
Effects Five Per Cent Dextrose-Water Infusions ...circ.ahajournals.org/content/37/5/832.full.pdf ·...
16
Effects of Five Per Cent Dextrose-Water Infusions in Normal and Hypertensive Man Evidence for Increased Proximal and Distal Tubular Sodium Rejection by Hypertensive Patients and Its Relation to Renal Hemodynamics By PAUL J. CANNON, M.D. SUMMARY During infusions of 5% dextrose in water urinary sodium excretion and the renal tubular rejection of filtered sodium (E/F Na %) were significantly higher in hyperten- sive than in normotensive subjects. Increased E/F Na % did not result from alterations in plasma sodium, in filtered sodium, or from an osmotic diuresis. Fractional sodium reabsorption in proximal (isosmotic) portions of the nephron was diminished in the hypertensive patients. Free water forrnation (CH20) rose with in- creased "distal" sodium delivery (V) in both groups; however, fractional sodium reabsorption in the "distal" nephron was significantly impaired in the hypertensive patients and urinary osmolality was increased. Mean arterial blood pressure and E/F Na % were related in curvilinear fashion in the 31 studies, and there was a direct relation between E/F Na % and the mag- nitude of renal vascular resistance. The data suggested that alterations of renal arterial pressure and vascular resistance in hypertensive disease modify sodium transport in proximal and diluting segments of the nephron and determine to a major extent the increased natriuresis exhibited by hypertensive subjects during in- fusions that expand extracellular fluid volume. Additional Indexing Words: Sodium excretion Extracellular fluid volume expansion Natriuresis Hypertension FACTORS that influence the rate of renal tubular sodium reabsorption under nor- mal circumstances have not been completely clarified. Studies from many laboratories have indicated that the diminished renal tubular sodium reabsorption developing in response to infusions of saline or Ringer's solution in normal animals does not result from changes From the Department of Medicine, College of Physicians and Surgeons, Columbia University and the Presbyterian Hospital, New York, New York. Supported by U.S. Public Health Service Grants HE 10182 and HE 05741. Dr. Cannon is a recipient of U.S. Public Health Service Career Development Award HE 15032 of the National Heart Institute. 832 in glomerular filtration rate, the filtered load of sodium, or aldosterone secretion.1 6 To explain this phenomenon of "saline diuresis" attention has recently been directed toward the presence of a "third factor,"7 which may either be a "natriuretic" hormonel 8410 or an intrarenal hemodynamic adjustment to extra- cellular fluid (ECF) volume expansion5 11,12 or a combination of both.13 Patients with arterial hypertension exhibit an exaggerated natriuresis in response to in- fusions of saline or mannitol.14-27 The mech- anism limiting tubular sodium reabsorption in hypertensive more than in normal subjects during the infusions remains unexplained. It is probably a functional abnorrnality rather Circulation, Volume XXXVII, May 1968 by guest on July 22, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript of Effects Five Per Cent Dextrose-Water Infusions ...circ.ahajournals.org/content/37/5/832.full.pdf ·...

Effects of Five Per Cent Dextrose-WaterInfusions in Normal and Hypertensive Man
Evidence for Increased Proximal and Distal TubularSodium Rejection by Hypertensive Patientsand Its Relation to Renal Hemodynamics
By PAUL J. CANNON, M.D.
SUMMARYDuring infusions of 5% dextrose in water urinary sodium excretion and the renal
tubular rejection of filtered sodium (E/F Na %) were significantly higher in hyperten-sive than in normotensive subjects. Increased E/F Na % did not result from alterationsin plasma sodium, in filtered sodium, or from an osmotic diuresis.
Fractional sodium reabsorption in proximal (isosmotic) portions of the nephron wasdiminished in the hypertensive patients. Free water forrnation (CH20) rose with in-creased "distal" sodium delivery (V) in both groups; however, fractional sodiumreabsorption in the "distal" nephron was significantly impaired in the hypertensivepatients and urinary osmolality was increased.Mean arterial blood pressure and E/F Na % were related in curvilinear fashion
in the 31 studies, and there was a direct relation between E/F Na % and the mag-nitude of renal vascular resistance. The data suggested that alterations of renalarterial pressure and vascular resistance in hypertensive disease modify sodiumtransport in proximal and diluting segments of the nephron and determine to amajor extent the increased natriuresis exhibited by hypertensive subjects during in-fusions that expand extracellular fluid volume.
Additional Indexing Words:Sodium excretion Extracellular fluid volume expansionNatriuresis
Hypertension
FACTORS that influence the rate of renaltubular sodium reabsorption under nor-
mal circumstances have not been completelyclarified. Studies from many laboratories haveindicated that the diminished renal tubularsodium reabsorption developing in responseto infusions of saline or Ringer's solution innormal animals does not result from changes
From the Department of Medicine, College ofPhysicians and Surgeons, Columbia University andthe Presbyterian Hospital, New York, New York.
Supported by U.S. Public Health Service GrantsHE 10182 and HE 05741.
Dr. Cannon is a recipient of U.S. Public HealthService Career Development Award HE 15032 of theNational Heart Institute.
832
in glomerular filtration rate, the filtered loadof sodium, or aldosterone secretion.1 6 Toexplain this phenomenon of "saline diuresis"attention has recently been directed towardthe presence of a "third factor,"7 which mayeither be a "natriuretic" hormonel 8410 or anintrarenal hemodynamic adjustment to extra-cellular fluid (ECF) volume expansion5 11,12or a combination of both.13
Patients with arterial hypertension exhibitan exaggerated natriuresis in response to in-fusions of saline or mannitol.14-27 The mech-anism limiting tubular sodium reabsorptionin hypertensive more than in normal subjectsduring the infusions remains unexplained. Itis probably a functional abnorrnality rather
Circulation, Volume XXXVII, May 1968
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from
FIVE PER CENT DEXTROSE-WATER INFUSIONS
than the result of structural damage to therenal tubules since (1) increased natriuresisby hypertensive subjects is manifest only dur-ing the infusions of saline or mannitol, and(2) renal salt wasting is not apparent inhypertensive subjects not receiving infusionswhen they are maintained on a normal or lowsodium intake.2' 28The present studies were designed to inves-
tigate hemodynamic factors that might beinvolved in the phenomenon of salt rejectionin normal and hypertensive man during amild degree of expansion of the extracellularfluid volume. To this end renal hemodynamicsand the natriuretic responses of hypertensivepatients were examined during rapid infu-sions of 5% dextrose in water and were com-pared to those of normal and salt-depletedcontrol subjects. The studies confirm observa-tions of Ek29 that an exaggerated natriuresisdoes occur in hypertensive patients in responseto infusion of 5% dextrose and water. In addi-tion they demonstrate (1) that in hypertensivepatients during the infusions, sodium reabsorp-tion is impaired not only in the proximaltubules but also in distal "diluting" segmentsof the nephron, and (2) that the degree ofsodium rejection is correlated with the meanarterial blood pressure and the renal vas-cular resistance.
MethodsThirty-one renal clearance studies were per-
formed in nine normal volunteers and 18 patientswith essential hypertension and one patient withhypertension caused by an aldosterone-secretingadenoma. Each of the hypertensive subjects andsix control subjects prior to study received a dietcontaining 4 to 6 g of sodium; five studies wereperformed after the control subjects had re-ceived a low-sodium diet (less than 0.875 g ofNaCl per day) for 4 to 7 days. None of thepatients received medication other than occa-sional bedtime sedation with barbiturates. Nonehad papilledema or congestive heart failure ora blood area nitrogen level above 26 mg/100 ml.
