
EHealth Meeting, Washington DC 18 November 2011 M. Carolina Danovaro, MD, MSc Regional Immunization...
38
eHealth Meeting, Washington DC 18 November 2011 M. Carolina Danovaro, MD, MSc Regional Immunization Advisor – PAHO eHealth for Immunization Programs in the American Region
-
Upload
derek-harrington -
Category
Documents
-
view
214 -
download
0
Transcript of EHealth Meeting, Washington DC 18 November 2011 M. Carolina Danovaro, MD, MSc Regional Immunization...

eHealth Meeting, Washington DC18 November 2011
M. Carolina Danovaro, MD, MScRegional Immunization Advisor – PAHO
eHealth for Immunization Programs in the American
Region

eHealth for ImmunizationeHealth for Immunization
Record management systems, mobile technology, technology for identification, barcodes, and multimedia, provide potentially useful tools to improve:
– immunization and surveillance data collection, quality, and timeliness of reporting;
– individualized follow-up of schedules; – monitoring of events supposedly attributable to vaccines
and immunization (ESAVI); – continuing education and training; – social mobilization, and – a more efficient management of vaccines and other
supplies, and the cold chain

eHealth for ImmunizationeHealth for Immunization
Immunization Information Systems– Nominal Immunization Registries– Systems for monitoring events supposedly attributable to
vaccines and immunization – Vaccine and supply stock management
Tools for training and for social communication– Multimedia– Web 2.0

TAG Recommendations 2009TAG Recommendations 2009
TAG reaffirms the recommendation (since 2002) that systematic and periodic assessment of coverage data accuracy, consistency, completeness, and timeliness should become a regular activity within national immunization programs.
– This assessment should be conducted within the context of regular on-going evaluation and supervisory activities.
Monitoring numerator trends by month and year and calculating drop-out rates between all doses, including DTP2, and monitoring denominator variations should be done systematically at all levels.
Immunization programs should be aware of the conduction of surveys that, among other health indicators, calculate vaccination coverage in order to ensure that questionnaires are adequate and interviewers properly trained to assess vaccination status, and that the results are internally consistent between biologicals.

TAG Recommendations 2009TAG Recommendations 2009
Countries using national computerized nominal immunization registries should document their experiences, successes, and lessons learned in order to share them with other countries – Re-issued in 2011
PAHO should continue supporting countries to improve their immunization data quality by promoting the evaluation of the quality of their immunization data and information systems.
– PAHO should also support the implementation follow-up of the recommendations resulting from such assessments.
PAHO’s immunization program should develop guidelines regarding coverage monitoring and data quality, and establish strategic alliances with entities specializing in vital statistics and demography to promote the generation and availability of accurate denominators figures to calculate vaccination coverage.

Current Systems to Monitor Vaccination Coverage
Current Systems to Monitor Vaccination Coverage
Example of EPI Data FlowExample of EPI Data Flow
• Vaccination Registry in forms predetermined by variables of:• Age• Sex• Vaccine• Dose• Region of residency
Local Level (Post/Health Center/all sectors)
Weekly (monthly in remote areas) flow, from the local to national levelInformation includes data from weekend and is reported on Tuesday

Vaccination CardsVaccination Cards

Tally sheets or equivalentTally sheets or equivalent

Individual Nominal RecordsIndividual Nominal Records
Dockets or other clinical chartDockets or other clinical chart


Computerized systems for number of doses
Computerized systems for number of doses

Monthly
aggregated
Reports
HEALTH
CENTER
District
NATIONAL
LEVEL
Monthly
aggregated
Reports
RegistersTally SheetsClinic CardMCH Month Reports
Example of EPI Data Flow
PRIVATE
PRACTITIONERSBy 5th working day of the following month
RevisedDenominators
Denominators
Quarterly feedback
Second week of the following month

Computerized Nominal Immunization Registries (NIRs)
Computerized Nominal Immunization Registries (NIRs)



HEALTH FACILITY
DISTRICTPrivate Sector
NGOs
Social Security
Informe
MensualNominal
Registry
Nominal
Registry
Other vacc. providers
Na
tion
al C
om
pu
teri
zed
N
om
inal
Imm
un
iza
tion
Re
gis
try
SUB-NATIONAL
NACIONAL

