EFFECT OF ESTROGEN ADMINISTATION - …ajbasweb.com/old/ajbas/2011/59-73.pdf · the direct effect of...
15
Australian Journal of Basic and Applied Sciences, 5(2): 59-73, 2011 ISSN 1991-8178 Effect of Estrogen Administration on The Prostate of the Adult Albino Rat (Histological, Ultrastructural and Immunohistological Studies) Mohamed Emad Eldin Ibrahim, Al-Moatasem-Bellah Mohamed Al-Sherif, Sherif Mohamed Zaki, Ahmed Fouad Al-Domairy Department of Anatomy, Faculty of Medicine, Cairo University. Abstract: Background: The prostate is considered to be an androgen dependent organ. On the other hand, the presence of estrogen receptors among different tissue components of the prostate indicates the direct effect of estrogen on the prostate, beside the known indirect effect through the hypothalamo- gonadal axis. Estrogen has been incriminated in the pathogenesis of certain prostatic diseases, namely, cancer prostate, benign prostatic hyperplasia and prostatitis. Methods: 57 adult male albino rats were used in this study. The rats were divided into two groups. Control groups (normal and sham) and experimental groups which were exposed to different estrogen treatments and were further subdivided into 3 subgroups: group LA (repeated low doses group), group TA (Therapeutic dose group) and group HA (single high dose group). The animals were sacrificed and the prostatic specimen were collected and prepared for light, electron microscopically and immunohistological studies. Results: The histological examination revealed the presence of epithelial and stromal hyperplasia in all the experimental groups in a dose dependant manner, the signs of epithelial hyperplasia included papillary projections, vesicular nuclei, marginated nucleoli and double nucleoli. Other common changes included inflammatory infiltration, apoptosis and acinar dilatation. Only the (TA) and (HA) groups showed signs of dysplasia in the form of pleomorphism and hyperchromatism. The ultrastructure examination of different experimental groups revealed variable degrees of degenerative changes. The changes included irregular cell membranes, poor cytoplasmic organelles, proliferated rough endoplasmic reticulum and the appearance of cytoplasmic vacuolations and fatty like inclusions. Nuclear changes included irregular nuclear membranes and pyknotic nuclei. Again, the profound degenerative changes were marked in both the (TA) and (HA) groups. Immunohistological examination revealed decreased immunostaining reactivity in all the experimental groups compared to the control groups. A further decrease was noted in both the (TA) and (HA) groups accompanying the severe dysplasia of these groups. Conclusion: It was concluded that estrogen induces prostatic hyperplasia and prostatic inflammation. Only therapeutic or high doses of estrogen produce dysplastic changes. Within certain limits, estrogen acts in a dose dependent manner. Recommendation: It could be recommended that estrogen treatment for cancer prostate should be restricted to specific cases. Maximum attention to serious side effects has to be ensured during estrogen treatments. Further investigations are needed to prove or exclude the role of estrogen in different prostatic diseases. Key words: Estrogen, Prostate, Rats. INTRODUCTION The normal anatomical and functional growth of the prostate is mainly controlled by androgens Niu et al., (2003). However, estrogen plays an important role in prostate physiology Singh and Handelsman, (1999) indicated by the stimulatory effect of low dose estrogen on the prostate Putz et al., (2001) and the presence of estrogen receptors (ERs) in prostatic tissues Weihua et al., (2002). A role of estrogen in the development of benign prostatic hyperplasia (BPH) has been suggested; administration of estrogen has been shown to stimulate BPH in dogs Bruengger et al., (1983). BPH in man is accompanied by decreased testosterone and elevated estrogen levels Prins et al., (1996). The relationship between estrogen and cancer prostate is controversial. Kastendieck and Altenahr, (1975) suggested that epithelial metaplasia of the prostate may be caused by estrogen-androgen imbalance; Risbridger et al. (2001) found that estrogen causes a metaplastic response in prostatic tissue and Ricke et al. (2006) Corresponding Author: Sherif Mohammed Zaki, Anatomy department, Faculty of Medicine, Cairo University, El-Kasr Al Aini Street, Cairo, Egypt. Tel.: +20226706317, +200127457431, E-mail: [email protected] 59
Transcript of EFFECT OF ESTROGEN ADMINISTATION - …ajbasweb.com/old/ajbas/2011/59-73.pdf · the direct effect of...

Australian Journal of Basic and Applied Sciences, 5(2): 59-73, 2011ISSN 1991-8178
Effect of Estrogen Administration on The Prostate of the Adult Albino Rat (Histological, Ultrastructural and Immunohistological Studies)
Mohamed Emad Eldin Ibrahim, Al-Moatasem-Bellah Mohamed Al-Sherif, Sherif Mohamed Zaki,Ahmed Fouad Al-Domairy
Department of Anatomy, Faculty of Medicine, Cairo University.