All experiments were performed at the sameearly morning hour with the subjects fasting,resting quietly in bed. Water diuresis was in-duced by oral administration of 500 ml of waterduring the hour prior to the infusion and wasmaintained by intravenous administration of a5% dextrose solution at a rate of 15 ml/min in
Circulation, Volume XXXVII, May 1968
26 studies and 9 ml/min in nine studies, heldconstant by a motor-driven pump. Urine col-lections were made and discarded until a steadystate of maximal urine flow was achieved. Threeor four 10-minute clearance periods were thenobtained.Venous blood samples were collected at appro-
priate intervals through an indwelling needle.Urine was collected continuously via an in-dwelling catheter. Blood pressure was measuredfrom the arm during the clearance periods by astandard cuff mercury sphygmomanometer.The rates of glomerular filtration (GFR) and
of effective renal plasma flow (ERPF) weremeasured by the administration of inulin or14C-inulin and para-aminohippuric acid (PAH). Ade-quate priming doses were given intravenously;then these substances were added to the 5% dex-trose infusion in amounts to maintain constantplasma concentrations. PAH was added to thesustaining infusion immediately before use toavoid the depression in PAH extraction that canoccur when PAH and dextrose are incubatedtogether for several hours.30 Plasma and urinesamples were analyzed for inulin by the anthronemethod,31 for 14C-inulin by the method of Cot-love,32 and for PAH by the method of Smith.33Sodium and potassium concentrations in plasmaand urine were measured by an InstrumentationAssociates flame photometer. Chloride concentra-tions were measured by potentiometric titrationwith the Cotlove chloridometer. Urine and plasmatotal-solute concentrations were measured with anAdvanced Instruments osmometer.
Calculations: Mean arterial blood pressurewas calculated as the average of systolic anddiastolic pressures in millimeters of mercury.Effective renal blood flow was calculated asthe clearance of PAH divided by 1 - hct andwas expressed in milliliters per minute. Renalvascular resistance was calculated by dividingeffective renal blood flow by the mean arterialblood pressure and was reported in arbitraryresistance units (RU). The glomerular filtrationrate was estimated from the clearance of inulin(CIN) and expressed in milliliters per minute.Osmolar and free water clearances were calcu-lated in the manner described by Smith:33COSm =UOSm V/POSM; CH20= V -UOSm V/Posm,where V is the urine flow in milliliters per minuteand Uosm and Posm are the solute concentrationsof urine and plasma in milliosmoles per kilogramof water. Filtered solute load was calculated asthe osmolality of plasma in micro-osmoles permilligram. H20 X CIN in milliliters per minutewas expressed as micro-osmoles per minute. Thepercentage of the urinary solute concentration dueto salt was calculated by the formula:UNamEq/L + UclmEq/L + UosmmOsnM/kgH20 x 100.
833
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from
CANNON
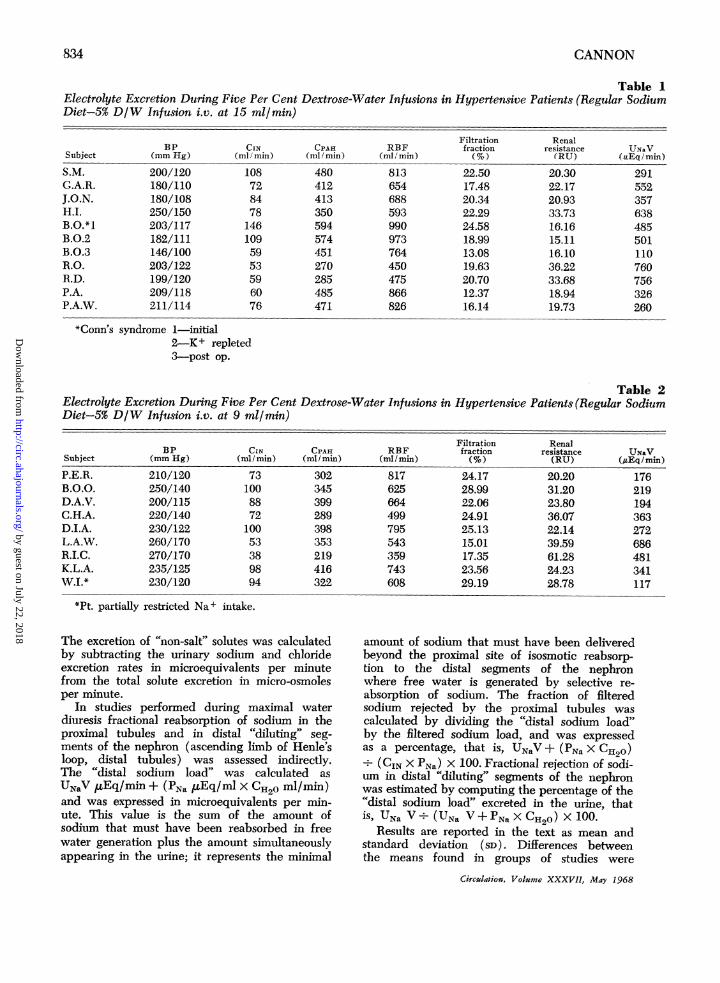
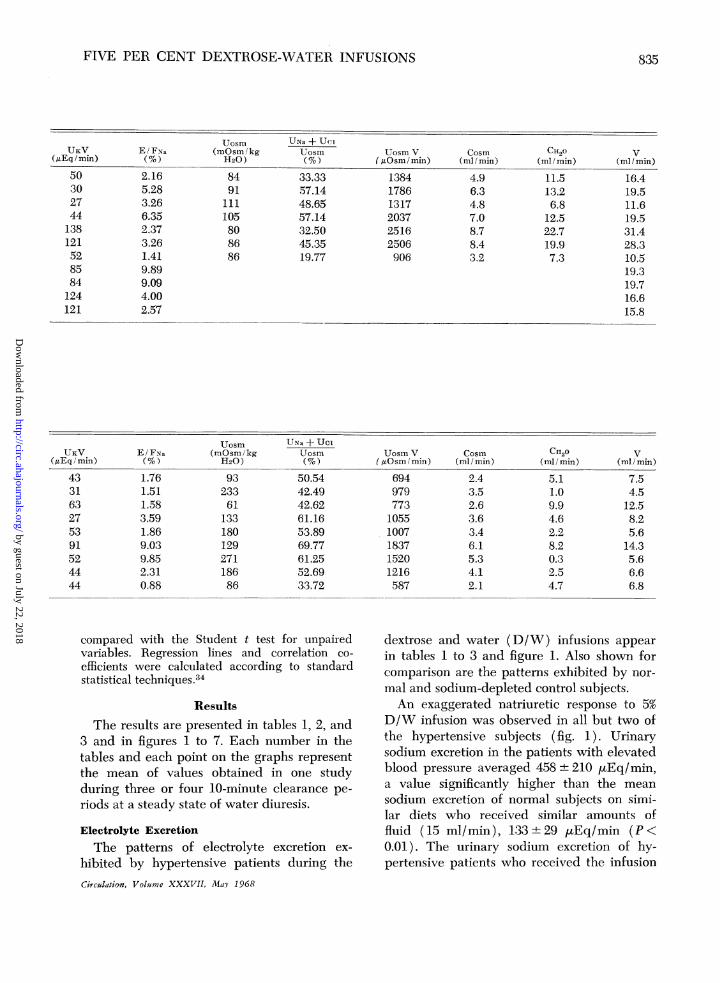
Table 1Electrolyte Excretion During Five Per Cent Dextrose-Water Infusions in Hypertensive Patients (Regular SodmDiet-5% D/W Infusion i.v. at 15 ml/min)BP.
CIN CPAH RBF(ml/min) (ml/min) (mllmin)
1087284781461095953596076
480412413350594574451270285485471
813654688593990973764450475866826
*Conn's syndrome 1-initial2-K + repleted3-post op.
Table 2Electrolyte Excretion During Five Per Cent Dextrose-Water Infusions in Hypertensive Patients (Regular SodiumDiet-5% D/W Infusion i.v. at 9 ml/min)
Filtration RenalBP CIN CPAH RBF fraction resistance UN&V
Subject (mm Hg) (ml min) (ml min) (ml/mmin) (%) (RU) (gEq/min)P.E.R.B.O.O.D.A.V.C.H.A.D.I.A.L.A.W.R.I.C.K.L.A.W.I.*
210/120250/140200/115220/140230/122260/170270/170235/125230/120
73100887210053389894
302345399289398353219416322
817625664499795543359743608
24.1728.9922.0624.9125.1315.0117.3523.5629.19
20.2031.2023.8036.0722.1439.5961.2824.2328.78
176219194363272686481341117
*Pt. partially restricted Na + intake.
