Prevalence of Elevated Blood Pressure and BMI in US Children and Adolescents OCONNOR
Upload
cardiacinfoCategory
view
657download
1description

Effects of BMI and bariatric surgery on the prevalence of osteoporosis at various body sites
Malcolm Reid Jr.
Briarcliff High School

Abstract: Body mass index (BMI) and bariatric surgery have repeatedly been found to
affect one’s risk of developing osteoporosis. This project studies the correlation between
BMI and osteoporosis as well as the correlation between weight loss from Roux-en-Y
gastric bypass (RYGB) surgery and decrease in bone mineral density (BMD). BMI was
gathered from 77 subjects who were admitted between 2006 and 2008 to St. Luke’s-
Roosevelt Hospital with a hip or spine fracture and were diagnosed with osteoporosis.
The median BMI of osteoporosis patients with spinal compression fractures fell in the
normal range. The greatest number of osteoporosis patients was in the normal range for
BMI, followed by the overweight, obese, and underweight. The results likely reflect the
shift in the United States population toward obesity. Part II of the project investigates the
adverse effects of RYGB, an increasingly common surgical treatment for obesity, on
bone metabolism. The BMDs of 7 obese subjects were measured by dual-energy X-ray
absorptiometry one month before and one year after the surgical procedure. BMD was
tested at the femoral neck, upper femoral neck, shaft, and total femur. There was a
significant decrease only at the femoral neck. Other studies have found a similar
decrease.
2

1. Introduction
1.1. Review of Literature
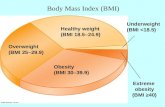
Obesity, defined as body mass index (BMI) of 30 kg/m2 or greater, is an
increasingly prevalent disease that has profound effects on the morbidity and mortality
of those who have it, increasing the risk of cardiovascular disease, type 2 diabetes
mellitus, hypertension, stroke, dyslipidemia, osteoarthritis, and certain cancers (1).
Overweight is the medical condition defined as a body mass index between 25 and 29.9
kg/m2. One study found the prevalence of these two diseases to be greater than 64% in
the United States adult population. This same study estimated that obesity has
increased more than 25% in the last thirty years and it continues to increase at an even
steeper incline (2).
There are various treatments for obesity and overweight, some proving more
effective than others. Treatments can be grouped into three categories: lifestyle
changes, pharmaceuticals, and surgery. Lifestyle changes are modifications in diet and
incorporation of exercise into one’s daily routine. The current pharmacological
treatments are either appetite suppressants or lipase inhibitors, but all have adverse
side effects and none is as effective as surgery (3). Bariatric surgery alters the anatomy
of a person’s digestive system to cause weight loss. It is an especially common
treatment for morbid obesity, defined as a BMI of 40 kg/m2 or higher. The surgeries are
either malabsorptive, restrictive, or a combination of the two. The participants in this
study have undergone either roux-en-y gastric bypass (RYGB) or lap-band adjustable
gastric banding (LAGB) with the majority having undergone the former. RYGB is mainly
malabsorptive, but has a restrictive component. In this procedure the duodenum, the
3

first part of the small intestine, is bypassed. The duodenum is the primary site of calorie
absorption. In addition, in RYGB the size of the stomach is reduced by the creation of a
small pouch and a route for digesting food that bypasses the rest of the stomach. Unlike
RYGB, LAGB is solely a restrictive procedure, resulting in it being less effective in
causing and maintaining weight loss that RYGB (4). In LAGB the surgeon ties an
inflatable band around the stomach to separate it into two pouches connected by a
small channel. This channel can be adjusted and is designed to remain for the rest of
the person’s life.
Bariatric surgery has negative effects on bone metabolism. A proposed cause of
these effects, specifically in gastric bypass and other malabsorptive surgeries, is that
calcium is primarily absorbed in the duodenum, while vitamin D is primarily absorbed in
the jejunum and ileum, the second and third parts of the small intestine (5). Several
studies have found that obese population has low vitamin D concentrations to begin
with (6-10). Ybarra et al. found in their study of 80 obese patients who did not undergo
bariatric surgery and 64 who did 36 months earlier that hypovitaminosis D and
secondary hyperparathyroidism were overwhelmingly common (80% of the patients in
the study) in the obese population prior to bariatric surgery and remained unchanged
following RYGB (11). Multiple other studies have found that calcium, parathyroid
hormone (PTH), and vitamin D concentrations generally remain the same after bariatric
surgery (12-15). However, other studies debate this claim, suggesting that RYGB
results in calcium and vitamin D deficiencies as well as elevations in PTH levels (16,
17). Little literature exists on the effects of LAGB on bone metabolism. One study by
Giusti found that LAGB, like RYGB, negatively affects bone metabolism by increasing
4

