Effective thrombolytic therapy of aortic thrombosis in the small premature infant
3
Effective Thrombolytic Therapy of Aortic Thrombosis in the Small Premature Infant By Robert Richardson, Harry Applebaum, Touraj Touran, Ralph E. Franceschini, Patrick A. Robbie, David D. Wirtschafter, and Paddy Taber Los Angeles, California 9 Aortic thrombosis in the very-low-birthweight prema-- ture infant has remained both a diagnostic and a thera- peutic dilemma. Nine small infants were evaluated for, symptoms of extremity and/or visceral ischemia. All were 9 found to have aortoiliac thrombosis most likely related to indwelling umbilical artery catheters. Diagnostic and thera- 9 peutic options were evaluated. An angiogram obtained. through the catheter was found to be the most effective diagnostic technique. Local infusion of intra-arterial strep-, tokinase (50 U/kg/h) directly into the clot for 36 hours resulted in resolution of ischemic symptoms. No complica- tions were encountered with the use of this protocol. 9 1988 by Grune & Stratton. Inc. INDEX WORDS: aortic thrombosis; flbrinolytic therapy; streptokinase; umbilical artery catheter. z/•RTIC THROMBOSIS in the small premature infant is a catastrophic event, with few intact survivors reported, la This problem is becoming more common because of the increasing ability of neona- tologists to successfully manage the very-low-birth- weight premature infant. The severe pulmonary disease commonly seen in these patients mandates maintaining umbilical artery catheters in place for extended periods of time. Most of these catheters eventually become a nidus for an attached intra-aortic thrombus, the great majority of which remain asymp- tomatic and eventually lyse.4'5 However, a small per- centage of these thrombi will enlarge to produce symptoms of arterial occlusion, usually with disastrous results. The smaller the size of the infant, the smaller the size of the thrombus needed to produce symptoms. Therapy must be instituted promptly before irrevers- ible gangrenous changes of the extremities or viscera develop. Minimal physiologic reserve and small size make these patients poor candidates for surgical aortic thrombectomy. The risk of intraventricular hemor- rhage makes anticoagulant therapy risky. From the Divisions of Pediatric Surgery, Neonatology, and Pediatric Radiology, Kaiser Permanente Medical Center, Los Angeles. Presented at the 19th Annual Meeting of the American Pediatric Surgical Association, Tucson, Arizona, May 11-14, 1988. Address reprint requests to Harry Applebaum, MD, Division of Pediatric Surgery, Kaiser Permanente Medical Center, 1526 N Edgemont St, Los Angeles, CA 90027. 9 1988 by Grune & Stratton, Inc. 0022-3468/88/2312-0023503.00/0 In our initial patients, intravenous (IV) heparin therapy instituted after the development of ischemic changes was unsuccessful in producing resolution or stabilization of the symptoms. Thrombolytic therapy was then evaluated as a more useful alternative, pro- gressing through use of IV streptokinase to a successful protocol using low-dose streptokinase infused directly into the clot via the umbilical artery catheter. MATERIALS AND METHODS During the M-month period from October 1985 to April 1988, nine very-low-birthweight (range, 540 g to 1,980 g; mean, 891 g) premature infants were diagnosed as having aortoiliac thrombosis. Symptoms prompting investigation included cyanotic discoloration of the toes ("catheter toes"); cold, blue, pulseless extremities; patchy gangrene of the skin; gastrointestinal bleeding; sudden onset of hypertension; and necrotizing enterocolitis. Doppler flow studies were used for initial diagnostic screening. During the study aortography became the favored definitive diag- nostic modality, supplanting ultrasonography and technetium radio- nucleide flow studies. Aortograms were performed in the angiogra- phy suite using an injection of dilute contrast solution (Conray 30, Mallinckrodt, Inc, St Louis; 1:1 dilution with normal saline, 1 cc/kg) directly into the umbilical artery catheter. A cranial sonogram was obtained before the infusion to document the absence of recent intraventricular hemorrhage. The patients were divided into three sequential treatment groups (Table 1), reflecting the evolution of an effective protocol. Group 1 included two patients who received IV heparin therapy instituted after the development of gangrenous changes. IV heparin was infused at a rate of 15 to 20 units/kg/h. Monitoring of heparin time was performed every six hours. Group 2 included the subsequent two patients who received IV heparin immediately following onset of early ischemic symptoms. When this was unsuccessful in arresting progression to gangrenous changes, IV streptokinase therapy was instituted. A loading dose of 2,500 U/kg was administered, followed by maintenance dosage of 1,000 U/kg/h. Group 3 included the most recent five patients. These were treated by infusion of low-dose streptokinase through the umbilical artery catheter directly into the thrombus at a rate of 50 U/kg/h for a period of 36 hours. Once symptoms had resolved and the infusion was completed, the catheter was removed. No further anticoagulation was used. All patients were monitored with prothrombin time (PT), partial thromboplastin time (PTT), fibrin split products, and fibrinogen levels. During heparin therapy the PTT was maintained at a level approximately twice the normal value. RESULTS Both patients in group 1 who received only heparin therapy died with progression of ischemic symptoms. One of the two patients in group 2 survived after the level of gangrene stabilized following institution of IV 1198 Journal of Pediatric Surgery, Vo123, No 12 (December),1988: pp 1198-1200
