EFFECTS OF SOCIOECONOMIC AND GEOGRAPHICAL FACTORS … PROJECT.pdf · As a result of concerted...
52
EFFECTS OF SOCIOECONOMIC AND GEOGRAPHICAL FACTORS IN THE UTILISATION OF IMMUNISATION SERVICES IN THREE SELECTED LOCAL GOVERNMENT AREAS OF ANAMBRA STATE, NIGERIA. Submitted by DR NJELITA CHUKWUDI UCHENNA (PGD/MPH/05/45394) IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE AWARD OF MASTER OF PUBLIC HEALTH DEPARTMENT OF COMMUNITY MEDICINE FACULTY OF MEDICAL SCIENCES UNIVERSITY OF NIGERIA SUPERVISOR: PROF CHIKA ONWASIGWE DEPARTMENT OF COMMUNITY MEDICINE FACULTY OF MEDICAL SCIENCES UNIVERSITY OF NIGERIA MAY 2009
Transcript of EFFECTS OF SOCIOECONOMIC AND GEOGRAPHICAL FACTORS … PROJECT.pdf · As a result of concerted...

EFFECTS OF SOCIOECONOMIC AND GEOGRAPHICAL FACTORS IN
THE UTILISATION OF IMMUNISATION SERVICES IN THREE
SELECTED LOCAL GOVERNMENT AREAS OF ANAMBRA STATE,
NIGERIA.
Submitted by
DR NJELITA CHUKWUDI UCHENNA
(PGD/MPH/05/45394)
IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE AWARD OF
MASTER OF PUBLIC HEALTH
DEPARTMENT OF COMMUNITY MEDICINE
FACULTY OF MEDICAL SCIENCES
UNIVERSITY OF NIGERIA
SUPERVISOR: PROF CHIKA ONWASIGWE
DEPARTMENT OF COMMUNITY MEDICINE
FACULTY OF MEDICAL SCIENCES
UNIVERSITY OF NIGERIA
MAY 2009

- 1 -
EFFECTS OF SOCIOECONOMIC AND GEOGRAPHICAL FACTORS IN THE
UTILISATION OF IMMUNISATION SERVICES IN THREE SELECTED LOCAL
GOVERNMENT AREAS OF ANAMBRA STATE, NIGERIA.
Submitted by
DR NJELITA CHUKWUDI UCHENNA
(PGD/MPH/05/45394)
IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE AWARD OF
MASTER OF PUBLIC HEALTH
DEPARTMENT OF COMMUNITY MEDICINE
FACULTY OF MEDICAL SCIENCES
UNIVERSITY OF NIGERIA
SUPERVISOR: PROF CHIKA ONWASIGWE
DEPARTMENT OF COMMUNITY MEDICINE
FACULTY OF MEDICAL SCIENCES
UNIVERSITY OF NIGERIA
MAY 2009

- 2 -
DECLARATION
I hereby declare that the study reported herein was done by me and any assistance
received is also acknowledged and that I have not previously submitted this
dissertation in part or in full for any examination or publication.
--------------------------------------
DR CHUKWUDI NJELITA
DEPARTMENT OF COMMUNITY MEDICINE
FACULTY OF MEDICAL SCIENCES
UNIVERSITY OF NIGERIA

- 3 -
CERTIFICATION
I hereby certify that the work for this dissertation, “socioeconomic and geographical
differentials in the utilisation of immunisation services in three selected Local
Government Areas of Anambra state, Nigeria”.
Submitted by
Dr Njelita Chukwudi Uchenna
Was supervised by me
--------------------------
Prof Chika Onwasigwe
Dept of Community Medicine
University of Nigeria
----------------------------------------
Prof M. N. Aghaji
Head of Department of Community Medicine
University of Nigeria

- 4 -
DEDICATION
I wish to dedicate this project to the children who receive their immunisations at the
various primary Health Care Centers in Njikoka L. G. A. where I work as Medical
Officer of Health.

- 5 -
TABLE OF CONTENTS
Title page…………………………………..…………….1
Declaration……………………………………………….2
Certification ……………………………………….…... 3
Dedication …………………………………...................4
Table of contents………………………………….………5
List of Acronyms…………………………………………7
Definition of terms ……………………………………….9
List of Tables…………………………………………….10
Acknowledgement ……………………………….….…...11
Abstract ………………………………….……..…..…….12
CHAPTER ONE: INTRODUCTION
1.1 Background of the study………………………...14
1.2 Statement of the problem……………………......15
1.3 Rational for the study ……………………………17
1.4 Objectives of the study…………………………..18
CHAPTER TWO: LITERATURE REVIEW
2.1 A review of the immunization activities
in Anambra state .……………….………….……..19
2.2 Factor that affect utilisation of
Immunisation services ……………………………20

- 6 -
CHAPTER THREE: MATERIALS AND METHODS
3.1 Study Area……………………………………………26
3.2 Study Population…………………………………..…28
3.3 Study design …………………………………………28
3.4 Sample size estimation ………………………………28
3.5 Inclusion criteria …………………………………….29
3.6 Sampling technique ………………………………….29
3.7 Data collection ……………………………………….29
3.8 Data analysis …………………………………………30
3.9 Limitations …………………………………………..30
3.10 Ethical considerations ………………………………30
CHAPTER FOUR: RESULTS ………………………….31
CHAPTER FIVE: DISCUSSION ……………………….44
5.1 Conclusion ……………………………………………46
5.2 Recommendation ……………………………………..46
Reference ………………………………………………..47
Questionnaire ……………………………………………49

- 7 -
LIST OF ACRONYMS
BCG Baccille Calmette-Guerin
DPT Diphtheria-Pertussis-Tetanus
DFID Department for International Development
EPI Expanded Programme on Immunisation
FMOH Federal Ministry of Health
FGD Focus Group Discussion
FOS Federal Office of Statistics
IDI In-depth Interview
IPC Interpersonal Communication
IPDs Immunisation Plus Days
LGA Local Government Area
LID Local Immunisation Day
MICS Multiple Indicator Composite Survey
MOEP Ministry of Economic Planning
MOH Medical Officer of Health
MOH&SS Ministry of Health and Social Services
NGO Non-Governmental Organisation
NICS National Immunisation Coverage Survey
NID National Immunisation Day
NPC National Population Commission
NPI National Programme on Immunisation
OPV Oral Polio Vaccine

