Efficacy of Clopidogrel Reloading in Patients With Acute Coronary Syndrome Undergoing Percutaneous...
7
Efficacy of Clopidogrel Reloading in Patients With Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention During Chronic Clopidogrel Therapy (from the Antiplatelet therapy for Reduction of MYocardial Damage during Angioplasty [ARMYDA-8 RELOAD-ACS] Trial) Giuseppe Patti, MD a, *, Vincenzo Pasceri, MD b , Fabio Mangiacapra, MD a , Giuseppe Colonna, MD c , Vincenzo Vizzi, MD a , Elisabetta Ricottini, MD a , Antonio Montinaro, MD c , Andrea D’Ambrosio, MD a , William Wijns, MD d , Emanuele Barbato, MD d , and Germano Di Sciascio, MD a , on behalf of the ARMYDA-8 RELOAD-ACS Investigators Whether an additional clopidogrel load in patients receiving chronic clopidogrel therapy and undergoing percutaneous coronary intervention (PCI) for acute coronary syndrome (ACS) is associated with clinical benefit has not been well characterized. The aim of the present study was to evaluate, in a randomized protocol, the safety and effectiveness of clopidogrel reload for patients with ACS undergoing PCI in the background of chronic clopidogrel therapy. A total of 242 patients with noneST-segment elevation ACS with >10 days of clopidogrel therapy randomly received a 600-mg loading dose of clopidogrel 4 to 8 hours before PCI (n [ 122) or placebo (n [ 120). The primary end point was the 30-day incidence of major adverse cardiac events (death, myocardial infarction, target vessel revascularization). The primary end point occurred in 4.1% of patients in the reload arm versus 14.1% in the placebo arm (odds ratio 0.26, 95% confidence interval 0.10 to 0.73, p [ 0.013). This benefit in the reload arm was mainly from the prevention of periproce- dural myocardial infarction (4.1% vs 13%, p [ 0.02) and was paralleled by lower peri- procedural platelet reactivity. The aggregometry data were consistent with the clinical outcome. No difference was found in the bleeding outcomes between the 2 groups. In conclusion, the results from the Antiplatelet therapy for Reduction of MYocardial Damage during Angioplasty (ARMYDA-8 RELOAD-ACS) trial have shown a significant clinical benefit from reloading patients with ACS receiving chronic clopidogrel therapy before PCI. These data might be relevant in clinical practice, given the large number of patients with ACS who are still currently treated with clopidogrel during PCI. Ó 2013 Elsevier Inc. All rights reserved. (Am J Cardiol 2013;-:-e-) The prevalence of patients undergoing percutaneous coronary intervention (PCI) receiving chronic clopidogrel therapy is relatively high, owing to previous drug-eluting stent implantation, acute coronary syndrome (ACS) during the preceding year, or staged PCI procedures. An interindi- vidual variability in the clopidogrel response has been largely demonstrated, and patients with low drug responsiveness have a poorer outcome after PCI. 1e3 Previous studies have shown that an additional 600-mg clopidogrel loading dose in patients receiving chronic therapy is associated with addi- tional inhibition of residual platelet reactivity and a reduction of nonresponders. 4 However, whether this pharmacodynamic benefit translates into improvement in the clinical outcomes has not been definitely characterized. 5 A clinical benefit from an additional loading dose with 600 mg clopidogrel in patients with ACS undergoing PCI while receiving chronic clopidogrel therapy was demonstrated in the prespecified subgroup analysis of the randomized Antiplatelet therapy for Reduction of MYocardial Damage during Angioplasty (ARMYDA-4 RELOAD) trial, 6 but this was not observed in a more recent, nonrandomized, retrospective investigation. 7 Thus, given those discrepancies, we designed a specific, prospective, randomized trial to evaluate the effectiveness and safety of a strategy of a 600-mg clopidogrel reload dose in patients with ACS undergoing PCI while receiving chronic clopidogrel therapy. The Clinicaltrials.gov number was 2011-005449-11. Methods The ARMYDA-8 RELOAD-ACS trial was a multicenter, unfunded, randomized, double-blind, clinical trial per- formed at 4 institutions (Campus Bio-Medico University of a Department of Cardiovascular Sciences, Campus Bio-Medico University of Rome, Rome, Italy; b Interventional Cardiology Unit, San Filippo Neri Hospital, Rome, Italy; c Interventional Cardiology Unit, Vito Fazzi Hospital, Lecce, Italy; and d Cardiovascular Center, OLV Hospital, Aalst, Belgium. Manuscript received December 21, 2012; revised manu- script received and accepted March 6, 2013. See page 6 for disclosure information. *Corresponding author: Tel: (þ39) 06-22-541-1612; fax: 06-22-541-1638. E-mail address: [email protected] (G. Patti). 0002-9149/13/$ - see front matter Ó 2013 Elsevier Inc. All rights reserved. www.ajconline.org http://dx.doi.org/10.1016/j.amjcard.2013.03.008
Transcript of Efficacy of Clopidogrel Reloading in Patients With Acute Coronary Syndrome Undergoing Percutaneous...

