to health privacy was derived from bill summaries contained on theLibrary of Congress’s THOMAS system, available online at http://thomas.loc.gov/home/thomas.html
University ofMichigan Business School Map Team 19 6

Universiti’ ofMjchi’gn Health System E-Health Stratev Business Plan
IlL Proposed Product and Service
A. Product Overview
NEWCO will develop a software engine that links existing patient information databases withappropriate educational content to create a Customized Patient Web Page (CPW) accessed bypatients using a unique patient ID and password. The web page will contain information aboutthe patient’s current conditions, treatments, medications, and procedures. In addition, the sitewill present basic health maintenance educational materials and provider communication. Aschematic of the CPW is available in Appendix B-i, page 39.
A basic review of the healthcare information technology industry reveals that 95% of health careinstitutions do not have the comprehensive electronic medical record (EMR) necessary toidentify a given patient’s cliiical conditions (Goldman, i999). No database describes a patient’ssocial history, past medical history, active diseases processes, current medications, or desiredhealth maintenance activities.
A clinician carrying the title of “patient educator” must select the appropriate educationalmaterials that apply to a given patient’s demographics, ethnicity, clinical condition, and healthstatus. Because the current process does not leverage existing patient data or contribute to areusable knowledge base, the task is repeated each time a new patient is encountered. As a result,health care entities must engage in an extremely expensive, labor-intensive process of repeatedlycollating a patient’s personalized educational materials (traditional or electronic) de novo.
There are unmet needs for high quality, personalized health care information. Encouraged by“my” web site fever (myYahoo.com, mySAP.com, etc.), consumers are now demanding accessto the right information at the right time on the Internet, not all information all of the time aspreviously thought. This holds particularly true for the healthcare information market.
B. ProductArchitecture
The proposed product is a set of software engines that perform several crucial functions:i. Interface to the reimbursement and EMR databases2. Translation and mapping of client-specific patient condition databases to a single,
common, reusable patient condition database3. Storage of patient education content in a single, reusable content database4. Linkage of the patient condition database to the content database5. Delivery of desired content as an HTML-based, secure and confidential web site
As the diagram below illustrates, the software engines will create three electronic databases toperform these five functions. The three electronic databases, described in greater detail below,are:
1. Patient-specific clinical conditions2. Patient education material3. Linkages between patient conditions and appropriate education materials
University ofMichigan Business School Map Team 19 7

Ilnivpr.clft, nfMlphirjran I1aIIh cv.ctni F-ffpalIh .cfratoi, Rnclnpvc Plan
Patient Clinical Condition and Reimbursement Database
Though the patient specific, discrete clinical data created by an EMR is not available at mosthealth systems, all entities involved in the health care delivery process must codif’ a patient’sclinical diagnoses and treatment in order to be reimbursed. Communication between clinicalproviders (health systems, hospitals, clinics, etc) and payors (government, private insurance, etc)occurs through three ubiquitous lexicons used throughout the United States:
1. Current procedural terminology (CPT) of 4,000 codes2. International classification of diagnoses (lCD) of 15,000 codes3. Diagnosis related groups (DRG)
All health care institutions must create electronic databases of patient CPT, lCD, and DRG codesin order to participate in the electronic data interchange (EDI) mandated by payors. The creationof these databases is a complex and confusing process. After disbursing clinical services, aclinician creates documentation necessary to accurately communicate the patient’s history,status, and care plan from one provider to another — the paper medical record. An abstractor orhealth record analyst (HRA) reviews this clinical documentation at a later date and identifieswhich CPT, lCD, and DRG codes apply to the clinical encounter and patient. Because theprimary purpose of this data is communication with payors, the codes selected by the HRAs areoptimized for maximum reimbursement. Several codes often describe a given condition, but aspecific code may be chosen based upon experience regarding its likelihood of acceptance andreimbursement by the patient’s specific payor. In isolation, a given lexicon’s single code may notaccurately represent a patient’s true clinical condition. When utilized in aggregate and withrelatively simple filters to exclude contradictory conclusions, the codes are capable of accuratelydescribing a patient’s clinical conditions. For example, these electronic databases are a crucial
Engine
For a more detailed product diagram, please review Appendix B-2, page 40:
University ofMichigan Business School Map Teaml9 8
University ofMichiL’an Health System E-Health Strate’v Business Plan
source of clinical information employed for clinical outcome research, individual clinician and
institutional benchmarking, and cost-per-case analysis.
As industry trends force health care institutions to migrate to EMR, increasing amounts of
patient information databases will be available. Once available, these EMR databases will be
employed in lieu of billing data to improve the specificity and accuracy of the educational
content delivered to the patient.
Patient Educational Material / Content Database
The second set of databases necessary to provide customized content is the patient education
information. This clinical content currently exists in many forms: pamphlets, clinical care
protocols, practice guidelines, web site content, and other published materials. It is available
from a variety of sources in the public and private domain ranging from government
organizations to for-profit medical content entities previously mentioned. To date, this content
has been stored and distributed at a macroscopic condition level (asthma) or health maintenance
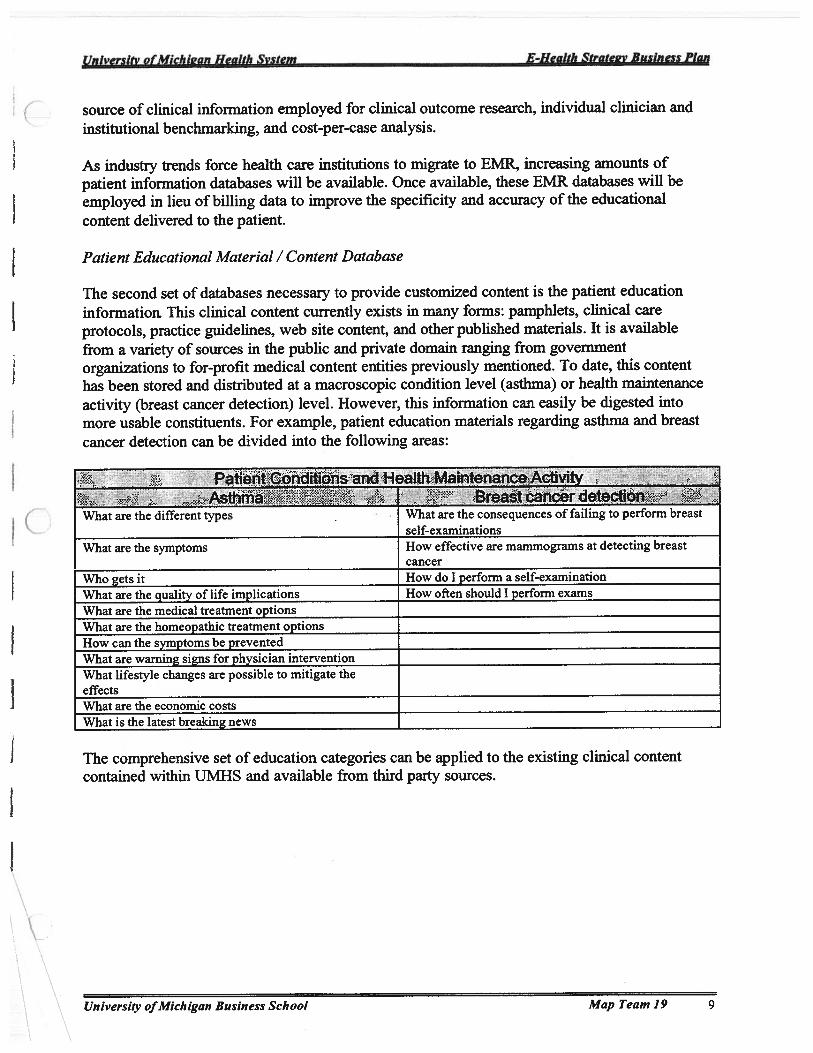
activity (breast cancer detection) level. However, this information can easily be digested into
more usable constituents. For example, patient education materials regarding asthma and breast
cancer detection can be divided into the following areas:
Patient Conditions and Health Maintenance ActivityAsthma Breast cancer detection
Vhat are the different types Vhat are the consequences of failing to perform breastself-examinations
What are the symptoms How effective are mammograms at detecting breastcancer
Who gets it How do I perform a self-examinationWhat are the quality of life implications How often should I perform examsWhat are the medical treatment optionsWhat are the homeopathic treatment optionsHow can the symptoms be preventedWhat are warning signs for physician interventionWhat lifestyle changes are possible to mitigate theeffectsWhat are the economic costsWhat is the latest breaking news
The comprehensive set of education categories can be applied to the existing clinical content
contained within UMHS and available from third party sources.
Unn ersiti’ ofMichigan Business School Map Team 19 9
11nivprcifr nfPfirhiornn 1-b’alIh v.cIm F-IIpalfh Stratepv Ruxincx Plan
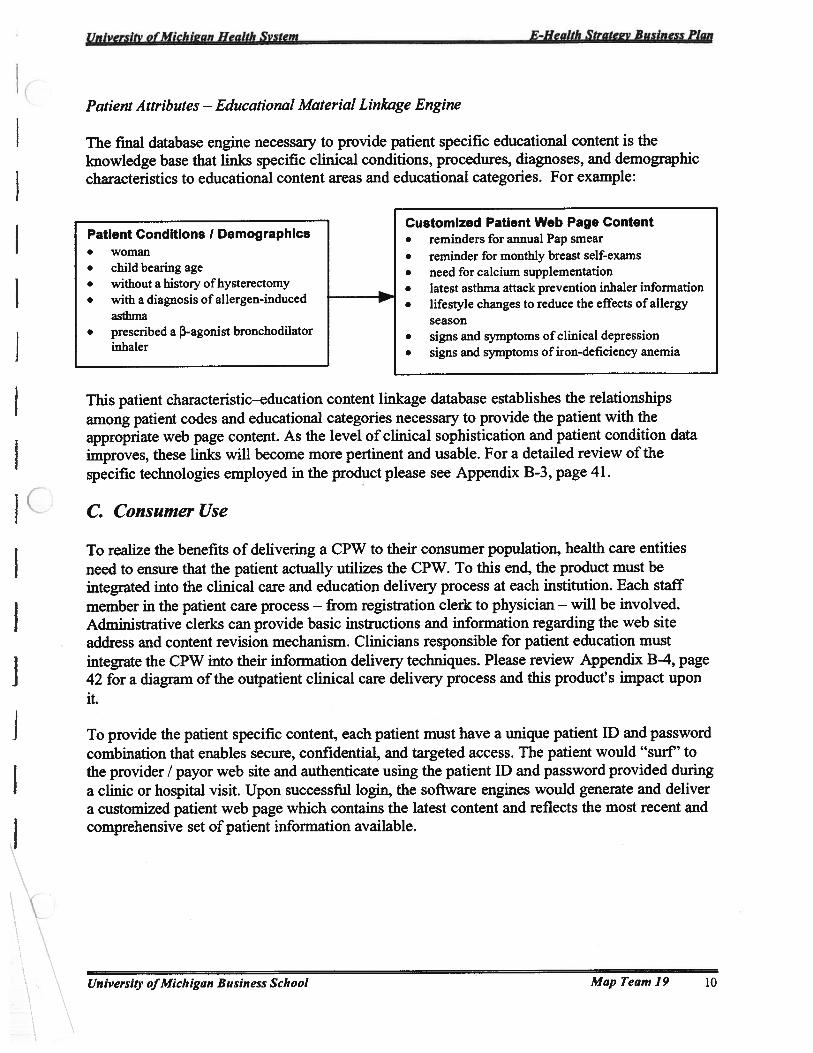
Patient Attributes — Educational Material Linkage Engine
The fmal database engine necessary to provide patient specific educational content is theknowledge base that links specific clinical conditions, procedures, diagnoses, and demographiccharacteristics to educational content areas and educational categories. For example:
This patient characteristic—education content linkage database establishes the relationshipsamong patient codes and educational categories necessary to provide the patient with theappropriate web page content. As the level of clinical sophistication and patient condition dataimproves, these links will become more pertinent and usable. For a detailed review of thespecific technologies employed in the product please see Appendix B-3, page 41.
C. Consumer Use
To realize the benefits of delivering a CPW to their consumer population, health care entitiesneed to ensure that the patient actually utilizes the CPW. To this end, the product must beintegrated into the clinical care and education delivery process at each institution. Each staffmember in the patient care process — from registration clerk to physician — will be involved.Administrative clerks can provide basic instructions and information regarding the web siteaddress and content revision mechanism. Clinicians responsible for patient education mustintegrate the CPW into their information delivery techniques. Please review Appendix B-4, page42 for a diagram of the outpatient clinical care delivery process and this product’s impact uponit.
To provide the patient specific content, each patient must have a unique patient ID and passwordcombination that enables secure, confidential, and targeted access. The patient would “surf’ tothe provider / payor web site and authenticate using the patient ID and password provided duringa clinic or hospital visit. Upon successful login, the software engines would generate and delivera customized patient web page which contains the latest content and reflects the most recent andcomprehensive set of patient information available.
University ofMichigan Business School Map Team 19 10
Patient Conditions I Demographics• woman• child bearing age• without a history of hysterectomy• with a diagnosis of allergen-induced
asthma• prescribed a 13-agonist bronchodilator
inhaler
Customized Patient Web Page Content• reminders for annual Pap smear• reminder for monthly breast self-exams• need for calcium supplementation• latest asthma attack prevention inhaler information• lifestyle changes to reduce the effects of allergy
season• signs and symptoms of clinical depression• signs and symptoms of iron-deficiency anemia

University ofMichigan Health System E-Health Stratev Business Plan
D. Product Benefits
The CPW, a consumer-focused product, actually provides benefits to all participants in thehealthcare delivery process. Thus, it is useful to review the salient benefits to each party:
Patient BenefitsTrustworthy information — The CPW enables patients to access medical informationwhich has been approved by UMHS and their personal physicians. It has been shown that77% of consumers preferred to receive information from their personal physician(FindJSVP Survey). Both the “Block M” and physician stamp of approval lend far greatercredibility than information obtained through third party web sites.
• Usable information — This categorization and digestion of educational content is crucialto providing an integrated educational experience that views the patient as a whole personrather than a list of diseases, conditions or demographic attributes. A patient withdiabetes and asthma needs to review the necessary lifestyle changes to mitigate the effectof their conditions as a whole, not as specific reactions to specific diagnoses.
• Empowerment in clinical care delivery — By actively and continuously participating inthe consumption of personalized medical information, the patient becomes more of anactive partner in the healthcare delivery process.
• Educational reinforcement — It is estimated that patients recall 43% of the informationgiven to them by physicians during clinical visits (Routine, 1999). The Internet providesan unprecedented opportunity to enable patients to access dynamic, individualizedmedical content at any time, thereby increasing their overall retention of information.
• Improved clinical outcomes — There is strong evidence suggesting that better patienteducation will improve clinical outcomes. A study of medication side effect reportingrevealed that informing patients of a medication’s side effect profile would decrease thelikelihood of complaints from 10% to 8% (Journal of Family Practice). In the healthmaintenance activity realm, timely and appropriate mammography screening can reducemortality by 16% in women aged 40-49 (Patient, 1999).
Clinician Benefits• Leverage Internet for patient education — Recent surveys indicate that physicians want
to use the internet to educate patients but do not feel they have appropriate sites available(Healtheon, 1999).
• Increased control over Internet information — A significant proportion of a clinician’seducational effort is expended to integrate and clarify the Internet content acquired by thepatient through third-party sources (Woolliscroft, 1999). 89% of physicians are affectedby Internet educational materials, but only 33% have any control over a web site(Healtheon, 1999).
• Ideal method for reinforcing education— In a survey of primary care patients, 54% ofrespondents would utilize educational tools that reiterated and reinforced informationoriginally offered by their physician (Nathan, 1994).
• More “efficient” use of valuable clinician time — Rather than repeating basic materialseasily delivered through a web page, clinicians will be able to focus their time on trulyintegrative and interactive information during the care episode.
University ofMichigan Business School Map Team 19 11

University ofMichi2an Health System E-Health Sfrate-v Business Plan
• Increased patient satisfaction — National Picker survey data establish that improvingpatient education efforts will directly improve overall patient satisfaction (Picker, 1999).
• Increased patient compliance — Recent studies have affirmed that computer aidededucation resulted in statistically significant increases in medication administrationcompliance and overall outcomes. (Edworthy, 1999)
Medical Institution and Payor Benefits• Increased patient satisfaction— More than 50% of patients that reviewed and discussed
Internet health information with their clinician reported they were more satisfied withtheir treatment as a result (Leaffer, 2000).
• Improved clinical outcomes — As mentioned in the Patient Benefits section, breastcancer detection research indicates that education improves compliance with healthmaintenance activities and treatment plans, which directly improved outcomes.
• Higher patient retention rates — By increasing patient satisfaction and clinicaloutcomes, health care entities will be able to prevent the common “health plan shuffle”.The higher retention rates obviate the expense of acquiring new patients to fill capacity oflost customers. Preliminary UMHS data indicate that for inpatient admissions, the costdifferential between retaining a patient and acquiring a new patient is several hundreds ofdollars (Bruck, 2000).
• Decreased resource utilization — A study by the LifeMasters corporation indicated thateducation alone can directly decrease health system resource utilization.
• More efficient use of clinician time — As mentioned earlier, the CPW will allowphysicians to focus on more complex educational encounters.
• Industry prestige and brand equity
E. Security and Confidentiality
The typical Internet user identifies security and confidentiality as one of the most significantconcerns regarding Internet transactions. The sensitive nature of personal health care raisessecurity concerns to an appropriately high level. Because the web site is provided by the patient’shealth system, concerns regarding communication of sensitive data to third parties is allayed;rather than using “healthinfo.com”, the patient would be using a trusted physician or healthsystem site, “myinfo.umich.edu” for example. The threat of emerging privacy standards such asHIPAA reinforce the critical value of this architecture.
The existing security mechanisms employed for the burgeoning eCommerce industry such assecure sockets layer (SSL) and 128-bit encryption will ensure that data security is notcompromised during electronic transmission from the health system site to the patient’s desktop.At institutions possessing an Internet firewall to ensure authenticated access to internal ITresources, the software engines will communicate securely across the firewall while ensuringeasy access to the consumer. The product will employ emerging security standards andtechnologies as they are developed by health care IT consortiums such as the 11.19 group.
Universii’ ofMichigan Business School Map Team 19 12