- 8 -
ORT Oral Re-hydration Therapy
PEI Polio Eradication Initiative
PHC Primary Health Care
PLA Participatory Learning and Action Approach
RI Routine Immunisation
TBAs Traditional Birth Attendants
UCI Universal Childhood Immunisation
UNICEF United Nations Children’s Fund
USP United States Pharmacopoeia Convention, Inc
VHWs Village Health Workers
WHO World Health Organisation
WPV Wild Polio Virus
FIC Fully Immunised Child/Children
FMoH Federal Ministry of Health
FOMWAN Federation of Muslim Women’s Organisations
GAVI Global Alliance for Vaccines & Immunisation
HBV Hepatitis B Vaccine
ICC Inter-agency Co-ordination Committee
ICHCS Integrated Child Health Cluster Survey
IMR Infant Mortality Rate
M&E Monitoring & Evaluation
NAFDAC National Agency for Food & Drugs’ Administration & Control
NC/CE National Co-ordinator/Chief Executive (NPI)
NDHS Nigeria Demographic & Health Survey
NICS Nigeria Immunisation Coverage Survey

- 9 -
NID National Immunisation Day/s
NPHCDA National Primary Health Care Development Agency
PAFA Population Activities’ Fund Agency
PATHS Partnership for Transforming Health Systems
PSVD Private Sector Vaccine Distributor
PTF Petroleum Trust Fund
SIA Supplemental Immunisation Activities
SMoH State Ministry of Health
SMoLG State Ministry of Local Government
SNID Sub-national Immunisation Day/s
TT Tetanus Toxoid
VPD Vaccine-preventable Disease/s
UN United Nations
UNDP United Nations’ Development Programme
UNICEF United Nations’ Children’s Fund
USAID United States’ Agency for International Development
WHO World Health Organisation
YF Yellow Fever
ZSDO Zonal State Desk Officer (NPI)
DEFINITION OF TERMS
1. Immunisation Coverage: The proportion of eligible children who have actually
received a particular immunisation.
2. Fully Immunised: A child who has received all the immunisations due to him
from birth to his present age.

- 10 -
LIST OF TABLES
Table 1: Socio-demographic characteristics of respondents 31
Table 2: Attitudes to immunization 33
Table 3: Factors that prevent taking the child to the immunization centre 34
Table 4: Problems that discourage going back to an immunization centre after a 35
Previous visit
Table 5: Amount paid for immunization in one visit 36
Table 6: Utilization of immunization services in relation to age 38
Table 7: Utilization of immunization services in relation to educational level 39
Table 8: Utilization of immunization services in relation to marital status 40
Table 9: Utilization of immunization services in relation to occupation 41
Table 10: Utilization of immunization services in relation to husband’s occupation 42
Table 11: Utilization of immunization services in relation to geographical location 43

- 11 -
ACKNOWLEDGEMENTS
I appreciate the assistance given to me by my supervisor Professor Chika Onwasigwe
in the prompt review of every stage of this research up to its final presentation.
Thanks to the Community Health Extension Workers in the local government system
of Anambra State for their co-operation in the data collection.

- 12 -
ABSTRACT
Objective: This survey studied the socio-economic factors that affect the uptake of
immunisation services in three selected Local Government Areas of Anambra State.
Materials and Methods: The study was a cross-sectional descriptive study.
Multistage sampling was done in which three LGAs were selected from the state;
these L.G.As are Njikoka, Ogbaru and Aguata. Four wards from each of these LGAs
were also selected. A research assistant was blindfolded and he randomly pointed a
number on the table of random numbers and the number was ‘3’. Every third house
was, therefore, entered in each ward to enquire for eligible respondents.
Only women of child bearing age who were present in the study area at the time of the
study were interviewed. Data collection instrument used is a semi-structured, pre-
tested, interviewer administered questionnaire. Research assistants were recruited
from the primary health centers in the selected wards.
Findings: As much as 53.7% of respondents knew that every child needs
immunization, while 55.1%, 35.1% and 18.2% believed that immunization should be
missed in the event of diarrhea, yellowness of the eyes and fever respectively. Up to
39.3% of women with only primary education missed their immunisation sessions
while 30% of women with tertiary education missed it. Only 23.5% of mothers who
are public/civil servants missed immunisation while 42.6% of mothers who are
farmers missed it. As high as 42% of women in Ogbaru (with very bad terrain) missed
immunisation while 23% of women in Njikoka (semi-urban) missed immunisation.
The study showed no correlation between the mother’s educational level and whether
she missed her child’s immunisation. This does not agree with the finding of National

- 13 -
Immunisation Coverage Survey (NICS) 2003;
there was a positive correlation
between mothers’ education and the fully immunised child: nationally 31.1% of
children of mothers with secondary education are fully immunised; the figure for
children of mothers with no education is 3.9%.3 The possible reason why this survey
varied from a previous study in 2003 is that public enlightenment campaigns on
immunisation have been so elaborately utilised in Anambra State that the importance
of immunisation is presently equally known to the illiterate as the literate.
Conclusion: The statistical significance of these compared variables shows that
occupation and geographical location significantly affect utilisation of immunisation
services in Anambra State, therefore, health education promotion and programming
must take into consideration such factors.

- 14 -
CHAPTER ONE
Introduction
1.1 Background of the study
In 1979 Nigeria’s Expanded Programme on Immunization (EPI) was initiated, and
was placed within the Department of Public Health and Communicable Disease
Control of the Federal Ministry of Health (FMOH) 1
. It was re-launched in 1984 due
to poor coverage.2
In 1996 it became the National Programme on Immunisation (NPI),
launched by the then First Lady, Mrs Abacha. Following a review of EPI, Decree 12
of 1997 created NPI as a parastatal. NPI has a sole responsibility of supervising and
enhancing routine and supplemental immunisations in Nigeria. 2
Routine immunisation (RI) is provided largely through the public health system, with
significant variations between the 36 States and Federal Capital Territory (FCT);
private or NGO providers are the source of up to one-third of RI in Anambra state.3
Public sector provision is by health staff based at facilities run by the 21 Local
Government Areas (LGAs) who have a Primary Health Care Coordinator (PHCC), a
Local Immunisation Officer and a Cold Chain Officer. These staff members are under
the control of the Head of Local Govt Administration and are employees of the State
Government (Ministry of Local Government and Local Government Service
Commission).