Abstract: Background: The prostate is considered to be an androgen dependent organ. On the otherhand, the presence of estrogen receptors among different tissue components of the prostate indicatesthe direct effect of estrogen on the prostate, beside the known indirect effect through the hypothalamo-gonadal axis. Estrogen has been incriminated in the pathogenesis of certain prostatic diseases, namely,cancer prostate, benign prostatic hyperplasia and prostatitis. Methods: 57 adult male albino rats wereused in this study. The rats were divided into two groups. Control groups (normal and sham) andexperimental groups which were exposed to different estrogen treatments and were further subdividedinto 3 subgroups: group LA (repeated low doses group), group TA (Therapeutic dose group) andgroup HA (single high dose group). The animals were sacrificed and the prostatic specimen werecollected and prepared for light, electron microscopically and immunohistological studies. Results: Thehistological examination revealed the presence of epithelial and stromal hyperplasia in all theexperimental groups in a dose dependant manner, the signs of epithelial hyperplasia included papillaryprojections, vesicular nuclei, marginated nucleoli and double nucleoli. Other common changes includedinflammatory infiltration, apoptosis and acinar dilatation. Only the (TA) and (HA) groups showedsigns of dysplasia in the form of pleomorphism and hyperchromatism. The ultrastructure examinationof different experimental groups revealed variable degrees of degenerative changes. The changesincluded irregular cell membranes, poor cytoplasmic organelles, proliferated rough endoplasmicreticulum and the appearance of cytoplasmic vacuolations and fatty like inclusions. Nuclear changesincluded irregular nuclear membranes and pyknotic nuclei. Again, the profound degenerative changeswere marked in both the (TA) and (HA) groups. Immunohistological examination revealed decreasedimmunostaining reactivity in all the experimental groups compared to the control groups. A furtherdecrease was noted in both the (TA) and (HA) groups accompanying the severe dysplasia of thesegroups. Conclusion: It was concluded that estrogen induces prostatic hyperplasia and prostaticinflammation. Only therapeutic or high doses of estrogen produce dysplastic changes. Within certainlimits, estrogen acts in a dose dependent manner. Recommendation: It could be recommended thatestrogen treatment for cancer prostate should be restricted to specific cases. Maximum attention toserious side effects has to be ensured during estrogen treatments. Further investigations are neededto prove or exclude the role of estrogen in different prostatic diseases.
Key words: Estrogen, Prostate, Rats.
INTRODUCTION
The normal anatomical and functional growth of the prostate is mainly controlled by androgens Niu et al.,(2003). However, estrogen plays an important role in prostate physiology Singh and Handelsman, (1999)indicated by the stimulatory effect of low dose estrogen on the prostate Putz et al., (2001) and the presenceof estrogen receptors (ERs) in prostatic tissues Weihua et al., (2002).
A role of estrogen in the development of benign prostatic hyperplasia (BPH) has been suggested;administration of estrogen has been shown to stimulate BPH in dogs Bruengger et al., (1983). BPH in manis accompanied by decreased testosterone and elevated estrogen levels Prins et al., (1996).
The relationship between estrogen and cancer prostate is controversial. Kastendieck and Altenahr, (1975)suggested that epithelial metaplasia of the prostate may be caused by estrogen-androgen imbalance; Risbridgeret al. (2001) found that estrogen causes a metaplastic response in prostatic tissue and Ricke et al. (2006)
Corresponding Author: Sherif Mohammed Zaki, Anatomy department, Faculty of Medicine, Cairo University, El-Kasr AlAini Street, Cairo, Egypt. Tel.: +20226706317, +200127457431, E-mail: [email protected]
59

Aust. J. Basic & Appl. Sci., 5(2): 59-73, 2011
concluded that estrogen accompanied by testosterone promotes prostatic cancer. On the other hand, a numberof therapeutic strategies including estrogens are actively being investigated in the treatment of prostate cancer,estrogens of various types have exhibited antitumor activities both in vitro and in vivo Smith et al., (1998).It has been postulated that different responses of prostatic tissue to estrogen may be mediated by differenthormone receptors Mobley et al., (2004).
The aim of the present work was to study the different effects of estrogen on prostatic tissue the adultalbino rat using histological, ultrastructural and immunohistological techniques, trying to clarify the role ofestrogen in the development of certain prostatic diseases as well as to explore the estrogen effect that mightbe used as a guide in the treatment of cancer prostate.
MATERIAL AND METHODS
The present study was carried out on 57 adult male rats weighing 236- 370 gm obtained from animalhouse, Faculty of Medicine, Cairo University. The rats were maintained in a controlled environment with afree access to food and water. The animals were divided into the following groups
Control Groups (Normal and Sham):each group included 6 rats. The sham group received oily injections at the same regimen of the
experimental groups. The rats of the control groups were sacrificed according to the same schedule of theexperimental group.
Experimental Groups:were further subdivided into 3 subgroups:
Group LA (Repeated Low Doses Group):included 15 rats, each rat received a weekly therapeutic dose (140 µg/kg body weight) of estradiol
benzoate as subcutaneous injections for four successive weeks and were sacrificed two days after the lastinjection Kohler-Samouilidis et al., (1998).
Group TA (Therapeutic Dose Group):included 15 rats, each rat received a daily therapeutic dose (1 mg/kg body weight) of estradiol benzoate
as subcutaneous injections for 21 days and were sacrificed two days after the last injection Chrouses et al.,(2001).
Group HA (Single High Dose Group):included 15 rats, each rat received a single high dose (25 mg/kg body weight) of estradiol benzoate as
subcutaneous injection and were sacrificed two days after the injection Garcia-Florez et al., (2005).In all the experimental subgroups, the time of sacrifice was based on the finding that the peak plasma level
of estrogen was reached two days after estradiol benzoate injection Oriowo et al., (1980).The drug used was estradiol benzoate (folone®) in the form of 5 mg/ml oily solution, produced by Misr
Co. For Pharm Ind SAE. If needed, the drug was diluted in corn oil and injected subcutaneously.Rats were sacrificed by cervical dislocation, dissected and prostate specimens were collected.
