EFFECTS ON OTHER LIPOPROTEINS
21
9/13/2017 1 Dyslipidemia: Going Beyond the Current Treatment Guidelines NCNP Las Vegas October 2017 Joyce L. Ross, MSN, CRNP, CS, FNLA, FPCNA Diplomate Accreditation Council For Clinical Lipidology Past President Preventive Cardiovascular Nurses Association Immediate Past President National Lipid Association Consultative Education Specialist, Cardiovascular Risk Intervention Clinical Affiliation: University Of Pennsylvania Health System - retired Philadelphia, Pennsylvania [email protected] Disclosures Speakers Bureau: KOWA AstraZeneca Amgen Sanofi/Regeneron Amarin Consultant: Akcea Therapeutics Kaneka America Kastle Therapeutics Program Objectives After attending this presentation the participant will be able to: 1. Discuss 2016 Updated ACC Guidelines, NLA and others Recommendations for Dyslipidemia Management 2. Recall that statin therapy is the first line medication treatment for risk reduction 3. Discuss considerations for addition of “other” classes of lipid lowering medication when combination medication therapy is warranted
Transcript of EFFECTS ON OTHER LIPOPROTEINS

9/13/2017
1
Dyslipidemia: Going Beyond the Current
Treatment GuidelinesNCNP Las Vegas
October 2017
J oy c e L . R os s , M S N , C R N P, C S , F N L A , F P C N AD i p l oma t e A c c re d i t a t i o n C ou n c i l F or C l i n i c a l
L i p i d ol og yP a s t P re s i d e n t P re v e n t i v e C a r d i ov a s c u l a r N u r s e s
A s s oc i a t i o nI mme d i a t e P a s t P re s i d e n t N a t i on a l L i p i d A s s oc i a t i o n
C on s u l t a t i v e E d u c a t i on S p e c i a l i s t , C a r d i ov a s c u l a r R i s k I n t e r v e n t i o n
C l i n i c a l A f f i l i a t i on : U n i v e r s i t y O f P e n n s y l v a n i a H e a l t h S y s t e m - re t i re d
P h i l a d e l p h i a , P e n n s y l v a n i aJ l r @ j oy c e r o s s n p . C o m
Disclosures
Speakers Bureau:
KOWA
AstraZeneca
Amgen
Sanofi/Regeneron
Amarin
Consultant:
Akcea Therapeutics
Kaneka America
Kastle Therapeutics
Program Objectives
After attending this presentation the participant will be able to:
1. Discuss 2016 Updated ACC Guidelines, NLA and others Recommendations for Dyslipidemia Management
2. Recall that statin therapy is the first line medication treatment for risk reduction
3. Discuss considerations for addition of “other” classes of lipid lowering medication when combination medication therapy is warranted

9/13/2017
2
Burden of Atherosclerotic Cardiovascular Disease
Annual rates in US
- Myocardial infarction – 1.1 million
- Strokes - 795,000
- CVD Mortality – 1,344,185 (every 30 seconds a death)
- Cardiac catheterization – 1.0 million
- Percutaneous revascularization – 492,000
- Surgical revascularization – 291,000
Annual cost – >$315 billion
American Heart Association. 2017 Heart and Stroke Statistical Update. At: http://www.americanheart.org. 4
AHA/ACC Focus on ASCVD Risk Reduction using
4 statin benefit groups
(those who would benefit most from treatment)
• Individuals with clinical ASCVD
Individuals with primary elevations of LDL-C >190 mg/dL
Individuals 40 to 75 years of age with DM and without ASCVD with LDL-C 70-189mg/dL
Individuals without clinical ASCVD or DM who are 40 to 75 years of age with LDL-C 70-189 mg/dL and an estimated 10 year ASCVD
risk of 7.5% or higher
Stone NJ, et al. 2013 ACC/AHA Blood Cholesterol Guideline
ACC 2016 – Why the need for change?
Since the publication of the last guidelines the Food and Drug Administration has approved a new class of meds
proprotein convertase subtillisin/kexin 9 or most often referred to as PCSK9 Inhibitors for at high-risk patients who may
require additional therapies to bring the LDL-C to a more
acceptable threshold
The recent results of the HPS2-THRIVE and IMPROVE-IT trials have also provided new data that provided new
evidence with regard to the addition of second
non-statin agents when additional lowering is warranted
Adapted from: 1) http://www.acc.org/latest in cardiology/ten points to remember 2016. (2) Http://www.lipid.org/nla/acc16-american
college cardiology scientific sessions highlights