- 15 -
Routine immunisations are done at the fixed posts in the health centres, health posts,
General hospitals and tertiary health facilities in the State. Supplemental
immunisations in the State are aimed at boosting the immunisation coverage and
mopping up missed opportunities.2 It also becomes imperative in epidemics.
2 These
supplemental immunisations are achieved through National Immunisation Days
(NIDs), Local Immunisation Days (LIDs), Immunisation Plus Days (IPDs) and Child
Health Week. 2
1.2 STATEMENT OF THE RESEARCH PROBLEM
Since they were first introduced in 1956, immunization activities in Nigeria have been
characterised by intermittent successes and failures.1 The expanded programme on
immunisation (EPI) introduced in 1979 with the aim of providing immunisation
services to children aged 0 – 23 months, experienced some initial success. However, a
few years after the programme started, it became obvious that it was no longer
achieving its stated objectives and had to be re-launched in 1984. 2
As a result of concerted efforts of the Federal Ministry of Health, State agencies, and
International Organisations, Nigeria attained universal childhood immunisation (UCI)
with 81.5 percent coverage for all antigens in 1990. 2
The success was not to last long
and by 1996, immunisation coverage had declined substantially to less than 30
percent for DPT3 and 21 percent for the three doses of oral poliovirus vaccine
(OPV).2 The situation has become even worse since then despite considerable donor
and Federal Government efforts to improve the provision and promotion of
immunisation services.

- 16 -
Today, coverage rates for the various childhood vaccines in Nigeria are among the
lowest in the world.3 Nigeria is now considered the greatest threat to the global
eradication of polio and there is an urgent need to address the problems facing
immunisation activities in the country and increase coverage.3
Research in other parts of the world has shown that social factors, economic factors,
community and systemic factors affect immunisation coverage. These factors are
potentially modifiable.
Anambra State, centrally located in the south eastern zone of the Federal Republic of
Nigeria is not immune to the catalogue of problems facing immunisation uptake in
Nigeria. Since the mid-1990s, Anambra State has continued to witness fluctuations in
immunisation coverage for all vaccine-preventable diseases and this has had grave
consequences on children’s health and survival. Data from the 2003 National
Immunisation Coverage Survey reveal a very gloomy picture with only 12.7 percent
of children aged 12-23 months receiving full immunisation service. Of great
significance and concern is the emerging status of Nigeria as the country with the
highest number of Wild Polioviruses (WPV) in the world. Increased widespread
transmission of the WPV was reported in the highly endemic States of Kano, Katsina,
Jigawa, Kaduna and Bauchi, while a fresh outbreak of WPV was confirmed in Kebbi.
Of epidemiological importance to Anambra State is the recent incident of WPV
outbreak in the neighbouring state of Enugu.
Against this background, the goal of this study is to provide data that would assist
programme staff and policy makers to design strategic interventions to improve
immunisation coverage in Anambra State in particular and Nigeria in general.

- 17 -
1.3 RATIONAL FOR THE STUDY
Routine immunization against DPT, measles, polio and TB is proven to be one of the
most cost-effective interventions for reducing childhood illness and mortality,
especially with the addition of other vaccines such as CSM and yellow fever in
endemic areas and TT injections for pregnant women1 and yet national coverage in
Nigeria for full immunization is less than 13%, one of the lowest rates in the world,
even lower than many countries in conflict, such as DRC.4 Some states in northern
Nigeria have coverage rates below 1%, and the average for the whole North West
Zone is just 4%. These coverage figures are much worse than in the neighbouring
countries of Benin, Niger, Chad and Cameroon. Both the Nigeria Demographic and
Health Survey (NDHS 2003), conducted by the National Population Commission, and
the Nigeria Immunization Coverage Survey (NICS 2003), conducted by the National
Programme on Immunization (NPI), provide the same irrefutable evidence.8 Nigeria’s
performance on routine immunization has continued to decline since the high point
achieved around 1990.
Vaccine-preventable deaths
In Nigeria, one child in five dies before its fifth birthday.8 This represented about
872,000 childhood deaths in 2002. Vaccine-preventable diseases (VPDs) account for
about 22% of deaths,4 therefore over 200,000 children a year are dying needlessly of
VPDs. Various well meaning researchers have conducted credible studies with a view
to unravelling the root cause of this decline in immunisation uptake. This research
study in three selected Local Government Areas in Anambra State is at discovering
the possible local causes of this decline in immunisation uptake in Anambra State.
The result of this research is meant to inform the health policy makers of the state on

- 18 -
areas of hence enhance rational resource allocation. The public will benefit from this
research as the result when published will show statistically the state of immunisation
activities in these selected LGAs.
1.4 OBJECTIVES OF THE STUDY
General Objective
The general objective of this study is to identify socioeconomic and geographical
factors which affect the utilisation of immunisation services in Anambra State.
Specific Objectives
The specific objectives of the study are to:
1. Identify the social, economic and geographical pattern of people requiring
immunisation services in Anambra State.
2. Assess the effect of social, economic and geographical factors on
immunisation uptake.
3. Identify factors hindering or fostering immunisation in the state.

- 19 -
CHAPTER TWO
LITERATURE REVIEW
2.1 A REVIEW OF IMMUNISATION ACTIVITIES IN ANAMBRA STATE.
Immunisation remains one of the cheapest and most cost effective means of protecting
the masses from vaccine preventable diseases.1 It has been widely employed in the
prevention and control of epidemic and endemic diseases in Nigeria since 1956.1
National Programme on Immunisation is the parastatal saddled with the responsibility
of immunisation in Nigeria.1
Another parastatal, the National Primary Health Care
Development Agency (NPHCDA), has responsibilities in immunisation. The
Anambra State office of the NPI oversees immunisation activities in the state. Routine
Immunisation (RI) is the major focus of the NPI.1 It has a schedule in Nigeria for the
full immunisation of every child before the age of one. Nigeria’s immunization
schedule contains tetanus toxoid (TT), BCG, Hepatitis B vaccine (HBV), OPV, DPT,
measles, cerebro-spinal meningitis vaccine (CSM) for types A and C, and yellow
fever (YF). 1
CSM is administered in an annual campaign in susceptible areas in the
north of Nigeria, to age groups which vary according to the quantity of vaccine
supplied.
Apart from the RI, the NPI employs supplemental immunisation to enhance
immunisation coverage. This is seen in the Polio Eradication Initiative (PEI). National
activities for polio eradication started in 1996, and the global effort to eradicate polio