Efficacy of Clopidogrel Reloading in Patients With Acute CoronarySyndrome Undergoing Percutaneous Coronary Intervention During
Chronic Clopidogrel Therapy (from the Antiplatelet therapyfor Reduction of MYocardial Damage during Angioplasty
[ARMYDA-8 RELOAD-ACS] Trial)
Giuseppe Patti, MDa,*, Vincenzo Pasceri, MDb, Fabio Mangiacapra, MDa, Giuseppe Colonna, MDc,Vincenzo Vizzi, MDa, Elisabetta Ricottini, MDa, Antonio Montinaro, MDc, Andrea D’Ambrosio, MDa,
William Wijns, MDd, Emanuele Barbato, MDd, and Germano Di Sciascio, MDa,on behalf of the ARMYDA-8 RELOAD-ACS Investigators
Whether an additional clopidogrel load in patients receiving chronic clopidogrel therapy
aDepartmentUniversity of RomFilippo Neri HospFazzi Hospital, LeAalst, Belgium. Mscript received and
See page 6 for*CorrespondinE-mail address
0002-9149/13/$ -http://dx.doi.org/1
and undergoing percutaneous coronary intervention (PCI) for acute coronary syndrome(ACS) is associated with clinical benefit has not been well characterized. The aim of thepresent study was to evaluate, in a randomized protocol, the safety and effectiveness ofclopidogrel reload for patients with ACS undergoing PCI in the background of chronicclopidogrel therapy. A total of 242 patients with noneST-segment elevation ACS with>10 days of clopidogrel therapy randomly received a 600-mg loading dose of clopidogrel4 to 8 hours before PCI (n [ 122) or placebo (n [ 120). The primary end point was the30-day incidence of major adverse cardiac events (death, myocardial infarction, targetvessel revascularization). The primary end point occurred in 4.1% of patients in the reloadarm versus 14.1% in the placebo arm (odds ratio 0.26, 95% confidence interval 0.10 to 0.73,p [ 0.013). This benefit in the reload arm was mainly from the prevention of periproce-dural myocardial infarction (4.1% vs 13%, p [ 0.02) and was paralleled by lower peri-procedural platelet reactivity. The aggregometry data were consistent with the clinicaloutcome. No difference was found in the bleeding outcomes between the 2 groups. Inconclusion, the results from the Antiplatelet therapy for Reduction of MYocardial Damageduring Angioplasty (ARMYDA-8 RELOAD-ACS) trial have shown a significant clinicalbenefit from reloading patients with ACS receiving chronic clopidogrel therapy before PCI.These data might be relevant in clinical practice, given the large number of patients withACS who are still currently treated with clopidogrel during PCI. � 2013 Elsevier Inc. Allrights reserved. (Am J Cardiol 2013;-:-e-)
The prevalence of patients undergoing percutaneouscoronary intervention (PCI) receiving chronic clopidogreltherapy is relatively high, owing to previous drug-elutingstent implantation, acute coronary syndrome (ACS) duringthe preceding year, or staged PCI procedures. An interindi-vidual variability in the clopidogrel response has been largelydemonstrated, and patients with low drug responsivenesshave a poorer outcome after PCI.1e3 Previous studies haveshown that an additional 600-mg clopidogrel loading dose inpatients receiving chronic therapy is associated with addi-tional inhibition of residual platelet reactivity and a reduction
of Cardiovascular Sciences, Campus Bio-Medicoe, Rome, Italy; bInterventional Cardiology Unit, Sanital, Rome, Italy; cInterventional Cardiology Unit, Vitocce, Italy; and dCardiovascular Center, OLV Hospital,anuscript received December 21, 2012; revised manu-accepted March 6, 2013.disclosure information.g author: Tel: (þ39) 06-22-541-1612; fax: 06-22-541-1638.: [email protected] (G. Patti).
see front matter � 2013 Elsevier Inc. All rights reserved.0.1016/j.amjcard.2013.03.008
of nonresponders.4 However, whether this pharmacodynamicbenefit translates into improvement in the clinical outcomeshas not been definitely characterized.5 A clinical benefit froman additional loading dose with 600 mg clopidogrel inpatients with ACS undergoing PCI while receiving chronicclopidogrel therapy was demonstrated in the prespecifiedsubgroup analysis of the randomized Antiplatelet therapy forReduction of MYocardial Damage during Angioplasty(ARMYDA-4 RELOAD) trial,6 but this was not observed ina more recent, nonrandomized, retrospective investigation.7
Thus, given those discrepancies, we designed a specific,prospective, randomized trial to evaluate the effectivenessand safety of a strategy of a 600-mg clopidogrel reload dosein patients with ACS undergoing PCI while receiving chronicclopidogrel therapy. The Clinicaltrials.gov number was2011-005449-11.
Methods
The ARMYDA-8 RELOAD-ACS trial was a multicenter,unfunded, randomized, double-blind, clinical trial per-formed at 4 institutions (Campus Bio-Medico University of
www.ajconline.org

ARMYDA-8 RELOAD-ACS: Study design
Figure 1. Design of ARMYDA-8 RELOAD-ACS trial. MI ¼ myocardial infarction; NSTE ¼ noneST-segment elevation; TVR ¼ target vesselrevascularization.
2 The American Journal of Cardiology (www.ajconline.org)
Rome, Rome, Italy; Vito Fazzi Hospital, Lecce, Italy; SanFilippo Neri Hospital, Rome, Italy; and OLV Hospital,Aalst, Belgium).