University ofMichkan Health System E-HealIh Strate2v Business Plan
F. Copyrights, Patents, and Trade Secrets
Traditionally, the software industry has not employed copyrights and patents as a means ofgaining a sustainable competitive advantage. Courts have previously deemed that user interfacescreens, business logic, and software functionality are not patentable intellectual property eventhough the source code base underlying them may be. However, recent developments in theindustry such as Amazon.com’s successful patent acquisition for the “One Click” shopping carthave raised new opportunities. During the development phase, legal counsel will be retained toinvestigate the patentable intellectual property and processes created by the company.
G. Product Liability
Clearly, the distribution of medical information can involve significant liability exposure. Theseparation of clinical care and instructions from educational material and information isparticularly dubious when the source of the information is the patient’s clinical provider. Thereexists significant legal precedent for this differentiation if the provider employs a proactivedisclaimer describing the educational intention of the content. In addition, an informed consentagreement can protect the health care institution from liability if it specifically addresses the useof the web site as an educational tool rather than clinical care delivery tool.
H. Product Extensions
The first generation CPW will be a launching pad to more a sophisticated and comprehensivepatient web site product line. Transactional functions such as appointment scheduling, medicalbill payment and review, direct physician communication, medication prescription fulfillment arelogical next steps in the maturation of the CPW and have been identified as “version 2.0”features.
New products targeted at a broader market and customer needs will be discussed in the FutureProducts section of this document.
IL Exit Strategy
Due to the rapid pace of development within the high tech industry, speed to market is critical.The profitability of the product is also important to ensure resources for future products. Atimeline of critical deadlines for product development and sales is included in Appendix B-5,page 43.
W. Company Description
A. Nature of the Business
The organization that will develop and launch this product will be a Michigan, for-profit taxablesubsidiary (NEWCO) under Michigan Health Corporation (MHC). NEWCO will be the vehiclethrough which UMHS can develop its eHealth strategy and future sources of revenue related to
University ofMichigan Business School Map Team 19 13

University ofMichiL’an Health System E-HeaJth Strate-v Business Plan
technology and health care delivery. Initially, the business will be responsible for thedevelopment and maintenance of the CPW, including all stages of testing and implementation. Inaddition, the business will market and distribute the product to organizations outside of UMHS.As the product is implemented within UMHS and other organizations, the company will provideuser support and customization as necessaiy. As future product lines develop, the company willbe responsible for all aspects of research, development and distribution. NEWCO will executeeHealth strategic product development in conjunction with Ulvl}{S leadership.
In order to succeed in this market, organizations must demonstrate the following characteristics:• Credible and tnsstworthy content• Direct access to patient clinical information• Brand recognition• User friendly web site design• Technology research and capabilities• Design support• User support• Speed of new products to market• Integration of systems• Support of institutional leadership, including individuals at all levels of the organization• Security of information
B. Distinctive Competencies and Unique Resources
Although NEWCO is independent of UMHS, it will be able to leverage many of the system’sstrengths while mitigating its weaknesses in the development and marketing of the CPW. Someof UMHS’ s competencies and unique resources include:
• Credibility• Direct access to patient data• Enormous base of intellectual capital and well-recognized centers of excellence• Existing Web-enabled clinical content• Leadership support for IT development• Crucial payor perspective of the M-CARE HMO• Access to resources and expertise of other University of Michigan professional schools• Existing technology infrastructure• Software development experience• Centralized clinical data repository• Extensive alumni network
Though the company leverages the strengths of the health system, it will be able to react to themarket more quickly and efficiently than a large academic medical center.
University ofMichigan Business School Map Team 19 14
(Jnlversitv ofMichian Health System E-Health Stratev Business Plan
V. Marketing and Sales Strate!v
A. Potential Customers and Needs Identification
Hospitals, physicians, medical insurance companies (payors) and self-insured companies arepotential purchasers of the CPW (Appendix C-i, page 45). Physicians are important consumersof the product, but we intend to reach them through organizations that are better able to affordour product. In the US, there are more than 6,000 hospitals (Hospitals, 1999) striving to maintainmarket share, increase patient satisfaction, improve clinical outcomes, and increase clinicalefficiency. A hospital market analysis is provided in Appendix C-2, page 46. In addition tohospitals, medical insurance companies and self-insured companies may be interested in thisproduct. There are 651 HMOs and 3,300 medical insurance companies in the United States as of1998 and 1996, respectively (Congressional, 1999; Insurance Handbook). HMOs and insurersare interested in decreasing patient utilization while maintaining the quality of care. Self-insuredcompanies which include many Fortune 100 companies have a similar interest in reducing healthcare risks and costs, improving the health condition of employees and their families, anddecreasing patient utilization.
B. Market Segments and Customer Prioritization
Potential customers can be segmented by category and size. Appendix C-3, page 47, illustrates,.—- market segmentation by size and category. Each segment should be prioritized for efficient and
I effective marketing and sales activities. Possible segment prioritization criteria include:• Size of the market• Potential market penetration level• Prestige of customers• Possibility of referral to other potential customers• Fit with organizational goals
A template for segment prioritization is provided in Appendix C-4, page 48.
Customers within each segment should be prioritized for efficient and effective marketing andsales. Possible customer prioritization criteria include:
• Financial capability• Possibility of continuous partnership• Prestige of customers• Possibility of referral to other potential customers• Fit with organizational goals
A template for customer prioritization is provided in Appendix C-5, page 49.
C. Pricing
A price for the product can be determined by assessing the customer value of the product.Customers of the product receive several benefits. The primary benefits include efficiencies
University ofMichigan Business School Map Team 19 15

nfMb.1.;,,,,.. U,IiI, E-Health Stratev Business Plan
gained from decreased clinicians’ and nurses’ patient education time spent at the point of care,decreased costs of patient cailbacks, reduced volume of triage calls, and potential reductions inthe patient education budget. These benefits can be quantified by estimating time saved at thepoint-of-care, analyzing the costs of triage before and after our product is implemented, andanalyzing patient education budget reports. An additional benefit, which is not quantifiable atthis point, is decreased variable cost per case. Further study on this benefit is important foraccurate product pricing. The most important benefit, however, is the intangible value ofbuilding brand equity through enhanced customer satisfaction. Institutions that introduce thisproduct may be more competitive than others because they are able to change the tide ofmisinformation by controlling information received by patients.
The MAP team identified potential price structures by estimating Economic Value Added (EVA)of primary benefits to the customer. EVA can be measured using three steps.
1. Estimate Total EVA to Customer (See Steps 1,2, 3 in chart below)2. Detennine customization cost per customer, which is equivalent to the variable cost per
license.3. Subtract the license fee (fixed cost), to arrive at customer value
EVA Pricing Method
800
600
$000s400-
—License200
0-— I
Total EVA to Total cost
Assumptions : 50% of first year’s primary benefits charged as the price(1) EVA of reduced physicians’ and nurses’ time spent educating patients(2) EVA of reduced number of triage calls(3) EVA of reduced expenses associated with patient education materials
The MAP team calculated a range of $230,000-$730,000 of customer EVA. Therefore, a price
C range of $120,000- $360,000 is possible based upon the category and size of the customer.Appendix C-6 on page 50 provides detailed calculations of EVA by customer segment.
Customervalue
550(1
Pricing range
‘JrI 60
Customizationcustomer costs
60
University ofMichigan Business School Map TeamI9 16

(Jniversifv ofMichifais Health System E-Health Sfratep-v Business Plan
Therefore, an appropriate pricing model for hospital customers would be:
Maximum Pricing = EVA(education efficiency gain) + EVA(patient callback efficiencygain) + EVA(decreased variable cost per case) + EVA(decrease in cost of patient educationmaterials)
An appropriate pricing model for payors and self-insured companies customers would be:
Maximum Pricing = EVA(decrease of patient utilization) + EVA(decrease in cost of patienteducation materials)
D. Distribution andPromotion
It is critical to understand the decision making process of medical software purchase in hospitalsand other companies in order to market the product. The purchasing process is usually initiatedby a ClO of the organization and finalized by an agreement within the management leadership.Consequently, ClO contact is very important. Another possible point of contact is the healthcarecost manager within a hospital or health system. To gain access to these key decision-makers, thecompany needs a direct sales force. This sales force will be responsible for contacting customers,
C generating Request for Proposals (RFPs), responding to questions from potential customers, anddemonstrating the product at the point-of-sales. The sales force should have or develop specificproduct knowledge, medical knowledge, IT skills and interpersonal skills. The number of salespeople required should be determined by sales projection of the product.
Another distribution option is to establish a partnership with another company. Partnerships aredescribed in a later section of this plan.
Effective promotion of our product requires deep consideration of costs associated withpromotion, ability to reach our target audience, and the degree of push and pull marketingnecessary. There are three main promotion tools in medical software sales practice.
• Medical information technology conferences• Advertising in health care magazines, newspapers, and websites and sponsorships at
medical conferences• Personal referrals citing the benefits of the products (word of mouth)
VL Oranization. Manaementg Ownership and Operations
A. Structure
The company, NEWCO, that will develop and launch the CPW will be established as a for-profitsubsidiary under MHC. The University of Michigan is a public institution, and as a result it issubject to certain restrictions. The MHC was established by the Regents of the University as a
University ofMichigan Business School Map Team 19 17
University ofMichwan Health System E-Health Strate’v Business Plan
vehicle to participate in, coordinate and develop health care related activities to maintain andenhance the educational, research and service missions of the University. Specifically, MHCexists to enable the University to pursue health care initiatives that it would not otherwise be ableto pursue.
The CPW will initially be launched by the eHealth subsidiary, with NEWCO controlling 100%interest in the company. However, as we begin marketing the product to outside organizations,the venture may be spun off into an independent business under the umbrella of the largereHealth subsidiary. This spin-off structure will facilitate partnerships and possible funding.Parties outside of UMHS will have the ability to assume partial ownership in the company. Inaddition, the company will offer two levels of stock options, one with voting rights and onewithout voting rights. MHC may maintain a controlling interest in any of the companieslaunched under it, but this will be decided by leadership based upon individual situations. Thediagram in Appendix D- 1, page 52 illustrates the structure of this entity.
B. Staffing — Product Development
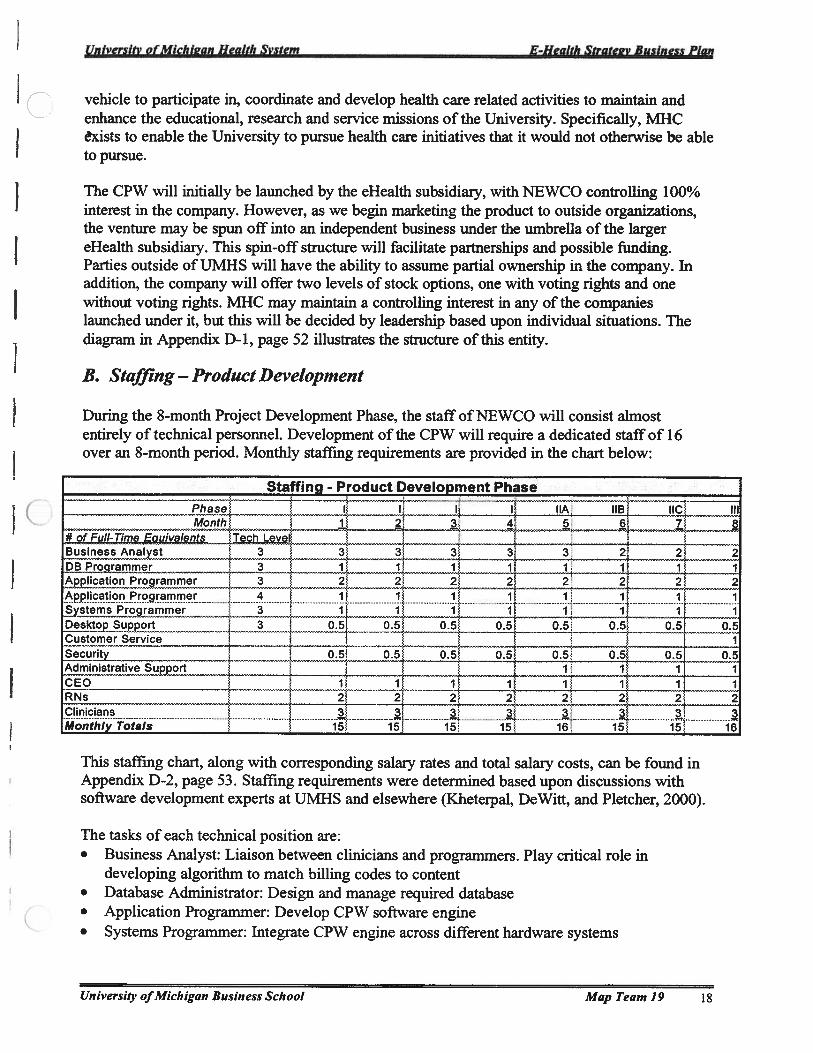
During the 8-month Project Development Phase, the staff of NEWCO will consist almostentirely of technical personnel. Development of the CPW will require a dedicated staff of 16over an 8-month period. Monthly staffmg requirements are provided in the chart below:
Staffing_-_Product_Development Phase
Phase I I I I hA IIB IICMonth 1 2 3 4 5 6 7 8
#9f Full-Time Equivalents Tech Level — — — — — —
Business Analyst 3 3 3 3 3 3 2 2 2DB Programmer 3 1 1 1 1 1 1 1 1Application Programmer 3 2 2 2 2 2 2 2 2Application Programmer 4 1 1 1 1 1 1 1 1Systems Programmer 3 1 1 1 1 1 1 1 1Desktop Support 3 05 05 05 05 05 05 05 05Customer Service ISecurity 05 05 05 05 05 05 05 05Administrative Support 1 1 1 1CEO 1 1 1 1 1 1 1 1RNs 2 2 2 2 2 2 2 2Clinicians 3. 3 3. 3 3. 3 3. 3Monthly Totals 15 15 15 15 16 15 15 16
This staffmg chart, along with corresponding salary rates and total salary costs, can be found inAppendix D-2, page 53. Staffing requirements were determined based upon discussions withsoftware development experts at UMHS and elsewhere (Kheterpal, DeWitt, and Pletcher, 2000).
The tasks of each technical position are:• Business Analyst: Liaison between clinicians and programmers. Play critical role in
developing algorithm to match billing codes to content• Database Administrator: Design and manage required database• Application Programmer: Develop CPW software engine• Systems Programmer: Integrate CPW engine across different hardware systems
University ofMichigan Business School Map Team 19 18

University ofMichk’an Health System E-Health Strate2’v Business Plan
C • Desktop Support: Provide and maintain productivity software for each employee
• Security Expert: Design and implement firewalls and other data security functions to ensure
integrity of data transmitted from host server to patient web site
• Clinician: Work with Business Analyst in providing expertise to match billing codes to
content• RN: Work with Business Analyst in providing expertise to match billing codes to content
• Customer Service: Provide support to test pilot customers and relay feedback to technical
team
C. Staffing — Operations
Staffmg requirements following product development were detennined based upon sales
projections. The number of new clients per year was used to assess the number of FTEs needed
at each functional level during the years 200 1-2005. Software industry standards of the number
of new clients that can be supported by each position were the basis of these calculations, and are
available in Appendix D-3, page 54. The following table lists the yearly staffmg requirements.
Staffing - Operations Phase
2000 2001 2O02 2003 2004 2005
# of Full-TimEowvaIents Tech Levei
Business Analyst 3 2 2 7
Dammer 3 J_AjjonProjarnmer 3 2 3 4
Pppcionfoqrarnn_ 4 ____1 1 2 2
....3 i23J 5 7
Desktopy__ 3 2 3 3
çustomerse_._,
12; 3 4
&.uñtyAdmhiistratjypj__RNs 2. 2 2 2 2
Chnicians 3 3 3. 3 3
CEOCFO 0, 1 1 I I
VP Marketing and S&es :ziztz iTh minessD 1 2 2
Marketing 1 2
Salespeople 2 7
Yearly Totals 16 26 36 49 60
%lncrease 63% 38% 36% 22%
Annual staffmg requirements, corresponding salary rates, and total salary costs are provided inAppendix D-3 on page 54.
D. Incentive Structure
One goal of NEWCO is to encourage UMHS faculty continue to use their knowledge to benefitpatients, the system, and themselves. As a result, the incentive structure is an important aspect of
this plan. Although participants will be offered cash compensation for their content
University ofMichigan Business School Map Team 19 19

University ofMichiL’an Health System E-Health Stratee-v Business Plan
C contributions, a stock option program will also be developed. There are several reasons for
offering such a plan.• “The principle underlying these systems is the use of rewards to create among
employees and management alike a shared sense of identity, commitment, and goalsfor the organization.” (Wilson, 1995)
• Physicians and other contributors will have reason to continue to participate in thelong-term development of content and applications
• Compensation for work will be competitive with consulting offers from organizations
such as Medscape and WebMD
Recognizing the support of physicians, nurses, clinical and non-clinical staff within the healthsystem will be critical to the success of the product, all UMHS employees will be offered
restricted stock options, regardless of their role in the development or use of the product. Theseoptions will not have voting rights. The purpose of this offering is to initiate support for theproduct as it is developed. Option packages will vary depending on the employee’s position
within UMHS.
During the product development phase, physician participation will be crucial to the product’ssuccess. We will offer the option of cash compensation, at approximately $250 per hour3,or
nonqualified stock options for consulting services (Miller Canfield Presentation; Brock, 2000).
f The nonqualified stock options will be available to individuals after they have completed aspecified service to the company. Ideally, NEWCO will recruit one physician from each
C department to assist with the development of appropriate content links. This can be facilitatedusing one of two methods. The first option is to recruit a representative from each department towork on the project for a certain percentage of their time designed to UMHS. This time will not
be considered consulting time. The second option is to employ the department representatives as
J consultants and require them to designate their four days of consulting work per month to the
development of the product. Nurse educators acting as consultants in the development phase willreceive similar stock options.
After the product has been developed, NEWCO will need ongoing support for contentdevelopment. An advisory board will be established to review future content and evaluate new
product lines. The advisory board will consist of five physicians from the original contentdevelopment team (department representatives), consumer representatives, and other individualsfrom inside or outside of the health system as deemed appropriate by company leadership. Theadvisory board will be rewarded with voting stock options consisting of approximately 10%-20% of the total stock. Physicians who continue to generate content for the site will becompensated with cash ($250 per hour) or restricted, non-voting stock options, based upon theirpreference.
Finally, individuals involved with the development of the product will be acknowledged inproduct descriptions included with the software package. However, individual names will not beattached to content segments. Clinicians are frequently involved in ventures that serve to provide
This is competitive with Oncology.com feesBased on Miller Canfield presentation regarding industry standards
University ofMichigan Business School Map Team 19 20
University ofMichi2an Health System E-Health Strate-v Business Plan
higher quality patient care, even if no personal financial reward is obtained. NEWCO will
provide an option for individuals to gain this job satisfaction while working within the UIvIHS.
It is important to avoid incentive structures that override the faculty’s primary obligation to theUniversity for research, education and care delivery. The current structure allows faculty toparticipate in ventures similar to NEWCO that are outside of the University. The proposed
incentive structure will incent faculty to help support UMHS’s missions.
Future questions that NEWCO will need to address include:• What will individuals pay for their shares? ($.0l or a price close to the IPO)
• How long until the shares are vested?• What happens if the company is sold?
E. Partnershzvs andAiiances
Partnerships and alliances are important to build relationships with potential customers andimprove effectiveness of business processes. While NEWCO possesses the necessary resources
to achieve specific business goals, it may not be equipped to handle the project the most efficientway possible. For the CPW product, three functional areas categorize potential partners: (1)marketing and distribution, (2) content production, and (3) development and implementation.
The advantage of marketing and distribution partnerships is to improve the effectiveness of sales
a (1 and build relationships with potential partners. This should be done while building the brand
j recognition and the reliability of the product. This is important in the CPW because of themarketing strategy of selling to health systems and third party payors (such as self-insured
companies) on a national basis. Potential partners include companies with an established
foothold in the healthcare technology market, such as pharmaceutical companies, EMR software
companies, medical content providers, and medical device companies. Marketing and
distribution partners would provide specific capabilities such as funding for promotion and
distribution, skilled salesforce, and most importantly, a connection to their established customerbase.
Content development partnerships could provide a useful way to tap into the existing base ofWeb-enabled medical content. While the majority of this content is general in nature, it couldprovide a basis for the CPW database. Additionally, the increase in knowledge through theinclusion of another content source could create synergies to provide NEWCO with more usefulinformation. Potential partners for content development are WebMD, Medscape, and DrKoop.These companies were selected based on their established presence in eHealth and history ofdistinguishing themselves through content, credibility, and infrastructure. However, a keyresource of UMHS is its faculty. The enormous amount of clinical knowledge available withinUMHS and that which afready exists within the UMHS data warehouse does not create animmediate need to pursue content partnerships (Hampton, 2000). Furthermore these companiesare unfavorable because they do not desire exclusive AMC alliances (Medscape, 2000).
The inclusion of a development partnership is aimed at reducing risk and improving the speed ofdevelopment. Technology based products and services must address the issues of time-to-market
University ofMichigan Business School Map Team 19 21

