Effect of prefrontal high frequency repetitive ... · Effect of prefrontal High Frequency...
93
Aus der Klinik für Psychiatrie und Psychotherapie der Universitätsmedizin Göttingen, Georg-August-Universität Göttingen Effect of prefrontal High Frequency repetitive Transcranial Magnetic Stimulation (rTMS) on Psychopathology and Working Memory in Patients with Schizophrenia and Healthy Controls Inaugural - Dissertation zur Erlangung des Grades eines Doktors der Naturwissenschaften in der Fakultät für Psychologie der RUHR - UNIVERSITÄT BOCHUM vorgelegt von: Dipl.-Psych. Birgit Guse
-
Upload
hoanghuong -
Category
Documents
-
view
227 -
download
0
Transcript of Effect of prefrontal high frequency repetitive ... · Effect of prefrontal High Frequency...

Aus der Klinik für Psychiatrie und Psychotherapie
der Universitätsmedizin Göttingen,
Georg-August-Universität Göttingen
Effect of prefrontal High Frequency repetitive Transcranial
Magnetic Stimulation (rTMS) on Psychopathology and Working
Memory in Patients with Schizophrenia and Healthy Controls
Inaugural - Dissertation
zur
Erlangung des Grades eines Doktors der Naturwissenschaften
in der
Fakultät für Psychologie
der
RUHR - UNIVERSITÄT BOCHUM
vorgelegt von:
Dipl.-Psych. Birgit Guse

Gedruckt mit Genehmigung der Fakultät für Psychologie der
RUHR-UNIVERSITÄT BOCHUM
Referent: Prof. Dr. Boris Suchan
Korreferent: PD Dr. Thomas Wobrock
Tag der mündlichen Prüfung: 18.06.2013

Contents
1 Introduction …………………………………………………………… 3
1.1 Schizophrenia ………………………………………………………………….. 3
1.1.1 Negative Symptoms and Cognition ………………………………...……… 5
1.1.2 Working Memory Deficits and Cerebral Correlates ………………......…… 6
1.2 Transcranial Magnetic Stimulation ……………………………………….….. 10
1.2.1 Physical and Physiological Principles ……………………………………. 10
1.2.2 Stimulation Parameters of Repetitive Transcranial Magnetic Stimulation . 11
1.2.3 Therapeutic Applications of rTMS ……………………………………….. 13
1.2.3.1 rTMS Effect on Psychopathology ………...………………………….. 14
1.2.3.2 rTMS Effect on Cognition ……………………………………………. 16
1.3 Functional Magnetic Resonance Imaging ………...………………………….. 18
1.3.1 Physical and Physiological Principles ……………………………………. 18
1.3.2 Imaging rTMS Effects ……………………………………………………. 20
1.4 Summary and Unresolved Issues ……………………………………………... 21
2 Publications ………………...………………………………………… 24
2.1 Repetitive transcranial magnetic stimulation for the treatment of negative
symptoms in residual schizophrenia: rationale and design of a sham-controlled,
randomized multicentre study ……...……………………………………….……. 25
2.2 Cognitive effects of high frequency repetitive transcranial magnetic stimulation
(rTMS) – a systematic review ………...………………………………………….. 35
2.3 The effect of long-term high frequency repetitive transcranial magnetic
stimulation on working memory in schizophrenia and healthy controls – a
randomized placebo-controlled, double-blind fMRI study ………………………. 54
3 Discussion …………………………………………………………...... 63
3.1 Does rTMS improve Psychopathology in Patients with Schizophrenia? …….. 64
3.2 Does rTMS influence Cognition? …………………………………………….. 66
3.3 Does rTMS improve WM Dysfunction in Patients with Schizophrenia? Does
rTMS alter Brain Activation within the WM Network? ………………..………… 67
3.4 General Limitations ………………...………………………………………… 71
- 1 -

3.5 Conclusion and Future Perspective ………………………..……………….… 74
4 References …………..………………………………………….…….. 75
Abbreviations ……………………………………………………………………….… 87
Acknowledgements ………………………...………………………………………… 88
Curriculum Vitae ……………...……………………………………………………… 89
List of Publications …...………………………………………………………………. 90
- 2 -

1. Introduction
1.1 Schizophrenia
According to the diagnostic guidelines of the International Statistical Classification
of Diseases and Related Health Problems (ICD-10) of the World Health Organization
(WHO) different symptoms can be clustered for the diagnosis of schizophrenia (for
details see the box below). The normal requirement for diagnosis is that a minimum of
one clear symptom (and usually two or more if less clear-cut) belonging to one of the
groups listed from (a) to (d) below, or symptoms from at least two of the groups from
(e) to (h), should clearly be present for most of the time during a period of 1 month or
more.
The ICD-10 encodes distinct subtypes of schizophrenia F20.0-F20.9, whereas the
paranoid subtype (F20.0) is most prominent with a prevalence of about 65%. The
clinical picture is dominated by relatively stable, often paranoid, delusions, usually
accompanied by hallucinations, particularly of the auditory variety, and perceptual
disturbances. These symptoms are commonly defined as positive or productive
symptoms as they occur in addition to “normal” behaviour (see box below, PANSS-
symptoms). Conversely, another symptom group is defined as negative symptoms and
encompasses clear behavioural deficits such as apathy, blunted affect or social and
emotional withdrawal (see box below, PANSS-symptoms; for details see chapter 1.1.1).
The course of paranoid schizophrenia may be episodic, with partial or complete
remissions, or chronic. In chronic cases, the florid symptoms persist over years and it is
difficult to distinguish discrete episodes.
A clear distinction of symptom clusters is essential for pharmacotherapeutic
intervention since positive symptoms may be associated with a hyper-aroused state that
usually responds well to antipsychotic medications, whereas negative symptoms consist
of deficit features that may represent a more stable component of the disease and are
often characterized by neuroleptic resistance (e.g. Kay et al., 1987). Depending on the
definition of treatment-resistant schizophrenia, about 10–30 % of patients have little or
no response to antipsychotic medication, and up to an additional 30% of patients have
only partial responses to treatment (Falkai et al. 2005, 2006). Even if a patient’s positive
symptoms remit with antipsychotic agents, persisting negative symptoms or cognitive
- 3 -

impairment often determine an unfavourable course of the illness leading to a reduction
of psychosocial functioning and quality of life. Second generation antipsychotics
(SGAs) provide some benefits in improving negative symptoms compared to
conventional neuroleptic treatment but there is still a considerable portion of patients
suffering from such symptoms (Falkai et al. 2005, 2006). Despite this clinical relevance
there are only few treatment strategies available. Therefore, insights into novel
techniques potentially modulating brain functions are promising for therapeutic
purposes.
ICD-10: Diagnostic Guidelines for Schizopnrenia, Symptom Clusters. (a) thought echo, thought insertion or withdrawal, and thought broadcasting; (b) delusions of control, influence, or passivity, clearly referred to body or limb movements or specific thoughts, actions, or sensations; delusional perception; (c) hallucinatory voices giving a running commentary on the patient's behaviour, or discussing the patient among themselves, or other types of hallucinatory voices coming from some part of the body; (d) persistent delusions of other kinds that are culturally inappropriate and completely impossible, such as religious or political identity, or superhuman powers and abilities (e.g. being able to control the weather, or being in communication with aliens from another world); (e) persistent hallucinations in any modality, when accompanied either by fleeting or half-formed delusions without clear affective content, or by persistent over-valued ideas, or when occurring every day for weeks or months on end; (f) breaks or interpolations in the train of thought, resulting in incoherence or irrelevant speech, or neologisms; (g) catatonic behaviour, such as excitement, posturing, or waxy flexibility, negativism, mutism, and stupor; (h) "negative" symptoms such as marked apathy, paucity of speech, and blunting or incongruity of emotional responses, usually resulting in social withdrawal and lowering of social performance; it must be clear that these are not due to depression or to neuroleptic medication; (i) a significant and consistent change in the overall quality of some aspects of personal behaviour, manifest as loss of interest, aimlessness, idleness, a self-absorbed attitude, and social withdrawal.
Positive and Negative Symptoms according to the Positive and Negative Syndrome Scale for Schizophrenia (PANSS, Kay et al., 1987): Positive Symptoms: Negative Symptoms:
Blunted affect Delusions Emotional withdrawal Conceptual disorganization Poor rapport Hallucinatory behaviour Passive/ apathic social withdrawal Excitement Difficulty in abstract thinking Grandiosity Lack of spontaneity Suspiciousness/ persecution Stereotyped thinking Hostility
- 4 -

1.1.1 Negative Symptoms and Cognition
According to the Positive and Negative Syndrome Scale (PANSS), developed and
standardized for the typological and dimensional assessment of schizophrenic
phenomena (Kay et al., 1987), the negative symptoms in schizophrenia are determined
by 7 different deficit features. (1.) Blunted affect describes the diminished emotional
responsiveness that is characterized by a reduction in facial expression, affective
modulation and communicative gestures. (2.) Emotional withdrawal is determined by
the lack of interest in, involvement with, and affective commitment to life’s events. (3.)
Poor rapport defines the lack of interpersonal empathy, the openness in conversation,
characterized by distancing and reduced verbal and non-verbal communication. (4.)
Social withdrawal describes a diminished interest and initiative in social interactions
due to passivity, apathy or avolition leading to neglect of daily activities. (5.) Difficulty
in abstract thinking implies the impairment in the use of the abstract-symbolic mode of
thinking, as evidenced by difficulty in classification, forming generalizations and
problem solving. (6.) Lack of spontaneity and flow of conversation describe the
reduction in the normal flow of communication associated with apathy, avolition,
defensiveness and cognitive deficit. This is manifested by diminished fluidity and
productivity of the verbal-interactional process. The last deficit feature describes (7.)
stereotyped thinking, the decreased fluidity, spontaneity and flexibility of thinking. That
is, rigid, repetitious or barren thought content. Taken together, the negative syndrome is
characterized by a range of interpersonal or social deficits as well as affective emotional
impairment that is connected to cognitive restraint.
A quantitative review of Heinrichs & Zakzanis (1998) indicates a reliable
neurocognitive deficit in schizophrenia compared to healthy controls. In the reviewed
literature, global verbal and nonverbal memory, attention and word fluency tests yielded
the highest proportion of significant test score differences between patients and
controls. More recently, Reichenberg (2010) reviewed meta-analytic studies in
consideration of neuropsychological functioning in schizophrenia. Results indicate
cognitive impairment in a broad range of domains reflecting a substantial impairment in
schizophrenia (Figure 1, Reichenberg et al., 2010). Importantly, there is some
consistency in documenting an association between negative symptoms and the severity
of cognitive impairment, particularly in executive functions (Green et al., 2000; Henry
- 5 -

& Crawford, 2005; Johnson-Selfridge & Zalewski, 2001; for a review see Reichenberg
et al. 2010). Conversely, relative inconsistency is reported with regard to the association
of positive symptoms and the severity of cognitive deficits (Aleman et al., 1999;
Johnson-Selfridge & Zalewski, 2001; for a review see Reichenberg et al., 2010).
Figure 1: Neuropsychological performance profile of schizophrenia. Summary of meta-analytic studies presented in effect size units (in Reichenberg et al., 2010).
Lesioning and neuroimaging studies have linked schizophrenia negative symptoms
to dysfunction of the prefrontal cortex (PFC), the limbic system, and the basal ganglia
(Goff & Evins 1998; Winterer & Weinberger, 2004). Beyond general attention deficits,
one of the core features of schizophrenia is working memory (WM) dysfunction as part
of a disturbed central executive system (Cannon et al., 2005; Silver et al., 2003), which
is the main objective of the third manuscript of the thesis (see 2.3).
1.1.2 Working Memory Deficits and Cerebral Correlates
Working memory implies the short-term retention of information that is no longer
accessible in the environment and the manipulation and processing of this information
for guiding behaviour (D’Esposito et al., 2000). Baddeley (1986, 2000) advanced the
- 6 -

approach that WM is composed of a central executive supervising three so-called slave
components: the visuo-spatial sketchpad, the phonological loop and the episodic buffer.
The phonological loop is supposed to be essential for speech or language perception/
comprehension and is involved in the temporary maintenance of verbal information via
subvocal rehearsal. The counterpart is built by the visuo-spatial sketchpad, which
temporarily sustains incoming information as visual images. The third system, the
episodic buffer, describes an unspecific multimodal storage with limited capacity that
integrates information from different sources as “chunks”. The central executive plays a
crucial role in the selection of appropriate control processes and their supervision as
well as flexible modulation in a changing environment. Therefore, a dynamic up- and
down regulation of neurotransmitter subsystems is necessary for higher order cognitive
processes. In this context, it is suggested that prospective and retrospective information
are needed for fast updating and modulation during WM performance. Regarding this
proposed model, working memory is an important concept for understanding
mechanisms of complex cognitive functioning such as planning, reasoning, speech
comprehension or decision-making (Funahashi, 2007).
Besides these abstract constructs, recent studies emphasized process-based models
using functional imaging techniques to investigate the corresponding cerebral
correlates. Over the past few decades, studies have provided a substantial body of
evidence that supports a crucial role for bilateral prefrontal, anterior cingulate and
parietal regions in mediating WM performance (e.g. Rypma et al., 2002; for review
Owen et al., 2005 or Smith and Jonides, 1999). The middle frontal gyrus (Brodmann
area (BA) 9/46) is described to be mainly activated during the manipulation and
executive monitoring of incoming stimuli (e.g. Smith et al., 1996; Menon et al., 2001),
whereas the inferior frontal gyrus (BA 44) and parts of the superior frontal gyrus
(premotor and supplementary motor area, BA 6) as well as parietal association cortices
are likely to be most sensitive for maintenance processes (e.g. Paulesu et al, 1993).
These results are in line with functional and cytoarchitectural studies pointing to a
tightly knit and specific network of frontal-mediated working memory functions (for
review Owen et al., 2005; Petrides, 2005; Wager et al., 2003). Overall, the prefrontal
cortex, especially the dorsolateral prefrontal part (DLPFC, BA 9/46), plays an important
role in WM operations. Results from functional imaging studies on schizophrenia
patients are heterogeneous as some report decreased prefrontal activation (so called
- 7 -

hypofrontality) and others increased activation (hyperfrontality) during cognitive tasks
that affect prefrontal regions (e.g. Callicott et al., 2000; Manoach et al., 1999; Volz et
al., 1999). Callicott et al. (2003) provided a model of an inverted-U-shaped curve of the
blood-oxygen-level-dependent (BOLD-) response in the DLPFC during a WM task with
parametric increasing demand (Figure 2A, Callicott et al., 2003).
A
B
Figure 2: Assumed inverted U-curves of (A) the relationship of BOLD-response in the DLPFC and increasing WM load in SZ patients (left) and HC (right) (in Callicott et al., 2003) and of (B) the relationship of dopamine transmission and working memory performance (in Williams & Castner, 2006). HC = healthy controls, SZ = patients with schizophrenia.
They supposed that patients operate on a distinct inverted U-curve that is assumed
to be left-shifted compared to healthy controls. A principle consideration in this study
was that patients’ WM capacity may be exceeded earlier compared to controls, leading
to a relative decrease of DLPFC activations at higher loads. The opposite was assumed
for lower demands, at which patients were supposed to exhibit relatively increased
DLPFC activations, possibly reflecting greater exertion at lower level. In place of the
- 8 -
controversial discussion of DLPFC dysfunction and the assumption of general
hypofrontality, an inefficient dynamic modulation of DLPFC activity during WM
operations has been supposed in schizophrenia, leading in general to poorer task
performance compared to healthy controls (Callicott et al., 2000 & 2003; Johnson et al.,
2005; Perlstein et al., 2001). Overall, results indicate different parts of the brain to be
hypo- and hyperfrontal depending on task demand and individual operating abilities.
In this context it is of importance that an imbalance in dopamine (DA) signalling
within the fronto-striatal circuit plays a crucial role in schizophrenia symptoms and
working memory deficits (Abi-Dargham, 2004; Menon et al., 2001; Williams &
Castner, 2006). Dopamine transmission in the DLPFC and the integrity of working
memory have been described to follow a similar inverted U-curve as it has been
provided for the BOLD-response mentioned above and depicted in Figure 2A (Herold
et al., 2008; Williams & Castner, 2006; Figure 2B, Williams & Castner, 2006). These
effects can be provoked by administration of dopamine DA1 receptor agonists or
antagonists leading to different working memory performances, respectively. An
optimal DA level is essential for WM processing, whereas hypo- or hyperdopaminergic
states result in WM impairment. This is the case for example in aging, acute stress or
different neuropsychiatric diseases such as schizophrenia (Arnsten et al., 1998; Herold
et al., 2008; Williams & Castner, 2006). In a study using Positron-Emission-
Tomography (PET) Okubo et al. (1997) found decreased prefrontal dopamine D1
receptors in schizophrenic patients that were related to the severity of negative
symptoms and to poor performance in the Wisconsin Card Sorting Test (WCST, a test
for executive functions, Grant & Berg et al., 1993). This is important against the
background that antipsychotic medication has not been shown to influence negative
symptoms or cognition to a sufficient extent. It seems obvious that these features may
underlie more stable mechanisms which can be poorly targeted with common agents.
Reduced receptor density is a structural deficit possibly requiring more than a transient
focal up-or down-regulation of neurotransmission. Transcranial magnetic stimulation
(TMS) for example has been demonstrated to act otherwise on neural systems than
antipsychotic medication (see 1.2). However, its applicability and impact for therapeutic
standard use is not known thoroughly. The next chapter provides an overview of the
principles of this technique with regard to clinical applications.
- 9 -

1.2 Transcranial Magnetic Stimulation
Transcranial magnetic stimulation was originally introduced by Barker et al. (1985)
as a non-invasive tool for the investigation of the motor cortex. TMS is based on an
electromagnetic coil applied to the scalp producing an intense, localized magnetic field
which either excites or inhibits a focal cortical area. Repetitive TMS uses alternating
magnetic fields to induce electric currents in the cortical tissue affecting electric
conducting structures (Burt et al., 2002). Today TMS has emerged as an important
technique in several areas of neuroscience. Originally contemplated as a method to
measure the responsiveness and conduction speed of neurons and synapses in the brain
and spinal cord, TMS now plays a crucial role in changing the activity of cerebral
neurons and thus of specific functions (e.g. Speer et al., 2000). TMS has further become
an essential adjunct to brain imaging or mapping methods described below.
1.2.1 Physical and Physiological Principles
The physical principle of TMS is electromagnetic induction due to Faraday’s law
(1830). A capacitor generates short intense discharges, which induce a changing
magnetic field of 2-2,5 Tesla in the TMS coil leading to an electric field in the adjacent
conductive cortical tissue. The magnetic field traverses intermediate structures (e.g.
scalp, skull, liquor) with quite minimal impedance, focally depolarizes neurons and
generates action potentials, provided amplitude, duration and direction are appropriate
(Rothwell et al., 1999; Siebner et al., 2003). Thereby, cortical axons are the electric
conducting structures. The field strength decreases proportional to the square of the
distance. Therefore, only cortical structures and no deeper subcortical regions can be
directly affected with TMS. The penetration depth for an effective neuronal excitation is
about 1,5-2 cm (Epstein et al., 1990) if stimulated with a figure-of-eight shaped coil
allowing a circumscribed stimulation of the brain (Cohen et al., 1990). Current direction
can be varied by coil shape (e.g. circular or 8-coil) and orientation (e.g. posterior-
anterior, lateral-medial) (Figure 3A, Maccabee & Amassian, 2008). In a standard
figure-8 coil two electric field loops are induced which superimpose maximally under
the long axis of the junction (Ueno et al., 1988). Given that the coil is oriented
- 10 -

tangentially to the skull, the induced magnetic field deflects perpendicular to the axis of
the coil leading to an orthogonal current flow parallel to the coil plane. The isopotential
lines of the induced electric field form an oval whose long axis is parallel to the
direction of current flow at the coil junction (Epstein, 2008; Sandbrink, 2008; Figure
3B, Eptein, 2008).
A B
Figure 3A, B: (A) Current direction (in Maccabee & Amassian, 2008) and (B) the relation to coil orientation and magnetic field (in Epstein, 2008).
TMS thus preferentially affects structures that are organized horizontally in the
cortical surface, e.g. axons of intra-cortical neurons. Within the homogeneous electric
field (along the cortical surface) only axons with a curved path are affected providing an
outwards directed depolarizing membrane current, that generates action potentials if
strength and duration are sufficient (see 1.2.2). Vertical neuron bundles are then excited
secondarily via trans-synaptic transmission (Sandbrink, 2008). Overall, focal TMS is
able to affect cortico-cortical or cortico-subcortical axons, but the specific outcome
depends on the stimulation protocol selected, on the area stimulated and on inter-
individual tissue properties.
1.2.2 Stimulation Parameters of Repetitive Transcranial Magnetic Stimulation
TMS can be applied in different modes dependent on the individual scientific
hypothesis. For therapeutic purposes TMS is commonly administered in an alternating
mode consisting of continuous series of stimuli with more than two single pulses of
constant repetition rate (for details of therapeutic applications see 1.2.3). A slow
repetition rate is determined ~1 Hz (low-frequency) and a fast repetition rate is >5 Hz
- 11 -

up to 50 Hz (high-frequency). The repetition rate is essential according to the intention
of inhibition or excitation of a particular cerebral region. Generally, low frequency
stimulation (≤1 Hz) is likely to cause temporal inhibition of neuronal firing, whereas
high frequency (>5 Hz) repetitive TMS (rTMS) for the most part evokes neuronal
depolarization leading to transient neuronal facilitation or enhancement (Fitzgerald et
al., 2006; Haraldsson et al., 2004; Klimesch et al., 2003). Some research has provided
evidence for an inverse relationship between regional cerebral blood flow (rCBF) and
low-frequency rTMS (in the sense of an excitatory effect of slow rTMS) when high
stimulation intensities or intensities at motor threshold are applied (Li et al., 2004; Speer
et al., 2003).
The resting motor threshold (RMT) is commonly used as reference to set the
stimulation intensity. The RMT is defined as the lowest intensity that produces a motor
evoked potential of <50µV in the relaxed first-dorsal interosseus muscle (FDI) in at
least five of ten trials. Therefore, a standard figure-of-eight coil is applied to the hand
area of the motor cortex and motor-evoked potentials are recorded via
electromyography (EMG) surface electrodes from the (FDI) (Rossini et al., 1994;
Rothwell et al., 1999). The stimulation can thus be conducted to e.g. 90, 100 or 110% of
this threshold. The standard rTMS protocol settings further include the definition of
number and duration of TMS trains (repetitive volleys) as well as the resting time
between trains, called inter-train-interval.
For exact coil placement, today, many researcher groups revert to neuro-navigated
targeting, especially when the outcome depends on the accuracy of the target area, e.g.
in case of specific functional interruption. In clinical trials the seed region is often
targeted using the electrode positions of the 10-20 EEG system (Figures 4A, B). The
nasion-to-inion axis (front-back distance) and the pre-auricular axis (right-left distance),
both crossing the vertex, are used as reference system to identify the target region. The
position of the coil centre can then be located at the electrode position (Fitzgerald et al.,
2009; Rusjan et al., 2010).
- 12 -

Figure 4A, B: 10-20 EEG-System coordinates for the identification of a target region1.
1.2.3 Therapeutic Applications of rTMS
Focal non-invasive stimulation of the brain represents a previously unprecedented
therapeutic potential in psychiatry and neurology due to the fact that systematically
administered pharmacological agents may be ineffective or cause treatment-interfering
side effects in many patients. TMS avoids systemic side effects and affects the brain
with a temporal and spatial specificity which currently cannot be achieved
pharmacologically or via methods such as electroconvulsive therapy (Lisanby, 2008).
The exact mechanisms by which focal intermittent brain stimulation could evoke lasting
effects in illnesses via distributed neuronal networks remain unclear. One possibility is
based on the demonstration that some established TMS protocols, which administer
repetitive pulses, have the capacity to induce plasticity shifts of the stimulated and
interconnected brain areas (Esser et al., 2006; for review see Reis et al., 2008). Plasticity
may be broadly defined as an activity-dependent enduring change in neural structure
and function, e.g. in synaptic efficacy (Vorel & Lisanby, 2008). Long-term potentiation
(LTP) is the most widely studied synaptic plasticity process and refers to enduring
strengthening of synapses due to ‘Hebbian’ characteristics (Hebb, 1949; Vorel &
Lisanby, 2008). Typically, synaptic strength is measured as a sum of excitatory
postsynaptic potentials (EPSPs) in response to electrical stimulation. This requires
repeated electrical stimulation of a pre-synaptic neuron as evidenced by an increase in
1 image source: http://www.bci2000.org/wiki/index.php/User_Tutorial:EEG_Measurement_Setup
- 13 -

EPSP. Beyond the hippocampus, LTP has been demonstrated in other brain areas such
as the prefrontal cortex (Floresco & Grace, 2003; Maroun & Richter-Levin, 2003; Vorel
& Lisanby, 2008). However, there is no clear knowledge about whether repetitive
transcranial magnetic stimulation would have the potential to trigger these processes in
such a way that would be essential for a beneficial clinical outcome. Principally, these
considerations provide the possibility of both cognitive and clinical improvement.
1.2.3.1 rTMS Effects on Psychopathology
Regarding the impact of rTMS on psychopathology, pilot studies have suggested a
putative application of repetitive TMS as a therapeutic tool, based on the idea of
targeted stimulation of dysfunctional cortico-subcortical circuits involved in the
pathophysiology (George et al. 2000; Lisanby et al. 2000; Wassermann and Lisanby
2001; Hoffman and Cavus 2002). During the last few decades, a prevalent issue has
been the application in major depression (for review Burt et al, 2002, Padberg et al.,
2009; Fitzgerald et al., 2006), characterized by potential reversible functional deviations
in limbic or para-limbic circuits, especially monoaminergic transmitter systems and
specific molecular mediating systems (Bajbouj, 2007; Padberg et al., 2007). According
to long-time research on this topic the target region in antidepressive rTMS
interventions is commonly the DLPFC, at which the left DLPFC is mainly stimulated at
high frequencies (5-20 Hz) or the right DLPFC at low frequencies (~1 Hz). However,
the clinical outcome does not reach the effect size of electroconvulsive therapy (ECT) in
medication resistant patients (review Padberg & George, 2009).
Similar rTMS protocols were used in studies which investigated the impact of
rTMS on negative symptoms in schizophrenic patients (Table 1). Based on encouraging
results of first case series (Cohen et al., 1999; Jandl et al., 2004; Sachdev et al., 2005;
Rollnik et al., 2001), some randomised double-blind sham- controlled studies have been
conducted in the field (Table 1). The first one applied low-frequency rTMS over the
right prefrontal cortex at 110 % motor threshold (total stimuli 1200) in 35 patients with
schizophrenic or schizoaffective psychoses. There were no significant group differences
except for the use of mood stabilizers in four participants of the active group (Klein et
al. 1999). Studies using high-frequency rTMS (10 Hz and 20 Hz) over the left DLPFC
revealed more success. In a cross-over study, a significant improvement compared to
- 14 -

sham in the average Brief Psychiatric Rating Scale (BPRS, Overall & Gorham, 1962)
score in the active stimulation group after application of a total of ten 20 Hz rTMS
adjuvant treatments with prefrontal stimulation of the dominant hemisphere at 80 % of
the motor threshold (total stimuli 8000) in 12 schizophrenia patients was reported
(Rollnik et al. 2000, Huber et al. 2003). The authors did not differentiate between
positive or negative schizophrenic symptoms. Concerning other symptoms such as
depression or anxiety, which were also recorded separately, no differences could be
detected due to the stimulation. Two other studies using 20 Hz rTMS revealed no
significant improvement of negative symptoms in the active group compared to sham
group (Nahas et al. 1999, Novak et al. 2006). In contrast, studies delivering 10 Hz
rTMS, applied over the left DLPFC (10 sessions in 2 weeks, 110 % motor threshold,
total stimuli 10000) demonstrated significant superiority of the active stimulation
compared to sham in the improvement of the negative score of the Positive and
Negative Syndrome Scale (PANSS, Kay et al., 1986) (Hajak et al. 2004, Cordes et al.
2005). In a double-blind cross-over dose finding study on 27 schizophrenia patients
with predominantly negative symptoms, a significantly higher therapeutic effect was
shown at an alpha EEG peak frequency determined for each individual subject at 8 -13
Hz rTMS over the dorsolateral prefrontal cortex at 80 % motor threshold compared to
treatment at 3 or 20 Hz and sham as controls (Jin et al. 2006). The above mentioned
studies represent the data status until implementation of our trial (Table 1). However,
more recent studies support these results (e.g. Prikryl et al., 2007, Goyal et al., 2007,
Fitzgerald et al., 2008; Schneider et al., 2008; for a meta-analysis see Slotema et al.,
2010).
- 15 -

Table 1: Randomised double-blind sham-controlled studies (including cross-over trials) in the treatment of negative symptoms until 2006.
Study N Location Frequency (Hz) MT (%) Stimuli (N) Significance (p)
Klein 1999 31 RPFC 1 110 1200 n.s.
Nahas 1999 8 LDLPFC 20 100 1600 n.s.
Rollnik 2000 12 DLPFC 20 80 8000 BPRS p = 0.015
Hajak 2004 20 LDLPFC 10 110 10000 PANSS negative subscale p = 0.046
Holi 2004 22 LDLPFC 10 100 10000 n.s.
Jin 2006 27 bilateral DLPFC
3, 10*, 20 80 1200, 4000, 8000
PANSS negative subscale p = 0.007 at 10* Hz
Cordes 2005 25 LDLPFC 10 110 10000 PANSS negative subscale p= 0.046
Novak 2006 16 LDLPFC 20 90 20000 n.s.
Legend: DLPFC: Dorsolateral Prefrontal Cortex, Hz: Hertz, LDLPFC: Left Dorsolateral Prefrontal Cortex, PANSS: Positive and Negative Syndrome Scale, RPFC: Right prefrontal cortex, MT: motor threshold, N.S.: Not significant, *: Individualized Alpha Frequency (8 – 13 Hz).
In conclusion, one can state that the data are convincing that the paradigm of 10 Hz
rTMS applied over the left DLFPC is the most promising design so far for the clinical
use in schizophrenia negative symptoms. However, results remain limited due to small
sample sizes, the lack of control groups or other methodological limitations. Further, the
underlying neurophysiological mechanisms are outstanding and have to be
systematically investigated using imaging or neurophysiological methods such as
functional magnetic resonance imaging (fMRI) or electroencephalography (EEG). Our
first manuscript, outlined in 2.1, addresses the influence of long-term high frequency
rTMS on negative symptoms and general psychopathology using a randomized double-
blind, placebo controlled parallel design.
1.2.3.2 rTMS Effects on Cognition
Let’s consider the impact of rTMS on cognition. Until our trial conception in
2007/2008, most of the results emerged from single session studies measuring the direct
after-effect of rTMS on cognitive processing. Evers et al. (2001) performed a study on
the impact of a single 20 Hz rTMS session on cognitive processing in 14 healthy
subjects as measured by visually evoked event-related potentials (ERP) and mean
choice reaction time. rTMS was applied over the left and right DLPFC consecutively
- 16 -

(about F3/ F4 according to the international 10-20-EEG system). Data were compared
to sham and to 1 Hz single TMS (a continuous series of stimuli). P3 latencies and
reaction time were significantly decreased after 20 Hz real rTMS over the left side, but
not for the right side. 1 Hz single TMS did not have any impact on ERP components.
The authors concluded that rTMS has a fascilitating effect on cognitive processing,
proven by objective neurophysiological measures (Evers et al., 2001). Boroojerdi et al.
(2001) aimed to investigate the role of the left DLPFC in analogic reasoning. They
demonstrated that rTMS over the left DLPFC (compared with right DLPFC, left motor
cortex and sham stimulation) in healthy subjects led to a significant decrease in
response times in the analogy condition without affecting accuracy. The results
underline the relevance of the left DLPFC in analogic reasoning but also indicate that
rTMS applied to this region can speed up solution time (Boroojerdi et al. (2001).
Töpper et al. (1998) and Mottaghy et al. (1999) could show an enhancing cognitive
effect of TMS over Wernicke’s area. Picture naming latencies were shortened in healthy
subjects when TMS was delivered to Wernicke’s area. Töpper et al. (1998) performed
suprathreshold TMS with varying inter-stimulus-intervals, Mottaghy et al. (1999)
applied 20 Hz high-frequency rTMS. Klimesch et al. (2003), could show that rTMS at
individual upper alpha frequency (IAF+1Hz) delivered mesial frontal (Fz) and the right
parietal (P6) cortex in healthy volunteers can enhance the performance in a mental
rotation task. These and many other results on this topic confirm the modulating effect
of one single session of high-frequency rTMS on cognitive processing. However,
neuronal enhancement with consequent cognitive improvement remained transient as
effects disappeared directly after the session. For therapeutic purposes extended effects
would be promising. Our review article (outlined in chapter 2.2) explicitly addresses
cognitive effects following long-term (repeated session) high-frequency rTMS
treatment.
To date, our knowledge about the exact mode of functioning of rTMS is restricted.
Future studies to investigate its effectiveness in the field of neuropsychiatry may prove
promising. For an adequate integration of results it is worth considering the combination
of rTMS with neurophysiological or imaging methods such as EEG or fMRI. This is
one objective of our manuscript outlined in 2.3. The following chapter provides an
insight into (f)MRI technique and gives an overview in combination with rTMS.
- 17 -

1.3 Functional Magnetic Resonance Imaging
The method of magnetic resonance imaging (MRI) has been enormously advanced
since its introduction in 1973 and is now used in clinical routine. Besides the non-
invasiveness of this diagnostic technique the impact of MRI relies on the ability of
imaging different tissue contrasts. Since 1992 then brain functions have been
investigated via functional MRI (Kellermann, 2007). To understand the principles of
MR technique and its modes of application some physical and physiological basics are
essential as described in the following section.
1.3.1 Physical and Physiological Principles
Subatomic particles have the impulse to spin around themselves, thus to produce a
magnetic field if these particles feature electric charge. The nucleus of a hydrogen atom
is composed of a positively charged proton with this property. Due to its high incidence
in the human organism the hydrogen atom is of great interest in medical MRI. If a
proton is arranged in an external magnetic field, the magnetic moment rotates (or
precesses) around the axis of this external magnetic field. The strength of the magnetic
field is measured in Tesla (T). The frequency of the proton precession around the
external magnetic field is called Lamor frequency and it is particle specific. Therefore,
the Lamor frequency increases proportionately to the strength of the external magnetic
field. Most of the spins align parallel to this external magnetic field leading to a
measurable magnetism in a probe (e.g. a patient) along the field direction (Kellermann,
2007; Kellermann et al., 2008). In the equilibrium state, after positioning a probe in a
magnetic field (or patient in a tomograph) and the alignment of all spins, there are no
further interactions. For the MR signal measure, this system has to be disequilibrated.
Therefore, an MR signal is generated by an electromagnetic high-frequency pulse (HF-
pulse) that has to be administered with the same Lamor frequency of the proton spins.
This HF pulse rotates the proton spins in the x-y-axis. When the pulse is turned off they
return back to thermodynamic equilibrium and the main magnetization becomes
realigned with the static magnetic field. During this process electromagnetic radiation is
emitted which is recorded by receiver coils due to Faraday’s law of induction
(Kellermann et al., 2008; Huettel et al., 2004).
- 18 -