The excretion of "non-salt" solutes was calculatedby subtracting the urinary sodium and chlorideexcretion rates in microequivalents per minutefrom the total solute excretion in micro-osmolesper minute.
In studies performed during maximal waterdiuresis fractional reabsorption of sodium in theproximal tubules and in distal "diluting" seg-ments of the nephron (ascending limb of Henle'sloop, distal tubules) was assessed indirectly.The "distal sodium load" was calculated as
UNaV ,Eq/min + (PNa ,uEq/ml X CH20 ml/min)and was expressed in microequivalents per min-ute. This value is the sum of the amount ofsodium that must have been reabsorbed in freewater generation plus the amount simultaneouslyappearing in the urine; it represents the minimal
amount of sodium that must have been deliveredbeyond the proximal site of isosmotic reabsorp-tion to the distal segments of the nephronwhere free water is generated by selective re-absorption of sodium. The fraction of filteredsodium rejected by the proximal tubules wascalculated by dividing the "distal sodium load"by the filtered sodium load, and was expressedas a percentage, that is, UNaV + (PNa X CH2O)*-(CIN X PNa) X 100. Fractional rejection of sodi-tim in distal "diluting" segments of the nephronwas estimated by computing the percentage of the"distal sodium load" excreted in the urine, thatI UNa V (UNa V + PNa X CH20) X 100.
Results are reported in the text as mean andstandard deviation (SD). Differences betweenthe means found in groups of studies were
Circulation, Volume XXXVII, May 1968
Subject
S.M.G.A.R.J.O.N.H.I.
B.O.*1
B.O.2B.O.3R.O.R.D.P.A.P.A.W.
BP(mm Hg)
200/120180/110180/108250/150203/117182/111146/100203/122199/120209/118211/114
Filtrationfraction(%)
22.5017.4820.3422.2924.5818.9913.0819.6320.7012.3716.14
Renalresistance(RU)
20.3022.1720.9333.7316.1615.1116.1036.2233.6818.9419.73
UNaV(uEq 1min)
291552357638485501110760756326260
834
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from
FIVE PER CENT DEXTROSE-WATER INFUSIONS
UKV( uEq min)
50302744138121528584124121
UKVUKV
(uEqImin)433163275391524444
E/FNa(%)
2.165.283.266.352.373.261.419.899.094.002.57
E/FNa(No)
1.761.511.583.591.869.039.852.310.88
Uosm(mOsm/ kgH20)
8491
111105808686
Uosm(MOSM /kgH20)
9323361
13318012927118686
UNa + UCiUosm(%)33.3357.1448.6557.1432.5045.3519.77
UNa + UcIUosm(%)
50.5442.4942.6261.1653.8969.7761.2552.6933.72
Uosm V( aOsm/min)
138417861317203725162506906
Uosm V{AOsm /min)
69497977310551007183715201216587
Cosm(mi/min)
4.96.34.87.08.78.43.2
Cosm(ml/min)
2.43.52.63.63.46.15.34.12.1
CH2O(ml/min)11.513.26.8
12.522.719.97.3
C H20(ml/min)
5.11.09.94.62.28.20.32.54.7
VV
(mi/min)16.419.511.619.531.428.310.519.319.716.615.8
V(mi/min)
7.54.5
12.58.25.6
14.35.66.66.8
compared with the Student t test for unpairedvariables. Regression lines and correlation co-efficients were calculated according to standardstatistical techniques.34
ResultsThe results are presented in tables 1, 2, and
3 and in figures 1 to 7. Each number in thetables and each point on the graphs representthe mean of values obtained in one studyduring three or four 10-minute clearance pe-riods at a steady state of water diuresis.
Electrolyte Excretion
The patterns of electrolyte excretion ex-hibited by hypertensive patients during theCirculation, Volume XXXVII, MaY 1968
dextrose and water (D/W) infusions appearin tables 1 to 3 and figure 1. Also shown forcomparison are the patterns exhibited by nor-mal and sodium-depleted control subjects.An exaggerated natriuretic response to 5%
D/W infusion was observed in all but two ofthe hypertensive subjects (fig. 1). Urinarysodium excretion in the patients with elevatedblood pressure averaged 458 ± 210 IuEq/min,a value significantly higher than the meansodium excretion of normal subjects on simi-lar diets who received similar amounts offluid (15 ml/min), 133 ± 29 .tEq/min (P <0.01). The urinary sodium excretion of hy-pertensive patients who received the infusion
835
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from

Table 3Electrolyte Excretion During Five Per Cent Dextrose-Water Infusions in Normal Subjects
CIN CPAH(ml l min) (ml / min)
Regular SodiumB.U.S.M.S.U.S.M.I.P.E.F.R.
Diet-5% D/W infusion i.v. at 15 ml/min128/68113/77109/70111/72108/60114/76
Low-Sodium Diet-5% D/WS.M. 110/72S.M.I. 105/60P.E. 94/64P.E.T. 100/64P.E. 98/70
103126160124148112
infusion i.v.
108129123179142
698897990613789654
at 15 ml/min640630592751630
800 r-
700 H
600 [
500 F
400 1-
300
200
100 F
0
U
0
0
a
a
a
a
a
a
..0
0
a
OCP 0
0
10 20 30V ml/min
Figure 1
Sodium excretion of hypertensive patients and normalsubjects during 5% D/W infusions is plotted againstthe simultaneous urinary volume in each study. Anexaggerated natriuresis was apparent in the hyperten-sive patients. In studies performed with a D/W in-fusion rate of 15 ml/min, the sodium excretion rate(UNa V) was higher in the hypertensive (-) than inthe normal (o) subjects, even when the urinary flowrates (V) were comparable. Values from studies ofhypertensive patients receiving D/W at 9 ml/minare indicated by a and from studies of salt-depletednormal subjects are indicated by a.
of D/W at the slower rate of 9 ml/min wasalso above normal and averaged 317 + 178uEq/min (P<0.02).Mean serum sodium concentration was not
significantly different in the hypertensive andnormal subjects (139 ± 6 mEq/L and 140±4 mEq/ L, respectively), and the mean fil-tered load of sodium was somewhat lowerin the hypertensive group as a consequenceof a lower mean glomerular filtration rate(vide infra). Despite this, the fraction offiltered sodium excreted in the urine (E/FNa(averaged 4.51 + 2.84% in the hypertensivesubjects and was significantly higher thanthe E/FNa of 0.74 + 0.17% noted in the controlsubjects (P <0.001). Mean E/FNa in hyper-tensive subjects who received the slower in-fusion was also increased to 3.60 ± 3.40%.
Dietary sodium depletion diminished thesodium excretion observed in the control sub-jects during a D/W infusion; in these studiesurinary sodium output averaged 39 + 18 ,uEq/min, and there was a corresponding declinein the tubular rejection fraction for sodiumto 0.21 ± 0.08%.