University ofMichiean Health System E-HealIh Strate-v Business Plan
as well as unique design capabilities. The CPW is a product that will be intricate in both itsdesign and capabilities. In order to fully enable UIvIHS to compete in this new market, it may benecessary to form a partnership an&or alliance with a technology or Internet software company.This option is being considered for numerous reasons, mainly issues concerning productdevelopment and implementation efficiency and the need for technological expertise. UMHSprovides value through its core competencies and key resources, namely its ability to providecredible healthcare content and access to its faculty. However, the potential value added from apartner could be two fold: technology and development expertise as well as security expertise tomaintain patient confidentiality and regulatory compliance. This type of partnership is necessaryin the early stages of implementation in order to achieve UMHS’s ultimate goals.
In order to explore the partnership/alliance option we have researched seven companies.Companies were selected on the basis of reputation, performance, and potential growth. In thecategory of potential product development partnerships i2 Technologies, Aspect Development,Ariba, and Commerce One have been analyzed. In the security partners realm, Entrust, yen Sign,and Baltimore Technologies (which recently acquired GTE Cybertrust) have been considered(Baltimore, 2000). Brief overviews of each company, comparative performance analysis, andpartnership recommendations can be found in Appendix D-5, page 57.
Product Development Partners
In order to consummate a beneficial development partnership, NEWCO will select a company
( that possesses specific capabilities. These include sufficient funding resources and developmentexpertise that will produce synergies through increased knowledge and development timeefficiency. i2 Technologies’ size and experience (established in 1988, i2 Technologies currentlyhas approximately 2800 employees) makes it the most attractive development partner forNEWCO (Hoovers, 2000).
The acquisition of Aspect Development and the alliance established with Ariba have solidified i2Technologies’ leadership position in the software industry (Aspect, 2000; MSDW, 2000). This,along with its illustrated growth (it is expected that they will sustain annual revenue growth of50% through 2005), has positioned it as the leading potential partner for UMHS in the productdevelopment of the CPW (Hoovers, 2000).
Security Partners
Entrust and VeriSign are the leading competitors in the security side of our partnership analysis.They employ two different business models: VeriSign utilizes a service model and entered themarket with a focus on the consumer. Entrust maintains a licensing model focusing on theenterprise but is expanding its offerings to include outsourced services. VeriSign is offered at ahigh premium over Entrust, and it is believed that this premium is unwarranted (Goldman Sachs,1999). This phenomenon may lead VeriSign to future instability. Additionally, Entrust’srevenues are growing faster than VeriSign’s and the revenue stream is more diverse (GoldmanSachs, 1999). These factors, when combined with their established healthcare presence, has ledus to recommend Entrust as the leading candidate for a security partnership (Entrust, 2000).
University ofMichigan Business School Map Team 19 22

University ofMichk’an Health System E-Health Stratev Business Plan
It is unclear as to whether or not a second alliance with a security partner for the development of
a co-branded product is necessary. Many of the software development firms have securityprecautions as an aspect of development. This avenue should be explored.
Potential Development Partner Analysis
Company Product/Service FE 1999 Revenue 12-month OverallAttributes ($ millions) Growth Assessment
i2 Technologies • General collaborative 571.1 57.8% +-t
solutions for B2BeCommerce
Aspect • Software 95.1 10.1% +++
Development development• Provision of
efficiencies ofprocurement, design,operationsmanagement, and thesupply chain
Ariba • Global eMarkets 45.4 1024.0% ++
Commerce One • Global eMarkets 33.6 1192.3% ++
Entrust • PM Technology 85.2 73.9% ++++
solutions• Digital certificates
VeriSign • Digital certificates 38.9 118.0% ±+++
Baltimore • Computer and 30.0 -H-
Technologies network securityservices
Companies in bold are highly recommendedforpartnershipPlus signs (+) on a scale of 1 to 5) denote the increasing level ofquality respective ofreputation, performance, and
potential growth‘‘ Information not availableOverall Assessment is based on information provided in Appendix D-5, page 57.
VIE Future Products
NEWCO will utilize the core competencies, customer information, and distribution channelsgained from the development and implementation of the CPW to launch future products. Theproducts to be developed, in chronological order, are:
• Physician Information Web Page• Decision Support System• Continuing Medical Education (developed in conjunction with JIT)
• Just-in-Time (JIT) Education (developed in conjunction with CME)
University ofMichigan Business School Map Team 19 23
University ofMichigan Health System E-Health Stralei’v Business Plan
The following are summary descriptions of NEWCO’s future products. Each summary describesthe product and the related synergies for previously developed products. For an overview ofproduct synergies based on core competencies, customer information, and distribution channels,see Appendix E- 1, page 61.
A. Physician Information Web Page (P1W)
The Physician Information Web Page (P1W) will be the second product launched by NEWCO.The P1W is similar in nature to the CPW in that it proactively “pushes” necessary information tothe customer, the physician. This product will be capable of delivering new drug information,latest breaking medical news, institutional concerns, and CME information. If the purchaserchooses to integrate the P1W with the CPW, the information will be able to help physicians innew ways such as informing them of cost differentials among pharmaceuticals or highlightingpatient concerns based on patient Web behavior.
B. Decision Support System
The Decision Support System will support clinicians’ diagnoses and treatment decisions byproactively providing information based on patient symptoms and diagnoses. Building upon thesoftware development skills and the learning experience of both the CPW and the P1W, NEWCOcan create a database driven Decision Support System that will be used as a tool by physicians
(. and their support staff. This product will compete directly with MDConsult but will have theadvantage of being able to “leap frog” the competitors’ technology and content. The DecisionSupport System will aggressively gain market share by utilizing distribution channels set up withprevious products. The product will incorporate UMHS patient care guidelines in its software aswell as drug and reference databases. It will be sold to hospitals and health systems for use byRNs, PAs, and other health professionals in triage decisions. Physicians will be targeted at thepoint of care once the system is validated.
C. Continuing Medical Education
CME programs have been ineffectively impacting physician behavior and are currently offeredfree of charge in many formats. There is an opportunity to generate revenue by developingCMEs that actually change physician behavior. The current lack of physician response to CMEsis due to the manner in which the CME has traditionally been delivered. Various studies haveshown that interactive CME courses, especially courses held over multiple periods, have hadpositive outcomes on physician performance (Davis, 1999). Utilizing concurrent developmentsof the MRT, the Visible Human, and MT Education, NEWCO can impact the way CMEs aretaught and fill the market need for superior CME.
D. Just-in-Time Education
Just-in-Time Education is the next natural progression from Decision Support Systems. Thedifference between the two products is that while Decision Support Systems can assist at thepoint of care for 80% - 90% of a physician’s cases, it is limited mostly to primary care and
University ofMichigan Business School Map Team 19 24

Iiniuorvitv nf PJipI, ionn I-IpnIWI, cvcii’n F..Th’i,Iiii .iraIpoi, R,,cinjicc Plnn
known clinical situation. Just-in-Time Education is the link between cutting edge research and
physicians at the point of care, involving everything from what to do in the case of rare druginteraction side-effects to reinforcing new diagnostic techniques learned in a CME course.
These four products will take advantage of concurrent developments already underway in the
realms of distance education and telemedicine, culminating in the advancement of telecare (see
Figure 7-1). Whereas “telemedicine” can be defmed as cost-effective examples of tele-radiology,
tele-consulting, and tele-disease management, “telecare” is seen as the advancement of these
areas which are currently limited by infrastructure feasibility and cost / reimbursement issues.
However, telecare is not only limited by infrastructure and reimbursement. Patient acceptance
and provider familiarity with technology are two obstacles that could slow the acceptance of
telecare. As the infrastructure for telecare becomes more ubiquitous, organizations that already
have a presence in health technology will be the first to gain acceptance with patients and
providers. It is due to these behavioral factors that NEWCO’ s future products will facilitate the
acceptance of UMHS as a premiere telecare provider.
f)istanccEducation
I.— 1)ecisiin
cp’v = —0
.1
___
Figure 7-1: The advancement of products to telecare
VIEL Performance Metrics
To evaluate the success of our product and company, it is necessary to defme and implement
specific performance metrics. This is particularly important because performance measures
gathered during the product’s use at UMHS can be used to market the product to potential
customers.
Performance Measure Method of Measurement Notes/CommentsIncrease in Patient Picker Surveys — comparison of scores Recent UM surveys indicate that informationSatisfaction before and after implementation of and education is highly correlated with
CPW overall patient satisfaction• 49% of patients indicated that they did
not get enough info aboutconditionltreatment
• 30% of patients indicated that they did
Telecare
University ofMichigan Business School Map Team 19 25
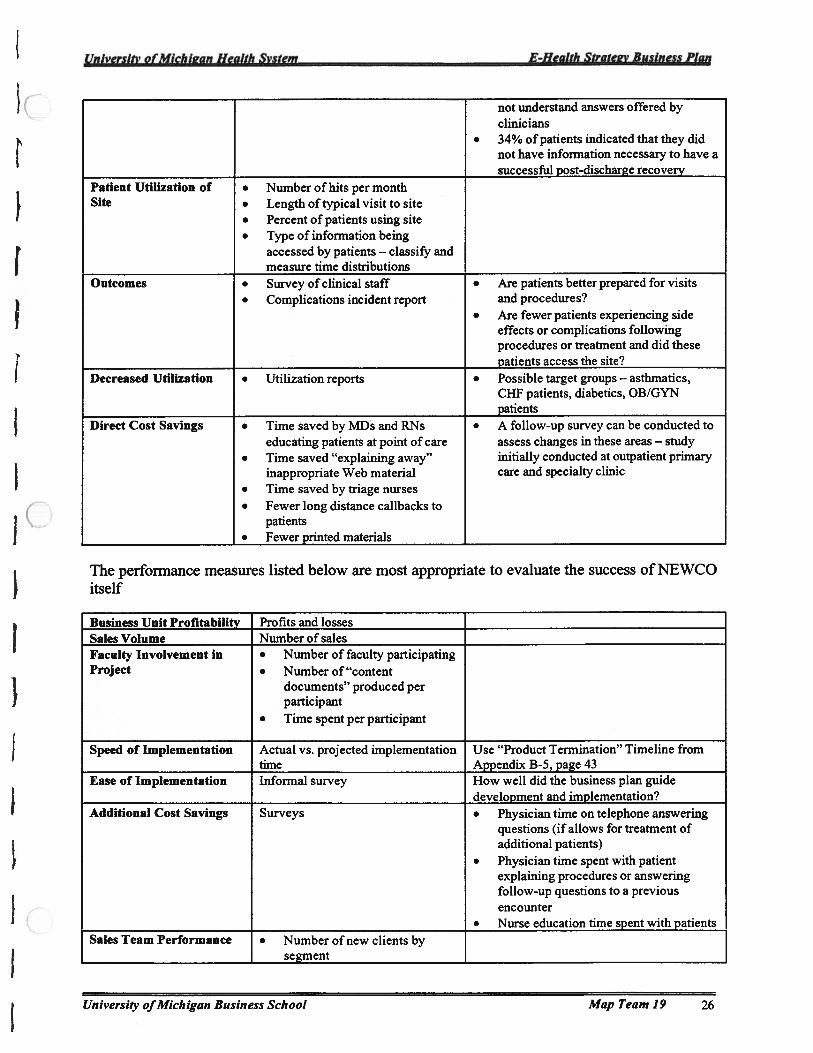
University ofMichigan Health System F-Health Stratev Business Plan
not understand answers offered byclinicians
. 34% of patients indicated that they didnot have information necessary to have asuccessful_post-discharge_recovery
Patient Utilization of • Number of hits per monthSite • Length of typical visit to site
• Percent of patients using site• Type of information being
accessed by patients — classify andmeasure time_distributions
Outcomes • Survey of clinical staff • Are patients better prepared for visits• Complications incident report and procedures?
• Are fewer patients experiencing sideeffects or complications followingprocedures or treatment and did thesepatients_access_the_site?
Decreased Utilization • Utilization reports • Possible target groups — asthmatics,CHF patients, diabetics, OB/GYNpatients
Direct Cost Savings • Time saved by MDs and RNs • A follow-up survey can be conducted toeducating patients at point of care assess changes in these areas — study
• Time saved “explaining away” initially conducted at outpatient primaryinappropriate Web material care and specialty clinic
• Time saved by triage nurses• Fewer long distance cailbacks to
patients• Fewer printed materials
The performance measures listed below are most appropriate to evaluate the success of NEWCOitself
Business Unit Profitability Profits and lossesSales Volume Number of salesFaculty Involvement in • Number of faculty participatingProject • Number of “content
documents” produced perparticipant
• Time spent per participant
Speed of Implementation Actual vs. projected implementation Use “Product Termination” Timeline fromtime Appendix B-5, page 43
Ease of Implementation Informal survey How well did the business plan guidedevelopment and implementation?
Additional Cost Savings Surveys • Physician time on telephone answeringquestions (if allows for treatment ofadditional patients)
• Physician time spent with patientexplaining procedures or answeringfollow-up questions to a previousencounter
• Nurse education time spent with patientsSales Team Performance J. Number of new clients by
j segment
University ofMichigan Business School Map Team 19 26

University of_Michi,an Health System -
E-Heaith Strate.v Business Plan
. Revenue generated
. Sales cycle time
. Sales budget management
(Budget vs. actual)
• Number of total clients
managed
Marketing Team • Marketing budget management
Performance (Budget vs. actual)
• Advertising/promotion
efficiency
•Reach
• Recognition
. Callback ratio
Synergy with UilRS Surveys to patients, nurses, • Does this help us to provide better
Mission physicians, other staff, students, patient care?
Picker surveys • Does this assist us with our educational
mission?
• Does this allow us to provide higher
quality research? (This is difficult to
measure initially, but continued
refinement of central data repository will
improve research possibilities)
IX. Funding Requirements
A. Current Funding Requirements
The CPW will first be developed and implemented at IJMHS through NEWCO. The currentestimated funding requirement is approximately $1.6 million, and the development period is
projected to take place over 8 months, beginning July 1, 2000 and ending March 1, 2001.
The costs of development are comprised of three primary components: salaries (70%), hardware
and software (18%), and other general and administrative costs (12%). Salary expenses will fund
the 16-person staff of software developers, clinicians, RNs and a CEO (see Organization:
Staffmg.) Hardware and software costs consist of a large development server, workstations, andapplication development, productivity, security and database software. Other general and
administrative consist of standard office expenses, such as rent, utilities, supplies, and
legal/accounting fees.
The CPW will be developed in three phases:
• Phase I — software development (59% of total development costs)
• Phase II — test/pilot (31% of total development costs)
• Phase III — launch/implementation (10% of total development costs)
Further information on the phases of product development can be found in Section III, Proposed
Product and Service. A summary of development costs is provided in Appendix F-2, page 65,‘c- and a detailed monthly breakdown in Appendix F-3, page 66.
University ofMichigan Business School Map Team 19 27

University ofMichigan Health System E-Health Strate2i’ Business Plan
Funding for the $1 .6M development of the CPW will come from UMHS as well as other
potential equity investors in NEWCO. NEWCO will explore the possibility of partnering with
fmancial andJor strategic investors to provide additional capital and strategic benefits. See the
Partnerships and Alliances section for further discussion on potential partners.
B. Funding Requirements Through 2005
Following implementation at UMHS, the CPW engine will be packaged, sold and implemented
at other customer sites. It is also assumed that NEWCO will embark upon research and
development to further enhance the CPW and develop new products (See Section VII, FutureProducts). All of these efforts will require an increase in staffmg, as well as operating expenses
(research and development, sales and marketing, and general and administrative costs). Staffingprojections can be found in the Staffing - Operations section. Operating expenses are projected to
increase as follows:
• Research and Development: $500,000 in 2001 to $4.5M in 2005 (CAGR of 73%)
• Sales and Marketing: $658,000 in 2001 to $7.1M in 2005 (CAGR of 79%)
• General Administrative: $2.0 M in 2001 to $7.6M in 2005 (CAGR of 40%)
In order to meet future funding requirements, NEWCO will use its own funds and continue
exploring the possibility of raising funds through private placements of capital. Outside investorswill be selected based upon their fmancial strength and ability to strategically benefit NEWCO in
key areas such as product development, distribution, and content creation.
C. Long Range Financial Strategy
Beyond 2005, NEWCO will continue to fmance the firm’s business activities through its own
funds as well as those of fmancial and strategic partners. NEWCO will explore raising additionalcapital through subsequent rounds of private placements, public offerings of stock, and
acquisitions of cash assets. NEWCO’s long range fmancial strategy is dependent upon a numberof factors, including:
• products selected for future development• nature of the markets in which these products are sold• financial and strategic partnerships negotiated in the near and medium-term
• condition of capital markets in the future
University ofMichigan Business School Map Team 19 28