By protocol, patients were eligible if they were receivingchronic (>10 days) therapy with clopidogrel (75 mg/day) andhad noneST-segment elevation ACS. NoneST-segmentelevation ACS was defined as symptoms of coronaryischemia <24 hours before hospital admission and �1 ofthe following findings: troponin or creatine kinase-MB(CK-MB) values greater than the upper limit of normal, ornew ST-segment depression >0.1 mV, or transient ST-segment elevation (<30 minutes)>0.1 mV in�2 contiguousleads. Excludedwere the patients undergoing primary PCI forST-segment elevation acute myocardial infarction, witha platelet count<70� 109/L, coronary bypass grafting in theprevious 3 months, chronic warfarin therapy, bleedingdiathesis, or major bleeding for <4 weeks. The design of thestudy is illustrated in Figure 1. A total of 271 patients ful-filling the enrollment criteria were randomized 4 to 8 hoursbefore diagnostic angiography to receive an additional600-mg clopidogrel loading dose (n ¼ 136) or placebo(n ¼ 135). The eligible patients were assigned to the alloca-tion arm using an electronic spreadsheet indicating the group
assignment by random number. Randomization blocks werecreated and distributed to all centers; in each center, theinvestigators involved in the process of the randomizationassignment were not involved in performing PCI orthe follow-up evaluations. After coronary angiography,29 patients (14 in the reload arm and 15 in the placebo arm)without an indication for PCI were excluded from the presentstudy (19 were treated medically and 10 underwent bypasssurgery). Thus, a total of 242 patients receiving “ad hoc” PCIimmediately after coronary angiography were enrolled andrepresent the study population. Of these 242 patients, 122were randomized to the 600-mg clopidogrel reloading doseand 120 to placebo. The physicians performing PCI were notaware of the randomization allocation.
All interventions were performed using a standard tech-nique. Glycoprotein IIb/IIIa inhibitors were used at theoperator’s discretion in both arms. All patients were takingaspirin at PCI. After the procedure, they received aspirin(100 mg/day) indefinitely. Clopidogrel was continued(75 mg/day) for 12 months, irrespective of the randomiza-tion assignment.
Blood samples were drawn before intervention and 6 and24 hours after PCI to measure the CK-MB and troponin I

Table 1Main clinical features
Variable ClopidogrelReload (n ¼ 122)
Placebo(n ¼ 120)
p Value
Age (yrs) 66 � 11 66 � 12 1Men 94 (77) 84 (70) 0.2Diabetes mellitus 33 (27) 37 (31) 0.6Systemic hypertension* 86 (70) 95 (79) 0.1Hypercholesterolemia† 82 (67) 76 (63) 0.6Current smoker 31 (25) 32 (27) 0.9BMI (kg/m2) 24.1 � 4.2 24.8 � 4.3 0.2Previous MI 23 (19) 36 (30) 0.052Previous PCI 29 (24) 44 (37) 0.036Previous coronary bypass 6 (5) 9 (7) 0.4Unstable angina pectoris 44 (36) 48 (40) 0.6NSTEMI 78 (64) 72 (60) 0.6LVEF (%) 57 � 9 56 � 9 0.4Multivessel coronary artery
disease53 (43) 55 (46) 0.8
Blood creatinine (mg/dl) 0.94 � 0.23 0.99 � 0.3 0.15TherapyAspirin 122 (100) 120 (100) 1Statins 110 (90) 102 (85) 0.2PPIs 67 (55) 77 (64) 0.18b Blockers 59 (48) 63 (52) 0.5ACE inhibitors 79 (65) 69 (57) 0.3
Data are presented as n (%) or mean � SD.ACE ¼ angiotensin-converting enzyme; BMI ¼ body mass index;
LVEF ¼ left ventricular ejection fraction; MI ¼ myocardial infarction;NSTEMI¼ noneST-segment elevation myocardial infarction; PPI¼ protonpump inhibitor.* Arterial pressure >160/90 mmHg.† Total cholesterol >200 mg/dl.
Table 2Procedural features
Variable ClopidogrelReload
(n ¼ 122)
Placebo(n ¼ 120)
pValue
Femoral access 122 (100) 120 (100) 1Coronary vessel treated 131 (100) 144 (100) eLeft main 1 (0.5) 2 (1.5) 1Left descending artery 56 (43) 66 (46) 0.6Left circumflex 34 (26) 35 (24) 0.8Right 39 (30) 38 (26) 0.6Saphenous vein graft 1 (0.5) 2 (1.5) 1Left internal mammary graft 0 1 (1) 1
Restenotic lesion 10 (8) 13 (11) 0.5Lesion type B2/C 82 (67) 76 (63) 0.6Chronic total occlusion (>3 mo) 3 (2) 3 (2) 1Multivessel coronary intervention 17 (14) 22 (18) 0.4Type of interventionBalloon only 6 (5) 6 (5) 1Stent 116 (95) 114 (95) 1
Bifurcation with kissing balloon 7 (6) 5 (4) 0.8Stents per patient (n) 1.3 � 0.8 1.3 � 0.9 1Stent diameter (mm) 2.9 � 0.9 2.9 � 0.9 1Total stent length (mm) 16.5 � 6 16 � 6 0.5Use of drug-eluting stent 57 (47) 52 (43) 0.6Direct stenting 49 (40) 42 (35) 0.4Predilation (n) 1.3 � 1.7 1.5 � 2 0.4Stent deployment pressure (atm) 12 � 4 12 � 4 1Duration of stent deployment (s) 21 � 8 21 � 9 1Total myocardial ischemia >120 s 23 (19) 25 (21) 0.7Use of postdilation 3 (2) 4 (3) 0.7Antithrombin regimen during
interventionBivalirudin 13 (11) 7 (6) 0.2Unfractionated heparin 109 (89) 113 (94) 0.3
Use of GPIIb/IIIa inhibitors(provisional)
14 (11) 19 (16) 0.3
Data are presented as n (%) or mean � SD.GP ¼ glycoprotein.