bone resorption resulting in a decrease in bone mineral content and BMD at the femoral
neck (18).
Although it is unclear whether vitamin D, calcium, and PTH levels change as a
result of bariatric surgery, it is clear that bariatric surgery affects BMD and bone mass.
Obesity has been shown to correlate with higher bone mass, thus it is considered a
“protective factor for osteoporosis (12). Osteoporosis, a disease that continuously
increases in prevalence, is defined as the increased porosity of bone. On a cellular
level, osteoporosis is caused by two different cells: osteoclasts and osteoblasts.
Osteoclasts are mononucleate cells that destroy and absorb part of the bone matrix.
Conversely, osteoblasts are mononucleate cells that rebuild the bone matrix.
Collectively, the process of bone resorption, done by osteoclasts, and bone formation,
done by osteoblasts, is called bone remodeling. About 10% of the body’s bone is
remodeled annually, with the most remodeling taking place in the trabecular bone.
Therefore, the sites with the greatest amounts of trabecular bone (the spine, the wrist,
and the hip) are the most common locations of osteoporotic fracture (19). Normally
human children’s osteoblasts deposit more bone matrix than their osteoclasts destroy.
Thus, the bone matrix gradually increases. When adulthood is reached, not only does
this process usually even out, but also it often tends to reverse. In other words, bone
resorption tends to destroy more bone than the amount of bone that is added by bone
formation. At mild levels, this imbalance is osteopenia, but at greater levels, this
imbalance is osteoporosis. The World health Organization has guidelines which are
virtually universally adhered to as markers of osteoporosis. T-score is a measure of how
one’s BMD compares to the BMDs of young adults of the same sex. A T-score of -2.5 or
5

lower is the definition of osteoporosis. A T-score of -1 to -2.5 is the definition of
osteopenia. A T-score of greater than -1 is in the normal range (20).
The reductions of significant amounts of body fat, as suspected, causes a
decrease in bone mass and BMD. The study of Duran de Campos et al. reported that
the aforementioned effects of bariatric surgery on bone metabolism likely take place
before 8 years after the surgery because of the prevalence of osteoporosis and
osteopenia despite the constancy of bone markers showing resorption (17). By
calculating bone mineral apparent density (BMaD), J. Fleischer et al. found that this loss
of body fat caused most of the BMD decrease (16). However, this study and others
have found a significant increase in bone remodeling as shown by biochemical markers
(12, 13, 16, 17).
It is unclear at which sites BMD decreases. Coates et al. found that BMD
decreased at the hip, the trochanter, the spine, and the total body from 3 to 9 months
after LRGB (21). Carrasco’s findings at two six-month intervals after RYGB support this
finding (22). Fleischer et al failed to find any decrease in BMD at the spine for 3, 6, and
12 months after RYGB (16). Pereira et al. found a decrease in BMD for one year after
RYGB at all sites tested: the forearm, the femoral neck, and the lumbar spine (LS) (L1-
L4) (11). Mahdy found a significant decrease in BMD at the total body for one year
following RYGB surgery (14). Johnson reported on 233 patients who underwent gastric
bypass or biliopancreatic diversion, another type of restrictive bariatric surgery, and
found that BMD decreased at the total forearm (TF), the radius bone the total hip, and
the LS after one year and subsequently remained stable. The TF BMD decreased even
more after a second year and subsequently remained stable (15). The findings in this
6

study are especially significant because it is the largest long-term study pertaining to
bariatric surgery’s effects on bone metabolism.
7