Universiti’ ofMichk’an Health System E-Health Stratev Business Plan
X. Financial Projections
A. Assumptions
NEWCO’s fmancial projections were developed based upon the following assumptions.
The development phase will require $1.6 million in funding over an eight month period, with a16 FTE staffmg. For detailed explanations and bases for these assumptions, please reviewAppendix F-i, page 64:
The operations phase assumptions are described below:
Item Assumption Basis of AssumptionTypes of Customers Large (>500 beds) and small MAP team market analysis. See
(100-300 beds) medical Section II. B., Target Market Analysisinstitutions, medical insurance for discussion of target marketcompanies, and self-insured segments.companies
Revenues:# Licenses Sold Equivalent to 20% market MAP team estimate of market share
share of large customer penetration.market, and 10% of smallcustomer market
# Customization Sold Equivalent to # licenses sold Each software license must becustomized to integrate properly intoclient infrastructure.
# Maintenance Sold Equivalent to # licenses sold NEWCO must provide each customerwith maintenance support.
# Content Modules Sold 20% of large customers buy MAP team estimate.content modules; 50% of smallcustomers
Price of License $300K -- large customer; MAP team assessment. See Economic$1 00K -- small customer Value Added (EVA) analysis in
Section V. C.Price of Customization $60K — large customer Software industry estimate based upon
$20K — small customer price of license.Price of Maintenance 15% of License Fee Software industry estimate based upon
price of license. Includes annualcontent updates, software updates andbug fixes.
Price of Content 10% of License Fee Software industry estimate based uponprice of license.
Expenses:Cost of Goods Sold 20% (primarily for sales Software industry average
commissions)
University ofMichigan Business School Map Team 19 29

1i,dmrciEi, nfAfi,’hk,nn 1lnIth Svctm F-IIpiilfIi fra1,ov Rz,.cina’cv P1,,,,
Research & Development 20% of new license revenues Software industry average
Sales & Marketing 20% of total gross revenues Software industry average
General & AdminStaffmg Needs Most positions are based on Software industry estimate of number
number of FTEs, per function, of clients that can be supported by eachneeded to meet sales position.
projections. See Appendix D3, pages 54-5 5 for assumptionper staffmg function.
Salaries See Appendix D-3, pages 54- Market salaries for software developers55 as determined by UMHS Ernst &
Young consulting study. Salaries for
other positions based upon currentmarket rates.
H/W and S/W Costs See Appendix F-4, page 67 Current market costs for required HJWand S/W. Annual H!W maintenancefees are 10% of original purchase price.New H!W and S/W purchased every 2years.
Other G&A Costs See Appendix F-4, page 67 Current market rates for these items.Includes various categoriessuch as rent, utilities, officesupplies, legallaccounting fees,
and fees paid to clinicians forcontent
Taxes 40% Corporate tax rate.
Discount Rate (for 15% Best estimate of return on alternative
purposes of calculating investment.
IRR and NPV)
B. 5-Year Projections
NEWCO is expected to achieve a 77% Internal Rate of Return and Net Present Value of $4.9Mbased upon projected cash flows through 2005. Projected revenues, expenses, net income, andcash flows are indicated in the table below. Detailed fmancial projections (income and cash flow
statements) can be found in Appendix F-5, page 68.
SUMMARY INCOME AND CASH FLOW STATEMENTS ($)
2Q1 22Net Revenues 2,925,000 6,108,000 11,172,000 19,599,000 30,930,000Operating Expenses 3,167,775 5,973,648 9,005,748 13,623,726 19,170,944Taxes 823.132 2.390.110 4.7O3.22Net Income (242,775) 134,352 1,343,121 3,585,165 7,055,434Cumulative Cash Flow (1,865,973) (1,731,621) (388,501) 3,196,664 10,252,097Project Investment 1,623,198Project NPV 4,919,754Project IRR 77%Discount Rate 15%Payback Period 3 years
University ofMichigan Business School Map Team 19 30

I
I
IIIII
SISAJVNV1Dfl{VT”
Viiiiuv
IIj
)

Appendix A-i: Technical Demands of Health-Related Applications of the Internet
Application Area Bandwidth Latency* Reliability Security UbiquityConsumer Health ++ + ++ ++++ ++±+Clinical Care ++++ +++ ++++ ++++ ++Health Care + + +++ +++-1- ++FinancingPublic Health + + +++ +++ ++Health Education +++ ++ ++ + +++Biomedical ++++ +++ ++ ++ ++Research
* Latency is the time requirea to transmit data across the network (i.e., the delay between a sender transmitting amessage and a recipient receiving it)Note: Plus signs (+) denote the relative importance of the technical feature within the designated application area. Asingle plus sign denotes minimal importance; four plus signs signif’ great importance.’
Appendix A-2: Competitive Analysis - Players
Competitive Analysis of the Consumer Information Market
Tier5 0
—.—.—.,
Tier 4 0: Medscape,
Ø.. .•:.
Tier 3 Companies offering individual produMedivation, lDXlChannelHealtb, Cerne
Tier 2 Other AMCs: Mayo, JohnsHopkins, Duke
Other AMCs withTier 1 individualized product:
NONE
Computer Science and Telecommunications Board, National Research Council. Networking Health: Prescriptionsfor the Internet. Prepublication Copy. National Academy Press, Washington, DC. 2000.
32

Appendix A-3: Competitive Analysis - Tier 4 Competitors
. Player Strengths •P0SSibl Future‘
Actions
Healtheon/ . Growing brand ubiquity . Yet to deliver . Integrates fillyWebMi) • Financial resources on promise of with Healtheon
• Strong partnerships connecting and corrals traffic. Astute deal-making patients and based on extensive
expertise physicians service offerings. Editonal staff with online . Acquires disease-
medical credentials • Not integrated specific and• Premier placement on well physician-focused
Yahoo! and MSN sites to grow. OnHealth acquisition offering
rounds out weilnessoffering and expandsaudience reach
. Provides medicalinformation toconsumers, doctors, andmsurance compames
. Also providing “backoffice” transactionprocessing services forphysicians
DrKoop.com . Strong medical brand . Challenge to • Forms affiliations::.. through Dr. C Everett separate with best-of-breed
Koop drkoop corn the transaction players. Premier placement on site from and content sites
AOL Drkoop the with strong• Co-branded content physician medical ties like
syndication with local • Slow to cut Mayo Clinic and• health centers deals Intellthealth — will
• SMS deal provides • Unstable still need toaccess to 2000 additional financial struggle to catchhealthcare organizations position up with WebMD
. sponsored by many of . Financiallyregional hospitals and unstablehealth insurancecompanies
Mediconsult • Acquisition of • Brand and • LeveragesPhysicians (POL) gives traffic strategy physician base ofaccess to doctors and dependent on POL.subscription revenue slow-to-adopt • Augments brand
• Visitors stay long and physicians through partners
33

• Brand credibility ofseven charter medicalassociations
• Trusted brand fordoctors
• Strong medicalmanagement
• Partnerships withmedical publishers andconference writers
• Provides clinicallyrelevant content tophysicians and othertypes of healthcareproviders
• Currently 300,000physicians useMedscape, 60% in theU.S. and 40%internationally
• Site has approximately30 specialty areas, 21 ofwhich have to do withmedical specialties
• Staff of medical writerswho produce the contentfor the site. 45physician-side writersand 35 consumer-sidewriters.
• Solidifiesphysician andassociationpartners
• Medscape expectse-commerceactivities, andconnectivity toserve as growthareas forMedscape’sprimarily content-driven business.
• In e-commerce,Medscape haspartnered withMedsite (a medicalbook publisher)and Drugstore.comto develop thisbusiness activity.Medscape foreseespartnering withmedical supplycompanies in thefuture as a furtherstepinthisdirection.
• Recent mergerwith MedicaLogicand F-Med willenable Medscapeto connect morephysicians.
visit often • Brand is weak like CBSHealthwatch andDiscovery HealthMedia
Medem • No site launchuntil mid-2000
• Board lacksinternetexperience
• Unstablefinancialposition
• Much revenuederived fromadvertising —
may be risky infuture
34
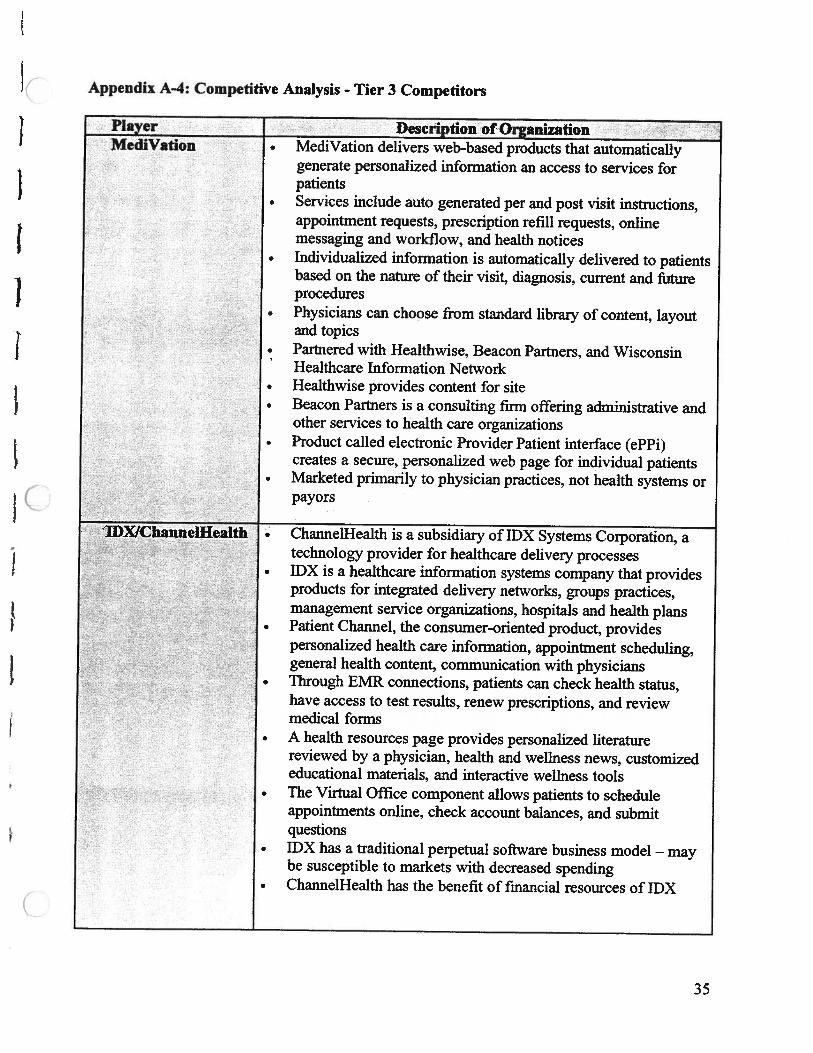
Appendix A-4: Competitive Anaiysis - Tier 3 Competitors
Player Description of OrganizationMediVation • MediVation delivers web-based products that automatically
generate personalized information an access to services forpatients
. Services include auto generated per and post visit instructions,appointment requests, prescription refill requests, onlinemessaging and workflow, and health notices
. Individualized information is automatically delivered to patientsbased on the nature of their visit, diagnosis, current and futureprocedures
• Physicians can choose from standard library of content, layout: and topics
. Partnered with Healthwise, Beacon Partners, and WisconsinHealthcare Information Network
• Healthwise provides content for site• Beacon Partners is a consulting firm offering administrative and
other services to health care organizations. Product called electronic Provider Patient interface (ePPi)
creates a secure, personalized web page for individual patients. Marketed primarily to physician practices, not health systems or
payors
IDXlChannelHealth • ChannelHealth is a subsidiary of IDX Systems Corporation, atechnology provider for healthcare delivery processes
• IPX is a healthcare mformation systems company that providesproducts for mtegrated delivery networks, groups practices,management service organizations, hospitals and health plans
. Patient Channel, the consumer-onented product, providespersonalized health care mformation, appomtment schedulmg,general health content, commumeation with physicians
. Through EMR connections, patients can check health status,have access to test results, renew prescnptions, and reviewmedical forms
• A health resources page provides personalized literaturereviewed by a physician, health and weliness news, customizededucational materials, and interactive weilness tools
• The Virtual Office component allows patients to scheduleappointments online, check account balances, and submitquestions
• IDX has a traditional perpetual software business model — maybe susceptible to markets with decreased spending
• ChannelHealth has the benefit of financial resources of IDX
35

Cerner Corporation Company Information• Cemer designs, develops, markets, installs and supports patient-
focused clinical and management information systems andservices throughout the health care industry
• Products can automate processes within individual clinicaldisciplines or link all aspects of an integrated health system
• Approx. 2,600 employees• Second largest shareholder of Healtheon• Application architecture is called Health Network Architecture
(HNA) which allows health care organizations to streamlineoperations, use EMRs, and reduce costs through efficiencies
• Building a presence overseas (5% of sales from outside the US)• Expected revenue for quarter ending June 2000 $87 million, and
gross margins are expected to be 79%, reflecting a higher mixof services an software in the quarterCompleted several successful implementations of HNAMillennium applications
• History of products that connect hospitals to insurance systems,phannacies and other health care parties
• Strong history of developing information systems• Contracts with approximately 1,100 hospitals worldwide for
• products• • Lower capital spending by health systems may negatively
• impact Cemer in future years
lQHealth — consumer-oriented product line• Individualized web site product produced under IQHealth,
Cerner’s consumer brand. Through IQHealth, consumers can:• Interact with physicians online• Track health information• Complete health assessment surveys• Access medications information• Track appointments and activities• Update personal health information• Pocket PowerChart allows clinicians to access patient data
_____________________
through personal_digital_assistants_(PDAs)
36
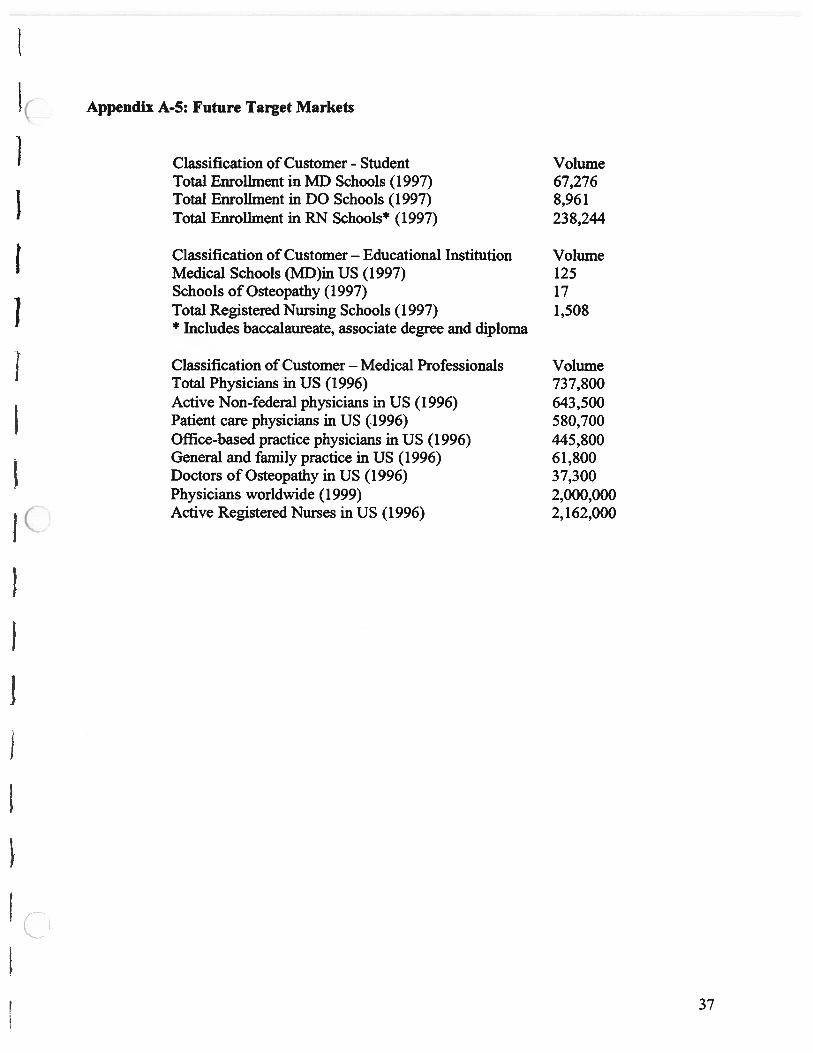
Appendix A-5: Future Target Markets
Classification of Customer - Student VolumeTotal Enrollment in MD Schools (1997) 67,276Total Enrollment in DO Schools (1997) 8,961Total Enrollment in RN Schools* (1997) 238,244
Classification of Customer — Educational Institution VolumeMedical Schools (MD)in US (1997) 125Schools of Osteopathy (1997) 17Total Registered Nursing Schools (1997) 1,508* Includes baccalaureate, associate degree and diploma
Classification of Customer — Medical Professionals VolumeTotal Physicians in US (1996) 737,800Active Non-federal physicians in US (1996) 643,500Patient care physicians in US (1996) 580,700Office-based practice physicians in US (1996) 445,800General and family practice in US (1996) 61,800Doctors of Osteopathy in US (1996) 37,300Physicians worldwide (1999) 2,000,000Active Registered Nurses in US (1996) 2,162,000
37

Appendix B
PROPOSED PRODUCT AND SERVICE
38

App
endi
xB
-i:
Ove
rvie
wof
CP
W
Sea
rch
engin
e•D
isea
se•l
nfo
Sourc
e•T
reat
men
t
Pat
ient
Info
:•N
arne
•Pat
ient
#
Bre
akin
gN
ews
•You
rdis
ease
•Gen
eral
Hea
lth
New
sI
UM
HS
New
s
Lif
lkto
oth
erS
ites
My
med
ical
info
•You
rdia
gnosi
s•Y
our
trea
tmen
t•Y
our
med
icin
e
Mes
sage
from
your
Dr.
Wha
tsh
ould
Ido?
•This
mon
th•T
his
wee
k•T
oday
Dis
clai
mer
39

——
——
*
App
endi
xB
-2:
Det
aile
dP
rod
uct
Map
Ce
——
S—
_-_
_*
—-
Eng
ine
•In
tegr
atio
nC
ust
om
ized
•C
usto
miz
atio
nP
atie
nt
•S
earc
hW
eb-D
ade
•Li
nk
I
UM
HS
pro
duct
IIu
M
IIA
vail
able
atan
y
I:.S
houl
dbe
dev
eloped
inm
ost
of
the
ho
spit
als
40