Light Microscopic Study:Part of the prostatic specimens was fixed in buffered formol saline, processed for paraffin sections of 5µm
thickness and sections were stained with haematoxylin and eosin (Hx. and E.) and Masson's trichrome stainsBancroft and Gamble, (2002) for histological study.
Ultrastructural Study:The other part of the prostatic specimens was cut into small pieces, fixed in 4% glutraldehyde then washed
in phosphate buffer and post fixed in 1% osmium tetraoxide. Fixation was followed by dehydration andembedding in epoxy resins. Semithin sections were stained with toluidine blue. Ultrathin sections were stainedwith uranyl acetate and lead citrate according to Dawes (1980) then examined using Philips CM100transmission electron microscope. The examination was done in Anatomy department, Faculty of Medicine,Ain Shams University.
60

Aust. J. Basic & Appl. Sci., 5(2): 59-73, 2011
Immunohistological Study:For detection of estrogen receptors, estrogen receptor Ab-14 (Clone 1D5+6F11) Mouse Monoclonal
Antibody Neo Markers, Fermont, USA was used for immunohistology using formalin/paraffin specimens.Two tissue control slides was used, a positive control specimen from breast known to be positive to
estrogen receptors was processed exactly as other samples, the specimen was provided by the National CancerInstitute, Cairo University, another negative control specimen was prepared from one of the control prostatictissue specimens but instead of using a primary antibody, a non immune solution was used.
Scoring of ER staining intensity was done, it was classified as negative (no staining), weak (+), moderate(++), or strong (+++). Specimens were reported negative when the staining did not differ from the negativecontrol sections Makela et al., (2000).
RESULTS AND DISCUSSION
A- Histological results:Control groups:
The histological examination of the different control groups revealed nearly the same findings. Examinationof the control group specimens revealed variable sized acini, abundant secretions, and minimal stroma. Theacini were lined by normal columnar or pseudostratified columnar epithelium (figs. 1-4).
Fig. 1: A photomicrograph of a section in the prostate of a normal control rat showing normal appearanceof acini with variable sizes, abundant secretions (Se) and minimal stroma (S). (Hx. & E.; × 40).
Fig. 2: A photomicrograph of a section in the prostate of a normal control rat showing normal appearanceof acini with variable sizes ( è). Hx. & E.; × 100).
Fig. 3: A photomicrograph of a section in the prostate of a normal control rat showing normalpseudostratified columnar epithelial lining (E). (Hx. & E.; × 1000).
61

Aust. J. Basic & Appl. Sci., 5(2): 59-73, 2011
Fig. 4: A photomicrograph of a section in the prostate of a normal control rat showing minimal stroma (S)and abundant secretions (Se). (Masson's trichrome; × 100).
Experimental groups:Low dose effect group (LA):
Examination of the (LA) group revealed acini full of inflammatory cellular infiltrate (fig. 5). There wasa moderate acinar dilatation and the acini were filled with secretion with low epithelial lining (fig. 6). Thesigns of the epithelial hyperplasia were observed in this group by the appearance of vesicular nuclei, doubleand marginated nucleoli (fig. 7). Also stromal hyperplasia was observed in this group (fig. 8).
Fig. 5: A photomicrograph of cross section in the prostate of (LA) group showing acini full of inflammatorycellular infiltrate (arrows). (Hx. & E.; × 40).
Fig. 6: A photomicrograph of a section in the prostate of (LA) group showing moderate acinar dilatation(67), the acini are filled with secretion (Se) with low epithelial lining (E). (Hx. & E.; ×100).
Therapeutic dose effect group (TA):Examination of the (TA) group revealed the presence of intraluminal inflammatory infiltration (fig. 9),
moderate stromal hyperplasia and acinar hyperplasia in the form of papillary projections with abundantsecretions (figs. 10, 11, 13). The examination also revealed the appearance of signs of dysplasia, in the formof deeply stained nuclei (hyperchromatism) and different types and shapes of cells (pleomorphism) (figs. 12,14). Also some desquamated cells were noted in the acinar lumen (fig. 14).
62

Aust. J. Basic & Appl. Sci., 5(2): 59-73, 2011
Fig. 7: A photomicrograph of a section in the prostate of (LA) group showing signs of hyperplasia (vesicularnuclei (VN), double nucleoli (DNu) and nuclei with marginated nucleolus (MNu). (Hx. & E.; ×1000).
Fig. 8: A photomicrograph of a section in the prostate of (LA) group showing mild stromal hyperplasia (S).(Masson's trichrome; ×100).
Fig. 9: A photomicrograph of a section in the prostate of (TA) group showing inflammatory infiltrates(arrows). (Hx. & E.; ×100).
Fig. 10: A photomicrograph of a section in the prostate of (TA) group showing moderate stromal hyperplasia(S) and acinar papillary projections (arrows). (Hx. & E.; ×100).
63

Aust. J. Basic & Appl. Sci., 5(2): 59-73, 2011
Fig. 11: A photomicrograph of a section in the prostate of (TA) group showing acinar hyperplasia in the formof papillary projections (arrows) with abundant secretions (Se). (Hx. & E.; × 200).