Urinary potassium output was 80 + 41 ,tEq/min and 50 ± 11 ,uEq/min in the two sets ofstudies of hypertensive patients, not signifi-cantly increased above the values observed innormal persons on regular sodium diets, 52 +
Circulation, Volume XXXVII, May 1968
SubjectBP
(mm Hg)RBF
(ml/min)
Filtrationfraction(N)
Renalresistance(RU)
UXaV(,aEqImin)
7.876.355.189.016.507.84
124614951736102112931211
1066105097012941068
79155148151119147
14.7614.0516.1620.2218.7717.13
16.8820.4820.7823.8322.54
8.547.908.146.347.87
2024466344
UNaVuEq/min
CANNON836
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from

FIVE PER CENT DEXTROSE-WATER INFUSIONS 837
Uosm UNa + UcIUKV E/FNa (mOsm/kg Uosm Uosm V Cosm CH20 V
(,uEqlmin) (%) H20) (%) (,Osm/min) (mllmin) (ml/min) (ml/mmin)
242972548154
12895353718
0.5430.8780.6510.8390.5950.958
0.1370.1390.3220.2100.226
645171595958
7470575635
12.529.418.330.515.324.1
4.054.287.008.90
11.40
1142797104682312051150
12461156908928512
4.12.93.72.94.24.1
4.54.23.33.21.8
13.612.711.211.016.115.6
12.412.312.413.512.9
17.715.614.913.920.319.7
16.916.515.716.714.7
23 uEq/min, or after sodium deprivation 63+ 47 ,iEq/min.Renal Hemodynamics
Mean arterial blood pressure of the hyper-tensive patients was significantly elevated andaveraged 158 ± 19 mm Hg during the 11studies with 5% D/W at 15 ml/min and 185 ±mm Hg during the nine studies at 9 ml/min(tables 1 and 2). Mean blood pressure during
studies of the control subjects who receivednormal sodium diets averaged 92 ± 5 mmHg (table 3). During studies of control subjectsafter sodium depletion mean arterial bloodpressure was reduced to 84 + 4 mm Hg.
Glomerular filtration rate of the hyper-tensive patients was reduced; the inulin clear-ance (CIN) was 82 ± 28 ml/min in thosewho received the more rapid D/W infusionsand 80+20 ml in the other group. In the
240
220 U8
0a
a aa*
S . vq 0* _
ft
OA O°aAA i
0
0
a
0
U
* a
* 0
0
.
0 0
A
400 800 1200 1600 0 40 80RBF ml /min GFR ml/min
Figure 2
cpa a aO
0
0
an
0 * *:so
00 0o
120 160 0 15FILT FX %
30
The level of mean arterial blood pressure during each study is plotted against the renal bloodflow (ERBF) in left column, the glomerular filtration rate (CIN) in center column, and againstthe filtration fraction (%) in right column.
Circulation, Volume XXXVII, May 1968
180MEANBYmm Hg
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from

CANNON
control subjects the CIN was 129 + 21 ml/minin those on regular sodium diets and 138 + 27ml/min in those who were deprived of sodium.Effective renal blood flow (ERBF) was alsodecreased in the two hypertensive groups, av-eraging 735 + 182 ml/min in the former and628 + 148 ml/min in the latter. In the controlsubjects ERBF was 1334 + 249 ml/min and1090 + 121 ml/min after sodium depletion.Among the entire group of studies of normal
and hypertensive patients there was an in-verse relationship between the height of meanblood pressure and the effective renal bloodflow (fig. 2 left). No directly inverse relation-ships between the level of blood pressure andthe glomerular filtration rate or filtration frac-tion were apparent however (fig. 2 left, cen-ter, and right).
Relationships Between Salt Excretionand Solute Load
In order to examine the possibility thatthe increased tubular salt rejection by hyper-tensive subjects might have resulted from anosmotic diuresis in these patients, various re-lationships between sodium excretion andsolute load were calculated. In the studies ofhypertensive patients and normotensive con-trol subjects there was a poor correlation be-tween the filtered solute load and the rate ofurinary sodium excretion (r = 0.493). Sim-ilarly, the correlation between the urinaryexcretion of solutes exclusive of sodium andchloride and the rate of urinary sodium ex-cretion was also poor (r - 0.083). The "non-salt" solute excretion was calculated per 100ml of glomerular filtration in both normal andhypertensive patients to correct for possi-ble differences in renal mass; this value alsodid not correlate well with the E/FNa%(r= 0.6468).Increased Sodium and Osmolar Concentrationsin Hypertensives (Table 1)During a steady state of water diuresis
urinary osmolality averaged 92 ± 12 mOsm/L in the hypertensive patients, a value sig-nificantly higher than the mean osmolality of69 + 7 mOsm/L observed in the normal sub-jects who received the same amounts of fluid(15 ml/min) (P < 0.01). Urinary osmolality
was 152 ± 70 mOsm/L in the hypertensivesubjects who received the D/W infusion at aslower rate, and was 58 ± 15 mOsm/L duringstudies of salt-depleted normal subjects.The increased urinary osmolality of the
hypertensive subject was largely due to in-creased urinary sodium and chloride concen-trations. During peak water diuresis theurinary sodium concentration (UNa) of the hy-pertensive patients averaged 38 ± 4 mEq/L,a value significantly higher than the (UNa)of 19 ± 4 mEq/L observed in control sub-jects receiving the same diet and similar D/Winfusions (15 ml/min) (P <0.01). The dataplotted in figure 1 indicate that hypertensivepatients excreted more sodium per unit vol-ume of urine even when urinary flow rateswere in the same range as those of the normalcontrols. The percentage of the urinary osmo-
lality due to salt ( UNa+ c %) averaged
43 + 14% and 52 + 11%, respectively, in thetwo groups of hypertensive patients but only22+8% in control subjects receiving regulardiets and 7 + 3% in control subjects aftersodium depletion. Thus the increased contribu-tion of sodium and chloride to urinary osmo-lality in the hypertensive patient was highlysignificant (P < 0.01).
Patterns of Solute and Free Water ClearanceDuring Water Diuresis (Table 1)
The urinary flow rate during the rapiddextrose-water infusion averaged 19.6 + 7.8ml/min in the hypertensive patients and17.0 + 2.6 mI/mim in the control subjects. Inthe hypertensive group the osmolar clear-ance (C0,, ) of 6.2 ± 2.0 ml/min was sig-nificantly increased above that of normalsubjects, 3.7 + 0.6 ml/min (P <0.02). How-ever, there was no significant difference inthe free water clearance (CH2O) of the twogroups; Cn2o averaged 13.4 + 6.0 ml/min inthe patients with hypertension and 13.4 +2.2 ml/min in the control subjects. In bothnormal and hypertensive subjects CH20 andthe urinary flow rate (V) were directly re-lated (fig. 3); however, less free water was
Circulation, Volume XXXVII, May 1968
838
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from

FIVE PER CENT DEXTROSE-WATER INFUSIONS
22.0 F
18.0 F
CH2 14.0ml/min
10.0 F
6.0 F2.0
30.0 r
00a
0
0l
0 *
25.0 F
20.0 tDISTAL No
REJECTION
0 4 8 12 16 20 24 28 32V ml/min
Figure 3
In studies performed during peak water diuresis(D/W at 15 ml/min) the urinary flow rate (V) isplotted against the simultaneous free water clearance(CH20). In both hypertensive and normal subjects,CH20 increased as the urinary flowv rate V rose. Lessfree water (CH20) was formed at each level of V inthe hypertensive group.
excreted per unit of urine flow in the hyper-tensive than in the normal subjects (fig. 3).Although not shown, the relationship betweenCH20 and V remained unchanged when thevalues in both groups were calculated per100 ml of glomerular filtrate.
Fractional Sodium Rejection in the Proximal(Isosmotic) and Distal (Diluting) Portionsof the Nephron
The fraction of filtered sodium rejectedfrom portions of the nephron, where reab-sorption is isosmotic (proximal tubules), hasbeen calculated for each study during peakwater diuresis (see Methods). The mean"proximal" sodium rejection observed dur-ing the rapid D/W infusions in the hyperten-sive patients averaged 17.9 ± 5.4% of thefiltered sodium load, a value that was higherthan the 11.4 + 2.6% observed in the normalgroup (P <0.05). Mean "proximal" rejectionwas not significantly reduced in the controlsubjects after sodium depletion, 9.5 + 1.8%(P < 0.2).The fraction of the "distal" sodium load
excreted during the infusions was also cal-culated for each study (see Methods). Thepercentage of the "distal sodium load" thatescaped reabsorption in the diluting segmentsof the nephron averaged 19.3 + 7.4% in theCirculation, Volume XXXVII, May 1968
15.0 F
100 t-
5.0
.0
0
0
0
00
0LaAn
1000 2000 3000 4000"DISTAL No LOAD".uEq/min
Figure 4
The amount of sodium that was delivered beyondsites of isosmotic (proximal) reabsorption was calcu-lated for each study during peak water diuresis (UNaV + PNa X C, 2 ). This "distal sodium load" is plot-ted against the percentage of the distal sodium loadexcreted in the urine-"distal rejection fraction %."At comparable levels of delivery of sodium to dilutingsegments of the nephron, the distal rejection fractionwas significantly elevated in the hypertensive patients(P <0.001).
hypertensive patients, a value signfficantlyabove the 6.8 + 1.7% found in the normalsubjects (P < 0.001). Distal sodium reab-sorption was increased by salt depletion inthe control subjects; the fraction of the distalsodium load that escaped reabsorption in thediluting segments was only 2.0 + 0.8% in thesestudies.