9/13/2017
3
2016 ACC Consensus Document onRole of Non-Statin Therapies for LDL-C Lowering
Lloyd-Jones DM, Morris PB, et al. J Am Coll Cardiol. 2016 (posted online April 1, 2016).
Statin Benefit Groups
Adults ≥21 yrs of age
with clinical ASCVD
on statin for 2°
prevention
Adults ≥21 yrs of age
with LDL-C ≥190 mg/dL
on stain for 1°
prevention
40-75 yrs w/o ASCVD
but with DM & LDL-C 70-
189 mg/dL on statin for
1o prevention
40-75 yrs w/o ASCVD or
DM, LDL-C 70-189 mg/dL
& 10-yr ASCVD risk
≥7.5%, on statin for 1°
prevention
Factors to consider
• Adherence and lifestyle
• Statin intolerance
• Control of other risk factors
• Clinician-patient discussion of the benefits, risks, and patient preferences regarding addition
of non-statin meds
• Percentage LDL-C reduction
• Monitoring of response to therapy, adherence, and lifestyle
Optional interventions to consider
• Referral to lipid specialist and registered dietitian
• Ezetimibe, bile acid sequestrants, or PCSK9 inhibitors
• Mipomersen, lomitapide, LDL apheresis may be considered by a lipid specialist for
patients with familial hypercholesterolemia
2016 ACC Consensus Document onRole of Non-Statin Therapies for LDL-C Lowering
First- and second-line non-statin medications to consider for
additional LDL-C lowering in the 4 statin benefit groups:
*Alternative to percentage LDL-C reduction as a marker for adequate response to therapy.PCSK9 = proprotein convertase subtilisin/kexin type 9 inhibitor; BAS = bile acid sequestrant; TG = triglyceride1. Jacobson TA, et al. J Clin Lipidol. 2014;8:473-488. 2. Jellinger PS, et al. Endocr Pract. 2012 Mar-Apr;18(suppl 1):1-78. 3. European Association for Cardiovascular Prevention & Rehabilitation, et al. Eur Heart J. 2011;32(14):1769-1818. 4. Anderson TJ, et al. Can J Cardiol. 2013;29(2):151-167. Lloyd-Jones DM, Morris PB, et al. J Am Coll Cardiol. 2016 (posted online April 1, 2016).
Risk Category Treat-to-target
goal*
First-line non-statin
agent
Second-line non-statin
agent
Clinical atherosclerotic
CVD
LDL-C <100
mg/dL
First-line: ezetimibe Second-line: PCSK9
inhibitor
LDL-C ≥190 mg/dL LDL-C <70 mg/dL First-line: ezetimibe or
PCSK9 inhibitor
Second-line: BAS
(alternative to ezetimibe
if TG <300 mg/dL)
DM and aged 40-75
years and LDL-C 70-189
mg/dL
LDL-C <100
mg/dL
First-line: ezetimibe Second-line: BAS
No DM and aged 40-75
years and LDL-C 70-189
mg/dL + 10-year ASCVD
risk ≥7.5%
LDL-C <100
mg/dL
First-line: ezetimibe Second-line: BAS
2017 AACE Guidelines for Management of Dyslipidemia and Prevention of CVD
Jellinger PS, et al. Endocr Pract. Apr 2017;23(Suppl 2):1-87.

