
Effect of Air Bubbles in the Coupling Medium on Efficacy of Extracorporeal Shock Wave Lithotripsy
8
Stone Disease Effect of Air Bubbles in the Coupling Medium on Efficacy of Extracorporeal Shock Wave Lithotripsy Arun Jain *, Tariq K. Shah Department of Urology, Bradford Teaching Hospitals NHS Foundation Trust, Bradford Royal Infirmary, Bradford, United Kingdom european urology 51 (2007) 1680–1687 available at www.sciencedirect.com journal homepage: www.europeanurology.com Article info Article history: Accepted October 23, 2006 Published online ahead of print on November 10, 2006 Keywords: Air bubbles Coupling medium Lithotripsy ESWL Gel Ultrasound Abstract Objectives: Replacement of the water bath by a water cushion in newer lithotriptors introduces an acoustic interface and an ideal coupling agent is required to prevent energy loss at this interface. We aim to study the effect of bubbles in the coupling media on efficacy of extracorporeal shock wave lithotripsy (ESWL) by an in vitro experiment. Methods: Using a standardised in vitro model 40 artificial stones were randomly treated on Modulith SLK 1 lithotriptor using either conven- tional ultrasound gel (high bubble content) before and after displacing visible bubbles, a thin ultrasound gel (Therasonic TM ) or silicon oil (both with negligible bubbles). Percentage area covered by bubbles in each case and the diameters and depth of crater created in each stone were measured by two blinded observers to determine the correlation between the bubble contents and disintegration efficacy. In vivo effect of two ultrasound gels was compared in terms of pain scores and stone fragmentation rates in ten patients treated with both gels. Results: Volume of the craters was significantly greater with the Therasonic TM gel (102.4 Æ 33.4 mm 3 ) or silicon oil (98.8 Æ 9.8 mm 3 ) than the conventional ultrasound gel (49.2 Æ 32.6 mm 3 ). But it was greatest ( p < 0.001) with ultrasound gel without bubbles (163.5 Æ 22.6 mm 3 ). Depth and volume of the stone crater increased significantly with decreasing bubble contents of gel ( p < 0.001). Compared to standard ultrasound gel, patients treated with Therasonic TM gel reported signifi- cantly higher pain scores (median 3.5 vs. 8.0; p < 0.001). Conclusions: Efficacy of ESWL is significantly correlated to air bubbles within the coupling gel and can be improved significantly by eliminating the bubbles from the coupling medium. # 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved. * Corresponding author. Department of Urology, Bradford Teaching Hospitals NHS Founda- tion Trust, Bradford Royal Infirmary, Duckworth Lane, Bradford BD9 6RJ, United Kingdom. Tel. +44 1274 383116; Fax: +44 1274 383159. E-mail address: [email protected] (A. Jain). 0302-2838/$ – see back matter # 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2006.10.049
Transcript of Effect of Air Bubbles in the Coupling Medium on Efficacy of Extracorporeal Shock Wave Lithotripsy

e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 6 8 0 – 1 6 8 7
Stone Disease
Effect of Air Bubbles in the Coupling Medium on Efficacy ofExtracorporeal Shock Wave Lithotripsy
Arun Jain *, Tariq K. Shah
Department of Urology, Bradford Teaching Hospitals NHS Foundation Trust, Bradford Royal Infirmary, Bradford, United Kingdom
avai lable at www.sc iencedi rect .com
journal homepage: www.europeanurology.com
Article info
Article history:Accepted October 23, 2006Published online ahead ofprint on November 10, 2006
Keywords:Air bubblesCoupling mediumLithotripsyESWLGelUltrasound
Abstract
Objectives: Replacement of the water bath by a water cushion in newerlithotriptors introduces an acoustic interface and an ideal coupling agentis required to prevent energy loss at this interface. We aim to study theeffect of bubbles in the coupling media on efficacy of extracorporealshock wave lithotripsy (ESWL) by an in vitro experiment.Methods: Using a standardised in vitro model 40 artificial stones wererandomly treated on Modulith SLK1 lithotriptor using either conven-tional ultrasound gel (high bubble content) before and after displacingvisible bubbles, a thin ultrasound gel (TherasonicTM) or silicon oil (bothwith negligible bubbles). Percentage area covered by bubbles in each caseand the diameters and depth of crater created in each stone weremeasured by two blinded observers to determine the correlationbetween the bubble contents and disintegration efficacy. In vivo effectof two ultrasound gels was compared in terms of pain scores and stonefragmentation rates in ten patients treated with both gels.Results: Volume of the craters was significantly greater with theTherasonicTM gel (102.4 � 33.4 mm3) or silicon oil (98.8 � 9.8 mm3) thanthe conventional ultrasound gel (49.2 � 32.6 mm3). But it was greatest( p < 0.001) with ultrasound gel without bubbles (163.5 � 22.6 mm3).Depth and volume of the stone crater increased significantly withdecreasing bubble contents of gel ( p < 0.001). Compared to standardultrasound gel, patients treated with TherasonicTM gel reported signifi-cantly higher pain scores (median 3.5 vs. 8.0; p < 0.001).Conclusions: Efficacy of ESWL is significantly correlated to air bubbleswithin the coupling gel and can be improved significantly by eliminatingthe bubbles from the coupling medium.# 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. Department of Urology, Bradford Teaching Hospitals NHS Founda-tion Trust, Bradford Royal Infirmary, Duckworth Lane, Bradford BD9 6RJ, United Kingdom.Tel. +44 1274 383116; Fax: +44 1274 383159.E-mail address: [email protected] (A. Jain).