Fig. 12: A photomicrograph of a section in the prostate of (TA) group showing signs of dysplasia; deeplystained nuclei (hyperchromatism) (arrow) and different types and shapes of cells (pleomorphism)(circle).(Hx. & E.; ×1000).
Fig. 13: A photomicrograph of a section in the prostate of (TA) group showing marked stromal hyperplasia(S). (Masson's trichrome; ×100).
Fig. 14: A photomicrograph of a section in the prostate of (TA) group showing dysplastic indented nuclei(arrows); some desquamated cells were noted in the acinar lumen (circle). (Toluidine blue; ×1000).
64
Aust. J. Basic & Appl. Sci., 5(2): 59-73, 2011
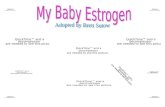
High dose effect group (HA):Examination of the (HA) group revealed the presence of acinar dilatation and epithelial hyperplasia in the
form of papillary projections (fig. 15). Also marked epithelial dysplasia (fig. 16) and stromal hyperplasia(fig. 17) were observed.
B- Ultrastructural results:Control groups:
Examination of the control groups revealed a normal appearance of the cells; the nuclei appeared normalwith apparent nucleoli and regular nuclear membranes. There were many cytoplasmic secretory granules(fig. 18).
Experimental groups:Low dose effect group (LA):
The examination of the (LA) group revealed a patchy effect, some fields showed normal cells with normalregular cellular membranes, well developed cytoplasmic organelles, secretory granules, regular nuclearmembranes and apparent nucleoli. Other fields showed cellular changes in the form of appearance ofcytoplasmic vacuolation, proliferated dilated rough endoplasmic reticulum (RER), nuclear membranesirregularity and heterolysosomes (figs. 19, 20).
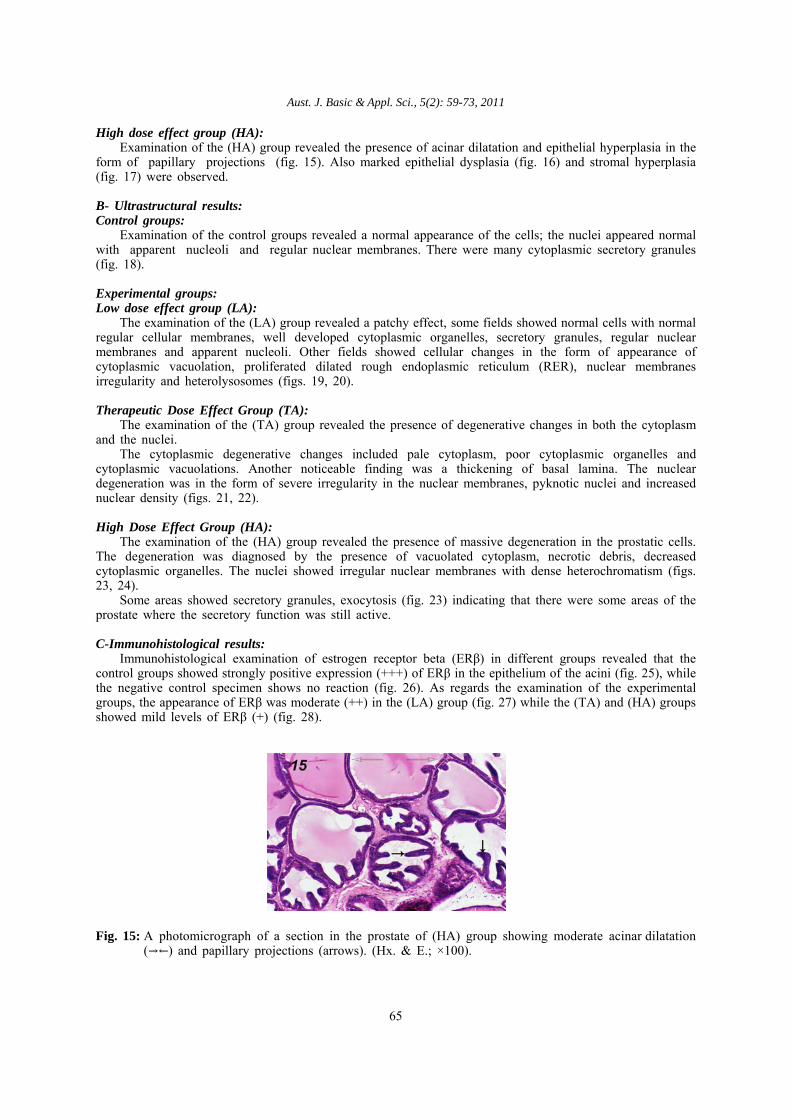
Therapeutic Dose Effect Group (TA):The examination of the (TA) group revealed the presence of degenerative changes in both the cytoplasm
and the nuclei. The cytoplasmic degenerative changes included pale cytoplasm, poor cytoplasmic organelles and
cytoplasmic vacuolations. Another noticeable finding was a thickening of basal lamina. The nucleardegeneration was in the form of severe irregularity in the nuclear membranes, pyknotic nuclei and increasednuclear density (figs. 21, 22).
High Dose Effect Group (HA):The examination of the (HA) group revealed the presence of massive degeneration in the prostatic cells.