9/13/2017
4
2016 ESC/EAS Guidelines for the Management of Dyslidemias
Riskcategory
Definition LDL-C Goal
Very high • Documented CVD• DM with target organ damage
or a major risk factor• 10-year risk ≥10% for fatal CVD
<70 mg/dL
Or ≥50% reduction
if LDL-C 70-135
mg/dL
High • Cholesterol >310 mg/dL or BP ≥180/110 mmHg
• Most people with DM
• Moderate CKD
• 10-year risk ≥5% for fatal CVD
<100 mg/dL
Or ≥50% reduction
if LDL-C 100-200
mg/dL
Moderate 10-year risk 1% - <5% for fatal
CVD
<115 mg/dL
Low 10-year risk <1%for fatal CVD <115 mg/dL
10
Catapano AL, et al. Eur Heart J. Oct 14 2016;37(39):2999-3058.
2014 IAS Global Recommendations for the Management of Dyslipidemia
Category Total long-term
risk*
Therapy LDL-C Non-HDL-C
Established ASCVD
NA Lipid-lowering therapy
<70 mg/dL <100 mg/dL
High risk ≥45% Lipid-lowering therapy
<100 mg/dL
<130 mg/dL
Moderatelyhigh risk
30-44% Consider lipid-loweringtherapy
<100 mg/dL
<130 mg/dL
Moderate risk 15-29% Lipid-lowering therapy optional
Low risk <15%
11
*Total long-term (lifetime) risk includes multiple risk factors (eg, LDL-C, smoking, hypertension, diabetes, low
HDL-C, family history of ASCVD); Calculated with Framingham or QRISK calculators
Expert Dyslipidemia Panel of the IAS. J Clin Lipidol. Jan-Feb 2014;8(1):29-60.
Who may need additional therapies beyond statins to control LDL-C?
• Any patient with hypercholesterolemia not achieving
LDL-C goal1,2
• Patients who are intolerant or have a inadequate
response to statin therapy3,4
• Difficult to treat patients5,6
– Familial hypercholesterolemia
– Diabetes
1. Ballantyne CM, et al. Am Heart J. 2005;149:464-73. 2. Karalis DG, et al. Cholesterol. 2012;2012:861924. 3. Sullivan D, et al.
JAMA. 2012;308(23):2497-2506. 4. Kataoka Y, et al. Arterioscler Thromb Vasc Biol. 2015;35(4):990-5. 5. Stein EA, et al. Am J
Cardiol. 2003;92(11):1287-93. 6. Stark Casgrande S, et al. Diabetes Care. 2013;36(8):2271-9.

9/13/2017
5
Integrating Emerging Clinical Data Into Clinical Practice: An Evolving Treatment Algorithm
Post-ACS/CAD patient with
hypercholesterolemia
ACC/AHA Guidelines:
Optimize statin therapy
LDL<70 LDL≥70
Add
ezetimibe
LDL<70 LDL ≥ 70
Add PCSK9 inhibitors
or other LLT
Statin
therapy
Step 1:
Statin
Statin +
Ezetimibe
Step 2:
Check LDL
Step 3:
Add Rx as needed*
Slide courtesy of Christopher Cannon, MD.
*This pathway is consistent with the Non-statin
Therapies Document for individuals with ASCVD with
comorbidity.
Applying the Guideline
SA is a 60 y.o patient with a long history of DM, which is well
controlled at this time and HTN
she has a strong family history of premature heart disease
and is worried about her risk given her DM, poor exercise
history, dietary status and family history
Meds currently include: Metformin ER 2,000 mg daily
Sitagliptin (januvia) 10 mg daily
Hyzaar (ARB) Hctz 50-12 mg/daily
Weight: 154 pounds, height 5’4”, BP 132/88, waist 30”
Last lipid panel > 1 year ago.
How do the guidelines apply?
Individuals 40 to 75 years of age with DM and without ASCVD with LDL-C 70-189mg/dL
The appropriate intensity of statin therapy should be used to reduce ASCVD risk in those most likely to benefit
A high level of evidence supports the use of moderate-intensity statin therapy in persons with diabetes 40 to 75 years of age.
In those of the same age group with diabetes high-intensity statin therapy preferentially for individuals with diabetes and a ≥7.5%