In figure 4 the amount of sodium deliveredbeyond the sites of isosmotic (proximal) re-absorption in studies of hypertensive andnormal subjects is plotted against the per-centage of this "distal sodium load" that es-caped reabsorption in the diluting segments.In the hypertensive patients the amounts ofsodium presented to the diluting segmentsof the nephron were as large as or largerthan those in normal subjects. Nevertheless,despite comparable or increased sodium de-livery to the distal nephron, the percentageof the "distal sodium load" that escaped
839
.
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from
CANNON
220[-
200 -
180
160 1-
a
a
a X
a**.U.0
0
: -140 F-
0
a cpa
so
1.0 3.0 5.0 7.0
E/F No%
Figure 5
9.0 11.0
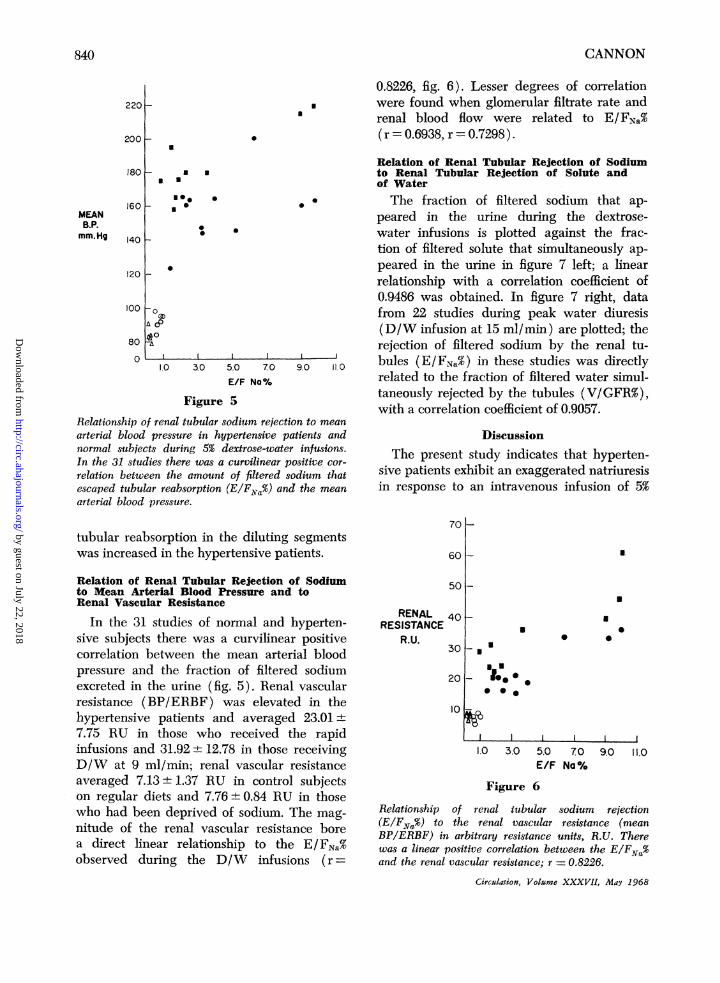
Relationship of renal tubular sodium rejection to meanarterial blood pressure in hypertensive patients andnormal subjects during 5% dextrose-water infusions.In the 31 studies there was a curvilinear positive cor-
relation between the amount of filtered sodium thatescaped tubular reabsorption (E/FNa%) and the mean
arterial blood pressure.
0.8226, fig. 6). Lesser degrees of correlationwere found when glomerular filtrate rate andrenal blood flow were related to E/FNa%(r=0.6938, r =0.7298).
Relation of Renal Tubular Rejection of Sodiumto Renal Tubular Rejection of Solute andof WaterThe fraction of filtered sodium that ap-
peared in the urine during the dextrose-water infusions is plotted against the frac-tion of filtered solute that simultaneously ap-peared in the urine in figure 7 left; a linearrelationship with a correlation coefficient of0.9486 was obtained. In figure 7 right, datafrom 22 studies during peak water diuresis(D/W infusion at 15 ml/min) are plotted; therejection of filtered sodium by the renal tu-bules (E/FNa%) in these studies was directlyrelated to the fraction of filtered water simul-taneously rejected by the tubules (V/GFR%),with a correlation coefficient of 0.9057.
DiscussionThe present study indicates that hyperten-
sive patients exhibit an exaggerated natriuresisin response to an intravenous infusion of 5%
tubular reabsorption in the diluting segmentswas increased in the hypertensive patients.
Relation of Renal Tubular Rejection of Sodiumto Mean Arterial Blood Pressure and toRenal Vascular Resistance
In the 31 studies of normal and hyperten-sive subjects there was a curvilinear positivecorrelation between the mean arterial bloodpressure and the fraction of filtered sodiumexcreted in the urine (fig. 5). Renal vascularresistance (BP/ERBF) was elevated in thehypertensive patients and averaged 23.01 +
7.75 RU in those who received the rapidinfusions and 31.92 12.78 in those receivingD/W at 9 ml/min; renal vascular resistanceaveraged 7.13+±1.37 RU in control subjectson regular diets and 7.76 0.84 RU in thosewho had been deprived of sodium. The mag-
nitude of the renal vascular resistance borea direct linear relationship to the E/FNa%observed during the D/W infusions (r =
701-
601- a
501-
RENAL 40
RESISTANCER.U.
30j
20
10
-
* 0 .
a
0
0.
I I I
1.0 3.0 5.0 70 9.0 11.0E/F Na%
Figure 6
Relationship of renal tubular sodium rejection(E/FNO%) to the renal vascular resistance (meanBP/ERBF) in arbitrary resistance units, R.U. Therewas a linear positive correlation between the E/FNa%and the renal vascular resistance; r 0.8226.
Circalation, Volume XXXVII, May 1968
MEANB.P.mm.Hg
120 1-
100
80
0
840
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from

FIVE PER CENT DEXTROSE-WATER INFUSIONS
01-
9
8
6
4
3
10a
9
8
7
6
0
0
0
.E/FNa %
a4
0
3
aU2 0
O.a4*an0
0
0 2 4 6 8 10 12 14E/F osm%
2
0
0
00 0
0 0 0
ooa ol
5 10 15 20V
GFR%
25 30 35 40
Figure 7
During 5% dextrose-water infusions in hypertensive patients there was direct relationshipbetween the tubular rejection of filtered sodium (E/FNO%) and the tubular rejection of filteredsolute (E/F'osm%) r= 0.9486. In studies performed during a steady state of water diuresis(D/W at 15 ml/min), the tubular rejection, of filtered sodium was also directly related to thetubular rejection of filtered water (V/GFR%); r = 0.9057.
dextrose and water. This finding confirmsa report by Ek,29 who in 1955 reported in-creased sodium excretion by hypertensivepatients in response to infusions of 5% D/W,but differs from observations of Hollander'35and Steinmetz and associates,36 who did notobserve increased natriuresis in hypertensivepatients during infusions of 3.5% and 2.5%glucose in water. As will be discussed subse-quently, differences in the degree of extra-cellular fluid expansion produced by theinfusions* and in the renal hemodynamics
*Undoubtedly both intracellular and extracellularfluid compartments increased as glucose present inthe 5% D/W was metabolized by the body. However,since the infusions were rapid, the rate of glucoseintake probably exceeded the rate of its metabolismas suggested by an occasional trace of glycosuria.Hence a greater expansion of the extracellular fluidcompartment was probably present throughout thestudies.Circulation, Volume XXXVII, May 1968
of the patients studied may account for thediscrepancy between the various reports.The increased urinary sodium excretion ex-
hibited by the hypertensive patients in thepresent studies did not result from larger in-creases in the filtered load of sodium in re-
sponse to 5% D/W because (1) mean serum
sodium concentration of the hypertensive pa-
tients during diuresis was not significantlyelevated above that of the control subjects,and (2) mean glomerular filtration rate was
lower in patients with increased blood pres-
sure. Since the fraction of filtered sodiumexcreted by the hypertensive subjects was
significantly increased above that of the con-
trol subjects, the data indicate that renaltubular sodium reabsorption was reduced inthe patients with arterial hypertension duringthe D/W infusions.