Coronary Artery Disease/Clopidogrel Reloading in Patients With ACS 3
(mass) values. Additional determinations were performed, ifclinically indicated. The measurements of CK-MB wereobtained using the Access 2 Immunochemiluminometricassay (Beckman Coulter, Fullerton, California). The normallimits were �3.6 ng/ml for CK-MB and �0.06 ng/ml fortroponin I. Patients treated at Campus Bio-Medico Univer-sity received platelet reactivity evaluation at baseline (4 to8 hours before intervention), in the catheterization labora-tory immediately before PCI and 6 and 24 hours after PCIusing the VerifyNow P2Y12 assay (Accumetrics, SanDiego, California). VerifyNow P2Y12 is a rapid, cartridge-based assay specifically measuring the direct effects ofclopidogrel on the platelet P2Y12 receptor.8,9 Themeasurement results are expressed as P2Y12 reaction units(PRU); the lower the PRU value, the greater the degree ofP2Y12 receptor inhibition by clopidogrel, and vice versa.Patients treated with glycoprotein IIb/IIIa inhibitors wereexcluded from the VerifyNow analysis, because these drugsinterfere with the PRU measurements.9,10
Clinical follow-up data were obtained at 30 days byoffice visits for all study patients. The physicians evaluatingthe patients during these follow-up visits were not aware ofthe randomization assignment. Each patient gave informedconsent for participation in the study. The institutionalreview board of the Campus Bio-Medico Universityapproved the study. The trial was not supported by anyexternal source of funding.
The primary end point of the ARMYDA-8 RELOAD-ACS trial was the 30-day incidence of major adverse cardiacevents (MACE; death, myocardial infarction, target vesselrevascularization). Periprocedural myocardial infarction wasdefined according to the pre-PCI clinical presentation. Forpatients with normal baseline CK-MB levels (i.e., under-going angioplasty for unstable angina), it was defined aspostintervention increases in CK-MB >3 � 99th percentileof the upper limit of normal.10 In patients with noneST-segment elevation myocardial infarction (i.e., elevatedbaseline CK-MB levels), a subsequent elevation of �50% ofthe baseline CK-MB value was applied to detect peri-procedural myocardial infarction.11 Target vessel revascu-larization included bypass surgery and repeat PCI of thetarget vessels.
The secondary end points were as follows: (1) theoccurrence of vascular or bleeding complications, includingmajor bleeding (intracranial bleeding or clinically overtbleeding associated with a decrease in hemoglobin >5 g/dl,according to the Thrombolysis In Myocardial infarctioncriteria12), minor bleeding (clinically overt hemorrhageassociated with a decrease in hemoglobin of �5 g/dl), and

% o
f p
atien
ts
600 mg Clopidogrel reload
Placebo
Composite primary end-point
30-day MACEIndividual components
0
3
6
9
12
15
18
4.1
0
3
6
9
12
15
18
0.8
13.3
4.1
Death MI TVR
P=0.012
% o
f p
atien
ts
14.1
ARMYDA-8 RELOAD-ACS: Primary end-point
Figure 2. Incidence of the primary end point in the 2 arms. MI ¼ myocardial infarction; TVR ¼ target vessel revascularization.
0.10 (0.01-0.73) 0.024
6.9 (0.88-54.9) 0.06
4.4 (1.2-15.9) 0.025
2.5 (0.91-6.7) 0.07
0.26 (0.10-0.73) 0.013
0 1 3 6 9 12
OR (95% CI) P
ARMYDA-8 RELOAD-ACS study
Figure 3. Multivariate analysis. CAD ¼ coronary artery disease; PPI ¼ proton pump inhibitors.
4 The American Journal of Cardiology (www.ajconline.org)
entry-site complications (hematoma >10 cm, pseudoaneur-ysm or arteriovenous fistula), and (2) the evaluation ofperiprocedural platelet reactivity at different points in the2 treatment arms using the VerifyNow assay.
In the ARMYDA-4 RELOAD study,6 subgroup analysisusing prespecified clinical subsets of patients with ACS,showed a MACE incidence of 6.4% in the reload arm versus16.3% in the placebo arm (odds ratio [OR] 0.34, multivar-iate analysis). For the sample size calculation of theARMYDA-8 RELOAD-ACS, we hypothesized a similar16% occurrence of MACE in the placebo group and asimilar 66% risk reduction in the clopidogrel reload arm.Thus, a study population of �240 patients would be neededto detect such a reduction with an a of 0.05 (2 tailed) anda b of 0.08.