9/13/2017
6
Risk Assessment
for this patient to estimated 10-year ASCVD risk
Problem: consideration for those with diabetes 40 to 75
years of age recognizes that these individuals are at
substantially increased lifetime risk for ASCVD events and
death
individuals with DM experience greater morbidity and worse survival follow the onset of ASCVD
In persons with diabetes <40 or >75 years of age, statin therapy
should be individualized based on considerations of ASCVD risk
reduction benefits, the potential for adverse effects and drug-
drug interactions, and patient preferences
Goal: establish the level of treatment with statin
therapy
Risk Factor Acceptable range of values
Patient Value
Sex M OR F F
Age 20 – 79 60
Total Cholesterol 130 320 mg/dL 290 md/dL
HDL Cholesterol 20 – 100 mg/dL 35 mg/dL
Systolic BP 90 – 200 mm Hg 132 mm Hg
Tx. For BP Y or N Y
Diabetes Y or N Y
Smoker Y or N N
Race AA or WH WH
10 year ASCVD Risk % 15.7 %
* The calculator only provides lifetime risk estimates for individuals 20 – 59 years of age
Risk Calculator which may be found online or can be
downloaded to smart phone etc.
Intensity of Statin Therapy
*Individual responses to statin therapy varied in the RCTs and should be expected to vary in clinical practice. There might be a biologic basis for a less-than-average response.
†Evidence from 1 RCT only: down-titration if unable to tolerate atorvastatin 80 mg in IDEAL (Pedersen et al).‡Although simvastatin 80 mg was evaluated in RCTs, initiation of simvastatin 80 mg or titration to 80 mg is not recommended by the FDA due to the increased risk of myopathy, including rhabdomyolysis.
High- Moderate- and Low-Intensity of Statin Therapy Expert Panel)*
High-Intensity Statin Therapy
Moderate-Intensity Statin Therapy
Low-Intensity Statin Therapy
Daily dose lowers LDL-C on average, by approximately ≥50%
Daily dose lowers LDL-C on average, by approximately 30% to <50%
Daily dose lowers LDL-C on average, by <30%
Atorvastatin (40†)-80 mgRosuvasatin 20 (40) mg
Atorvastatin 10 (20) mgRosuvastatin (5) 10 mgSimvastatin 20-40 mg‡Pravstatin 40 (80) mgLovastatin 40 mgFluvastatin XL 80 mgFluvastatin 40 mg bidPitavastatin 2-4 mg
Simvastatin 10 mgPravastatin 10-20 mgLovastatin 20 mgFluvastatin 20-40 mgPitavastatin 1 mg

9/13/2017
7
Initiating statin therapy in individuals with clinical
ASCVD
Not currently on statin therapy Initial evaluation prior to statin
initiation
Fasting lipid panel
ALT
CPK
Consider evaluation for other secondary causes or conditions that may
influence statin safety
Aged <75 y without contraindications, conditions or drug-drug
interactions
influencing statin safety, or a history of statin intolerance
• - Initiate high-intensity statin therapy
• - Counsel on healthy lifestyle habits
Progression of Atherogenic Cholesterol-Lowering Drug
Therapy20
Stone NJ, et al. 2013 ACC/AHA Blood Cholesterol Guideline
Lifestyle as the Foundation for ASCVD Risk Reduction
Efforts
Newest ACC/AHA guidelines adds increased emphasis on
lifestyle management for treatment
It must be emphasized that lifestyle modification (i.e., adhering
to a heart healthy diet, regular exercise habits, avoidance of
tobacco products, and maintenance of a healthy weight)
remains a critical component of health promotion and ASCVD
risk reduction
both prior to and in concert with the use
of cholesterol- lowering drug therapies. Healthy
diet or lifestyle modifications were recommended as
background therapy for the RCTs of cholesterol-lowering drug
therapy.
Stone NJ, et al. 2013 ACC/AHA Blood Cholesterol Guideline

9/13/2017
8
HMG CoA Reductase Inhibitors (Statins)
Competitive Inhibition
Cholesterol production
Expression of LDL
receptors
LDL, VLDL, and
IDL particles
LDL-C Lowering
Acetyl CoA
HMG-CoA
Mevalonate
Cholesterol production
Statins - HMG CoA-Reductase Inhibitors22
VLDL=Very Low Density
Lipoprotein
IDL
HMG-CoA reductase inhibitors
Wwwlipid.org wwwlipid.org NLA
NEWSFLASH !!!!!
All Statins Are Not Created Equal
• How are they different ?
• strength at starting dose
• way the body metabolizes it
• hydro/lipophilic
Taking a walk on the Cytochrome
P450 Pathway
Ross J 2004