0302-2838/$ – see back matter # 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2006.10.049
e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 6 8 0 – 1 6 8 7 1681
1. Introduction
In spite of tremendous advances in the lithotriptortechnology over the last 25 years the first producedlithotriptor, unmodified Dornier HM3 device, con-tinues to be regarded as the gold standard [1].Essential principle of a lithotriptor is to generateshock waves and to deliver maximum possibleenergy at a remote focal point after transmissionthrough the body tissues. Transmission of the shockwaves across the delivery head to the skin results indistortion of these high frequency ultrasonic wavesas they cross different media. The original HM3lithotriptor [2] eliminated any energy absorbingacoustic interface by immersing both the sourceand the patient in a water bath. Replacement of thewater bath by a water-filled cushion in secondgeneration machines [3] was a major breakthroughin lithotriptor technology that revolutionised theergonomics of lithotriptor design. Unfortunately,inclusion of the water-filled cushion also created anacoustic interface in the path of shock waves and a
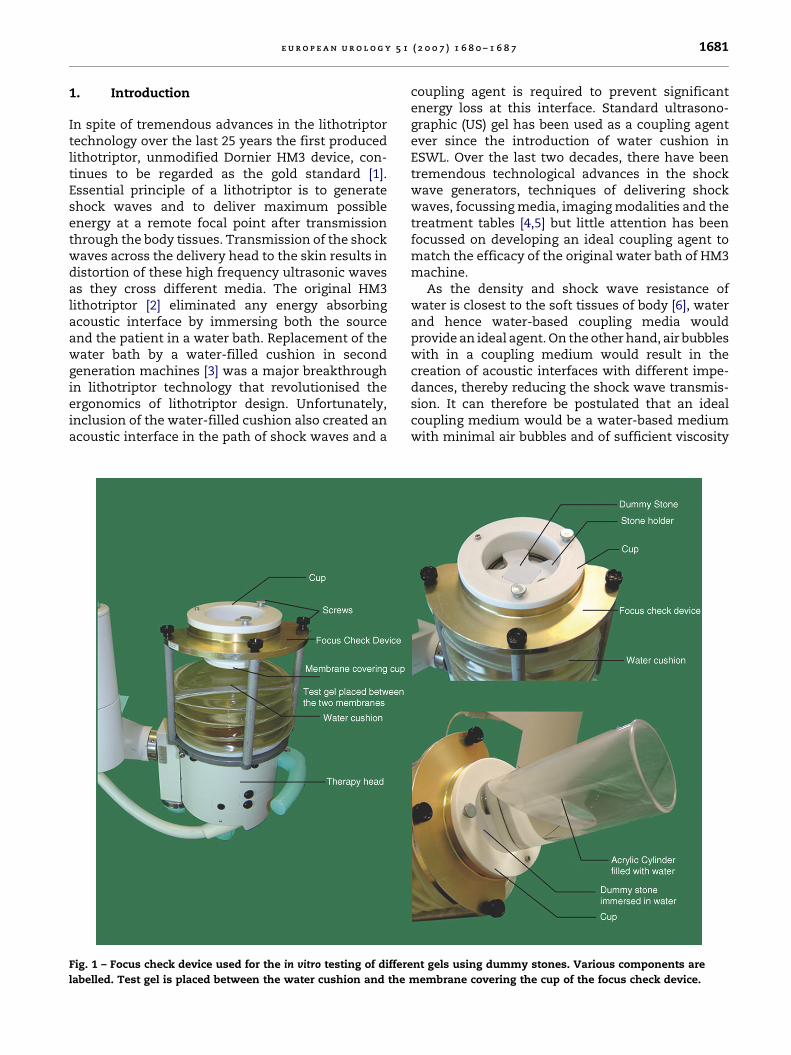
Fig. 1 – Focus check device used for the in vitro testing of differe
labelled. Test gel is placed between the water cushion and the
coupling agent is required to prevent significantenergy loss at this interface. Standard ultrasono-graphic (US) gel has been used as a coupling agentever since the introduction of water cushion inESWL. Over the last two decades, there have beentremendous technological advances in the shockwave generators, techniques of delivering shockwaves, focussing media, imaging modalities and thetreatment tables [4,5] but little attention has beenfocussed on developing an ideal coupling agent tomatch the efficacy of the original water bath of HM3machine.