Categorical variables are expressed as percentages andcontinuous variables as the mean � SD, unless otherwisespecified. Proportions were compared using Fisher’s exact test
when the expected frequencywas<5, otherwise the chi-squaretest (Yates’ corrected) was applied. Continuous variablesbetween the 2 armswere compared using the t test for normallydistributed values (as assessed by the Kolmogorov-Smirnovtest), otherwise, the Mann-Whitney U test was used. ORs and95% confidence intervals assessing the risk of the primary endpoint according to potential confounding variables wereassessed by logistic regression analysis. All variables listed inTables 1 and 2 were evaluated first in a univariate model, and,for those with p <0.15, in a multivariate logistic regressionanalysis. All calculations were performed using the StatisticalPackage for Social Sciences, version 12.0, and p <0.05(2 tailed) was considered significant.
Results
The clinical and procedural variables in the 2 arms arelisted in Tables 1 and 2, respectively. The timing of study

228±48
238±69244±93
221±92
199±86
224±51
185±90
172±83
Study drug PCI 6 hrs 24 hrs
120
140
160
180
200
220
240
260
PR
U
P=0.16
Placebo
Clopidogrel
600 mg
Placebo
Clopidogrel
reload
P=0.011
P=0.012
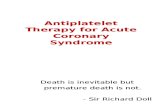
ARMYDA-8 RELOAD-ACS: Platelet aggregometry
Figure 4. Aggregometry data.
Coronary Artery Disease/Clopidogrel Reloading in Patients With ACS 5
drug administration versus placebo before PCI (6 � 0.4 vs6 � 0.5 hours, p ¼ 0.89) and the prevalence of diabetesmellitus (27% vs 31%), noneST-segment elevationmyocardial infarction (64% vs 60%), and the use of drug-eluting stents (47% vs 43%) were similar. The largemajority of patients were receiving statin therapy at PCI(90% vs 85%). The mean duration of chronic clopidogreltherapy was 5 months in both arms. In the overall studypopulation, the indication for chronic clopidogrel therapywas mainly previous ACS or drug-eluting stent implanta-tion, without differences in the prevalence of these indica-tions between the 2 arms. Among the initial population ofpatients meeting the enrollment criteria (n ¼ 271), aftercoronary angiography, 19 patients (7%) were excludedbecause they received medical therapy and 10 patients (4%)because they were deemed to require surgical revasculari-zation. Of the 10 patients treated with bypass surgery, 5were randomized to the reload arm, but they had no excessbleeding during the perioperative period. Among the 19patients treated medically because of nonsignificant coro-nary disease or disease not suitable for PCI, 10 wererandomized to the reload arm and 9 to the placebo arm; noneof the 19 patients had any additional events during the studyperiod.
In the overall population, procedural success, defined asresidual coronary stenosis <30%, was achieved in 239 of242 patients (120 of 122 in the reload arm [98.4%] and 119of 120 [99.2%] in the placebo arm, p ¼ 0.99). An unsuc-cessful procedure resulted from an inability to cross a totalocclusion in all cases. No-reflow phenomenon occurred in 4patients (1 in the reload and 3 in the placebo arm), whosuccessfully received intracoronary nitrates, adenosine, andglycoprotein IIb/IIIa inhibitors. No evident vessel or sidebranch (�2 mm) closure occurred when bifurcating lesionswere treated.
The incidence of the composite primary end point ofdeath, myocardial infarction, and target vessel revasculari-zation at 1 month was 4.1% (5 of 122 patients) in the reloadarm versus 14.1% (17 of 120) in the placebo arm (p ¼0.012; Figure 2). The occurrence of 30-day MACE wasessentially owing to periprocedural myocardial infarction inboth arms: 5 of 122 patients (4.1%) versus 16 of 120 (13%;p ¼ 0.02). The rates of large periprocedural myocardialinfarction, defined as post-PCI CK-MB elevation 5 times the
upper limit of normal, were also lower in the reload arm(0.8% vs 7.5%; p ¼ 0.022). One patient in the placebogroup experienced sudden cardiac death 7 days after theindex procedure. No patient required emergency coronaryartery bypass surgery or repeat PCI within 30 days. Multi-variate logistic regression analysis showed that clopidogrelreload was an independent predictor of a decreased risk ofMACE at 1 month (OR 0.26, 95% confidence interval 0.10to 0.73, p ¼ 0.013; Figure 3). The risk of events was alsolower in male patients (OR 0.10, 95% confidence interval0.01 to 0.73, p ¼ 0.024) and was greater in patientsreceiving proton pump inhibitors (OR 4.4, 95% confidenceinterval 1.2 to 15.9, p ¼ 0.025).
No patient in the present study had major bleeding orrequired transfusions. Minor bleeding occurred in 2.5% ofpatients (3 of 122) in the reload arm versus 3.3% (4 of 120)of those in the placebo arm (p ¼ 0.98). Minor bleedingincluded 3 urethral bleeding events, 1 conjunctival bleedingevent, and 3 gum bleeding events. The incidence of hema-tomas >10 cm was 4% (5 of 122) versus 5% (6 of 120) inthe reload and placebo group, respectively (p ¼ 0.98). Incontrast, postintervention femoral arteriovenous fistulaswere observed in 1.6% (2 of 122) and 1.7% (2 of 120) ofpatients (p ¼ 0.63).