Topic of current interestTopic of current interest
Dec 2010 – European meeting on nominal imm. registriesJan 2011 – Bill Gates raises the issue of mobile technologiesFe 2011 – PAHO workshop on nominal immunization registries

James L. Goddard, M.D., M.P.H., 8th CDC Director,
1962 – 1966CDC Public Health Image Library (PHIL)
“…perhaps in the rather distant future, the capabilities of electronic computers for storing and retrieving information could greatly facilitate our immunization programs…A nationwide computer system could put us well on the road to efficient national follow-up of births for maintenance of immunization levels.”
2nd National Immunization Conference, 1965
Topic “dreamt about” in the 1960’sTopic “dreamt about” in the 1960’s

Information for action:– Appointments, (SMS) recall-reminders– Deal with migration and internal mobility– Lot tracking down to people receiving the vaccine– Vaccination records can be printed– Integration with epi surveillance and other health data
• Cohort studies vaccine effectiveness and safetyAllows a detailed analysis of who is not getting vaccinated,
facilitating developing tailored strategiesAllows detailed analysis of vaccination timeliness (more
and more important to maximize vaccination benefits)
Expected Benefits of Imm. Info SystemsExpected Benefits of Imm. Info Systems

Expected Benefits of Imm. Info SystemsExpected Benefits of Imm. Info Systems
Data Quality:– Better, more complete and timely data
Dynamic monitoring of vaccination coverage by cohort (rather than annual targets) – If exhaustive registry
– More precise monitoring of vaccinated people by facility may improve vaccine and supply forecast and stock management
Supply chain management – vaccines in the right place at the right time
If well designed and implemented, may be easy to use and well accepted and can make data collection at point of vaccination more efficient
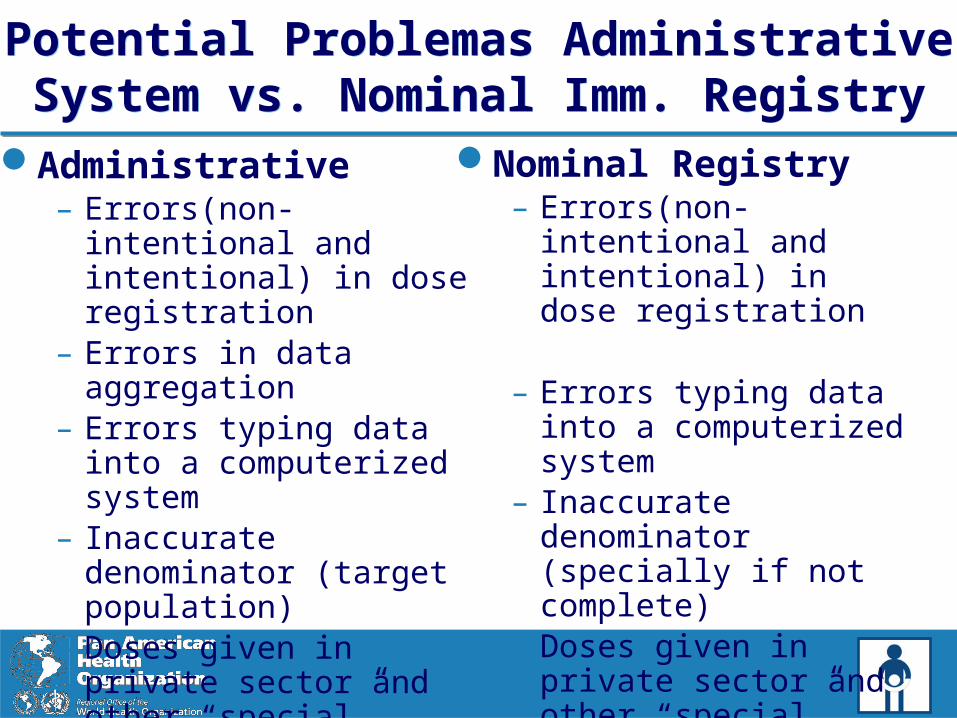
Potential Problemas Administrative System vs. Nominal Imm. RegistryPotential Problemas Administrative System vs. Nominal Imm. Registry
Administrative– Errors(non-intentional and
intentional) in dose registration
– Errors in data aggregation– Errors typing data into a
computerized system– Inaccurate denominator
(target population)– Doses given in private
sector and other “special” sectors not included
Nominal Registry – Errors(non-intentional and
intentional) in dose registration
– Errors typing data into a computerized system
– Inaccurate denominator (specially if not complete)
– Doses given in private sector and other “special” sectors not included

