Renal Failure and Complications of Hemodialysis Paul B. Jones PGY3 – May 8th.
Upload
jose-luis-sanchezCategory
view
214download
0
Efficacy and safety of ustekinumab in a patient with
chronic renal failure on hemodialysis
Dear Editor,Moderate to severe psoriasis is a chronic immune-
mediated disorder that may require long-term therapy.Ustekinumab, the most recent biological agent approvedfor treatment of adult patients with moderate to severepsoriasis, is a fully human monoclonal antibody thatbinds to the p40 subunit of interleukin (IL)-12 and IL-23.1 Renal impairment is considered to be a relative orabsolute contraindication to several drugs and may aug-ment their toxicity.2 Nevertheless, the literature containslimited information regarding the use of biological drugsin patients with renal failure.3 We report the use ofustekinumab in a 65-year-old man with severe refractorypsoriasis and end-stage renal failure on hemodialysis.A 65-year-old patient had been followed-up with a
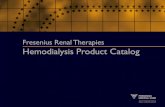
diagnosis of psoriasis for 27 years. He had also sufferedfrom hypertension, ischemic heart disease, and chronicrenal failure four years ago. After failure of other treat-ments, such as methotrexate, cyclosporine, acitretin, andphototherapy, he was given etanercept 50 mg/week, whichdid not improve his psoriasis and was stopped afterseven months. The patient showed a PASI score (Fig. 1) of15, so we switched the him to ustekinumab treatment at astandard dose of 45 mg subcutaneously initially and onceagain four weeks later, followed by 45 mg once every12 weeks. The patient showed a significant improvementof the PASI score already after four weeks of treatment,
and further improvements were observed throughout thetreatment (Fig. 2). Subsequently, after reaching a glomeru-lar filtration rate of 13.5 mL/min, hemodialysis was initi-ated, but we decided to go on with the treatment withustekinumab. After 17 months of treatment, significantremission has been observed, and no relevant changes inrenal function have been noted.Safety data from the studies suggest that ustekinumab
is generally safe and well tolerated, but there is no infor-mation on the treatment with ustekinumab for patientswith end-stage renal failure on hemodialysis.Kauffman et al. evaluated safety, pharmacokinetics, and
clinical response of single intravenous (IV) administrationsof ustekinumab in an open-label, sequential dose escalationstudy.4 Ustekinumab demonstrated linear pharmacokinet-ics over the dose range evaluated. Dose-proportionalincreases in maximum serum concentration were observed,and similar elimination rates were seen in all doses. Theauthors concluded that single IV administrations ofustekinumab were safe and well tolerated, and improve-ments in clinical response were dose dependent.4 Similarendpoints were evaluated in another Phase I study con-ducted by Gottlieb et al.5 In this study, authors assessedsafety, pharmacokinetics, pharmacodynamics, and efficacyof ustekinumab, following a single subcutaneous adminis-tration, in subjects with moderate-to-severe plaque psoria-sis. Dose-proportional peak concentrations were observed,the half-life was approximately 20 days, and the time topeak concentration for ustekinumab was approximately
(a) (b)
Figure 1 (a and b) Lesions on the trunk before starting treatment with ustekinumab
ª 2013 The International Society of Dermatology International Journal of Dermatology 2014, 53, e240–e316
Correspondence e299

12 days. The most commonly reported adverse events wereupper respiratory infection, creatine phosphokinaseincrease, and lymphopenia. The findings of this studyindicated that a single subcutaneous administration ofustekinumab was generally well tolerated in subjects withmoderate-to-severe psoriasis, and results also demonstrateda linear pharmacokinetic profile.5
With anti-tumor necrosis factor-alpha drugs, the liter-ature contains little information that suggests they canbe safely used in patients on dialysis.6,7 Don et al.8
administered etanercept to six patients undergoing he-modialysis, and assessed pre- and post-dialysis serumetanercept concentration, without observing any changeor side effects. Pharmacokinetics of biological drugs inpatients undergoing dialysis is not exactly known, butit is possible to suggest that they have fewer sideeffects compared with other immunosuppressors, whichshould be administered under close monitoring andfollow-up.To our knowledge, this is the first report of treatment
with ustekinumab in a patient with psoriasis on hemodi-alysis. This report suggests that either etanercept orustekinumab can be safely used in the setting of renalfailure. It also shows that hemodialysis does not appearto affect ustekinumab clearance and that ustekinumab isunaffected by renal function. Thus, ustekinumab could bean alternative treatment choice for patients with severerefractory psoriasis and renal failure on hemodialysis,although this fact needs to be studied in large cohorts ofpatients with such comorbidity.