2. Methods
2.1 Part I
2.1.1. Study Design
BMI was obtained from the medical record for each subject. In the case that the BMI
was not reported, BMI was calculated using the National Institutes of Health’s BMI
calculator at http://www.nhlbisupport.com/bmi/ with the height and weight of the subject
as noted by the chart, most often by the nutritionist’s note.
2.1.2. Subjects
Medical record information from 77 adults with spinal compression fractures who were
admitted to the research facility from 2006-2008 and diagnosed with osteoporosis was
used for this retrospective chart review. Subjects were excluded if the origin of their
osteoporosis diagnoses was unknown.
2.1.3. Research Question
Is there a significant negative correlation between BMI and osteoporosis as shown by a
random sample of osteoporotic subjects?
2.1.4. Hypotheses
H: Osteoporosis is significantly more prevalent in underweight (BMI<18.5) people than
in overweight (BMI of 25.0 – 29.9) and obese (BMI>30) people. Osteoporosis is
disproportionately more prevalent in underweight people.
H0: Osteoporosis is not significantly more prevalent in the underweight group than the
overweight and obese group. There is an approximately even distribution of
osteoporosis across the different weight groups of the population or osteoporosis is
disproportionately present in obese subjects.
8

2.1.5. Statistical Analysis
Of the 77, the median BMI was calculated to demonstrate whether or not the prevalence
of osteoporosis was significantly greater in one weight group than another (underweight,
normal, overweight, or obese). A tally of the people with osteoporosis in each group was
also taken.
9

2.2. Part II
2.2.1. Study Design
Patients in this study were seen twice: prior to bariatric surgery and after bariatric
surgery. The baseline visit to the hospital took place 15 to 30 days prior to the bariatric
surgery. The follow-up visit to the hospital took place about 1 year after the bariatric
surgery. The first baseline visit was in January of 2008, and the first follow-up visit was
in January of 2009.
2.2.2. Subjects
Seven obese adult female subjects, aged 48.4±10.1 (ranging in age from 34.7 to 66.4)
served as research subjects in this study. The subjects were fully apprised of the
nature of the study and the procedures by the consent form. The physical
characteristics of the subjects at the start of the study are displayed in Table 1. All of
the subjects underwent RYGB at Cornell University Hospital in New York City, starting
in January of 2008. 4 subjects were excluded from taking part in this study: 2 exceeded
the table’s weight limitation (300 pounds); 2 exceeded the table’s width limitation (60
inches). DXA’s weight and width limitations have limited research on obese subjects,
causing manufacturers to make stronger and wider tables.
Age (years) 48.4±10.1
Height (in.) 64.2±3.3
Weight (lb.)
257.9±33.
9
BMI (kg/m2) 43.8±3.1
Fat mass (kg) 81.6±43.8
10
Figure 1: Physical Characteristics of Subjects Prior to Bariatric Surgery (Reported as mean ± standard deviation)

Fat (%) 56.3±6.0
2.2.3. Research Questions
Does BMD decrease at all sites of the hip (upper neck, neck, shaft, and total femur)
when measured with iDXA after a patient has undergone RYGB?
Does BMaD fully account for all changes in BMD?
2.2.4. Hypotheses
H: BMD decreases significantly (P<0.05) at the upper neck, neck, shaft, and total femur
when measured by iDXA after the subject has undergone RYGB.
H0: BMD does not decrease at all four of these sites when measured by iDXA after the
subject has undergone RYGB. P>0.05 for at least one of the sites or at least one of the
sites does not have any decrease in BMD.
H: BMaD does not fully account for all changes in BMD. When BMaD is calculated, it
will still be lower than the subject’s BMD prior to the bariatric surgery.
H0: BMaD fully accounts for all changes in BMD. When BMaD is calculated, it will be
the same as or higher than the subject’s BMD prior to the bariatric surgery.
2.2.5. DXA Procedure
BMD was measured at the neck, upper neck, shaft, and total femur at each visit. Seven
patients’ BMDs were measured using an iDXA absorptiometer (LUNAR DXA-IQ DXA,
Madison, WI, USA) and one patient’s BMD was measured using a Hologic
absorptiometer (HOLOGIC MODEL DELPHI W; HOLOGIC, WALTHAM, MA). Patients
were positioned on the table and the scans were executed with the straps and plastic
trapezoid provided with the scanner. All of a patient’s scans were performed one after
11