As the density and shock wave resistance ofwater is closest to the soft tissues of body [6], waterand hence water-based coupling media wouldprovide an ideal agent. On the other hand, air bubbleswith in a coupling medium would result in thecreation of acoustic interfaces with different impe-dances, thereby reducing the shock wave transmis-sion. It can therefore be postulated that an idealcoupling medium would be a water-based mediumwith minimal air bubbles and of sufficient viscosity
nt gels using dummy stones. Various components are
membrane covering the cup of the focus check device.

Fig. 2 – Picture of the bubbles in the gel (actual size
28.4 � 21.3 inch) superimposed by a grid of one square
inch divisions to calculate the percentage area occupied by
the bubbles.
e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 6 8 0 – 1 6 8 71682
to stay in contact with the skin. We thereforecompared the efficacy of two different water-basedUS gels with different viscosities and differentpropensities to form air bubbles against siliconoil, an oil based relatively bubble-free medium,using an in vitro model. Effect of eliminating themacroscopically visible bubbles from the conven-tional US gel on the disintegration efficacy was alsostudied.
2. Methods
2.1. In vitro stone model
A total of 40 plaster of Paris dummy stones were randomly
divided into four groups and treated using a standardised
in vitro model using a stone test phantom (a modified focus
check device) on StorzTM Modulith SLK lithotriptor. Briefly the
method involved placement of the test stone at the focal point
of the lithotriptor after placing it in a stone holder (Fig. 1). Each
stone was soaked in water for ten minutes immediately before
treatment. The stone holder was inserted into a cup located in
the centre of a frame fixed to the therapy head of the
lithotriptor. A silicon membrane mounted on one side of the
cup separated the stone immersed in water from the water
cushion of the lithotriptor (Fig. 1). With the treatment head in
vertical position, 30 ml of test gel was placed on the water
cushion and the cushion was inflated to level 7.5 to couple
tightly with the silicon membrane mounted on the cup of the
test phantom device. The treatment head was then rotated
to lie at 458 angle to the horizontal. Each stone was treated
with 200 shock waves at a rate of 60 shocks/min and at a
power setting of 90 MPa using either conventional US gel (high
bubble content) before and after displacing visible bubbles, a
thin US gel (TherasonicTM Gel) or silicon oil (both with
negligible bubbles) in a random order. The two diameters
and depth of the crater created in each stone were measured
by two independent observers, blinded to the coupling
medium, using Vernier callipers. Each reading was taken in
duplicate and the mean value was used for calculation of the
crater volume by the formula 1/3 � p � r2 � h (formula for
measuring the cone volume), where r is the mean of the
two radii and h the depth of the crater.
2.2. Objective measurement of bubble contents in each gel
A high-resolution (3.1 megapixel) photograph of the layer of
coupling gel separating the water cushion of the lithotriptor
from the membrane mounted on the side of cup was taken
each time before placing the stone. A grid with one square inch
division was placed on each photograph (on-screen image
size: 28.4 � 21.3 inch) under standard conditions using
Adobe Photoshop version 7.0 software (Fig. 2). The number
of complete squares covered by the gel as well as the number
of squares covered with bubbles were counted in each of the
40 cases by two observers blinded to the type of gel used. Mean
values were recorded in each case. The degree of bubbles
formed in each case was calculated as the percentage of
squares covered by the bubbles.
2.3. In vivo study
The ESWL database maintained at our hospital for patients
treated between February 2004 and August 2005 was retro-
spectively analysed to identify all patients who required more
than one treatment for a given stone and were treated with
both TherasonicTM gel and conventional US gel at consecutive
treatment sessions. During the study period, either of the two
gels was used depending solely on the availability on a
particular day. All patients were offered 100 mg diclofenac
suppository or 1 g paracetamol plus 60 mg codein phosphate
orally (if diclofenac was contraindicated) approximately
30 minutes prior to treatment. Maximum pain during the
treatment was recorded on an analog scale (0–10) at the end of
each treatment. Stone fragmentation was assessed by
comparing the pre- and post-treatment plain X-ray. Effect of
the two different US gels was compared in vivo in terms of the
pain scores and stone fragmentation rates among these ten
paired-sets.