-
Upload
robert-richardson -
Category
Documents
-
view
212 -
download
0
Transcript of Effective thrombolytic therapy of aortic thrombosis in the small premature infant

Effective Thrombolytic Therapy of Aortic Thrombosis in the Small Premature Infant
By Robert Richardson, Harry Applebaum, Touraj Touran, Ralph E. Franceschini, Patrick A. Robbie, David D. Wirtschafter, and Paddy Taber
Los Angeles, California
�9 Aortic thrombosis in the very-low-birthweight prema-- ture infant has remained both a diagnostic and a thera- peutic dilemma. Nine small infants were evaluated for , symptoms of extremity and/or visceral ischemia. All were �9 found to have aortoiliac thrombosis most likely related to indwelling umbilical artery catheters. Diagnostic and thera- �9 peutic options were evaluated. An angiogram obtained. through the catheter was found to be the most effective diagnostic technique. Local infusion of intra-arterial s t rep- , tokinase (50 U / k g / h ) directly into the clot for 36 hours resulted in resolution of ischemic symptoms. No complica- tions were encountered with the use of this protocol. �9 1988 by Grune & Stratton. Inc.
INDEX WORDS: aortic thrombosis; flbrinolytic therapy; streptokinase; umbilical artery catheter.
z / • R T I C THROMBOSIS in the small premature infant is a catastrophic event, with few intact
survivors reported, la This problem is becoming more common because of the increasing ability of neona- tologists to successfully manage the very-low-birth- weight premature infant. The severe pulmonary disease commonly seen in these patients mandates maintaining umbilical artery catheters in place for extended periods of time. Most of these catheters eventually become a nidus for an attached intra-aortic thrombus, the great majority of which remain asymp- tomatic and eventually lyse. 4'5 However, a small per- centage of these thrombi will enlarge to produce symptoms of arterial occlusion, usually with disastrous results. The smaller the size of the infant, the smaller the size of the thrombus needed to produce symptoms. Therapy must be instituted promptly before irrevers- ible gangrenous changes of the extremities or viscera develop. Minimal physiologic reserve and small size make these patients poor candidates for surgical aortic thrombectomy. The risk of intraventricular hemor- rhage makes anticoagulant therapy risky.
From the Divisions of Pediatric Surgery, Neonatology, and Pediatric Radiology, Kaiser Permanente Medical Center, Los Angeles.
Presented at the 19th Annual Meeting of the American Pediatric Surgical Association, Tucson, Arizona, May 11-14, 1988.
Address reprint requests to Harry Applebaum, MD, Division of Pediatric Surgery, Kaiser Permanente Medical Center, 1526 N Edgemont St, Los Angeles, CA 90027.
�9 1988 by Grune & Stratton, Inc. 0022-3468/88/2312-0023503.00/0
In our initial patients, intravenous (IV) heparin therapy instituted after the development of ischemic changes was unsuccessful in producing resolution or stabilization of the symptoms. Thrombolytic therapy was then evaluated as a more useful alternative, pro- gressing through use of IV streptokinase to a successful protocol using low-dose streptokinase infused directly into the clot via the umbilical artery catheter.
MATERIALS AND METHODS
During the M-month period from October 1985 to April 1988, nine very-low-birthweight (range, 540 g to 1,980 g; mean, 891 g) premature infants were diagnosed as having aortoiliac thrombosis. Symptoms prompting investigation included cyanotic discoloration of the toes ("catheter toes"); cold, blue, pulseless extremities; patchy gangrene of the skin; gastrointestinal bleeding; sudden onset of hypertension; and necrotizing enterocolitis.
Doppler flow studies were used for initial diagnostic screening. During the study aortography became the favored definitive diag- nostic modality, supplanting ultrasonography and technetium radio- nucleide flow studies. Aortograms were performed in the angiogra- phy suite using an injection of dilute contrast solution (Conray 30, Mallinckrodt, Inc, St Louis; 1:1 dilution with normal saline, 1 cc/kg) directly into the umbilical artery catheter. A cranial sonogram was obtained before the infusion to document the absence of recent intraventricular hemorrhage.