In the study of Ek,29 the possibility thatincreased natriuresis in patients with hyper-tension resulted from a concomitant glucose
E/FNo% 5 _
vrt IE
841
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from

CANNON
osmotic diuresis was not rigidly excluded. Itseems most unlikely that an osmotic diuresisaccounted for the impaired renal tubularsodium reabsorption observed in hypertensivepatients in the present studies for severalreasons: (1) there was a poor correlationbetween the filtered osmotic load and therejection fraction of sodium, (2) increasedtubular rejection of filtered sodium was ap-parent in individual hypertensive subjectswho exhibited rates of glomerular filtrationthat equaled or exceeded those of individualcontrol subjects (table 1), (3) the percentageof the urinary osmolality due to sodium andchloride was increased more than twofoldabove normal in the hypertensive patients,and (4) there was a poor correlation betweenthe excretion rate of solutes other than so-dium and chloride and the urinary sodiumoutput.
It also seems unlikely that an osmotic diu-resis of functioning residual nephrons ac-counts for the increased E/FNa% of hyper-tensive patients during D/W loading, eventhough such a mechanism may explain inpart the increased sodium rejection observedin uremic patients7: First, none of the hyper-tensive patients subjected to D/W infusionhad a blood urea nitrogen greater than 25mg%; with only a few exceptions they ex-hibited only moderate reductions of glomer-ular filtration. Second, during an osmoticdiuresis of residual nephrons, a linear cor-relation would be anticipated between theexcretion of solutes other than sodium andchloride calculated per 100 ml of glomerularfiltration and the fraction of filtered sodiumthat escaped reabsorption; the absence ofsuch a correlation in the present study tendsto make this mechanism an unlikely causefor increased salt rejection by the hyperten-sive patients.From an analysis of the patterns of solute
and free water clearance that accompanytubular salt rejection during water diuresis,one may ascertain whether impaired tubularsodium transport occurred in portions of thenephron where reabsorption is isosmotic(proximal tubules) or in more distal portions
of the nephron where osmotically free wateris generated by the selective reabsorption ofsodium (loops of Henle, distal tubules).The finding that the "proximal" sodium
rejection fraction was increased in hyperten-sive patients (P <0.05) suggests that someof the increased sodium rejection inducedby a D/W infusion in the hypertensive groupmay have occurred in the proximal tubules.This interpretation is consistent with the re-port of Metzger and associates,37 who foundthat CH20/GFR per unit Cosm/GFR wasincreased in hypertensive patients duringoral water loads. In animal studies extra-cellular volume expansion by infusion ofsaline or Ringer's solution has been demon-strated to depress proximal tubular reabsorp-tion in rats'3' 38, 39 and dogs40 by a mech-anism independent of glomerular filtrationrate, plasma protein concentration, aldoste-rone activity, or antidiuretic hormone.4' Thatextracellular fluid (ECF) expansion with di-lute dextrose solutions can produce a similareffect on proximal salt reabsorption in animalsis supported by observations of Martino andEarley42; these investigators noted depressedfractional reabsorption of sodium in the prox-imal tubules of dogs with diuretic-inducedblockade of distal tubular sodium reabsorp-tion during rapid infusions of distilled wateror dilute solutions of glucose.To assess accurately sodium reabsorption
in "distal" segments of the nephron it isnecessary to consider both the delivery ofsodium to the diluting sites and also theintrinsic characteristics of sodium reabsorp-tion in these areas.43 Since little water escapesfrom the distal segments at high rates ofwater diuresis, the urinary flow rate, V, wastaken as an approximation of the amount ofsodium-containing fluid reaching the dilutingsegments, and CH20 was taken as an approxi-mation of selective sodium reabsorption inthese areas.* As delivery of sodium-containing
*Although C,1,20 actually represents the amount offree water generated in the ascending limb anddistal tubules minus any back diffusion of water thatoccurs in the distal tubule and collecting duct, it is
Circulation, Volume XXXVII, May 1968
842
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from

FIVE PER CENT DEXTROSE-WATER INFUSIONS
fluid to the diluting segments increased inboth the normals and hypertensives, C1920also increased (fig. 3). Thus during the D/Wload a complete inhibition of distal sodiumreabsorption was not apparent in either groupof subjects, nor was a transfer maximum fordistal sodium transport demonstrated overthe range of distal delivery achieved in thesestudies.However, fractional sodium reabsorption in
diluting segments of the nephron was de-pressed in the hypertensives during the D/Winfusions. Nineteen per cent of the "distalsodium load" of the hypertensive patientswas excreted in the urine whereas only 7%of the "distal sodium load" escaped reab-sorption in the normal subjects on regulardiets, and only 2% in normals after sodiumdepletion. The difference between hyperten-sive and normal subjects in fractional rejec-tion of the sodium delivered to the distalnephron was highly significant (P < 0.001)and was proportionally greater than theincrease in "proximal" rejection found inhypertensive patients during the same in-fusions.
Micropuncture studies in normal rats3 38, 39and dogs40 have indicated that the markeddepression of fractional sodium reabsorptionthat occurs in the proximal tubules duringECF volume expansion with saline is ac-companied by a much smaller change insodium excretion, because there occurs simul-taneously an increased reabsorption of sodiumin the distal nephron, particularly in theloops of Henle. The present finding that thefractional "distal" sodium reabsorption wasreduced 12% below normal in hypertensivepatients during 5% D/W infusion suggeststhat reduced distal tubular sodium transportmay explain to a major extent why hyperten-sive patients excrete more sodium than nor-mal subjects in response to infusions thatexpand extracellular fluid volume.
uinlikely that back diffusion of water was significantlydiminished in hypertensive patients with increasedurinary flow rates, since (Uos, ) was increased, notdecreased, in those patients.
Circulation, Volume XXXVII, May 1968
Other data also indicate that urinary dilu-tion was altered in the hypertensive patientsduring the (15 ml/min) D/W infusions: (1)mean Uosm and UNa were higher in the hyper-tensive than in the normal subjects; (2)mean CH20/GFR per Cosm/GFR was lowerin the hypertensive patients; (3) slightlyless CH120 was formed by hypertensive pa-tients at any given urinary flow rate (fig. 3);and (4) at comparable levels of "distal so-dium load," the hypertensive patients ex-hibited greater "distal" tubular sodium rejec-tion (fig. 4) and were unable to lower UO,mand UNa to the levels attained by normalsubjects.Whether the altered urinary dilution and
the reduced fractional "distal" sodium reab-sorption demonstrated in hypertensive pa-tients during the D/W infusions occurred inthe loop of Henle or in the "corticaY' dilutingsegment43 or in both sites cannot be ascer-tained from the present studies. However,reductions in urinary concentrating abilityin dehydrated hypertensive patients havebeen reported by other investigators.'7 4' 45Moreover, Buckalew, Ramirez, and Gold-berg46 have recently found a reduced TCH1,,per unit Cos01 during the natriuresis inducedby hypertonic saline in antidiuretic hyperten-sive patients. Together with the present find-ings the accumulated observations suggestthat at least some of the impaired urinarydilution and 'distal" sodium rejection ob-served in hypertensive patients during ECFvolume expansion results from a defect insodium reabsorption in the ascending limbof the loop of Henle.The curvilinear positive correlation be-
tween the level of mean arterial blood pres-sure and tubular sodium rejection observedin the normal and hypertensive subjects dur-ing the D/W infusions (fig. 5) suggests thatrenal arterial pressure is in some way in-volved in the mechanism for increased sodiumrejection by the latter group. Rough correla-tions between the magnitude of natriuresisand the height of blood pressure have beenreported in several studies of hypertensivepatients receiving saline loads.'8 20.21 25 In
843
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from
CANNON
addition, a variety of renal perfusion studieshave indicated that increases of renal arterialblood pressure may increase urinary salt andwater excretion without affecting glomerularfiltration rate.47A9 In stop-flow studies of
Tobian and associates50 the "distal" nephron
was the site of impaired sodium reabsorptionin rat kidneys that were perfused with bloodat elevated pressures.