The clinical relevance of the MRI method results from the fact that different
imaging contrasts can be extracted due to different tissue characteristics. For fMRI
experiments static contrasts are used to determine brain anatomy. These contrasts are
sensitive to type, number and relaxation properties of atomic nuclei. Typical static
contrasts include density (e.g. proton density), relaxation time (T1, T2, T2*), content of a
particular molecular type (e.g. magnetization transfer to detect large or small
molecules), and general chemical content (e.g. spectroscopy) (Huettel et al., 2004).
For the reconstruction of images it is essential to decode the origin of the signal. For
this purpose, proportions of the MR signal have to be attributed to predefined 3D-
volumes (voxels) within the probe. Gradient coils enable this correlation by generating
gradient fields which slightly overlay the static magnetic field. Lamor frequencies of the
protons thus differ according to their spatial position. The MR image can then be
reconstructed due to a frequency analysis (Fourier-Analysis) of the measured MR signal
by extracting the spatial position of the different frequency proportions (Huettel et al.,
2004; Kellermann et al., 2008).
There are two factors that govern the time in which MR images are collected. The
first is the time interval between successive excitation pulses, which is known as
repetition time or TR. The other factor is the echo time (TE) used for BOLD-contrast
fMRI images. The TE describes the time interval between an excitation pulse and data
acquisition, expressed in milliseconds (Huettel et al., 2004).
For the creation of images that are sensitive to brain function, thus, for
functional imaging (fMRI), it is necessary to identify a biophysical property that is
altered by information processing within the brain. The basis of functional imaging is
due to the fact that information-processing activity of neurons increases their metabolic
requirements. For this purpose, energy has to be provided. The vascular system supplies
cells with two fuel sources, glucose and oxygen, whereby the latter bounds to
haemoglobin molecules. Haemoglobin has magnetic properties depending on whether
or not it is bound to oxygen. Oxygenated haemoglobin (Hb) is diamagnetic, that is the
property of a weak repulsion from a magnetic field. Deoxygenated haemoglobin (dHb)
has a paramagnetic property. The magnetic susceptibility of dHb blood is about 20%
greater than fully oxygenated blood. This leads to a differentiability of arterial blood
(which contains only oxygenated haemoglobin) and venous blood (which contains both
- 19 -
oxy- and deoxygenated haemoglobin). MR pulse sequences sensitive to T2* show more
MR signal where blood is highly oxygenated, that is in case of neuronal activity during
cognitive processes, and less MR Signal where blood is highly deoxygenated. This
provides a basis for measurement of blood oxygenation changes using the so-called
blood-oxygen-level-dependent (BOLD) fMRI. The BOLD contrast is defined to be the
difference in signal on T2* -weighted images as the function of amount of deoxygenated
haemoglobin. BOLD fMRI today plays an important role in the field of cognitive
neuroscience as this technique enables the relation of changes in brain physiology over
time to an experimental manipulation due to specific cognitive tasks (Huettel et al.,
2004).
1.3.2 Imaging rTMS Effects
One possibility to modulate activity states and to interfere with the function of
certain brain areas is the application of rTMS. Physiological studies of the primary
motor cortex conducted in healthy subjects indicate that repetitive TMS can induce a
long-lasting enhancement or reduction of cortical excitability (for review see Ziemann
et al., 2008; Hallet, 2007). These and other effects can be mapped on-or offline using
different imaging methods. So far, various functional imaging techniques have been
used to visualize effects of rTMS on the brain. These include functional magnetic
resonance imaging (fMRI), positron emission computed tomography (PET), and single
photon emission computed tomography (SPECT). rTMS can serve as a probe of
functional connectivity when combined with these techniques. Pioneering studies
demonstrated that rTMS delivered to the frontal eye field or to the primary motor cortex
produced a pattern of dose-dependent distal effects in connected brain regions (Paus et
al. 1997; Fox et al. 1997). Similarly, studies showed that rTMS of the prefrontal cortex
modulated brain activity at both the stimulation site and in several distant regions
presumably connected with the stimulated cortex (Teneback et al. 1999; Paus et al.
2001; Shajahan et al. 2002; Kimbrell et al. 2002). Additionally, amongst healthy
volunteers rTMS of the left prefrontal cortex was shown to cause a reduction in [11C]
raclopride binding resulting from the release of endogenous dopamine in the left dorsal
caudate nucleus (Strafella et al. 2001). It was possible to induce dopamine release by
direct stimulation of corticofugal axons or by reducing GABA-mediated intra-cortical
- 20 -

inhibition and to image this effect using PET. Apart from imaging direct after-effects or
using online- rTMS during the fMRI session, one should consider imaging outlasting
effects off-line. Combining rTMS with functional imaging provides great impact for
research in cognitive neuroscience and raises new insights into the pathophysiology of
neuropsychiatric disorders. Triggering neural network firing with specific cognitive
tasks as well as imaging their manipulation following rTMS is of special interest in the
field. In our third presented work (see 2.3) we aimed to cope with these issues and
combined rTMS with offline fMRI. The primary objective of the study is the
investigation of long-term rTMS effects on working memory processes.
1.4 Summary and Unresolved Issues
Negative symptoms (such as apathy, blunted affect and social/ emotional
withdrawal) often occur in patients with schizophrenia and have been described to be
closely connected to DLPFC dysfunction due to deficient neuronal integrity and brain
metabolism. Inefficient dynamic modulation of DLPFC activity has been revealed to
impair working memory and other executive processes in schizophrenia (Cannon et al.,
2005; Goff & Evins 1998; Silver et al., 2003; Winterer & Weinberger, 2004). Some
consistency has been documented in the association between negative symptoms and
the severity of cognitive impairment, particularly in executive functions (Green et al.,
2000; Henry & Crawford, 2005; Johnson-Selfridge & Zalewski, 2001; for a review see
Reichenberg et al. 2010). Since negative symptoms and cognitive disturbance are often
persistent after antipsychotic medication, other therapeutic interventions should be
evaluated to increase life quality. Repetitive TMS is a method that is proven to evoke
outlasting or consolidation effects in the human motor system indicating behavioural
effects (e.g. Reis et al., 2008, 2009; Ziemann et al. 2008). Some TMS protocols which
administer repetitive pulses have the capacity to induce plasticity shifts of the
stimulated and interconnected brain areas (Esser et al., 2006; Reis et al., 2008).
Plasticity has been broadly defined as an activity-dependent enduring change in neural
structure and function, e.g. in synaptic efficacy (Vorel & Lisanby, 2008). According to
the ‘Hebbian’ characteristics of long-term potentiation (LTP), repeated electrical
stimulation of a pre-synaptic neuron increases the sum of excitatory postsynaptic
potentials (EPSP) with consequent synaptic strengthening and functional changes
- 21 -

(Hebb, 1949; Vorel & Lisanby, 2008). These mechanisms have been demonstrated also
in brain areas such as the prefrontal cortex (Floresco & Grace, 2003; Maroun & Richter-
Levin, 2003; Vorel & Lisanby, 2008). However, the mechanisms by which intermittent
brain stimulation such as excitatory rTMS could evoke lasting neuroplastic changes in
illnesses remain unclear until today. The effectiveness of rTMS in symptom
improvement or cognitive modulation is still outstanding. As we know from clinical
pilot trials on depression or schizophrenia, long-term high-frequency rTMS over the
right or left DLPFC seems to be a promising technique to improve certain depressive or
negative symptoms, respectively (see 1.2.3.1). However, the impact of rTMS on
cognitive processing remains questionable at this time. Single session TMS studies have
provided evidence for a transient enhancing effect of focal higher frequency stimulation
(e.g. Boroojerdi et al., 2001; Evers et al., 2001; Klimesch et al., 2003; Mottaghy et al.,
1999; Töpper et al., 1998). But there is no clear knowledge about the effect of repeated
rTMS sessions on cognition and the neurophysiological mechanisms. It seems likely
that repeated rTMS sessions cumulate the occurring effects and that intermittent
stimulation supports neuronal integration and consolidation. Systematic studies
addressing this issue are promising for potential clinical implementation. Furthermore,
brain imaging techniques such as fMRI would provide more profound insight into the
working mechanism of rTMS in the brain.
- 22 -

This thesis aims to reply to the following major questions:
Does long-term high frequency rTMS improve psychopathology, primarily
negative symptoms, in patients with schizophrenia?
This question will be addressed in the first multi-centre study outlined in chapter
2.1.
Does long-term high frequency rTMS influence cognition?
This question is main part of the second manuscript, the review article, illustrated in
chapter 2.2.
Does long-term high frequency rTMS improve WM dysfunction in patients
with schizophrenia?
Does long-term high frequency rTMS alter brain activation within the WM
network?
This twofold question will be addressed in the third presented study outlined in
chapter 2.3.
The third study is a sub-project of the first multi-centre study following the same
methodology in a smaller sample. The most relevant difference of the third study is
the clear focus on working memory and the additional implementation of fMRI
measures. Only in the sub-project has a healthy control group been included.
- 23 -

2 Publications
This chapter is comprised of the following articles that were either published or
accepted for publication up to submission of the thesis.
1. Cordes J, Falkai P, Guse B, Hasan A, Schneider-Axmann T, Arends M et al.
(2009). Repetitive transcranial magnetic stimulation for the treatment of negative
symptoms in residual schizophrenia: rationale and design of a sham-controlled,
randomized multicentre study. European Archives of Psychiatry and Clinical
Neuroscience 259 (Suppl 2):189-97.
2. Guse B, Falkai P, Wobrock T (2010). Cognitive effects of high-frequency
repetitive transcranial magnetic stimulation: a systematic review. Journal of
Neural Transmission 117(1): 105-22.
3. Guse B, Falkai P, Gruber O, Whalley H, Gibson L, Hasan A et al. (2013). The
effect of long-term high frequency repetitive transcranial magnetic stimulation on
working memory in schizophrenia and healthy controls – a randomized placebo-
controlled, double-blind fMRI study. Behavioural Brain Research, Jan 15,
237:300-7.
Further publications can be found at the end of this thesis.
- 24 -

2.1 Repetitive transcranial magnetic stimulation for the treatment of negative
symptoms in residual schizophrenia: rationale and design of a sham-controlled,
randomized multicentre study
This study addresses the effect of long-term excitatory rTMS over the left DLPFC
on negative symptoms in schizophrenia patients. The current manuscript describes the
trial design and rationale to provide an overview of this complex issue. The trial is
constructed as a randomized, placebo-controlled, observer-and patient-blind, parallel-
group treatment over three participating centres. Primary objective is to prove whether
active rTMS is more effective than sham rTMS regarding the improvement of negative
symptoms. Patients in the active condition receive 15 successive sessions of high
frequency 10 Hz rTMS over the left DLPFC (F3, EEG-System), with an intensity of
110% of the individual resting motor threshold, 1000 Stimuli per session (15000 in
total) with an inter-train interval of 30 seconds. In the placebo condition the same coil is
positioned 5 cm latero-caudal to F3 and distorted 45° away from the skull. The
intervention is in addition to antipsychotic medication. The primary efficacy endpoint is
a reduction of negative symptoms as assessed by the negative sum score of the Positive
and Negative Syndrome Scale (PANSS). A sample size of 63 in each group has 80%
power to detect an effect size of 0.50. Besides psychopathological ratings, further
outcome measures are social functioning, quality of life and some neurobiological and
neurocognitive parameters. The outcome is evaluated pre- versus post-treatment and
during a 12 weeks follow-up. Data analysis is based on the intention- to- treat
population.
- 25 -

Repetitive transcranial magnetic stimulation for the treatmentof negative symptoms in residual schizophrenia: rationaleand design of a sham-controlled, randomized multicenter study
Joachim Cordes Æ P. Falkai Æ B. Guse Æ A. Hasan Æ T. Schneider-Axmann Æ M. Arends Æ G. Winterer ÆW. Wolwer Æ E. Ben Sliman Æ M. Ramacher Æ C. Schmidt-Kraepelin Æ C. Ohmann Æ B. Langguth ÆM. Landgrebe Æ P. Eichhammer Æ E. Frank Æ J. Burger Æ G. Hajak Æ M. Rietschel Æ T. Wobrock
� Springer-Verlag 2009
Abstract Current meta-analysis revealed small, but sig-
nificant effects of repetitive transcranial magnetic stimu-
lation (rTMS) on negative symptoms in patients with
schizophrenia. There is a need for further controlled,
multicenter trials to assess the clinical efficacy of rTMS on
negative symptoms in schizophrenia in a larger sample of
patients. The objective of this multicenter, randomized,
sham-controlled, rater- and patient-blind clinical trial is to
investigate the efficacy of 3-week 10-Hz high frequency
rTMS add on to antipsychotic therapy, 15 sessions per
3 weeks, 1,000 stimuli per session, stimulation intensity
110% of the individual motor threshold) of the left
dorsolateral prefrontal cortex for treating negative symp-
toms in schizophrenia, and to evaluate the effect during a
12 weeks of follow-up. The primary efficacy endpoint is a
reduction of negative symptoms as assessed by the nega-
tive sum score of the positive and negative symptom score
(PANSS). A sample size of 63 in each group will have 80%
power to detect an effect size of 0.50. Data analysis will be
based on the intention to treat population. The study will be
conducted at three university hospitals in Germany. This
study will provide information about the efficacy of rTMS
in the treatment of negative symptoms. In addition to
psychopathology, other outcome measures such as neuro-
cognition, social functioning, quality of life and neuro-
biological parameters will be assessed to investigate basic
mechanisms of rTMS in schizophrenia. Main limitations of
the trial are the potential influence of antipsychotic dosage
changes and the difficulty to ensure adequate blinding.
Keywords Residual schizophrenia � Repetitive
transcranial magnetic stimulation � Neurobiology
Background
Depending on the definition of treatment-resistant schizo-
phrenia, about 10–30% of patients have little or no
response, and up to 30% have only partial responses to
antipsychotic medication [7, 8]. Residual symptoms, e.g.
negative symptoms and cognitive impairment, often persist
and determine an unfavorable course of the disease
including disabilities in many domains such as a reduction
in the quality of life. Second generation antipsychotics
provide some benefits by improving negative symptoms
compared with conventional antipsychotic treatment, but
still a considerable number of patients suffer from negative
Trial registration: clinicaltrials.gov NCT00783120.
J. Cordes (&) � M. Arends � G. Winterer � W. Wolwer �E. B. Sliman � M. Ramacher � C. Schmidt-Kraepelin
Department of Psychiatry and Psychotherapy,
Heinrich-Heine University of Dusseldorf,
Bergische Landstr. 2, 40629 Dusseldorf, Germany
e-mail: [email protected]
P. Falkai � B. Guse � A. Hasan � T. Schneider-Axmann �T. Wobrock
Department of Psychiatry and Psychotherapy,
University of Gottingen, Gottingen, Germany
B. Langguth � M. Landgrebe � P. Eichhammer � E. Frank �J. Burger � G. Hajak
Department of Psychiatry and Psychotherapy,
University of Regensburg, Regensburg, Germany
C. Ohmann
Coordination Centre for Clinical Trials,
Heinrich-Heine University, Dusseldorf, Germany
M. Rietschel
Department of Genetic Epidemiology in Psychiatry,
Institute of Central Mental Health, Mannheim, Germany
123
Eur Arch Psychiatry Clin Neurosci (2009) 259 (Suppl 2):S189–S197
DOI 10.1007/s00406-009-0060-y
- 26 -

symptoms associated with cognitive deficits, apathy,
anhedonia, depressive mood and affective flattening [7, 8].
Despite the clinical relevance of these negative symptoms,
there are only few treatment strategies available. Therefore,
looking for alternative treatment approaches to negative
symptoms is currently a central issue in schizophrenia
research [8].
Repetitive transcranial magnetic stimulation (rTMS)
modulates cortical excitability and function in a non-
invasive way. It uses alternating magnetic fields to induce
electric currents in cortical tissue in specific brain regions
[3]. Several studies have found that high frequency rTMS
increased excitability in various brain areas [16]. Evidence
from lesioning and neuroimaging studies has linked nega-
tive symptoms to dysfunctions of the dorsolateral pre-
frontal cortex (DLPFC), the limbic system, and the basal
ganglia, which has been associated with diminished
dopamine signaling in DLPFC [13, 40]. Activation of
mesostriatal dopaminergic pathways by excitatory high
frequency rTMS applied over the DLPFC has been dem-
onstrated in clinical studies [37].
Pilot studies have suggested an application of rTMS as a
novel therapeutic tool in schizophrenia, based on the idea
of targeted stimulation of dysfunctional cortico-subcortical
circuits involved in the pathophysiology of schizophrenia
[10, 18, 25, 26, 39]. Present evidence suggests that rTMS
may be considered safe [27]. Stimulation of the DLPFC
may trans-synaptically lead to an activation of dopami-
nergic neurons in the mesencephalon, and noradrenergic
and serotonergic neurons in the brainstem. RTMS appears
to have an effect on neurotransmitter systems which are
involved in the pathophysiology of negative symptoms in
schizophrenia [37]. Negative symptoms and acoustic hal-
lucinations were the target of interventions by rTMS in
previous studies [4, 9, 16]. At the time our trial was
designed, three out of four controlled high frequency 10 Hz
studies indicated a significant improvement of negative
symptoms. Other studies (one with 1 Hz and three with
20 Hz stimulation frequency) did not show this effect in
schizophrenia patients. In a double-blind crossover dose-
finding study on 27 schizophrenic patients with predomi-
nantly negative symptoms, a significantly higher thera-
peutic effect was shown at an alpha EEG peak frequency
determined for each individual subject 8–13 Hz rTMS over
the DLPFC at 80% motor threshold compared with treat-
ment at 3 or 20 Hz and sham as controls [21]. Freitas et al.
pooled the results of eight studies assessing negative
symptoms, and compared the results of post-rTMS treat-
ment versus baseline. High frequency rTMS induced a
significant reduction in negative symptoms [9]. These
authors did not assess whether the therapeutic effects were
longlasting as only a few studies report follow-up assess-
ments. In summary, high frequency rTMS is a promising
technique to treat negative symptoms in schizophrenia.
However, available trials are characterized by small sample
sizes and heterogeneous results [4, 9, 16, 33].
Thus, randomized controlled trials with higher statistical
power and improved methodology are needed. For this
reason, a randomized, multicenter study to investigate the
efficacy of high frequency rTMS in the treatment of neg-
ative symptoms in schizophrenia in Germany was designed
by the authors [repetitive rTMS for the treatment of neg-
ative symptoms in schizophrenia—a multicenter study
(RESIS Trial)]. After the successful application for funding
by the German Research Foundation in December 2006,
active recruitment was started in January 2008.
Methods
Design of the trial
The trial is a randomized, sham-controlled, observer- and
patient-blind, two-arm, parallel group study of 3-week high
frequency (10 Hz) rTMS treatment plus 3 months follow-up
in schizophrenia patients with predominantly negative
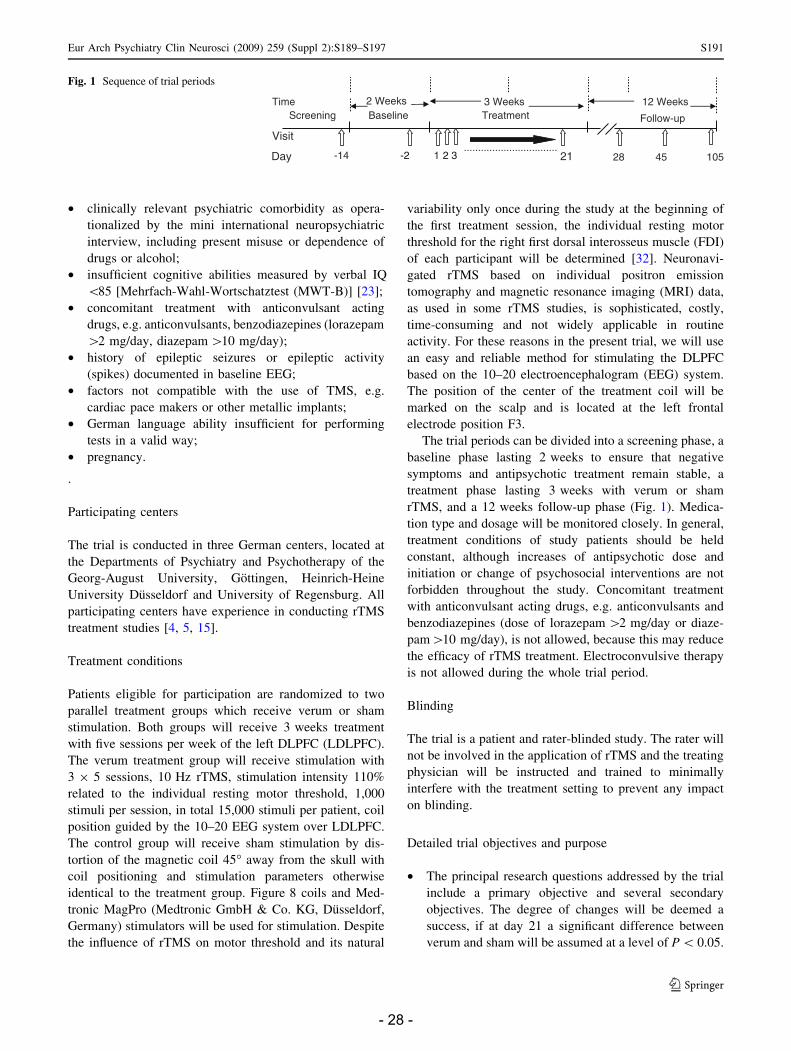
symptoms (see Fig. 1).
Study population, inclusion and exclusion criteria
The inclusion criteria warrant that patients with predomi-
nantly and clinically relevant negative syndromes will be
recruited for the trial. Female and male in- and outpatients
aged 18–60 years are eligible for study participation if they
meet the following key inclusion criteria:
• signed informed consent, patient able and willing to
participate in the study;
• diagnosis of schizophrenia according to the interna-
tional classification of disorders (ICD-10) F 20 criteria.
The mini international neuropsychiatric interview
(MINI-Plus) is a structured interview for classification
of axis-I disorders according to DSM-IV and ICD-10)
[35]. Illness duration [1 year;
• positive and negative symptom score (PANSS)-nega-
tive sum score [20 points, at least one of the PANSS-
negative items N1–N7 (range 1–7) C4 (at least
moderate, clinically relevant negative symptoms),
improvement in PANSS-negative sum score (N1–N7
items with a range 1–7) \10% in the last 2 weeks,
stable medication intake for C2 weeks.
Key exclusion criteria are
• involuntary stay in hospital at the time of recruitment;
• clinically relevant unstable medical conditions;
• previous treatment by rTMS;
S190 Eur Arch Psychiatry Clin Neurosci (2009) 259 (Suppl 2):S189–S197
123
- 27 -
• clinically relevant psychiatric comorbidity as opera-
tionalized by the mini international neuropsychiatric
interview, including present misuse or dependence of
drugs or alcohol;
• insufficient cognitive abilities measured by verbal IQ
\85 [Mehrfach-Wahl-Wortschatztest (MWT-B)] [23];
• concomitant treatment with anticonvulsant acting
drugs, e.g. anticonvulsants, benzodiazepines (lorazepam
[2 mg/day, diazepam [10 mg/day);
• history of epileptic seizures or epileptic activity
(spikes) documented in baseline EEG;
• factors not compatible with the use of TMS, e.g.
cardiac pace makers or other metallic implants;
• German language ability insufficient for performing
tests in a valid way;
• pregnancy.
.
Participating centers
The trial is conducted in three German centers, located at
the Departments of Psychiatry and Psychotherapy of the
Georg-August University, Gottingen, Heinrich-Heine
University Dusseldorf and University of Regensburg. All
participating centers have experience in conducting rTMS
treatment studies [4, 5, 15].
Treatment conditions
Patients eligible for participation are randomized to two
parallel treatment groups which receive verum or sham
stimulation. Both groups will receive 3 weeks treatment
with five sessions per week of the left DLPFC (LDLPFC).
The verum treatment group will receive stimulation with
3 9 5 sessions, 10 Hz rTMS, stimulation intensity 110%
related to the individual resting motor threshold, 1,000
stimuli per session, in total 15,000 stimuli per patient, coil
position guided by the 10–20 EEG system over LDLPFC.
The control group will receive sham stimulation by dis-
tortion of the magnetic coil 45� away from the skull with
coil positioning and stimulation parameters otherwise
identical to the treatment group. Figure 8 coils and Med-
tronic MagPro (Medtronic GmbH & Co. KG, Dusseldorf,
Germany) stimulators will be used for stimulation. Despite
the influence of rTMS on motor threshold and its natural
variability only once during the study at the beginning of
the first treatment session, the individual resting motor
threshold for the right first dorsal interosseus muscle (FDI)
of each participant will be determined [32]. Neuronavi-
gated rTMS based on individual positron emission
tomography and magnetic resonance imaging (MRI) data,
as used in some rTMS studies, is sophisticated, costly,
time-consuming and not widely applicable in routine
activity. For these reasons in the present trial, we will use
an easy and reliable method for stimulating the DLPFC
based on the 10–20 electroencephalogram (EEG) system.
The position of the center of the treatment coil will be
marked on the scalp and is located at the left frontal
electrode position F3.
The trial periods can be divided into a screening phase, a
baseline phase lasting 2 weeks to ensure that negative
symptoms and antipsychotic treatment remain stable, a
treatment phase lasting 3 weeks with verum or sham
rTMS, and a 12 weeks follow-up phase (Fig. 1). Medica-
tion type and dosage will be monitored closely. In general,
treatment conditions of study patients should be held
constant, although increases of antipsychotic dose and
initiation or change of psychosocial interventions are not
forbidden throughout the study. Concomitant treatment
with anticonvulsant acting drugs, e.g. anticonvulsants and
benzodiazepines (dose of lorazepam [2 mg/day or diaze-
pam[10 mg/day), is not allowed, because this may reduce
the efficacy of rTMS treatment. Electroconvulsive therapy
is not allowed during the whole trial period.
Blinding
The trial is a patient and rater-blinded study. The rater will
not be involved in the application of rTMS and the treating
physician will be instructed and trained to minimally
interfere with the treatment setting to prevent any impact
on blinding.
Detailed trial objectives and purpose
• The principal research questions addressed by the trial
include a primary objective and several secondary
objectives. The degree of changes will be deemed a
success, if at day 21 a significant difference between
verum and sham will be assumed at a level of P \ 0.05.
Follow-up
Day 1 21 .................................
Screening Baseline Treatment
Visit
skeeW21skeeW3skeeW2Time
-2 2 3 45 10528 -14
Fig. 1 Sequence of trial periods
Eur Arch Psychiatry Clin Neurosci (2009) 259 (Suppl 2):S189–S197 S191
123
- 28 -

Primary objective
• The primary objective of the study is to prove if verum
rTMS is clinically more effective than sham rTMS as
an add-on treatment in schizophrenic patients with
predominantly negative symptoms as measured by
showing a superior improvement in the PANSS-nega-
tive score [22] (day 21).
Secondary objectives
To evaluate the efficacy of verum rTMS versus sham rTMS
on later time points than the primary objective.
• In reducing negative symptoms measured at follow-up by
change of PANSS-negative score on any of these days (days
28, 45, 105) and additional clinical response defined as
improvement of C20% PANSS-negative baseline score.
• Influence on positive symptoms immediately after
finishing intervention (day 21) and at follow-up mea-
sured by change of PANSS-positive score (days 28, 45,
105).
• In reducing depressive symptoms immediately after
finishing intervention (day 21) and at follow-up mea-
sured by change of Calgary Depression Rating Scale
for Schizophrenia [1] and Montgomery and Asberg
Depression Rating Scale [28] (days 28, 45, 105).
• In changes of global functioning and disease severity
measured by changes in CGI and GAF score [6], and
social adjustment/life quality by changes in scale for
quality of life (SAS II score) [36] immediately after
finishing intervention (day 21) and at follow-up (days
28, 45, 105). On cognition measured by changes in
scores of Wisconsin card sorting test [14], Regens-
burger Wortflussigkeits test [2], Verbaler Lern- und
Merkfahigkeitstest [17] the trail making test to organic
brain damage (TMT A/B) [30] and digit span [38]
immediately after finishing intervention (day 21) and at
follow-up (days 28, 45, 105).
• On extrapyramidal motoric symptoms (EPS) measured
by changes in St. Hans scale score [11, 31] immediately
after finishing intervention (day 21) and at follow-up
(days 28, 45, 105).
Neurobiological markers as adjunctive secondary out-
come measures are to evaluate the efficacy of real rTMS
versus sham rTMS:
• Changes in short interval cortical inhibition (SICI,
interstimulus interval 3 ms), intracortical facilitation
(ICF, interstimulus interval 15 ms) and duration of
contralateral cortical silent period (CSP) in the FDI are
measured by paired- and single-pulse dTMS of the right
and left motor cortex.
• Changes in spontaneous EEG frequency spectrum
activity changes will be registered by 28 electrodes
according to the extended 10/20 system.
• Changes in the identification rate of facial expressions
after presenting ‘‘pictures of facial affect’’ will be
assessed and evoked potentials during facial expression
recognition tests at about 170 ms (N170) and 240 ms
(P240) amplitudes will be recorded.
• Changes in regional brain metabolism will be measured
by changes in metabolite ratios (N-acetylaspartate
(NAA)/creatine ratio or NAA/choline ratio) with single
voxel proton magnetic resonance spectroscopy,
whereby voxels are placed in right dorsal prefrontal
areas, in basal ganglia (covering caudate nucleus/
putamen), the internal capsule, and in the hippocampus.
• Changes in prefrontal attentional network activation
during a selective attention requiring visual oddball task
measured with simultaneously acquired EEG/functional
MRI (fMRI), i.e., BOLD-response, slow wave (‘‘Theta’’)
oscillations for a subgroup of individuals.
• Changes in mRNA/protein expression of selected
candidate genes measured by blood tests.
• And to evaluate the influence of genetic background on
the response to rTMS. The groups will be stratified, e.g.
comparing BDNF Val66Met polymophisms (Val/Val
vs. ValMet).
Key safety parameters in this trial are vital signs (blood
pressure, heart rate), EEG recording immediately before
and after the rTMS treatment period (day 21), and stan-
dardized questions about physical and mental state during
and after daily tTMS treatment.
Visit schedule and data collection/management
An overview on the time schedule for assessing and
recording of efficacy and safety parameters is given in
Table 1. An independent data safety and monitor board
(DSMB) consisting of clinical and statistical experts will
critically assess adherence to the study protocol as well as
to International Conference on Harmonization of Technical
Requirements for Registration of Pharmaceuticals for
Human Use (ICH)—Good Clinical Practice (GCP)—
guidelines. Together with the sponsor, the DSMB will
decide whether the trial has to be terminated prematurely.
Any patient eligible for participation in the investigation
according to the inclusion criteria will be advised of
potential risks and benefits before signing the patient
consent form. Patient information and consent forms were
approved by the responsible ethics committees.
The data management follows a remote data entry
approach. The electronical case report form (eCRF) is
implemented in a modern clinical data management system
S192 Eur Arch Psychiatry Clin Neurosci (2009) 259 (Suppl 2):S189–S197
123
- 29 -

(CDMS) with electronical data capture functionality. The
system complies with the relevant international standards
and provides the capability to perform the major data
management activities within a consistent, auditable, and
integrated electronical environment (query management,
data entry, data validation).
All measures concerning monitoring/quality assurance
are conducted in accordance to ICH-GCP. Monitoring is
conducted according to the harmonized standard operating
procedures of the coordination center for clinical trials
study-specific processes are described in detail by working
instructions.
Power and sample size justification
Sample size calculation is motivated by the primary end-
point, based on the PANSS-negative symptoms score on
day 21. This score has been documented with a mean value
Table 1 Study visits and assessments
Study visit V0 (t0) V1 (t1) V2 (t2) V3 (t3) V4 (t4) V5 (t5) V6 (t6)
Phase Screening Baseline Treatment Follow-up
Day -28 bis -14 -14 0 21 28 45 105
Inclusion/exclusion x
MINI-Plus x
Informed consent x
Demographic data x
Psychiatric history x
Medical history x
EHI x
Randomization x
Concomitant medication x x x x x x x
Adverse events x x x x x x x
UKU x x x x x
St. Hans scale x x x x x
PANSS x x x x x x x
CDSS x x x x x
MADRS x x x x x
CGI x x x x
GAF x x x x
SAS II x x x x
Neuropsychology x x x x
EEG x x
ERP x x
ECG x
Physical examination x
Vital signs (BP, HR) x x x x x x
MRI/MRS x x
EEG/fMRI x x
dTMS x x x
Laboratory x x
Genetics x x x
Visit V1–V4 are scheduled on the respective day ±2 days, visit V5–V6 ±1 week
At day 0 the stimulation period starts
MINI-Plus MINI-Plus Interview for ICD-10 and DSM-IV diagnosis, EHI Edinburgh Handedness Inventory, UKU Udvalg for Kliniske Und-
ersogelser—detailed Side-Effect Rating Scale, St. Hans Scale Scale for the rating of extrapyramidal motoric symptoms, PANSS positive- and
negative syndrome scale in schizophrenia, CDSS Calgary depression rating scale for schizophrenia, MADRS Montgomery and Asberg depression
rating scale, CGI clinical global impression, GAF global assessment scale of functioning, SAS II scale for quality of life, EEG electroen-
cephalogram, ECG electrocardiogram, BP blood pressure, HR heart rate, MRI magnetic resonance imaging, MRS magnetic resonance spec-
troscopy, fMRI functional magnetic resonance imaging, dTMS diagnostic transcranial magnetic stimulation
Eur Arch Psychiatry Clin Neurosci (2009) 259 (Suppl 2):S189–S197 S193
123
- 30 -

ranging from 20 to 24 points at baseline in previous studies
of our target population. In the control group an
improvement of about three points is expected for day 21.
Standard deviation has been reported with values between
four and six points [5, 15, 24]. A difference of three points
is considered as a clinically relevant difference. Power
calculations show that a sample size of 63 in each group
will have a 80% power to detect an effect size of 0.50,
which corresponds to a change of three points between
control and treatment group.
Randomization
The patients selected for participation will be randomly
assigned to either the control or experimental intervention
by a computer-generated multiblock randomization sche-
dule generated at the coordination center for clinical trials.
The schedule will be a 1:1 ratio, permutated in setting
blocks of 4, 6, and 8 patients. Randomization will be
stratified by participating hospitals and randomized allo-
cation to one of two treatment arms will take place after
assessment of eligibility and after obtaining informed
consent from the patients for participation.
Statistics
The efficacy analysis with primary and secondary outcome
criteria will be done in the intention to treat population.
Conclusions of the trial will be based only on the intention to
treat population. For confirmatory analysis, a modeling
approach will be applied. A linear model will be used:
yi,j,c = l ? aj ? gc ? ei,j,c (ei,j,c : random effects), where
yi,j,c is the response of individual i (i = 1,…, mC) random-
ized to treatment j (j = 1, 2) for the center c (c = 1,…, C).
The parameters in the model are l (the grand mean), aj (the
group effects) and gc (the center effects). The parameters of
interest in this analysis are the mean of the control group
l ? a1 and the contrast of means a1 ? a2 (which indicates
treatment effect). Estimation of model parameters will be
calculated with maximum likelihood. Treatment effects will
be tested with a likelihood ratio test. In addition, centers
effects will be analyzed. Distributional assumptions will be
assessed (e.g. residual analysis) and transformation on the
response variable will be done if it is necessary. In addition, if
adjustment for covariates is necessary, these will be included
in the model. Descriptive statistics will be calculated for each
treatment group. Demographic and baseline data will be
compared using appropriate statistical techniques.
Recruitment
By the end of June 2009, we have included 93 schizo-
phrenia patients suffering from predominant negative
symptomatic in the trial. The baseline data from 70 patients
were already captured in the electronic database. Half of
the sample received active verum stimulation and the other
half sham stimulation. In Table 2 some preliminary base-
line data are presented. The majority of patients are male.
The psychopathological data (PANSS scores) seem to be
comparable to that of pharmacological studies involving
chronically ill schizophrenia patients. In summary, the
included patients may represent the typical schizophrenia
patient population treated in a hospital setting in the three
participating centers.
Owing to the safety assessment, 23 adverse events were
observed in 17 patients. In seven patients, the adverse
events were classified as severe: two patients showed
worsening of positive symptoms, but only in one patient a
relationship between study intervention and worsening of
psychopathology was estimated as possible; four patients
displayed depressive mood, two of them with suicidal
thoughts; and one patient suffered from severe sleeplessness
and was admitted to hospital. The other adverse events
included headache (1 patients), flu-like symptoms (3
patients), nausea (2 patients), transient tinnitus (1 patient),
increased anxiety (1 patient), depressive mood (2 patients),
sleeplessness and muscle pain during the stimulation period
(1 patient), parkinsonoid (1 patient), thyroidal dysfunction
(1 patient), increased libido (1 patient), dizziness and
intermittent vertigo (1 patient) and an elevation of the
muscle enzyme creatine kinase (1 patient). The majority of
these adverse events (14 of 23) could not be attributed to the
study intervention. Overall, the rTMS treatment seems to be
safe and well tolerated. Until the end of the stimulation
period (day 21), nine patients dropped out. Four patients
dropped out because of the above-described adverse events.
Discussion
High frequency rTMS over LDLPFC applied as an adju-
vant to antipsychotic medication offers a new treatment
Table 2 Preliminary baseline parameters of included patients (June
2009)
Verum
(n = 35)
Sham
(n = 35)
Male/female (%) 83/17 73/27
Education years (m/SD) 10.8 (1.8) 10.6 (1.7)
PANSS-positive score (m/SD) 12.3 (3.2) 13.1 (3.2)
PANSS-negative score (m/SD) 26.1 (4.2) 27.3 (5.2)
PANSS general psychopathology score
(m/SD)
38.9 (10.6) 38.2 (8.4)
PANSS total score (m/SD) 76.8 (15.2) 79.0 (11.1)
m mean, SD standard deviation
S194 Eur Arch Psychiatry Clin Neurosci (2009) 259 (Suppl 2):S189–S197
123
- 31 -