A total of 85 patients underwent a complete plateletreactivity evaluation, 44 in the reload group and 41 in theplacebo group (Figure 4). In the placebo arm, the PRUvalues at PCI remained essentially unchanged comparedwith baseline (224 � 51 vs 228 � 48, p ¼ 0.52), increasedat 6 hours (244 � 93, p ¼ 0.05, vs baseline), and decreasedat 24 hours to levels similar to those at baseline (221 � 92,p ¼ 0.67). After clopidogrel reload, the platelet reactivity atPCI was significantly attenuated compared with at baseline(199 � 86 vs 238 � 69 PRU, p ¼ 0.02), with an additionalprogressive decrease of PRU levels at 6 hours (185 � 90PRU, p ¼ 0.003, vs baseline) and 24 hours (172 � 83 PRU,p <0.0001). As a result, patients randomized to the clopi-dogrel reload arm had lower PRU levels (i.e., greater plateletinhibition) than the placebo arm at PCI and at both post-PCIdeterminations (Figure 4).
Discussion
The ARMYDA-8 RELOAD-ACS trial investigated theissue of whether an additional 600-mg clopidogrel loadingdose in the background of chronic clopidogrel therapywould provide a significant clinical benefit in patients withnoneST-segment elevation ACS undergoing early PCI. Ourresults have indicated that in this setting a reloading strategyreduces the cumulative incidence of adverse events at 30days.
Previous studies have demonstrated that 600 mg clopi-dogrel in patients with coronary artery disease receiving thechronic 75 mg/day dose was associated with 68% additionalinhibition of adenosine diphosphate (5 mmol/L)-inducedplatelet aggregation at 6 hours4 and with a reduction ofinterindividual variability in the response to the drug.13 Thiscould be critical, because recent data have shown that thedegree of platelet reactivity with clopidogrel therapycorrelates with the clinical outcome after PCI, with anincreased risk of cardiac events, including stent thrombosis,

Ch
Pri
InvCa
Sa
Vi
Ca
6 The American Journal of Cardiology (www.ajconline.org)
in patients with high on-treatment platelet reactivity.3 Therandomized ARMYDA-4 RELOAD trial included patientsreceiving chronic clopidogrel therapy receiving PCI fora variety of clinical syndromes and suggested that in thesubgroup of patients with ACS, a reloading strategy wasassociated with a 66% relative risk reduction of 30-dayMACE.6 This was a negative study in the overall compar-ison, and it was possibly underpowered for subgroup anal-ysis. A more recent investigation demonstrated no clinicalbenefit for clopidogrel reloading in patients receiving long-term clopidogrel therapy and undergoing coronary stentingfor ACS.7 However, this was a retrospective, single-centerstudy, and the results were not adjusted for possibleconfounders. Given these results, we specifically designeda prospective, multicenter, randomized protocol to clarifythis issue.
The results of the ARMYDA-8 RELOAD-ACS trial haveindicated that an additional 600 mg clopidogrel load given 6hours before PCI is associated with a lower incidence ofMACE at 1 month in patients receiving chronic clopidogreltherapy admitted for ACS. In particular, the risk reduction ofevents was 74% on multivariate analysis, and this clinicalbenefit on the composite end point was mainly driven by theprevention of periprocedural myocardial infarction. Theclinical value of periprocedural myocardial infarction asdetected by cardiac marker elevation, without symptoms orelectrocardiographic or echocardiographic changes, is notwell established. However, even small cardiac markerreleases are an expression of true infarction, as assessed bycontrast-enhanced magnetic resonance imaging, and mightnegatively affect the prognosis during follow-up.14,15 In thereload arm, the occurrence of periprocedural myocardialinfarction was lower, also considering the more specificdefinition of larger infarction (post-PCI CK-MB elevation 5times the upper limit of normal). Patients with ACS presentwith enhanced baseline platelet activity and an impairedresponse to standard doses of clopidogrel, with an increasedprevalence of high on-treatment platelet reactivity.16,17
Thus, an additional antiplatelet effect beyond that achievedwith the currently recommended maintenance dose of clo-pidogrel might be indicated before PCI for such patients toachieve a significant clinical benefit. Patients who developACS during dual antiplatelet therapy are potentially at evengreater risk of early ischemic events and might derive thegreatest benefit from “more aggressive” antiplatelet strate-gies (i.e., more liberal use of glycoprotein IIb/IIIa inhibitors,a switch to ticagrelor, or a reload dose with clopidogrel, ifticagrelor is contraindicated because of high bleeding risk).In the ARMYDA-8 RELOAD-ACS trial, the prevention ofperiprocedural ischemic events using a clopidogrel reload-ing dose was associated with attenuation of platelet reac-tivity at PCI that continued in the first hours after theprocedure. In contrast, as expected, in the placebo group,procedural platelet activation occurred, with a peak at 6hours, that was not observed in the active treatment arm.Our aggregometry data indicated that the periproceduraldegree of platelet inhibition in response to clopidogrel caninfluence the early outcome, with lower ischemic eventsparalleled by lower residual platelet reactivity in the reloadarm. Importantly, our study showed no increased bleedingrisk with the reload approach. These findings are reassuring,
considering the strong negative prognostic effect of peri-procedural hemorrhage.18 The administration of glycopro-tein IIb/IIIa inhibitors was limited in the ARMYDA-8RELOAD-ACS trial; therefore, the study did not drawconclusions about the bleeding risk if both reloading andglycoprotein IIb/IIIa inhibitors were used. Moreover, thedrug-eluting stent penetration was low (44%), reflecting thepractice patterns in Europe and centers involved in thepresent study.