The degeneration was diagnosed by the presence of vacuolated cytoplasm, necrotic debris, decreasedcytoplasmic organelles. The nuclei showed irregular nuclear membranes with dense heterochromatism (figs.23, 24).
Some areas showed secretory granules, exocytosis (fig. 23) indicating that there were some areas of theprostate where the secretory function was still active.
C-Immunohistological results:Immunohistological examination of estrogen receptor beta (ERβ) in different groups revealed that the
control groups showed strongly positive expression (+++) of ERβ in the epithelium of the acini (fig. 25), whilethe negative control specimen shows no reaction (fig. 26). As regards the examination of the experimentalgroups, the appearance of ERβ was moderate (++) in the (LA) group (fig. 27) while the (TA) and (HA) groupsshowed mild levels of ERβ (+) (fig. 28).
Fig. 15: A photomicrograph of a section in the prostate of (HA) group showing moderate acinar dilatation(YZ) and papillary projections (arrows). (Hx. & E.; ×100).
65

Aust. J. Basic & Appl. Sci., 5(2): 59-73, 2011
Fig. 16: A photomicrograph of a section in the prostate of (HA) group showing signs of dysplasia,hyperchromatism (arrows) and pleomorphism (circle). (Hx. & E.; ×400).
Fig. 17: A photomicrograph of a section in the prostate of (HA) showing marked stromal hyperplasia (S).(Masson's trichrome; ×100).
Fig. 18: A photomicrograph of a section in the prostate of a normal control rat showing normal part ofprostatic acini, the cells shows normal nucleus (N) with regular nuclear membrane (NM), apparentnucleolus (Nu) and secretory granules (SG). (Uranyl acetate × 3000).
66

Aust. J. Basic & Appl. Sci., 5(2): 59-73, 2011
Fig. 19: A photomicrograph of a section in the prostate of (LA) group showing patchy effect, cells withproliferated RER, other cells with dilated RER (arrow), and nuclear membrane irregularity (NM).(Uranyl acetate × 3900).
Fig. 20: A photomicrograph of a section in the prostate of (LA) group showing irregular nuclear membrane(NM) and cytoplasmic vacuolation (V), the neighboring cells shows heterolysosomes (arrows). (Uranylacetate × 11500).
Fig. 21: A photomicrograph of a section in the prostate of (TA) group showing irregular nuclear membrane(NM), pale cytoplasm (C), poor cytoplasmic organelles and thickening of the basal lamina (BL).(Uranyl acetate × 4000).
67
Aust. J. Basic & Appl. Sci., 5(2): 59-73, 2011
Fig. 22: A photomicrograph of a section in the prostate of (TA) group showing pyknotic nuclei (N), there isincreased nuclear density, the nuclear membrane shows marked irregularity (NM) and the cytoplasm(C) shows massive vacuolations (V). (Uranyl acetate × 8000).
Fig. 23: A photomicrograph of a section in the prostate of (HA) group showing luminal part of prostatic aciniwith secretory granules (SG), vacuolated cytoplasm (V), necrotic debris (arrow), decreased cytoplasmicorganelles, and exocytosis (Ex). (Uranyl acetate × 4000).
Fig. 24: A photomicrograph of a section in the prostate of (HA) group showing degenerated and rarifiedcytoplasm (C) and irregular nuclear membrane (NM) with dense heterochromatism (Ch). (Uranylacetate × 4000).
68

Aust. J. Basic & Appl. Sci., 5(2): 59-73, 2011
Fig. 25: A photomicrograph of a section in the prostate of control rat showing strongly positive (+++)immunoreactivity of ERβ (marked by the dark brown stain) (arrows). (× 400).
Fig. 26: A photomicrograph of a section in a negative control slide showing negative immunoreactivity of ERβ.(× 400).
Fig. 27: A photomicrograph of a section in the prostate of (LA) group showing moderately positive (++)immunoreactivity of ERβ (arrows). (× 400).
69

Aust. J. Basic & Appl. Sci., 5(2): 59-73, 2011
Fig. 28: A photomicrograph of a section in the prostate of (TA) group showing mildly positive (+)immunoreactivity of ERβ (arrows). (× 400).
Discussion:Estrogen plays an important role in prostate physiology Singh and Handelsman, (1999). The mechanism
of action of estrogen on the prostate includes the indirect effect through hypothalamo-pituitary-gonadal axisBrewester et al., (1997). Direct effect of estrogen on the prostate was also suggested Garcia-Florez, (2005).Estrogen may also act by reduction of testosterone synthesis either by direct effect on the testis Prins, (1992) or indirectly through LH inhibition Lane et al., (1997), prolactin release stimulation Lane et al., (1997) andaltered androgen receptor expression Pelletier, (2002).
Simulating previous studies Yoshida, (1975), the histological findings of the control groups revealed thepresence of acini variable in size, lined by columnar epithelium with minimal stroma. The ultrastructuralfindings revealed the presence of normal epithelial arrangement, well developed cytoplasmic organelles as wellas abundant cytoplasmic secretory granules. The nuclei showed regular nuclear membrane with apparentnucleoli.
Our experience revealed the presence of intraluminal inflammatory infiltrate in the all experimental groups;this finding agreed with Naslund et al. (1988) who found increased incidence and severity of non bacterialprostatitis after treating adult rats with estrogen, even treatment of neonatal rats with estrogen inducedimprinting prostatitis in adulthood. These inflammatory cells migrate to the acinar lumen through the stromaand the epithelium of the prostate (Bianco et al., 2002; Kawamura, 2002).