Blanca de Unamuno Bustos, MD
Rosa Ballester S�anchez, MD
Vicente Oliver Martínez, PhD
Jos�e Luis S�anchez Carazo, MD
Department of DermatologyValencia General University HospitalValenciaSpainE-mail: [email protected]
There is no conflict of interest
References1 Gordon KB, Papp KA, Langley RG, et al. Long-
term safety experience of ustekinumab in patients withmoderate to severe psoriasis (Part II of II): results fromanalyses of infections and malignancy from pooled phaseII and III clinical trials. J Am Acad Dermatol 2012; 66:742–751.
2 Hammoudeh M. Infliximab treatment in a patient withrheumatoid arthritis on haemodialysis. Rheumatology
(Oxford) 2006; 45: 357–359.3 Kobak S. Efficacy and safety of adalimumab in a patient
with ankylosing spondylitis on peritoneal dialysis.Rheumatol Int 2012; 32: 1785–1787.
4 Kauffman CL, Aria N, Toichi E, et al. A phase I studyevaluating the safety, pharmacokinetics and clinicalresponse of a human IL-12 p40 antibody in subjects withplaque psoriasis. J Invest Dermatol 2004; 123:1037–1044.
5 Gottlieb AB, Cooper KD, McCormick TS, et al.A phase 1, double-blind, placebo-controlled, evaluatingsingle subcutaneous administrations of a humaninterleukin-12/23 monoclonal antibody in subjects withplaque psoriasis. Curr Med Res Opin 2007; 23:1081–1092.
(a) (b)
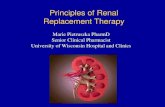
Figure 2 (a and b) Complete clearance was achieved after 6 months of treatment with ustekinumab
International Journal of Dermatology 2014, 53, e240–e316 ª 2013 The International Society of Dermatology
Correspondencee300

6 Cassano N, Vena GA. Etanercept treatment in ahemodialysis patient with severe cyclosporine-resistantpsoriasis and hepatitis C virus infection. Int J Dermatol
2008; 47: 980–981.7 Senel S, Kisacik B, Ugan Y, et al. The efficacy and safety
of etanercept in patients with rheumatoid arthritis and
spondyloarthropathy on hemodialysis. Clin Rheumatol
2011; 30: 1369–1372.8 Don BR, Spin G, Nestorov I, et al. The
pharmacokinetics of etanercept in patients with end-stagerenal disease on haemodialysis. J Pharm Pharmacol
2005; 57: 1407–1413.
Coix lacryma-jobi associated symmetrical drug-related
intertriginous and flexural exanthema
Baboon syndrome refers to a specific skin eruption char-acterized by a symmetric erythema of the gluteal andintertriginous areas in the absence of systemic involve-ment.1,2 In this report, we describe a patient withsymmetrical drug-related intertriginous and flexural exan-thema, likely associated with Coix lacryma-jobi.
A 53-year-old woman presented with a 3-day historyof multiple progressive erythematous and pruritic skinlesions on her trunk and inguinal area. To date, she hadbeen treated for hypertension with oral medications, noneof which had been changed over the past year. Notably,one week before, she had begun taking Ibane� (JWPharm., Seoul, Korea), an over-the-counter medicationcontaining riboflavin, pyridoxine, ascorbic acid, nicotin-amide, biotin, L-cysteine, and Coix lacryma-jobi that isapproved by the Korean Food and Drug Administrationfor the treatment of recurrent aphthous stomatitis.Examination revealed multiple erythematous plaques
with secondary superficial pustules distributed over the
trunk and inguinal areas (Fig. 1). The patient wasafebrile, and the laboratory tests obtained were unre-markable except for elevation of acute phase reactants.Skin biopsy revealed numerous intraepidermal and peri-vascular mononuclear and eosinophil infiltrates (Fig. 2).A diagnosis of symmetrical drug-related intertriginousand flexural exanthema was made, possibly resultingfrom ingestion of Coix lacryma-jobi-containing medica-tions. She was advised to discontinue Ibane�, and overthe following two weeks, all skin lesions graduallyresolved, leaving some degree of post-inflammatory hy-perpigmentation. The patient was followed up for morethan three months without recurrence.Ibane� – the prime candidate for the offending drug in
the case described here – is a mixture of riboflavin, pyri-doxine, ascorbic acid, nicotinamide, biotin, L-cysteine andCoix lacryma-jobi. We presume that components in Coix
lacryma-jobi could be significantly associated with thebaboon-like exanthema described here. Coix lacryma-
jobi – a major component of Ibane�, known colloquiallyas Job’s tears, coixseed, or adlai – has long been used in
(a) (b)
(c)
Figure 1 (a) Extensive erythematous plaques with superficial pustules on the trunk and in the inguinal area, demonstratingsymmetrical drug-related intertriginous and flexural exanthema (b) involving inframammary folds, but (c) relatively sparing theback
ª 2013 The International Society of Dermatology International Journal of Dermatology 2014, 53, e240–e316
Correspondence e301