Although depressed glomerular filtrationrate and renal blood flow were to some ex-
tent correlated with increased E/FNa% in thepresent studies, these correlations were lesssignificant than the linear positive relation-ship between the degree of tubular sodiumrejection and the calculated renal vascularresistance (fig. 6). This finding is similar tothe direct correlation between salt rejectionand renal vascular resistance noted by Cottier,Weller, and Hoobler24 in a group of hyperten-sive patients given saline infusions. Renal vas-
cular resistance is a numerical expression ofthe intensity of hypertensive renovasculardisease; these observations therefore suggestthat alterations of renal pressure and vascularresistance in the kidneys of hypertensive pa-
tients may determine the increased salt re-
jection exhibited by these patients duringsaline, mannitol, or 5% D/W infusions.
It has been suggested that proximal tubularsodium reabsorption is regulated by a natri-uretic hormone of extrarenal'0 or intrarenalorigin.51 Whether greater amounts of a pos-
tulated natriuretic hormone are elicited byvolume expansion in patients with increasedblood pressure and increased vascular resis-
tance, or whether normal amounts of thissubstance elicit greater natriuresis in hyper-tensive patients because of abnormalities ofrenal hemodyamics are questions that awaitfurther study.
Alternatively, physical factors may influencetubular sodium transport. Earley and associ-ates,5' 12 have provided evidence to sup-
port the hypothesis that transmission ofarterial blood pressure along the renal vas-
culature may act to inhibit tubular sodiumtransport, possibly by altering renal interstitialvolume. In the present studies during water
diuresis the rejection fraction of sodium wasdirectly related not only to the rejectionfraction of total solute (E/FFosm%) but alsoto that of filtered water (V/GFR%). Sucha balance between the fractional excretionof sodium and water is not characteristic ofthe action of any known hormone and sug-gests that the changes in sodium and wateroutput were mediated by physical factors.Mechanisms whereby the combination of in-creased blood pressure and increased renalvascular resistance could produce proportion-ate changes in the tubular rejection of filteredsodium, solute, and water during ECF ex-pansion in hypertensive man remain specula-tive at this time. It is conceivable howeverthat (1) medullary washout secondary to apressure induced increase in medullary bloodflow52; (2) increased passive back diffusionof reabsorbed sodium and water due to al-tered pressure and resistance in peritubularcapillaries,12 13, 53 or (3) a pressure-induceddistortion of the normal relationship betweenthe quantity of glomerular filtrate and tubularvolume, with a consequent increased linearvelocity of tubular flow,54 could contributeto a hemodynamically mediated natriuresisin these patients.
References1. MILLS, I. H., DE WARDENER, H. E., HAYTER,
C. J., AND CLAPHAM, W. F.: Studies on theafferent mechanism of the sodium diuresiswhich follows the administration of intravenoussaline in the dog. Clin Sci 21: 259, 1961.
2. LEVINSKY, N. G., AND LALONE, R. C.: Mechanismof sodium diuresis after saline infusion in thedog. J Clin Invest 42: 1261, 1963.
3. BLYTHE, W. B., AND WELT, L. G.: Dissociationbetween filtered load of sodium and its rateof excretion in the urine. J Clin Invest 42:1491, 1963.
4. RECTOR, F. C., JR., VAN GIESEN, G., KIIL, F., ANDSELDIN, D. W.: Influence of expansion ofextracellular volume on tubular reabsorptionof sodium independent of changes in glomeru-lar filtration rate and aldosterone activity.J Clin Invest 43: 341, 1964.
5. EARLEY, L. E., AND FRIEDLER, R. M.: Observa-tions on the mechanism of decreased tubularreabsorption of sodium and water during salineloading. J Clin Invest 43: 1928, 1964.
Circulation, Volume XXXVIl, May 1968
844
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from
FIVE PER CENT DEXTROSE-WATER INFUSIONS
6. STEIN, R. M., BERCOVITCH, D. D., AND LEVITT1,M. D.: Dual effects of saline loading on renaltubular sodium reabsorption in the dog. AmerJ Physiol 207: 826, 1964.
7. BRICKER, N. S.: Control of sodium excretionwith normal and reduced nephron populations:Pre-eminence of third factor. Amer J Med43: 313, 1967.
8. JOHNSTON, C. I., AND DAVIS, J. O.: Evidencefrom cross circulation studies for a humoralmechanism in the natriuresis of saline loading.Proc Soc Exp Biol Med 121: 1058, 1966.
9. LIcHARDUS, B., AND PEARCE, J. W.: Evidencefor a humoral natriuretic factor released byblood volume expansion. Nature (London)209: 407, 1966.
10. MARTINEZ-MALDONADO, M., KURTZMAN, N. A.,RECTOR, F. C., JR., AND SELDIN, D.: Evidencefor a hormonal inhibitor of proximal tubularreabsorption. (Abstr.) J Clin Invest 46: 1091,1967.
1 1. EARLEY, L. E., AND FRIEDLER, R. M.: Effects ofcombined renal vasodilatation and pressor
agents on renal hemodynamics and the tubu-lar reabsorption of saline. J Clin Invest 45:542, 1966.
12. EARLEY, L. E., MARTINO, J. A., AND FRIEDLER,R. M.: Factors affecting sodium reabsorptionby the proximal tubule as determined duringblockade of distal sodium reabsorption. J ClinInvest 45: 1668, 1966.
13. RECTOR, F. C., JR., SELLMAN, J. D., MARTINEZ-MALDONADO, M., AND SELDIN, D. W.: Mecha-nism of suppression of proximal tubular re-
absorption by saline infusion. J Clin Invest46: 47, 1967.
14. FARNSWORTH, E. B.: Renal reabsorption ofchloride and phosphate in normal subjects andin patients with essential hypertension. J ClinInvest 35: 897, 1946.
15. GREEN, D. M., WEDELL, H. G., WALD, M. H.,AND LEARNED, B.: Relation of water andsodium excretion to blood pressure in humansubjects. Circulation 6: 919, 1952.
16. BIRCHALL, R., TUTHILL, S. W., JACOBS, W. S.,TRAUTTMAN, W. J., JR., AND FINDLEY, T.: Renalexcretion of water, sodium, and chloride: Com-parison of the responses of hypertensive pa-
tients with those of normal subjects, patientswith specific adrenal or pituitary defects, anda normal subject primed with various hor-mones. Circulation 7: 258, 1953.
17. BRODSKY, W. A., AND GRAUBARTH, H. N.: Ex-cretion of water and electrolytes in patientswith essential hypertension. J Lab Clin Med41: 43, 1953.
18. GREEN, D. M., AND ELLIS, E. J.: Sodium output-blood pressure relationships and their modifica-tion by treatment. Circulation 10: 536, 1954.
Circulation, Volume XXXVII, May 1968
19. GREEN, D. M., JOHNSON, A. C., BRIDGES, W. C.,AND LEHMAN, J. N.: Stages of salt ex-
change in essential hypertension. Circulation9: 416, 1954.
20. THOMPSON, J. E., SILVA, T. F., KINSEY, D.,AND SMITHWICK, R. H.: Effect of acute saltloads on the urinary sodium output of normo-
tensive and hypertensive patients before andafter surgery. Circulation 10: 912, 1954.