The recent guidelines of the European Society ofCardiology on noneST-segment elevation ACS assigneda level of recommendation of 1B for prasugrel and tica-grelor, with clopidogrel recommended for patients whocannot receive prasugrel or ticagrerlor.19 Nevertheless, wedo not believe that the use of clopidogrel has been outdatedbecause of concerns related to major bleeding and cost.
Disclosures
The authors have no conflicts of interest to disclose.
Appendix
The following investigators participated in theARMYDA-8 RELOAD-ACS trial:
airman: Germano Di Sciascio, MD, Campus Bio-Medico University, Romencipal investigator: Giuseppe Patti, MD, CampusBio-Medico University, Romeestigators:mpus Bio-Medico University, Rome: AndreaD’Ambrosio, MD, Fabio Mangiacapra, MD,Vincenzo Vizzi, MD, Elisabetta Ricottini, MD,Annunziata Nusca, MD, Rosetta Melfi, MD, MarcoMiglionico, MD, Rocco Contuzzi, MD, PaoloGallo, MD.n Filippo Neri Hospital, Rome: Vincenzo Pasceri,MD,Giulio Speciale,MD,Christian Pristipino,MD,Massimo Santini, MD, Francesco Pelliccia, MD.to Fazzi Hospital, Lecce: Giuseppe Colonna, MD,Antonio Montinaro, MD, Luigi Cavallo, LuisellaSerafino, Dorella Pelagalli, Anita Stanga, PatriziaPetrachi, Pietro Montuori, Ramona Chiriatti,Patrizia Cascione, Maria Grazia Perrone, AnnaProtopapa, Lucia Martella, Emanuela Mele,Caterina Carlino.rdiovascular Center, OLV Hospital of Aalst: WilliamWijns, MD, Emanuele Barbato, MD, Bernard DeBruyne, MD, Jozef Bartunek, MD, Marc Vander-heyden, MD, Carlos Van Mieghem, MD, Aaron JPeace, MD.
1. Gurbel PA, Bliden KP, Hiatt BL, O’Connor CM. Clopidogrel forcoronary stenting: response variability, drug resistance, and the effectof pretreatment platelet reactivity. Circulation 2003;107:2908e2913.
2. Serebruany VL, Steinhubl SR, Berger PB, Malinin AI, Bhatt DL, TopolEJ. Variability in platelet responsiveness to clopidogrel among 544individuals. J Am Coll Cardiol 2005;45:246e251.
3. Brar SS, ten Berg J, Marcucci R, Price MJ, Valgimigli M, Kim HS,Patti G, Breet NJ, DiSciascio G, Cuisset T, Dangas G. Impact ofplatelet reactivity on clinical outcomes after percutaneous coronary

Coronary Artery Disease/Clopidogrel Reloading in Patients With ACS 7
intervention: a collaborative meta-analysis of individual participantdata. J Am Coll Cardiol 2011;58:1945e1954.
4. Kastrati A, vonBeckerathN, Joost A, Pogatsa-MurrayG,GorchakovaO,Schömig A. Loading with 600 mg clopidogrel in patients with coronaryartery disease with and without chronic clopidogrel therapy. Circulation2004;110:1916e1919.
5. Williams DO, Abbott JD. What to do with patients receiving long-termclopidogrel: reload or relax? Circulation 2008;118:1219e1222.
6. Di Sciascio G, Patti G, Pasceri V, Colonna G, Mangiacapra F,Montinaro A; ARMYDA-4 RELOAD Investigators. Clopidogrelreloading in patients undergoing percutaneous coronary intervention onchronic clopidogrel therapy: results of the ARMYDA-4 RELOAD(Antiplatelet therapy for Reduction of MYocardial Damage duringAngioplasty) randomized trial. Eur Heart J 2010;31:1337e1343.
7. Mahmoudi M, Syed AI, Ben-Dor I, Gonzalez M, Maluenda G,Gaglia MA Jr, Sardi G, Wakabayashi K, Torguson R, Xue Z, Satler LF,Suddath WO, Pichard AD, Waksman R. Safety and efficacy of clopi-dogrel reloading in patients on chronic clopidogrel therapy who presentwith an acute coronary syndrome and undergo percutaneous coronaryintervention. Am J Cardiol 2011;107:1779e1782.
8. Malinin A, Pokov A, Swaim L, Kotob M, Serebruany V. Validation ofa VerifyNow-P2Y12 cartridge for monitoring platelet inhibition withclopidogrel. Methods Find Exp Clin Pharmacol 2006;28:315e322.