3. Results
Fig. 3 shows a representative image of the degree ofair bubbles formed within each of the four differentgels used. It is obvious that the conventional US gelforms the highest number of air bubbles whereasboth silicon oil and TherasonicTM gel formedminimal bubbles. Fig. 4 gives a representativepicture of the crater formed in the phantom stoneusing the four different gels. Mean values of the twodiameters, depth, and volume of the crater foreach of the four coupling agents used are given inTable 1. As shown in Fig. 5A the area occupied bythe bubbles (i.e. degree of bubbles) was significantlyhigher with the conventional US gel as compared to
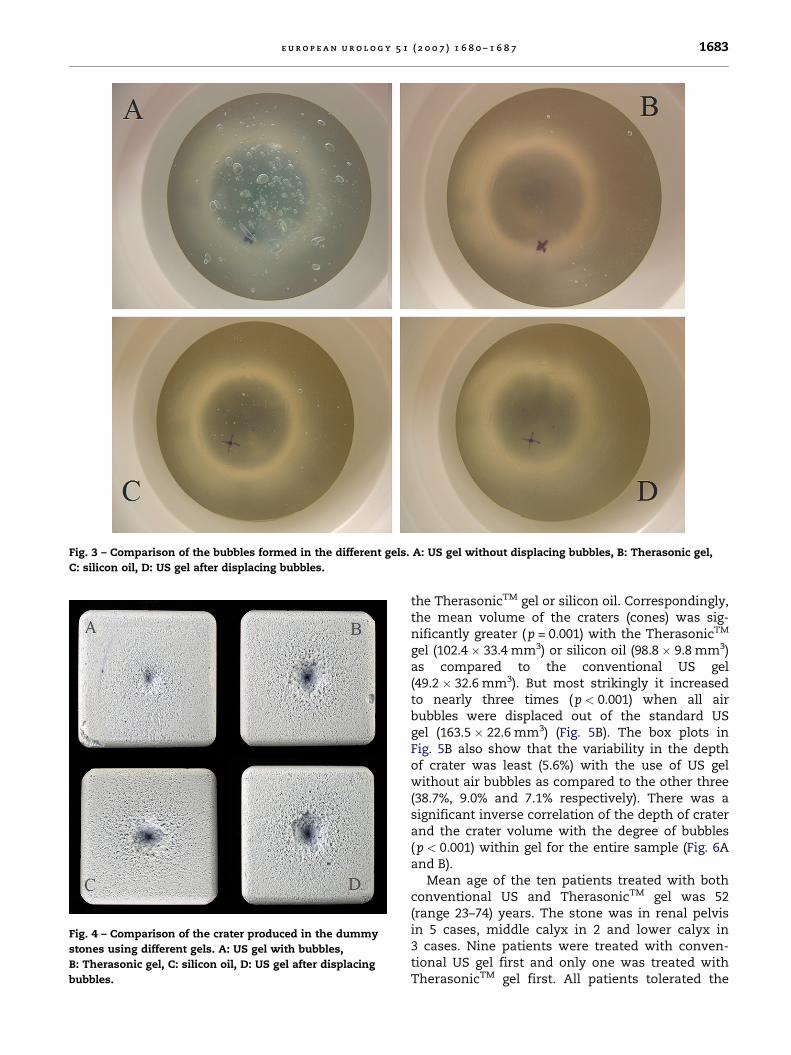
Fig. 3 – Comparison of the bubbles formed in the different gels. A: US gel without displacing bubbles, B: Therasonic gel,
C: silicon oil, D: US gel after displacing bubbles.
Fig. 4 – Comparison of the crater produced in the dummy
stones using different gels. A: US gel with bubbles,
B: Therasonic gel, C: silicon oil, D: US gel after displacing
bubbles.
e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 6 8 0 – 1 6 8 7 1683
the TherasonicTM gel or silicon oil. Correspondingly,the mean volume of the craters (cones) was sig-nificantly greater (p = 0.001) with the TherasonicTM
gel (102.4 � 33.4 mm3) or silicon oil (98.8 � 9.8 mm3)as compared to the conventional US gel(49.2 � 32.6 mm3). But most strikingly it increasedto nearly three times (p < 0.001) when all airbubbles were displaced out of the standard USgel (163.5 � 22.6 mm3) (Fig. 5B). The box plots inFig. 5B also show that the variability in the depthof crater was least (5.6%) with the use of US gelwithout air bubbles as compared to the other three(38.7%, 9.0% and 7.1% respectively). There was asignificant inverse correlation of the depth of craterand the crater volume with the degree of bubbles(p < 0.001) within gel for the entire sample (Fig. 6Aand B).