option for negative symptoms in patients with schizo-
phrenia. Regarding clinical and neurobiological results,
there is increasing evidence for the efficacy of 10 Hz rTMS
treatment in negative symptoms.
Possible explanations for the moderate effect size and
for the divergence across studies can be offered. One
explanation might be the variation of the baseline psy-
chopathology that probably influences the treatment
response [9]. It seems that trials with stimuli lower than
10,000 delivered negative [19] or worse results [20] and
better results were detected when total number of stimuli
were 10,000 or higher [29, 34]. In most studies, cognitive
and functional outcome measures were scarcely used, but
led to interesting results. All studies available consisted of
small sample sizes. Data are convincing that the paradigm
of 10 Hz rTMS applied over left DLFPC is the most
promising design to be proven in a trial with larger sample
size. If the efficacy and effectiveness of this treatment is
proven in a larger sized sample, this technique will be easy
to establish and highly feasible in clinical practice. A dose-
finding trial to detect significant advantages between dif-
ferent stimulation frequencies, different rates of total
stimuli numbers and different treatment durations will
require a very high sample size. In our study, an active
rTMS treatment period over 3 weeks (total number of
stimuli = 15,000) is planned. Because a review clearly
identified number of days with stimulus application as a
main outcome factor of rTMS in depression [12], we
considered a longer period (3 weeks) of active treatment
than previous studies (2 weeks) in schizophrenia to
improve the outcome. Efficacy of 10 Hz rTMS in patients
with predominantly negative symptoms was only demon-
strated in two trials [5, 21]. Clinical efficacy and psycho-
social outcome was not investigated in previous studies.
Negative symptoms may account for psychosocial
impairment, but relevant ratings of social functioning,
quality of life and the fulfillment of the ability to handle the
daily occurrences, relevant to clinical practice were not
performed. A follow-up evaluation is missing in the pub-
lished studies. The quality of blinding has not been asses-
sed in available studies. In our study patients will be asked
about their guess, which stimulation condition they may
have been received to control for blinding and to avoid a
systematic bias.
Clinical data on the efficacy of rTMS are limited, mainly
due to the small sample sizes of available studies. Sham-
controlled studies of larger patient samples with defined
disease stages and a clear diagnostic typing are required.
Several methodological advantages had to be considered in
the design of our trial. We evaluate a large sample size with
a high total stimuli number and investigate whether a
lasting effect during the follow-up period can be achieved.
Also, we provide a longer period of active treatment than
previous studies (2 weeks) in schizophrenia, and this may
improve outcome.
In addition to psychopathology, a wide range of neu-
ropsychological test performances and social adaptation
will be evaluated in our trial. We will measure several
neurobiological parameters to investigate the basic mech-
anisms of rTMS efficacy in schizophrenia. Limitations of
our trial are the short period of medication stability and
changes of the antipsychotic dosage during intervention,
and the exclusive inclusion of in patients. However, rTMS
was employed almost exclusively as an adjuvant therapy to
antipsychotic pharmacotherapy, whereby most studies
provided no or only little information about the nature and
dose of the employed antipsychotics or the duration of
antipsychotic treatment. The accompanying medication
will be completely assessed and will be mentioned as a
confounding factor in our study. The type of medication
and the antipsychotic dose will be handled as a covariate in
the statistical analysis. Because anticonvulsive medication
may reduce the therapeutic effect of rTMS, treatment with
anticonvulsants is an exclusion criterion in our study.
An ongoing issue in controlled clinical studies is the
question of an adequate control condition [25]. For the
proposed study, we will use angulations of the active
magnetic coil 45� away from the skull as the control con-
dition. This procedure minimizes the magnetic field effect
on the brain, but simultaneously generates some skull
sensation [25]. An alternative option is the use of a
so-called ‘‘sham-coil system’’, mimicking the sound of a
real coil without generating any magnetic field. However,
this sham-coil system does not elicit a skull sensation. The
above-described procedure as a control condition has the
major advantage to induce sensations similar to the verum
condition. In terms of blinding conditions, skull sensation
makes it more difficult for patients to guess whether they
receive verum or sham TMS application.
The implementation of a randomized patient allocation
to either the verum or the sham group, and particularly the
sham control itself deserve special methodological con-
sideration. A modified double-blind design will be applied,
in which patients and clinical observers will be blind to
treatment conditions. Patients have to be naıve regarding
verum or sham rTMS treatment and will not be informed
about technical details of rTMS application. As the treating
physician knows whether verum or sham rTMS is applied,
and because automatic rTMS is methodologically not fea-
sible in clinical settings to date, the personnel applying
rTMS will be instructed and trained to minimally interfere
with the treatment setting to prevent any impact on
blinding. The rating and all study-specific procedures are
carried out by a person who is not involved in the rTMS
treatment. To avoid any impact of side-effect complaints
on the clinical rating, side effects will be assessed by the
Eur Arch Psychiatry Clin Neurosci (2009) 259 (Suppl 2):S189–S197 S195
123
- 32 -

rTMS performing physician immediately after each
rTMS session and at follow-up using a standardized
questionnaire.
The design of our rTMS trial has to consider ethical
aspects. Applied under previously published safety guide-
lines [39], rTMS has been proven to be a safe and well
tolerated therapy in a broad range of studies encompassing
distinct neuropsychiatric diseases [27]. The study protocol
as well as the documents to obtain patient’s informed
consent has been approved by the ethics committees. The
study will be performed in accordance with the ethics
principles that have their origin in the Declaration of
Helsinki and are consistent with the ICH Guidelines for
Good Clinical Practice and expert consensus.
The study protocol takes into account all of the descri-
bed methodological difficulties and will hopefully dem-
onstrate the feasibility and efficacy of a controlled
multicenter rTMS trial thereby enhancing the quality of the
collected data on the role of rTMS for treating mental
disorders.
Trial centres
Department of Psychiatry and Psychotherapy, Georg-
August-University Gottingen, Germany.
Department of Psychiatry, University of Dusseldorf,
Germany.
Department of Psychiatry and Psychotherapy, Univer-
sity of Regensburg.
Monitoring
Coordination Centre for Clinical Trials, University of
Dusseldorf.
Additional trial site
Department of Genetic Epidemiology, Institute of Central
Mental Health, Mannheim, performing the genetic
analyses.
Acknowledgment This study is funded by the German Research
Foundation (DFG: grant FA 241/10-1).
Conflict of interest statement T. Wobrock has participated in
speaker bureaus for AstraZeneca, Bristol-Myers Squibb, Janssen-
Cilag, Eli Lilly, Organon, Pfizer, Sanofi-Synthelabo/Aventis, and
Alpine-Biomed and received grant/research support from Astra
Zeneca. J. Cordes has participated in speakers bureaus for Janssen-
Cilag, Eli Lilly, Alpine-Biomed and has received grant/research
support from Eli Lilly, Janssen-Cilag, and Pfizer. G. Winterer has
participated in speakers bureaus for Janssen-Cilag, Pfizer, AstraZeneca.
He has recived research support from Eli Lilly, AstraZeneca, Janssen-
Cilag and Johnson & Johnson. P. Falkai is a member of a speakers’
bureau for AstraZeneca, Eli Lilly, Janssen-Cilag and Lundbeck, and
has accepted paid speaking engagements in industry-sponsored
symposia from AstraZeneca, Bristol-Myers-Squibb, Eli-Lilly,
Janssen-Cilag, Lundbeck and Pfizer, and travel or hospitality not
related to a speaking engagement from Astra Zeneca, Bristol-Myers-
Squibb, Eli Lilly, Janssen Cilag, Lundbeck and Sanofi-Synthelabo,
and received a research grant from Astra Zeneca. B. Langguth has
participated in speakers bureaus for Eli Lilly, Boehringer-Ingelheim,
Pfizer, Alpine-Biomed and has received grant/research support
from Astra Zeneca and the Tinnitus Research Initative. W. Wolwer,
A. Hasan, B. Guse, E. Ben Sliman, T. Schneider-Axmann, M. Arends,
M. Ramacher, C. Schmidt-Kraepelin, C. Ohmann, M. Landgrebe,
P. Eichhammer, E. Frank, J. Burger, G. Hajak and M. Rietschel report
no additional financial or other relationships relevant to the subject of
this article.
References
1. Addington D, Addington J, Maticka-Tyndale E (1993) Assessing
depression in schizophrenia: the Calgary depression scale. Br J
Psychiatry 22(Suppl):39–44
2. Aschenbrenner S, Tucha O, Lange KW (2000) Regensburger
Wortflussigkeits-Test (RWT): Handanweisung. Hogrefe, Verlag
fur Psychologie, Gottingen
3. Burt T, Lisanby SH, Sackeim HA (2002) Neuropsychiatric
applications of transcranial magnetic stimulation: a meta-analy-
sis. Int J Neuropsychopharmacol 5:73–103
4. Cordes J, Arends M, Mobascher A, Brinkmeyer J, Kornischka J,
Eichhammer P, Klimke A, Winterer G, Agelink MW (2006)
Potential clinical targets of repetitive transcranial magnetic stim-
ulation treatment in schizophrenia. Neuropsychobiology 54:87–99
5. Cordes J, Thunker J, Agelink MW, Arends M, Mobascher A,
Wobrock T, Schneider-Axmann T, Brinkmeyer J, Mittrach M,
Regenbrecht G, Wolwer W, Winterer G, Gaebel W (2009)
Effects of 10 Hz repetitive transcranial magnetic stimulation
(rTMS) on Clinical Global Impression in chronic schizophrenia.
Psychiatry Res (accepted)
6. Endicott J, Spitzer RL, Fleiss JL, Cohen J (1976) The global
assessment scale: a procedure for measuring overall severity of
psychiatric disturbance. Arch Gen Psychiatry 33:766–771
7. Falkai P, Wobrock T, Lieberman J, Glenthoj B, Gattaz WF,
Moller HJ (2005) WFSBP Task Force on Treatment Guidelines
for Schizophrenia Guidelines for biological treatment of schizo-
phrenia, part 1: acute treatment of schizophrenia. World J Biol
Psychiatry 6:132–191
8. Falkai P, Wobrock T, Lieberman J, Glenthoj B, Gattaz WF,
Moller HJ (2006) WFSBP Task Force on Treatment Guidelines
for Schizophrenia Guidelines for biological treatment of schizo-
phrenia, part 2: long-term treatment of schizophrenia. World J
Biol Psychiatry 7:5–40
9. Freitas C, Fregni F, Pascual-Leone A (2009) Meta-analysis of the
effects of repetitive transcranial magnetic stimulation (rTMS) on
negative and positive symptoms in schizophrenia. Schizophr Res
108:11–24
10. George MS, Nahas Z, Molloy M, Speer AM, Oliver NC, Li XB,
Arana GW, Risch SC, Ballenger JC (2000) A controlled trial of
daily left prefrontal cortex TMS for treating depression. Biol
Psychiatry 48:962–970
11. Gerlach J, Korsgaard S, Clemmesen P, Lauersen AM, Magelund
G, Noring U, Povlsen UJ, Bech P, Casey DE (1993) The St Hans
Rating Scale for extrapyramidal syndromes: reliability and
validity. Acta Psychiatr Scand 87:244–252
12. Gershon AA, Dannon PN, Grunhaus L (2003) Transcranial
magnetic stimulation in the treatment of depression. Am J Psy-
chiatry 160:835–845
S196 Eur Arch Psychiatry Clin Neurosci (2009) 259 (Suppl 2):S189–S197
123
- 33 -

13. Goff DC, Evins AE (1998) Negative symptoms in schizophrenia:
neurobiological models and treatment response. Harv Rev Psy-
chiatry 6:59–77
14. Grant DA, Berg EA (1993) Wisconsin card sorting test. Hofgrefe,
Gottingen
15. Hajak G, Marienhagen J, Langguth B, Werner S, Binder H,
Eichhammer P (2004) High-frequency repetitive transcranial
magnetic stimulation in schizophrenia: a combined treatment and
neuroimaging study. Psychol Med 34:1157–1163
16. Haraldsson HM, Ferrarelli F, Kalin NH, Tononi G (2004)
Transcranial magnetic stimulation in the investigation and treat-
ment of schizophrenia: a review. Schizophr Res 71:1–16
17. Helmstaedter C, Lendt M, Lux S (2000) Testhandbuch Verbaler
Lern- und Merkfahigkeitstest. Hogrefe, Gottingen
18. Hoffman RE, Cavus I (2002) Slow transcranial magnetic stimu-
lation, long-term depotentiation, and brain hyperexcitability dis-
orders. Am J Psychiatry 159:1093–1102
19. Holi MM, Eronen M, Toivonen K, Toivonen P, Marttunen M,
Naukkarinen H (2004) Left prefrontal repetitive transcranial
magnetic stimulation in schizophrenia. Schizophr Bull 30:429–
434
20. Jandl M, Bittner R, Sack A, Weber B, Gunther T, Maurer K,
Kaschka WP (2005) Therapeutic effects of individualized alpha
frequency transcranial magnetic stimulation (aTMS) on the neg-
ative symptoms of schizophrenia. Schizophr Bull 112:955–967
21. Jin Y, Potkin SG, Kemp AS, Huerta ST, Alva G, Thai TM,
Carreon D, Bunney WE Jr (2005) Therapeutic effects of indi-
vidualized alpha frequency transcranial magnetic stimulation
(aTMS) on the negative symptoms of schizophrenia. Schizophr
Bull 32:556–p561
22. Kay SR, Fiszbein A, Opler LA (1987) The positive and negative
syndrome scale (PANSS) for schizophrenia. Schizophr Bull
13:261–276
23. Lehrl S (1991) Manual zum MWT-B. (3 uberarbeitete Auflage).
Perimed-Fachbuch Verlagsgesellschaft Erlangen
24. Lewis SW, Barnes TR, Davies L, Murray RM, Dunn G, Hayhurst
KP, Markwick A, Lloyd H, Jones PB (2006) Randomized con-
trolled trial of effect of prescription of clozapine versus other
second-generation antipsychotic drugs in resistant schizophrenia.
Schizophr Bull 32:715–723
25. Lisanby SH, Luber B, Perera T, Sackeim HA (2000) Transcranial
magnetic stimulation: applications in basic neuroscience and
neuropsychopharmacology. Int J Neuropsychopharm 3:259–273
26. Lisanby SH, Belmaker RH (2000) Animal models of the mech-
anisms of action of repetitive transcranial magnetic stimulation
(RTMS): comparisons with electroconvulsive shock (ECS).
Depress Anxiety 12:78–87
27. Loo CK, McFarquhar TF, Mitchell PB (2008) A review of the
safety of repetitive transcranial magnetic stimulation as a clinical
treatment for depression. Int J Neuropsychopharmacol 11:131–147
28. Montgomery SA, Asberg M (1979) A new depression scale
designed to be sensitive to change. Br J Psychiatry 134:382–389
29. Prikryl R, Kasparek T, Skotakova S, Ustohal L, Kucerova H,
Ceskova E (2007) Treatment of negative symptoms of schizo-
phrenia using repetitive transcranial magnetic stimulation in a
double-blind, randomized controlled study. Schizophr Res
95(1–3):151–157
30. Reitan RM (1958) The relation of the trail making test to organic
brain damage. J Consult Psychology 19:393–394
31. Ringo DL, Half LM, Faustman WO (1996) Validating the St.
Hans rating scale with the abnormal involuntary movement scale
(AIMS) in the assessment of tardive dyskinesia. J Clin Psycho-
pharmacol 16(1):94–95
32. Rossini PM, Barker AT, Berardelli A, Caramia MD, Caruso G,
Cracco RQ, Dimitrijevic MR, Hallett M, Katayama Y, Lucking
CH et al (1994) Non-invasive electrical and magnetic stimulation
of the brain, spinal cord and roots: basic principles and proce-
dures for routine clinical application: report of an IFCN com-
mittee. Electroencephalogr Clin Neurophysiol 91:79–92
33. Saba G, Schurhoff F, Leboyer M (2006) Therapeutic and neu-
rophysiologic aspects of transcranial magnetic stimulation in
schizophrenia. Neurophysiol Clin 36(3):185–194
34. Sachdev P, Loo C, Mitchell P, Malhi G (2005) Transcranial
magnetic stimulation for the deficit syndrome of schizophrenia: a
pilot investigation. Psychiatry Clin Neurosci 59(3):354–357
35. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J,
Weiller E, Hergueta T, Baker R, Dubar GC (1998) The mini-
international neuropsychiatric interview: the development and
validation of a structured diagnostic psychiatric interview for
DSM-IV and ICD-10. J Clin Psychiatry 59(Suppl 20):22–33
36. Schooler NR, Hogarty GE, Weissman MM (1979) Social
Adjustment Scale II. In: Hargreaves WP, Attkisson CC, Sorenson
JE (eds) Resource materials for community health program
evaluations, 2nd edn. US Department of Health, Education, and
Welfare, Rockville, pp 290–302
37. Strafella AP, Paus T, Barrett J, Dagher A (2001) Repetitive
transcranial magnetic stimulation of the human prefrontal cortex
induces dopamine release in the caudate nucleus. J Neurosci 21
(15): RC157, 1–4
38. Tewes U (1991) Hamburg-Wechsler-Intelligenztest fur Erwach-
sene. Handbuch und Testanweisung. Revision. Verlag Hans
Huber, Bern
39. Wassermann EM (1998) Risk and safety of repetitive transcranial
magnetic stimulation: report and suggested guidelines from the
international workshop on the safety of repetitive transcranial
magnetic stimulation, June 5–7, 1996. Electroencephalogr Clin
Neurophysiol 1998:1–16
40. Winterer G, Coppola R, Egan MF, Goldberg TE, Weinberger DR
(2003) Functional and effective frontotemporal connectivity and
genetic risk for schizophrenia. Biol Psychiatry 54(11):1181–1192
Eur Arch Psychiatry Clin Neurosci (2009) 259 (Suppl 2):S189–S197 S197
123
- 34 -

2.2 Cognitive effects of high-frequency repetitive transcranial magnetic
stimulation: a systematic review
This systematic review addresses cognitive effects of long-term prefrontal high
frequency rTMS treatment. It comprises clinical rTMS trials (1999-2009) which
assessed cognitive functioning in the field of neuropsychiatry. Primary objective is the
analysis of cognitive effects with regard to the impact of clinical status (patients/
healthy volunteers) and stimulation type (active/ placebo). Results indicate that rTMS at
10-20 Hz, applied over the left DLPFC, within a range of 10-15 successive sessions and
an intensity of 80-110% of the individual motor threshold, is most effective in causing
cognitive improvement. Patients seem to benefit more than healthy participants, and
active stimulation is in some cases superior to sham stimulation. However, some studies
do not include placebo stimulation or additional healthy control groups. Systematic
investigations considering the pathophysiological and neurobiological basis of cognitive
improvement are lacking in the field. Studies comprising genetics, experimental
neurophysiology and functional brain imaging are necessary to explore stimulation
related functional changes in the brain.
- 35 -
DEMENTIAS - REVIEW ARTICLE
Cognitive effects of high-frequency repetitive transcranialmagnetic stimulation: a systematic review
Birgit Guse • Peter Falkai • Thomas Wobrock
Received: 29 April 2009 / Accepted: 7 October 2009
� Springer-Verlag 2009
Abstract Transcranial magnetic stimulation (TMS) was
introduced as a non-invasive tool for the investigation of
the motor cortex. The repetitive application (rTMS),
causing longer lasting effects, was used to study the
influence on a variety of cerebral functions. High-fre-
quency ([1 Hz) rTMS is known to depolarize neurons
under the stimulating coil and to indirectly affect areas
being connected and related to emotion and behavior.
Researchers found selective cognitive improvement after
high-frequency (HF) stimulation specifically over the left
dorsolateral prefrontal cortex (DLPFC). This article pro-
vides a systematic review of HF-rTMS studies (1999–
2009) stimulating over the prefrontal cortex of patients
suffering from psychiatric/neurological diseases or healthy
volunteers, where the effects on cognitive functions were
measured. The cognitive effect was analyzed with regard to
the impact of clinical status (patients/healthy volunteers)
and stimulation type (verum/sham). RTMS at 10, 15 or
20 Hz, applied over the left DLPFC, within a range of 10–
15 successive sessions and an individual motor threshold of
80–110%, is most likely to cause significant cognitive
improvement. In comparison, patients tend to reach a
greater improvement than healthy participants. Limitations
concern the absence of healthy groups in clinical studies
and partly the absence of sham groups. Thus, future
investigations are needed to assess cognitive rTMS effects
in different psychiatric disorders versus healthy subjects
using an extended standardized neuropsychological test
battery. Since the pathophysiological and neurobiological
basis of cognitive improvement with rTMS remains
unclear, additional studies including genetics, experimental
neurophysiology and functional brain imaging are neces-
sary to explore stimulation-related functional changes in
the brain.
Keywords Transcranial magnetic stimulation �High-frequency rTMS � Prefrontal cortex � Cognition
Abbreviations
DLFPC Dorsolateral prefrontal cortex
TMS Transcranial magnetic stimulation
rTMS Repetitive transcranial magnetic
stimulation
D Depression
BD Bipolar disorder
ExDys Executive dysfunction
H Healthy
MC Memory complaints
PD ? D Parkinson’s Disease ? Depression
Pstr D Poststroke depression
SZ Schizophrenia
PC Parietal cortex
AMI Autobiographical Memory Interview
(R)/(H)AVLT (Rey)/(Hopkins) Auditory Verbal
Learning Test
BSRT Buschke Selective Reminding Test
BVRT Benton’s Visual Retention Test
COWAT Controlled Oral Word Association
Test
CPM Colored Progressive Matrices
CPT Continuous Performance Test
CVLT California Verbal Learning Test
DSST Digit Symbol Substitution Test
B. Guse (&) � P. Falkai � T. Wobrock
Department of Psychiatry and Psychotherapy,
Georg-August-University Gottingen,
Von-Siebold-Straße 5, 37075 Gottingen, Germany
e-mail: [email protected]
123
J Neural Transm
DOI 10.1007/s00702-009-0333-7
- 36 -

EPAT Expanded Paired Associate Test
GOAT Galveston Orientation and Amnesia
Test
HVOT Hooper Visual Organization Test
JLO Judgement of line orientation
LPS Lernprufsystem
MMST Mini Mental Status Test
MPT Memory for Past Test
MVG Munchner Verbaler Gedachtnistest
NART New Adult Reading Test
NCT Number Connection Test
PAG ‘Traffic Lights Test’
SILS Shipley Institute of Living Scale
SSMQ Squire Subjective Memory
Questionnaire
Stroop Stroop Interference Test
TMT (A/B) Trail Making Test Version A/B
VFT (Letter) Verbal Fluency Test
VPAL Visual paired associates learning
WAIS(-R) Wechsler intelligence scale
(Revised)
WMS(-R)/WMSIII Wechsler memory scale
(Revised)/3 version
ExFunction Executive function
WM Working memory
Introduction
Since transcranial magnetic stimulation (TMS) was intro-
duced by Barker et al. (1985) as a non-invasive tool for the
investigation of the motor cortex, repetitive applications of
this technique (rTMS) were used to study the influence on a
variety of cerebral functions. TMS is based on an electro-
magnetic coil applied to the scalp producing an intense,
localized magnetic field which either excites or inhibits
a focal cortical area. Repetitive TMS uses alternating
magnetic fields to induce electric currents in the cortical
tissue (Burt et al. 2002). Low-frequency (B1 Hz) rTMS is
likely to cause inhibition of neuronal firing in a localized
area, whereas high-frequency ([1 Hz) rTMS inversely
leads to neuronal depolarization under the stimulating coil
(Haraldsson et al. 2004). The effects induced are not limited
to the targeted cortical region, changes can also occur at
distant interconnected sites in the brain. The efficacy of
rTMS treatment on affective disorders may not be restricted
to the activating effects under the stimulated prefrontal area,
but also due to the secondary affection of subcortical areas
being functionally related to emotion and behavior (Burt
et al. 2002; Post and Keck 2001; Ben-Shachar et al. 1997;
Conca et al. 1996; Cordes et al. 2005; Gershon et al. 2003).
Recently, rTMS has also been employed to explore the
treatment options for schizophrenia patients due to the
growing observation of non-responders to antipsychotic
agents (Hajak et al. 2004; Hoffmann et al. 2005; Jandl et al.
2004). According to different stimulation protocols evi-
dence is accumulating about the improving effect of rTMS
on acoustic hallucinations and negative symptoms in schizo-
phrenia (Hoffmann et al. 2005; Jandl et al. 2004, 2005; Poulet
et al. 2005). The well-established electroconvulsive therapy
(ECT) exhibits proven antidepressant effects, but it is also
known to produce temporary adverse cognitive effects (e.g.
memory deficits) (Squire 1982; Sackeim et al. 1986; Weiner
et al. 1986). Behind this background many rTMS studies were
used to assess cognitive functions additionally to control for
cognitive disturbances (Triggs et al. 1999; Padberg et al.
1999; Schulze-Rauschenbach et al. 2005). In contrast to the
original assumption of cognitive deterioration selective
improvements in patients after high-frequency rTMS (10 Hz
or 20 Hz) over the left prefrontal sites were observed.
This finding leads to further investigations measuring
rTMS-related cognitive changes in patients or healthy
volunteers. However, the influence of the various stimulation
parameters (e.g. frequency, intensity, train duration and
duration of whole stimulation period) on cognition and
the extent of changes in cognitive performance remained
unclear.
The aim of the presented work is to provide a systematic
overview of high-frequency rTMS (HF-rTMS) studies
assessing neurocognition for better understanding the
potential of rTMS to induce long-term effects on cognition.
In addition, the efficacy of HF-rTMS on distinct cognitive
domains will be outlined. The aim of the review is not to
summarize the effects of studies with rTMS to study cog-
nitive function by creating a ‘functional lesion’. Most of
these studies use rTMS as ‘‘online rTMS’’ to interfere
temporarily with neuronal functioning in order to gain
information about the functional contribution of the stim-
ulated area during performing a particular task (Sack
and Linden 2003). We primarily included studies in our
systematic review which investigate the after effects of
HF-rTMS, as ‘‘offline rTMS’’, at first glance independent
of the amount of rTMS sessions, but we were interested in
studies investigating cognitive effects using more than a
single rTMS session.
Method
We performed a systematic literature search in the fol-
lowing databases: PubMed (1999–2009) and MEDLINE
(1999–2009). A great range of search terms were used:
‘‘repetitive TMS’’ or ‘‘rTMS’’ and ‘‘cognition’’ or ‘‘cognitive
dysfunction’’, ‘‘cognitive impairment’’, ‘‘executive function’’,
B. Guse et al.
123
- 37 -

‘‘information processing’’, ‘‘processing speed’’, ‘‘reaction
time’’, ‘‘learning’’, ‘‘memory’’, ‘‘set shifting’’, ‘‘flexibility’’,
‘‘Wisconsin Card Sorting Test’’, ‘‘response inhibition’’,
‘‘response suppression’’, ‘‘attention’’ or ‘‘verbal fluency’’.
In the literature search, we identified 80 hits that
appeared to be suitable upon careful review of their titles
and abstracts. Of these 80 publications there were 5 studies
dealing with effects of other stimulation techniques (e.g.
transcranial direct current stimulation, tDCS) and exclu-
ded, 45 studies using low-frequency repetitive transcranial
magnetic stimulation (LF-rTMS) and 30 studies with
HF-rTMS. We then read through the full text of the 30
papers summarizing the results of HF-rTMS studies,
evaluated and included the data in our review. Review
papers and the references in the appraised studies were
therefore used for a renewed search for further relevant
literature. This did not lead to further inclusions in our
systematic review. Studies were considered only if they
had been published in English or German language and
described adequately the sample, the application procedure
and the trial design. We only included offline-paradigms.
Although we focused on high-frequency stimulation, we
initially took into account low-frequency studies (n = 45)
to better evaluate frequency-dependent cognitive changes.
A great amount of them were excluded (n = 41) subse-
quently because (1) they focus on disruptive effect mea-
sures (e.g. by inducing ‘virtual lesions’ in online-
paradigms), or (2) they focus on other topics not describing
cognitive testing or the stimulation procedure adequately
(e.g. methodology and safety studies, some case reports or
meta-analyses).
In conclusion, all studies fulfilling our predefined
selection criteria were taken into account and evaluated
according to their relative cognitive outcome.
Results
Description of the studies
The identified publications consist of 6 open studies and
24 controlled studies including within-subject-, sham-
controlled- or crossover designs. The studies comprise
22 clinical trials with major depression, that contain one
comparative trial with healthy subjects being matched to
the patient population in age, gender and level of educa-
tion. One of these studies includes patients with Parkinson
Disease and major or minor depression, one includes only
elders (between 40 and 90 years) with major depression
and another one contains post-stroke depressives. Further,
three clinical studies integrate schizophrenic patients, one
study contains patients with cerebrovascular disease and
mild executive dysfunction, another trial investigates elder
people with memory complaints. Overall, three studies
involve only healthy volunteers. The majority of the
included psychiatric patients were diagnosed and classified
on operational criterion-based systems for depression
(Diagnostic and Statistical Manual of Mental Disorder IV),
a smaller part met criteria by formal diagnostic interview
on the Structured Clinical Interview for DSM-IV Axis I
Disorders (SCID). The others were rated by means of
particular neurological/psychological tests and imaging
data. The characteristics of the included subjects, stimu-
lation protocols, cognitive ratings and outcomes of all
identified studies assessing the efficacy of rTMS on cog-
nition are outlined in Table 1.
The cognitive assessments used in the listed studies
differ from study to study, no standardized cognitive test
battery has been used consistently. Therefore, various
cognitive domains are involved to perform the selected
cognitive testing and the results of the studies are not
completely comparable.
Cognitive effects of high-frequency rTMS
over the prefrontal cortex
The differential cognitive effect of excitatory rTMS is
outlined in Table 2. Cognitive domains are subdivided and
the reported ameliorations, deteriorations or missing cog-
nitive rTMS effects are linked to the corresponding studies.
The studies were grouped by significant improvement or
deterioration in the columns, studies showing trends toward
improvements or deterioration were summarized among in
the column ‘‘no effects (n. s.)’’. One study (Vanderhasselt
et al. 2009) was not included in the table because cognitive
effects were too specific to be adequately categorized.
In the literature search about 19 studies were found
assessing changes of attention after stimulation, showing
inconsistent results. Among these studies there are 13
clinical trials and 3 non-clinical trials. In alertness/simple
reaction time no significant effect was found when mea-
sured separately (Padberg et al. 1999; Loo 2001; Shajahan
et al. 2002). With the Go-/No Go- or the Stroop-Paradigm
some authors could detect improvements in selective
attention (Hausmann et al. 2004; Martis et al. 2003;
Rektorova et al. 2005), some others did not find statistically
relevant effects (Avery et al. 2006; Boggio et al. 2005;
Huang et al. 2004; Jorge et al. 2004; Moser et al. 2002;
Mosimann et al. 2004; Speer et al. 2001; Vanderhasselt
et al. 2006; Wagner et al. 2006). One of these stud-
ies reports on deteriorations in visual reaction time in
the subtest divided attention of the ‘‘Testbatterie zur
Aufmerksamkeitsprufung (TAP, Zimmermann and Fimm
1997)’’ (Wagner et al. 2006). In sustained attention/con-
centration two studies give implications for improvements
(Hoppner et al. 2003; Rektorova et al. 2005), others failed
Cognitive effects of prefrontal rTMS
123
- 38 -