The patients were divided into three sequential treatment groups (Table 1), reflecting the evolution of an effective protocol. Group 1 included two patients who received IV heparin therapy instituted after the development of gangrenous changes. IV heparin was infused at a rate of 15 to 20 units/kg/h. Monitoring of heparin time was performed every six hours. Group 2 included the subsequent two patients who received IV heparin immediately following onset of early ischemic symptoms. When this was unsuccessful in arresting progression to gangrenous changes, IV streptokinase therapy was instituted. A loading dose of 2,500 U/kg was administered, followed by maintenance dosage of 1,000 U/kg/h. Group 3 included the most recent five patients. These were treated by infusion of low-dose streptokinase through the umbilical artery catheter directly into the thrombus at a rate of 50 U/kg/h for a period of 36 hours. Once symptoms had resolved and the infusion was completed, the catheter was removed. No further anticoagulation was used. All patients were monitored with prothrombin time (PT), partial thromboplastin time (PTT), fibrin split products, and fibrinogen levels. During heparin therapy the PTT was maintained at a level approximately twice the normal value.
RESULTS
Both patients in group 1 who received only heparin therapy died with progression of ischemic symptoms. One of the two patients in group 2 survived after the level of gangrene stabilized following institution of IV
1198 Journal of Pediatric Surgery, Vo123, No 12 (December), 1988: pp 1198-1200

THROMBOLYTIC THERAPY OF AORTIC THROMBOSIS
Table1. ClinmalFindings, Treetment, and Results in Nine Low Birth WeightPatientsWith Aortic Thrombosis
1199
Gestational Age Patient (wk)/VVeight (g) Problems Symptoms Treatment Results
1 26/720 HMD; BPD; NEC Cyanotic legs, anuria IV heparin Progressive symptoms; sepsis; death
2 36/1,980 Multiple congenital SVC syndrome, gangre- IV heparin Progressive symptoms; anomaly; NEC nous toes sepsis; death
3 26/930 HMD; BPD Patchy gangrene, right IV heparin; IV Right above-the-knee lag streptokinase amputation; alive
4 25/540 HMD; BPD; NEe Cyanotic legs IV heparin; IV Sepsis; death streptokinase
5 29/850 BPD; PDA; sepsis Cyanotic right leg; HTN IA streptokinase Improvement; alive 6 27/810 8PD; PDA; sepsis Decreased femoral IA streptokinsse Improvement; death of
pulses; HTN unrelated causes 7 26/890 NEC; sepsis Cyanotic right leg IA streptokinase Improvement; death of
unrelated causes 8 27/700 BPD; PDA; sepsis Cyanotic left lag IA streptokinase Improvement; alive 9 26/600 Patent ductus; HMD Cool, pulseless right leg IA streptokinase Improvement; alive
Abbreviations: HMD, hyaline membrane disease; BPD, bronchopulmonary dysplasia; NEe, necrotizing enterocolitis; SVC, superior vena cava; HTN, hypertension; IV, intravenous; IA, intra-aortic,
streptokinase, but required a right above-the-knee amputation. The other died with progressive ischemic changes. All five patients in group 3 who received intra-aortic streptokinase therapy improved with respect to occlusive symptoms. Two later died of causes unrelated to aortic thrombosis or thrombolytic thera- py. No recurrence of symptoms was detected in any patient in this group. Parameters measured during intra-arterial streptokinase therapy were mildly abnor- mal, with a slight increase in fibrin split products and decrease in fibrinogen level.
DISCUSSION
Aortoiliac thrombosis has become an increasingly recognized problem in the neonatal intensive care unit because of the markedly improved salvage rate of very-low-birthweight premature infants. Because of a commonly prolonged period of poor respiratory status, there is often a perceived need to maintain an umbili- cal artery catheter in place for extended periods of time, often with infusion of hypertonic solutions. Thus, the risk of development of thrombi large enough to become symptomatic is greatly increased. 6
The problem is frequently underdiagnosed, with early symptoms often wrongly attributed to presum- ably benign causes such as arterial spasm ("catheter toes"). All patients in our study who were initially thought to have arterial spasm were later proven to harbor large aortic thrombi. Later signs of developing thrombi were those common to any vascular throm- botic occlusion, starting with signs of poor perfusion, with progression to cold cyanotic pulseless extremities, and sometimes to a level of demarcation across the upper abdomen. In other infants, IV infiltration sites progressed to small areas of patchy gangrene with
intervening viable tissue before aortic thrombosis was suspected. It is likely that ischemic tissues contributed to the formation of these gangrenous changes in what would otherwise have been an easily healed process. The sudden onset of renovascular hypertension was the first sign of aortic thrombosis in one patient. The hypertension resolved soon after the institution of intra-aortic streptokinase therapy.