9/13/2017
9
Role of CYP450 3A4 in Drug Metabolism
• Responsible for converting lipophilic
substrates to water-soluble products to
facilitate urinary excretion
• High potential for drug-drug interactions, as
approximately 50% of drugs are metabolized
by this enzyme
• Hydrophilic agents do not require clinically
significant metabolism through this pathway
Wilson. Pharmacokinetics: the dynamics of drug absorption, distribution, and elimination. Hardman et al, eds. In: Goodman and Gilman’s The Pharmacological
Basis of Therapeutics. 10th ed. New York, NY: McGraw-Hill; 2003:3-30.
Dose Efficacy of Statin-Based Therapies for LDL-C Reduction (%)
Dose Efficacy in STELLAR1*
Drug 10 mg 20 mg 40 mg 80 mg
CRESTOR® (rosuvastatin calcium) 46 52 55
Lipitor® (atorvastatin calcium) 37 43 48 51
Pravachol®
(pravastatin sodium)
20 24 30 *
Zocor® (simvastatin) 28 35 39 46
•VytorinTM (ezetimibe 10 mg/simvastatin)* reduces LDL-C by 46% to 59%2*
•Data derived from the prescribing information for Vytorin •Peter H. Jones, MD, Michael H. Davidson, MDComparison of the Efficacy and Safety of Rosuvastatin Versus Atorvastatin, Simvastatin, and Pravastatin Across Doses
(STELLAR* Trial) The American Journal of Cardiology Vol. 93 July 15, 2003
ACC/AHA/NHLBI Clinical Advisory Risk Factors for Statin-Myopathy
Advanced age (especially >80 yr; women > men)
Severe chronic kidney disease
Impaired liver function
Perioperative periods
Alcohol abuse
Large quantities of grapefruit juice (certain statins)
Interacting medications
Hypothyroidism
27
Pasternak RC et al. J Am Col Cardiol. 2002;40:567-572.

9/13/2017
10
Managing Statin-Associated Myalgia
Well Accepted:
Rule out secondary causes
Switch to a different statin
Alternate day dosing of higher potency statins
Use lowest statin dose that is tolerated; adding a second agent if needed
Debatable:
Red yeast rice (Monascus purpureus) 2400 mg/day
Vitamin D supplementation
Coenzyme Q10 (CoQ10) supplementation
Ahmed W, et al. Translational Research 2009;153:11–16.
Reindl EK, et al, Ann Pharmacother 2010;44:1459–1470.
Halbert SC, et al. Am J Cardiol 2010;105:198 –204) Marcoff L, Thompson PD. J Am Coll Cardiol. 2007;49:2231–2237.
Meanwhile back to our patient
High risk patient R/T DM, HTN, Dyslipidemia
Full lipid panel needed: TG 203, TC 290, HDL 40, LDL 169, Glucose 118, HbA1c 6.5, TSH, ALT/AST, Renal function all WNL
Lipid Dx: Familial Combined Hyperlipidemia
LDL Threshold: < 100/70 ?
Treatment Plan
Lifestyle Management
Exercise and Diet
Medications
Rosuvastatin 20 mg
Low dose ASA
No change with DM meds
No change with ARB/HCTZ for
BP control and renal protection
Labs and RTC X 6 WKS
1st FOLLOW UP APPT.
Returns in 6 weeks with some change in lifestyle management
Tolerating changes in the medication regimen without untoward side effects
Labs: TG: 150, TC: 170, HDL: 38, Non-HDL: 132 , LDL 102, other studies WML
Weight: 151, BP 116/78
Treatment Plan:
Congratulate on changes, continue with same
LDL at 102 ? Enough?
Could increase statin to 40 mg for 6% further reduction or consider a cholesterol absorption inhibitor for a 20% further reduction
No change with other medications

9/13/2017
11
Cholesterol Absorption Inhibitor
Ezetimibe
Mechanism of Action
Inhibits cholesterol absorption in the intestine thereby increasing hepatic LDL receptors
Dose and Route of Administration
10 mg orally once daily
Lipoprotein Effects
Decreases LDL 15-20 %
Decreases TGs 10 %
Increases HDL 1-2 %
Contraindications
None
IMPROVE-IT: Conclusions
• First trial demonstrating incremental clinical benefit
when adding a non-statin agent (ezetimibe) to statin
therapy:
– Non-statin lowering LDL-C with ezetimibe reduces
cardiovascular events
– Even lower is even better (achieved mean LDL-C 54 vs.
70 mg/dL at 1 year)
– Confirms ezetimibe safety profile
• Reaffirms the LDL hypothesis, which suggests that
reducing LDL-C prevents cardiovascular events
Primary end point (cardiovascular death, MI, unstable angina, coronary revascularization, or stroke).
Cannon CP, et al. N Engl J Med. 2015;372(25):2387-97.
Case Study # 2
- 50 y.o. male with + family history of premature
ASCVD (Father fatal MI age 52)
- Presents for evaluation and recommendations for
cardiovascular risk
- PMH: Known HTN X 5yrs, Rx: HCTZ 25 mg
- Denies history of CAD, DM, or Thyroid disease
- Denies chest pain, SOB, or calf pain when walking