Ta
ble
1H
igh
-fre
qu
ency
rTM
San
dco
gn
itio
n
Auth
ors
Subje
cts
trea
ted/
sham
,
refe
rence
Dia
gnosi
sL
oca
tion
Whole
sess
ions/
wee
ks
Fre
quen
cyT
rain
dura
tion
Inte
rtra
in-
inte
rval
Puls
es
per
sess
ion
Moto
r
thre
shold
Cognit
ive
rati
ngs
Cognit
ive
dom
ain
Cognit
ive
effe
ct
Pad
ber
get
al.
(1999
)
(1)
6/6
(2)
6
DL
eft
DL
PF
C
5(1
)10
Hz
(2)
0.3
Hz
(1)
5s
(1)
30
s250
90% (n
.a.)
n.
a.V
erbal
lear
nin
gan
dm
emory
,
aler
tnes
s/at
tenti
on
(1)
Impro
vem
ent
inver
bal
mem
ory
(2)
No
effe
ct
Tri
ggs
etal
.
(1999
)
10
DL
eft
PF
C10/2
wee
ks
20
Hz
2s
n.
a.2,0
00
80% (n
.a.)
HV
LT
,W
AIS
-R,
CO
WA
T,
Bost
on
Nam
ing
Tes
t
Ver
bal
lear
nin
g/m
emory
,
ExF
unct
ion/W
M
Impro
vem
ent
inE
xF
unct
ion
(ver
bal
fluen
cy)
Lit
tle
etal
.
(2000
)
10
DL
eft
DL
PF
C
10/2
wee
ks
1H
z/
20
Hz
60
s/2
s5
sper
10
puls
es/
60
s
800
80% (n
.a.)
BS
RT
,C
NB
Ver
bal
/spat
ial
lear
nin
g/
mem
ory
,E
xF
unct
ion
(ver
bal
fluen
cy/r
etri
eval
)
Impro
vem
ent
of
word
reca
ll
afte
r1
wee
kin
1H
zan
d
20
Hz
condit
ion;
tren
dto
war
d
impro
ved
vis
uosp
atia
l
mem
ory
afte
r2
wee
ks
of
20
Hz
stim
ula
tion
Roll
nik
etal
.
(2000
)
12
SZ
Lef
t
DL
PF
C
10/2
wee
ks
real
?
10/2
wee
ks
sham
20
Hz
2s
61
s800
80% (n
.a.)
NC
TP
sych
om
oto
rsp
eed
No
sign
of
impro
vem
ent
Loo
etal
.
2001
9/9
DL
eft
DL
PF
C
10/ 2
wee
ks
min
.,
20/4
wee
ks
max
10
Hz
5s
25
sn.
a.110%
RM
T
RA
VL
T,
VP
AL
,
Tow
erof
London,
CO
WA
T,
MM
ST
,
AM
I,W
MS
Vis
ual
(ass
oci
ativ
e)/v
erbal
lear
nin
g/m
emory
,
ExF
unct
ion,
gen
eral
cognit
ive
stat
e,
auto
bio
gra
phic
alm
emory
,
sim
ple
and
com
ple
x
reac
tion
tim
e
No
sign
of
impro
vem
ents
;
det
erio
rati
on
inR
AV
LT
(n=
1)
Spee
ret
al.
2001
18
D,
BD
Lef
tP
FC
10/2
wee
ks
1H
z/
20
Hz
26
min
/
2s
0/2
8s
1,6
00
100%
AM
T
BS
RT
,C
olo
rado
Neu
ropsy
cholo
gic
Bat
tery
,V
erbal
/
Cat
egory
Flu
ency
Tas
k,
CP
T,
WA
IS/
SIL
S
Ver
bal
/spat
ial
lear
nin
g/
mem
ory
,E
xF
unct
ion
(ver
bal
fluen
cy,
cognit
ive
flex
ibil
ity),
atte
nti
on/
conce
ntr
atio
n,
moto
rsp
eed,
inte
llig
ence
Ten
den
cyof
impro
vem
ent
in
ver
bal
fluen
cyaf
ter
20
Hz
Mose
ret
al.
(2002
)
9/1
0D
Lef
t
DL
PF
C
520
Hz
2s
60
sn.
a.80% (n
.a.)
TM
T(A
/B),
Str
oop,
WA
IS-R
,
CO
WA
T,
Bost
on
Nam
ing
Tes
t,
RA
VL
T,
JLO
Moto
rsp
eed/a
tten
tion,
WM
/
ExF
unct
ion,
vis
ual
asso
ciat
ive
lear
nin
g,
ver
bal
lear
nin
g/m
emory
,
vis
uosp
atia
lper
cepti
on/
anal
ysi
s
Impro
vem
ent
inE
xF
unct
ion
(cognit
ive
flex
ibil
ity)
Shaj
ahan
etal
.
(2002
)
15
DL
eft
DL
PF
C
10/2
wee
ks
5,
10
or
20
Hz
4,
2,
1s
60
s500
80% RM
T
Ver
bal
fluen
cy,
WM
S-R
,W
AIS
,
DS
ST
,A
VL
T,
Tes
tof
Ever
yday
Att
enti
on,
PA
G
WM
/ExF
unct
ion,
ver
bal
lear
nin
g/m
emory
,at
tenti
on,
reac
tion
tim
e
No
sign
effe
ct
B. Guse et al.
123
- 39 -
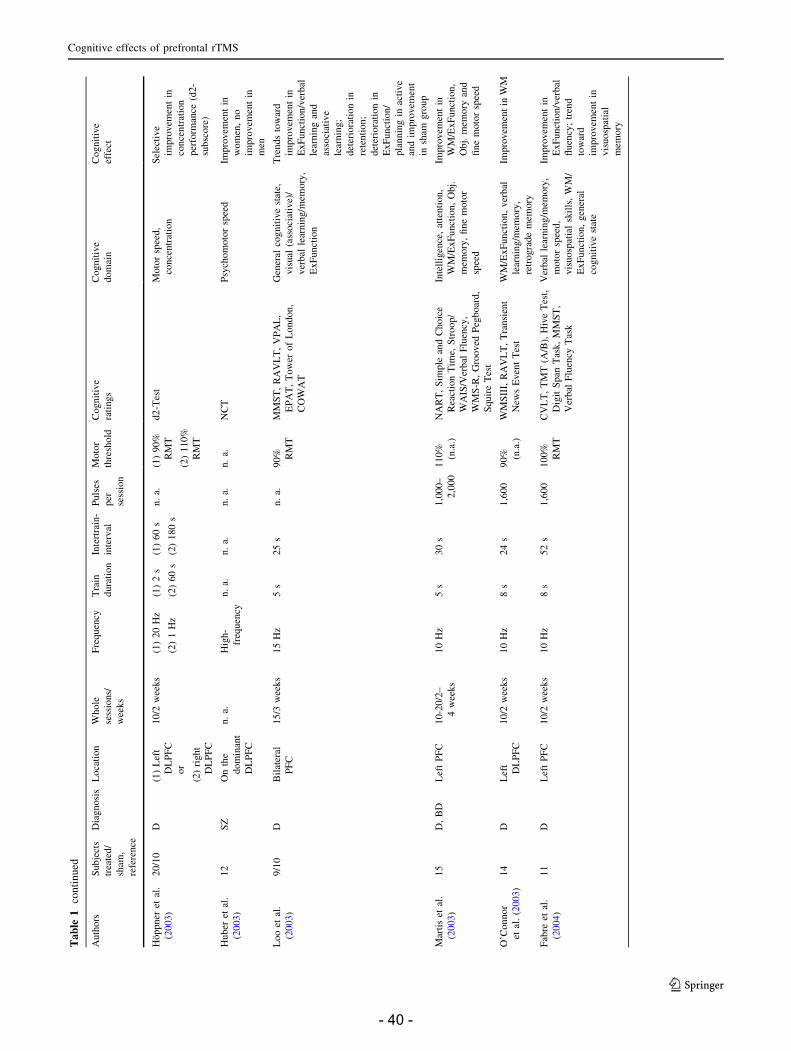
Ta
ble
1co
nti
nu
ed
Auth
ors
Subje
cts
trea
ted/
sham
,
refe
rence
Dia
gnosi
sL
oca
tion
Whole
sess
ions/
wee
ks
Fre
quen
cyT
rain
dura
tion
Inte
rtra
in-
inte
rval
Puls
es
per
sess
ion
Moto
r
thre
shold
Cognit
ive
rati
ngs
Cognit
ive
dom
ain
Cognit
ive
effe
ct
Hoppner
etal
.
(2003
)
20/1
0D
(1)
Lef
t
DL
PF
C
or
(2)
right
DL
PF
C
10/2
wee
ks
(1)
20
Hz
(2)
1H
z
(1)
2s
(2)
60
s
(1)
60
s
(2)
180
s
n.
a.(1
)90%
RM
T
(2)
110%
RM
T
d2-T
est
Moto
rsp
eed,
conce
ntr
atio
n
Sel
ecti
ve
impro
vem
ent
in
conce
ntr
atio
n
per
form
ance
(d2-
subsc
ore
)
Huber
etal
.
(2003
)
12
SZ
On
the
dom
inan
t
DL
PF
C
n.
a.H
igh-
freq
uen
cy
n.
a.n.
a.n.
a.n.
a.N
CT
Psy
chom
oto
rsp
eed
Impro
vem
ent
in
wom
en,
no
impro
vem
ent
in
men
Loo
etal
.
(2003
)
9/1
0D
Bil
ater
al
PF
C
15/3
wee
ks
15
Hz
5s
25
sn.
a.90% RM
T
MM
ST
,R
AV
LT
,V
PA
L,
EP
AT
,T
ow
erof
London,
CO
WA
T
Gen
eral
cognit
ive
stat
e,
vis
ual
(ass
oci
ativ
e)/
ver
bal
lear
nin
g/m
emory
,
ExF
unct
ion
Tre
nds
tow
ard
impro
vem
ent
in
ExF
unct
ion/v
erbal
lear
nin
gan
d
asso
ciat
ive
lear
nin
g;
det
erio
rati
on
in
rete
nti
on;
det
erio
rati
on
in
ExF
unct
ion/
pla
nnin
gin
acti
ve
and
impro
vem
ent
insh
amgro
up
Mar
tis
etal
.
(2003
)
15
D,
BD
Lef
tP
FC
10-2
0/2
–
4w
eeks
10
Hz
5s
30
s1,0
00–
2,0
00
110%
(n.a
.)
NA
RT
,S
imple
and
Choic
e
Rea
ctio
nT
ime,
Str
oop/
WA
IS/V
erbal
Flu
ency
,
WM
S-R
,G
rooved
Peg
boar
d,
Squir
eT
est
Inte
llig
ence
,at
tenti
on,
WM
/ExF
unct
ion,
Obj.
mem
ory
,fi
ne
moto
r
spee
d
Impro
vem
ent
in
WM
/ExF
unct
ion,
Obj.
mem
ory
and
fine
moto
rsp
eed
O’C
onnor
etal
.(2
003
)
14
DL
eft
DL
PF
C
10/2
wee
ks
10
Hz
8s
24
s1,6
00
90% (n
.a.)
WM
SII
I,R
AV
LT
,T
ransi
ent
New
sE
ven
tT
est
WM
/ExF
unct
ion,
ver
bal
lear
nin
g/m
emory
,
retr
ogra
de
mem
ory
Impro
vem
ent
inW
M
Fab
reet
al.
(2004
)
11
DL
eft
PF
C10/2
wee
ks
10
Hz
8s
52
s1,6
00
100%
RM
T
CV
LT
,T
MT
(A/B
),H
ive
Tes
t,
Dig
itS
pan
Tas
k,
MM
ST
,
Ver
bal
Flu
ency
Tas
k
Ver
bal
lear
nin
g/m
emory
,
moto
rsp
eed,
vis
uosp
atia
lsk
ills
,W
M/
ExF
unct
ion,
gen
eral
cognit
ive
stat
e
Impro
vem
ent
in
ExF
unct
ion/v
erbal
fluen
cy;
tren
d
tow
ard
impro
vem
ent
in
vis
uosp
atia
l
mem
ory
Cognitive effects of prefrontal rTMS
123
- 40 -

Ta
ble
1co
nti
nu
ed
Auth
ors
Subje
cts
trea
ted/
sham
,
refe
rence
Dia
gnosi
sL
oca
tion
Whole
sess
ions/
wee
ks
Fre
quen
cyT
rain
dura
tion
Inte
rtra
in-
inte
rval
Puls
es
per
sess
ion
Moto
r
thre
shold
Cognit
ive
rati
ngs
Cognit
ive
dom
ain
Cognit
ive
effe
ct
Hau
sman
n
etal
.(2
004
)
26/1
3D
(1)
left
DL
PF
Cor
(2)
bil
ater
al
DL
PF
C
(3)
sham
10/2
wee
ks
(1)
20
Hz
(2)
20
Hz
left
?1
Hz
right
10
s90
s(1
)2,0
00
(2)
2,0
00/
2,6
00
(1)
100%
RM
T
(2)
120%
RM
T
TM
T(A
/B),
Str
oop,
MV
G,
CO
WA
T
Moto
rsp
eed,
atte
nti
on,
Short
-/lo
ng-t
erm
mem
ory
,W
M/
ExF
unct
ion
Impro
vem
ent
in
colo
rnam
ing/
resp
onse
inhib
itio
n
(Str
oop);
moto
r
Spee
d/c
ognit
ive
flex
ibil
ity
(TM
T);
tren
dto
war
dbet
ter
ExF
unct
ion/v
erbal
fluen
cy
Huan
get
al.
(2004
)
24
HL
eft
DL
PF
C1
real
?1
sham
5H
z8
s23
s1,6
00
100%
(n.a
.)
TA
P(G
o/N
oG
o-
Tas
k)
Sel
ecti
ve
atte
nti
on
Nei
ther
impro
vem
ent
nor
det
erio
rati
on
in
cognit
ion
Jorg
eet
al.
(2004
)
10/1
0P
Str
DL
eft
PF
C10/2
wee
ks
10
Hz
5s
60
s1,0
00
100%
(n.a
.)
Bar
ona
Equat
ions,
MM
ST
,T
MT
(A/B
),S
troop,
CO
WA
T,
RA
VL
T,
BV
RT
,B
ost
on
Nam
ing
Tes
t,
Token
Tes
t,
WA
ISII
I,
Lin
eB
isec
tion
Tes
t
Pre
morb
id
inte
llig
ence
,gen
eral
cognit
ive
stat
e,
atte
nti
on,
ExF
unct
ion,
ver
bal
and
nonver
bal
lear
nin
g/m
emory
,
languag
e
com
pre
hen
sion/
repet
itio
n,
vis
uosp
atia
l/
vis
uoco
nst
ruct
ive
funct
ions/
neg
lect
Tre
nd
tow
ard
gen
eral
cognit
ive
impro
vem
ent;
no
dif
fere
nce
bet
wee
nac
tive
and
sham
gro
up
Mosi
man
n
etal
.(2
004
)
12/1
2D
(40–90
yea
rs)
Lef
tD
LP
FC
10/2
wee
ks
20
Hz
2s
28
s1,6
00
100%
(n.a
.)
MM
ST
,V
LT
,
Str
oop,
TM
T
A/B
,V
erbal
Flu
ency
Tas
k
Glo
bal
cognit
ive
funct
ion,
ver
bal
lear
nin
g/m
emory
,
atte
nti
on,
ExF
unct
ions
(flex
ibil
ity,
ver
bal
fluen
cy)
No
det
erio
rati
on,
no
signifi
cant
impro
vem
ent;
no
dif
fere
nce
bet
wee
n
acti
ve
and
sham
gro
up
Boggio
etal
.
(2005
)
13/1
2P
D?
DL
eft
DL
PF
C10/2
wee
ks
15
Hz
5s
n.
a.3,0
00
110%
(n.a
.)
WC
ST
,T
MT
(B),
CO
WA
T,
Str
oop,
HV
OT
,C
PM
,
Dig
itS
pan
Tes
t
WM
/ExF
unct
ion,
atte
nti
on,
vis
uosp
atia
lab
ilit
y,
reas
onin
g
Tre
nd
tow
ard
impro
vem
ent
in
ExF
unct
ion
(WC
ST
-
per
sever
atio
nan
d
Str
oop-
inte
rfer
ence
);no
dif
fere
nce
bet
wee
n
acti
ve
and
sham
gro
up
B. Guse et al.
123
- 41 -

Ta
ble
1co
nti
nu
ed
Auth
ors
Subje
cts
trea
ted/
sham
,
refe
rence
Dia
gnosi
sL
oca
tion
Whole
sess
ions/
wee
ks
Fre
quen
cyT
rain
dura
tion
Inte
rtra
in-
inte
rval
Puls
es
per
sess
ion
Moto
r
thre
shold
Cognit
ive
rati
ngs
Cognit
ive
dom
ain
Cognit
ive
effe
ct
Rek
toro
va
etal
.
(2005
)
7E
xD
ys
Lef
t
DL
PF
C
or
left
MC
1re
al?
1
sham
10
Hz
1s
10
s450
100%
(n.a
.)
TM
T(A
/B),
WA
IS-R
,
Str
oop,
VF
T,
Rey
-
Fig
ure
,W
MS
Moto
rsp
eed,
atte
nti
on,
WM
/
ExF
unct
ion,
vis
uoco
nst
ruct
ion/-
mem
ory
Sel
ecti
ve
impro
vem
ent
in
the
Str
oop-
inte
rfer
ence
afte
r
DL
PF
C
stim
ula
tion;
impro
vem
ent
in
dig
itsy
mbols
-
per
form
ance
indep
enden
tof
loca
tion
of
stim
ula
tion
Sac
hdev
etal
.
(2005
)
4S
ZL
eft
DL
PF
C
4w
eeks
15
Hz
5s
25
s1,8
00
90%
(n.a
.)M
MS
E,
Dig
itS
pan
,
TM
TA
/B,
Sym
bol-
Dig
it-C
odin
g,
Ver
bal
Flu
ency
,
WC
ST
Gen
eral
cognit
ive
stat
e,E
xF
unct
ion/
WM
(WM
,ver
bal
fluen
cy,
Cogn.
flex
ibil
ity),
psy
chom
oto
rsp
eed
No
signifi
cant
impro
vem
ent
Sch
ulz
e-
Rau
schen
bac
h
etal
.2005
16,
14/1
5D
,H
Lef
t
DL
PF
C
ca.
10
(2–3/
wee
k)
10
Hz
2s
5s
400–600
100%
(n.a
.)
AV
LT
,M
PT
,F
our-
Car
d-T
ask,
AM
I,
SS
MQ
,M
MS
T,
TM
T(A
/B),
WA
IS-
R,
Let
ter-
Num
ber
-
Span
-Tes
t,L
PS
Ver
bal
lear
nin
g/
mem
ory
,
subje
ctiv
e
mem
ory
,m
oto
r
spee
d,
WM
/
ExF
unct
ion
Impro
vem
ent
in
ver
bal
mem
ory
and
subje
ctiv
em
emory
inrT
MS
gro
up
Aver
yet
al.
(2006
)
35/3
3D
Lef
t
DL
PF
C
15/4
wee
ks
10
Hz
5s
25–30
s1,6
00
110%
RM
T
MM
ST
,R
AV
LT
,
WA
IS-R
,T
MT
(A/
B),
CO
WA
T,
Str
oop,
GO
AT
Gen
eral
cognit
ive
stat
e,ver
bal
lear
nin
g/m
emory
,
WM
/ExF
unct
ion,
moto
rsp
eed,
atte
nti
on,
ori
enta
tion
Impro
vem
ents
in
cognit
ive
funct
ions
atfo
llow
up
in
both
gro
ups
Kuro
da
etal
.
(2006
)
9D
Lef
t
DL
PF
C
10/2
wee
ks
10
Hz
5s
25
s1,0
00
100%
(n.a
.)
MM
ST
,W
MS
-R,
TM
T(A
/B)
Ass
oci
atio
n(v
erbal
)
lear
nin
g/m
emory
,
moto
rsp
eed,
ExF
unct
ion
(cognit
ive
flex
ibil
ity)
Impro
vem
ent
in
asso
ciat
ion
(ver
bal
)le
arnin
g/
mem
ory
(unre
late
d
word
s,del
ayed
reca
ll)
Cognitive effects of prefrontal rTMS
123
- 42 -

Ta
ble
1co
nti
nu
ed
Auth
ors
Subje
cts
trea
ted/
sham
,
refe
rence
Dia
gnosi
sL
oca
tion
Whole
sess
ions/
wee
ks
Fre
quen
cyT
rain
dura
tion
Inte
rtra
in-
inte
rval
Puls
es
per
sess
ion
Moto
r
thre
shold
Cognit
ive
rati
ngs
Cognit
ive
dom
ain
Cognit
ive
effe
ct
Rosa
etal
.
(2006)
20/1
5D
Lef
t
DL
PF
C
20/4
wee
ks
10
Hz
10
s20
s2,5
00
100%
(n.a
.)
WA
IS-R
,W
MS
-R,
RB
MT
ExF
unct
ion
(work
ing
mem
ory
),dif
fere
nt
com
ponen
tsof
mem
ory
No
signifi
cant
impro
vem
ent;
tren
dto
war
d
impro
vem
ent
in
RB
MT
inrT
MS
gro
up;
det
erio
rati
on
in
EC
Tgro
up
afte
r
2w
eeks
and
4w
eeks
Sole
-Pad
ull
es
etal
.(2
006
)
20/1
9M
CL
eft
PF
C1
5H
z10
s20
s500
80%
(n.a
.)F
ace-
Nam
e-M
emory
-
Tas
ks,
MM
ST
(Ass
oci
atio
n)
Lea
rnin
g/
mem
ory
,gen
eral
cognit
ive
stat
e
Impro
vem
ent
in
Ass
oci
ativ
e
Mem
ory
;no
dif
fere
nce
bet
wee
n
acti
ve
and
sham
gro
up
Van
der
has
selt
etal
.(2
006
)
28
HL
eft
DL
PF
C
1re
al?
1
sham
10
Hz
n.
a.26,
1s
1,5
60
110%
(n.a
.)
Str
oop
Pro
cess
ing
spee
d,
sele
ctiv
e
atte
nti
on
Impro
vem
ent
in
pro
cess
ing
spee
d,
i.e.
inse
lect
ive
atte
nti
on
over
all
tria
ls(c
ongru
ent/
inco
ngru
ent)
Wag
ner
etal
.
(2006)
17
HL
eft
DL
PF
C
1re
al?
1
sham
20
Hz
2s
28
s1,6
00
100%
(n.a
.)
Str
oop,
WC
ST
,T
AP
(Div
ided
Att
enti
on)
Sel
ecti
ve/
div
ided
atte
nti
on,
ExF
unct
ion
Det
erio
rati
on
in
vis
ual
reac
tion
tim
e(T
AP
)
30
min
.af
ter
stim
ula
tion;
no
(del
ayed
)ef
fect
in
ExF
unct
ion
Mogg
etal
.
(2008)
29/3
0D
Lef
t
DL
PF
C
10
10
Hz
5s
55
s1,0
00
110%
RM
T
CA
MC
OG
,W
AIS
-R,
Gro
oved
Peg
boar
dT
est
Gen
eral
cognit
ive
stat
e,
atte
nti
on,
ExF
unct
ion
(work
ing
mem
ory
),
moto
rfu
nct
ion
No
signifi
cant
effe
ct
atan
yti
me
poin
t
B. Guse et al.
123
- 43 -
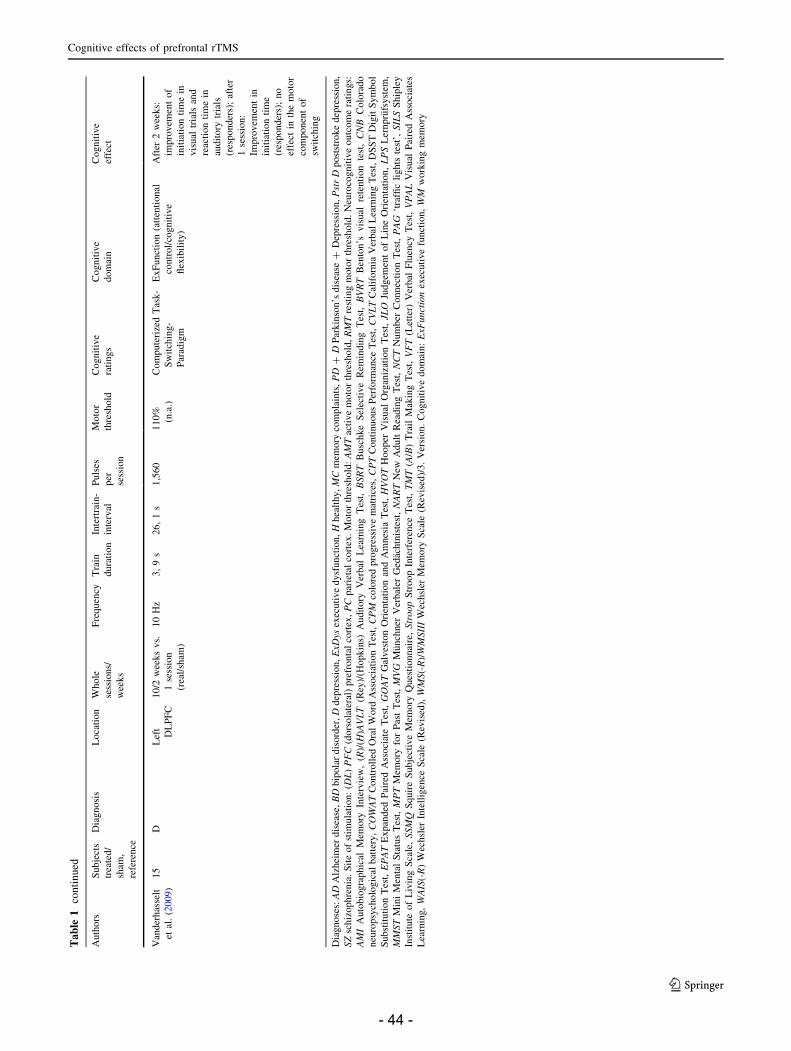
Ta
ble
1co
nti
nu
ed
Auth
ors
Subje
cts
trea
ted/
sham
,
refe
rence
Dia
gnosi
sL
oca
tion
Whole
sess
ions/
wee
ks
Fre
quen
cyT
rain
dura
tion
Inte
rtra
in-
inte
rval
Puls
es
per
sess
ion
Moto
r
thre
shold
Cognit
ive
rati
ngs
Cognit
ive
dom
ain
Cognit
ive
effe
ct
Van
der
has
selt
etal
.(2
009
)
15
DL
eft
DL
PF
C
10/2
wee
ks
vs.
1se
ssio
n
(rea
l/sh
am)
10
Hz
3,
9s
26,
1s
1,5
60
110%
(n.a
.)
Com
pute
rize
dT
ask-
Sw
itch
ing-
Par
adig
m
ExF
unct
ion
(att
enti
onal
contr
ol/
cognit
ive
flex
ibil
ity)
Aft
er2
wee
ks:
impro
vem
ent
of
init
iati
on
tim
ein
vis
ual
tria
lsan
d
reac
tion
tim
ein
audit
ory
tria
ls
(res
ponder
s);
afte
r
1se
ssio
n:
Impro
vem
ent
in
init
iati
on
tim
e
(res
ponder
s);
no
effe
ctin
the
moto
r
com
ponen
tof
swit
chin
g
Dia
gnose
s:A
DA
lzhei
mer
dis
ease
,B
Dbip
ola
rdis
ord
er,
Ddep
ress
ion,
ExD
ysex
ecuti
ve
dysf
unct
ion,
Hhea
lthy,
MC
mem
ory
com
pla
ints
,P
D?
DP
arkin
son’s
dis
ease
?D
epre
ssio
n,
Pst
rD
post
stro
ke
dep
ress
ion,
SZ
schiz
ophre
nia
.S
ite
of
stim
ula
tion:
(DL
)P
FC
(dors
ola
tera
l)pre
fronta
lco
rtex
,P
Cpar
ieta
lco
rtex
.M
oto
rth
resh
old
:A
MT
acti
ve
moto
rth
resh
old
,R
MT
rest
ing
moto
rth
resh
old
.N
euro
cognit
ive
outc
om
era
tings:
AM
IA
uto
bio
gra
phic
alM
emory
Inte
rvie
w,
(R)/
(H)A
VL
T(R
ey)/
(Hopkin
s)A
udit
ory
Ver
bal
Lea
rnin
gT
est,
BSR
TB
usc
hke
Sel
ecti
ve
Rem
indin
gT
est,
BV
RT
Ben
ton’s
vis
ual
rete
nti
on
test
,C
NB
Colo
rado
neu
ropsy
cholo
gic
albat
tery
,C
OW
AT
Contr
oll
edO
ral
Word
Ass
oci
atio
nT
est,
CP
Mco
lore
dpro
gre
ssiv
em
atri
ces,
CP
TC
onti
nuous
Per
form
ance
Tes
t,C
VL
TC
alif
orn
iaV
erbal
Lea
rnin
gT
est,
DS
ST
Dig
itS
ym
bol
Subst
ituti
on
Tes
t,E
PA
TE
xpan
ded
Pai
red
Ass
oci
ate
Tes
t,G
OA
TG
alves
ton
Ori
enta
tion
and
Am
nes
iaT
est,
HV
OT
Hooper
Vis
ual
Org
aniz
atio
nT
est,
JLO
Judgem
ent
of
Lin
eO
rien
tati
on,
LP
SL
ernpru
fsyst
em,
MM
ST
Min
iM
enta
lS
tatu
sT
est,
MP
TM
emory
for
Pas
tT
est,
MV
GM
unch
ner
Ver
bal
erG
edac
htn
iste
st,
NA
RT
New
Adult
Rea
din
gT
est,
NC
TN
um
ber
Connec
tion
Tes
t,P
AG
‘tra
ffic
lights
test
’,SIL
SS
hip
ley
Inst
itute
of
Liv
ing
Sca
le,
SSM
QS
quir
eS
ubje
ctiv
eM
emory
Ques
tionnai
re,
Str
oop
Str
oop
Inte
rfer
ence
Tes
t,T
MT
(A/B
)T
rail
Mak
ing
Tes
t,V
FT
(Let
ter)
Ver
bal
Flu
ency
Tes
t,V
PA
LV
isual
Pai
red
Ass
oci
ates
Lea
rnin
g,
WA
IS(-
R)
Wec
hsl
erIn
tell
igen
ceS
cale
(Rev
ised
),W
MS(-
R)/
WM
SII
IW
echsl
erM
emory
Sca
le(R
evis
ed)/
3.
Ver
sion.
Cognit
ive
dom
ain:
ExF
unct
ion
exec
uti
ve
funct
ion,
WM
work
ing
mem
ory
Cognitive effects of prefrontal rTMS
123
- 44 -

Table 2 Differential cognitive effects of HF rTMS
Cognitive domain Improvement No effect (n. s.) Deterioration
Attention
Alertness/Simple reaction 3 (Padberg et al. 1999; Loo 2001; Shajahan et al.
2002)
Selective/Focused attention;
Response inhibition
3 (Martis et al. 2003;
Hausmann et al. 2004;
Rektorova et al. 2005)
9 (Speer et al. 2001; Moser et al. 2002; Huang
et al. 2004 (H); Jorge et al. 2004; Mosimann
et al. 2004; Boggio et al. 2005; Avery et al.
2006; Vanderhasselt et al. 2006 (H); Wagner
et al. 2006 (H))
Divided attention 1 (Wagner et al. 2006
(H))
Sustained attention/
Concentration
2 (Hoppner et al. 2003;
Rektorova et al. 2005)
2 (Speer et al. 2001; Mogg et al. 2008)
Executive functions/Working memory
Working memory (Short-
term storage/Manipulation/
Monitoring)
2 (Martis et al. 2003;
O’Connor et al. 2003)
10 (Triggs et al. 1999; Shajahan et al. 2002;
Fabre et al. 2004; Boggio et al. 2005;
Rektorova et al. 2005; Sachdev et al. 2005;
Schulze-Rauschenbach et al. 2005; Avery
et al. 2006; Rosa et al. 2006; Mogg et al. 2008)
Cognitive flexibility 2 (Moser et al. 2002;
Hausmann et al. 2004)
10 (Speer et al. 2001; Fabre et al. 2004; Jorge
et al. 2004; Mosimann et al. 2004; Boggio
et al. 2005; Sachdev et al. 2005; Schulze-
Rauschenbach et al. 2005; Avery et al. 2006;
Kuroda et al. 2006; Wagner et al. 2006 (H))
Verbal fluency/Retrieval 3 (Triggs et al. 1999; Martis
et al. 2003; Fabre et al. 2004)
14 (Little et al. 2000; Loo 2001; Speer et al.
2001; Moser et al. 2002; Shajahan et al. 2002;
Loo et al. 2003; Hausmann et al. 2004; Jorge
et al. 2004; Mosimann et al. 2004; Boggio
et al. 2005; Rektorova et al. 2005; Sachdev
et al. 2005; Schulze-Rauschenbach et al. 2005;
Avery et al. 2006)
Problem solving/Planning/
Reasoning
2 (Loo 2001; Boggio et al. 2005) 1 (Loo et al. 2003)
Learning ? Memory (Intermediate-/Long-term storage)
Verbal learning ? Memory 3 (Padberg et al. 1999; Little
et al. 2000 (recall); Schulze-
Rauschenbach et al. 2005)
12 (Triggs et al. 1999; Speer et al. 2001; Moser
et al. 2002; Shajahan et al. 2002; Loo et al.
2003 (Learning); O’Connor et al. 2003; Fabre
et al. 2004; Hausmann et al. 2004; Jorge et al.
2004; Mosimann et al. 2004; Avery et al.
2006, Rosa et al. 2006)
2 (Loo 2001; Loo et al.
2003 (Retention))
Spatial learning ? Memory/
Objective learning ?
Memory
1 (Martis et al. 2003) 5 (Little et al. 2000; Speer et al. 2001; Fabre
et al. 2004; Jorge et al. 2004, Rosa et al. 2006)
(Visual) Associative learning
? Memory
2 (Kuroda et al. 2006; Sole-
Padulles et al. 2006)
3 (Loo 2001; Moser et al. 2002; Loo et al. 2003)
Retrograde/Autobiographic
memory
1 (Schulze-Rauschenbach et al.
2005)
2 (Loo 2001; O’Connor et al. 2003)
Psychomotor speed
Psychomotor speed/
Processing speed
4 (Martis et al. 2003;
Hausmann et al. 2004; Huber
et al. 2003 (females);
Vanderhasselt et al. 2006
(H))
13 (Rollnik et al. 2000; Loo 2001; Speer et al.
2001; Moser et al. 2002; Hoppner et al. 2003;
Huber et al. 2003 (males); Fabre et al. 2004;
Rektorova et al. 2005; Sachdev et al. 2005;
Schulze-Rauschenbach et al. 2005; Avery
et al. 2006; Kuroda et al. 2006; Mogg et al.
2008)
Vanderhasselt et al. 2009 not included; (H) healthy sample
B. Guse et al.
123
- 45 -

to find a significant effect in this domain (Mogg et al.
2008; Speer et al. 2001).
Regarding the allocated studies, about 23 assessed
executive functions/working memory in patients (21) and/or
healthy subjects (2). Significant improvements were found
in the domains working memory, cognitive flexibility and
verbal fluency/retrieval (Fabre et al. 2004; Hausmann et al.
2004; Little et al. 2000; Martis et al. 2003; Moser et al.
2002; O’Connor et al. 2003; Triggs et al. 1999; Vander-
hasselt et al. 2009). Problem solving/reasoning remained
without any beneficial but one adverse effect (Boggio et al.
2005; Loo 2001; Loo et al. 2003). In a great amount of
studies improvements were slight and failed to reach sig-
nificance, but a variety of studies report on trends (for more
details see, Tables 1, 2).
Concerning the results of the learning and memory
section there are 19 studies quantifying this dimension.
Little et al. (2000), Padberg et al. (1999) and Schulze-
Rauschenbach et al. (2005) discovered verbal learning/
memory improvements, but a great range of authors did
not find such statistically relevant effects (see, Table 2).
Loo (2001) found an individual temporary deterioration
in verbal learning/memory, two years later the same
group manifested a selective deterioration in the retention
of verbal material (Loo et al. 2003). However, amelio-
rations were reported in spatial and objective learning/
memory (Little et al. 2000; Martis et al. 2003). In other
studies subjects did not exhibit any relevant objective
memory change (Fabre et al. 2004; Jorge et al. 2004;
Speer et al. 2001). Subjects of other studies reached high
scores in associative learning/memory (Kuroda et al.
2006; Sole-Padulles et al. 2006) and in autobiographic
memory (Schulze-Rauschenbach et al. 2005). Missing
effects in the latter categories are described by Loo et al.
(2001, 2003), Moser et al. (2002) and O’Connor et al.
(2003).
As much as 16 studies explicitly assessed psychomotor
speed/processing speed with the Trail-Making-Test (Ver-
sion A), the d2-Test or the Stroop-Paradigm. Overall, three
studies stated improved psychomotor speed in different
tasks (Hausmann et al. 2004; Martis et al. 2003; Vander-
hasselt et al. 2006), one found gender differences in terms
of improvements in women and no improvements in men
(Huber et al. 2003), the others did not find relevant effects
(for details see, Table 2).
Effect of clinical status and stimulation type
on cognitive changes
As mentioned above our review reports the results of 27
clinical studies (involving patients with distinct diseases)
and 3 non-clinical studies (including only healthy volun-
teers). At first, we compare the different groups with regard
to the cognitive stimulation effect. We then summarize the
stimulation parameters in terms of their relative cognitive
effect. Finally, we contrast the stimulation conditions ‘‘real
(verum)’’ and ‘‘placebo (sham)’’ to give an overview of
placebo- or real rTMS-induced effects.
Clinical versus non-clinical group
One of the non-clinical groups stimulating over the (left)
PFC showed ameliorations in processing speed (Vander-
hasselt et al. 2006), whereas the others did not exhibit
relevant improving effects (Huang et al. 2004; Wagner
et al. 2006). However, Wagner et al. (2006) found an
individual deterioration in divided attention (visual reac-
tion time was slowed). Over all non-clinical groups a single
amelioration (in processing speed) can be manifested.
Regarding the clinical groups, there are 22 reported ame-
liorations spanning the domains attention (selective, sus-
tained), executive functions (working memory, cognitive
flexibility and verbal fluency/retrieval), learning and
memory (verbal, nonverbal) and processing speed. Never-
theless, a great number of studies did not find significant
effects over these domains (Table 2). Deteriorations are
reported in verbal learning/memory (Loo 2001; Loo et al.
2003) and in planning (Loo et al. 2003).
Stimulation parameters
In the majority of studies (18) subjects had 10 stimulation
sessions in 2 weeks (see, Table 1). The frequencies range
between 10 Hz and 20 Hz, the motor threshold between 80
and 100%. There is a notable difference between intertrain
intervals ranging from 5 s over 24–28 s up to about 60–
90 s. In consideration of all positive cognitive outcomes
(15), those studies using stimulation frequencies of 10 Hz
up to 20 Hz over a period of 2 up to 4 weeks (22) seem to
be most effective. Two studies which attained significant
improving effects with 10–20 Hz assessed five rTMS ses-
sions only (Moser et al. 2002; Triggs et al. 1999), in the
two other studies participants received one sham and one
real rTMS session (Rektorova et al. 2005; Vanderhasselt
et al. 2006). Seven studies with abovementioned stimula-
tion parameters (10–20 Hz, 2–4 weeks) are lacking sig-
nificant cognitive improvement, but indicate a trend of
cognitive amelioration anyhow (Boggio et al. 2005; Jorge
et al. 2004; Loo et al. 2003; Mosimann et al. 2004; Rosa
et al. 2006; Speer et al. 2001). Three others do not report
on any improving effect at these stimulation conditions
(Loo 2001; Mogg et al. 2008; Shajahan et al. 2002). With
regard studies using frequencies at the lower end of the
high-frequency range (5 Hz), there were no marked
improvements in cognitive functions (Huang et al. 2004;
Shajahan et al. 2002), one study found a tendency of
Cognitive effects of prefrontal rTMS
123
- 46 -

cognitive ameliorations (Sole-Padulles et al. 2006), but,
except for the latter case, the studies are composed of
single stimulation sessions.
Onset of cognitive measure
We looked into the studies to identify the time interval
between last rTMS administration and test onset. All
studies performed baseline cognitive testing prior or one
day before the first rTMS session. Most studies (19)
reported on cognitive measures the day of completing all
sessions without specifying the exact onset (Avery et al.
2006; Boggio et al. 2005; Hausmann et al. 2004; Hoppner
et al. 2003; Huber et al. 2003; Jorge et al. 2004; Loo
2001; Loo et al. 2003; Mogg et al. 2008; Moser et al.
2002; Mosimann et al. 2004; O’Connor et al. 2003;
Padberg et al. 1999; Rollnik et al. 2000; Rosa et al. 2006;
Sachdev et al. 2005; Speer et al. 2001; Triggs et al. 1999;
Vanderhasselt et al. 2006). Among these studies 18 used
frequencies of 10–20 Hz over a longer period (10–20
sessions (n = 16), 5 sessions (n = 2)), but only 6 of them
described significant positive cognitive outcomes being
associated with rTMS intervention. The others mainly
showed either a trend of cognitive improvement in verum
group or did not detect differences between groups (see,
Sect. Discussion). Two further studies exhibited tempo-
rary deteriorations.
The other studies described adequately the delay
between stimulation and test onset ranging from immediate
testing (Huang et al. 2004; Rektorova et al. 2005; Shajahan
et al. 2002; Sole-Padulles et al. 2006), 10–30 min (Little
et al. 2000; Wagner et al. 2006; Vanderhasselt et al. 2009),
20–24 h (Fabre et al. 2004), one or 3 days (Kuroda et al.
2006; Martis et al. 2003) up to one week (Schulze-Raus-
chenbach et al. 2005). Five studies integrated follow-up
measures (Boggio et al. 2005; Hoppner et al. 2003; Mogg
et al. 2008; O’Connor et al. 2003; Triggs et al. 1999), eight
studies intermediate measures (Triggs et al. 1999; Loo
2001; Rollnik et al. 2000; Shajahan et al. 2002; Little et al.
2000; O’Connor et al. 2003; Rosa et al. 2006; Vander-
hasselt et al. 2009).
Verum versus sham stimulation
Overall, 19 studies are sham-controlled, among these
studies 7 are designed crossover and ‘‘within subject’’ or
‘‘within group’’. Two of these studies were excluded
because of a small sham-sample (Little et al. 2000) or of
only a single sham session crossover (Vanderhasselt et al.
2009). For the sham procedure there were 13 studies using
active coils angulated at 45� or 90� and 4 studies using
sham coils. Therefore, we did not perform a comparison of
the different sham procedures. In the presentation of results
we only considered the main outcome of each analysis. The
impact of clinical status and stimulation condition (real vs.
sham) is outlined in regard to the relative cognitive effect
in Table 3.
Thus, individual (may be opposing) results were not
listed separately, but integrated in the overall report.
According to the hypothesis, 7 studies confirm a signifi-
cantly greater improvement of cognition in verum than in
sham condition. Another 8 studies do not reveal relevant
differences in cognition between stimulation conditions (in
terms of no significant improvement in both conditions).
The latter studies include trends toward improvements as
well as significant improvements in individual domains
that are not reported in detail. For that reason a reclassifi-
cation of some cases into the last category (‘‘overall cog-
nitive improvement’’, see Table 3) can be argued. There is
no greater sham than verum effect, but interestingly, one
study implicates a selective advantage in a planning task of
sham over verum stimulation (Loo et al. 2003). Two
studies report on overall cognitive improvement, i.e.
ameliorations in both stimulation conditions (Avery et al.
2006; Sole-Padulles et al. 2006), that could be due to
practice or placebo effects.
High-frequency versus low-frequency stimulation
Low-frequency studies meeting the predefined criteria are
outlined in Table 4. To overview their cognitive outcome,
low-frequency stimulation (=1 Hz) seems to deteriorate
cognitive functioning in lieu of having improving effects.
Table 3 Comparison sham
versus verum stimulation in
high-frequency studies: main
outcome
Group specific cognitive effect Studies contrasting real and placebo stimulation
No significant improvement: Verum =
Sham
8 (Loo 2001; Loo et al. 2003; Hausmann et al. 2004; Huang et al.
2004; Jorge et al. 2004; Mosimann et al. 2004; Boggio et al.
2005; Mogg et al. 2008)
Selective improvement: Verum[Sham 7 (Padberg et al. 1999; Rollnik et al. 2000; Speer et al. 2001;
Moser et al. 2002; Hoppner et al. 2003; Vanderhasselt et al.
2006; Wagner et al. 2006)
Selective improvement: Sham[Verum n. a.
Overall improvement (placebo-/
practice effect): Verum = Sham
2 (Avery et al. 2006; Sole-Padulles et al. 2006)
B. Guse et al.
123
- 47 -