- 20 -
has made PEI National Immunisation Days (NIDs) and Sub-NIDs the main focus of
NPI’s attention since 1998.
“One of the problems with NIDs is that it tends to undermine the importance of the
routine immunization. The publicity given to NIDs usually makes the routine look
like it is non-existent. However, recently RI has received some attention in Nigeria
through the series of trainings of health workers in RI by European Union Partnership
to Reinforce Immunisation Efficiency (EU-PRIME) in 18 states of the federation
including Anambra state. Cases of polio genetically linked to the wild polio virus is
endemic in Nigeria. This has recently been discovered in Enugu State which is a close
neighbour to Anambra state.4 This WPV has been found not only in 13 African
countries but also in Indonesia and Yemen. 4
In spite of the considerable efforts that
have been put into immunisation programme in Nigeria, immunisation uptake remains
generally low in the country, especially in the northern states. Each year, thousands of
children die or are maimed for life as a result of diseases that are preventable through
immunisation. Preliminary results from the 2003 Demographic and Health Survey
(DHS) revealed a DPT3 coverage rate of 21% among children aged 12 – 23 months.
Moreover, Nigeria remains one of the few reservoirs of polio around the world. Data
for 2003 shows that with 347 cases, Nigeria has the highest number of children
paralysed by the poliovirus.
2.2 FACTORS THAT AFFECT UTILISATION OF IMMUNISATION
SERVICES.
In 2004 survey on the individual and community factors affecting the uptake of
immunization in four northern and two southern states of Nigeria, a total of 7200
respondents, mostly women with under-5 children, were interviewed. One finding

- 21 -
from the survey is that there is a strong correlation between household poverty level
(measured in terms of the socio-economic status of the household) and the prevalence
of full immunization.5 The paper also explored the mediating role of mother's
decision-making power in this relationship. It was deduced that the stronger the
mothers decision-making power, the higher the likelihood of full immunisation. The
woman's decision-making power was measured through a set of questions that
assessed the woman's contribution to specific household decisions.5
This study by Babalola showed that poverty is likely to distract parents from placing
high premium on disease prevention as is the case in immunisation. This must be due
to the pressure on the family scarce resources hence giving the men and women no
chance to think about essentials like immunisation. This study clearly showed that the
lower the socio-economic class, the less likelihood for full immunisation. Furthermore,
the study showed that spousal communication around child immunization
significantly is a function of education, socio-economic status and exposure to
immunization-related information on the media or through community sources.
Specifically, spousal communication increases steadily with the woman’s education
such that the women least likely to report discussion with their spouse are the
illiterates. Exposure to immunization related information is associated with increased
spousal communication, indicating that the information obtained served as a point for
discussion about immunization among spouses.
In a study of the effects of geographical differentials in the utilisation of immunisation
services, Jegede et al x rayed the accessibility of information on immunisation to

- 22 -
Nigeria women.6 A random sample of 1,554 women of reproductive age who have
given birth to, at least one child in the last five years in the south-east Zone of Nigeria
were recruited for the study. Their responses indicated limited access to information
in the rural areas than the urban areas. For those who have received information in the
urban areas, their major sources of information are electronic media (television and
radio), whereas the main sources of information in the rural areas were health workers,
traditional rulers, friends and neighbours. These sources differed by place of residence,
age, level of education and occupation of mothers. Data showed that respondents from
urban areas utilise immunisation better than those in the rural areas. Thus, it is
concluded that access to health information may be influenced by geographical
location and social class, therefore, health education promotion and programming
must take into consideration such factors.6
Elsewhere, a study done by Christopher Oluwadare on the social determinants of
routine immunisation in Ekiti State of Nigeria in 2005 concluded that the biggest
factor affecting uptake of immunisation appears to be whether a family lives in a rural
area or a town. This rural/urban factor is linked directly to the availability of services.
Most rural areas are without a sitting qualified nurse or senior health officer and most
are left to the least skilled assistants. Access to central supply of vaccines is hindered
by poor commitment to the service, non release of financial support and bad road
networks. Other rural people must travel considerable distances to urban health
facilities to access routine immunisation offered on specific days. Although many
health workers claimed to carry out ‘outreach’ for routine immunisation to rural areas,
there was no evidence of it.7

- 23 -
Public health specialists see immunisation as one of the most accessible primary
health interventions. In many countries routine immunisation coverage for the poorest
group is lower than for higher income groups, but the disparity is less marked than for
other health interventions.8
In Nigeria widespread differences persist in immunisation
coverage. The child of parents in the lowest socio-economic quartile is nearly 12
times less likely to be immunised than children of parents in the highest. There is a
positive correlation between mothers’ level of education and the fully immunised
child: nationally 31.1% of children of mothers with secondary education are fully
immunised; the figure for children of mothers with no education is 3.9%. Children in
rural areas, especially in the north, are particularly disadvantaged.
The NICS (2003) states that nationally 7% of rural children and 25% of urban
children have been fully immunised. Full immunisation coverage is less than 13%
nationally, and below 4% in the North West Zone.8
Among the population as a whole,
only 70% of Nigerians had access to health care of any description (public, private,
traditional; primary, secondary, tertiary) in 2001. This figure is lower in rural areas.9
Barrier to equitable routine immunisation access and uptake remains a challenge to
many Nigerians.9 Barriers may be gender-linked (e.g. women not wishing to see a
male health worker; women not being given permission to visit a health facility with
their child); financial (e.g. inability to pay for transport, vaccine and/or syringes);
physical (e.g. terrain and amount of time needed to trek to the nearest health facility).
There may be opportunity costs (e.g. time taken out from wage labour).9

- 24 -
Incorrect knowledge as to the preventive role of routine immunisation is widespread
in Nigeria. Quantitative research conducted in six States in 2004 reveals that in rural
Enugu, diarrhoea, fever, convulsion, vomiting and malaria are believed to be vaccine-
preventable diseases (VPDs), while in rural and urban Kano, malaria, teething
problems, vomiting, convulsion and pneumonia are listed.10
During pilot community
research in March 2005 a number of immunisation decision-makers and caregivers in
Katsina State stated that polio immunisation is all that is required: once a child has
received its polio ‘drops’, it is immunised against any childhood illness, including
those for which there is no vaccine available, e.g. acute respiratory infection.11
Those
least likely to demonstrate high levels of correct knowledge include people who do
not use public facilities for the treatment of common illnesses, those who lack easy
access to public health facilities, and illiterates.13
Many decision-makers and caregivers reject routine immunisation due to rumour,
incorrect information, and fear. The National Immunisation Coverage Survey 2003
report describes such perceptions as ‘wrong ideas’: this is an inadequate interpretation.
Attempts to increase coverage must seek to understand people’s attitudes and the
influence of these on behaviour. Fears regarding routine immunisation are expressed
in many parts of Nigeria. Fathers of partially immunised children in Muslim rural
communities in Lagos State see hidden motives, linked with attempts by NGOs
sponsored by unknown enemies in developed countries, to reduce the local population
and increase mortality rates among Nigerians.3 Belief in a secret immunisation agenda
is resonant in Jigawa, Kano and Yobe States, where many believe activities are