Appendix B-3: Technical Architecture
The technical leadership of the proposed business entity will determine the specific technicalarchitecture and platform utilized. However, the range of options available is limited and will beaddressed here.
Industry standard communication protocols will be employed to establish the interface fromexisting client-specific reimbursement databases to the common clinical condition database usedby the software engine. Current standards include the health level 7 (HL7) 2.5 specification andthe emerging extensible markup language (XML) healthcare data type defmition (DTDs). Theseprotocols are already used by the vast majority of health care institutions through an intermediary communication hub. They can acquire all necessary patient data including, but notlimited to:• demographics (age, gender, ethnicity)• diagnoses, procedures, and diagnoses groups• laboratory tests• medication and treatment orders
The interface engines will be developed in accepted third-generation languages (3GL) such asC++ that posses proven performance capabilities. Storage of the acquired data will be inindustry standard relational database management systems (RDBMS) such as Oracle 8i,Microsoft SQL Server 7.0, or IBM DB/2. Decades of usage in health care and other industrieshave proven these RDBMS technologies to be a secure, reliable, high-performance, and cost-effective means of storing large amounts of data.
The actual web page creation and delivery platform must have unquestionable security andreliability characteristics, while enabling the flexibility and graphical user interfacesophistication necessary for a consumer web site. Candidate languages and platforms include:IBM Visual Age with AIX server software, Microsoft Internet Information Server deliveringActive Server Pages on Windows 2000 server software, or ColdFusion dynamic web pages. Thelist of web content delivery tools is constantly changing and growing in number and capabilitiesand must be actively evaluated at the time of product development.
41

-.—
.,,-
,—
.-
.—
.--.--
——
,—
-%
___
——
——
——
.--.
—
App
endi
xB
-4:
Edu
cati
onD
eliv
ery
Pro
cess
Appoin
tmen
tP
atie
nt
vis
itD
ata
input
Dat
aD
ata
rev
iew
mat
chin
g
Dia
gnos
isC
hart
ing
Tre
atm
ent
New
pro
cess
Cli
nic
ian
Pat
ient
educ
atio
n-
Cur
rent
pro
cess
Cle
rkN
urse
IMA
Bill
ing
Dep
t.In
puts
(1)
Get
spe
rmis
sion
Info
rmat
ion
RN
and
appo
intm
ent
touse
CPw
inpu
tA
dm
inda
ta(2
)E
xpla
ins
use
of
Sta
ffC
PW
Mak
esP
atie
ntvi
sit
Pat
ient
revi
ews
Pat
ien
tap
poin
tmen
tda
taon
the
CP
w
Info
rmat
ion
CP
W
_________
mat
chin
gsy
stem
CPW
gene
rati
on
42
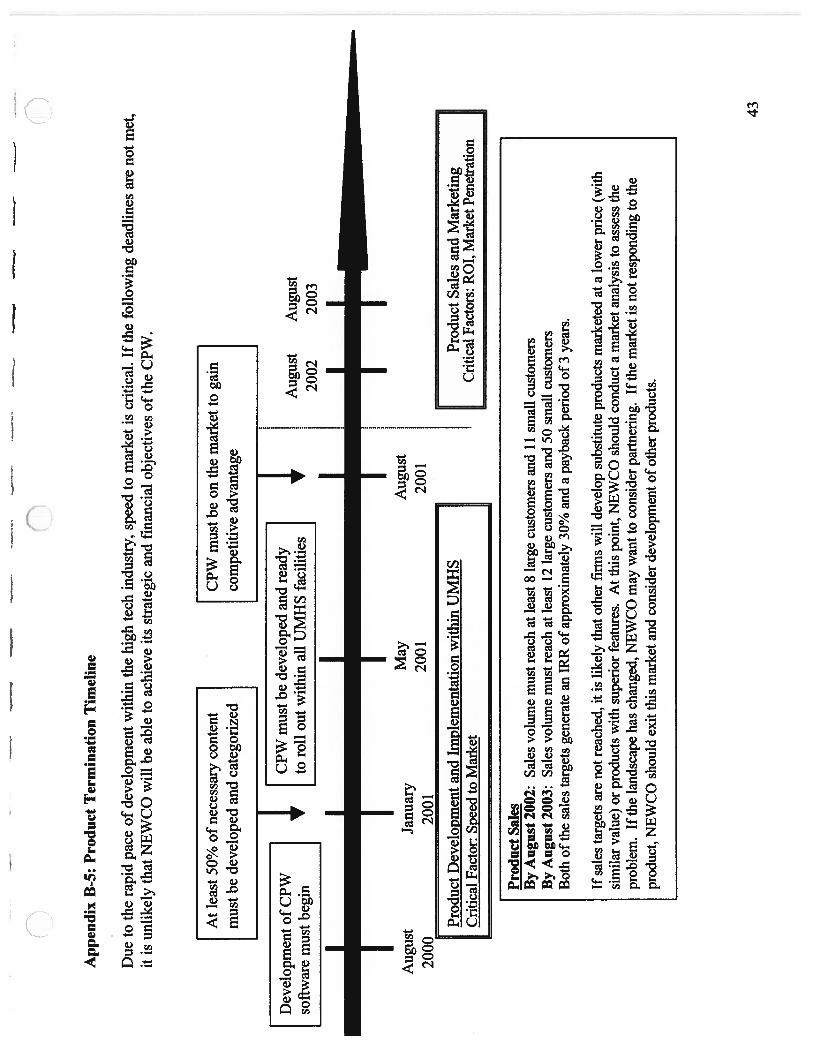
——
—--
App
endi
xB
-5:
Pro
duct
Ter
min
atio
nT
imel
ine
Due
toth
era
pid
pace
ofde
velo
pmen
tw
ithin
the
high
tech
indu
stry
,sp
eed
tom
arke
tis
criti
cal.
Ifth
efo
llow
ing
dead
lines
are
not
met
,it
isun
like
lyth
atN
EW
CO
will
beab
leto
achi
eve
itsst
rate
gic
and
fina
ncia
lob
ject
ives
ofth
eC
PW.
Dev
elop
men
to
fCPW
soft
war
em
ust
begi
n
I
CP
Wm
ust
bede
velo
ped
and
read
yto
roll
out
with
inal
lU
MH
Sfa
cilit
ies
I
At
leas
t50
%of
nece
ssar
yco
nten
tm
ustb
ede
velo
ped
and
cate
gori
zed
1
CPW
mus
tbe
onth
em
arke
tto
gain
com
petit
ive
adva
ntag
e I
Aug
ust
2000
Aug
ust
2002
Janu
ary
2001
Aug
ust
2003
I
May
2001
Prod
uct
Dev
elop
men
tan
dIm
plem
enta
tion
with
inU
MH
SC
ritic
alFa
ctor
:Sp
eed
toM
arke
t
Aug
ust
2001
HP
rodu
ctSa
les
and
Mar
keti
ngC
ritic
alFa
ctor
s:RO
T,M
arke
tPen
etra
tion
NP
rodu
ctSa
les
By
Aug
ust2
002:
Sale
svo
lum
em
ustr
each
atle
ast8
larg
ecu
stom
ers
and
11sm
allc
usto
mer
sB
yA
ugus
t200
3:Sa
les
volu
me
mus
trea
chat
leas
t12
larg
ecu
stom
ers
and
50sm
all
cust
omer
sB
oth
ofth
esa
les
targ
ets
gene
rate
anIR
Rof
appr
oxim
atel
y30
%an
da
payb
ack
peri
odof
3ye
ars.
Ifsa
les
targ
ets
are
notr
each
ed,i
tis
likel
yth
atot
her
firm
sw
illde
velo
psu
bstit
ute
prod
ucts
mar
kete
dat
alo
wer
pric
e(w
ithsi
mila
rva
lue)
orpr
oduc
tsw
ithsu
peri
orfe
atur
es.
Att
his
poin
t,N
EW
CO
shou
ldco
nduc
tam
arke
tana
lysi
sto
asse
ssth
epr
oble
m.
Ifth
ela
ndsc
ape
has
chan
ged,
NE
WC
Om
ayw
antt
oco
nsid
erpa
rtner
ing.
Ifth
em
arke
tis
not r
espo
ndin
gto
the
prod
uct,
NE
WC
Osh
ould
exit
this
mar
keta
ndco
nsid
erde
velo
pmen
tofo
ther
prod
ucts
.
43
Appendix C
SALES AND MARKETiNG
44
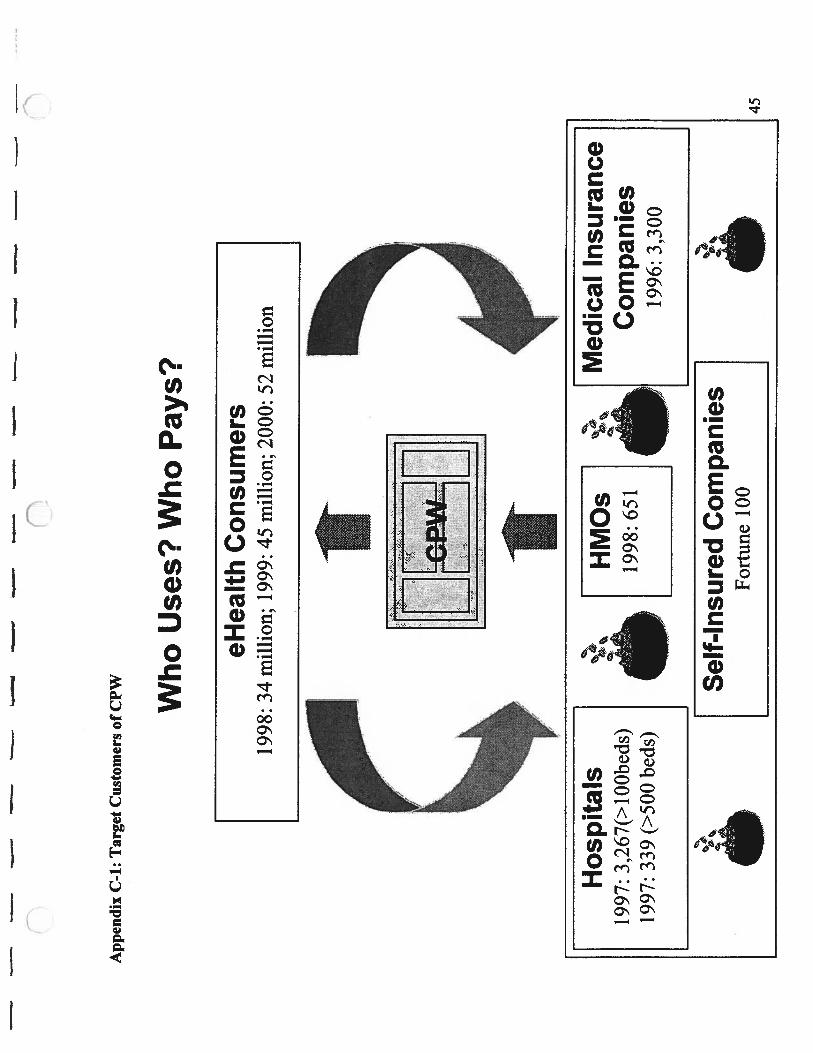
--
——
.—
——
——
——
——
.—
.—
——
——
nn
C
App
endi
xC
-i:
Tar
get
Cus
tom
ers
ofC
PW
Who
Use
s?W
ho
Pay
s?
Sel
f-In
sure
dC
ompa
nies
Fort
une
100
Med
ical
Insu
ranc
eC
ompa
nies
1996
:3,
300
eHea
lth
Consu
mer
s19
98:
34m
illi
on;
1999
:45
mill
ion;
2000
:52
mil
lion L
iiH
ospi
tals
1997
:3,
267(
>l0
0bed
s)19
97:
339
(>50
0be
ds)
HM
Os
1998
:65
1
ç:
Q.. c
45

——
——
——
-—
——
—_
e—
——
—-
—-—
nn
App
endi
xC
-2:
Pot
enti
alC
usto
mer
Ana
lysi
s
Hosp
ital
s
Tot
alO
utpa
tien
tvi
sits
Out
pati
ent
Siz
e(#
ofbed
s)#
hosp
ital
s#
bed
s#
adm
issi
ons
Inpa
tien
td
ays
Em
erge
ncy
Non
-Em
erge
ncy
Tot
alF
acto
r<1
002,
830
148,
565
3,95
7,23
628
,072
,079
16,6
89,3
9472
,069
,008
88,7
58,4
022.
1110
0-29
92,
279
399,
602
13,5
06,6
8990
,778
,321
43,2
05,7
3916
5,27
5,70
220
8,48
1,44
12.
1130
0-49
964
924
5,37
48,
810,
562
61,0
17,1
9421
,851
,514
102,
950,
748
124,
802,
262
2.11
>50
033
924
1,84
97,
349,
813
65,5
96,0
6115
,681
,160
82,8
76,9
0498
,558
,064
2.11
Tot
al6,
097
1,03
5,39
033
,624
,300
245,
463,
655
97,4
27,8
0742
3,17
2,36
252
0,60
0,16
92.
11U
MH
S76
033
,761
209,
841
1,00
2,58
21.
47
Ave
rage
Out
pati
ent
visi
tsE
stim
ated
Siz
e(#
ofb
eds)
#hosp
ital
s#
bed
s#
adm
issi
ons
Inpa
tien
td
ays
Em
erge
ncy
Non
-Em
erge
ncy
Tot
alre
venu
e($M
)<1
002,
830
521,
398
9,91
95,
897
25,4
6631
,363
21.8
100—
299
2,27
917
55,
927
39,8
3318
,958
72,5
2191
,479
74.6
300—
499
649
378
13,5
7694
,017
33,6
7015
8,63
019
2,29
916
3.4
>500
339
713
21,6
8119
3,49
946
,257
244,
475
290,
732
254.
0S
ou
rce:
1999
Hos
pita
lsS
tati
stic
s,C
ost
Per
Cas
eIn
itia
tive
(UM
HS)
Ass
um
pti
ons:
1.C
PC
issa
me
aslo
cal
com
pet
itor
aver
age
of
$6,0
00ac
ross
size
2.O
utpa
tien
tfa
ctor
issa
me
asH
FHSs
2.11
3.O
utpa
tien
tca
ses
has
sam
evi
sit
num
ber
asU
MH
S
46

——
*—
——
——
——
——
——
——
App
endi
xC
-3:
Mar
ket
Seg
men
tati
on
n
Siz
e
Lar
ge
Med
ium
Sm
all
Fo
rtu
ne
100
Nat
ion-
wid
e>
500
bed
sco
mpan
ies
MIC
s
Fo
rtu
ne
500
Reg
ional
MIC
s300499
bed
sco
rnpan
ies
Oth
erS
mal
lM
lCs
I00
299
bed
sse
lf-i
nsu
red
com
pan
ies
Sel
f-in
sure
dC
om
pan
ies
Med
ical
Insu
rance
Com
pan
ies
(MIC
5)
Cu
sto
mer
Cat
egory
Ho
spit
als
47

----r
--
-.--
——
,—
——
—-
——
—-
nn
App
endi
xC
-4:
Seg
men
tP
rior
itiz
atio
nT
empl
ate
Siz
eof
the
mar
ket
Po
ten
tial
Pre
stig
eof
Po
ssib
ilit
yF
itto
_______
________
________
pen
etra
tio
ncu
stom
ers
ofre
ferr
alorg
aniz
atio
n#
ofA
vera
geT
otal
leve
lgoal
spl
ayer
sre
venu
ere
venu
e
Sco
re(1
)(2
)(3
)(4
)(5
)(6
)(7
)(1
)*(2
)
Wei
ght
40%
30%
10%
10%
10%
Tot
al(3
)*40
%+
(4)*
30%
+(5
)*10
%+
(6)*
10%
+(7
)*10
%=
Tot
alsc
ore
score
Not
e:(3
)-
Sta
ndar
dize
dnu
mbe
rto
I I0
scal
esc
ore
(4),
(5),
(6),
(7)
-1-
10sc
ale
scor
es
48

-—
——
—--
——
—
n
App
endi
xC
-5:
Cus
tom
erP
rior
itiz
atio
nT
empl
ate
Fin
anci
alca
pab
ilit
yP
oss
ibil
ity
Pre
stig
eof
Po
ssib
ilit
yF
itto
ofcu
stom
erof
refe
rral
org
aniz
atio
n#
ofR
even
uePr
ofit
con
tin
uo
us
goal
sp
atie
nts
part
ners
hip
Sco
re(1
)(2
)(3
)(4
)(5
)(6
)(7
)
Wei
ght
40%
30%
10%
10%
10%
Tot
al[A
vera
ge{(
1),(
2),(
3)}]
*40%
+(4
)*30
%+
(5)*
10%
+(6
)*1O
%+
(7)*
10%
=T
otal
score
sco
re
Not
e:(1
),(2
),(3
)-S
tandar
diz
edn
um
ber
to1-
10sc
ale
score
(4),
(5),
(6),
(7)
-1—
I 0sc
ale
score
s
49

—_
——
-_I
——
——
——
App
endi
xC
-6:
EV
Aan
alys
is
Lar
ge
Hosp
ital
s(>
500
bed
s)1)
Red
uces
Phys
icia
ns’
and
Nur
ses’
time
educ
atin
gpa
tien
tsPo
tent
ial
Pat
ient
-spe
cifi
csi
tesa
ves:
#outp
atie
nts
lyea
r%
rene
atpa
tien
tsT
otal
hour
ssa
ved
#F
TE
ssa
ved
Cost
Sav
ings
Pri
cepo
int
MD
min
utes
lpat
ient
129
0,73
240
%2,
907
1.9
326,
141
RN
min
utes
Ipat
ient
229
0,73
240
%5,
815
3.7
223,
640
Tot
al54
9,78
12)
Red
uces
num
ber
and
cost
oftr
iage
call
s70
,372
3)R
educ
espa
tien
teduca
tion
mat
eria
lsex
pen
ses
incu
rred
109,
956
Tot
alEV
A73
0,10
936
0,00
0
Med
ium
Ho
spit
als(
300-4
99
bed
s)1)
Red
uces
Phys
icia
ns’
and
Nur
ses’
time
educ
atin
gp
atie
nts
Pot
enti
alP
atie
nt-s
peci
fic
site
save
s:#
outn
atie
nts
lyea
r%
rene
atna
tien
tsT
otal
hour
ssa
ved
#FT
Es
save
dC
ostS
avin
asP
rice
noin
tM
Dm
inut
esip
atie
nt1
192,
299
40%
1,92
31.
221
5,72
0R
Nm
inut
eslp
atie
nt2
192,
299
40%
3,84
62.
514
7,92
3
Tot
al36
3,64
32)
Red
uces
num
ber
and
cost
oftr
iage
call
s46
,548
3)R
educ
espa
tien
tedu
cati
onm
ater
ials
expe
nses
incu
rred
72,7
29T
otal
EVA
482,
918
240,
000
Sm
all
Ho
spit
als(
100-2
99
bed
s)1)
Red
uces
Phys
icia
ns’
and
Nur
ses’
time
educ
atin
gpa
tien
tsP
oten
tial
Pat
ient
-spe
cifi
csi
tesa
ves:
#ou
tnal
ient
s!ye
ar%
rene
atpa
tien
tsT
otal
hour
ssa
ved
#FT
Es
save
dC
ost S
avin
gsPr
ice
noin
tM
Dm
inut
eslp
atie
nt1
91,4
7940
%91
50.
610
2,62
1R
Nm
inut
es!p
atie
nt2
91,4
7940
%1,
830
1.2
70,3
69T
otal
172,
990
2)R
educ
esnu
mbe
ran
dco
stof
tria
geca
lls
22,1
433)
Red
uces
pati
ente
duca
tion
mat
eria
lsex
pens
esin
curr
ed34
,598
Tot
alEV
A22
9,73
012
0,00
0
50