Ta
ble
4L
ow
-fre
qu
ency
rTM
San
dco
gn
itio
n
Au
tho
rsS
ub
ject
s
trea
ted
/
sham
,
refe
ren
ce
Dia
gn
osi
sL
oca
tio
nW
ho
le
sess
ion
s/
wee
ks
Fre
qu
ency
(Hz)
Tra
in
du
rati
on
(min
)
Inte
rtra
in-
inte
rval
Pu
lses
per
sess
ion
Mo
tor
thre
sho
ld
Co
gn
itiv
e
rati
ng
s
Co
gn
itiv
e
do
mai
n
Co
gn
itiv
e
effe
ct
Fit
zger
ald
etal
.
(20
05
)
17
/16
SZ
(au
dit
ory
hal
luci
nat
ion
s)
TP
3(1
0-
20
-EE
G-
Sy
stem
)
10
/2w
eek
s1
15
–n
.a.
90
%R
MT
HV
LT
,v
erb
al
flu
ency
,d
igit
span
(fo
rwar
ds,
bac
kw
ard
s/
vis
uo
spat
ial)
,
VS
MT
Ver
bal
lear
nin
gan
d
mem
ory
,W
M/
exec
uti
ve
fun
ctio
n
No
det
erio
rati
on
in
cog
nit
ive
test
ing
Fre
gn
i
etal
.
(20
06
)
12
/9M
CD
,
refr
acto
ry
epil
epsy
Sit
eo
f
lesi
on
51
20
–1
,20
07
0%
max
.
stim
ula
tor
ou
tpu
t
Dig
itsp
an(f
orw
ard
,
bac
kw
ard
),si
mp
le
reac
tio
n,
Str
oo
p
test
WM
/Ex
Fu
nct
ion
,
sim
ple
reac
tio
n
tim
e,se
lect
ive
atte
nti
on
Sig
nifi
can
t
imp
rov
emen
tin
sim
ple
reac
tio
n
tim
ean
dS
tro
op
Tas
k;
no
effe
ctin
sho
rtte
rm/w
ork
ing
mem
ory
Jan
uel
etal
.
(20
06
)
11
/16
DR
igh
t
DL
PF
C
16
/4w
eek
s:
1./
2.
wee
k
dai
ly,
3./
4.
wee
kev
ery
two
day
s
12
91
3m
inn
.a.
90
%(n
.a.)
Gro
ber
and
Bu
sch
ke’
sT
est,
Str
oo
pT
est,
TM
T,
WA
IS-R
,
Car
deb
at’s
Flu
ency
Tes
t
Ver
bal
lear
nin
gan
d
mem
ory
,
sele
ctiv
e
atte
nti
on
,
psy
cho
mo
tor
spee
d,
Ex
Fu
nct
ion
No
sig
n.
dif
fere
nce
s
(Bas
elin
e/D
ay1
4)
Tro
jan
o
etal
.
(20
06
)
16
/8H
P3
(n=
8)
or
P4
(n=
8)
(10
-20
-
EE
G-
Sy
stem
)
11
10
–6
00
80
%(n
.a.)
Co
ord
inat
eta
sk,
cate
go
rica
lta
sk
Pro
cess
ing
of
cate
go
rica
lan
d
coo
rdin
ate
spat
ial
rela
tio
ns
Sel
ecti
ve
det
erio
rati
on
of
fun
ctio
nin
gin
acti
ve
gro
up
(im
med
iate
lyaf
ter
rTM
San
d1
0m
in.
afte
rrT
MS
),
pro
gre
ssiv
e
imp
rov
emen
tin
con
tro
lg
rou
p
Dia
gn
ose
s:D
Dep
ress
ion
,E
xDys
exec
uti
ve
dy
sfu
nct
ion
,H
hea
lth
y,
MC
Dm
ild
cog
nit
ive
dis
ord
er,
SZ
sch
izo
ph
ren
ia.
Neu
roco
gn
itiv
eo
utc
om
era
tin
gs
(H)A
VL
T(H
op
kin
s)A
ud
ito
ryV
erb
al
Lea
rnin
gT
est,
TM
TT
rail
Mak
ing
Tes
t,V
SM
TV
isu
osp
atia
lM
emo
ryT
est.
Mo
tor
thre
sho
ld:
AM
Tac
tiv
em
oto
rth
resh
old
,R
MT
rest
ing
mo
tor
thre
sho
ld.C
og
nit
ive
do
mai
n:
ExF
un
ctio
nex
ecu
tiv
e
fun
ctio
n,
WM
wo
rkin
gm
emo
ry
Cognitive effects of prefrontal rTMS
123
- 48 -

One study described improved simple reaction times and
better scores in the Stroop Task, but this had been associ-
ated with a reduced seizure activity in epilepsy patients by
the authors (Fregni et al. 2006). Two studies report no
worsening cognitive effects (Fitzgerald et al. 2005; Januel
et al. 2006), and one study by Trojano et al. (2006) referred
a selective deterioration of functioning directly and after
10 min of 1-Hz stimulation.
Discussion
Overall results and limitations of the studies
To summarize the results, we can state that high-frequency
rTMS (10–20 Hz) is most likely to cause significant cog-
nitive improvement when applied over the left (dorsolat-
eral) prefrontal cortex, within a range of 10–15 successive
sessions and an individual motor threshold between 80 and
110%. Regarding the analyses of clinical status and stim-
ulation condition concerning the efficacy of rTMS, the
clinical group is superior to the non-clinical group and
verum stimulation is in general superior to sham stimula-
tion. All in all, many studies failed to demonstrate signif-
icant cognitive effects, but they could show trends toward
selective cognitive improvements. In comparison with
studies using 1-Hz stimulation, high-frequency studies
seem to be superior concerning the cognitive outcome.
However, the evaluation is limited due to partly method-
ological differences between and within studies or to the
marginal number of low-frequency studies. General limi-
tations concern the absence of healthy control groups as
well as sham conditions to some extent. Important to note
is the marginal number of studies using functional imaging
and integrating follow-up measures for the exploration of
long-term effects. The relative high number of studies
giving evidence of placebo or practice effects requires
future amendment of control conditions. There are dis-
crepancies concerning the onsets of cognitive testing after
rTMS administration being substantially relevant for the
outcome. Therefore, results seem to be inconsistent
throughout the literature and the particular biological
mechanism of rTMS for cognitive improvement seems to
be questionable until the underlying pathophysiology
remains unclear. We do not know how long the effects of
rTMS on cognitive function will persist. Studies investi-
gating systematically the duration of the induced cognitive
effects are lacking, but one can assume, based on the
remaining effects on psychopathology (e.g. improvement
of mood), that also the cognitive improvement will persist
for a certain period of time. Future work is needed to
systematically investigate the impact of different test
onsets after rTMS application.
It should also be further addressed that the correct
positioning of the coil is important for the effects of rTMS.
Most of the studies used the method of Pascual-Leone
(placing the coil 5 cm rostrally from the hot spot of pri-
mary motor cortex) to identify the DLPCF or localized the
left DLPFC by the 10-20 EEG-system. While recent
studies on neuronavigation for TMS have shown that ste-
reotactically neuronavigated TMS results in stronger and
more robust TMS effects, neuronavigation may be impor-
tant for inducing long-lasting cognitive improvement. For
example, one study demonstrated a systematic difference in
the behavioral effect size due to the way of localization.
Individual fMRI-guided TMS neuronavigation yielded the
strongest and the 10-20 EEG-system stimulation approach
the smallest behavioral effect size (Sack et al. 2009). There
was a nearly tenfold increase in the needed number of
probands to induce the same behavioral effect when using
the 10-20 system compared to fMRI-guided neuronaviga-
tion. In addition, a previous study demonstrated clearly that
in most cases the DLPFC was not targeted correctly when
compared to the commonly used method of Pascual-Leone
with neuronavigated coil positioning (Herwig et al. 2001).
Effects on different cognitive domains
To discuss the effect of rTMS on attention, one has to
consider the different elements that build attentional pro-
cesses. A basal part of attention is the alertness, which is
generally separated in tonic alertness, representing the
enduring alert state over the day, and phasic alertness,
implying the temporary enhancement of this state due to an
internal or external stimulus (Posner 1975). The mainte-
nance of concentration over a longer period of time under
monotonous stimulus conditions is called sustained atten-
tion (Davies et al. 1984), whereas divided attention is
commonly characterized by keeping on line two or more
currently relevant (classes of) stimuli or mental operations
at the same time. Therefore, divided attention requires the
simultaneous monitoring of different information channels
to quickly detect relevant events and to execute actions
according to the actual demand (Posner and Boies 1971).
The essential function of selective or focused attention is
the selection of a particular subset of the available stimuli
for preferential processing and, consequently, the simulta-
neous suppression of currently irrelevant information
(Kinchla 1992). Important to note is that the concept of
divided and selective attention is closely connected to the
concept of executive functions. The studies reviewed in our
work mainly found improvements in selective and sus-
tained attention, not in alertness. The concept of executive
function describes higher cognitive processes like problem
solving, mental planning, initiation and inhibition of
behavior as well as action control. The main function of the
B. Guse et al.
123
- 49 -

executive system is monitoring cognitive (sub-) processes
and their flexible dynamic regulation due to changing
environments. Such adaptive behavior necessitates a flex-
ible mind, which maintains and updates currently relevant
information and exerts top–down control over the percep-
tion of incoming information and execution of outgoing
behavior. This control is most commonly associated with
the anterior pole of the brain, the prefrontal cortex (PFC)
(Fuster 1987; Miller and Cohen 2001; Chao and Knight
1995). For successfully using executive control the ability
of dynamic attentional shifting is necessary. Working
memory consists of the short-term storage of incoming
information and a set of executive processes. Short-term
storage involves the active maintenance of a limited
amount of information for a matter of seconds and is a
necessary component of many higher cognitive functions
mediated in part by the prefrontal cortex (PFC). The
executive component implies the mental manipulation of
maintained information (Carpenter et al. 1990; Fuster
1987; Goldmann-Rakic (1997); Stuss and Benson 1986).
Therefore, working memory is often operationalized by
continuous performance tasks requiring the permanent
maintenance and manipulation of incoming information.
As executive function and working memory were attrib-
uted to prefrontal cortex, one could expect a significant
influence of rTMS on these cognitive domains. Neverthe-
less, the presented studies do not exhibit high significances.
They mainly report on improvements in ‘‘working mem-
ory’’, ‘‘cognitive flexibility’’ or ‘‘verbal fluency’’, but there
are no effects in problem solving, planning or reasoning.
Maybe such higher cognitions require too specific modu-
lations of activity than they could be effectively modified
by rTMS. We do not know whether executive improve-
ments underlie alterations in basic functions like attention
or concentration.
Concerning the learning and memory section, memory
refers to intermediate- and long-term storage of informa-
tion and has to be distinguished from short-term storage or
working memory described above. It contains the encod-
ing, consolidation and retention of verbal and nonverbal
material. Therefore, tasks used are requiring the immediate
and delayed free recall or cued recognition of information.
With regard to the well known memory complaints after
electroconvulsive therapy (ECT), it is important to note
that no marked memory deficits have been found after
rTMS. In addition to this outcome beneficial therapeutic
(e.g. antidepressant) effects have been the consequence.
RTMS (compared to ECT) seems to be a more sensitive
technique while exhibiting therapeutic and even improving
cognitive effects.
Psychomotor speed/processing speed describes the time
a person needs to process incoming stimuli and to ade-
quately react to them or initiate behavior, e. g. connecting
numbers as fast as possible in ascending order. Only a few
studies indicate significant increase in processing/motor
speed when measured solely.
All in all, there are inconsistencies between results that
may be attributed to differences in methodology (e.g.
stimulation protocols, number of sessions, for details see,
Table 1) or sample constitution. Missing statistical power
in some cases may be due to marginal psychometric
test properties. The evaluation of results is difficult on
account of the sometimes overlapping contents of cognitive
domains.
What kind of cerebral changes due to rTMS may result
in improving behavioral outcomes?
Regarding the differential rTMS effects throughout the
literature, evidence is growing about the modification of
cerebral blood flow, glucose metabolism and neuronal
excitability in the stimulated area as well as in intercon-
nected brain regions (Conca et al. 2002; Fox et al. 1997).
Moreover, short-/long-term potentiation of synapses and
rapid dynamic alterations in gray matter (GM) density are
reported (Esser et al. 2006; May et al. 2007). The latter
result resembles structural changes in normal learning
mechanisms that could be triggered by high-frequency
rTMS pulses. The reported dynamic shift of gray matter
density after about 5 days of stimulation is attended by
clinical ameliorations within the same time. The occur-
rence of structural alterations mirrored by changes in
functional processing exemplifies structural neuroplastic-
ity as a counterpart of function. Furthermore, there is a
large body of literature suggesting an association of
hypofrontality in schizophrenia with negative symptoms
and cognitive deficits (Dolan et al. 1993; George and
Belmaker 2000; Weinberger et al. 1988). High-frequency
rTMS (especially at 10 Hz) seems to be a promising
technique to improve such negative symptoms (Hajak
et al. 2004; Cordes et al. 2005; Jin et al. 2006). Conse-
quently, high-frequency rTMS can be suggested to be able
to evoke improvements in both negative symptoms and
cognition. The herein reviewed rTMS studies assessing
cognition in schizophrenia did not show convincing
effects toward a cognitive improvement. Additionally, it
remains unclear whether structural changes, alterations in
metabolism or neurotransmission under the stimulated
area or in the connected neuronal network (or the com-
bination of all) may produce behavioral outcomes (e.g.
May et al. 2007; Strafella et al. 2001). Regarding the
stimulation location (PFC) one could expect improve-
ments in most of the abovementioned cognitive functions,
because they all underlie (at least in part) this area.
Nevertheless, the results of the studies do not exhibit such
consistent pattern.
Cognitive effects of prefrontal rTMS
123
- 50 -

The mechanism how rTMS may lead to an improvement
of cognitive function is rather complex and raises some
difficulties in interpretation. TMS-induced enhancement of
performance might be the result of the excitation of a
functionally relevant task-supporting activation, the exci-
tation of an area that inhibits competing functions, the
inhibition of an area that suppresses the execution of the
task, or the inhibition of an area that promotes competing
functions (Sack and Linden 2003). This is complicated by
the fact that the same stimulation pattern (e.g. supra-
threshold rTMS with 10 Hz) could lead to different effects
on cerebral blood flow depending on the stimulation site
(e.g. increase when stimulating the frontal eye field and
decrease during rTMS of the primary motor cortex) (Sack
and Linden 2003). The effects of rTMS also depend on the
history of synaptic activity in the stimulated region. For
example, if 6-Hz rTMS is applied for a short period (below
the threshold for any lasting after-effects), then the sup-
pressive effect of a subsequent period of 1-Hz rTMS is
enhanced (Ridding and Rothwell 2007). Generally, a prior
history of increased activity seems to increase the effec-
tiveness of rTMS protocols that decrease excitability,
whereas a prior history of reduced activity increases the
effect of facilitatory rTMS.
Further differential investigations are necessary to
expand knowledge of rTMS functioning and the under-
lying biological mechanisms by linking structural and
functional imaging data (including spectroscopy data)
with behavioral outcome variables. For a detailed analysis
of functional cerebral alterations, the rTMS procedure
could be conducted during fMRI-scanning. Such a
simultaneous approach provides the opportunity to
investigate the local response to TMS at a neurophysio-
logical level with high spatial resolution, thus helping to
determine in vivo the brain areas that are directly or
transsynaptically affected by TMS. Nevertheless using
fMRI tends to create also problems with interpretation;
for example, whether changes in perfusion or BOLD
signal reflect changes in excitatory, inhibitory or com-
bined neural activity.
An interesting topic in this context could also be to
evaluate and compare the contrast of brain alterations and
differences in activated neuronal networks in diseased
and healthy people to explore different coping strategies.
All in all, investigations have to prove the efficacy of
rTMS in randomized sham-controlled trials with higher
statistical power using larger sample sizes and improved
methodology. This may even become more interesting
while stimulation protocols inducing longer-lasting
effects like theta-burst stimulation (TBS) have been
developed. Currently studies are underway to test these
TBS in terms of affecting not only motor response, but
also cognition.
Acknowledgments T. Wobrock is a member of a speakers’ bureau
for AstraZeneca, Eli Lilly and Janssen-Cilag, and has accepted paid
speaking engagements in industry-sponsored symposia from Astra-
Zeneca, Bristol-Myers-Squibb, Eli-Lilly, Janssen Cilag and Pfizer,
and travel or hospitality not related to a speaking engagement from
Astra Zeneca, Bristol-Myers-Squibb, Eli Lilly, Janssen Cilag, and
Sanofi-Synthelabo, and received a research grant from Astra Zeneca.
B. Guse reports no competing interests.
References
Avery DH, Hotzheimer PE, Fawaz W, Russo J, Neumaier J, Dunner
DL, Haynor DR, Claypoole KH, Wajdik C, Roy-Byrne P (2006)
A controlled study of repetitive transcranial magnetic stimula-
tion in medication-resistant major depression. Biol Psychiatry
59:187–194
Barker AT, Jalinous R, Freeston IL (1985) Non-invasive magnetic
stimulation of human motor cortex (letter). Lancet 1:1106–1107
Ben-Shachar D, Belmaker RH, Grisaru N, Klein E (1997) Transcra-
nial magnetic stimulation induces alternations in brain mono-
amines. J Neural Transm 104:191–197
Boggio PS, Fregni F, Bermpohl F, Mansur CG, Rosa M, Rumi DO,
Barbosa ER, Rosa MO, Pascual-Leone A, Rigonatti SP, Marc-
olin MA, Silva MTA (2005) Effect of repetitive TMS and
fluoxetine on cognitive function in patients with Parkinson’s
disease and concurrent depression. Brief reports. Mov Disord
20(9):1178–1219
Burt T, Lisanby SH, Sackheim HA (2002) Neuropsychiatric appli-
cations of transcranial magnetic stimulation: a meta analysis. Int
J Neuropsychopharmacol 5:73–103
Carpenter PA, Just MA, Shell P (1990) What one intelligence test
measures: a theoretical account of the processing in the Raven
Progressive Matrices Test. Psychol Rev 97:404–431
Chao LL, Knight RT (1995) Human prefrontal lesions increase
distractibility to irrelevant sensory inputs. Neuroreport 21:1605–
1610
Conca A, Koppi S, Konig P, Swoboda E, Krecke N (1996)
Transcranial magnetic stimulation: a novel antidepressive strat-
egy? Neuropsychobiology 34:204–207
Conca A, Peschina W, Konig P, Fritzsche H, Hausmann A (2002)
Effect of chronic repetitive transcranial magnetic stimulation on
regional cerebral blood flow and regional glucose uptake in drug
treatment-resistant depressives: a brief report. Neuropsychobi-
ology 45:27–31
Cordes J, Mobascher A, Arends M, Agelink MW, Klimke A (2005)
A new method for the treatment of depression: Transcranial
magnetic stimulation. Dtsch Med Wochenschr 130:889–892
Davies DR, Jones DM, Taylor A (1984) Selective and sustained-
attention tasks: Individual and group differences. In: Parasur-
aman R, Davies DR (eds) Varieties of Attention. Academic,
Orlando
Dolan RJ, Bench CJ, Liddle PF (1993) Dorsolateral prefrontal cortex
dysfunction in the major psychoses: symptoms or disease
specificity? J Neurosurg Psychiatr 56:1290–1294
Esser SK, Huber R, Massimini M, Peterson MJ, Ferrarelli F, Tononi
G (2006) A direct demonstration of cortical LTP in humans: A
combined TMS/EEG study. J Brain Res Bull 69(1):86–94
Fabre I, Galinowski A, Oppenheim C, Gallarda T, Meder JF, de
Montigny C, Olie JP, Poirier MF (2004) Antidepressant efficacy
and cognitive effects of repetitive transcranial magnetic stimu-
lation in vascular depression: an open trial. Int J Geriatr
Psychiatry 19:833–842
Fitzgerald PB, Benitez J, Daskalakis JZ, Brown TL, Marston N, de
Castella A, Kulkarni J (2005) A double-blind sham-controlled
B. Guse et al.
123
- 51 -

trial of repetitive transcranial magnetic stimulation in the
treatment of refractory auditory hallucinations. J Clin Psycho-
pharmacol 25(4):358–362
Fox P, Ingham R, George MS, Mayberg H, Ingham J, Roby J, Martin
C, Jerabek P (1997) Imaging human intra-cerebral connectivity
ba PET during rTMS. Neuroreport 8:2787–2791
Fregni F, Otachi P, do Valle A, Boggio PS, Thut G, Rigonatti S,
Pascual-Leone A, Valente KD (2006) A randomized clinical trial
of repetitive transcranial magnetic stimulation in patients with
refractory epilepsy. Ann Neurol 60:447–455
Fuster JM (1987) The prefrontal cortex: anatomy, physiology, and
neuropsychology of the frontal lobe. Lippincott-Raven, New
York
George MS, Belmaker RH (2000) Transcranial magnetic stimulation
in neuropsychiatry. American Psychiatric Association,
Washington
Gershon AA, Dannon PN, Grunhaus L (2003) Transcranial magnetic
stimulation in the treatment of depression. Am J Psychiatry
160:835–845
Goldmann-Rakic PS (1997) Circuitry of primate prefrontal cortex and
regulation of behaviour by representational memory. In: Plum F
(ed) Handbook of physiology. Nervous system, vol 5. Higher
functions of the brain. American Physiological Society,
Bethesda, pp 373–417
Hajak G, Marienhagen J, Langguth B, Werner S, Binder H,
Eichhammer P (2004) High frequency transcranial magnetic
stimulation in schizophrenia: a combined treatment and neuro-
imaging study. Psychol Med 34:1157–1163
Haraldsson HM, Ferrarelli F, Kalin NH, Tononi G (2004) Transcra-
nial magnetic stimulation in the investigation and treatment of
schizophrenia: a review. Schizophr Res 71:1–16
Hausmann A, Pascual-Leone A, Kemmler G, Rupp CI, Lechner-
Schoner T, Kramer-Reinstadler K, Walpoth M, Mechtcheriakov
S, Conca A, Weiss EM (2004) No deterioration of cognitive
performance in an aggressive unilateral and bilateral antidepres-
sant rTMS add-on trial. J Clin Psychiatry 65(6):772–782
Herwig U, Padberg F, Unger J, Spitzer M, Schonfeldt-Lecuona C
(2001) Transcranial magnetic stimulation in therapy studies:
examination of the reliability of ‘‘standard’’ coil positioning by
neuronavigation. Biol Psychiatry 50(1):58–61
Hoffmann RE, Gueorguieva R, Hawkins KA, Varanko M, Boutros
NN, Wu YT, Caroll K, Krystal JH (2005) Temporoparietal
transcranial magnetic stimulation for auditory hallucinations:
safety, efficacy and moderators in a fifty patients sample. Biol
Psychiatry 58:97–104
Hoppner J, Schulz M, Mau R, Schlafke D, Richter J (2003)
Antidepressant efficacy of two different rTMS procedures. Eur
Arch Psychiatry Clin Neurosci 253:103–109
Huang CC, Su TP, Shan IK, Wei IH (2004) Effect of 5 Hz repetitive
transcranial magnetic stimulation on cognition during a Go/
NoGo task. J Psychiatr Res 38:513–520
Huber TJ, Schneider U, Rollnik J (2003) Gender differences in the
effect of repetitive transcranial magnetic stimulation in schizo-
phrenia. Psychiatry Res 120(1):103–105
Jandl M, Bittner R, Sack A, Weber B, Gunther T, Maurer K, Kaschka
WP (2004) Effects of rTMS on negative symptoms and EEG-
topography in schizophrenic patients. Eur Psychiatry 19(Suppl
1):164
Jandl M, Bittner R, Sack A, Weber B, Gunther T, Pieschl D, Kaschka
WP, Maurer K (2005) Changes in negative symptoms and EEG
in schizophrenic patients after repetitive transcranial magnetic
stimulation (rTMS): an open-label pilot study. J Neural Transm
112:955–967
Januel D, Dumortier G, Verdon CM, Stamatiadis L, Saba G, Cabaret
W, Benadhira R, Rocamora JF, Braha S, Kalalou K, Vicaut PE,
Fermanian J (2006) A double-blind sham controlled study of
right prefrontal repetitive transcranial magnetic stimulation
(rTMS): Therapeutic and cognitive effect in medication free
unipolar depression during 4 weeks. Prog Neuropsychopharma-
col Biol Psychiatry 30(1):126–130
Jin Y, Potkin SG, Kemp AS, Huerta ST, Alva G, Thai TM, Carreon
D, Bunney WE Jr (2006) Therapeutic effects of individualized
alpha frequency transcranial magnetic stimulation (alpha rTMS) on
negative symptoms of schizophrenia. Schizophr Bull 32:556–561
Jorge RE, Robinson RG, Tateno A, Narushima K, Acion L, Moser L,
Arndt S, Chemerinski E (2004) Repetitive transcranial magnetic
stimulation as treatment of poststroke depression: a preliminary
study. Biol Psychiatry 55:398–405
Kinchla RA (1992) Attention. Annu Rev Psychol 43:711–742
Kuroda Y, Motohashi N, Ito H, Ito S, Takano A, Nishikawa T, Suhara
T (2006) Effects of repetitive transcranial magnetic stimulation
on [11C] raclopride binding and cognitive function in patients
with depression. J Affect Disord 95:35–42
Little JT, Kimbrell TA, Wassermann EM, Grafman J, Figueras S,
Dunn RT, Danielson A, Repella J, Huggins T, George MS, Post
RM (2000) Cognitive effects of 1- and 20-Hertz repetitive
transcranial magnetic stimulation in depression: preliminary
report. Neuropsychiatry Neuropsychol Behav Neurol 13(2):
119–124
Loo C (2001) Effects of a 2- to 4-week course of repetitive
transcranial magnetic stimulation (rTMS) on neuropsychologic
functioning, electroencephalogram, and auditory threshold in
depressed patients. Biol Psychiatry 49:615–623
Loo C, Mitchell PB, Croker VM, Malhi GS, Wen W, Gandevia SC,
Sachdev PS (2003) Double-blind controlled investigation of
bilateral prefrontal transcranial magnetic stimulation for the
treatment of resistant major depression. Psychol Med 33:33–40
Martis B, Alam D, Dowd SM, Hill SK, Sharma RP, Rosen C, Pliskin
N, Martin E, Carson V, Janicak PG (2003) Neurocognitive
effects of repetitive transcranial magnetic stimulation in severe
major depression. Clin Neurophysiol 114:1125–1132
May A, Hajak G, Gansbauer S, Steffens T, Langguth B, Kleinjung T,
Eichhammer P (2007) Structural brain alterations following 5
days of intervention: dynamic aspects of neuroplasticity. Cereb
Cortex 17:205–210
Miller EK, Cohen JD (2001) An integrative theory of prefrontal
cortex function. A Rev Neurosci 24:167–202
Mogg A, Pluck G, Eranti SV, Landau S, Purvis R, Brown RG, Curtis
V, Howard R, Philpot M, McLoughlin DM (2008) A randomized
controlled trial with 4-month follow-up of adjunctive repetitive
transcranial magnetic stimulation of the left prefrontal cortex for
depression. Psychol Med 38(3):323–333
Moser DJ, Jorge RE, Manes MD, Paradiso S, Benjamin BS, Robinson
RG (2002) Improved executive functioning following repetitive
transcranial magnetic stimulation. Neurology 58:1288–1290
Mosimann UP, Schmitt W, Greenberg BD, Kosel M, Muri RM,
Berkhoff M, Hess CW, Fisch HU, Schlaepfer TE (2004)
Repetitive transcranial magnetic stimulation: a putative add on
treatment for major depression in elderly patients. Psychiatr Res
126:123–133
O’Connor M, Brenninkmeyer C, Morgan A, Bloomingdale K, Thall
M, Vasile R, Pascual Leone A (2003) Magnetic stimulation and
electroconvulsive therapy on mood and memory: a neurocogni-
tive risk-benefit-analysis. Cogn Behav Neurol 6(2):118–127
Padberg F, Zwanzger P, Thoma H, Kathmann N, Haag C, Greenberg
BD, Hampel H, Moller HJ (1999) Repetitive transcranial
magnetic stimulation (rTMS) in pharmacotherapy-refractory
major depression: comparative study of fast, slow and sham
rTMS. Psychiatry Res 88(3):163–171
Posner MI (1975) The psychology of attention. In: Gazzaniga MS,
Blakemore C (eds) Handbook of psychology. Academic,
New York
Cognitive effects of prefrontal rTMS
123
- 52 -

Posner MI, Boies SW (1971) Components of attention. Psychol Rev
78:391–408
Post A, Keck ME (2001) Transcranial magnetic stimulation as a
therapeutic tool in psychiatry: what do we know about the
neurobiological mechanism? J Psychiatr Res 35:193–215
Poulet E, Brunelin J, Bediou B, Forgeard L, Daleru J, D’Amato T,
Saoud M (2005) Slow transcranial magnetic stimulation can
rapidly reduce resistant auditory hallucinations in schizophrenia.
Biol Psychiatry 57:188–191
Rektorova I, Megova S, Bares M, Rektor I (2005) Cognitive
functioning after repetitive transcranial magnetic stimulation in
patients with cerebrovascular disease without dementia: a pilot
study of seven patients. J Neurol Sci 229–230:157–161
Ridding MC, Rothwell JC (2007) Is there a future for therapeutic
use of transcranial magnetic stimulation? NatRevNeurosci 8(7):
559–567
Rollnik JD, Huber TJ, Mogk H, Siggelkow S, Kropp S, Dengler R,
Emrich HM, Schneider U (2000) High frequency repetitive
transcranial magnetic stimulation (rTMS) of the dorsolateral
prefrontal cortex in schizophrenic patients. NeuroReport 11:
4013–4015
Rosa MA, Gattaz WF, Pascual-Leone A, Fregni F, Rosa MO, Rumi
DO, Myczkowski M, Silva MF, Mansur C, Rigonatti SP,
Teixeira MJ, Marcolin MA (2006) Comparison of repetitive
transcranial magnetic stimulation and electroconvulsive therapy
in unipolar non-psychotic depression: a randomized single-blind
study. Int J Neuropsychopharmacol 9(6):667–676
Sachdev P, Loo C, Mitchell P, Malhi G (2005) Transcranial magnetic
stimulation for the deficit syndrome of schizophrenia: A pilot
investigation. Psychiatry Clin Neurosci 59(3):354–357
Sack AT, Linden DE (2003) Combining transcranial magnetic
stimulation and functional imaging in cognitive brain research:
possibilities and limitations. Brain Res Brain Res Rev 43(1):
41–56
Sack AT, Cohen Kadosh R, Schumann T, Moerel M, Walsh V,
Goebel R (2009) Optimizing functional accuracy of TMS in
cognitive studies: a comparison of methods. J Cogn Neurosci
21(2):207–221
Sackeim HA, Portnoy S, Neeley P, Steif BL, Decina P, Malitz S
(1986) Cognitive consequences of low-dosage electroconvulsive
therapy. Ann NY Acad Sci 462:326–340
Schulze-Rauschenbach SC, Harms U, Schlaepfer TE, Maier W,
Falkai F, Wagner M (2005) Distinctive neurocognitive effects of
repetitive transcranial magnetic stimulation and electroconvul-
sive therapy in major depression. Br J Psychiatry 186:410–416
Shajahan PM, Glabus MF, Steele JD, Doris AB, Anderson K, Jenkins
JA, Gooding PA, Ebmeier KP (2002) Left dorso-lateral repet-
itive transcranial magnetic stimulation affects cortical
excitability and functional connectivity, but does not impair
cognition in major depression. Prog Neuropsychopharmacol Biol
Psychiatry 26(5):945–954
Sole-Padulles C, Bartres-Faz D, Junque C, Clemente IC, Molinuevo
JL, Bargallo N, Sanchez-Aldeguer J, Bosch B, Falcon C, Valls-
Sole J (2006) Repetitive transcranial magnetic stimulation
effects on brain function and cognition among elders with
memory dysfunction. A randomized sham-controlled study.
Cereb Cortex 16:1487–1493
Speer AM, Repella JD, Figueras S, Demian NK, Kimbrell TA,
Wasserman EM, Post RM (2001) Lack of adverse cognitive
effects of 1 Hz and 20 Hz repetitive transcranial magnetic
stimulation at 100% of motor threshold over left prefrontal
cortex in depression. J ECT 17(4):259–263
Squire LR (1982) Memory and electroconvulsive therapy (Letter).
Am J Psychiatry 139:1221
Strafella A, Paus T, Barrett J, Dagher A (2001) Repetitive transcranial
magnetic stimulation of the human prefrontal cortex induces
dopamine release in the caudate nucleus. J Neurosci 21(157):1–4
Stuss DT, Benson DF (1986) The frontal lobes. Raven, New York
Triggs WJ, McCoy KJM, Greer R, Rossi F, Bowers D, Kortenkamp S,
Nadeau SE, Heilman KM, Goodman WK (1999) Effects of left
frontal transcranial magnetic stimulation on depressed mood,
cognition, and corticomotor threshold. Biol Psychiatry 45(11):
1440–1446
Trojano L, Conson M, Maffei R, Grossi D (2006) Categorial and
coordinate spatial processing in the imagery domain investigated
by rTMS. Neuropsychologia 44(9):1569–1574
Vanderhasselt MA, De Raedt R, Baeken C, Leyman L, D’haenen H
(2006) The influence of rTMS over the left dorsolateral
prefrontal cortex on Stroop task performance. Exp Brain Res
169:279–282
Vanderhasselt MA, De Raedt R, Leyman L, Baeken C (2009) Acute
effects of repetitive transcranial magnetic stimulation on atten-
tional control are related to antidepressant outcomes. J Psychi-
atry Neurosci 34(2):119–126
Wagner W, Rihs TA, Mosimann UP, Fisch HU, Schlaepfer TE (2006)
Repetitive transcranial magnetic stimulation of the dorsolateral
prefrontal cortex affects divided attention immediately after
cessation of stimulation. J Psychiatr Res 40:315–321
Weinberger DR, Berman KF, Chase TN (1988) Mesocortical
dopaminergic function and human cognition. Ann NY Acad
Sci 537:330–338
Weiner RD, Rogers HJ, Davidson JR, Squire LR (1986) Effects of
stimulus parameters on cognitive side effects. Ann NY Acad Sci
462:315–325
Zimmermann P, Fimm B (1997) Test for Attentional Performance
(TAP), version 1.5. Psytest Press, Freiburg
B. Guse et al.
123
- 53 -