- 25 -
fuelled by Western countries determined to impose population control on local
Muslim communities.10, 13
Confusion remains high in Katsina, with several issues emerging: not only lack of
correct knowledge, but uncertainty as to the reasons why a healthy infant should
receive an injection. Understanding the links between preventive health care and good
health is often weak; as a result, there is growing fear of the possibility of infection
and disease.13
Other factors contributing to rejection of routine immunisation include an apparently
deep-rooted suspicion in Kano State of western-style health services, dating from the
1980s. These suspicions link to national population policy: some northerners continue
to see routine immunisation as a means of fertility control. The situation is said to
have been exacerbated by drug trials by an American company, apparently conducted
without proper ethical standards and approval, which led to children’s deaths.12
Lack of confidence and trust in routine immunisation as effective health interventions
appear to be relatively common in many parts of Nigeria.13
A 2003 study in Kano
State found that 9.2% of respondents (mothers aged 15-49) had ‘no faith in
immunisation’, while 6.7% expressed ‘fear of side reactions’.14
For many,
immunisation is seen to provide at best only partial immunity, e.g. in Kano and
Enugu.10
The widespread misconception that immunisation can prevent all childhood
illnesses reduces trust: when, as it must, immunisation fails to give such protection,
faith is lost in immunisation as an intervention, for any or all diseases.

- 26 -
CHAPTER THREE
MATERIALS AND METHODS
3.1 STUDY AREA
The area for this study is three Local Governments in Anambra State; Njikoka,
Aguata and Ogbaru. Anambra State is in the south-eastern zone of Nigeria. Anambra
people are predominantly of the Igbo tribe. It is in the rain forest region. The state has
total population estimated at 5 million. There are 21 local governments in the state
with Awka as the state capital. There are urban, semi-urban and rural LGAs in the
state. For the purpose of this study, three LGAs have been selected.
1. NJIKOKA LGA
Njikoka Local Government Area was created in 1976 and it is one of the twenty one
LGAs in Anambra state with headquarters at Abagana. It is bound in the North by
Awka North LGA and Awka South LGA and in the South by Dunukofia LGA. It has
a target population for routine immunization for children under the age of one and
pregnant women as 6,276 and 7,845 respectively and a total population of 156,895
from the 2006 census. It is classified as semi urban LGA of the state and is occupied
by mostly Igbos. They are predominantly traders. The indigenes are mainly Christians
with Roman Catholic and Anglican adherents dominating others. Njikoka Local
Government Area is made up of 7 districts, 18 political wards and 93 settlements.
There are 22 health facilities that provide routine immunization in Njikoka LGA.8

- 27 -
2. PROFILE OF OGBARU LGA
Ogbaru LGA is one of the twenty-one LGAs in Anambra State with its headquarters
at Atani. It has a population of 133,066. It is one of the largest LGA in the state
tapering towards the Okpoko end in the north and broadening towards the Ogwu-
Aniocha and Ogwu-Ikpele communities in the south. The River Niger covers the
whole North West and south west of the LGA. It shares boundaries with Onitsha
South, Idemili North, Ekwusigo and Ihiala LGAs in the northeast and southeast areas
of the LGA. The LGA is bound in the south by Delta and Rivers states. There are
twenty-eight health facilities in Ogbaru LGA. They all provide routine immunization.
Generally the LGA has a very bad terrain throughout the year that worsens during the
rainy season when River Niger overflows its banks and blocks the only major link
road (Onitsha-Atani road) that traverses the LGA. The Igbos are the dominant tribe in
the LGA. The inhabitants are predominantly yam and vegetable farmers and
fishermen. There are twelve health districts and sixteen political wards in Ogbaru
LGA. The wards are Atani 1 and 11; Iyiowa/Odekpe/Ohita; Akili Ozizor;
Ochuche/Ogbakuba/Amiyi/Umuzu; Umunankwo/Mputu; Ossomala; Akili
Ogidi/Obeagwe; Ogwu-Ikpele; Ogwuaniocha; Okpoko1, 11,111,1V,Vand V1.8
3. PROFILE OF AGUATA LGA
Aguata LGA is one of the largest and oldest LGA in Anambra State. It is located at
the northern part of Anambra State. It is bound in the north by Orumba North; in the
south by Akokwa in Abia state; and at the east by Orumba South. The people of
Aguata LGA are predominantly Christians. They are mainly farmers, traders and civil
servants. Aguata LGA has areas of thick forests, erosion sites and gullies around

- 28 -
Umuchu, Igboukwu, and Ora-Eri communities. The indigenes are mostly Igbo
speaking people. It has twenty districts and fourteen autonomous communities with
forty-two health facilities that provide routine immunization. They are: Ekwulobia,
Isuofia, Igboukwu, Ora-Eri, Ikenga, Umuona, Ezinifite, Amesi,Achina,
Aguluezechukwu, Nkpologwu, Umuchu, Uga and Akpo. Aguata LGA has twenty-one
districts with seven health centers and fifteen health posts. Routine immunizations are
carried out at these facilities. Aguata LGA has a population of about 163,301 and
routine immunization population (0-11mths) of 6,532.
3.2 STUDY POPULATION
The study population is women of child bearing age. A sample of this population was
studied.
3.3 STUDY DESIGN
It is a cross-sectional descriptive study.
3.4 SAMPLE SIZE ESTIMATION
n = z2pq
15
d2
Where,
n = the minimum sample size
z = standard normal deviate (1.96) at confidence level of 95%.
p = proportion of women of child bearing age in