9/13/2017
12
Lifestyle evaluation:
- no regular exercise program
- high stress job as manager in an investment firm
- Diet: often “eats on the run”
- Smoking 24 year history approximately 1pk/day
- ETOH: generally has 2-3 drinks per day after long hours at work (feels it helps him to unwind)
- Social history: married with 3 children
Laboratory Studies &
Physical Exam
• Lipids:• TG 584• TC 302• HDL 29• LDL 204 (d)• Non-HDL: 273
• Glucose 118• BUN/Creatinine: WNLs, GFR: <
60• ALT/AST: WNLs
Physical Exam: unremarkable except
- Extremities: normal pulses throughout, mild bilateral achilles tendon xanthomas > L side
BP: 146/84HR: 92BMI: 28Waist: 38.5”
The elbow and feet of the patient showing xanthomas at 10 years of age
(a,b). Complete regression of xanthomas shown at the age of 23 (c,d).
S. Lind et al., J Int Med 2004; 256: 406-12
Eruptive Xanthomas
Before and After Treatment

9/13/2017
13
Courtesy of Anne Goldberg, MD
Tendon Xanthomas & Arcus Cornea
Focus on ASCVD Risk Reduction
Individuals with LDL–C ≥190 mg/dL or triglycerides ≥500 mg/dL should be evaluated for secondary causes of hyperlipidemia
Adults ≥21 years of age with primary LDL–C ≥190 mg/dL should be treated with statin therapy (10-year ASCVD risk estimation is not required)
Use high-intensity statin therapy unless
contraindicated
Stone NJ, et al. 2013 ACC/AHA Blood Cholesterol Guideline
Applying Guideline
Patient has a combined lipid problem but current
LDL-C suggests potential FH with superimposed
elevated TGs and Non-HDL-C
Would not need to use Global Risk Assessment
since 10-year and lifetime risk are very high with FH
Would treat with high intensity statin therapy along
with lifestyle management

9/13/2017
14
Dx. & Treatment Plan
Problem List:
Dyslipidemia &
Smoking (low HDL)
Overweight
High Stress
High ETOH intake (high TG)
Elevated glucose
Elevated BP
Lifestyle Management Smoke Cessation Meet with dietician Decrease ETOH Exercise for risk management and
decrease stress – stress test first?
Medications ASA 81 mg
rosuvastatin 40 mg ? Why
Add ace inhibitor, continue with HCTZ
RTC: 6 weeks with labs including HbA1c & TSH. CMP and lipids with Lp(a)
1st Follow Up Appt.
Stress test WNL
Coronary Arterial Calcium Score: 216 = 90% for age
Returns with changes in diet as recommended by dietician, walking 1 X week, wt. down 3 pounds
No changes with ETOH
Changed office hours to be home for dinner with family
Taking all medications without difficulty
BP with combination therapy – 130/82
Labs on return:
Glucose 129, HbA1c 7.2
TSH: normal range
ALT/AST: WNL
Renal: WNL
Lipids:
TG 316
TC 180
HDL 31
Non HDL 149
LDL 96
Lp(a) 107 mg/dL
Treatment Plan
Continue with lifestyle changes – congratulate for all efforts made BUT:
Decrease ETOH
Stop smoking
Increase exercise
Decrease Kcal to 1,800 daily for ongoing wt. loss
Medications:
Change with current medications
Need to add further LLM & possibly some changes for elevated glucose
Would you:
Change statin to simvastatin?
Add ezetimibe 10 mg?
Add PCSK9 Inhibitor?
Add glucophage 500 mg BID?
Add sulfonylurea?
Add omega 3 fatty acid?