2.3 The effect of long-term high frequency repetitive transcranial magnetic
stimulation on working memory in schizophrenia and healthy controls – a
randomized placebo-controlled, double-blind fMRI study
This uni-centric rTMS and fMRI study investigates schizophrenia patients and
healthy controls. We ask whether a three-week excitatory 10 Hz rTMS applied to the
left DLPFC can improve verbal WM and modulate brain activation. We suppose that
patients’ probable benefit in working memory performance would be higher compared
to healthy controls due to ceiling effects in healthy controls. In addition, we hypothesize
that patients’ WM activations would approximate those of controls in the sense of
“normalized” system recruitment due to rTMS intervention. As in the first described
main study (see 2.1), rTMS is conducted over a period of 15 total sessions at 10 Hz,
110% of the individual resting motor threshold, with 1000 stimuli per session (15.000 in
total) and an inter-train interval of 30 seconds. In the placebo condition the same coil is
positioned 5 cm latero-caudal to F3 and distorted 45° away from the skull. Patients
(n=25) and healthy controls (n= 22) are assigned to either placebo or active stimulation
and compared to each other at every time point. Additional cognitive tasks are
administered targeting domains other than working memory. Contrary to our
hypothesis, functional imaging results indicate no statistical significant activity change
in the WM network over time in any contrast or sample. According to the ANOVAs for
repeated measures, cognitive performance remains without statistically relevant
alteration in all groups. As no analysis reveals relevant interaction effects, outlasting
after-effects following long-term high-frequency rTMS on brain activity or WM
performance can not be confirmed.
- 54 -

R
Tsr
BKa
b
c
d
e
f
h
����
a
ARRAA
KrfMSHLWC
a3
0h
Behavioural Brain Research 237 (2013) 300– 307
Contents lists available at SciVerse ScienceDirect
Behavioural Brain Research
j ourna l ho me pa ge: www.elsev ier .com/ locate /bbr
esearch report
he effect of long-term high frequency repetitive transcranial magnetictimulation on working memory in schizophrenia and healthy controls—Aandomized placebo-controlled, double-blind fMRI study
irgit Gusea,b,∗, Peter Falkaia, Oliver Grubera, Heather Whalleyc, Lydia Gibsond, Alkomiet Hasana,atrin Obste, Peter Dechent f, Andrew McIntoshc, Boris Suchanb, Thomas Wobrocka
University Medical Centre, Department of Psychiatry and Psychotherapy, Georg August University Göttingen, von-Siebold-Str. 5, D-37075 Göttingen, GermanyInstitute of Cognitive Neuroscience, Department of Neuropsychology, Ruhr University Bochum, Universitätsstr. 150, D-44780 Bochum, GermanyDivision of Psychiatry, Royal Edinburgh Hospital, University of Edinburgh, Kennedy Tower, Morningside, Edinburgh EH10 5HF, UKInstitute of Psychology, Department of Experimental Psychology, Georg-August-University Göttingen, Goßlerstraße 14, D-37073 Göttingen, GermanyInstitute of Psychology, Department of Social Psychology, University Jena, Humboldtstr. 26, D-07743 Jena, GermanyMR-Research in Neurology and Psychiatry, University Medical Center Göttingen, Robert-Koch-Str. 40, D-37075 Göttingen, Germany
i g h l i g h t s
3-week HF rTMS does not alter brain activation during working memory.Schizophrenia patients do not significantly differ from controls after treatment.Long-term HF rTMS does not change cognitive performance.Active rTMS is not superior to placebo rTMS.
r t i c l e i n f o
rticle history:eceived 31 May 2012eceived in revised form 29 August 2012ccepted 17 September 2012vailable online xxx
eywords:TMSMRI
iddle frontal gyruschizophreniaealthy controlsong term effect
orking memoryognition
a b s t r a c t
In schizophrenia patients negative symptoms and cognitive impairment often persist despite treatmentwith second generation antipsychotics leading to reduced quality of life and psychosocial functioning.One core cognitive deficit is impaired working memory (WM) suggesting malfunctioning of the dorso-lateral prefrontal cortex. High frequency repetitive transcranial magnetic stimulation (rTMS) has beenused to transiently facilitate or consolidate neuronal processes. Pilot studies using rTMS have demon-strated improvement of psychopathology in other psychiatric disorders, but a systematic investigation ofworking memory effects outlasting the stimulation procedure has not been performed so far. The aim ofour study was to explore the effect of a 3-week high frequency active or sham 10 Hz rTMS on cognition,specifically on working memory, in schizophrenia patients (n = 25) in addition to antipsychotic therapyand in healthy controls (n = 22). We used functional magnetic resonance imaging (fMRI) to compare acti-vation patterns during verbal WM (letter 2-back task) before and after 3-weeks treatment with rTMS.Additionally, other cognitive tasks were conducted. 10 Hz rTMS was applied over the left posterior middlefrontal gyrus (EEG electrode location F3) with an intensity of 110% of the individual resting motor thresh-
old (RMT) over a total of 15 sessions. Participants recruited the common fronto- parietal and subcorticalWM network. Multiple regression analyses revealed no significant activation differences over time inany contrast or sample. According to the ANOVAs for repeated measures performance remained withoutalterations in all groups. This is the first fMRI study that has systematically investigated this topic withina randomized, placebo-controlled, double-blind design, contrasting the effects in schizophrenia patientsand healthy controls.∗ Corresponding author at: University Medical Centre, Department of Psychiatrynd Psychotherapy, Georg-August-University Göttingen, Von-Siebold-Straße 5, D-7075 Göttingen, Germany. Tel.: +49 0 551 39 10114; fax: +49 0 551 39 9337.
E-mail address: [email protected] (B. Guse).
166-4328/$ – see front matter © 2012 Elsevier B.V. All rights reserved.ttp://dx.doi.org/10.1016/j.bbr.2012.09.034
- 55
© 2012 Elsevier B.V. All rights reserved.
1. Introduction
Schizophrenia is a major mental illness characterized by posi-tive symptoms (e.g. delusions, hallucinations), negative symptoms(e.g. apathy, blunted affect, emotional/social withdrawal) and cog-nitive dysfunction. Research from the last twenty years indicates
-

ain Re
ttdmawdtttgvfimmigta(
smp(atwfvtartrcucolbcqce(cthDcaidrmAir
rsfs
B. Guse et al. / Behavioural Br
hat these impairments in cognition are one of the main predic-ors for poor social and functional outcome and a main reason forisability in schizophrenia patients [16,18,24]. Cognitive impair-ent in schizophrenia generally includes the domains of attention
nd concentration, psychomotor speed, learning and memory asell as executive functions [30,32]. One of the core cognitiveeficits is working memory (WM) as part of a disturbed cen-ral executive system [6,53]. Working memory implies the shorterm retention of information that is no longer accessible inhe environment and the manipulation of this information foruiding behavior [9]. Over the past few decades, studies have pro-ided a substantial body of evidence supporting a critical roleor bilateral prefrontal, anterior cingulate and parietal regionsn mediating WM performance (e.g. [50]; for review [54]). The
iddle frontal gyrus (Brodmann area (BA) 9/46) is known to beainly activated during the manipulation and executive monitor-
ng of incoming stimuli (e.g. [55]), whereas the inferior frontalyrus (BA 44) and parts of the superior frontal gyrus (premo-or and supplementary motor area, BA 6) as well as parietalssociation cortices are most sensitive for maintenance processese.g. [38]).
These results are in line with functional and cytoarchitecturaltudies pointing to a tightly knit and specific network of frontal-ediated working memory functions (for review [35,40,56]). The
refrontal cortex, especially the dorsolateral prefrontal cortexDLPFC, BA 9/46), has an important role in working memorynd is, above all, well located for transcranial magnetic stimula-ion (TMS) [27]. In this context, Mull and Seyal [33] investigatedhether transient functional disruption of the dorsolateral pre-
rontal cortex (DLPFC) with TMS would impair performance in aerbal WM task. Participants were presented sequences of let-ers and asked to decide if the letter just displayed was the sames the letter presented three trials back (n-back task). The studyevealed an effect on task accuracy when TMS was applied tohe left DLPFC between letter presentations. Thus, as inhibitoryepetitive TMS (rTMS) induces virtual lesion in the prefrontalortex interfering with cognitive performance, facilitatory stim-lation has been discussed to have the potential to improveognitive performance and memory functions [41]. The applicationf transcranial magnetic stimulation is one possibility to modu-ate activity states and to interfere with the function of certainrain areas. Physiological studies of the primary motor cortexonducted in healthy subjects indicate that, dependent on the fre-uency and pattern of the stimulation protocol, repetitive TMSan induce a long-lasting enhancement or reduction of corticalxcitability (for review see [20,61]). In general, low frequency<1 Hz) rTMS reduces and high frequency rTMS (>5 Hz) enhancesortical excitability, but the recently introduced theta-burst pro-ocol (TBS, a modified repetitive TMS protocol) applied at veryigh-frequencies (50 Hz) does not follow this frequency-rule [44].ependent on whether the TBS is applied in an intermittent orontinuous pattern, the effects are facilitatory or inhibitory. Inddition to that, we also know from recently published stud-es that the effects of TBS and rTMS are dependent on manyifferent factors, like history of synaptic plasticity, the interneu-on networks recruited by the TMS pulse, current activity of theembrane potential, and pharmacological modulation [44,21,22].ll these factors contribute to the high interindividual variabil-
ty of physiological and behavioral responses following TBS andTMS.
However, there is emerging evidence that some establishedepetitive TMS protocols have the capacity to induce plasticity
hifts of the stimulated and interconnected brain areas and, there-ore, to modulate behavioral and cognitive functions (for reviewee [41,61,44,48]).- 56 -
search 237 (2013) 300– 307 301
Based on these physiological findings, repetitive TMS has beensuccessfully used to improve motor performance and motor learn-ing [4,11,37,41]. Beyond the influence on the motor system there isgrowing evidence showing transient neuronal facilitation and cog-nitive process enhancement due to rTMS in healthy subjects. Everset al. [12] studied visually evoked event-related potentials (ERP)and mean choice reaction time measured before and after 20 HzrTMS (compared to sham and 1 Hz single TMS) applied to the leftand right prefrontal cortex in healthy subjects. Results revealed asignificant decrease of P3 latencies and reaction time due to 20 HzrTMS of the left but not right PFC. In a combined study using TMSand near-infrared spectroscopy, Yamanaka et al. [60] administered5 Hz or sham TMS to the left or right parietal cortex of healthy sub-jects during the delay period of a spatial WM task (control task:visuospatial attention task). Reaction times improved in the spa-tial WM task only after active stimulation of the right parietalcortex. This effect was attended by significantly increased frontaloxygenated hemoglobin (oxy-Hb) levels during the WM task andreduced levels during the control task reflecting a selectively facil-itating effect on spatial WM. Klimesch et al. [29] could show thatrTMS at individual upper alpha frequency (IAF + 1 Hz) delivered tothe mesial frontal (Fz) and right parietal (P6) cortex can enhancethe performance in a mental rotation task.
However, most studies raise limitations concerning the focuson direct cognitive effects of single sessions. Repeated sessiondesigns applying daily rTMS to test gradual or cumulative alter-ations in after-effects should be proven for therapeutic purposes.Until now, some circumscribed outlasting or consolidation effectsof rTMS and other non-invasive brain stimulation techniques havebeen described in the human motor system indicating long-lastingbehavioral effects (e.g. [41,42,61], see above). The transfer of thesemotor-system findings to prefrontal regions and the increase ofstimulation sessions is essential for treatment application in neu-ropsychiatric diseases associated with working memory and othercognitive deficits.
We have recently reviewed the effects of high-frequencyrepetitive TMS (>1 Hz) on cognitive functions and revealed thatstimulation protocols using frequencies between 10 Hz and 20 Hzand 80–110% of the individual resting motor threshold are mostlikely to result in an improvement of cognitive functions. Fur-thermore, our review indicates that improvements depend on therepetition rate of rTMS sessions and that patients with neuropsy-chiatric disorders do show usually greater improvements thanhealthy controls [19]. In schizophrenia patients, facilitatory rTMSapplied to the frontal lobe has been discussed to be effective inthe treatment of negative symptoms (Meta-Analysis and review[10]). Within some of these studies targeting negative symptomsvia frontal repetitive TMS, cognitive effects of the stimulationwere additionally investigated, whereas only one of five random-ized controlled trials showed a beneficial effect in schizophreniapatients [8].
To explore the neurobiology underlying non-invasive brainstimulation related functional changes in the frontal lobe, placebo-controlled, randomized and double-blind studies using techniquesof experimental neurophysiology and functional brain imaging arenecessary.
In particular, multimodal studies contrasting effects on the dis-eased versus healthy brain are needed to get a better understandingof process in the frontal cortex. Therefore, the aim of our combinedlong-term rTMS and fMRI study was to investigate whether long-term rTMS is a promising tool to modulate working memory inhealthy subjects and in schizophrenia patients that outlasts the
stimulation procedure. In this context, we were interested in func-tional cerebral alterations of the frontal lobe evaluated by fMRI aswell as behavioral performance effects due to rTMS treatment.
302 B. Guse et al. / Behavioural Brain Research 237 (2013) 300– 307
Table 1Demography of the sample.
SZ active SZ sham HC active HC sham SZ all HC all
Number 13 12 11 11 25 22Sex (m:f) 10:3 9:3 8:3 8:3 19:6 16:6Educational level (mean years) 15.5 12.6 16.4 12.5 14.1 14.5
H
2
2
piSdaMbpprs
mtdjptBta
2
motmfdi
s3(b1tmswttr
TF
Er
Age average (range) 37 (22–58) 36 (20–51)
C = healthy controls, SZ = schizophrenia, f = female, m = male.
. Methods
.1. Subjects
We studied 25 right-handed in- and out-patients (real/active, n = 13,lacebo/sham, n = 12) with an ICD-10 diagnosis of schizophrenia with predom-
nant negative symptoms (>20 points according to the Positive and Negativeyndrome Scale (PANSS) [28]) and with an illness duration for at least 6 months (foremography see Table 1). All patients were on stable doses of second generationntipsychotics and had stable PANSS scores 2 weeks before inclusion in the study.edication was not changed throughout the study. Anticonvulsive or high-dose
enzodiazepine treatment was prohibited. This experimental fMRI-study is a sub-roject of a large randomized multicenter clinical trial (NCT00783120). Therefore,atients were centrally randomized to placebo or real intervention group (designeported in [7]). Rater, investigators and patients were blind across all parts of thetudy.
22 healthy right-handed comparison subjects (active, n = 11, sham, n = 11), pair-atched for age (maximal difference of 2 years), gender and educational level were
reated in the same stimulation condition as their equivalent patient. Three subjectsropped out before stimulation due to withdrawal of their consent. Comparison sub-
ects were excluded if they had a first-degree relative with schizophrenia or anothersychiatric disorder. A history of neurologic illness (especially epileptic seizures) orhose with contraindications to MRI scanning e.g. magnetic implants were excluded.efore inclusion subjects signed written informed consent after complete descrip-ion of the study. The study was in accordance with the Declaration of Helsinki andpproved by the local ethic committee of the University Medical Center Göttingen.
.2. Stimulation procedure
rTMS was performed with a MagProX100 (Medtronic/Denmark) magnetic sti-ulator according to international safety guidelines [46,58]. For the determination
f the individual resting motor threshold (RMT), single pulse TMS was appliedhrough a standard figure-of-eight coil to the hand area of the left motor cortex and
otor-evoked potentials (MEPs) were recorded via electromyography (EMG) sur-ace electrodes from the right first-dorsal interosseus muscle (FDI). The RMT wasefined as the lowest intensity that produced a motor evoked potential of <50 �V
n the relaxed FDI in at least five of ten trials [47].rTMS intervention was then conducted over a period of 3 weeks (15 total ses-
ions, 1 session/weekday) at 10 Hz, 110% of the individual RMT, inter-train interval0 s with 1000 stimuli per session, delivering 15,000 stimuli per patient in totalTable 2). Coil position over the left DLPFC was guaranteed in active and sham groupy a coil positioning method using the 10–20-EEG system. In brief, the standard0–20 EEG electrode positions were individually measured and marked. The posi-ion of the coil center was then located at the electrode position F3 (left posterior
iddle frontal gyrus, BA 46) [14,49]. For active stimulation the coil was placed at theame point tangentially to the scull oriented posterior to anterior. Sham stimulation
as delivered at the same parameters but with the coil positioned 5 cm laterocaudalo F3 and with one wing angulated 45◦ away from the scull. This method was usedo evoke slight temporal skull sensations without effective stimulation of the targetegion.
able 2low chart.
EG: Electroencephalography; fMRI: functional magnetic resonance imaging; RMT:esting motor threshold; rTMS: repetitive transcranial magnetic stimulation.
- 57
36 (20–58) 36 (21–52) 36 (20–58) 36 (20–58)
2.3. fMRI scanning procedure
For functional MRI, axial gradient-echo echo planar images (EPI) were acquiredon a 3 T Siemens Magnetom Tim Trio scanner. Images were obtained using a standard8-channel-head-coil. The head was stabilized with small cushions to minimizemovement during scanning. Functional imaging was performed with the follow-ing parameter settings: echo time 36 ms, repetition time 2000 ms, flip angle 70◦ ,field of view 256 mm, voxel size 2 mm × 2 mm × 4 mm, 22 axial slices parallel to theAC–PC plane acquired in ascending order. Acquisition was run for 400 volumes inone single session, of which the first six volumes were discarded for the analysis.Triggering of the stimulation by the scanner pulses was conducted using Presen-tation Software. Before functional scanning, T1-weighted anatomical imaging wasperformed for each subject (voxel size 1 mm × 1 mm × 1 mm).
2.4. Neuropsychological assessment
During the fMRI session, subjects performed a verbal n-back working memorytask with parametrically varied WM load among 0, 1 and 2 items [39]. Subjectsviewed sequences of capital letters (A–E) displayed in the middle of a visual screen(700 ms each letter; 1800 ms inter-stimulus interval, offset to onset) and provideddominant hand button press at every stimulus. In the 0-back (control) condition, thetarget was any letter that matched the pre-specified letter “X”. In the 1- and 2-backcondition, the target was any letter that corresponded to the one presented one ortwo trials preceding it, respectively. Demands of stimulus encoding and responseremained constant across conditions, only requirements of maintenance and manip-ulation differed with increasing amounts of information. Subjects responded to eachrandomly presented letter, pressing one button for targets (33%) and another fornon-targets. Conditions were run block-wise in the same order (0-1-2-0-1-2. . .),with 18 blocks à 15 stimuli. Prior to each trial, subjects were given short instructions(e.g. “1-back”, presented 3500 ms on the screen).
Additional “off-line” neuropsychological ratings were conducted prior to thefirst and at least one hour after the last rTMS session. Neuropsychological tests wereadministered in a fixed order by the same blinded rater. All tests were designed toindicate deficits in parts of the dorsolateral prefrontal cortex and interconnectedbrain regions, respectively. The Trail Making Test (TMT-A/B) requires complex visualscanning, motor speed (Version A) and the ability of flexible shifting (Version B) (e.g.[43]). The Tübinger Aufmerksamkeitsprüfung (TAP) is a computer based test batteryand its subtests “selective attention” and “divided attention” were conducted tomeasure basal attention processes [62]. The divided attention task comprises anauditory and a visual component requiring keeping both sensory inputs on line. Thecomputer based Wisconsin Card Sorting Test (WCST) is commonly used to assesscognitive flexibility and abstract reasoning [17].
2.5. Psychopathological baseline assessment
Psychopathological assessment at baseline was conducted using the PANSS
(Table 3). This scale is standardized for typical and dimensional assessment ofschizophrenia symptoms and evaluates positive, negative and other dimensions onbasis of a formal semi-structured clinical interview [28]. Additional validated ratingscales were conducted to assess other psychopathological symptoms: the CalgaryDepression Rating Scale for Schizophrenia (CDSS) [1], the Montgomery and AsbergTable 3Schizophrenia sample. Baseline results of the clinical ratings.
Clinical rating scales Baseline
M (SD) active M (SD) sham p
PANSSTotal score 81.7 (11.9) 72.1 (12.0) 0.08Psychopathology 42.3 (7.2) 37.2 (8.2) 0.14Positive scale 15.3 (4.4) 11.9 (3.1) 0.06Negative scale 23.9 (3.5) 23.3 (2.2) 0.62
MADRS 12.4 (3.1) 14.1 (7.3) 0.48CDSS 2.2 (1.8) 3.8 (4.7) 0.33CGI 4.1 (0.5) 3.7 (0.95) 0.37GAF 56.9 (7.0) 60.1 (7.8) 0.35
Means (M) and standard deviations (SD) of test scores at baseline.
-

ain Re
Dtdo
2
2
rpMicnMwfi
gwortamc
anafdpe
rccoopae
2
Cfii
2Eousiei(stthbic
2s
3
3
3
r
B. Guse et al. / Behavioural Br
epression Rating Scale (MADRS) [31], the Clinical Global Impression (CGI) [34] andhe Global Assessment Scale of Functioning (GAF) [59] (Table 3). Ratings were con-ucted by the same experienced and blinded investigator. The psychopathologicalutcome over all subjects will be published within the multicenter trial.
.6. Data analysis
.6.1. Functional imaging dataFor movement correction the reconstructed and converted EPI images were
ealigned to the mean functional image using SPM5 (Statistical Parametric Map-ing; http://www.fil.ion.ucl.ac.uk/spm/) running in Matlab (MathWorks, Natick,assachusetts). Slice time correction was then carried out to minimize differences
n acquisition times. The source (structural) and reference (functional) image wereo-registered, the anatomic image was segmented. This output file was then used toormalize the realigned functional data into standard stereotactic space (using theontreal Neurologic Institute (MNI) template provided by SPM5). Finally, the EPIsere smoothed with an 8 mm × 8 mm × 8 mm full-width half-maximum Gaussianlter.
Statistical analyses were conducted using the General Linear Model in SPM,enerating a matrix that allowed mapping brain activity alterations associatedith different experimental task demands. The design comprised three conditions,
ne for each task difficulty (0-, 1-, 2-back). In order to produce the hemodynamicesponse for each experimental condition (sustained activity over the whole blocks),he vectors were convolved with a canonical hemodynamic response function using
box-car function. For additional movement correction at the first-level the realign-ent output file was fitted in as regressor. Linear t-contrasts were then defined
omprising vectors for 1-back vs. 0-back, 2-back vs. 0-back and 2-back vs. 1-back.The resulting single-subject images were taken to a second-level random effects
nalysis. First, we were interested in whether all groups recruited the common WMetwork reported in the literature and whether groups differed in WM activationt baseline. Initially, one-sample t-tests were performed for each group (SZ, HC)or WM demand (2-back vs. 0-back, 1-back vs. 0-back). We then looked for groupifferences and calculated different two factorial analyses of variance (ANOVA) com-rising “diagnostic group” (SZ, HC) and “stimulation condition” (active, sham) forach contrast of interest.
In order to study the effect of stimulation pre- to post-treatment within aepeated measure design we performed a multiple regression analysis for eachontrast constructing a vector for each subject (n = 47) and condition (n = 8) asovariate. This vector specifically encoded which scores in different conditions werebtained from the same subject. Thus, every subject was assigned to schizophreniar healthy group, to active or sham stimulation and to both time points (pre- andost-treatment). Therefore, the row component of variance was obtained to evalu-te activation differences pre- to post-treatment within groups and their interactionffects.
.6.2. Behavioral dataBehavioral data were analyzed using SPSS software (version 18.0, SPSS Inc.,
hicago, IL, USA). Since active and sham group had been centrally randomized, werstly explored whether educational level, gender, age, medication and stimulation
ntensity (RMT) were balanced at baseline.
.6.2.1. Neuropsychology. Accuracy data and reaction times (RTs) were aggregated.rror and omission trials were excluded from the reaction time analysis. Meansf active and sham groups were compared for schizophrenia patients and controlssing Student’s t-tests. Data of the schizophrenia and control sample were theneparately pooled and compared with each other to increase test power and tonvestigate the effect of psychopathological symptoms on baseline measures. Wexpected that schizophrenia patients would perform worse than healthy controlsn all neurocognitive measures. For treatment effects data were submitted to a 2time of measurement: pre-treatment vs. post-treatment) × 2 (diagnostic group:chizophrenia vs. healthy controls) × 2 (stimulation condition: active vs. sham) fac-orial design with time of measurement as within-subjects factor. Thus, for eachest variable an ANOVA for repeated measures was performed with additional postoc analyses using paired, two tailed t-tests in case of significant results indicatedy interactions in the ANOVA with all p-values corrected for multiple compar-
sons. Moreover, Cohen’s d for repeated measures was calculated for all relevantomparisons.
.6.2.2. Psychopathology. Means of active and sham groups were compared forchizophrenia patients using Student’s t-tests.
. Results
.1. Functional imaging data
.1.1. BaselineIn line with previous studies within group analyses (SZ/HC)
evealed recruitment of bilateral fronto-parietal regions during
- 58 -
search 237 (2013) 300– 307 303
2-back WM performance (Fig. 1) with some activation in subcor-tical regions such as insula, caudate nucleus and thalamus (e.g.[35,40]). For detailed activation coordinates see SupplementaryTables 1 and 2. Between group analysis yielded no main effectof diagnostic group (HC/SZ), no main effect of stimulation con-dition (active/sham) and no interaction effect of diagnosticgroup × stimulation condition at a threshold of p < .001 uncor-rected. At the 1-back difficulty all participants activated the samenetwork to a lower extent than in the 2-back condition, so werestricted to report the 2-back vs. 0-back contrast.
3.1.2. Treatment effectsThe multiple regression analyses were performed regarding
each diagnostic group (healthy controls and schizophreniapatients) in each condition (active and sham stimulation) at bothtime points (before and after stimulation). Contrary to our initialhypothesis, the multiple regression analysis revealed no statisti-cally significant activation difference pre- to post- treatment withineither the schizophrenic or the control sample and no relevantinteraction effect over all contrasts of interest at a threshold ofp < .001, uncorrected. Post hoc t-tests confirmed a lack of activa-tion difference between these groups after stimulation at p < .001uncorrected. MNI activation coordinates including correspondingcluster sizes and T-values at pre- and post- treatment during the2-back condition can be found in Supplementary Tables 1 and 2.
Overall, results revealed no significant activation differencesbetween schizophrenia patients and healthy controls at baselineor at post-treatment and no differences between or within groupsover time. The same is the case for both stimulation conditions,active and sham groups did not differ significantly.
3.2. Behavioral data
3.2.1. BaselineDemographic parameters were balanced across groups, but
active stimulation groups had higher mean educational levels thansham groups (Table 1). There were also more male individualsin both the active and sham groups. Regarding the stimulationintensity in the active samples, RMT was marginally higher in theschizophrenia than healthy group. Antipsychotic dosage (chlor-promazine equivalents) was balanced across sub-samples. Activeand sham stimulated patients differed significantly in the numberof correct trials in the 2-back condition of the verbal working mem-ory task (n-back) with a higher number of correct trials in the activegroup (t(23) = 3.11, p = .01). All remaining neuropsychological com-parisons between sham and active groups were non-significant.No significant clinical differences emerged between active andsham stimulated patients. Between-group comparisons demon-strated a decreased number of correct responses and increasedreaction times in the 0-back condition of the verbal WM taskin the schizophrenia group compared to the healthy controlgroup (t(29.5) = −2.47, p < .05 and t(36.7) = 2.52, p < .05, respec-tively). Further, a decreased number of correct responses in the1-back and 2-back working memory demand of the WM task inschizophrenia patients has been revealed (t(30.1) = −2.86, p < .05and t(44) = −2.80, p < .05, respectively) but no increase in reactiontimes. Schizophrenia patients had significantly increased reactiontimes than healthy controls in the TMT-B (t(34) = 2.09, p < .05) aswell as in the WCST (t(29) = 3.56, p = .001) and in the selectiveattention task (t(38) = 2.86, p < .05). No differences emerged in theremaining neurocognitive measures. Neuropsychological baselineresults can be found in Supplementary Tables 3 and 4.
3.2.2. Treatment effects, neuropsychologyVerbal working memory (n-back task). For the 0-back task an
ANOVA for repeated measures revealed a significant main effect

304 B. Guse et al. / Behavioural Brain Research 237 (2013) 300– 307
Fig. 1. Overview of the activations in the 2-back working memory condition. Brain regions activated in the 2-back vs. 0-back WM contrast, p < 0.001 (uncorrected) forillustration purposes. HC: healthy controls; SZ: schizophrenic patients.
otttmoto4e4i
rA3(ntbadgoaagsaa
f diagnostic group on accuracy (F(1, 42) = 9.66, p < .01) and reac-ion times (F(1, 42) = 6.89, p < .05) (Table 4). The same ANOVA forhe 1-back task demonstrated a significant main effect of diagnos-ic group on accuracy (F(1, 42) = 8.42, p < .01), further a significant
ain effect of time of measurement (F(1, 42) = 10.26, p < .01) andf diagnostic group on reaction times (F(1, 42) = 4.72, p < .05). Inhe accuracy ANOVA of the 2-back task significant main effectsf diagnostic group (F(1, 42) = 12.24, p < .01) and stimulation (F(1,2) = 13.60, p < .01) were found. Additionally, a significant mainffect of time of measurement on reaction times was revealed (F(1,2) = 14.22, p < .01). All in all, no significant interactions could be
dentified in the working memory domain.Visual scanning/motor speed, flexible shifting (TMT). The ANOVA
evealed a main effect of time of measurement for both the TMT- (F(1, 32) = 5.90, p < .05) and the TMT-B in “reaction times” (F(1,2) = 10.94, p < .01), but no interaction effects. Selective attentionTAP). Analysis on the selective attention task did not reveal any sig-ificant effects for accuracy. In contrast, for reaction times of correctrials a main effect for diagnostic group (F(1, 36) = 7.68, p < .01) coulde found and a time of measurement × stimulation interaction at
trend level (F(1, 36) = 3.09, p < .10). However, post hoc analysesid not indicate significant changes in reaction times in neitherroup and thus could not confirm this interaction effect. Resultsf the post hoc t-Tests can be found in Supplementary Tables 3nd 4. Divided attention (TAP). Accuracy data analysis of the dividedttention task indicated a significant main effect of diagnostic
roup (F(1, 35) = 6.95, p < .05) and a significant time of mea-urement × stimulation interaction (F(1, 35) = 5.13, p < .05). Furthernalysis of these effects did not indicate any significant changes inccuracy. The ANOVA on reaction times revealed significant main- 59
effects of time of measurement (F(1, 35) = 4.53, p < .05) and of stimu-lation (F(1, 35) = 5.52, p < .05). Furthermore, a significant diagnosticgroup × stimulation interaction was found (F(1, 35) = 4.39, p < .05).Again, this interaction effect could not be confirmed by subsequentt-tests as no significant differences over time could be found. Cogni-tive flexibility, abstract reasoning (WCST). In regard to the accuracy,the ANOVA indicated no significant differences. For reaction times(correct responses) in the WCST main effects could be found fortime of measurement (F(1, 26) = 24.62, p < .001) and for diagnos-tic group (F(1, 26) = 9.31, p < .01). Additionally, the ANOVA revealeda significant time of measurement × diagnostic group interaction(F(1, 26) = 5.30, p < .05). Subsequent analysis indicated that reactiontimes decreased in schizophrenic patients in both stimulation con-ditions (t(6) = 3.25, p < .05 for the active group, t(5) = 3.06, p = .056for the sham group).
4. Discussion
This is the first multimodal study investigating the cognitiveeffect and the underlying brain activations of long-term rTMS inhealthy subjects and schizophrenia patients. We asked whether athree-week excitatory 10 Hz rTMS applied to the left DLPFC canimprove verbal working memory and modulate brain activationin healthy controls and schizophrenia patients. Furthermore, wesupposed that patients’ probable benefit in working memory per-formance would be higher compared to healthy controls due to
ceiling effects in healthy controls. In addition, we hypothesizedthat patients’ WM activations would approximate those of con-trols in the sense of “normalized” system recruitment due to rTMSintervention.-