- 29 -
Anambra State. (22% = 0.22). 1
q = 1.0 – p = 1- 0.22 = 0.78
d = degree of accuracy desired. (0.05)
Therefore,
n = 1.96 x 1.96 x 0.22 x 0.78
0.05 x 0.05
n = 0.6592
0.0025
n = 263.68 (approx. 264)
3.5 INCLUSION CRITERIA
The study was of women, who were of child bearing age and were in Anambra State
at the time of this study,
3.6 SAMPLING TECHNIQUE
Multistage sampling technique was used.16
Anambra State is the study area. Three
LGAs were selected from the state by simple random sampling. Four wards from each
of these LGAs were also selected by simple random sampling. A research assistant
was blindfolded and he randomly pointed a number on the table of random numbers
and ‘3’ was picked, therefore, every third house was entered in search of eligible
respondents. At the village square of the selected wards, a coca-cola bottle was spun
on the ground to randomly determine the direction to be followed by the data
collectors. The questionnaires were equally distributed in the three LGAs
3.7 DATA COLLECTION
Data collection instrument used is a structured, pre-tested, interviewer administered
questionnaire. The questionnaire was validated by pre-testing it in a small survey of

- 30 -
20 respondents conducted in Urum, Awka North L.G.A. Data collectors who were
recruited from the primary health centers in the selected wards were thoroughly
trained in the meanings of all the terms in the questionnaire. The data from the pre-
test did not form part of the study.
3.8 DATA ANALYSIS
Data collected were entered into computer and analysed using the SPSS version 13.
The relevant means and standard deviations were calculated. The confidence limit of
this study is 95%; therefore the hypothesis was tested at 0.05 level of significance.
Chi-square test was also done to ascertain the significance levels between proportions.
3.9 LIMITATIONS
The limitation we had was that we were in short supply of funds for transporting the
interviewers around throughout the period of the research.
3.10 ETHICAL CONSIDERATIONS
Ethical clearance was obtained from the Health Research Ethics Committee of the
University of Nigeria Teaching Hospital Ituku-Ozalla. Verbal consent was obtained
from respondents before the administration of questionnaires.

- 31 -
CHAPTER FOUR
RESULTS
300 questionnaires were distributed but 285 were appropriately filled and returned
from the field, therefore the response rate was (285/300 X 100%) = 95%
Table 1: Socio-demographic characteristics of respondents
Characteristic Frequency (n = 285) Percent Age group (years):
15 – 19 24 8.4
20 – 24 56 19.5
25 – 29 66 23.2
30 – 34 64 22.5
35 – 39 43 15.1
≥ 40 32 11.3
Educational level:
Primary school 28 9.8
Secondary attempted 42 14.7
Secondary completed 126 44.3
Tertiary attempted 49 17.2
Tertiary completed 40 14.0
Marital status:
Married 241 84.5
Divorced 23 8.1
Single 15 5.3
Widowed 6 2.1
Occupation:
Public / civil servant 132 46.3
Trader 127 44.6
Farmer 26 9.1
Husband’s occupation:
Public / civil servant 160 56.1
Trader 110 38.6
Farmer 15 5.3
Mean age of respondents = 29.6 years, standard deviation = 7.3 years

- 32 -
The mean age of the respondents was 29.6 years with standard deviation of 7.3 years
and most fell within the age range of 25-34 years, followed by 20-24 while 15-19 year
age range has the least number of respondents. The modal educational level of
respondents was secondary completed. Women of child bearing age in Anambra State
were predominantly literate. Most of them were literate with over 90% having
attended a minimum of secondary education. 9.1% of them were farmers while 46.3%
and 44.6% of them were public/civil servants and traders respectively.

- 33 -
Table 2: Knowledge/Conception to immunization
Knowledge/Conception Frequency (n = 285) Percent
Every child needs immunization 153 53.7
A child’s immunization should be
missed if there is:
Diarrhoea 157 55.1
Yellowness of the eyes 100 35.1
Fever 52 18.2
Findings on correct knowledge of immunization revealed that 53.7% knew that every
child needs immunization. While 46.3%, believed that immunization should be
missed in the event of diarrhea, yellowness of the eyes or fever. There were multiple
entries. This shows that more that half of the population surveyed had the right
attitude towards immunisation.

- 34 -
Table 3: Factors that mostly prevent taking the child to the immunization centre
Factor Frequency Percent
Husband’s decision 115 40.4
Lacks knowledge of the need for
immunisation 111 38.9
Bad roads 28 9.8
Long distance 14 4.9
Religious belief 13 4.6
Others 4 1.4
Total 285 100.0
There was a very high dependence on the decision of the husbands for a child’s
immunisation. This is shown in Table 3 where 40.4% of the women would see
husband’s decision as the commonest reason for missing an immunisation session.
Lack of knowledge of the need for immunisation is viewed by 38.9% as the most
deterring factor as they don’t know why, where and when they should get immunised.

- 35 -
Table 4: Problems that discourage going back to an immunization centre after a
previous visit
Problem Frequency (n 285) Percent
Health workers’ attitude 119 41.8
Long waiting time at the health
facility 104 36.5
Long distance 51 17.9
Immunization charges 15 5.3
Unavailability of vaccines 4 1.4
Table 4 shows that the most frequent reason for not going back to an immunisation
centre after a previous visit was health workers’ attitude. This is followed by the long
waiting time at the centre.

- 36 -
Table 5: Amount paid for immunization in one visit
Amount in Naira Frequency (n 285) Percent
< 200 59 20.7
200 – 500 223 78.2
> 500 3 1.1
Total 285 100.0
Table 5 shows that most of the women (78.2%) paid between 200 and 500 Naira in
one immunisation visit.

- 37 -
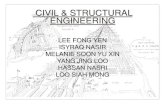
Fig 1: Utilization of immunization services
Above is a pie chart which shows that 68.1% of the respondents did not miss their
immunisation at any time.

- 38 -
Table 6: Utilization of immunization services in relation to age
Age group (years) Missed
immunization
Did not miss
immunization
Total (%)
Frequency (%) Frequency (%)
< 30 42 (28.8) 104 (71.2) 146 (100.0)
≥ 30 49 (35.3) 90 (64.7) 139 (100.0)
Total 91 (31.9) 194 (68.1) 285 (100.0)
χ2 = 1.378, df = 1, p = 0.240 (not statistically significant)
This table compares two age groups of the respondents; below 30years and above 30
years with compliance to immunisation. The chi square test shows that there is no
significant association between the two variables.

