EFFECTS OF INTRAVENOUS DIPHOSPHONATES ON RENAL FUNCTION
1
1328 that the tissue distribution in rats given Al together with PTH was similar to that of patients with dialysis dementia. It may be that in this patient the repeatedly increased PTH levels caused a marked increase in Al absorption from the gut which produced a significant body burden and toxicity. I thank Dr C. R. Morris, Department of Pediatrics, University of North Carolina, School of Medicine, and Dr John Savory, Department of Pathology, University of Virginia Medical Center, for their valuable contributions. Department of Pathology, University of Virginia Medical Center, Charlottesville, Virginia, USA MARCUS E. RANDALL EFFECTS OF INTRAVENOUS DIPHOSPHONATES ON RENAL FUNCTION SiR,—Dr Bounameaux and colleagues (Feb 26, p 471) suggest that the use of intravenous diphosphonates for the treatment of hypercalcaemia may cause renal impairment. The nephrotoxicity of agents in patients with progressive renal impairment is difficult to assess; nonetheless the evidence for a causal relation between intravenous diphosphonate and renal impairment in case 1 seems convincing. The bolus injection of. large doses of intravenous diphosphonates induces structural renal abnormalities in dogs.2 2 These effects may be due to the high concentrations of diphosphonate achieved in the circulation, resulting in the formation of complexes with cations and of diphosphonate aggregates. Adverse effects can be avoided when the same dose is given by infusion, according to the manufacturers (Proctor and Gamble). We prefer smaller doses of diphosphonate (up to 300 mg daily), given by intravenous infusion over 2-3 h in the treatment of hypercalcaemia and for the rapid control of Paget’s disease. In our experience the hypocalcaemic response probably reaches a peak at this dose and is not likely to be augmented by higher doses. We have not observed progressive renal impairment in more than 40 patients treated with disodium etidronate (EHDP) or disodium clodronate (Cl2MDP) up to a total dose of 14’ 5 g. In patients with normal renal function (figure) EHDP appears to be associated with a rise in mean plasma creatinine which was reversed when infusions were 1. Naik RB, Cundy T, Robinson BHB, Russell RGG, Kanis JA. Effects of vitamin D metabolites and analogues on renal function. Nephron 1981; 28: 17-25. 2. Hintze KL, D’Amato RA. Comparative toxicity of two diphosphonates. Toxicologist 1982; 2: 192. discontinued. The changes were not significant, but the trend W2; also associated with a similar trend in creatinine clearance suggesting an effect on the kidney rather than on creatinine production. Other investigators have used intravenous EHDP in patients with hypercalcaemia due to malignancy with moderate renal impairment’ and not observed renal toxicity. In thirteen patients given infusions of EHDP (7 - 5 mg/kg daily for 1-3 days) mean plasma creatinine fell from 275 to 240 mol/1 over 10 days.3 In common with our experience, seven of these patients showed a small and transient use in serum creatinine. We saw no effect ofC12MDP on plasma creatinine but transient proteinuria was noted in three patients immediately after each intravenous infusion. In nine patients with impaired renal function due to myeloma (mean serum creatinine 252±SEM 36 pmol/1) we have not observed any deleterious effects of Cl2MDP on renal function. We have not given intravenous EHDP to patients with significantly impaired renal function. We have found that intravenous diphosphonates reverse hypercalcaemia where this is due to increased bone resorption C12MDP is particularly well tolerated and appears to be free from adverse effects, including the impairment of bone mineralisation seen with high doses of EHDP. These drugs therefore offer several advantages over many other specific agents available for treatment of increased bone resorption or hypercalcaemia, such as mithramycin, calcitonins, corticosteroids, or those agents (eg, sodium phosphate or sulphate) which chelate calcium within the extracellular fluid compartment. Department of Human Metabolism and Clinical Biochemistry, Sheffield University Medical School, Sheffield S10 2RX J. A. KANIS C. J. PRESTON A. J. P. YATES R. C. PERCIVAL K. I. MUNDY R. G. G. RUSSELL SUBSTANCE P: A NEUROPEPTIDE INVOLVED IN LOW BACK PAIN? SIR,-The key nerve connection mediating low back pain is the sinovertebral nerve, which arises just distal to the spinal ganglion, joins a sympathetic branch, and passes into the spinal canal, where it splits into terminal branches. The posterior longitudinal ligament contains many nerve terminals, while few are found in the 3. Martodam RR, Taylor JT, Davis TE, Golomb HM. The effects of intravenous Didronel on hypercalcaemia of malignant origin Calcif Tissue Int 1983, 35; A36 p< 0 001 Effects of intravenous EHDP or C12MDP on serum calcium and creatinine. Before (A), at end of 3-7 days of treatment (B), and 1 week (C) and 1 month (D) after stopping treatment. All patients had normal renal function as judged b) ser’ creatinine, and patients are divided into those with hypercalcaemia due to increased bone resorption and normocalcaemic patients (Paget’s disease and PrOSIL-1, carcinoma). Results as mean ±SEM.