B. Guse et al. / Behavioural Brain Re
Table 4Analysis of Variance (ANOVA) for repeated measures. Neurocognitive measures,treatment effects.
Neurocognitive tests Df, error F- value p-value
Verbal WM (0-back)Group AC 1, 42 9.66 0.003b
Group RT 1, 42 6.89 0.017a
Verbal WM (1-back)Group AC 1, 42 8.42 0.008b
Group RT 1, 42 4.72 0.052b
Time RT 1, 42 10.26 0.004b
Verbal WM (2-back)Group AC 1, 42 12.24 0.002b
Stimulation AC 1, 42 13.60 0.001b
Time RT 1, 42 14.22 0.001b
TMT-ATime RTd 1, 32 5.90 0.021a
TMT-BTime RTd 1, 32 10.94 0.002b
Selective attention (TAP)Group RT 1, 36 7.68 0.009b
Stimulation × time RT 1, 36 3.09 0.088c
Divided attention (TAP)Group AC 1, 35 6.95 0.012a
Stimulation RT 1, 35 5.52 0.025a
Time RT 1, 35 4.53 0.041a
Time AC 1, 35 3.37 0.075a
Stimulation × time AC 1, 35 5.13 0.030a
Group × time RT 1, 35 4.39 0.043a
WCSTGroup RT 1, 26 9.31 0.005b
Time AC 1, 26 3.38 0.077c
Time RT 1, 26 24.62 < 0.001b
Group × time RT 1, 26 5.30 0.03a
ANOVA for repeated measures (group × stimulation × time), with time as within-subjects factor. For illustration purposes this table includes statistically significant(p < .05) and trend level results (p < .10). AC: accuracy, RT: reaction time (correctresponses).
a p < .05.b p < .01.c p < .10.
4
tststafihs(dbdeCmttspsAoo
d RT: total time needed.
.1. Functional imaging and behavioral neuropsychology
Imaging results were contrary to our initial hypothesis. Mul-iple regression analyses for each contrast revealed no statisticalignificant activity change in the working memory network overime, neither in the schizophrenia nor in the healthy controlsample. As analyses did not reveal relevant main effects or interac-ions, after-effects following high-frequency rTMS on frontal brainctivity during working memory performance could not be con-rmed in our study. In line with current literature, patients andealthy controls activated a network including fronto- parietal andubcortical regions during verbal working memory performancee.g. [35,40]). These regions demonstrated increased activationsuring the 2-back condition of the task compared to the 1-ack condition. Thus, participants enhanced activation at higheremands requiring maintenance and manipulation abilities. Thisffect was equivalent for all groups over all stimulation conditions.oncerning the behavioral data, the initial ANOVAs for repeatedeasures either remained either without interaction effects, or
hese interactions were not confirmed by post hoc t-tests. Reac-ion times in the WSCT significantly improved in the schizophreniaample after active stimulation, but to a minor extent also afterlacebo stimulation. Most of the main effects were “time of mea-
urement” and can be explained by training effects over all groups.lterations over time could not be clearly attributed to the kindf stimulation or group. Thus, the impact of high frequency rTMSn neuronal activation or cognitive enhancement outlasting the- 60 -
search 237 (2013) 300– 307 305
stimulation procedure remains questionable at this time. How-ever, there is some evidence that reaction time is more likely tobe modulated as performance accuracy.
One recently published randomized double-blind, placebo-controlled study investigated the effect of a single 20 Hz rTMSsession applied to the DLPFC on gamma-oscillatory activityevoked during the execution of an n-back working memory taskin schizophrenia patients and healthy controls [3]. This singlesession reduced frontal gamma-oscillatory activity in schizophre-nia patients, but enhanced it in healthy subjects in particularduring the three-back part of the n-back task [3]. The authorsexplained these effects by a complex interplay between inhibitorygamma–aminobutric acid (GABA) neurotransmission and homeo-static metaplasticity. One open-label study showed that theconsecutive 5-day application of 10 Hz rTMS over the left DLPFCimproves negative symptoms in schizophrenia patients andchanged EEG frequency bands in various cortical regions [26].
However, despite these findings of rTMS induced modulationsin EEG frequency bands, our study has not been able to revealchanges in fMRI-based network activations of the frontal lobe. Inthis context, various models for explanation can be discussed. Oneimportant fMRI study conducted on schizophrenia patients andhealthy controls indicated that the variance of prefrontal cortexactivation during the execution of an n-back task may be asso-ciated with differences in performance levels [5]. In this study,the activation pattern was dependent on the task-performanceand schizophrenia patients with a poor performance showed areduced frontal activation. On the other hand, patients with ahigh performance which was closer to that of the healthy controlgroup demonstrated an enhanced activation. These findings sup-port the hypotheses that working memory deficits in schizophreniapatients, as also observed in our study, cannot exclusively beexplained by a hypo- or hyperactivation of frontal lobe networks[5].
Though revealing performance differences in working memorybetween groups, we were not able to detect differences in BOLDactivation, at baseline. Thus, assuming that rTMS can only mod-ulate cortical networks with an abnormal activation pattern, thelacking baseline difference in BOLD activity might explain our neg-ative finding. Finally, it can be discussed that the activity differencesof the 2-back paradigms are not pronounced enough to be modu-lated by long-term rTMS. As discussed above, one study revealedrTMS-induced differences in gamma-oscillations, which were mostpronounced in the 3-back paradigm [3].
In general, the inclusion rate of patients exhibiting more severesymptoms was low due to the long intervention phase. This factmay contribute to a statistical ceiling effect in the schizophreniagroup. Furthermore, the sensitivity of instruments measuring these(slight) effects is important. Though TMS has been demonstratedto modulate local field potentials and BOLD-responses [2,51], long-lasting after-effects may be more difficult to map as they arelikely to be smaller than direct effects. Moreover, there is stillno clear knowledge about the time period that rTMS treatmenteffects would be detectable. It is possible that other techniques,like e.g. EEG, MEG or multimodal imaging would be more suit-able to detect smaller changes in brain activity. Also, computerizedcognitive performance tests may be more sensitive for the detec-tion of subtle alterations (e.g. several subtests of the TAP system).One final methodological limitation in our study is that sam-ple sizes differed between subtests with consequent effects onstatistical power. Assuming that high frequency rTMS has thepotential to facilitate and consolidate neural processing to a cer-
tain extent, one should consider concomitant cognitive trainingsor other interventions (e.g. application of d-cycloserin) to improvethe modulation of complex cognitive functions by a metaplasticapproach.
3 ain Re
C
r
A
aANoPt
G
A
t
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
06 B. Guse et al. / Behavioural Br
onflict of interest
The authors report no actual or potential conflicts of interest aselated to this report.
cknowledgments
This work was supported by the University Medical Centernd the MR-Research in Neurology and Psychiatry, Georg-ugust-University Goettingen and by the Institute of Cognitiveeuroscience, Ruhr-University Bochum, further by the Departmentf Psychology, University of Edinburgh, UK. We specially thank I.fahlert, U. Engelhardt and M. Keil for their individual contributiono this study.
This work is a subproject of a multicenter trial funded by theerman Research Foundation (DFG: grant FA 241/10-1).
ppendix A. Supplementary data
Supplementary data associated with this article can be found, inhe online version, at http://dx.doi.org/10.1016/j.bbr.2012.09.034.
eferences
[1] Addington D, Addington J, Maticka-Tyndale E. Assessing depression inschizophrenia: the Calgary Depression Scale. British Journal of Psychiatry(Suppl) 1993;22:39–44.
[2] Allen EA, Pasley BN, Duong T, Freeman RD. Transcranial magnetic stim-ulation elicits coupled neural and hemodynamic consequences. Science2007;317:1918–21.
[3] Barr MS, Farzan F, Arenovich T, Chen R, Fitzgerald PB, Daskalakis ZJ. The effectof repetitive transcranial magnetic stimulation on gamma oscillatory activityin schizophrenia. PLoS ONE 2011;6(7):1–11.
[4] Butefisch CM, Khurana V, Kopylev L, Cohen LG. Enhancing encoding of a motormemory in the primary motor cortex by cortical stimulation. Journal of Neu-rophysiology 2004;91:2110–6.
[5] Callicott JH, Mattay VS, Verschinski BA, Marenco S, Egan MF, Weinberger DR.Complexity of prefrontal cortical dysfunction in schizophrenia: more than upor down. American Journal of Psychiatry 2003;160:2209–15.
[6] Cannon TD, Glahn DC, Kim J, Van Erp TGM, Karlsgodt K, Cohen MS, et al. Dor-solateral prefrontal cortex activity during maintenance and manipulation ofinformation in working memory in patients with schizophrenia. Archives ofGeneral Psychiatry 2005;62:1071–80.
[7] Cordes J, Falkai P, Guse B, Hasan A, Schneider-Axmann T, Arends M, et al. Repet-itive transcranial magnetic stimulation for treatment of negative symptoms inresidual schizophrenia: rationale and design of a sham-controlled, randomizedmulticenter study. European Archives of Psychiatry and Clinical Neuroscience2009;259(Suppl. 2):189–97.
[8] Demirtas-Tatlidede A, Vahabzadeh-Hagh A, Pascual-Leone A. Can noninvasivebrain stimulation enhance cognition in neuropsychiatric disorders? Neu-ropharmacology 2012 [PMID: 22749945, epub ahead of print].
[9] D’Esposito M, Postle BR, Rypma B. Prefrontal cortical contributions to work-ing memory: evidence from event-related fMRI studies. Experimental BrainResearch 2000;133:3–11.
10] Dlabac-de Lange J, Knegtering R, Aleman A. Repetitive transcranial magneticstimulation for negative symptoms of schizophrenia: review and meta-analysis. Journal of Clinical Psychiatry 2010;71(4):411–8.
11] Duque J, Mazzocchio R, Stefan K, Hummel F, Olivier E, Cohen LG. Memoryformation in the motor cortex ipsilateral to a training hand. Cerebral Cortex2008;18:1395–406.
12] Evers S, Böckermann I, Nyhuis PW. The impact of transcranial magnetic stimu-lation on cognitive processing: an event-related potential study. NeuroReport2001;12:2915–8.
14] Fitzgerald PB, Maller JJ, Hoy KE, Thomson R, Daskalakis ZJ. Exploring the optimalsite for the localization of dorsolateral prefrontal cortex in brain stimulationexperiments. Brain Stimulation 2009;2:234–7.
16] Goff DC, Hill M, Barch D. The treatment of cognitive impairment in schizophre-nia. Pharmacology Biochemistry and Behavior 2011;99(2):245–53.
17] Grant DA, Berg EA. Wisconsin card sorting test. Göttingen: Hofgrefe-Verlag;1993.
18] Green MF. What are the functional consequences of neurocognitive deficits inschizophrenia? American Journal of Psychiatry 1996;153(3):321–30.
19] Guse B, Wobrock T, Falkai P. Cognitive effects of high frequency repetitivetranscranial magnetic stimulation: a systematic review. Journal of NeuralTransmission 2010;117(1):105–22.
20] Hallett M. Transcranial magnetic stimulation – a primer. Neuron 2007;55(2):187–99.
[
[
- 61
search 237 (2013) 300– 307
21] Hamada M, Murase N, Hasan A, Balaratnam M, Rothwell JC. The role of interneu-ron networks in driving human motor cortical plasticity. Cerebral Cortex 2012[epub ahead of print, PMID: 22661405].
22] Hasan A, Hamada M, Nitsche MA, Ruge D, Galea JM, Wobrock T,et al. Direct-current-dependent shift of theta-burst-induced plasticity inthe human motor cortex. Experimental Brain Research 2012;217(1):15–23.
24] Hoe M, Nakagami E, Green MF, Brekke JS. The causal relationships betweenneurocognition, social cognition and functional outcome over time inschizophrenia: a latent difference score approach. Psychological Medicine2012;5::1–13.
26] Jandl M, Bittner R, Sack A, Weber B, Günther T, Pieschl D, et al. Changes innegative symptoms and EEG in schizophrenic patients after repetitive transcra-nial magnetic stimulation (rTMS): an open-label pilot study. Journal of NeuralTransmission 2005;112(7):955–67.
27] Kaminski JA, Korb FM, Villringer A, Ott DVM. Transcranial magnetic stimulationintensities in cognitive paradigms. PLoS 2011;6(9):1–11.
28] Kay S, Fiszbein A, Opler L. The positive and negative syndrome scale (PANSS)for Schizophrenia. Schizophrenia Bulletin 1987;13:261–76.
29] Klimesch W, Sauseng P, Gerloff C. Enhancing cognitive performance with trans-cranial magnetic stimulation at human individual alpha frequency. EuropeanJournal of Neuroscience 2003;17:1129–33.
30] Mesholam-Gately RI, Giulliano AJ, Goff KP, Faraone SV, Seidman LJ. Neurocogni-tion in first-episode schizophrenia: a meta-analytic review. Neuropsychology2009;23(3):315–36.
31] Montgomery SA, Asberg M. A new depression scale designed to be sensitive tochange. British Journal of Psychiatry 1979;134:382–9.
32] Mueser KT, McGurk SR. Schizophrenia: review article. Lancet 2004;363:2063–72.
33] Mull BR, Seyal M. Transcranial magnetic stimulation of left prefrontal corteximpairs working memory. Clinical Neurophysiology 2001;112:1672–5.
34] NIMH. Clinical Global Impression (CGI). 1976.35] Owen AM, McMillan KM, Laird AR, Bullmore E. N-back working memory
paradigm: a meta-analysis of normative functional neuroimaging studies.Human Brain Mapping 2005;25:46–59.
37] Pascual-Leone A, Valls-Sole J, Wassermann EM, Hallett M. Responses to rapid-rate transcranial magnetic stimulation of the human motor cortex. Brain1994;117:847–58.
38] Paulesu E, Frith CD, Frackowiak RS. The neural correlates of the verbal compo-nent of working memory. Nature 1993;362:342–5.
39] Perlstein WM, Dixit NK, Carter CS, Noll DC, Cohen JD. Prefrontal cortex dys-function mediates deficits in working memory and prepotent responding inschizophrenia. Biological Psychiatry 2003;53:25–38.
40] Petrides M. Lateral prefrontal cortex: architectonic and functional organization.Philosophical Transactions of the Royal Society of London, Series B: BiologicalSciences 2005;360:781–95.
41] Reis J, Robertson E, Krakauer JW, Rothwell J, Marshall L, Gerloff C, et al. Consen-sus: can tDCS and TMS enhance motor learning and memory formation? BrainStimulation 2008;1(4):363–9.
42] Reis J, Schambra HM, Cohen LG, Buch ER, Fritsch B, Zarahn E, et al. Noninva-sive cortical stimulation enhances motor skill acquisition over multiple daysthrough an effect on consolidation. Proceedings of the National Academy ofSciences, United States of America 2009;106:1590–5.
43] Reitan RM. The relation of the trail making test to organic brain damage. Journalof Constructivist Psychology 1958;19:393–4.
44] Ridding MC, Ziemann U. Determinants of the induction of cortical plasticityby non-invasive brain stimulation in healthy subjects. Journal of Physiology2010;588(13):2291–304.
46] Rossi S, Hallett M, Rossini PM, Pascual-Leone A, Safety of TMS ConsensusGroup. Safety, ethical considerations, and application guidelines for the useof transcranial magnetic stimulation in clinical practice and research. ClinicalNeurophysiology 2009;120(12):2008–39.
47] Rossini PM, Barker AT, Berardelli A, Caramia MD, Caruso G, Cracco RQ, et al.Non-invasive electrical and magnetic stimulation of the brain, spinal cord androots: basic principles and procedures for routine clinical application. Reportof an IFCN committee. Electroencephalography and Clinical Neurophysiology1994;91:79–92.
48] Rothwell JC. Using transcranial magnetic stimulation methods to probe con-nectivity between motor areas of the brain. Human Movement Science2011;30(5):906–15.
49] Rusjan PM, Barr MS, Farzan F, Arenovich T, Maller JJ, Fitzgerald PB, DaskalakisZJ. Optimal transcranial magnetic stimulation coil placement for targeting thedorsolateral prefrontal cortex using novel magnetic resonance image-guidedneuronavigation. Human Brain Mapping 2010;31:1643–52.
50] Rypma B, Berger JS, D’Esposito M. The influence of working-memory demandand subject performance on prefrontal cortical activity. Journal of CognitiveNeuroscience 2002;14:721–31.
51] Sarfeld AS, Diekhoff S, Wang LE, Liuzzi G, Uludag K, Eickhoff SB, et al. Con-vergence of human brain mapping tools: neuronavigated TMS parametersand fMRI activity in the hand motor area. Human Brain Mapping 2011,http://dx.doi.org/10.1002/hbm.21272.
53] Silver H, Feldman P, Bilker W. Working memory deficit as a core neu-ropsychological dysfunction in schizophrenia. American Journal of Psychiatry2003;160:1809–16.
54] Smith EE, Jonides J. Storage and executive processes in the frontal lobes. Science1999;283:1657–61.
-

ain Re
[
[
[
[
[
[
B. Guse et al. / Behavioural Br
55] Smith EE, Jonides J, Koeppe RA. Dissociating verbal and spatial working memoryusing PET. Cerebral Cortex 1996;6:11–20.
56] Wager TD, Smith EE. Neuroimaging studies of working memory: a meta-analysis. Cognitive, Affective, and Behavioral Neuroscience 2003;3:255–74.
58] Wassermann EM. Risk and safety of repetitive transcranial magnetic stim-
ulation: report and suggested guidelines from the International Workshopof Repetitive Transcranial Magnetic Stimulation. Electroencephalography andClinical Neurophysiology 1998;108(1):1–16.59] Wittchen, Kohler, Zauding (dt. Bearbeitung). Global assessment scale of func-tioning (GAF); 1989.
[
- 62 -
search 237 (2013) 300– 307 307
60] Yamanaka K, Yamagata B, Tomioka H, Kawasaki S, Mimura M. Trans-cranial magnetic stimulation of the parietal cortex facilitates spatialworking memory: near-infrared spectroscopy study. Cerebral Cortex 2010;20:1037–45.
61] Ziemann U, Paulus W, Nitsche MA, Pascual-Leone A, Byblow WD, Berardelli
A, et al. Consensus: motor cortex plasticity protocols. Brain Stimulation2008;1:164–82.62] Zimmermann, P, Fimm, B. Neuropsychologische Testbatterie zur Erfassung vonAufmerksamkeitsdefiziten. Freiburg: Psychologisches Institut der Universität;1989.

3 Discussion
Prior to submission of the thesis, recruitment and data acquisition for the first
described trial (see 2.1.) was completed while data analysis for all centres is still
ongoing. Nevertheless, a first insight into the unpublished psychopathological findings
from our sub-sample will be provided in the following discussion. This chapter is
subdivided into a brief introduction, followed by a question-based discussion of our
results, some general study limitations and a conclusion including future perspectives.
Regarding the scientific basis, negative symptoms in schizophrenia have been closely
linked to DLPFC dysfunction due to deficient neuronal integrity and brain metabolism.
Inefficient dynamic modulation of DLPFC activity has been shown to impair working
memory performance in schizophrenia. TMS is a non-invasive method that is able to
modulate activity states in the brain and to evoke focal plasticity shifts (Esser et al.,
2006; Reis et al., 2008). rTMS has further been proven to produce outlasting
consolidation effects in the human motor system that indicate behavioural changes (e.g.
Reis et al., 2008, 2009; Ziemann et al. 2008). According to the “Hebbian”
characteristics of synaptic plasticity, long-term potentiation (LTP) can be triggered
using repetitive TMS (Hebb, 1949; Esser et al., 2006). However, these mechanisms
have been mainly studied in the motor cortex (Ilic & Ziemann, 2005). Vorel and
Lisanby (2008) provided an issue of the potential clinical relevance of synaptic
plasticity in the prefrontal cortex: LTP could selectively strengthen specific inputs into
the PFC, thereby filtering other inputs and thus representing a cellular mechanism of
attention. Alternatively, LTP could strengthen neuronal circuits within the PFC or boost
PFC metabolism and function overall, including executive, planning and motor
function. Single session rTMS studies have demonstrated transient cognitive
enhancement at higher frequencies (see 1.2.3.2). The cognitive effect of repeated
sessions has been rather unexplored in the field. However, for therapeutic purposes
outlasting rTMS effects would be essential. So far, long-term rTMS has been
successfully applied in clinical settings aiming at psychopathological improvement (see
1.2.3.1). But systematic investigations in larger samples with improved methodology
- 63 -
are lacking. Furthermore, the outlasting effect on cognition and brain physiology has to
be studied systematically.
Therefore, the major aim of this thesis was to establish if 1.) high frequency long-
term rTMS is able to improve psychopathology, specifically negative symptoms, in
patients with schizophrenia, if 2.) high frequency long-term rTMS has a beneficial
effect on cognition, and if 3.) high frequency long-term rTMS can improve WM
dysfunction in patients with schizophrenia compared to healthy controls. A further
objective was to investigate whether this kind of brain stimulation influences brain
activation within the WM network effectively.
3.1 Does rTMS improve Psychopathology in Patients with Schizophrenia?
Below, preliminary psychopathological findings are provided from our sub-sample
(see 2.3). To date this data is unpublished as it is the main objective of the multicentre-
trial outlined in chapter 2.1.
Psychopathological results indicate a tendency to selective psychopathological
improvement due to long-term rTMS treatment. No deterioration has been found.
Firstly, with regard to the primary outcome variable, analysis on the negative symptom
subscale of the PANSS demonstrated a significant main effect of time of measurement
(F(1, 23) = 33.12, p < .001) and no statistically relevant interactions. The PANSS
negative symptoms improved in both stimulation conditions and thus, cannot be
attributed to rTMS intervention. More interestingly, an improvement in the PANSS
positive symptoms score emerged after active stimulation. The ANOVA revealed a
significant main effect of time of measurement (F(1, 20) = 9.96, p < .01) and a time of
measurement x stimulation interaction at a trend level (F(1, 20) = 2.99, p < .10). Further
analysis revealed a significant improvement only for the active stimulation group (t(11)
= 3.05, p < .05) and thus confirmed this interaction. A similar pattern was found for the
general psychopathology subscale of the PANSS. The ANOVA indicated a significant
main effect for the time of measurement (F(1, 20) = 7.50, p < .05) but the time of
measurement x stimulation interaction did not reach significance (F(1, 20) = 2.42, p <
.14). For the PANSS total score an ANOVA revealed a significant main effect of time
of measurement (F(1, 20) = 20.96, p < .001) and a time of measurement x stimulation
- 64 -

interaction at a trend level (F(1, 20 = 3.08, p < .10). The PANSS total score
improvement can be explained by selective subscale improvement. Depressive
symptoms (MADRS) decreased after active stimulation compared to sham stimulation.
An ANOVA performed for the MADRS revealed a significant main effect for the time
of measurement (F(1, 22) = 8.87, p < .01) and a time of measurement x stimulation
interaction at a trend level (F(1, 22) = 3.73, p < .10). Post-hoc t-tests demonstrated a
significant decrease in the MADRS score for schizophrenia patients in the active
stimulation group (t(12) = 3.16, p < .01). With respect to the remaining measures
(CDSS, CGI, GAF), active stimulation could not be shown to be superior to sham
stimulation. Results point to a general clinical benefit for schizophrenia patients from a
3-week 10 Hz rTMS intervention over the DLPFC as it has been shown that certain
depressive and positive psychotic symptoms (MADRS, PANSS) selectively improved.
However, most of the above results remain on a trend level but point to symptom
improvement. These results are only preliminary and evaluation with more statistical
power is indispensable.
Nevertheless, in the event of replication in a larger sample, the effect on the
PANSS positive symptoms is amazing as we initially targeted negative symptoms with
prefrontal stimulation. However, since sum scores of the positive syndrome scale were
analyzed, there is no clear evidence about which kind of positive symptoms exactly
improved. Further investigations are necessary to subsume a specific cluster or
symptom.
Auditory hallucinations, as part of the positive syndrome scale, have been mostly
targeted using inhibitory rTMS applied to the left temporo-parietal cortex (e.g. Hoffman
et al, 2000, 2003; 2005; Poulet et al., 2005; for a review see Fitzgerald & Daskalakis,
2008 or Poulet et al., 2010). Based on this preliminary finding one should take into
account that prefrontal stimulation may trigger similar processes, possibly via inhibition
of clinically relevant remote areas. Therefore, it seems more likely that prefrontal
stimulation enhances some kind of control or coping mechanisms with consequent
effects on individual symptom management.
- 65 -

3.2 Does rTMS influence Cognition?
Our review article (see 2.2) aimed to cope with this objective and investigated the
impact of rTMS on cognition for a potential therapeutic application. We therefore
reviewed long-term high frequency rTMS studies between 1999 and 2009 stimulating
the prefrontal cortex of patients suffering from neuropsychiatric illnesses or healthy
volunteers, where the effects on cognitive functions were measured. The behavioural
outcome, subdivided in different cognitive domains, was analyzed with regard to the
impact of clinical status (patient/healthy volunteer) and stimulation type (active/sham).
The results indicate that rTMS applied at 10 Hz up to 20 Hz, over the left DLPFC,
within a range of 10-15 successive sessions at the intensity of 80-110% of the individual
motor threshold, seems to be most effective in improving cognition. In comparison,
patients (generally independent of the kind of diagnosis) tend to reach greater
improvement than healthy subjects. One of the non-clinical (healthy) groups showed
ameliorations in processing speed, all the others did not show any significant alteration.
When contrasting the clinical groups, 22 studies reported improvements spanning the
domains of attention (selective, sustained), executive functions (working memory,
cognitive flexibility and verbal fluency/ retrieval), learning and memory (verbal,
nonverbal) and processing speed. However, many studies failed to demonstrate
significant cognitive effects, but in some of them trends towards selective cognitive
improvement emerged. One can speculate as to whether healthy subjects generally
respond to a minor extent due to ceiling effects. But the amount of studies explicitly
contrasting patients with healthy controls is rare. In general, most of the clinical trials
studied the effect in depression. 3 studies stimulated patients with schizophrenia with
non-significant results for cognitive enhancement. While in 7 studies a superiority of
active stimulation towards placebo stimulation emerged in terms of significantly greater
improvement in the active condition. One limitation concerns the unanswered question
about the onset of neurocognitive testing. Most studies did not quote their exact onset
times. The delay period is important as immediate measures would record direct after-
effects rather than cumulative effects of the whole series. Taken together, results give
reason to extend research in this field as long-term high frequency rTMS has been
shown to selectively enhance cognitive processing. However, the impact of rTMS on
- 66 -

cognition has to be evaluated within systematic investigations taking into consideration
the neurobiological basis of cognitive improvement. Our third study (see 2.3) explicitly
used the combination of rTMS and fMRI to assess rTMS induced activity changes. The
results are discussed in the following section.
3.3 Does rTMS improve WM Dysfunction in Patients with Schizophrenia? Does
rTMS alter Brain Activation within the WM Network?
To address this twofold question we performed a combined rTMS and fMRI study
(see 2.3) and tried to find out whether a three-week excitatory 10 Hz rTMS applied to
the left DLPFC can improve verbal WM and modulate brain activation in schizophrenia
patients compared to healthy controls. We supposed that patients’ probable benefit in
WM performance would be higher compared to healthy controls due to ceiling effects in
healthy controls. Further, we hypothesized that patients’ WM activations would
approximate those of controls in the sense of “normalized” system recruitment due to
the intervention.
Looking at the behavioural baseline results, patients performed relatively well over
all cognitive subtests but differed from healthy subjects in several tasks. Comparisons
demonstrated a decreased number of correct responses and increased reaction times in
the 0-back condition of the verbal WM task in the schizophrenia group. Further,
decreased accuracy in the 1-back and 2-back demand of the WM task in schizophrenia
patients has been revealed. Patients showed significantly increased reaction times in the
Trail-Making Test (TMT-B, Reitan, 1958), in the Wisconsin Card Sorting Test (WCST,
Grant & Berg, 1993) and in the selective attention task of the “Tübinger
Aufmerksamkeitsbatterie” (TAP, Zimmermann & Fimm, 1989). This was expected
according to the literature (e.g. Heinrichs & Zakzanis 1998). Regarding the stimulation
effect on cognitive performance over time, the initial ANOVAs for repeated measures
remained either without interaction effects, or the interactions could not be confirmed
by post-hoc t-tests. Reaction times in the WCST significantly improved in the
schizophrenia sample after active stimulation, but to a minor extent also after placebo
stimulation. Most of the occurring effects can be explained by training effects.
Alterations over time could not be clearly attributed to type of stimulation or group.
- 67 -

Thus, an effect of real rTMS on cognitive performance cannot be confirmed in this
study. However, there is some evidence in our study that reaction time rather than
accuracy can be modulated. A recent near-infrared spectroscopy study (Yamanaka et al.
2010) shares this observation. In this single session study 5 Hz or sham TMS was
administered to the left or right parietal cortex of healthy subjects during the delay
period of a spatial WM task (control task: visuospatial attention task). Reaction times
improved in the spatial WM task after active stimulation of the right parietal cortex,
whereas accuracy did not improve. Another current rTMS/ fMRI crossover study on
healthy subjects identified neuroplastic alterations in prefrontally connected networks as
a substrate of behavioural changes (Esslinger et al., 2012). They administered once 5 Hz
real and sham rTMS to the right DLPFC and could show that reaction times after real
stimulation were significantly shorter. In our study, we aimed to improve performance
accuracy with repeated rTMS and our study failed to demonstrate accuracy effects.
However, reaction time decreases at unchanged accuracy may also reflect an
improvement in performance.
Regarding the fMRI results, multiple regression analyses revealed no statistical
significant activity change in the WM network over time, neither in the schizophrenia
nor in the healthy control sample. Active stimulation did not significantly differ from
placebo stimulation. As analyses did not reveal relevant main effects or interactions,
outlasting after-effects in the prefrontal region following high-frequency rTMS could
not be confirmed in this study.
However, consistent with the literature patients and healthy controls activated a
network including fronto- parietal and some subcortical regions during verbal WM
performance (e.g. Owen et al., 2005; Petrides, 2005). These regions demonstrated
increased activations during the 2-back condition of the task compared to the 1-back
condition. Thus, all participants enhanced activation at higher demands requiring
maintenance and manipulation abilities. The effect was equivalent for all groups over all
stimulation conditions and time points. For an overview of cortical activations in the 2-
back condition of the WM task see Figure 5 (in supplement material, 2.3).
- 68 -

Post-Treatment Pre-Treatment
HC, Sham
HC, active
SZ, sham
SZ, active
Figure 5: Brain regions activated in the 2- vs. 0-back WM contrast, p<0.001 (uncorrected) for illustration purposes. HC: healthy controls; SZ: schizophrenic patients.
The outcome is divergent from the model introduced by Callicott et al. (2003). They
assumed an inverted U-shaped BOLD-response curve during WM performance that
would be left-shifted in patients compared to controls (see 1.1.2, Figure 2A). Contrary
to this theory, patients and controls in our study seemed to follow a similar activity
curve but with some differences in performance accuracy and speed.
Our baseline results indicated performance differences in WM between groups, but
we were not able to detect differences in BOLD activation. Different explanations for
our negative findings can be discussed. Assuming that rTMS can only modulate cortical
networks with an abnormal activation pattern, the lacking baseline difference in BOLD
activity between groups might explain our results. It can be discussed that the activity
differences of the 2-back paradigms are not pronounced enough to be modulated by
long-term rTMS. One randomized double-blind, placebo-controlled study investigated
the effect of a single 20 Hz rTMS session applied to the DLPFC on gamma-oscillatory
activity evoked during the execution of an n-back WM task in schizophrenia patients
and healthy controls (Barr et al. 2011). This single session reduced frontal gamma-
- 69 -

oscillatory activity in schizophrenia patients, but enhanced it in healthy subjects, in
particular during the 3-back part of the n-back task. In line with this, a recently
published study from the same group (Barr et a., 2012) investigated, similarly to our
study, the cumulative behavioural effect of high-frequency rTMS on WM performance
in schizophrenia patients. The stimulation procedure was a little different to ours as they
stimulated over 4 weeks with 20 Hz rTMS, at 90% of the individual RMT, sequentially
over the left and right DLPFC. Performance differences between active and sham
treated patients were measured between 1- and 3-back verbal WM tasks pre- to post-
treatment. Behavioural data were compared with a non-stimulated healthy control
group. They hypothesized that rTMS intervention would normalize patients’ WM
performance to levels comparable to healthy subjects. Interestingly, they could
demonstrate that active rTMS significantly improved the accuracy in the 3-back task.
Performance levels increased in patients with active stimulation and approximated those
of controls. Reaction times and psychopathology did not improve. Apart from some
differences in methodology or samples, it seems likely that the higher demanding 3-
back condition or the sequential bilateral stimulation has been the essential factor for
this beneficial outcome. Unfortunately, the authors did not quote the exact onset of
cognitive testing after the last rTMS session. Further, additional structural/functional
MRI or neurophysiological recordings have not been conducted. However, this is an
important finding opening future perspectives in the field of neuropsychiatry which has
to be replicated in a larger sample with additional brain functional measures as the
question about whether long-term rTMS treatment is able to modulate brain activity in a
sustainable manner remains unanswered here.
Another important issue may be the possibility of diagnosis unspecific but ability
specific differences. Following this hypothesis, Callicott et al. (2003) conducted a study
on schizophrenia patients and healthy controls indicating that the variance of prefrontal
cortex activation during the execution of an n-back WM task may be associated with
differences in performance levels. In that study, the activation pattern was dependent on
the task-performance and schizophrenia patients with poor performance showed
reduced frontal activation. On the other hand, high performing patients, close to healthy
controls, demonstrated enhanced activation. These findings support the hypotheses that
WM deficits in patients with schizophrenia, as also observed in our study, cannot
exclusively be explained by a hypo- or hyperactivation of frontal lobe networks in
- 70 -

patients (Callicott et al., 2003). In our study we could not compare high- with low-
performers afterwards since groups were not adequately balanced after cut-off scoring.
Allen et al. (2007) and Sarfeld et al. (2011) have demonstrated for example that TMS
is able to modulate local field potentials and BOLD-responses. But it seems possible
that outlasting after-effects are more difficult to map than direct effects. Moreover, there
is still no clear knowledge about the time period that rTMS treatment effects would be
detectable. An optimal time schedule is substantially relevant for the outcome. Our
review indicates, as also mentioned in 3.1, discrepancies throughout the literature
concerning the onsets of cognitive testing after rTMS administration. Studies
investigating systematically the duration of the induced cognitive effects were lacking,
but one can assume, based on the effects on psychopathology (e.g. improvement of
mood), that also the cognitive improvement persists for a certain period of time. Bäumer
et al. (2003) systematically evaluated the after-effects of two premotor 1 Hz rTMS on
motor cortex excitability in healthy humans. Direct effects after the first session lasted
for less than 30 min., whereas after the second session at day 2 this effect lasted for at
least 2 hours. Stimulation on day 1 and 7 (with increased decay) only led to a 30 min.
after-effect again. The authors concluded that rTMS evokes cumulative plastic changes
of motor cortex excitability when repeated within 24h but not after 1 week, implying
memory formation after the first train lasting more than a day but less than a week.
Based on these and other results we conducted our fMRI and neuropsychological post-
measure around 1-2 hours after the last rTMS session. However, it is possible that
neuroplastic alterations, as it has been shown for the motor cortex, are not directly
transferable into other brain areas. Results of an rTMS study stimulating over the left
superior temporal area in healthy volunteers indicate dynamic alterations of gray matter
(GM) density after 5 days of real rTMS (1 Hz, 110% of RMT) (May et al., 2007).
These effects were not attended by differences in pure tone audiometry (behavioural
outcome) rather pointing to alterations in auditory processing. Selective gray matter
increase in the target region could not be clearly confirmed to be behaviorally relevant.
Nevertheless, the authors concluded that this period of time corresponds to the onset of
therapeutic effects in neuropsychiatric diseases following rTMS or antipsychotic agents
(Stahl et al., 2001; Tergau et al., 1999). The results underline the cumulative effect of
consecutive rTMS out of the motor cortex and indicate a similar onset of
- 71 -

psychopathological changes and neuroplastic alterations which generally confirms our
methodology.
It still remains possible, that there are no neuroplastic effects following rTMS
intervention in our study. However, given that subtle functional-behavioural changes
due to rTMS occurred but just remained undetected in our study, one should consider
the application of other techniques like EEG, MEG, NIRS or multimodal imaging being
more suitable to detect subtle changes in brain activity. Further, it would be promising
to introduce more specific cognitive performance tests which are more sensitive for
subtle alterations (e.g. computerized tests such as the subtests of the TAP-system,
Zimmermann & Fimm, 1989).
Assuming that high frequency rTMS generally has the potential to facilitate and
consolidate neural processing to a certain extent, it could be worth adding concomitant
cognitive trainings to improve the modulation of complex cognitive functions. A study
by Bentwich et al. (2011) supports the potential of synergistic effects. Results indicate
beneficial effects of rTMS combined with cognitive training (COG) in Alzheimer’s
disease (AD). Patients, treated with cholinesterase inhibitors, were subjected to daily
rTMS-COG sessions for 6 weeks, followed by maintenance sessions (2/week) for 3
months. Six brain regions were stimulated, three of them separately each day. COG
tasks fitted these regions and comprised different verbal, spatial or executive domains
(see Alzheimer Disease Assessment Scale-cognition/ ADAS-cog, Rosen et al., 1984).
Task difficulty was individually adjusted once a week. Overall results showed
significant improvement of about 4 points for ADAS-cog scores after 6 weeks and 4.5
months. An average improvement of less than 2.6 points in ADAS-cog scores was
recorded in studies with the same treatment periods but using COG alone (e.g. Orrell et
al., 2005; Tárraga et al., 2006). Moreover, the average improvement with the currently
approved drugs for AD are about 2.7 ADAS-cog points for a similar time condition
(Birks et al., 2009; for an overview see Bentwich et al., 2011). These results reflect the
impact of rTMS on the potentiation or fascilitation of cognitive training effects. If
replicated in other contexts or disorders results provide future perspectives for target-
oriented cognitive modulation.
In short, the impact of high frequency rTMS on neuronal activation or cognitive
enhancement outlasting the stimulation procedure remains questionable at this time.
However, data are convincing that we should take into account higher cognitive
- 72 -

demands in future studies. Furthermore, we should prove systematically whether
(sequential) bilateral stimulation would be superior to unilateral stimulation with regard
to cognitive improvement. Methodology has to be advanced, measuring instruments to
be more sensitive towards subtle alterations. Importantly, the synergistic effect of rTMS
and cognitive training should be refined in future studies.
3.4 General Limitations
A general limitation concerns the quite low inclusion rate of patients exhibiting more
severe symptoms that is possibly due to the long intervention phase. This may have
contributed to a statistical ceiling effect in the schizophrenia group (as well as minor
task difficulty). Further, sample sizes differed between cognitive subtests with
consequent effects on statistical power. Fortunately, some of the tests will be evaluated
multi-centrically providing increased power. Another restriction may be the relatively
short period of medication stability of 2 weeks before inclusion in our trial.
Nevertheless, active and sham group had balanced medication levels (chlorpromazine
adjusted) at baseline and their doses were stable in the course of the study. A further
limitation may concern the question about optimal stimulation parameters for the
induction of neuroplastic changes. Apart from the stimulation frequency or intensity, it
might be essential to set the optimal inter-train-interval (time between TMS trains/
relaxation time) for plasticity induction. One unresolved issue is our still limited
knowledge about whether these parameters are transferable from the motor cortex to
prefrontal areas.
- 73 -