Although cause and effect relationship is unclear, necrotizing enterocolitis developed in several of these patients, often as a terminal event. The visceral ischemia caused by an aortic thrombus may have led to
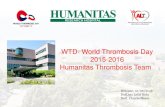
Fig 1. Abdominal ultrasound demonstrating aortic thrombus associated with umbilical artery catheter. 1, aorta; 2, umbilical artery catheter; 3. thrombus.

1200 RICHARDSON ET AL
distal mesenteric vascular thrombosis, or a low flow state due to sepsis may have independently caused these same effects. Fibrinolytic therapy could have an important future role in preventing or halting pro- gression of early, nonhemorrhagic necrotizing entero- colitis.
Most cases of aortic thrombosis are readily apparent clinically if a proper index of suspicion is maintained. Once the diagnosis is considered, it is important to leave the umbilical artery catheter in place in order to perform an angiogram and administer fibrinolytic therapy if appropriate. The angiogram must be per- formed and treatment instituted before irreversible gangrenous changes occur. In our study, vascular scans, while reliable, were relatively difficult to pro- cure and were lengthy procedures which had to be performed in the nuclear medicine department. These logistical problems relegated this procedure to a sec- ondary role. Aortic ultrasound (Fig 1), reported to be extremely reliable in full-term infants, proved extremely difficult to interpret in these very small infants.
Surgical treatment of aortoiliac thrombosis has been associated with technical difficulties and poor outcome even in much larger infants. 7 The systemic hepariniza- tion that is required after thrombectomy is performed puts the patients at risk for bleeding complications. The small size and extreme prematurity of the patient
population now most commonly affected would make any major surgical procedure extremely hazardous and unlikely to be effective.
Streptokinase achieves its effect by activating plas- minogen, which is then converted to plasmin. Plasmin causes clot dissolution by direct proteolytic enzyme activity, s In a patient population at risk for intraven- tricular hemorrhage, fibrinolytic therapy has been looked upon with trepidation. The commonly recom- mended dosage of streptokinase has been 70 to 100 U/kg /h . Recently, Pritehard et al 9 experienced suc- cess with low-dose streptokinase in treating arterial and venous thrombosis in older infants. In our five patients treated with intra-aortic streptokinase at the much lower dosage of 50 U/kg /h , no bleeding prob- lems were encountered. It is apparent that when strep- tokinase is infused directly into the thrombus the desired thrombolytic effect of the agent is achievable at a much lower, safer dose than that which is often recommended.
The current emphasis on avoidance of long-term umbilical artery catheters and routine low-dose hepa- rinization of infusate has decreased catheter-related complications. When thrombotic complications do occur, rapid diagnosis and treatment are imperative. Local infusion of low-dose fibrinolytic therapy offers a therapeutic option that is rapid, safe, and effective.
REFERENCES
1. Henry CG, Gutierrez F, Lee JT, et al: Aortic thrombosis presenting as congestive heart failure; an umbilical artery catheter complication. J Pediatr 98:820-822, 1981
2. Tyson JE, De Sa D J, Moore S: Thromboatheromatous compli- cations of umbilical arterial catheterization in the newborn period. Arch Dis Child 51:744, 1976
3. Marsh JL, King W, Fonkalsrud EW, et al: Serious complica- tions after umbilical artery catheterization for neonatal monitoring. Arch Surg 110:1203, 1975
4. Mokrohisky ST, Levine RL, Blumhagen JD, et al: Low positioning of umbilical artery catheters increases associated compli- cations in newborn infants. N Engl J Med 299:561, 1978
5. Neal WA, Reynolds JW, Jarvis CW, et al: Umbilical artery
catheterization: Demonstration of arterial thrombosis by aortogra- phy. Pediatrics 50:6, 1972
6. Alpert J, O'Donnell JA, Parsonnet V, et al: Clinically recog- nized limb ischemia in the neonate after umbilical artery catheteri- zation. Am J Surg 140:413-418, 1980
7. O'Neill JA Jr, Neblett WW, Born ML: Management of major thromboembolic complications of umbilical artery catheters. J Pedi- atr Surg 16:972@78, 1981
8. Kwaan HC: Hematologic aspects of thrombolytic therapy, in Camerota AJ (ed): Thrombolytic Therapy. Philadelphia, Grune & Stratton, 1988, pp 17-28
9. Pritchard SL, Gordon Culham JA, Rogers PC J: Low dose fibrinolytic therapy in infants. Pediatrics 106:594-598, 1985