another, with the only time in between the scans being used to adjust the patient and
scanner.
2.2.6. BMaD Calculation
The following formula was used for the calculations: BMaD = BMC/bone area1.5. BMC is
an abbreviation for bone mineral content, the measure of the mass of one’s bone. DXA
produces BMC readings based on the measured attenuation of the X-rays.
2.2.7. Statistical Analysis
All statistical analyses were performed using Statistical Package for Social Sciences
(SPSS/Windows version 12, SPSS, Chicago, IL, USA). Descriptive statistics are
presented as mean ± standard deviation except where otherwise stated. A two-tailed P
value ≤ 0.05 was considered statistically significant. Spearman’s rank correlation
coefficients were used to assess the strength of the association between decrease in
weight and change in bone mineral density.
12

3. Results
3.1 Part I
Underweight: 10/77
Normal: 32/77
Overweight: 21/77
Obese: 14/77
Median BMI: 24.6 kg/m2
13
Figure 2: Bar Graph
Underweight Normal Overweight Obese0
5
10
15
20
25
30
35
Patients with osteoporosis grouped by BMI
BMI Category
Num
ber o
f Ost
eopo
rotic
Pati
ents
(Tot
al =
77)
Figure 2: Bar Graph

3.2 Part II:
NeckUpper Neck Shaft
Total Femur
Baseline BMD (g/cm2)
1.043±0.174
0.862±0.205
1.324±0.161
1.112±0.144
Follow-up BMD (g/cm2)
0.996±0.146
0.806±0.163
1.249±0.163
1.044±0.140
Difference in BMD (g/cm2)
-0.047±0.22
3
-0.056±0.24
7
-0.075±0.21
8
-0.068±0.20
3Baseline BMaD (g/cm3)
0.473±0.101
Follow-up BMaD (g/cm3)
0.462±0.101
Difference in BMaD (g/cm3)
-0.011±0.02
9
Age (years) 49.8±10.1Weight (lb.) 188.2±40.9BMI (kg/m2) 31.8±6.3Fat mass (kg) 37.2±16.4Fat (%) 41.4±9.2
14
Figure 3: Physical Characteristics of Subjects 1 Year After Bariatric Surgery

4. Discussion
It is well-established that osteoporosis is more common in underweight people
than overweight people. The findings in Part I do not contradict this, but they do show
that osteoporosis is found in people of all different BMIs. The lowest BMI was 14.9,
which is markedly underweight. The highest BMI was 59.8, which is morbidly obese. A
possible explanation for the median BMI being in the normal range is that as the United
States population moves toward obesity, osteoporosis is increasing in prevalence in
normal and overweight people.
Part II examined bariatric surgery, which has drastically increased in prevalence
in the United States and found that it causes a significant decrease in BMD. Several
studies have reached the same conclusion (11, 14, 15, 16, 21, 22). BMaD has only
once been used for a similar study. That study, unlike this one, found that BMaD
accounted for the BMD loss in its entirety (16). The significant decrease in BMD, which
was found only at the neck lacks much support in the literature because most articles in
the field group all of the sites that this study tested as the femoral neck and do not
further test the smaller sites of the hip.
This study has some weaknesses. The bariatric surgery sample size is small, but
not extraordinarily small when compared to the standard sample size in similar studies.
Many similar studies that observe the effect of bariatric surgery on BMD have fewer
than 50 subjects (5-7, 9, 11, 12). In the future more subjects should be used in these
15