- 39 -
Table 7: Utilization of immunization services in relation to educational level
Educational level Missed
immunization
Did not miss
immunization
χ2 p-value
Frequency (%) Frequency (%)
Primary school (n = 28) 11 (39.3) 17 (60.7) 0.773 0.379
Secondary attempted (n =
42) 18 (42.9)
24 (57.1) 2.706 0.100
Secondary completed (n =
126) 33 (26.2)
93 (73.8) 3.423 0.064
Tertiary attempted (n =
49) 17 (34.7)
32 (65.3) 0.208 0.648
Tertiary completed (n =
40) 12 (30.0)
28 (70.0) 0.080 0.778
Total (n = 285) 91 (31.9) 194 (68.1)
χ2 = 5.155, df = 4, p = 0.272 (not statistically significant)
This table compares the educational level of the respondents with compliance to
immunisation. Women who completed their secondary education and those who had
tertiary education fared better in immunising their children, although there was no
statistically significant difference among the various educational levels.

- 40 -
Table 8: Utilization of immunization services in relation to marital status
Marital status Missed
immunization
Did not miss
immunization
χ2 p-value
Frequency (%) Frequency (%)
Married (n = 241) 75 (31.1) 166 (68.9) 1.131 0.287
Divorced (n = 23) 9 (39.1) 14 (60.9) 0.597 0.440
Single (n = 15) 4 (26.7) 11 (73.3) 0.027 0.869Y
Widowed (n = 6) 3 (50.0) 3 (50.0) 0.267 0.065Y
Total (n = 285) 91 (31.9) 194 (68.1)
Y = Yates correction
χ2 = 1.714, df = 3, p = 0.634 (not statistically significant)
This table compares the marital status of the respondents with compliance to
immunisation. The table shows that marital status does not affect compliance to
immunisation. There were no significant variations in compliance among the various
groups.

- 41 -
Table 9: Utilization of immunization services in relation to occupation
Occupation Missed
immunization
Did not miss
immunization
χ2 p-value
Frequency (%) Frequency (%)
Public / civil servant (n =
132) 31 (23.5)
101 (76.5) 8.086 0.005*
Trader (n = 127) 48 (37.8) 79 (62.2) 3.626 0.057
Farmer (n = 26) 12 (46.2) 14 (53.8) 2.663 0.103
Total (n = 285) 91 (31.9) 194 (68.1)
*Statistically significant
χ2 = 8.762, df = 2, p = 0.013 (statistically significant)
Table 9 compares the occupation of the respondents and their compliance to
immunisation. The table shows that occupation affects compliance to immunisation.
Farmers were more likely to miss immunisation appointments than traders and traders
more than public/civil servants. This association was tested using the Chi square and
it showed statistical significance.

- 42 -
Table 10: Utilization of immunization services in relation to husband’s occupation
Occupation Missed
immunization
Did not miss
immunization
χ2 p-value
Frequency (%) Frequency (%)
Public / civil servant (n =
160) 55 (34.4)
105 (65.6) 1.004 0.316
Trader (n = 110) 30 (27.3) 80 (72.7) 1.788 0.181
Farmer (n = 15) 6 (40.0) 9 (60.0) 0.474 0.491
Total (n = 285) 91 (31.9) 194 (68.1)
χ2 = 1.987, df = 2, p = 0.370 (not statistically significant)
This table compares the occupation of the respondent’s husband and their compliance
to immunisation. The table shows that Husband’s occupation does not affect
compliance to immunisation. There were no significant variations in compliance
among the various groups.

- 43 -
Table 11: Utilization of immunization services in relation to geographical location
(LGA)
LGA Missed
immunization
Did not miss
immunization
χ2 p-value
Frequency (%) Frequency (%)
Njikoka (n = 100) 23 (23.0) 77 (77.0) 5.652 0.017
Ogbaru (n = 100) 42 (42.0) 58 (58.0) 7.188 0.007
Aguata (n = 85) 26 (30.6) 59 (69.4) 0.100 0.751
Total (n = 285) 91 (31.9) 194 (68.1)
χ2 = 8.405, df = 2, p = 0.015 (statistically significant)
This table compares the geographical location of the respondents and their
compliance to immunisation. The table shows that geographical location affects
compliance to immunisation. Ogbaru women were more likely to miss immunisation
appointments than Aguata women and Aguata women more than Njikoka women.
This association was tested using the Chi square and it showed statistical significance

- 44 -
CHAPTER FIVE
DISCUSSION
The study was conducted on the socio-economic and geographical differentials in the
utilization of immunization services in Anambra State of Nigeria. A total of three
local government areas were studied under the following socio-demographic
parameters; age group, educational level, marital status, occupation and husband’s
occupation.
Findings from this study showed that the husbands’ decision (40.4%) was the factor
that most often prevented a child’s immunisation. This showed the role of the husband
in the Igbo family system. Critical decisions in a family are usually the sole
responsibility of the husband. There are, however, some variations in cases where the
woman is well educated or the bread winner of the family. In 2004 survey on the
individual and community factors affecting the uptake of immunization in four
northern and two southern states of Nigeria, a total of 7200 respondents, mostly
women with under-5 children, were interviewed. The paper explored the mediating
role of mother's decision-making power in this relationship. It was deduced that the
stronger the mothers decision-making power, the higher the likelihood of full
immunisation. The woman's decision-making power was measured through a set of
questions that assessed the woman's contribution to specific household decisions.5
The study showed no correlation between the mother’s educational level and whether
she missed her child’s immunisation. This does not agree with the finding of National

- 45 -
Immunisation Coverage Survey (NICS) 2003;
there was a positive correlation
between mothers’ education and the fully immunised child: nationally 31.1% of
children of mothers with secondary education are fully immunised; the figure for
children of mothers with no education is 3.9%.3 The possible reason why this survey
varied from a previous study in 2003 is that public enlightenment campaigns on
immunisation have been so elaborately utilised in Anambra State that the importance
of immunisation is presently equally known to the illiterate as the literate.
Only 23.5% of mothers who are public/civil servants missed immunisation while
42.6% of mothers who are farmers missed it. An association was found between the
respondent’s occupation and completeness of their child’s immunisation. This is
comparable with the study by Babalola in 2004 on the individual and community
factors affecting the uptake of immunization in four northern and two southern states
of Nigeria, One finding from the survey is that there is a strong association between
household poverty level (measured in terms of the socio-economic status of the
household) and the prevalence of full immunization.5 This study by Babalola showed
that poverty is likely to distract parents from placing high premium on disease
prevention as is the case in immunisation. This must be due to the pressure on the
family scarce resources hence giving the men and women no chance to think about
essentials like immunisation. This study clearly showed that the lower the socio-
economic class, the less likelihood for full immunisation.
This study showed that 23% of the respondents in Njikoka Local Government, a semi-
urban L.G.A missed immunisation while 42% of respondents in Ogbaru, a
predominantly rural L.G.A. with difficult terrain missed immunisation. The study