Apoptosis was another common feature in all the experimental groups ; this finding is shared by Tayloret al. (2005) who suggested the appearance of apoptotic cells to the down regulation effect of estrogen onthe androgen receptors.
Comparison between the histological appearances of the different experimental groups showed theappearance of stromal hyperplasia as reported by other authors (Bianco et al., 2002; Holterhus et al., 1993).
This was confirmed by the ultrastructural study as there was thickening of the basal lamina of the prostaticacini in the (TA) group. This thickening might be due to marked fibromuscular hypertrophy and widedistribution of collagen and elastic fibers adjacent to the epithelial basal lamina of the prostatic acini Scaranoet al., (2005).
Beside the stromal hyperplasia, there was also epithelial hyperplasia in the all experimental groups in theform of vesicular nuclei, double nucleoli and nuclei with marginated nucleoli. These findings were nearlysimilar to those of Bianco et al. (2002).
Estrogen was incriminated in the pathogenesis of BPH. In our study, stromal hyperplasia of the prostatewas found in all the experimental groups, in a dose dependant manner. The marked fibromuscular hypertrophyobserved after estrogen treatment in animals simulates the stromal modifications observed in BPH Scarano etal., (2005). However, regarding estrogen as a causative agent of BPH still needs further investigations.On the other hand, signs of dysplasia were only found in the (TA) and (HA) groups. The dysplastic signsincluded hyperchromatism, pleomorphism, increased mitotic figures, and damaged cytoplasmic organelles withthe presence of severe nuclear changes. These findings were previously recorded by Bernoulli et al. (2008)who correlated the dysplastic changes to the associating inflammation and stated that estrogen played asignificant role in the induction of both features.
It was apparent that the histological picture was more affected in the (TA) and (HA) groups, thehyperplasia was marked and the dysplasia was profound. The more obvious effect noticed in the (TA) and(HA) groups supported the dose dependant manner finding of Putz et al. (2001) who examined the effect of
70

Aust. J. Basic & Appl. Sci., 5(2): 59-73, 2011
seven logarithmic ranges of doses and found a dose related increased effect. The correlation of estrogen to cancer prostate is still bidirectional. The appearance of dysplasia strongly
suggests the carcinogenicity. Ho et al. (1995) stated that the administration of estrogen with androgen producesa unique lesion in the prostate, characterized by simultaneous occurrence of proliferation and apoptosisdisturbing the balance between both processes, this disturbance is often seen during cancer development. Liet al. (2001) referred its cause to epithelial basement membrane and stromal alteration leading to its hydration,a condition which is in favor of tumor growth and invasion. Furthermore, Scarano et al. (2004) reported thepattern of epithelial stratification characteristic of prostatic intraepithelial neoplasia after chronic treatment withestrogen. However, other investigators (Smith et al., 1998; Oh et al., 2004) had proven the anti cancer prostateeffect of estrogen. Estrogen has previously been extensively used in cancer prostate treatment, mostly due toits indirect inhibition of androgen through the hypothalamo-pituitary-gonadal axis. Lam et al. (2006) stated thatsecondary hormonal therapy (including estrogenic compounds) serves as an excellent therapeutic option inpatients with androgen insensitive cancer prostate patients even in which primary hormonal therapy has failed.
Like other authors (Scarano et al., 2004), our observation revealed the presence of cellular degenerationin the all experimental groups. The degenerative changes in the (LA) group were mild and patchy while inthe (TA) and (HA) groups were marked. These degenerative changes included decreased cytoplasmicorganelles, proliferated RER, decreased secretory bodies, appearance of lipid like inclusion and thick stroma.Also, there were irregular nuclear membranes and partial loss of exocytosis of the cell membranes facing thelumen indicating diminished secretory functions. These findings support the previous reports of Merk et al.(1986) who found a regression in the size of the secretory granules after estrogen treatment and the findingsof Holterhus et al. (1993) who recorded complete loss of secretory granules.
As suggested by others Makela et al., (2000), the immunohistological examination in the current workproved the presence of estrogen receptor beta (ERβ) in the cells of adult prostate, the presence of ERβ in theprostatic tissues confirms the direct effect of estrogen on the prostate. The control groups showed abundantexpression of ERβ in the epithelium of the acini (strongly positive +++), a decrease in this expression wasnoted in all the experimental groups, the appearance of ERβ was moderate (++) in most groups, furtherdecrease in ERβ level was noted in the (TA) and (HA) groups which showed mild levels of ERβ (+). Theseresults support the previous findings of Lau et al. (1998) who found a decrease in the expression of ERβfollowing the use of estrogen or orchidectomy. The further decrease of ERβ in both TA and HA groups maybe due to the fact that ERβ decreases accompanying the appearance of severe dysplasia or carcinogenesis Leavet al., (2001) due to loss of growth control Yuen et al., (2005).
Immunohistological examination for ERβ was chosen in the present study due to its importance, asdifferent ER predominance was another suggested factor which could play a role in detecting whether estrogenhas a carcinogenic effect on prostate or not. Horvath et al. (2001) demonstrated a reduction in ERβ expressionin association with the process of carcinogenesis, suggesting that ERβ might be important for the maintenanceof normal prostate epithelium and probably guarding against cancer. However, it is not yet proved if reductionin ERβ expression is causally related to the development of neoplasia or just an associated finding Harkonenand Makela, (2004).