Appendix B
ORGANIZATION ANDPARTNERSHIP
51

——
*—
--
—*
—*__
*—
App
endi
xD
-1:
Org
aniz
atio
nC
har
tof
NE
WC
O
n
CE
O
•B
usi
nes
sD
evel
opm
ent
•A
dm
inis
trat
ive
Support
Boar
dof
Dir
ecto
rs
Tec
hnic
alst
aff
IAdv
isor
yB
oar
d
VP
ofM
arke
ting
and
Sal
esC
FO
•A
ppli
cati
onp
rogra
mm
er•
Dat
abas
ead
min
istr
ato
r•
Bu
sin
ess
anal
yst
•S
yst
emp
rogra
mm
er•
Des
kto
psu
pp
ort
•S
ecuri
tyex
pert
•M
arke
ting
•S
ales
peo
ple
•C
ust
om
erS
ervic
e
•C
onsu
ltin
gcl
inic
ians
•C
onsu
ltin
gR
Ns
•C
on
ten
tpro
vid
ing
clin
icia
ns
52
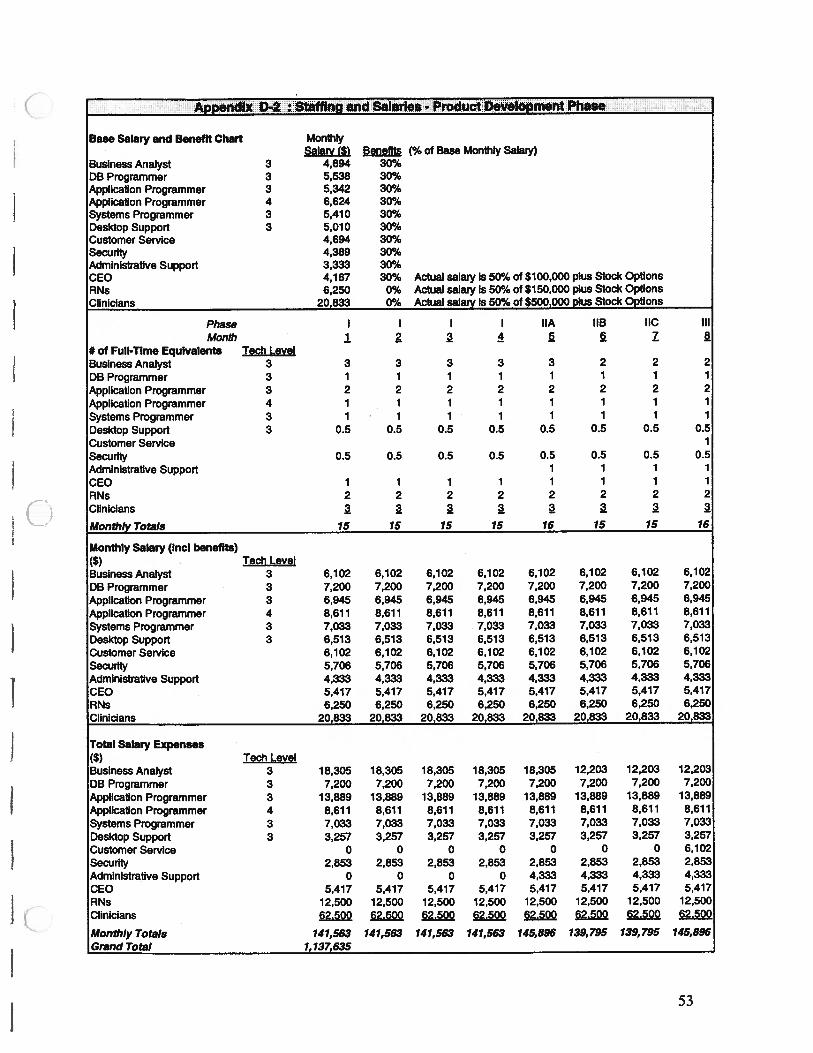
Appefldl* D2 :; StafflngaAd Salaries-Product Development Phase
MonthlySalary (5) Benefits (% of Base Monthly Salaly)
3 4,694 30%3 5,538 30%3 5,342 30%4 6,624 30%3 5,410 30%3 5,010 30%
4,694 30%4,389 30%3,333 30%4,167 30% Actual salary is 50% of $100,000 plus Stock Options6,250 0% Actual salaly is 50% of $150,000 plus Stock Options
20,833 0% Actual salary Is 50% of $500,000 plus Stock Options
Phase I I I I hA IIB IIC IllMonth 1 2 2 3 3 Z 3
# of Full-Time Equivalents Tedi LevelBusiness Analyst 3DB Programmer 3Application Programmer 3Application Programmer 4Systems Programmer 3Desktop Support 3Customer ServiceSecurityAdministrative SupportCEORNsClinicians
Monthly Totals
Monthly Salary (md benefits)(5) Tech LevelBusiness Analyst 3 6,102 6,102 6,102 6,102 6,102 6,102 6,102 6,102
DB Programmer 3 7,200 7,200 7,200 7,200 7,200 7,200 7,200 7,200
Application Ptgrammer 3 6,945 6,945 6,945 6,945 6,945 6,945 6,945 6,945
Application Programmer 4 8,611 8,611 8,611 8,611 8,611 8,611 8,611 8,611Systems Programmer 3 7,033 7,033 7,033 7,033 7,033 7,033 7,033 7,033Desktop Support 3 6,513 6,513 6,513 6,513 6,513 6,513 6,513 6,513Customer Service 6,102 6,102 6,102 6,102 6,102 6,102 6,102 6,102Security 5,706 5,706 5,706 5,706 5,706 5,706 5,706 5,706Administrative Support 4,333 4,333 4,333 4,333 4,333 4,333 4,333 4,333CEO 5,417 5,417 5,417 5,417 5,417 5,417 5,417 5,417RNs 6,250 6,250 6,250 6,250 6,250 6,250 6,250 6,250Clinicians 20,833 20,833 20,833 20,833 20,833 20,833 20,833 20,833
Total Salary Expenses($) Tech LevelBusiness Analyst 3 18,305 18,305 18,305 18,305 18,305 12,203 12,203 12,203DB Programmer 3 7,200 7,200 7,200 7,200 7,200 7,200 7,200 7,200Application Programmer 3 13,889 13,889 13,889 13,889 13,889 13,889 13,889 13,889Application Programmer 4 8,611 8,611 8,611 8,611 8,611 8,611 8,611 8,611Systems Programmer 3 7,033 7,033 7,033 7,033 7,033 7,033 7,033 7,033Desktop Support 3 3,257 3,257 3,257 3,257 3,257 3,257 3,257 3,257Customer Service 0 0 0 0 0 0 0 6,102Security 2,853 2,853 2,853 2,853 2,853 2,853 2,853 2,853Administrative Support 0 0 0 0 4,333 4,333 4,333 4,333CEO 5,417 5,417 5,417 5,417 5,417 5,417 5,417 5,417RNs 12,500 12,500 12,500 12,500 12,500 12,500 12,500 12,500Clinicians 62.500 62.500 62.500 62.500 62.500 62.500 62500 62.500
Monthly Totals 141,563 141,563 141,563 141,563 145,896 139,795 139,795 145,896Grand Total 1,137,635
Base Salary and Benefit Chart
Business AnalystDB ProgrammerApplication ProgrammerApplication ProgrammerSystems ProgrammerDesktop SupportCustomer ServiceSecurityAdministrative SupportCEORNsClinicians
3 3 3 3 3 2 2 21 1 1 1 1 1 1 12 2 2 2 2 2 2 21 1 1 1 1 1 1 11 1 1 1 1 1 1 1
0.5 0.5 0.5 0.5 0.5 0.5 0.5 0.5
0.5 0.5 0.5 0.5 0.5 0.5 0.5 0.51 1 1 1
1 1 1 1 1 1 1 12 2 2 2 2 2 2 2
3 2 3 2 2 2 2 215 15 15 15 16 15 15 16
53
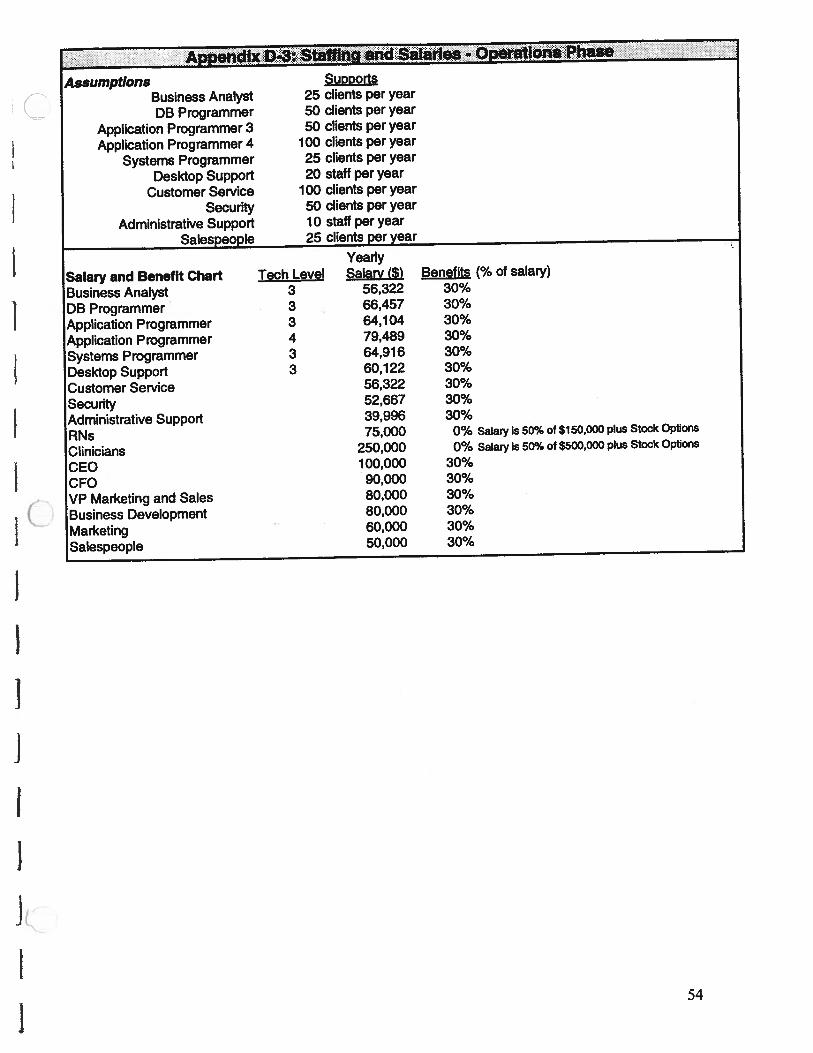
(flU
)
00
00
..
00
øu
)
.a.E
.
If)
00
u)U
)0
(c
00
0IQ
4’1
00
9o
oo
oo
oo
o0
00
00
00
00
1C)
COCO
COCO
COCO
COCO
COCO
COCO
COCO
a)’
II
I..L...
hI...
Icacacacaca
cacaca
jc,J
rt0
)C
0C
%iC
%.I
F’..(
D0
00
0O
OO
O>
>.>
‘>
flO
U)i-C
%JN
CD
O)00000
00
0II)L
I>
-coU
)o
)o
oo
oo
oq
qa>
oa)
w>
ww
>,C
DC
D’t0
)0
C0
CJ0
)U
)0
00
0O
O°
cac
CD1%
(0CD
U)
U)
COF—
U)0
0)
(0(0
CDU
)O
Iou)coooD
.0cO
0)
0ca
——
——
——
—0
1C
CC
Cc:
CC
C>
-CO
izI.!
.2.9
.!ca
.2.!
ca(l)I5
Z5o
Z5Z5
IZ5
3i
U)000L
00000U
)a)
1C
.IU)U
)0C
%lC
J0U
)’C’J
>101fC
OC
OC
OC
OC
O
0I01I-I
CO0)
0)
E8
81cE
EE
E°
<E
EC
cc
00)0(00)
(0I.
0)0
)•
00)
EE
0o
co
-2
2o
-1
°E
E0
.
zicE
C).
0o
E0)0).S
Cl)C
OO
OhO
co
w‘-‘-0
)0.
0)cQ
)w
caE..
Cl)aa
0
0.0
.CO
CI)0
.
0.0
.>
.0)
z0
Z=
ww
oD
CO
__
__
__
__
__
Ø<
cC
CO
QO
C0<
ClC
OO
C)>
CflC
O
U—
-—
-—
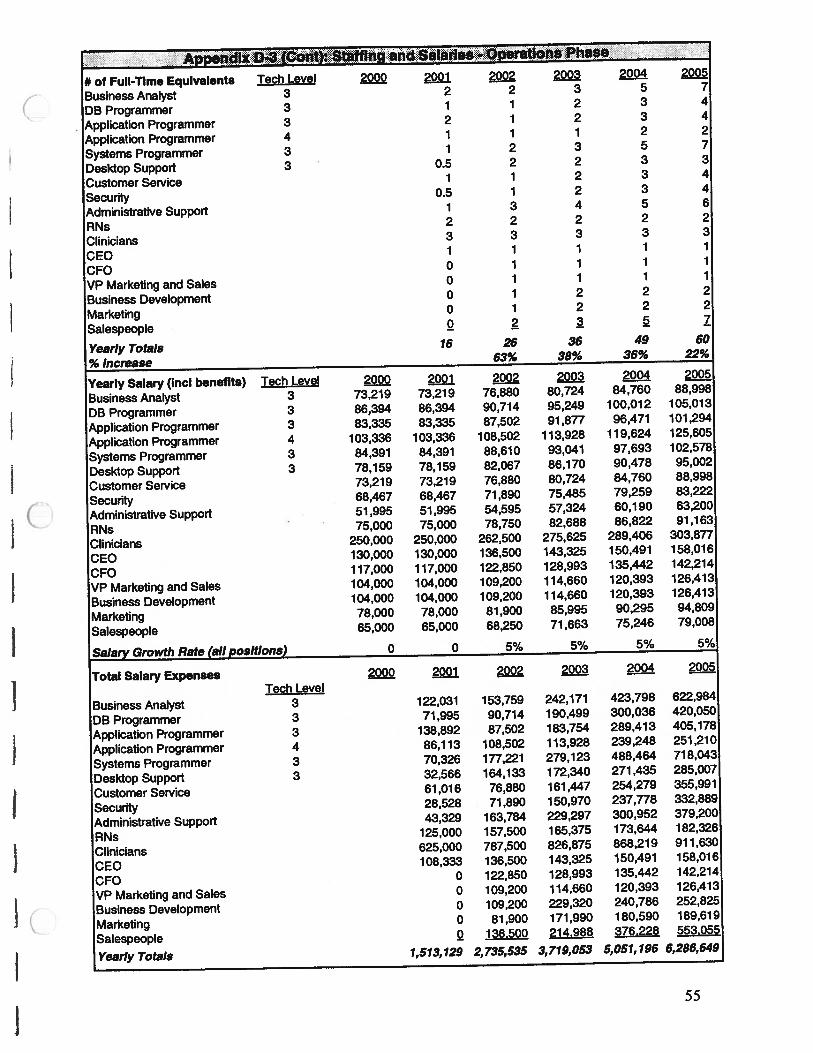
and Salaries op tlOflSPhasE:.
# of Full-Time Equivalents Tech Level 2222 2221 2222 2222 2224 222k
Business Analyst 3 2 2 3 5 7
DB Programmer 3 1 1 2 3 4
Application Programmer 3 2 1 2 3 4
Application Programmer 4 1 1 1 2 2
Systems Programmer 3 1 2 3 5 7
Desktop Support 3 0.5 2 2 3 3
Customer Service 1 1 2 3 4
Security 0.5 1 2 3 4
Administrative Support 1 3 4 5 6
RNs 2 2 2 2 2
Clinicians 3 3 3 3 3
CEO 1 1 1 1 1
CFO 0 1 1 1 1
VP Marketing and Sales 0 1 1 1 1
Business Development 0 1 2 2 2
Marketing 0 1 2 2 2
Salespeople 2 2 Z
Yearly Totals 16 26 36 49 60
%lncrease 63% 38% 36% 22%
Yearly Salary (mci benefits) Tech Level 2222 2221 2222 2222 2224 2222
Business Analyst 3 73,219 73,219 76,880 80,724 84,760 88,998
DB Programmer 3 86,394 86,394 90,714 95,249 100,012 105,013
Application Programmer 3 83,335 83,335 87,502 91,877 96,471 101,294
Application Programmer 4 103,336 103,336 108,502 113,928 119,624 125,605
Systems Programmer 3 84,391 84,391 88,610 93,041 97,693 102,578
Desktop Support 3 78,159 78,159 82,067 86,170 90,478 95,002
Customer Service 73,219 73,219 76,880 80,724 84,760 88,998
Security 68,467 68,467 71,890 75,485 79,259 83,222
Administrative Support 51,995 51,995 54,595 57,324 60,190 63,200
RNs 75,000 75,000 78,750 82,688 86,822 91,163
Clinicians 250,000 250,000 262,500 275,625 289,406 303,877
CEO 130,000 130,000 136,500 143,325 150,491 158,016
CFO 117,000 117,000 122,850 128,993 135,442 142,214
VP Marketing and Sales 104,000 104,000 109,200 114,660 120,393 126,413
Business Development 104,000 104,000 109,200 114,660 120,393 126,413
Marketing 78,000 78,000 81,900 85,995 90,295 94,809
Salespeople 65,000 65,000 68,250 71,663 75,246 79,008
Salary Growth Rate (all positions) 0 0 5% 5% 5% 5%
Total Salary Expenses 2222 2221 2922 2222 2224 2222Tech Level
Business Analyst 3 122,031 153,759 242,171 423,798 622,984
DB Programmer 3 71,995 90,714 190,499 300,036 420,050
Application Programmer 3 138,892 87,502 183,754 289,413 405,178
Application Programmer 4 86,113 108,502 113,928 239,248 251,210
Systems Programmer 3 70,326 177,221 279,123 488,464 718,043
Desktop Support 3 32,566 164,133 172,340 271,435 285,007
Customer Service 61,016 76,880 161,447 254,279 355,991
Security 28,528 71,890 150,970 237,778 332,889
Administrative Support 43,329 163,784 229,297 300,952 379,200
RNs 125,000 157,500 165,375 173,644 182,326
Clinicians 625,000 787,500 826,875 868,219 911,630
CEO 108,333 136,500 143,325 150,491 158,016
CFO 0 122,850 128,993 135,442 142,214
VP Marketing and Sales 0 109,200 114,660 120,393 126,413
Business Development 0 109,200 229,320 240,786 252,825
Marketing 0 81,900 171,990 180,590 189,619
Salespeople 2 136.500 21 4.988 376.228 553.055
Yearly Totals 1,513,129 2,735,535 3,719,053 5,051,196 6,286,649
55
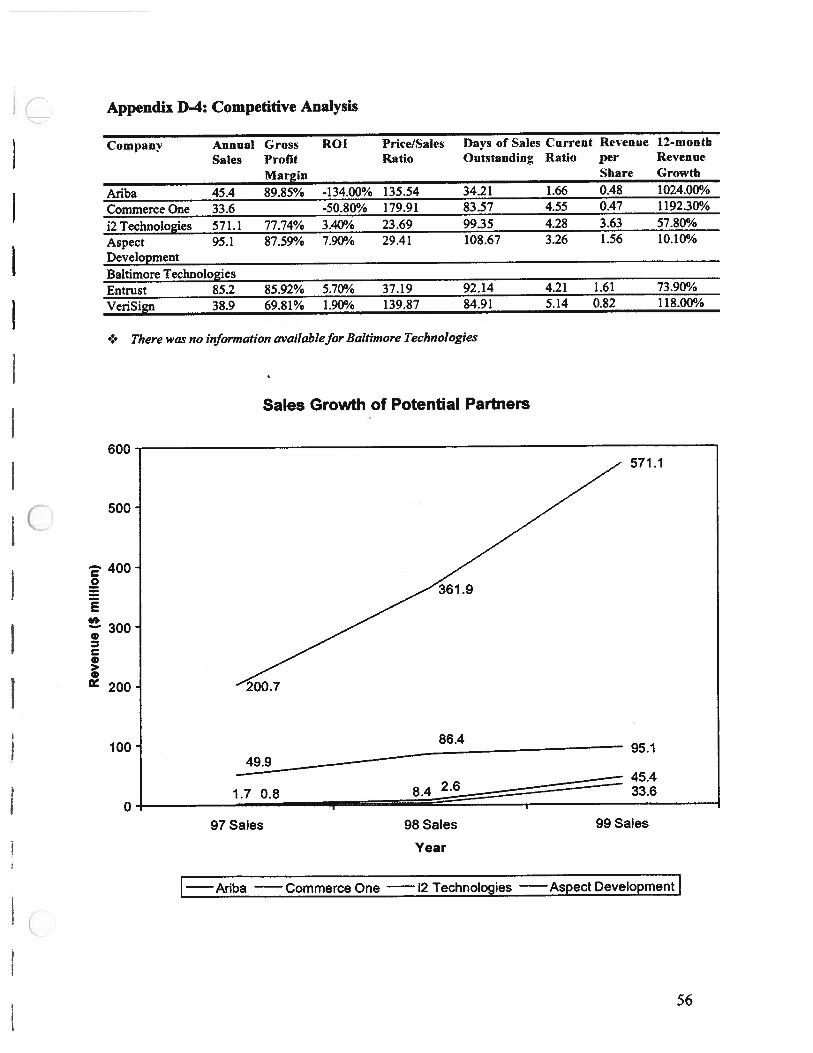
nR
even
ue
(Sm
illi
on)
-C
i)01
0)
oo
00
00
00
00
00
0() 0 0
C) I
<T
j
. C/)
t—
.—
.
-I
)00
OO
Vi-
.cQ
3
0’0
0.O
Vi
aoco
i-
t’.)
00
00
—w
ca
000
)
O 0 I.
•:.
0•
0) C) 0 3 3 CD CD 0 CD r,’) —1
CD C,
0 0 CD CD (0 () 0 CD C,
CD CD 0 V 3 CD
(0 (I)
0) CD U) (0
<c0
(D
Om
0) U) CD (0 ci)
0) CD Cl)
00
00
Vi
00
0
00
00
Vi
0 0 Vi
Vi
0 0000 a
C’,
m 0 0 -‘ 0 0 -‘I -o 0 (D -V 0 CD
tJ—
\0‘)-
—‘0
\Q
C) C C C C! - -4
)
C
-l
C 00
0
I.
Vi
—)
—
(11
00
O
“0
—— C
—000
w..
—L
Vi0
’0
%0
0V
i0
0—
00
00
C0
a
co C 00
p C C0
0 C
Vi
00 C
C “3 C C 0
0