21. COTTIER, P. T., WELLER, J. M., AND HOOBLER,S. W.: Sodium chloride excretion followingsalt loading in hypertensive subjects. Circula-tion 18: 196, 1958.
22. HOLLANDER, W., AND JUI)SON, W. E., Electrolyteand water excretion in arterial hypertension:I. Studies in non medically treated subjectswith essential hypertension. J Clin Invest 36:1460, 1957.
23. BALDWIN, D. S., BIGGS, A. V., GOLDRING, W.,HULET, W. H., AND CHAsIs, H.: Exaggeratednatriuresis in essential hypertension. Amer JMed 24: 893, 1958.
24. COTTIER, P., WELLER, J. M., AND HOOBLER,S. W.: Effect of intravenous sodium chlorideload on renal hemodynamics and electrolyteexcretion in essential hypertension. Circulation17: 750, 1958.
25. HANENSON, I. B., TAUSSKY, H. H., POLASKY, N.,RAUSOHOFF, W., AND MILLER, B. F.: Renalexcretion of sodium in arterial hypertension.Circulation 20: 498, 1959.
26. PAPPER, S., BELSKY, J. L., AND BLEIFER, K. H.:Response to the administration of an isotonicsodium chloride-lactate solution in patientswith essential hypertension. J Clin Invest 39:876, 1960.
27. ULRYCH, M., HOFMAN, J., AND HEJL, Z.: Cardiacand renal hyper responsiveness to acute plasmavolume expansion in hypertension. Amer HeartJ 68: 193, 1964.
28. WESTON, R. E., HELLMAN, L., ESCHER, D. J. W.,EDELMAN, I. S., GROSSMAN, J., AND LEITER, L.:Studies on the influence of the low sodiumcardiac diet and the Kempner regimen on
renal hemodynamics and electrolyte excretionin hypertensive subjects. J Clin Invest 29: 639,1950.
29. EK, J.: Influence of heavy hydration on therenal function in normal and hypertensiveman. Scand J Clin Lab Invest 7: (suppl. 19):1, 1955.
30. BALDWIN, D. S., SCHREINER, G. E., BREED, E. S.,WESSON, L. G., JR., AND MAXWELL, M. H.:Depression of apparent p-amino hippurate ex-
traction ratio by glucose. J Clin Invest 29:614, 1950.
31. FUHR, J., KACZMARCZYK, J., UND KRiiTTGEN, C.:Eine einfache colorimetrische Methode zur
Inulinbestimmung fur Nieren-Clearance-Unter-
845
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from
CANNON
suchungen bei Stoffwechselgesunden und Di-abetikern. Klin Wschr 33: 729, 1955.
32. CoTLOvE, E.: C14 inulin method, carboxy-labeledinulin as a tracer for inulin. Fed Proc 14:32, 1955.
33. SMITH, H. W.: Principles of Renal Physiology.New York, Oxford University Press, 1956.
34. DIXON, W. J., AND MASSEY, F. J., JR.: Introduc-tion to Statistical Analysis. New York, Mc-Graw-Hill Book Co., 1957.
35. HOLLANDER, W.: Effects of intravenous hydra-tion and pitressin on renal function in sub-jects with essential hypertension. Circulation19: 691, 1959.
36. STEINMETZ, P. R., EISINGER, R. P., GOMBOS, E.A., CHASIS, H., AND BALDWIN, D. S.: Excretionof free water and solute during maximal waterdiuresis in normal and hypertensive subjects.J Lab Clin Med 64: 238, 1964.
37. METZGER, R., VAAMONDE, L., VAAMONDE, C., ANDPAPPER, S.: Renal sodium excretion duringoral water loading in hypertensive patients.(Abstr.) Clin Res 15: 365, 1967.
38. LANDWEHR, D. M., AND KLOSE, R. M.: Micro-puncture study of sodium in saline loadedrats. Proc Int Cong Nephrol 3: 227, 1966.
39. HAYSLETT, J. P., KASHGARIAN, M., AND EPSTEIN,F. H.: Changes in proximal and distal tubularreabsorption produced by rapid expansion ofextracellular fluid. J Clin Invest 46: 1254, 1967.
40. DIRKS, J. H., CIRKSENA, W. J., AND BERLINER,R. W.: Effect of saline infusion on sodiumreabsorption by the proximal tubule of thedog. J Clin Invest 44: 1160, 1965.
41. LEVINSKY, N.: Non aldosterone influences onrenal sodium transport. Ann NY Acad Sci 139:295, 1966.
42. MARTINO, J. A., AND EARLEY, L. E.: Effects ofinfusion of water on renal hemodynamics andthe tubular reabsorption of sodium. J ClinInvest 46: 1229, 1967.
43. SELDIN, D. W., EKNOYAN, G., SuKi, W. N., ANDRECTOR, F. C., JR.: Localization of diureticaction from the pattern of water and electro-lyte excretion. Ann NY Acad Sci 139: 328,1966.
44. DE LEON, A. C., JR., DREIFUS, L. S., AND BELLET,S.: Urinary osmolar concentration: A means
of evaluating early renal function changes inessential hypertension. Amer J Med Sci 1:144, 1960.
45. BALDWIN, D. S., GOMBOS, E. A., AND CHUSIS,H.: Urinary concentrating mechanism in essen-tial hypertension. Amer J Med 38: 864, 1965.
46. BUCKALEW, V. M., JR., RAMIREZ, M. A., ANDGOLDBERG, M.: Relationship between exag-gerated natriuresis and renal concentratingdefect in hypertensive man. (Abstr.) ProgramFirst Annual Meeting American Society ofNephrology, Los Angeles, Oct. 1967, p. 10.
47. SELKURT, E. E.: Effect of pulse pressure andmean arterial pressure modification on renalhemodynamics and electrolyte and water ex-
cretion. Circulation 4: 541, 1951.48. SHIPLEY, R. E., AND STUDY, R. S.: Changes in
renal blood flow, extraction of inulin, glomeru-lar filtration rate, tissue pressure and urineflow with acute alterations of renal arteryblood pressure. Amer J Physiol 167: 676, 1951.
49. McDONALD, S. J., AND DE WARDENER, H. E.:Relationship between the renal arterial per-fusion pressure and the increase in sodiumexcretion which occurs during an infusion ofsaline. Nephron 2: 1, 1965.
50. TOBIAN, L., COFFEE, K., FERREIRA, D., AND
MEUILI, J.: Effect of renal perfusion on thenet transport of sodium out of distal tubularurine as studied with the stop-flow technique.J Clin Invest 43: 118, 1964.
51. DAVIS, J. O., HOWARMS, S. S., JOHNSTON, C. 1.,AND WRIGHT, F. S.: Renin, sodium-retainingand sodium-excreting hormones and experi-mental renal hypertension. Circulation Re-search 20-21 (suppl. II): II-167, 1967.
52. SELKURT, E. E., WOMACK, I., AND DAILEY, W.N.: Mechanism of natriuresis and diuresis dur-ing elevated renal arterial pressure. Amer JPhysiol 209: 95, 1965.
53. SWANN, H. G., AND PRINE, J. M.: Relation ofintrarenal pressure to blood pressure and toperinephric hypertension. (Abstr.) Fed Proc19: 134, 1951.
54. GERTZ, K. H., MANGOS, J. A., BRAUN, G., ANDPAGEL, H. D.: On the glomerular tubularbalance in the rat kidney. Pfluegers ArchivGes Physiol 285: 360, 1965.
Circulation, Volume XXXVII, May 1968
846
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from

PAUL J. CANNONHypertensive Patients and Its Relation to Renal Hemodynamics
Man: Evidence for Increased Proximal and Distal Tubular Sodium Rejection by Effects of Five Per Cent Dextrose-Water Infusions in Normal and Hypertensive
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1968 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.37.5.832
1968;37:832-846Circulation.
http://circ.ahajournals.org/content/37/5/832located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 22, 2018http://circ.ahajournals.org/
Dow
nloaded from


