studies. Another weakness of this study is that it does not take note of the nutrition and
supplements, if any, of the subjects. Supplemental Vitamin D and Calcium would likely
reduce the decrease in BMD of patients who intake it. If subjects in this study were
taking these supplements, the results of this study may be stronger than actual,
showing a greater decrease in BMD at all sites. Most likely, however, there would still
be a disproportionate decrease at the femoral neck as compared to the other sites. A
final weakness of this study is that the spine BMD was not measured in the bariatric
surgery subjects. As previously noted, some studies have found a significant decrease
in BMD at the spine in subjects who have undergone RYGB. Also, the spine BMD is
important for the most accurate assessment of BMaD because each spine vertebra is
more cubical than any part of the hip.
The research in this study has many implications in both the global and the
medical communities. The observance of osteoporosis in greater numbers of individuals
with higher BMDs means that more people should be tested for the disease. As a “silent
disease,” osteoporosis is often diagnosed too late, only after at least one fracture has
already taken place. The results of this study suggest that osteoporosis may be even
more underdiagnosed than is estimated. Also, this research demonstrates a possible
complication of RYGB. Persons who undergo this procedure should supplement their
diets with calcium and Vitamin D, as doing so has been shown to reduce the decrease
in BMD in some studies (5, 6, 8, 11, 15).
This study calls for some changes in traditional clinical practice. Physicians,
especially orthopedists, are arguably the most able persons to combat the
underdiagnosis of osteoporosis. The only way they can do this is by recommending that
16

more of their patients receive DXA scans. As shown by this study, persons of various
sizes can have osteoporosis. Physicians should also take on the task of informing
prospective bariatric surgery patients of the risk of bone loss. Members of the medical
community need to help the patients fight this bone loss by supplementing their diets
with adequate amounts of calcium and Vitamin D before and after the surgery.
Part II of this research project is ongoing and will ultimately finish in June of 2010
with a total of 35 subjects. Those additional patients will likely support the finding in this
study. Further research is needed in many aspects of the field. To better understand
bone loss after weight loss, there must be research in three areas: longer time period,
larger weight loss, and the relation between BMD, BMD, and bone area. Once this
research is done, the medical community will be much closer to knowing how to stop or
reduce bone loss after significant weight loss, such as bariatric surgery. Further
research should also be done on how other, less common types of bariatric surgery
affect bone loss.
5. Conclusion
5.1. Part I
The median BMI of 4.6 kg/m2 falls in the normal range. The smallest number of patients
diagnosed with osteoporosis was the underweight group.
5.2. Part II
The bariatric surgery was successful with a mean weight loss of 69 pounds. BMD
decreased significantly at the neck after bariatric surgery, but insignificantly at the other
sites tested: the upper neck, the shaft, and the total femur. A decrease in volumetric
17

bone density, as measured by BMaD, suggests that this decrease in BMD is not solely
a result of the significant weight loss.
6. References
(1) World Health Organization. (2000). Obesity: preventing and managing the global epidemic. World Health Organization Techincal Report Series, 894, 6-8.
(2) Flegal, K., Carroll, M., Kuczmarski, R., & Johnson, C. (1998). Overweight and obesity in the United States: prevalence and trends, 1960-1994 . International Journal of Obesity Related Metabolic Disorders, 22(1), 39-47.
(3) Snow, V., Barry, P., Fitterman, N., Qaseem, A., & Weiss, K. (2005).
Pharmacologic and surgical management of obesity in primary care: a clinical practice guideline from the American College of Physicians.. Ann Intern Med, 142(7), 525-531.
(4) Chapin BL, LeMar HJ, Knodel DH et al. Secondary hyperparathyroidism following biliopancreatic diversion. Arch Surg 1996; 113:1048-1052
(5) Davies, D., Baxter, J., & Baxter, J. (2007). Nutritional deficiencies after bariatric surgery. Obesity Surgery, 17(9), 1150-1158.
(6) Bell, N., Epstein, S., Green, A., Shary, J., Oexmann, M., & Shaw, S. (1985). Evidence for alteration of the vitamin D-endocrine system in obese subjects. Journal of Clinical Investigation, 76, 370-373.
(7) Liel, Y., Ulmer, E., Shary, J., Hollis, B. W., & Bell, N. H. (1988). Low circulating vitamin D in obesity. Calcified Tissue International, 43(4), 199-201.
(8) Wortsman, J., Matsuoka, L. Y., Chen, T. C., Lu, Z., & Holick, M. F. (2000). Decreased bioavailability of vitamin D in obesity. American Journal of Clinical Nutrition, 72(3), 690-693.
(9) Buffington, C., Walker, B., Cowan Jr., G. S., & Scruggs, D. (1993). Vitamin D deficiency in the morbidly obese. Obesity Surgery, 3(4), 421-424.
(10) Holick, M. F. (2000). Calcium and vitamin D. Diagnostics and therapeutics. Clinics in Laboratory Medicine, 20(3), 569-590.
18