Challenges – Nominal Imm. RegistriesChallenges – Nominal Imm. Registries
Costs – development, implementation and maintenance Need for frequent updates Training, training, training Time for data entry – particularly new records Acceptability and transition from current systems to nominal
ones (current systems “work”) Risk of having an incomplete registry Data flow and data security: where to enter the data, (hardware,
maintenance, security), data transmission (connectivity) or timely database consolidation if not on-line, managing duplicates
Confidentiality – risks of misuse of personal data

Linking mHealth to Nominal Imm. Registries
Linking mHealth to Nominal Imm. Registries
Data entry– For other interventions, evidence that improves data quality
and time– May reduce number of records completed at time of
vaccination
Recall-reminder systems for immunization– Proven to work in developed countries– For other interventions, evidence that sending SMS reduces
missed appointments

Mobile Services Evolution 2008-2018, Chetan Sharma, June 2008
Mobile Use Distribution1998-2018
Global Penetration 5% 55% 96%
3G+ penetration 0% 18% 90%
Speed <50Kpbs Up to 2 Mbps Up to 1 Gbps
Dispositive cost $200 $130 <$20
Smartphone penetration
<1% 10% 40%
Battery life time avg. 2 hours 2.5 hours 24 hours
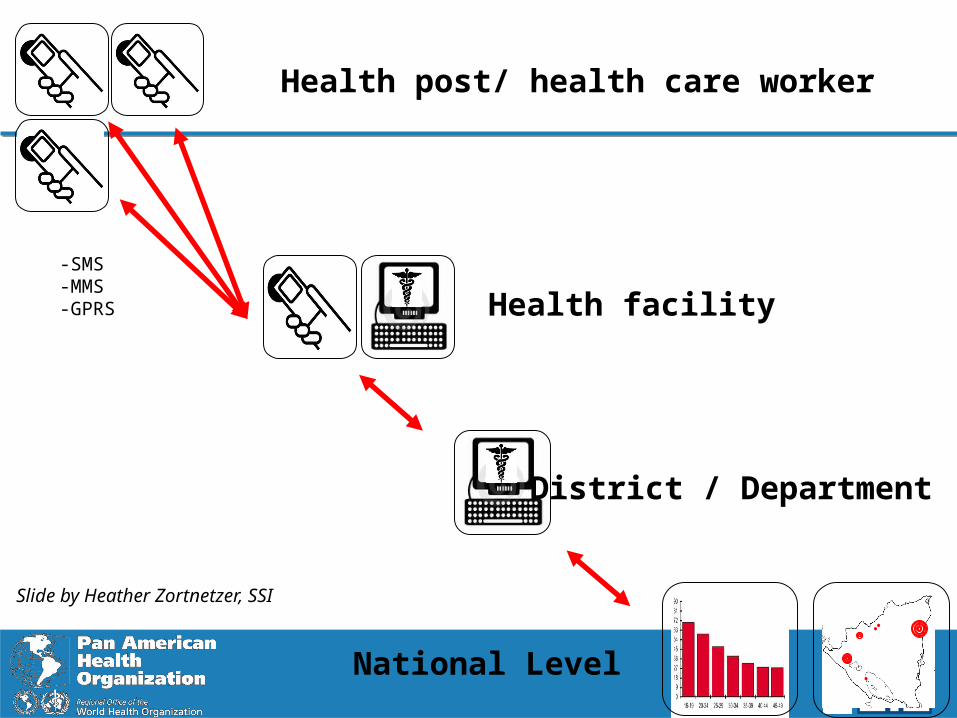
Health post/ health care worker
Health facility
District / Department
National Level
-SMS-MMS-GPRS
Slide by Heather Zortnetzer, SSI

Access to DataAccess to Data
I.I.S.1. Web application 2. Mobile application
3. Paper flow
Slide by Jan Grevendonk, PATH