Transcript of EFFECTS OF INTRAVENOUS DIPHOSPHONATES ON RENAL FUNCTION

1328
that the tissue distribution in rats given Al together with PTH wassimilar to that of patients with dialysis dementia. It may be that inthis patient the repeatedly increased PTH levels caused a markedincrease in Al absorption from the gut which produced a significantbody burden and toxicity.
I thank Dr C. R. Morris, Department of Pediatrics, University of NorthCarolina, School of Medicine, and Dr John Savory, Department of Pathology,University of Virginia Medical Center, for their valuable contributions.
Department of Pathology,University of Virginia Medical Center,Charlottesville, Virginia, USA MARCUS E. RANDALL
EFFECTS OF INTRAVENOUS DIPHOSPHONATES ONRENAL FUNCTION
SiR,—Dr Bounameaux and colleagues (Feb 26, p 471) suggest thatthe use of intravenous diphosphonates for the treatment of
hypercalcaemia may cause renal impairment. The nephrotoxicity ofagents in patients with progressive renal impairment is difficult toassess; nonetheless the evidence for a causal relation betweenintravenous diphosphonate and renal impairment in case 1 seems
convincing. The bolus injection of. large doses of intravenousdiphosphonates induces structural renal abnormalities in dogs.2 2These effects may be due to the high concentrations of
diphosphonate achieved in the circulation, resulting in theformation of complexes with cations and of diphosphonateaggregates. Adverse effects can be avoided when the same dose is
given by infusion, according to the manufacturers (Proctor andGamble).We prefer smaller doses of diphosphonate (up to 300 mg daily),
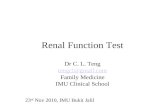
given by intravenous infusion over 2-3 h in the treatment ofhypercalcaemia and for the rapid control of Paget’s disease. In ourexperience the hypocalcaemic response probably reaches a peak atthis dose and is not likely to be augmented by higher doses. We havenot observed progressive renal impairment in more than 40 patientstreated with disodium etidronate (EHDP) or disodium clodronate(Cl2MDP) up to a total dose of 14’ 5 g. In patients with normal renalfunction (figure) EHDP appears to be associated with a rise in meanplasma creatinine which was reversed when infusions were
1. Naik RB, Cundy T, Robinson BHB, Russell RGG, Kanis JA. Effects of vitamin Dmetabolites and analogues on renal function. Nephron 1981; 28: 17-25.
2. Hintze KL, D’Amato RA. Comparative toxicity of two diphosphonates. Toxicologist1982; 2: 192.
discontinued. The changes were not significant, but the trend W2;also associated with a similar trend in creatinine clearance
suggesting an effect on the kidney rather than on creatinine
production.Other investigators have used intravenous EHDP in patients with
hypercalcaemia due to malignancy with moderate renal impairment’and not observed renal toxicity. In thirteen patients given infusionsof EHDP (7 - 5 mg/kg daily for 1-3 days) mean plasma creatinine fellfrom 275 to 240 mol/1 over 10 days.3 In common with ourexperience, seven of these patients showed a small and transient usein serum creatinine.We saw no effect ofC12MDP on plasma creatinine but transient
proteinuria was noted in three patients immediately after eachintravenous infusion. In nine patients with impaired renal functiondue to myeloma (mean serum creatinine 252±SEM 36 pmol/1) wehave not observed any deleterious effects of Cl2MDP on renalfunction. We have not given intravenous EHDP to patients withsignificantly impaired renal function.We have found that intravenous diphosphonates reverse
hypercalcaemia where this is due to increased bone resorptionC12MDP is particularly well tolerated and appears to be free fromadverse effects, including the impairment of bone mineralisationseen with high doses of EHDP. These drugs therefore offer severaladvantages over many other specific agents available for treatmentof increased bone resorption or hypercalcaemia, such as
mithramycin, calcitonins, corticosteroids, or those agents (eg,sodium phosphate or sulphate) which chelate calcium within theextracellular fluid compartment.
Department of Human Metabolismand Clinical Biochemistry,
Sheffield University Medical School,Sheffield S10 2RX
J. A. KANISC. J. PRESTONA. J. P. YATESR. C. PERCIVALK. I. MUNDYR. G. G. RUSSELL
SUBSTANCE P: A NEUROPEPTIDE INVOLVED IN LOWBACK PAIN?
SIR,-The key nerve connection mediating low back pain is thesinovertebral nerve, which arises just distal to the spinal ganglion,joins a sympathetic branch, and passes into the spinal canal, where itsplits into terminal branches. The posterior longitudinal ligamentcontains many nerve terminals, while few are found in the
3. Martodam RR, Taylor JT, Davis TE, Golomb HM. The effects of intravenousDidronel on hypercalcaemia of malignant origin Calcif Tissue Int 1983, 35; A36
*** p< 0 001
Effects of intravenous EHDP or C12MDP on serum calcium and creatinine.
Before (A), at end of 3-7 days of treatment (B), and 1 week (C) and 1 month (D) after stopping treatment. All patients had normal renal function as judged b) ser’creatinine, and patients are divided into those with hypercalcaemia due to increased bone resorption and normocalcaemic patients (Paget’s disease and PrOSIL-1,carcinoma). Results as mean ±SEM.