3.5 Conclusion and Future Perspective
Overall, it still remains possible that repeated rTMS is not able to influence cognitive
performance or underlying activation pattern effectively. However, it seems likely that
some limitations in our study concerning the sample (e.g. size, severity of symptoms/
duration of illness) or some kind of methodology (e.g. sensitivity of measuring
instruments, task difficulty) have contributed to this negative cognitive outcome. In
comparison with the recently published study from Barr et al. (2012), one main point
explaining our negative finding could be the relative ceiling effect of patients and
controls at the task difficulties 1- and 2-back. Given that only deviant activation pattern
and deficient behaviour are able to be modulated with rTMS, it seems possible that the
task demand has to be increased to get more pronounced activation and behavioural
differences. In line with Barr et al. (2012) we therefore assume, that an additional 3-
back task would have been beneficial for the outcome. Further, a (sequential) bilateral
stimulation may provide a promising perspective. Most of the pilot studies investigating
psychopathological or cognitive effects stimulated unilaterally (see 1.2.3, Table 1 or see
2.2 for the review article). However, in the study from Barr et al. (2012) the cognitive-
behavioural effects were not attended by psychopathological improvement. With
respect to our psychopathological results, we were able to show preliminary but trend-
setting findings towards improvement in depressive symptoms and some positive
symptoms. These have to be proven in a larger sample. An important consideration for
future studies could be the systematic investigation of synergistic effects. rTMS has
been shown to facilitate cognitive processes to a certain extent and might thus be able to
potentiate or strengthen specific cognitive training effects.
However, it is obvious that brain stimulation itself is not able to modulate the
complex interplay of functional networks in such a way that would be necessary e.g. for
social interactions. Thus, regarding the spectrum and complexity of psychosis
symptoms, one should take into account psychotherapeutic interventions such as
training of social and emotional competence, interpersonal therapy and training of
problem solving strategies. Another essential part could be anti-stigmatism or
empowerment programs to increase self-esteem in patients. Combining different
interventions may increase the effectiveness.
- 74 -

References
Abi-Dargham A (2004). Do we still believe in the dopamine hypothesis? New data bring
new evidence. Int J Neuropsychop 7(Supplement 1):1-5.
Addington D, Addington J, Maticka-Tyndale E (1993) Assessing depression in
schizophrenia: the Calgary Depression Scale. Br J Psychiatry (Suppl.) 22: 39-44.
Aleman A, Hijman R, de Haan EH, Kahn RS (1999). Memory impairment in schizophrenia:
a meta-analysis. Am J Psychiatry 156:1358-66.
Allen EA, Pasley BN, Duong T, Freeman RD (2007). Transcranial magnetic stimulation
elicits coupled neural and hemodynamic consequences. Science 317:1918-21.
Arnsten AF, Goldman-Rakic PS (1998). Noise stress impairs prefrontal cortical cognitive
function in monkeys: evidence for a hyperdopaminergic mechanism. Arch Gen
Psychiatry 55(4):362-8.
Baddeley A (1986). Working Memory. Oxford: Oxford University Press.
Baddeley A (2000). The episodic buffer: a new component of working memory? Trends in
Cognitive Science 4:417-23.
Bajbouj M (2007). Psychiatrische Erkrankungen. In H Siebner, U Ziemann (eds.), Das TMS-
Buch. Transkranielle Magnetstimulation (pp 297-303). Heidelberg: Springer Verlag.
Barker AT, Jalinous R, Freeston IL (1985). Non - invasive magnetic stimulation of human
cortex. Lancet 1 (8437):1106-7.
Barr MS, Farzan F, Arenovich T, Chen R, Fitzgerald PB, Daskalakis ZJ (2011). The effect
of repetitive transcranial magnetic stimulation on gamma oscillatory activity in
schizophrenia. PLoS ONE 6(7):1-11.
Barr MS, Farzan F, Rajji TK, Voineskos AN, Blumberger DM, Arenovich T et al. (2012).
Can Repetitive Magnetic Stimulation Improve Cognition in Schiophrenia? Pilot Data
from a Randomized Controlled Trial. Biol Psychiatry.doi:pii: S0006-3223(12)00730-
.10.1016/j.biopsych.2012.08.020. [Epub ahead of print] .
- 75 -

Bäumer T, Lange R, Liepert J, Weiller C, Siebner HR, Rothwell JC et al. (2003). Repeated
premotor rTMS leads to cumulative plastic changes of motor cortex excitability in
humans. NeuroImage 20:550-60.
Bentwich J, Dobronevsky E, Aichenbaum S, Shorer R, Peretz R, Khaigrekht M, et al.
(2011). Beneficial effect of repetitive transcranial magnetic stimulation combined with
cognitive training for the treatment of Alzheimer’s disease: a proof of concept study. J
Neural Transm 118:463-71.
Boroojerdi B, Phipps M, Kopylev L, Wharton CM, Cohen LG, Grafman J (2001).
Enhancing analogic reasoning with rTMS over the left prefrontal cortex. Neurology
56:526-8.
Burt T, Lisanby SH, Sackheim HA (2002). Neuropsychiatric applications of transcranial
magnetic stimulation: a meta analysis. Int J Neuropsychopharmacol 5:73-103.
Callicott JH, Bertolino A, Mattay VS, Langheim FJ, Duyn J, Coppola R et al. (2000).
Physiological dysfunction of the dorsolateral prefrontal cortex in schizophrenia
revisited. Cereb Cortex 10:1078–92.
Callicott JH, Mattay VS, Verschinski BA, Marenco S, Egan MF, Weinberger DR (2003).
Complexity of Prefrontal Cortical Dysfunction in Schizophrenia: More than Up or
Down. American Journal of Psychiatry 160: 2209-15.
Cannon TD, Glahn DC, Kim J, Van Erp TGM, Karlsgodt K, Cohen MS et al. (2005).
Dorsolateral prefrontal cortex activity during maintenance and manipulation of
information in working memory in patients with schizophrenia. Arch Gen Psychiatry
62:1071-80.
Cohen LG, Roth BJ, Nilsson J (1990). Effects of coil design on delivery of focal magnetic
stimulation. Technical considerations. Electroencepahlogr Clin Neurophysiol 75, 350-
57.
Cohen E, Bernardo M, Masana J, Arrufat FJ, Navarro V, Valls-Sole et al. (1999). Repetitive
transcranial magnetic stimulation in the treatment of chronic negative schizophrenia: a
pilot study. J Neurol Neurosurg Psychiatry 67(1): 129-30.
Cordes J, Brinkmeyer J, Kotrotsios G, Arends M, Mobascher A, Agelink MW et al. (2005)
.The effect of high frequency repetitive transcranial magnetic stimulation (rTMS) on
- 76 -

negative symptoms and electrophysiological correlates of facial affect recognition in
schizophrenia. Schizophr Bull 31(2):510.
Deutsche Gesellschaft für Psychiatrie, Psychotherapie und Nervenheilkunde (DGPPN)
(Hrsg.) (2006) S3 – Praxisleitlinien in Psychiatrie und Psychotherapie. Band 1,
Behandlungsleitlinie Schizophrenie. Leitlinienprojektgruppe: W. Gaebel, P. Falkai, S.
Weinmann, T. Wobrock. Darmstadt: Steinkopff- Verlag.
D’Esposito M, Postle BR, & Rypma B (2000). Prefrontal cortical contributions to working
memory: Evidence from event-related fMRI studies. Experimental Brain Research 133,
3–11.
Epstein CM, Schwartzberg DG, Davey KR (1990). Localizing the site of magnetic brain
stimulation in human. Neurology 40, 666 – 70.
Epstein CM (2008). TMS stimulation coils. In EM Wassermann, CM Epstein, U Ziemann,
V Walsh, T Paus, SH Lisanby (eds.), The Oxford Handbook of Transcranial Magnetic
Stimulation (pp 24-32). New York: Oxford University Press.
Esser SK, Huber R, Massimini M, Peterson MJ, Ferrarelli F, Tononi G (2006). A direct
demonstration of cortical LTP in humans: a combined TMS/EEG study.
Esslinger C, Schüler N, Sauer C, Gass D, Mier D, Braun U et al., (2012). Induction and
Quantification of Prefrontal Cortical Network Plasticity Using 5 Hz rTMS and fMRI.
Hum Brain Mapp. doi: 10.1002/hbm.22165. [Epub ahead of print].
Evers S, Böckermann I, Nyhuis PW (2001). The impact of transcranial magnetic stimulation
on cognitive processing: an event-related potential study. Neuroreport 12:2915-8.
Falkai P, Wobrock T, Lieberman J, Glenthoj B, Gattaz WF, Möller HJ. WFSBP Task Force
on Treatment Guidelines for Schizophrenia (2005) Guidelines for biological treatment
of schizophrenia, part 1: acute treatment of schizophrenia. World J Biol Psychiatry 6
(3): 132-91.
Falkai P, Wobrock T, Lieberman J, Glenthoj B, Gattaz WF, Moller HJ. WFSBP Task Force
on Treatment Guidelines for Schizophrenia (2006) Guidelines for biological treatment
of schizophrenia, part 2: long-term treatment of schizophrenia. World J Biol Psychiatry
7(1): 5-40.
- 77 -

Fitzgerald PB, Benitez J, de Castella A, Daskalakis ZJ, Brown TL, Kulkarni J (2006). A
randomized, controlled trial of sequential bilateral repetitive transcranial magnetic
stimulation for treatment-resistant depression. American Journal of Psychiatry 163:88-
94.
Fitzgerald PB, Daskalakis ZJ (2008). A review of repetitive transcranial magnetic
stimulation use in the treatment of schizophrenia. Can J Psychiatry 53(9):567-76.
Floresco SB, Grace AA (2003). Gating of hippocampal-evoked activity in prefrontal cortical
neurons by inputs from the mediodorsal thalamus and ventral tegmental area. J Neurosci
21:2851-60.
Fox P, Ingham R, George MS, Mayberg H, Ingham J, Roby J et al. (1997). Imaging human
intra-cerebral connectivity by PET during TMS. NeuroReport 8: 2787-91.
Funahashi S (2007). The general purpose working memory system and functions of the
dorsolateral prefrontal cortex. In N Osaka, RH Logie, M D’Esposito (eds.), The
Cognitive Neuroscience of Working Memory (pp. 213-229). New York: Oxford
University Press.
Goff DC, Evins AE (1998) Negative symptoms in schizophrenia: neurobiological models
and treatment response. Harv Rev Psychiatry 6(2): 59-77.
George MS, Belmaker RH (2000) Transcranial magnetic stimulation in neuropsychiatry.
APA, Washington DC.
Green MF, Kern RS, Braff DL, Mintz J (2000). Neurocognitive deficits and functional
outcome in schizophrenia: are we measuring the “right stuff”? Schizophr Bull 26:119-
36.
Grant DA, Berg EA (1993). Wisconsin card sorting test. Göttingen, Hogrefe-Verlag.
Hajak G, Marienhagen J, Langguth B, Werner S, Binder H, Eichhammer P (2004). High-
frequency repetitive transcranial magnetic stimulation in schizophrenia: a combined
treatment and neuroimaging study. Psychol Med 34 (7):1157-63.
Hallett M. (2007). Transcranial magnetic stimulation: a primer. Neuron 55(2):187-99.
Haraldsson HM, Ferrarelli F, Kalin NH, Tononi G (2004). Transcranial magnetic
stimulation in the investigation and treatment of schizophrenia: a review. Schizophr Res
71:1-16.
- 78 -

Hebb DO (1949). The Organization of Behaviour. Wiley, New York.
Heinrichs RW, Zakzanis KK (1998). Neurocognitive deficit in schizophrenia: a quantitative
review of the evidence. Neuropsychol 12(3):426-45.
Henry JD, Crawford JR (2005). A meta-analytic review of verbal fluency deficits in
schizophrenia relative to other neurocognitive deficits. Cogn Neuropsychiatry 10:1-33.
Herold C, Diekamp B, Güntürkün O (2008). Stimulation of dopamine D1 receptors in the
avian fronto-striatal system adjusts daily cognitive fluctuations. Behav Brain Res
194:223-9.
Hoffman RE, Boutros NN, Hu S, Berman RM, Krystal JH, Charney DS (2000). Transcranial
magnetic stimulation and auditory hallucinations in schizophrenia. Lancet 355:1073-5.
Hoffman RE, Cavus I (2002). Slow transcranial magnetic stimulation, long-term
depotentiation, and brain hyperexcitability disorders. Am J Psychiatry 159: 1093-102.
Hoffman RE, Gueorguieva R, Hawkins KA, Varanko M, Boutros NN, Wu YT, et al. (2005).
Temporoparietal transcranial magnetic stimulation for auditory hallucinations: safety,
efficacy and moderators in a fifty patient sample. Biol Psychiatry 58(2):97-104.
Hoffman RE, Hawkins KA, Gueorguieva R, Boutros NN, Rachid F, Carrol K et al. (2003).
Transcranial magnetic stimulation of the left temporoparietal cortex and medication-
resistant auditory hallucinations. Arch Gen Psychiatry 60(1):49-56.
Huber TJ, Schneider U, Rollnik JD (2003). Gender differences in the effect of repetitive
transcranial magnetic stimulation in schizophrenia. J Psychiatry Res 30, 120(1): 103-5.
Huettel SA, Song AW, McCarthy G (eds.) (2004). Functional Magnetic Resonance
Imaging. Sinauer Associates, Inc. Publishers Sunderland, Massachusetts, U.S.A.
Ilic TV, Ziemann U (2005). Exploring motor cortical plasticity using transcranial magnetic
stimulation in humans. Annals of the New York Academy of Sciences 1048:175-84.
Jandl M, Bittner R, Sack A, Weber B, Günther T, Maurer K et al. (2004). Effects of rTMS
on negative symptoms and EEG-topography in schizophrenic patients. European
Psychiatry 19 (Suppl. 1):164.
- 79 -
Jin Y, Potkin SG, Kemp AS, Huerta ST, Alva G, Thai TM et al. (2006). Therapeutic effects
of individualized alpha frequency transcranial magnetic stimulation ({alpha}TMS) on
the negative symptoms of schizophrenia. Schizophr Bull 32(3):556-61.
Johnson MR, Morris NA, Astur RS, Calhoun VD, Mathalon DH, Kiehl KA et al. (2006). A
Functional Magnetic Resonance Imaging Study of Working Memory Abnormalities in
Schizophrenia. Biological Psychiatry 60: 11-21.
Johnson-Selfridge M, Zalewski C (2001). Moderator variables of executive functioning in
schizophrenia: meta-analytic findings. Schizophr Bull 27:305-16.
Kay SR, Fiszbein A, Opler LA (1987). The Positive and Negative Syndrome Scale (PANSS)
for schizophrenia. Schizophrenia Bulltin 13:261-76.
Kellermann T (2007). Evaluation von Gruppenunterschieden bei fMRI- Daten an einem
Beispiel aus der psychiatrischen Forschung (S 13-17). Dissertationsschrift, Rheinisch-
Westfälische Technische Hochschule Aachen.
Kellermann T, Stöcker T, Shah NJ (2008). Methodik der funktionellen
Magnetresonanztomographie. In T Kircher, S Gauggel (Hrsg.), Neuropsychologie der
Schizophrenie. Symptome, Kognition, Gehirn (S 20-35). Heidelberg: Springer-Verlag.
Kimbrell TA, Dunn RT, George MS, Danielson AL, Willis MW, Repella JD et al. (2002).
Left prefrontal-repetitive transcranial magnetic stimulation (rTMS) and regional
cerebral glucose metabolism in normal volunteers. Psychiatry Res 115:101-13.
Klein E, Kolsky Y, Puyerovsky M, Koren D, Chistyakov A, Feinsod M (1999). Right
prefrontal slow repetitive magnetic stimulation in schizophrenia: a double-blind sham-
controlled pilot study. Biol Psychiatry 46: 1451-4.
Klimesch W, Sauseng P, Gerloff C (2003). Enhancing cognitive performance with
transcranial magnetic stimulation at human individual alpha frequency. Eur. J.
Neurosci. 17:1129-33.
Lisanby SH (2008).Therapeutic applications of TMS. In EM Wassermann, CM Epstein, U
Ziemann, V Walsh, T Paus, SH Lisanby (eds.), The Oxford Handbook of Transcranial
Magnetic Stimulation (p 609). New York: Oxford University Press.
- 80 -

Lisanby SH, Luber B, Perera T, Sackeim HA (2000). Transcranial magnetic stimulation:
Applications in basic neuroscience and neuropsychopharmacology. Int J
Neuropsychopharm 3: 259-73.
Maccabee PJ, Amassian VE (2008). Lessons learned from magnetic stimulation of physical
models and peripheral nerve in vitro. In EM Wassermann, CM Epstein, U Ziemann, V
Walsh, T Paus, SH Lisanby (eds.), The Oxford Handbook of Transcranial Magnetic
Stimulation (pp 47-56). New York: Oxford University Press.
Manoach DS, Press DZ, Thangaraj V, Searl MM, Goff DC, Halpern E et al. (1999).
Schizophrenic subjects activate dorsolateral prefrontal cortex during a working memory
task, as measured by fMRI. Biol Psychiatry 45:1128–37.
Maroun M, Richter-Levin G (2003). Exposure to acute stress blocks the induction of long-
term potentiation of amygdale-prefrontal cortex pathway in vivo. J Neurosci 23:4406-9.
Martin JL, Barbanoj MJ, Schlaepfer TE, Clos S, Pérez V, Kulisevsky J, Gironell A (2002).
Transcranial magnetic stimulation for treating depression. Cochrane Database Syst Rev
2:CD003493.
May A, Hajak G, Gänßbauer S, Steffens T, Langguth B, Kleinjung T, et al. (2007).
Structural Brain Alterations following 5 Days of Intervention: Dynamic Aspects of
Neuroplasticity. Cereb Cortex 17:205-10.
Menon V, Anagnoson RT, Mathalon DH, Glover GH, Pfefferbaum A (2001). Functional
Neuroanatomy of Auditory Working Memory in Schizophrenia: Relation to Positive
and Negative Symptoms. NeuroImage 13:433-46.
Montgomery SA, Asberg M (1979) A new depression scale designed to be sensitive to
change. Br J Psychiatry 134: 382-9.
Mottaghy FM, Hungs M, Brügmann M, Sparing R, Boroojerdi B,, Foltys H, et al. (1999).
Facilitation of picture naming after repetitive transcranial magnetic stimulation.
Neurology 53:1806-12.
Nahas Z, Molloy M, Risch SC, George MS (2000). TMS in schizophrenia. In: George MS,
Belmaker RH (eds.): Transcranial magnetic stimulation in neuropsychiatry.
Washington, DC: American Psychiatric Press 237– 52.
NIMH. Clinical Gloabal Impression (CGI). 1976.
- 81 -

Novak T, Horacek J, Mohr P, Kopecek M, Rodriguez M, Spaniel F et al. (2006). The
double-blind sham-controlled study of high-frequency rTMS (20Hz) for negative
symptoms in schizophrenia: negative results. Neuro Endocrinol Lett 27(1-2):209-13.
Okubo Y, Suhara T, Suzuki K, Kobayashi K, Inoue O, Terasaki O et al. (1997). Decreased
prefrontal dopamine D1 receptors in schizophrenia revealed by PET. Nature
385(6617):634-6.
Orrell M, Spector A, Thorgrimsen L, Woods B (2005). A pilot study examining the
effectiveness of maintenance Cognitive Stimulation Therapy (MCST) for people with
dementia. Int J Geriatr Psychiatr 20:446-51.
Overall JE, Gorham DR (1962). The brief psychiatric rating scale. Psychological Reports
1962 vol. 10, 799-812.
Owen AM, McMillan KM, Laird AR, Bullmore E (2005). N-back working memory
paradigm: a meta-analysis of normative functional neuroimaging studies. Hum Brain
Mapp 25:46-59.
Padberg F, Großheinrich N, Schläpfer TE (2007). Depressive Erkrankungen. In H Siebner,
U Ziemann (eds.), Das TMS-Buch. Transkranielle Magnetstimulation (pp 609-619).
Heidelberg: Springer Verlag.
Paulesu E, Frith CD, Frackowiak RS (1993). The neural correlates of the verbal component
of working memory. Nature (362):342-5.
Paus T, Castro-Alamancos MA, Petrides M (2001). Cortico-cortical connectivity of the
human mid-dorsolateral frontal cortex and its modulation by repetitive transcranial
magnetic stimulation. Eur J Neurosci 14: 1405-11.
Paus T, Jech R, Thompson CJ, Comeau R, Peters T, Evans AC (1997). Transcranial
magnetic stimulation during positron emission tomography: a new method for studying
connectivity of the human cerebral cortex. J Neurosci 17:3178-84.
Perlstein WM, Carter CS, Noll DC, Cohen JD (2001). Relation of prefrontal cortex
dysfunction to working memory and symptoms in schizophrenia. American Journal of
Psychiatry 158:1105-13.
- 82 -

Poulet E, Brunelin J, Bediou B, Bation R, Forgeard L, Dalery J et al. (2005). Slow
transcranial magnetic stimulation can rapidly reduce resistant auditory hallucinations in
schizophrenia. Biol Psychiatry 57(2):188-91.
Poulet E, Haesebaert F, Saoud M, Suaud-Chagny MF, Brunelin J (2010). Treatment of
schizophrenia patients and rTMS. Psychiatr Danub Suppl 1: 143-6.
Reichenberg A (2010). The assessment of neuropsychological functioning in schizophrenia.
Dialogues Clin Neurosci 12:383-92.
Reis J, Robertson E, Krakauer JW, Rothwell J, Marshall L, Gerloff C et al. (2008).
Consensus: Can tDCS and TMS enhance motor learning and memory formation? Brain
Stimul. 1(4):363-9.
Reis J, Schambra HM, Cohen LG, Buch ER, Fritsch B, Zarahn E et al. (2009). Noninvasive
cortical stimulation enhances motor skill acquisition over multiple days through an
effect on consolidation. PNAS 106:1590-5.
Reitan RM (1958). The relation of the trail making test to organic brain damage. J of Constr
Psychol. 19:393-4.
Rollnik JD, Huber TJ, Mogk H, Siggelkow S, Kropp S, Dengler R et al. (2000). High
frequency repetitive transcranial magnetic stimulation (rTMS) of the dorsolateral
prefrontal cortex in schizophrenic patients. Neuroreport 11(18): 4013 – 5.
Rollnik JD, Seifert J, Huber TJ, Becker H, Panning B, Schneider U, Emrich HM (2001)
Repetitive transcranial magnetic stimulation and electroconvulsive therapy in a patient
with treatment-resistant schizoaffective disorder. Depress Anxiety 13(2): 103-4.
Rosen WG, Mohs RC, Davis KL (1984). A new rating scale for Alzheimer’s disease. Am J
Psychiatr 141(11):1356-64.
Rossini PM, Barker AT, Berardelli A, Caramia MD, Caruso G, Cracco RQ et al. (1994).
Non-invasive electrical and magnetic stimulation of the brain, spinal cord and roots:
basic principles and procedures for routine clinical application. Report of an IFCN
committee. Electroenceph Clin Neurophysiol 91:79-92.
Rothwell JC, Hallett M, Berardelli A, Eisen A, Rossini P, Paulus W (1999). Magnetic
stimulation: motor evoked potentials. The International Federation of Clinical
Neurophysiology. Electroencephalogr Clin Neurophysiol Suppl 52:97-103.
- 83 -

Rypma, B., Berger, J. S., & D’Esposito, M. (2002). The influence of working-memory
demand and subject performance on prefrontal cortical activity. Journal of Cognitive
Neuroscience, 14, 721–31.
Sachdev P, Loo C, Mitchell P, Malhi G (2005). Transcranial magnetic stimulation for the
deficit syndrome of schizophrenia: a pilot investigation. Psychiatry Clin Neurosci 59(3):
354-7.
Sandbrink F (2008). The MEP in clinical neurodiagnosis. In EM Wassermann, CM Epstein,
U Ziemann, V Walsh, T Paus, SH Lisanby (eds.), The Oxford Handbook of
Transcranial Magnetic Stimulation (pp 24-32). New York: Oxford University Press.
Sarfeld AS, Diekhoff S, Wang LE, Liuzzi G, Uludag K, Eickhoff SB et al. (2011).
Convergence of human brain mapping tools: Neuronavigated TMS parameters and
fMRI activity in the hand motor area. Hum Brain Mapp. Doi: 10.1002/hbm.21272.
Shajahan PM, Glabus MF, Steele JD, Doris AB, Anderson K, Jenkins JA et al. (2002). Left
dorso-lateral repetitive transcranial magnetic stimulation affects cortical excitability and
functional connectivity, but does not impair cognition in major depression. Prog Neuro-
Psychoph 26:945-54.
Siebner HR, Rothwell J (2003). Transcranial magnetic stimulation: new insights into
representational cortical plasticity. Exp Brain Res148:1-16.
Silver H, Feldman P, Bilker W (2003). Working memory deficit as a core
neuropsychological dysfunction in schizophrenia. Am J Psychiatry 160: 1809–16.
Smith EE, Jonides J (1999). Storage and executive processes in the frontal lobes. Science
283:1657-61.
Smith EE, Jonides J, Koeppe RA (1996). Dissociating verbal and spatial working memory
using PET. Cereb. Cortex 6:11-20.
Speer AM, Kimbrell TA, Wassermann EM, Repella JD, Willis MW, Herscovitch P, Post
RM (2000). Opposite Effects of High and Low Frequency rTMS on Regional Brain
Activity in Depressed Patients. Society of Biological Psychiatry 48:1133-41.
Stahl SM, Nierenberg AA, Gorman JM (2001). Evidence of early onset of antidepressant
effect in randomized controlled trials. J Clin Psychiatry 62(Suppl4):17-23, discussion
37-40.
- 84 -

Strafella AP, Paus T, Barrett J, Dagher A (2001). Repetitive transcranial magnetic
stimulation of the human prefrontal cortex induces dopamine release in the caudate
nucleus. J Neurosci 21 (15):RC 157.
Tárraga L, Boada M, Modinos G, Espinosa A, Diego S, Morera A, et al. (2006). A
randomised pilot study to assess the efficacy of an interactive, multimedia tool of
cognitive stimulation in Alzheimer’s disease. J Neurol Neurosurg Psychiatr
77(10):1116-21.
Teneback CC, Nahas Z, Speer AM., Molloy M, Stallings LE, Spicer KM et al. (1999).
Changes in prefrontal cortex and paralimbic activity in depression following two weeks
of daily left prefrontal TMS. J Neuropsychiatry Clin Neurosci 11: 426-35.
Tergau F, Naumann U, Paulus W, Steinhoff BJ (1999). Low-frequency repetitive
transcranial magnetic stimulation improves intractable epilepsy. Lancet 353:2209.
Töpper R, Mottaghy FM, Brügmann M, Noth J, Huber W (1998). Facilitation of picture
naming by focal transcranial magnetic stimulation of Wernicke’s area. Exp. Brain Res.
121:371-8.
Ueno S, Tashiro T, Harada K (1988). Localized stimulation of neural tissues by means of a
paired configurationof time-varying magnetic fields. Journal of Applied Physiology 64,
5862-4.
Volz H, Gaser C, Hager F, Rzanny R, Ponisch J, Mentzel H et al. (1999). Decreased frontal
activation in schizophrenics during stimulation with the Continuous Performance Test -
a functional magnetic resonance imaging study. Eur Psychiatry14:17–24.
Vorel SR, Lisanby SH (2008). Therapeutic potential of TMS-induced plasticity in the
prefrontal cortex. In EM Wassermann, CM Epstein, U Ziemann, V Walsh, T Paus, SH
Lisanby (eds.), The Oxford Handbook of Transcranial Magnetic Stimulation (pp 611-
20). New York: Oxford University Press.
Wassermann EM, Lisanby SH (2001). Therapeutic application of repetitive transcranial
magnetic stimulation: a review. Clin Neurophysiol 112: 1367-77.
Winterer G, Weinberger DR (2004). Schizophrenia: Genes, dopamine and cortical signal-
to-noise ratio in schizophrenia. Trends in Neurosci 27:683-90.
- 85 -
Williams GV, Castner SA (2006). Under the curve: critical issues for elucidating D1
receptor function in working memory. Neuroscience 139:263–76.
Wittchen, Kohler, Zauding (1998) (dt. Bearbeitung). Global Assessment Scale of
Functioning (GAF).
Yamanaka K, Yamagata B, Tomioka H, Kawasaki S, Mimura M (2010). Transcranial
magnetic stimulation of the parietal cortex facilitates spatial working memory: near-
infrared spectroscopy study. Cereb Cortex 20:1037-45.
Ziemann U, Paulus W, Nitsche MA, Pascual-Leone A, Byblow WD, Berardelli A et al.
(2008). Consensus: motor cortex plasticity protocols. Brain Stim 1:164-82.
Zimmermann, P. & Fimm, B. (1989): Neuropsychologische Testbatterie zur Erfassung von
Aufmerksamkeitsdefiziten. Freiburg: Psychologisches Institut der Universität.
Internet Sources:
http://www.bci2000.org/wiki/index.php/User_Tutorial:EEG_Measurement_Setup
- 86 -

Abbreviations ADAS-cog = Alzheimer Disease Assessment Scale-cognition BA = Brodmann area BOLD = blood-oxygen-level-dependent BPRS = Brief Psychiatric Rating Scale CDSS = Calgary Depression Rating Scale for Schizophrenia CGI = the Clinical Global Impression COG = cognitive training DA(1) = dopamine dHb = deoxygenated haemoglobin DLPFC = dorsolateral prefrontal cortex ECT = electroconvulsive therapy EEG = Electroencephalography EF = electric field EMG = electromyography EPSP = excitatory postsynaptic potential ERP = Event-related potential FDI = first-dorsal interosseus muscle fMRI = functional magnetic resonance imaging GABA = gamma-aminobutyric acid GAF = the Global Assessment Scale of Functioning Hb = haemoglobin HC = healthy controls HF = high frequency Hz = Hertz (frequency) ICD-10 = International Statistical Classification of Diseases and Related Health Problems LTD = long-term depression LTP = long-term potentiation MADRS = the Montgomery and Asberg Depression Rating Scale MEG = Magnetoencephalography NIRS = Near Infrared Spectroscopy PANSS = Positive and Negative Syndrome Scale for Schizophrenia PET = Positron-Emission-Tomography PFC = prefrontal cortex rCBF = regional cerebral blood flow RMT = resting motor threshold rTMS = repetitive transcranial magnetic stimulation SGAs = second generation antipsychotics SPECT = single photon emission computed tomography SZ = schizophrenia TAP = Tübinger Aufmerksamkeitsprüfung (a test battery, by Zimmermann & Fimm, 1989) TE = echo time TR = repetition time WHO = World Health Organization WM = working memory
- 87 -

Acknowledgements
Research on working memory and the underlying cerebral network in schizophrenia
would not be possible without the aid of many participating patients and healthy
volunteers. I would like to thank all those participants who supported this work. I am
particularly indebted to PD Dr. Thomas Wobrock and Prof. Dr. Peter Falkai for
providing the opportunity to study this interesting field in combination with TMS and
fMRI. I have very much appreciated their advice, encouragement and support during the
whole phase of this thesis. I thank Prof. Dr. Boris Suchan for his external support and
supervision. For their individual contribution to this thesis and to my emotional
wellbeing I am deeply grateful to Alkomiet Hasan, Petra Bellmann-Knieps, Katrin
Radenbach, Katja Jamrozinski, Maria Keil and last but not least to my dear family. My
special thanks is also extended to all the others who contributed to this work.
- 88 -

Curriculum Vitae
Name Birgit Guse
Date of birth August 15, 1980
Place of birth Duisburg, NRW, Germany
04/11 Lab visit, University of Edinburgh, Scotland
since 2008 Ph.D. student, Institute of Cognitive Neuroscience, Ruhr-
University Bochum and University Medical Centre Goettingen,
Graduate student, Graduate Institute for Clinical Behavioural Therapy
(AWKV Kassel), Cognitive Behavioural Therapy,
Clinical associate, Dpt. for Psychiatry and Psychotherapy, University
Medical Centre, Georg-August-University Goettingen
since 2007 Research assistant, Dpt. for Psychiatry and Psychotherapy,
University Medical Centre, Georg-August-University Goettingen
2007 Diploma
2000-2007 Undergraduate student of Psychology, Ruhr-University Bochum
1991-2000 Secondary school, Geschwister-Scholl Gymnasium Marl
1987-1991 Elementary school, August-Doehr Grundschule Marl
- 89 -

List of Publications
2009
Cordes J, Falkai P, Guse B, Hasan A, Schneider-Axmann T, Arends M, et al. (2009).
Repetitive transcranial magnetic stimulation for the treatment of negative symptoms in
residual schizophrenia: rationale and design of a sham-controlled, randomized
multicenter study. European Archives of Psychiatry and Clinical Neuroscience 259
Suppl 2: S189-97.
2010
Guse B, Falkai P, Wobrock T (2010). Cognitive effects of high-frequency repetitive
transcranial magnetic stimulation: a systematic review. Journal of Neural Transmission
117(1): 105-22.
Wobrock T, Hasan A, Malchow B, Wolff-Menzler C, Guse B, Lang N, Schneider-
Axmann T, Ecker UK, Falkai P (2010). Increased cortical inhibition deficits in first-
episode schizophrenia with comorbid cannabis abuse. Psychopharmacology (Berl)
208(3): 353-63.
2011
Hasan A, Kremer L, Gruber O, Schneider-Axmann T, Guse B, Reith W, Falkai P,
Wobrock T (2011). Planum temporale asymmetry to the right hemisphere in first-
episode schizophrenia. Psychiatry Research 193(1): 56-9.
Hasan A, Nitsche MA, Rein B, Schneider-Axmann T, Guse B, Gruber O, Falkai P,
Wobrock T (2011). Dysfunctional long-term potentiation-like plasticity in
schizophrenia revealed by transcranial direct current stimulation. Behavioural Brain
Research 224(1):15-22.
Hasan A, Wobrock T, Falkai P, Schneider-Axmann T, Guse B, Backens M, Ecker UK,
Heimes J, Galea JM, Gruber O, Scherk H (2011). Hippocampal integrity and
neurocognition in first-episode schizophrenia: A multidimensional study. World J Biol
Psychiatry (Epub. ahead of print).
- 90 -

2013
Birgit Guse, Peter Falkai, Oliver Gruber, Heather Whalley, Lydia Gibson, Alkomiet
Hasan et al. (2013). The effect of long-term high frequency repetitive transcranial
magnetic stimulation on working memory in schizophrenia and healthy controls – a
randomized placebo-controlled, double-blind fMRI study. Behavioural Brain Research,
Jan 15, 237:300-7.
- 91 -