- 46 -
showed a association between geographical location and likelihood for full
immunisation. This agrees with a previous study done by Christopher Oluwadare on
the social determinants of routine immunisation in Ekiti State of Nigeria in 2005 in
which he concluded that the biggest factor affecting uptake of immunisation appears
to be whether a family lives in a rural area or a town. This rural/urban factor is linked
directly to the availability of services.7
5.1 CONCLUSIONS
Husband’s decision is the most important factor that prevents a child’s
immunisation.
Health workers’ attitude is the biggest factor that deters mothers from going
back for further immunisation after an initial immunisation session.
Educational level has no association with adherence to immunisation schedule
in Anambra State unlike elsewhere.
Mother’s occupation has a direct association with adherence to immunisation
schedule
Geographical location has direct association with adherence to immunisation
schedule. People in urban areas are more likely to be fully immunised than
people in rural areas.
5.2 RECOMMENDATIONS
A more detailed study should be done to analyse the husband decision
factor as it affects immunisation of a child.
Further study should be carried out on the effect of educational level
on immunisation in Anambra State.

- 47 -
REFERENCES
1. National Programme on Immunisation (NPI). Basic Guide for Routine
Immunization service providers, 2nd edition, Abuja, Amana publishers, 2004.
2. Awosika A. Boosting Routine Immunization in Nigeria: issues and proposed
action points, power point presentation developed by NPI and BASICS, Abuja,
September 2000.
3. National Programme on Immunisation (NPI). National Immunisation coverage
survey, Abuja, 2003.
4. World Health Organisation (WHO). Global Summary on immunization,
www.who.int/vaccines/globalsummary/immunization/countryprofileresult.cfm
(accessed 20th March 2009)
5. Babalola S O. Poverty and immunization coverage in Nigeria: the mediating
role of mothers’ decision making power, a presentation at the 133rd annual
meeting and exposition of American Public Health Association10th – 14th
December 2005, Philadelphia, PA, 2005.
6. Jegede A S, Idemudia E, Madu S N. Factors affecting access to health
information among Nigerian nursing mothers. Research for Development,
2004 vol 6 pg 15.
7. Oluwadare C. The social determinants of routine immunization in Ekiti State
Nigeria, department of sociology, University of Ado Ekiti, Ado Ekiti, Nigeria.
2005, vol 3 pg 20.
8. National population commission (NPC). Nigeria demographic and health
survey 2003, Abuja, 2004.

- 48 -
9. United Nations’ Development Programme (UNDP). Human development
Report, New York, 2004.
10. Babalola S, Aina O. Community and systemic factors affecting the uptake of
immunization in Nigeria: A qualitative study in five states, Abuja, 2004.
11. Brieger W R, Salami K K, Ogunlade B P. Catchment area planning and
action: Documentation of the community-based approach in Nigeria,
Arlington, Va, BASICS II for USAID, 2004.
12. Brieger W R. The polio epidemic in Nigeria; a public health emergency,
2004. www.nigeriavillagesquare1.com (accessed on 15th April 2009).
13. Babalola S. and Adewuyi. Addendum to existing qualitative and quantitative
immunization survey. Health-link international for PATHS, London & Abuja,
2005.
14. Yola A W. Report on Child Immunization Clusters Survey (CICS)
conducted in 12 LGs of Kano State, BASICS II, Lagos, 2003.
15. Araoye M O. Research methodology with statistics for health and social
sciences. Ilorin Nigeria, NATHADEX publishers, 2004.
16. Onwasigwe C. Principles and methods of epidemiology, Enugu Nigeria,
Institute for Development Studies UNEC, 2004.

- 49 -
QUESTIONNAIRE ON SOCIOECONOMIC AND GEOGRAPHICAL
DIFFERENTIALS IN THE UTILISATION OF IMMUNISATION SERVICES
IN ANAMBRA STATE
This is an academic research project by Dr Njelita Chukwudi, an MPH student of
University of Nigeria, Enugu Campus.
Questionnaire No: ---------------------------
Date: ---------------------------
Name of interviewer: ---------------------------
LGA: ---------------------------
This questionnaire is intended to obtain information on the socio-economic and
geographical differentials in the utilisation of immunisation services in Anambra state.
Your responses to the questions will be treated as confidential. Thank you for your
co-operation.
BIODATA
1. Sex: 1) Male……….. 2) Female………….
2. How old are you? …………
3. What is your level of education?
1) No formal education………….
2) Primary School ……………….
3) Secondary Attempted…………
4) Secondary Completed…………
5) Tertiary Attempted ……………
6) Tertiary Completed …………...
4. What is your marital status?
1) Single ………………

- 50 -
2) Married …………….
3) Divorced ……………
4) Widow ……………...
5. Do you think every child really needs immunisation?
(1) YES ……. (2) NO ………
6. Has your child missed any immunisation so far?
(1) Yes…..… (2) No ………
7. Do you think a child’s immunisation appointment should be missed due to any of
these?
1) fever
2) diarrhoea
3) yellow eyes
8. What is your occupation?
1) Farmer…………
2) Trader …………
3) Public/Civil Servant ………
4) Others, please specify …….
9. What is your husband’s occupation?
1) Farmer…………
2) Trader …………
3) Public/Civil Servant ………
4) Others, please specify …….

- 51 -
10. What factors deter you from taking your child to the immunisation centre?
1) long distance
2) Bad road
3) Husband’s decision
4) Religious belief
5) Lack of information
6) Others, please specify ………………………..
11. How much money do you spend for immunisation
in one visit.
1) Less than 200
2) Between 200 and 500
3) above 500
12. What problems discourage you from going back to an
immunization centre after your previous visit to the place.
1) Immunisation charges
2) Health workers’ attitude
3) Unavailability of vaccines
4) Long waiting time at the health facilities.
5) Long distance
6) Others, please specify ………………………..