Appendix D-5: Potential Partners Company Descriptions
Product development partners
12 Technologies
i2 Technologies has over 34% market share in the growing eBusiness market. This in
conjunction with the defmitive agreement reached to purchase Aspect Development in a
$9.3 billion stock-for-stock deal (Aspect Development will become a subsidiary of i2
Technologies), has solidified its position as the global leader in collaborative solutions
for B2B eCommerce. i2 Technologies is an attractive product development partner
because of its extensive experience. As much as 20% of sales have been allocated for
research and development to enable i2 to explore unchartered markets. Currently, they
have operations throughout the world, with 68% of 1999 sales coming from the US and
16% from Europe.
Aspect DevelopmentRecently acquired by i2 Technologies, Aspect Development has over 180 of the world’s
largest companies as customers and 1999 revenue of $95.1 million, with software
accounting for nearly 60% of sales. They provide value to their customers by providing
efficiencies in procurement, design, operations management and the supply chain.
AribaAriba is using acquisitions and joint ventures to combat competition, and like other
Internet companies, it has yet to show an annual profit. However, it is forecast that Ariba
will achieve 2000 revenues of $127.2 million and 2001 revenues of $239 million.2 Ariba
is currently operating 50 marketplaces, compared to 35 for Commerce One and 3 for
Oracle.
Commerce OneCommerce One offers products and services to simplify and offer access and connectivity
to global eMarkets. They mainly offer product catalogs through their BuySite software
and seamless eCommerce transactions through their MarketSite.net website. Commerce
One also provides services including content management, order availability information,
status tracking, and transaction support. While their expertise is needed, it may not be
directly relevant to UMHS and the Customized Web Page. A larger company
(Commerce One boasts $ 33.6 million in revenue for 1999) with more diverse experience
may be of value for UMHS.
Security Partners
EntrustEntrust is the market leader in PKJ technology solutions. While Entrust dominates
internal PKI solutions, they have taken an aggressive move to extend its outsourced based
solutions, procuring a leading market share of approximately 45% of the digital
57

certificate market. Entrust has an established presence in the healthcare market and is
familiar with the changing landscape of healthcare and its affects on security issues and
connectivity. They are familiar with HIPPA and other regulatory issues that directly
affect security compliance. Entrust’s 2000 revenue growth is estimated to be 65% (GS).
VeriSignVeriSign is the market leader in browser-based certificates. VeriSign provides digital
IDs, also known as digital certificates, with encrypted information to protect against
unauthorized access to information over the Internet, intranet, and extranets. VeriSign
has three primary business segments/product lines: Outsourced PKI, general security
solutions including firewalls, and web-server certificates. They supply their services on a
subscription basis, and their clients include large companies such as Microsoft, Cisco
Systems, and Visa. VeriSign is looking to extend its services and client base by opening
up to other forms of revenue and alliances. This is evidenced by its recent alignment
with Novell, a consumer related company, through the offering of a co-branded product.
VeriSign is also looking to expand its geographic horizons to increase international sales
from 15% of total revenues.
Baltimore TechnologiesBased in Dublin, Ireland, Baltimore Securities is an established leader in the development
and marketing of computer and network security in Europe. In order to increase their US
market base they acquired GTE Cybertrust on March 28, 2000. Based in the Boston area,
Cybertrust was a leader in PKI security. It is expected that Cybertrust software will
eventually be phased out in favor of Baltimore’s due to the acquisition. Baltimore
reported $30 million in revenue in 1999, while Cybertrust was approximately half of that.
However, some of Cybertrust’s key customers are concerned by the acquisition. A large
portion of Cybertrust’s customers are government agencies, such as the Department of
Defense, and the fact that Baltimore is based overseas worries them. This may also have
its ramifications on a potential partnership due to US specific regulations concerning the
security of healthcare data and patient specific records.
58

Appendix D-6: Required Capabilities of Potential Partners
Form of Partnership Capabilities
Marketing and distribution partner — Connection to customers— Funding for promotion and distribution
— Skilled salesforce— Reduction of distribution cost
— Ability to establish reliability of the product
— Co-branding ability
• Content development partner — Reduction of content development cost
— Capability to increase efficiency in development
time— Creation of synergies through increased knowledge
base
• Co-development partner — Funding for product and content development
— Capability to speed up product development•
— Ability to successfully launch new product
59
Appendix E
FUTURE PRODUCTS
60

Appendix E-1: Product Synergies
‘Jduct Customer Core Ussh**ss’o( DiettibutionCompetencies Core Needed
_
Needed Codes
p..__ —
writing data ‘N/A force to
CPW: Patients management, “‘ hospitals,
content payors,development employerssoftware Direct saleswriting, data forveto
Dm7. .
+4+4r i. vi’. Providers management,
content
____________
development
Decision S&fls
above also,U)0 Providers consensus of
Systems: 1 clinical care(eg guidelines)
online courseCME: Physiciansit development
data
I management, force to
lIT: Providers infrastructuremaintenanceskillsallofthe
Providersand above,plus
Telecare Patients many others
Usefulness is rated on the followmg scale: It CMPc ,.r
+ not useful++ some of previous items useful; need many more items for
success+-4-+ most of the previous items are useful; however more
items still needed++-H- most of the previous items are useful for success; little
else is needed+-H-++ previous items create a large success in this area
The above table displays synergies created along the dimensions of customer
connectivity, core competencies, and distribution channels between products and their
predecessors. Customer connectivity is the degree to which NEWCO is able to obtain
information regarding customer habits and needs. The higher the degree of connectivity,
shown in column three, the more flexible NEWCO is in adapting future products to the
exact needs of the customer’. Core competencies are the skill sets NEWCO has at its
This is especially important as part of an overall strategy. The more connected an organization is to its
customers, the more the organization will learn about customer habits and how to improve service with
upgraded products and new products. This is exactly the way America Online and Amazon.com began;
they established a presence “fast rather than perfect” for the sole purpose of gaining connectivity to the
customer.
CusmerIDteliblon*ompre4ou ceptance
pret4OUS
61
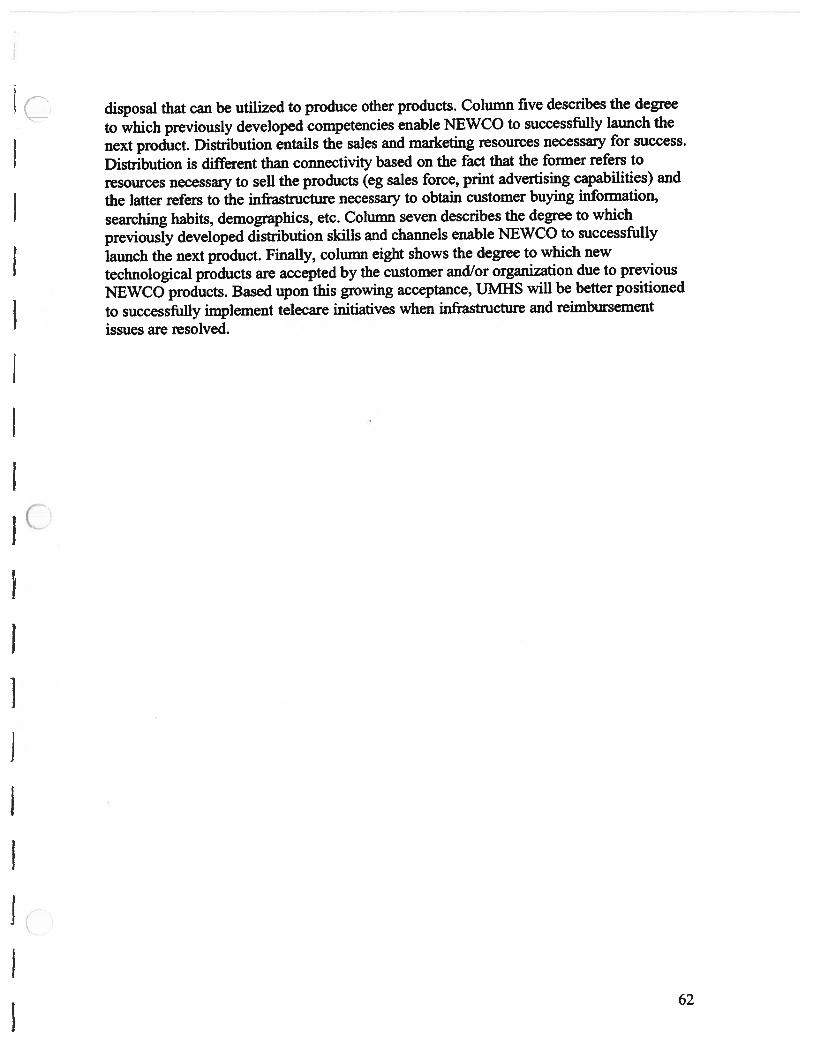
disposal that can be utilized to produce other products. Column five describes the degree
to which previously developed competencies enable NEWCO to successfully launch the
next product. Distribution entails the sales and marketing resources necessary for success.
Distribution is different than connectivity based on the fact that the former refers to
resources necessary to sell the products (eg sales force, print advertising capabilities) and
the latter refers to the infrastructure necessary to obtain customer buying information,
searching habits, demographics, etc. Column seven describes the degree to which
previously developed distribution skills and channels enable NEWCO to successfully
launch the next product. Finally, column eight shows the degree to which new
technological products are accepted by the customer and/or organization due to previous
NEWCO products. Based upon this growing acceptance, UMHS will be better positioned
to successfully implement telecare initiatives when infrastructure and reimbursement
issues are resolved.
62

9*—
a—
.-_
‘-a—
•—
___
——
——
—-
——
——
-
:/fl
n C) II C C ci)
0

Appendix F-i: Development Phase Financial Projection Assumptions
Item Assumption Basis of AssumptionLength of Development 8 months MAP team assessment basedPhase upon estimates by internal and
external software devresources
Project Development Costs $1.6 million Sum of the following fivecategories:
Staffmg Needs 16 FTEs Best estimate by internal andexternal software dev experts.
Salaries See Appendix D-2 on page 53 Market salaries for softwaredevelopers as determined byUMHS Ernst & Youngconsulting study. Salaries forother positions based uponcurrent market rates.
HJW and S/W Costs See Appendix F-3 on page 66 Current market costs forrequired H/W and S/W.
Patient Testing Stipends $20/hour; 100 patient hours per test Estimate of hours to conductphase of product development necessary software testing.
Other General & Admin see Appendix F-3 on page 66. Current market rates for theseIncludes various categories such as items.rent, utilities, office supplies,legallaccounting fees, and fees paidto clinicians for content
Nc64
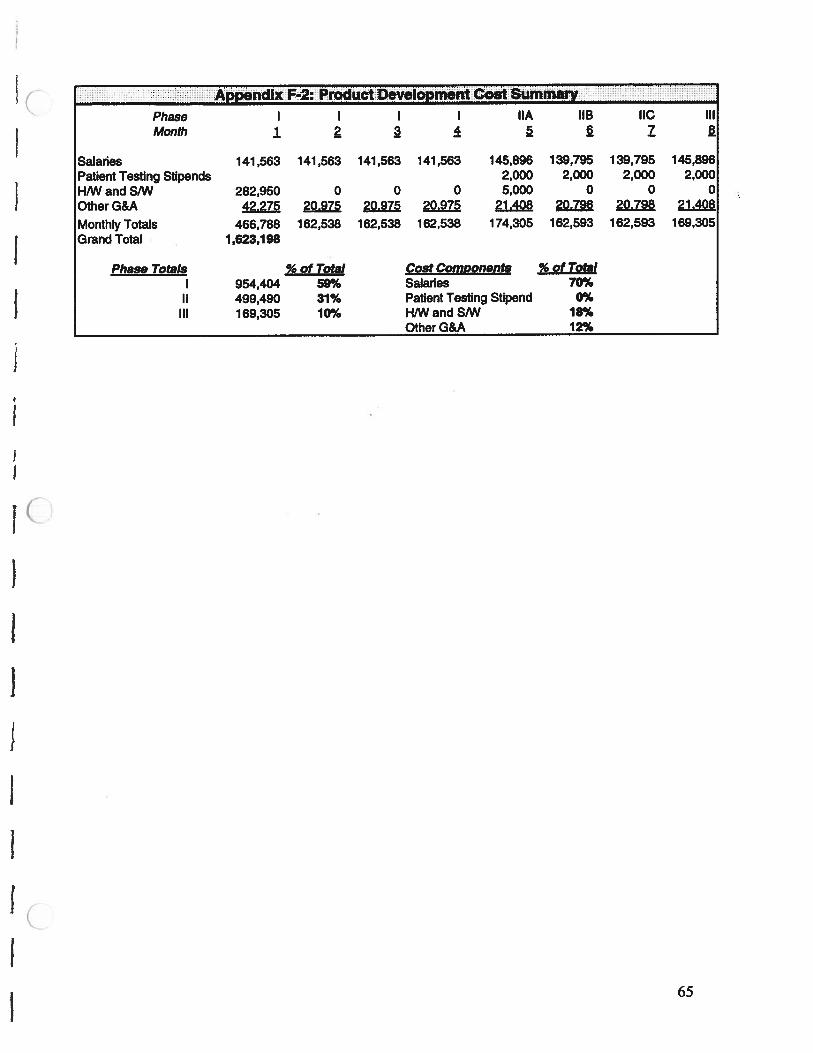
Appfldix F2: PrOduCtDeveIOprnaflt:oM Surnrna:
Phase I I I I hA IIB NC IIIMonth i. a z
Salaries 141,563 141,563 141,563 141,563 145,896 139,795 139,795 145,896Patient Testing Stipends 2,000 2,000 2,000 2,000H/W and SIW 282,950 0 0 0 5,000 0 0 0OtherG&A 42,275 20.975 20.975 20.975 21.408 20.798 20.798 21.408
Monthly Totals 466,788 162,538 162,538 162,538 174,305 162,593 162,593 169,305Grand Total 1,623,198
Phase Totals % of Total Cost Comøonents % of Total954,404 59% Salaries 70%
II 499,490 31% Patient Testing Stipend 0%III 169,305 10% HAN and SAN 18%
Other G&A 12%
65