(11) Ybarra, J., Sanchez-Hernandez, J., Gich, I., Leiva, A. D., Rius, X., Espinosa, J., & Perez, A. (2005). Unchanged Hypovitaminosis D and Secondary Hyperparathyroidism in Morbid Obesity after Bariatric Surgery. Obesity Surgery, 15(3), 330-335.
(12) Pereira, F., Castro, J. d., Santos, J. d., Foss, M., & Paula, F. (2007). Impact of marked weight loss induced by bariatric surgery on bone mineral density and remodeling. Brazilian Journal of Medical and Biological Research, 40(4), 509-517.
(13) Bano, G., Rodin, D., Pazianas, M., & Nussey, S. (1999). Reduced bone mineral density after surgical treatment for obesity. International Journal of Obesity Related Metabolic Disorders, 23(4), 361-365.
(14) Mahdy, T., Atia, S., Farid, M., & Adulatif, A. (2008). Effect of Roux-en Y Gastric Bypass on Bone Metabolism in Patients with Morbid Obesity: Mansoura Experiences. Obesity Surgery, 18(12), 1526-1531.
(15) Johnson, J., Maher, J., Samuel, I., Heitshusen, D., Doherty, C., & Downs, R. (2005). Effects of gastric bypass procedures on bone mineral density, calcium, parathyroid hormone, and vitamin d. Journal of Gastrointestinal Surgery, 9(8), 1106-1111.
(16) Fleischer, J., Stein, E., Bessler, M., Badia, M. D., Restuccia, N., Olivero-Rivera, L., McMahon, D., & Silverberg, S. (2008). The decline in hip bone density after gastric bypass surgery is associated with extent of weight loss. The Journal of Clinical Endocrinology & Metabolism, 93(10), 3735-3740.
(17) de Campos, C. D., Dalcanale, L., Pajecki, D., Jr, A. G., & Halpern, A.
(2008). Calcium Intake and Metabolic Bone Disease after Eight Years of Roux-en-Y Gastric Bypass. Obesity Surgery, 18(4), 386-390.
(18) Giusti, V., Gasteyger, C., Suter, M., Heraief, E., Gaillard, R., & Burckhardt, P. (2005). Gastric banding induces negative bone remodeling in the absence of secondary hyperparathyroidism: potential role of serum C telopeptides for follow-up. International Journal of Obesity, 29, 1429-1435.
(19) Cummings, S., & Melton, L. (2002). Epidemiology and outcomes of osteoporotic fractures. The Lancet, 359(9319), 1761-1767.
(20) Kanis, J., & Kanis, J. (1994). Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: Synopsis of a WHO report. Osteoporosis International, 4(6), 368-381.
19

(21) Coates, P., Fernstrom, J., Fernstrom, M., Schauer, P., & Greenspan, S. (2004). Gastric bypass surgery for morbid obesity leads to an increase in bone turnover and a decrease in bone mass. The Journal of Clinical Endocrinology & Metabolism, 89(3), 1061-1065.
(22) Carrasco, F., Papapietro, K., Csendes, A., Salazar, G., Echenique, C., Lisboa, C., Díaz, E., & Rojas, J. (2007). Changes in resting energy expenditure and body composition after weight loss following Roux-en-Y gastric bypass. Obesity Surgery, 17(5), 608-616.
20