9. Malinin A, Pokov A, Spergling M, Defranco A, Schwartz K, SchwartzD, Mahmud E, Atar D, Serebruany V. Monitoring platelet inhibitionafter clopidogrel with the VerifyNow-P2Y12(R) rapid analyzer: theVERIfy Thrombosis risk ASsessment (VERITAS) study. Thromb Res2007;119:277e284.
10. Lim CC, van Gaal WJ, Testa L, Cuculi F, Arnold JR, Karamitsos T,Francis JM, Petersen SE, Digby JE, Westaby S, Antoniades C, Khar-banda RK, Burrell LM, Neubauer S, Banning AP. With the “universaldefinition,” measurement of creatine kinase-myocardial band ratherthan troponin allows more accurate diagnosis of periproceduralnecrosis and infarction after coronary intervention. J Am Coll Cardiol2011;57:653e661.
11. Prasad A, Gersh BJ, Bertrand ME, Lincoff AM, Moses JW, OhmanEM, White HD, Pocock SJ, McLaurin BT, Cox DA, Lansky AJ,Mehran R, Stone GW. Prognostic significance of periprocedural versusspontaneously occurring myocardial infarction after percutaneouscoronary intervention in patients with acute coronary syndromes: ananalysis from the ACUITY (Acute Catheterization and Urgent Inter-vention Triage Strategy) trial. J Am Coll Cardiol 2009;54:477e486.
12. Rao AK, Pratt C, Berke A, Jaffe A, Ockene I, Schreiber TL, Bell WR,Knatterud G, Robertson TL, Terrin ML. Thrombolysis In MyocardialInfarction (TIMI) trial—phase I: hemorrhagic manifestations andchanges in plasma fibrinogen and the fibrinolytic system in patients
treated with recombinant tissue plasminogen activator and streptoki-nase. J Am Coll Cardiol 1988;11:1e11.
13. Collet JP, Silvain J, Landivier A, Tanguy ML, Cayla G, Bellemain A,Vignolles N, Gallier S, Beygui F, Pena A, Montalescot G. Dose effectof clopidogrel reloading in patients already on 75-mg maintenancedose: the Reload with Clopidogrel Before Coronary Angioplasty inSubjects Treated Long Term with Dual Antiplatelet Therapy(RELOAD) study. Circulation 2008;118:1225e1233.
14. Ricciardi MJ, Wu E, Davidson CJ, Choi KM, Klocke FJ, Bonow RO,Judd RM, Kim RJ. Visualization of discrete microinfarction afterpercutaneous coronary intervention associated with mild creatinekinase-MB elevation. Circulation 2001;103:2780e2783.
15. Ioannidis JPA, Karvouni E, Katritis DG. Mortality risk conferred bysmall elevations of creatine-kinase MB isoenzyme after percutaneousintervention. J Am Coll Cardiol 2003;42:1406e1411.
16. Geisler T, Kapp M, Göhring-Frischholz K, Daub K, Dösch C, BigalkeB, Langer H, Herdeg C, Gawaz M. Residual platelet activity isincreased in clopidogrel- and ASA-treated patients with coronarystenting for acute coronary syndromes compared with stable coronaryartery disease. Heart 2008;94:743e747.
17. Ault KA, Cannon CP, Mitchell J, McCahan J, Tracy RP, Novotny WF,Reimann JD, Braunwald E. Platelet activation in patients after an acutecoronary syndrome: results from the TIMI-12 trial. Thrombolysis inMyocardial Infarction. J Am Coll Cardiol 1999;33:634e639.
18. Rao SV, O’Grady K, Pieper KS, Granger CB, Newby LK, Van de WerfF, Mahaffey KW, Califf RM, Harrington RA. Impact of bleedingseverity on clinical outcomes among patients with acute coronarysyndromes. Am J Cardiol 2005;96:1200e1206.
19. Hamm CW, Bassand JP, Agewall S, Bax J, Boersma E, Bueno H, CasoP, Dudek D, Gielen S, Huber K, Ohman M, Petrie MC, Sonntag F, UvaMS, Storey RF, Wijns W, Zahger D, ESC Committee for PracticeGuidelines, Bax JJ, Auricchio A, Baumgartner H, Ceconi C, Dean V,Deaton C, Fagard R, Funck-Brentano C, Hasdai D, Hoes A, Knuuti J,Kolh P, McDonagh T, Moulin C, Poldermans D, Popescu BA, Reiner Z,Sechtem U, Sirnes PA, Torbicki A, Vahanian A, Windecker S, Docu-ment Reviewers, Windecker S, Achenbach S, Badimon L, Bertrand M,Bøtker HE, Collet JP, Crea F, Danchin N, Falk E, Goudevenos J, GulbaD, Hambrecht R, Herrmann J, Kastrati A, Kjeldsen K, Kristensen SD,Lancellotti P, Mehilli J, Merkely B, Montalescot G, Neumann FJ,Neyses L, Perk J, RoffiM, Romeo F, Ruda M, Swahn E, Valgimigli M,Vrints CJ, Widimsky P. The task force for the management of acutecoronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). ESCGuidelines for the management of acute coronary syndromes in patientspresenting without persistent ST-segment elevation. Eur Heart J2011;32:2999e3054.