:APPSfldIX F-3:DetaIIedPodUotEDeVeIQpmefltVOSt$..Assumptions
Development Period 8 months (Start: July 1, 2000; End: March 1, 2001)Rent $15 per sq. ft. per yearSpace Needed Per Person 50 sq. ft.Common Area 500 sq. ft.Space Required-Development 1300 sq. ft.Lease Term 2 yearsUtilities $0.15 per sq. ft. per monthOffice Fumiture $500 per FTE and ClinicianOffice Supplies-FTE $75 per FTE per month (includes leasing of copiers)Office Supplies-Clinicians $25 per clinician per monthOther Expenses 10% of Total Salaly ExpensesH/W and SAN based upon current market pricesH/W maintenance 50% of original purchase price per year (new HIW bought eveiy 2 years)Phone Service $35 per FTE per monthFax, Internet based upon current market prices for fax machine and dedicated lineClinician Fees $250 per hourDays/wk to create content 1 day per Clinical FTEPatient Testing Stipends $20 per hour
100 patient hours per phase (NA, lIB, lIC, Ill)Legal Accounting Fees $60,000 per year
Phase I I I I lIA IIB NCMonth 1 a 2 Z
Hardware and Software CostsProductivity S/W 10,000Visual Age 84,975SecurelD 5,000DataJunction 15,000AIX platform (Server) 40,000Workstation 27,000Printers 6,000Oracle 8i 15,000AIX 84,975
Patient Testing Stipends 2,000 2,000 2,000 2,000Salaries (from Staffing Spdsht) 141,563 141,563 141,563 141,563 145,896 139,795 139,795 145,896Other G&A Costs
Fax Machine 300Phone Service 350 350 350 350 350 350 350 350Internet Access/hosting 400 400 400 400 400 400 400 400Rent 13,000Utilities 244 244 244 244 244 244 244 244Office furniture 8,000Office supplies 825 825 825 825 825 825 825 825Other expenses 14,156 14,156 14,156 14,156 14,590 13,979 13,979 14,590LegaL/Accounting Fees QQQ Q 2QQ Q22 .&QQ
MONTHLY TOTALS 466,788 162,538 162,538 162,538 174,305 162,593 162,593 169,305GRAND TOTAL 1,623,198
66

n00)
lii
U,
-IrO
OO
OcU
3U
11
OO
),c,C
fl<
Oc1
O’U
tiO
OO
Ocro
cn
uz4oV
CD
O
—C
.-‘
CD
),
2.c
DcD
5—
U)C
CD
O—
>.z
Q_
mcna,-n0oz
XC
CC
CD
_O
t,V
’-T
CDD
3C
DCD
CDC
DQ
)cn
zc,
CDz
D)
C)CD
CDs
CD0
CDCO
—.
-CD
oC,
Cl)
CD.
CO
N.
CD
D)0
oCO
-.
CO (0
0•
ft
U)
U)
Cl)
CO
ir’3
010
01C
C0C
00-O
-
IC00C
J10o1r01
D.
VV
00
VV
VV
’<0)
0V
•C
DW
CD
C)C
DO
4’C
DC
DC
DC
DC
D.0m
—C
—0
C4
-‘
-.—
-t
U)-‘
‘oi’)-
biC
)0101
--
1%)
W0-’0)
‘rrbci
10
-i
co
-o
’0101001
10
3VU
IC
i)0
Cl)000
0000
()
I-’
5V
‘0.
CDCD
Cl)
?.CD
bi
C41
U)-J
.0.Jr’3
Ci)
...L
(p)
.—
0)
00
Cl)-
010).
001
I)-J
Ci)
Ci)0
-J!‘
!‘
P’r
mn
CDo
CDg
-
‘oo
b0
1)
Q-
rbi
coc
bii
bib
bib
01(7
1.
010
CDV
CDZ
.0
00
10
0.’)0
)0
Ci)0)0000000)0
10
0)
0)
OO
Cl)000C
J1000
010)0000000)0
Irs)
-4.
C)CD
oCD
Cl)
_‘
-,
-4.
C.)
oCD
Cl)
Ci)
XU)
O0.JC
i)
Ci)
..A
%)
-4
ooL
py1o)p..p1
0)N
)01
bø
0-
-b
biebb
01
(71
010
CD.
00000’30r’3C
4)
010)0000000)0
10
0)
000100001000
Cl)0)0000000)0
IC’)
CD
0)
01:L
Ci)
01
b-
0•01
I’.)
—r)
(71
00011s.)
O)0)014).O
i)0.J)\)1
r%)
°-oi-boi
-bibbibc,i
01o
IcCD
CO
43
0O
I)000I\)0O
)C
,)
(00)0000000)0
100)
00
00
00
01
00
00)0)0000000)0
ID.
CD
—1
CD
bi(0)
0).
0F’
.)C)
101
F’.)
0)
F).
5•F’
).
00
0)
1%)
010
)01.
010
)F’
)0
)J
04
F’)
P301
CD..<
.obbbi-’.
ooib
oboio
i.ro
o.
ooo)o
oor’
.)ooc..)
Doooo000coo
Ic000100001000
(00)0000000)0
101

iSSUMPTlONS
PricesLicense CS) Customization CS)Large customer 300,000 Large customer 60,000Small customer 100,000 Small customer 20,000
Content 10% (% of License) Maintenance 15% (% of License)Large customer 30,000 Large customer 45,000Small customer 10,000 Small customer 15,000
ExpensesMaintenance Renewal - includes annual content updates, software updates, and bug fixesContent Purchases 20% of Large Customers Buy ContentContent Purchases 50% of Small Customers Buy ContentCOGS: 20% of New license Revenues (mostly sales commissions)R&D 20% of New license RevenuesS&M 20% of Total Gross RevenuesTaxes 40%
Market Share Penetration Estimates20% market share large customers10% market share small customers
Unit Sales Projections22i ZQQ 224 2Q
# New Licenses Sold large customer 5 8 12 19 25
small customer 10 25 50 90 150
# CustomIzation Sold large customer 5 8 12 19 25small customer 10 25 50 90 150
# Content Sold large customer 1 2 2 4 5
small customer 2 5 10 18 30
# Maintenance Sold large customer 5 8 12 19 25
small customer 10 25 50 90 150
It Maintenance Renewals large customer 5 13 25 44
small customer 10 35 85 175
INCOME STATEMENT
RevenuesLicenses large customer 1,500,000 2,400,000 3,600,000 5,700,000 7,500,000
small customer 1,000,000 2,500,000 5,000,000 9,000,000 15,000,000
Customization large customer 300,000 480,000 720,000 1,140,000 1,500,000
small customer 200,000 500,000 1,000,000 1,800,000 3,000,000
Content large customer 30,000 48,000 72,000 114,000 150,000
small customer 20,000 50,000 100,000 180,000 300,000
Maintenance large customer 225,000 585,000 1,125,000 1,980,000 3,105,000
small customer 150.000 525.000 1.275.000 2.625.000 4.875.000
Gross Revenues 3,425,000 7,088,000 12,892,000 22,539,000 35,430,000
Cost of Goods Sold (COGS) 500,000 980,000 1,720,000 2,940,000 4,500,000
Net Revenues 2,925,000 6,108,000 11,172,000 19,599,000 30,930,000Gross Margin 85% 86% 87% 87% 87%
Operating Expenses R&D 500,000 980,000 1,720,000 2,940,000 4,500,000
Sales and Mktg 685,000 1,417,600 2,578,400 4,507,800 7,086,000
General and Admin 1,982,775 3,576,048 4,707,348 6,175,926 7,584,944
Operating Income (242,775) 134,352 2,166,252 5,975,274 11,759,056
Taxes 0 0 823.132 2.390,110 4.703.622
Net Income (242,775) 134,352 1,343,121 3,585,165 7,055,434
STATEMENT OF CASH FLOWS
Net Income (242,775) 134,352 1,343,121 3,585,165 7,055,434Project Investment 1,623,198 0 0 0 0
Yearly Cash Flow (1,865,973) 134,352 1,343,121 3,585,165 7,055,434Cumulative Cash Row (1,865,973) (1,731,621) (388,501) 3,196,664 10,252,097Project NPV 4,919,754 (through 2005)Project IRR 77% (through 2005)Discount Rate 15%Payback Penod 3 years
68

Appendix F-6: Sensitivity Analysis
Gross Revenue
Aggressive scenarioBase scenarioConservative scenario
Net IncomeAggressive scenarioBase scenarioConservative scenario
Yearly Cash Flow
Aggressive scenarioBase scenarioConservative scenario
2001 2002 2003 2004 2005
4,932,000 10,815,000 17,557,000 28,065,000 40,629,000
3,425,000 7,088,000 12,892,000 22,539,000 35,430,000
2,740,000 6,465,000 10,017,000 17,172,000 24,865,000
2001 2002 2003 2004 2005
313,695 1,245,571 2,818,951 5,443,012 8,594,836
(242,775) 134,352 1,343,121 3,585,165 7,055,434
(590,775) (197,028) 1,154,237 2,473,721 4,327,747
2001 2002 2003 2004 2005
(1,309,503) 1,245,571 2,818,951 5,443,012 8,594,836
(1,865,973) 134,352 1,343,121 3,585,165 7,055,434
(2,213,973) (197,028) 1,154,237 2,473,721 4,327,747
Project NPVAggressive scenarioBase scenarioConservative scenario
Project IRRAggressive scenarioBase scenarioConservative scenario
2001-20059,041,8514,919,754
2,250,767
2001-2005168%77%45%
Cumulative Cash Flow 2001 2002 2003 2004 2005
Aggressive scenario (1,309,503) (63,932) 2,755,019 8,198,031 16,792,867
Base scenario (1,865,973) (1,731,621) (388,501) 3,196,664 10,252,097
Conservative scenario (2,213,973) (2,411,001) (1,256,764) 1,216,957 5,544,704
69
——
—_
_-
—_
—*
I-.
——
——
—— n
II rJ) C
C

Appendix G: List of Interviews
UMHS Internal- Doug Strong, Office of Executive Vice Provost for Medical Affairs- Deborah Rich, Manager, Customer Satisfaction Research- Glenn Hiller, Director, Medical School Infonnation Systems (MSIS)- Wayne Wilson, Assistant Director Information Technology (MSIS)- Tom Daily, UMH Managed Care Contracting- Tom Campbell, UMH Managed Care Contracting- Erica Hanns, Compensation, Assistant To the Dean - Medical School- Brian Athey, Virtual Human, Assistant Professor, Cell & Development Biology Dept- Jim Wooliscroft, Associate Dean and Director, Graduate Medical Education- Tim Pletcher, Director of Research and Business Information Systems- Jocelyn DeWitt, Chief Information Officer- Casey White, Director, Learning Resource Center- Elaine Brock, Associate Director - DRDA, Div of Research Devel & Admin- Ed Goldman, Medical Center Attorney, Office of the General Counsel- Kallie Michels, Assistant Director Hospital Public Relations- Linda Warren, Coordinator Nursing Service, UMH Ambulatory Care Nursing- Margaret Calarco, Associate Hospital Administrator- Mike Harrison, Director of Public Relations and Marketing Communications- Rashid Bashshur, Telemedicine, Project Director Clinical Information Systems- Sharon Sheldon, Patient Education and Community Health Promotion- Amy Mehaffie, Patient Education and Community Health Promotion- Kemp Ceise, Disease Management, Associate Chief; Division of Hematology-
Oncology, Associate Chair for Business Development - Department of InternalMedicine
- Doug Cox, Disease Management, Business Manager, Internal Medicine Department- Larry Warren, Executive Director-University Hospitals and Health Centers- Jack Billi, Associate Professor, Internal Medicine, Associate Dean, Clinical Affairs,
Medical School- Joe Fantone, educational curriculum, Assistant Professor, Internal Medicine
Department- Michelle Nypaver, Assistant Director of Emergency Medicine- Van Harrison, CME, Director of Academic Programs, Department of Medical
Education- Wayne Davis, Professor, Department of Medical Education- Tom Biggs, Interim Chief Financial Officer- Phil Hampton, Data Warehouse Services, MCIT
University of Michigan (non UMHS)- Brent Chrite, Ph.D., Co-Managing Director, Davidson Institute- Jeff Ogden, UM Intemet2 Coordinator, Merit- Ted Hanss, Director, Applications Development, Internet2- Graham Mercer, University of Michigan Business School (UMBS) Global MBA- Keith Crocker, UMBS Economics Department
71

- Dee Edington, Employee Health Programs- Jay Anand, Assistant Strategy Professor, School of Business
Outside University of Michigan- Ben Galbo, WebMD- Mike McNally, Medscape- Gene Murray, Midwest Sales Representative, Blackboard.com- Vie Strecher, Health Media
72
C BIBLIOGRAPHY
1. Advisory Board Daily Briefing, (2000, March 30).
2. Becker, D. (2000, January). Healthcare Consumerism Presentation, UMHS.
3. Billi, J. (1999, January). New Mode/for Health Care, Ford Global Healthcare
Management Conference.
4. Carrington, C. (2000, March 6). Top 10 Selections Honor the Best Telemedicine
Programs in the US, Telehealth Magazine.
5. Center for Applied Information Technology in Health Care Delivery and Education
(2000). Summary Document.
6. Computer Science and Telecommunications Board, National Research Council
(2000). Networking Health. Prescriptionsfor the Internet. Prepublication Copy.
National Academy Press, Washington, DC.
7. Congressional Information Service, Inc. (1999). Health Care Facilities and Services,
Statistical Abstract ofthe US.
8. Coyle, M. (2000, March 2). Bridging the Clinical Digital Divide. e-Healthcare
Leadership Roundtable.
9. Daniel, D. (2000, January 7). Learnsoft Launches Online University, Computing
Canada, 36.
10. Davis D, et. al. (1999). Impact of Formal Continuing Medical Education. JAMA.
282:867-874.
11. Department of Health and Human Services, www.hhs.gov.
12. Dun and Bradstreet, (1999, June 30). Business information Report: University of
Michigan.
13. Dunn, 5, (2000, March/April). The Virtualizing of Education, The Futurist, 34-3 8.
14.Edworthy, 5, (1999, August). Improving Medication Adherence through Patient
Education Distinguishing between Appropriate and Inappropriate Information.
Journal ofRheumatology.
15. E-Health Roundup: Newsflashes from Cyberspace. (1999, October 27). American
Health Line.
C 16. Forrester. Full Service Health Sites Arise-Action. (2000).
www.forrester.com/ER/Research/Report/Action.
73

17. Goldman Sachs, (1999, December). Healthcare Information Technology, InvestmentResearch Report.
18. Goldman Sachs, (1999, May 28). Entrust technologies: The One to Own in PM,Investment Research Report.
19. Goldman Sachs, (1999, November 11). Health-e Opportunities in Health?, InvestmentResearch Report.
20. Goldman Sachs, (2000, March 14). 12 Technologies Company Profile.
21. Health Insurance Sourcebook: Basic Information A bout Managed CareOrganizations and Traditional Fee-for-Service Insurance, (1997). Omnigraphics.Detroit, Michigan.
22. Healtheon Presentation, (1999, May).
23. Hospitals Statistics, (1999). Healthcare Info Source. Chicago, Illinois.
24. htt:/!thomas.1oc.gov,’horne/thornas.htm1
25. Katzman, C. (2000, January 31). Web Wise; Leading-edge Providers Take Internet toits Limits Modern Healthcare.
} 26. Leaffer, T. (2000, January). The Internet: an Underutilized Tool in Patient Education,Computers in Nursing.
27. Mangan, K. (2000, February 25). Teaching Surgery Without a Patient, The Chroniclefor Higher Education, 49-50.
28. Maquire, P. (2000, March). Medicine Eyes Market for Online Health Information,Computers & Medicine, 8-9.
29. Messmer, E. (2000, January). Net Security Firms Baltimore, Cybertrust Unite,Network World, 14-15.
30. Morgan Stanley Dean Witter, (2000, March 14). Ariba: In the Sweet Spot, EquityResearch Report.
31. Nathan R., (1994, June). Patient Interest in Receiving Audiotapes of InformationPresented by Their Physicians, Archives ofFamily Medicine.
32.Networking Health: Prescriptions for the Internet, (2000). National Research Council.
33. Patients Reports of Counseling on Mammography Screening by Health CareProviders, (1999). JAMA.
34. Penn, M. (2000, February 28). Going for the Whin, Business and Technology, 20-22.
74

35. Physician Survey, MAP Team, (2000).
36. Reid, C. (2000, February 28). Ubell Builds Web Program at Stevens, PublishersWeekly, 18-20.
37. Routine Communication in STD Clinics (1999, May). American Journal ofPublicHealth.
38. Sanders, 3. (2000, March 6). Moving Forward, Looking back: Telemedicine in theYear Ahead. Telehealth Magazine.
39. Spanier, G. (2000, February 1). Today’s University: Five Issues That Affect theFuture of a Nation Vital Speeches ofthe Day; New York.
40. The Picker Institute, (1999, October). University of Michigan Health System AdultInpatient Report.
41. Wilson, T. (1995). Creating a Stake in the Business. Innovative Reward Systemsforthe Changing Workplace. McGraw-Hill, Inc. New York. 1995.
42. www.aamc.org
43. www.ariba.com/corp/AribaSo1utions/overview.asp
J 44. www.aspectdv.com/services.htm1
45. www.comnierceone.com
46. www.entrust.com
47.www.forbes.comlasap/99/0405/tearsheet.asp?rank=5&category=software
48. www.forrester.conilER!Research!ReportlAction
49. www.hcfa.gov
50. www.hoovers.com
51. www.intel.com/pressroom
52. www.internet2.edu
53. www.mayo.edulmcs
54. www.med.umich.edulopm/newspage/details.htm
55. www.nces.ed.gov/fastfacts/
56. www.telehea1thmag.com
75

57. www.verisign.com
58. Yasin, R. (1999, June 21). More Building Blocks for Secure E-Biz, Internetweek, 33.
59. Yasin, R. (2000, March 20). VeriSign, NSI Deal Has Bright Future, ComputerReseller News, 64.
60. Young, J. (2000, February 18). Instructor Takes Steps to Enliven Online Class, TheChroniclefor Higher Education, 54-55.
76


