It could be concluded that estrogen induces prostatic hyperplasia and prostatic inflammation. Onlytherapeutic or high doses of estrogen produce dysplastic changes. Within certain limits, estrogen acts in a dosedependent manner. So, it could be recommended that estrogen treatment for cancer prostate should be restrictedto specific cases. Maximum attention to serious side effects has to be ensured during estrogen treatments.Further investigations are needed to prove or exclude the role of estrogen in different prostatic diseases.
REFERENCES
Bancroft, J.D. and M. Gamble, 2002. Theory and practice of histological techniques. Fifth ed., ChurchillLivingstone. London, Edinburgh, New York, Philadelphia, St Louis, Sydney and Toronto, pp: 167-170.
Bernoulli, J., E. Yatkin, A. Laakso, M. Anttinen, M. Bosland, K. Vega, M. Kallajoki, R. Santti and L.Pylkkanen, 2008. Histopathological evidence for an association of inflammation with ductal pin like lesionsbut not with ductal adenocarcinoma in the prostate of the noble rat. Prostate, 68(7): 728-739.
Bianco, J.J., D.J. Handelsman, J.S. Pedersen and G.P. Risbridger, 2002. Direct response of the murineprostate gland and seminal vesicle to estradiol. Endocrinology, 143(12): 4922-4933.
Brewester, M.E., W.R. Anderson and E. Pop, 1997. Effect of Sustained Estradiol Release in the IntactMale Rat: Correlation of Estradiol Serum Levels with Actions on Body Weight, Serum Testosterone andPeripheral Androgen Dependent Tissues. Physiology & Behaviour, 61(2): 225-229.
Bruengger, A., G. Bartsch, B.E. Hollinger, B. Holly and H.P. Rohr, 1983. Smooth muscle cell of thecanine prostate in spontaneous benign hyperplasia, steroid induced hyperplasia and estrogen or tamoxifentreated dogs. J Urol. Dec., 130(6): 1208-1210.
71

Aust. J. Basic & Appl. Sci., 5(2): 59-73, 2011
Chrouses , G.P., E. Zoumakis and A. Gravanis, 2001. The gonadal hormones and inhibitors. In: Basic andclinical pharmacology, Katzung BG (ed.) pp: 679-687.
Dawes, C.J., 1980. Biological Techniques of Transmission Electron Microscopy, Ladel Research IndustriesInc. Pub.:1st ed. pp: 1- 16.
Garcia-Florez, M., C.A. Oliveira and H.F. Carvalho, 2005. Early effects of estrogen on the rat ventralprostate. Braz J Med Biol Res., 38(4): 487-497.
Kastendieck, H. and E. Altenahr, 1975. Morphogenesis and significance of epithelial metaplasia in thehuman prostate gland. An electron microscopic study. Virchows Arch A Pathol Anat Histol., 365(2):137-50;Quoted from Leav et al. (2001).
Kawamura, H., T. Nonogaki, K. Yoshikawa, M. Kimura and T. Nakano, 2002. Morphology of accessorysex organs from neonatally DES and DES-dp injected mouse. Okajimas Folia Anat Jpn., 78(6): 245-252.
Kohler-Samouilidis, G., N. Papaioannou, V.P. Kotsaki-Kovatsi and A. Vadarakis, 1998. Effect of estradiolvalerate on the male reproductive organs and various semen parameters in rats. Berl. Munch. Tierarztl.Wochenschr, 111(1): 1-5.
Li, S.C., G.F. Chen, P.S. Chan, H.L. Choi, S.M. Ho and F.L. Chan, 2001. Altered expression ofextracellular matrix and proteinases in Noble rat prostate gland after long term treatment with sex steroids.Prostate, 49(1): 58-71.
Lam, J.S., J.T. Leppert, S.N. Vemulapalli, O. Shvarts and A.S. Belldegrum, 2006. Secondary hormonaltherapy for advanced prostate cancer. J. Urol., 175(1): 27-34.
Lau, K.M., I Leav. and S.M. Ho, 1998. Rat estrogen receptor alpha and beta, and progesterone receptormRNA expression in various prostatic lobes and microdissected normal and dysplastic epithelial tissues of theNoble rats. Endocrinology, 139(1): 424-427.
Leav, I., K.M. Lau, J.Y. Adams, J.E. McNeal, M.E. Taplin, J. Wang, H. Singh and S.M. Ho, 2001.Comparative studies of the estrogen receptors β and α and the androgen receptor in normal human prostateglands, dysplasia, and in primary and metastatic carcinoma. Am. J. Pathol., 159(1): 79-92.
Lane, K.E., I. Leav, J. Ziar, R.S. Bridges, W.M. Rand and S.M. Ho, 1997. Suppression of testosteroneand estradiol-17beta induced dysplasia in the dorsolateral prostate of noble rats by bromocriptine.Carcinogenesis, 18: 1505-1510.
Merk, F.B., M.J. Warhol, P.W. Kwan, I. Leav, J. Alroy, P. Ofner, G.S. Pinkus, 1986. Multiple phenotypesof prostatic glandular cells in castrated dogs after individual or combined treatment with androgen and estrogen.Morphometric, ultrastructural and cytochemical distinctions. Lab. Invest., 54: 442-456.