Mobile use for Recall-RemindersMobile use for Recall-Reminders
IIS
National Database Engine (YAWL) Mobile ap(openXdata)
Info on people vaccinated
Message management by schedules
Slide by Jan Grevendonk, PATH

mVAC consorcio
mHealth+immunization: examples
• 2 countries- Ghana, India
• Based on mobile phones and open source code
• Focus on maternal-child health
• back end = OpenMRS
• primary users include HCWs and families
• Linked to birth registration
• Collaboration: Ghana Health Service, Grameen Foundation,
• Columbia U., U. Southern Maine
• $ = Gates Foundation
MoTECH
• Several sites in 5+ countries- Norway, Pakistan, India, Uganda, Nicaragua
• Based on mobile phones and PDAs and open source code
• Focused on cold chain and stock management
• Flexible and interoperable with other registries and back-end systems
• Some tools integrate with OXD (barcode, GPS, etc.)
• Several primary users
• Coordinated by Bergen University, Norway
• $ = Norwegian Research Council
Slide by Heather Zortnetzer, SSI
Looking to the Future – TAG Recommendations 2011
Looking to the Future – TAG Recommendations 2011
TAG welcomes the progress on the development and implementation of national computerized nominal immunization registries (NIRs) in the Region.
Countries and PAHO should continue documenting and exchanging experiences on the development and implementation of computerized NIRs
NIRs should aim at ensuring interoperability with other information systems.
PAHO should work in coordination with other sectors and initiatives related to e-government, information and communication technologies (ICTs), birth registration, among others.
Next StepsNext Steps
Consolidating and documenting the experiences using NIRs in the Americas
Linking NIRs with other immunization info systems– Vaccine stock management, ESAVI monitoring, surveillance
Evaluating their effectiveness and cost-effectivenessWorking on a framework that takes into consideration
PAHO’s eHealth resolutionImplementing pilots for mHealth solutionsEvaluating use of biometrics for unique identification
Acknowledgments Acknowledgments
Countries of the Americas– In particular, immunization programs
PAHO Immunization colleagues
Jan Grevendonk, PATH
Heather Zortnetzer, SSI
WHO colleagues– In particular, Marta Gacic-Dobo, Tony Burton
Global Immunization Division, CDC

THANK YOU!THANK YOU!
www.paho.org/immunization
Visit PAHO’s Immunization Newsletter: www.paho.org/inb

Electronic Health Record Status, USA 2007 Electronic Health Record Status, USA 2007
DesRoches et al published “Electronic Health Records in Ambulatory Care – A National Survey of Physicians” in NEJM in July 2008 and concluded that of about 1,800 physicians surveyed:
– EHRs were more prevalent with younger physicians; larger practices; and in the western United States.
– < 20% of the physicians responding to the survey had a fully functional or basic EHR.
– Barriers to adoption of EHRs included: cost; ability to meet practice needs; ROI; and application life cycle.
– Facilitators to adoption of EHRs included: incentives for purchase; payment for use; and liability protection.

• President Obama’s administration introduced the HITECH Act which was passed by Congress in 2009 to support the adoption and use of Electronic Health Records (EHRs)
• The purpose of HITECH is to achieve significant improvements in care through meaningful use of EHRs by health care providers.
• Established incentive payments to eligible professionals and hospitals to promote the adoption and meaningful use of interoperable HIT and qualified electronic health records (EHRs)
Health Information Technology for Economic and Clinical Health Act (HITECH)
Health Information Technology for Economic and Clinical Health Act (HITECH)
PAHO strategies to improve vital statistics and health information systems
PAHO strategies to improve vital statistics and health information systems
2007: PAHO RESOLUTION CSP27.R12 – Strategy For Strengthening Vital And Health Statistics in the Countries of the Americas
–http://www.paho.org/english/gov/csp/csp27.r12-e.pdf
2008: PAHO RESOLUTION CD48.R6 – Regional Plan of Action for Strengthening of Vital and Health Statistics
–http://www.paho.org/english/gov/cd/cd48.r6-e.pdf
2011: PAHO RESOLUTION CD51. eHealth2011: PAHO plan for the implementation of the recommendations from the
Commission on Information and Accountability for MCH (recomm 1-3)Initiatives: Several alliances to assess and improve health info systems in
the Americas (HMN, MEASURE-Evaluation, USAID, HMN-TSP, PRISM)PAHO cooperation with ECLAC (Latin America and Caribbean
Demographic Center)–Data use, analysis and revision of population estimates and mortality tables


