9/13/2017
15
We should consider use of PCSK9-Inhibitors in
patients with:
known CAD or those identified and those who have very
high risk
whose LDL-C cannot be lowered to an acceptable range (goal , generally < 70 mg/dL)
who are on maximally tolerated statin therapy
Use of PCSK9 Inhibitors
*Alternative to percentage LDL-C reduction as a marker for adequate response to therapy.
PCSK9 = proprotein convertase subtilisin/kexin type 9 inhibitor; BAS = bile acid sequestrant; TG = triglyceride
Jacobson TA, et al. J Clin Lipidol. 2014;8:473-488. 2. Jellinger PS, et al. Endocr Pract. 2012 Mar-Apr;18(suppl 1):1-78. 3. European Association for
Lloyd-Jones DM, Morris PB, et al. J Am Coll Cardiol. 2016 (posted online April 1, 2016).
PCSK9 Inhibitors
PCSK9 Inhibitors: Obtaining Approval
Low rates of approval for PCSK9 inhibitors FH and LDL-C >190 mg/dL despite LLT
63.3% of PCSK9 prescriptions rejected
9% of ezetimibe prescriptions rejected
Clinical ASCVD and LDL-C >100 mg/dL despite LLT
57.5% of PCSK9 prescriptions rejected
8.2% of ezetimibe prescriptions rejected
Gaining approval requires use of strong definitions:
Heterozygous or homozygous FH
Clinical ASCVD
Maximally tolerated statin dose
45
Knowles JW, et al. Circulation. May 30 2017;135(22):2204-2206.

9/13/2017
16
Barrier Studies and Recommendations
National Lipid Association – A recent study conducted by the National Lipid Association found that 70% of respondents wait more than 30 days from the time of writing the PCSK9i prescription to fulfillment of the first prescription for their patients with FH. Approximately 50% of respondents spend more than 1 hour per week on each patient’s prior authorization.
Carl E. Orringer, MD, Terry A. Jacobson, MD, Joseph J. Saseen, PharmD, Alan S. Brown, MD, Antonio M. Gotto, MD, Joyce L. Ross MSN, CRNP, James A. Underberg, MD. National Lipid Association Updated Recommendations on the Use of PCSK9. Available online at NLA website
Baum SJ, Toth PP, Underberg JA, Jellinger P, Ross J. & Wilemon, Clin Cardiol. 2017 Mar 22. PCSK9 inhibitor access barriers-issues and recommendations: Improving the access process for patients, clinicians and payers.
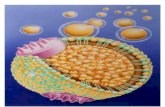
Proprotein Convertase Subtilisin/KexinType 9 (PCSK9)
• PCSK9: plays an important role in regulating the
expression of the LDL-receptor (LDL-R)
– Secreted primarily by hepatocytes into circulation and
binds to LDL-R on the surface liver cells
– The PCSK9/LDL-R/LDL-C complex is internalized into
hepatocytes and undergoes lysosomal degradation
Abifadel M, et al. Curr Atheroscler Rep. 2014;16(9):439.
PCSK9 Inhibitors: Mechanism of Action
PCSK9 self-processing,
secretion, and export
PCSK9
PCSK9
LDL
Particle
LDL-R
Endocytosis of
LDL-R/PCSK9
complex
Plasma
LDL, LDL-R,
and PCSK9
degradationLysosome
Endosome
LDL-R = LDL receptors
Adapted by Lilian McVey from
Shimada YJ, Cannon CP.
Eur Heart J. 2015;36(36):2415-2424.
Used with permission.

9/13/2017
17
Currently Available PCSK9 Inhibitors
Alirocumab Evolocumab
FDA Approval July 2015 August 2015
Indication
Adjunct to diet and maximum-
tolerated statin for adults with HeFH
or clinical ASCVD who require
additional lowering of LDL-C
Adjunct to diet and maximum-
tolerated statin for adults with
HeFH or clinical ASCVD who
require additional lowering of
LDL-C, HoFH patients on other LLT
Dosing 75-150 mg SC Q2W140 mg SC Q2W or 420 mg SC
monthly
How Supplied
Single-dose pre-filled autoinjector
pens and pre-filled glass syringes that
deliver 75 mg/mL or 150 mg/mL
Single-use pre-filled syringe or
autoinjector pens that deliver 1 mL
of 140 mg/mL
MonitoringCheck LDL-C levels 4 to 8 weeks
after initiating or after titrating therapy
Check LDL-C levels 4 to 8 weeks
after initiating therapy
HeFH = heterozygous familial hypercholesterolemia; HoFH = homozygous familial hypercholesterolemia; SC =
subcutaneous.
www.fda.gov. Praluent [package insert]. Bridgewater, NJ: sanofi-aventis; 2015. Repatha [package insert]. Thousand Oaks,
CA: Amgen; 2015.
Available PCSK9 Inhibitors
Alirocumab
Fully human IgG1 mAB
Indicated for:
HeFH
Clinical ASCVD
Dose:
75-150 mg SQ q 2 weeks
LDL reduction:
50% to 60%
Evolocumab
Fully human IgG2 mAB
Indicated for: HeFH
Clinical ASCVD
HoFH
Dose: 140 mg SQ q 2 weeks or
420 mg SQ (3 injections) q month
LDL reduction: 50% to 60%
HeFH = heterozygous familial hypercholesterolemia, HoFH = homozygous familial hypercholesterolemia.
Alirocumab [injection] Prescribing Information, 2015; Evolocumab Prescribing Information, 2015; Dadu RT, Ballantyne CM. Nat Rev Cardiol. 2014;11(10):563-575; Gumbiner B, et al. Circulation. 2012;126:a13322; www.clinicaltrials.gov; www.pharmacist.com/express-scripts-cover-both-new-cholesterol-drugs.
OSLER Program: LDL-C
0
140
40
100
80
120
20
Med
ian
LD
L-C
(m
g/d
L)
Baseline
N=4465
60
4 weeks
N=1258
12 weeks
N=4259
24 weeks
N=4204
36 weeks
N=1243
48 weeks
N=3727
61% Reduction (95% CI, 0.59-0.63), P<0.0001
Absolute Reduction: 73 mg/dL (95% CI, 71-76)
Standard of Care Alone
Evolocumab + Standard of Care
OSLER = Open-Label Study of Long-Term Evaluation Against LDL-CSabatine MS, et al. N Engl J Med. 2015;372:1500-1509.
OSLER-1 and OSLER-2 are open-label extension studies of phase 2 and 3
evolocumab trials, respectively
(Parent Study)