Makela, S., L. Strauss, G. Kuiper, E. Valve, S. Salmi, R. Santti and J.A. Gustafsson, 2000. Differentialexpression of estrogen receptors α and β in adult rat accessory sex glands and lower urinary tract. Molecularand Cellular Molecular and Cellular Endocrinology, 164: 109-116.
Mobley, J.A., J.O.L. Esperance, M. Wu, C.J. Friel, R.H. Hanson and S.M. Ho, 2004. The novel estrogen17α-20Z-21-[(4-amino) phenyl]-19-norpregna-1, 3, 5(10), 20-tetraene-3, 17β-diol induces apoptosis in prostatecancer cell lines at nonmolar concentrations in vitro. Mol Cancer Ther., 3: 587-596.
Naslund, M.J., J.D. Strandberg and D.S. Coffey, 1988. The role of androgens and estrogens in thepathogenesis of experimental nonbacterial prostatitis. J. of Urology, 140: 1050-1053.
Niu, Y.J., T.X. Ma, J. Zhang, Y. Xu, R.F. Han and G. Sun, 2003. Androgen and prostatic stroma. AsianJ Androl. Mar., 5(1): 19-26.
Oh, W.K., P.W. Kantoff, V. Weinberg, G. Jones, B.I. Rini and M.K. Derynck, 2004. Prospective,multicenter, randomized phase II trial of the herbal supplement, PC-SPES, and diethylstilbestrol in patients withandrogen independent prostate cancer. J. Clin. Oncol., 22: 3705.
Oriowo, M.A., B.M Landgren, B. Stenstorm and E. Diczfalusy, 1980. A comparison of thepharmacokinetic properties of three estradiol esters. Contraception. Apr, 21(4): 415-424.
Prins, G.S., 1992. Neonatal estrogen exposure induces lobe specific alterations in adult rat prostateandrogen receptor expression. Endocrinology, 130: 3703-3714.
Pelletier, G., 2002. Effects of Estradiol on Prostate Epithelial Cells in the Castrated Rat. The Journal ofHistochemistry & Cytochemistry, 50(11): 1517-1523.
Prins, G.S., L. Brich, S.H. Ye and V. Ray, 1996. Estrogen exposure leads to prostate lobe specificdysplasia and adenomas in the aging rat. 21st Annual Meeting of the American society of andrology,Minneapolis MN, p: 52.
Putz, O., C.B. Schwartz, S. Kim, G.A. LeBlanc, R.L. Cooper and G.S. Prins, 2001. Neonatal Low andHigh Dose Exposure to Estradiol Benzoate in the Male Rat: Effects on the Prostate Gland. Biology ofReproduction, 65: 1496-1505.
Risbridger, G.P., H. Wang, M. Frydenberg and G. Cunha, 2001. The metaplastic effect of estrogen onmouse prostate epithelium: proliferation of cells with basal cell phenotype. Endocrinology, 142(6): 2443-2450.
72

Aust. J. Basic & Appl. Sci., 5(2): 59-73, 2011
Ricke, W.A., K. Ishii, E.A. Ricke, J. Simko, Y. Wang, S.W. Hayward and G.R. Cunha, 2006. Steroidhormones stimulate human prostate cancer progression and metastasis. Int J Cancer., 118(9): 2123-2131.
Scarano, W.R., R.S. Cordeiro, R.M. Goes, H.F. Carvalho and S.R. Taboga, 2005. Tissue remodeling inGuinea pig lateral prostate at different ages after estradiol treatment. Cell. Biol. Int., 29(9): 778-784.
Scarano, W.R., R.S. Cordeiro, R.M. Goes and S.R. Taboga, 2004. Intraepithelial alterations in the guineapig lateral prostate at different ages after estradiol treatment. J. Submicrosc. Cytol. Pathol., 36(2): 141-148.
Singh , J. and D.J. Handelsman, 1999. Morphometric studies of neonatal estrogen imprinting in the maturemouse prostate. J. Endocrinol., 162: 39-48.
Smith, D.C., B.G. Redman, L.E. Flaherty, L. Li, M. Strawderman and K.J.A. Pienta, 1998. phase II trialof oral diethylstilbesterol as a second line hormonal agent in advanced prostate cancer. Urology, 52: 257-260.
Taylor, R.A., P. Cowin, J.F. Couse, K.S. Korach and G.P. Risbridger, 2005. 17 β-Estradiol InducesApoptosis in the Developing Rodent Prostate Independently of ER-α or ER-β. Endocrinology, 147(1): 191-200.
Weihua, Z., M. Warner and J.A. Gustafsson, 2002. Estrogen receptor beta in the prostate. Molecular andCellular Endocrinology, 193: 1-5.
Yoshida, K., 1975. Ultrastructure of anterior lobe epithelium of the prostate of rat. Initial changes inepithelial cells following administration of estrogen. Nippon Hinyokika Gakkai Zasshi, 66(7): 383-399; Quotedfrom Scarano et al. (2004).
Yuen, M.T., L.K. Leung, J. Wang, Y.C. Wong and F.L. Chan, 2005. Enhanced induction of prostaticdysplasia and carcinoma in Noble rat model by combination of neonatal estrogen exposure and hormonaltreatments at adulthood. Int. J. Oncol., 27(6): 1685-1695.
73