9/13/2017
18
Adverse Events
Alirocumab Placebo
Nasopharyngitis
11% 11%
Influenza 6% 5%
UTI 5% 5%
Injection site reaction
7% 5%
LFT >3x ULN 1.7% 1.4%
Myalgias 4% 3%
Drug discontinuatio
n0.4% 0.2%
Neurocognitive
0.8% 0.7%
Antidrug antibodies
(ADAs)5% 0.6%
Neutralizing antibody (Nab)
1.2% (of which, in 0.3% led to
decreased efficacy)0
Alirocumab [injection] Prescribing Information, 2015.
Evolocumab – Adverse Events
Evolocumab Placebo
Nasopharyngitis 11% 10%
Influenza 8% 6%
UTI 5% 4%
Injection site reaction 6% 5%
Myalgias 4% 3%
Drug discontinuation 2% 1%
Neurocognitive ≤0.2% ≤0.2%
Antidrug antibodies (ADAs) 0.1% 0
Neutralizing antibody (Nab) 0 0
http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/125522s000lbl.pdf.
FOURIER Trial - Evolocumab
Sabatine MS et al. Am H J 2016; 173: 94-101
54
Primary end point was the composite of cardiovascular death, myocardial infarction,stroke, hospitalization for unstable angina, or coronary revascularization.

9/13/2017
19
Fourier Trial lipid results
Sabatine MS et al. Am H J 2016; 173: 94-101
55
Fourier Trial: Primary Outcome
Sabatine, M.S. et al. NEJM March 17, 2017DOI: 10.1056/NEJMoa1615664NEJM 2017
15% RRR
56
Fourier Trial: MI/Stroke/CV Death
20% RRR
Sabatine, M.S. et al. NEJM March 17, 2017DOI: 10.1056/NEJMoa1615664NEJM 2017
57

9/13/2017
20
2nd Follow Up Appt
Returns looking and feeling well with no changes to healthcare status since last visit
Continues to slowly implement lifestyle recommendations
No difficulty with toleration of current medications
Considering a change in employment
Wt. reduced 4 pounds
No changes with smoking
Now only 2 drinks/day
Walking now 2-3Xs week with family
B/P 128/70
Labs: glucose 89, - HbA1c 7
TG 175, TC 125, HDL 37, Non-HDL 88, LDL 53
Immediate Questions
Is his LDL too low?
Should you stop or decrease statin?
What needs to be done with his still abnormal TG and Non-HDL?
Nothing his LDL is GREAT
Just continue lifestyle management
Continue lifestyle management and add omega 3 fatty acids?
Treating Other Factors
Smoking – offer aides to assist with stopping
Metabolic Syndrome: Elevated TGs, low HDL, Blood Pressure, waist circumference
1. congratulate on all his accomplishments
2. decrease ETOH
3. weight loss
4. exercise

9/13/2017
21
Thank you for your
kind attention
We will now open the
floor to questions &
discussion