Mean age of the ten patients treated with bothconventional US and TherasonicTM gel was 52(range 23–74) years. The stone was in renal pelvisin 5 cases, middle calyx in 2 and lower calyx in3 cases. Nine patients were treated with conven-tional US gel first and only one was treated withTherasonicTM gel first. All patients tolerated the
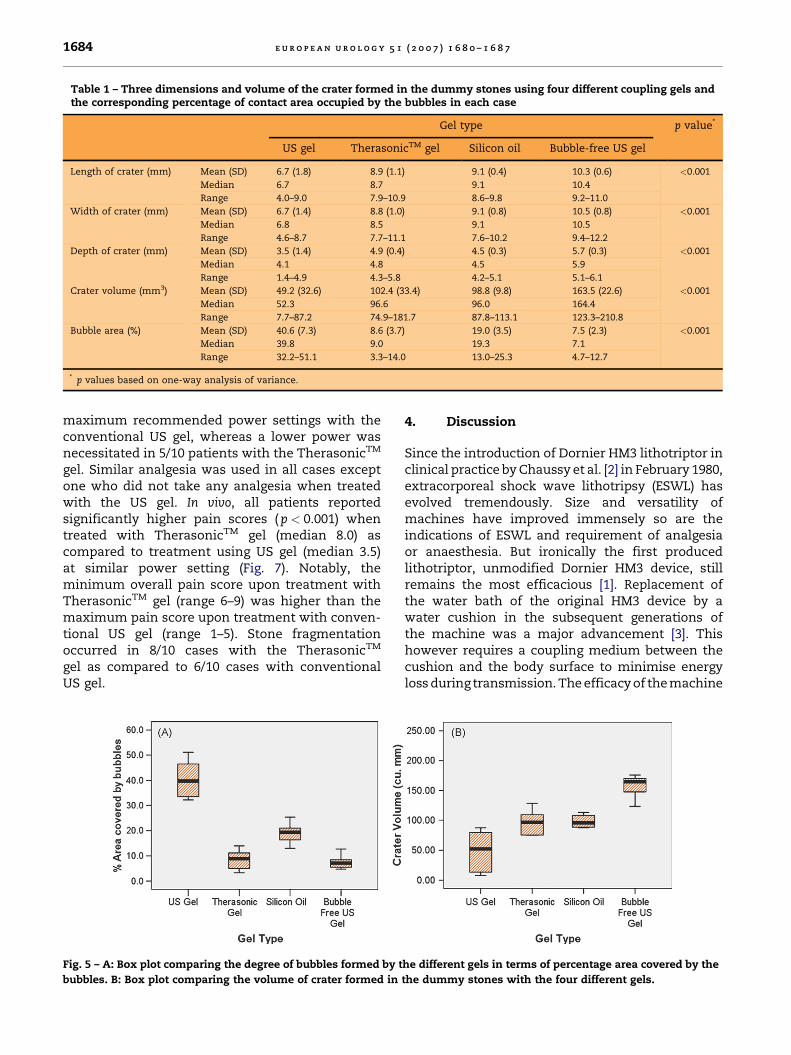
Table 1 – Three dimensions and volume of the crater formed in the dummy stones using four different coupling gels andthe corresponding percentage of contact area occupied by the bubbles in each case
Gel type p value*
US gel TherasonicTM gel Silicon oil Bubble-free US gel
Length of crater (mm) Mean (SD) 6.7 (1.8) 8.9 (1.1) 9.1 (0.4) 10.3 (0.6) <0.001
Median 6.7 8.7 9.1 10.4
Range 4.0–9.0 7.9–10.9 8.6–9.8 9.2–11.0
Width of crater (mm) Mean (SD) 6.7 (1.4) 8.8 (1.0) 9.1 (0.8) 10.5 (0.8) <0.001
Median 6.8 8.5 9.1 10.5
Range 4.6–8.7 7.7–11.1 7.6–10.2 9.4–12.2
Depth of crater (mm) Mean (SD) 3.5 (1.4) 4.9 (0.4) 4.5 (0.3) 5.7 (0.3) <0.001
Median 4.1 4.8 4.5 5.9
Range 1.4–4.9 4.3–5.8 4.2–5.1 5.1–6.1
Crater volume (mm3) Mean (SD) 49.2 (32.6) 102.4 (33.4) 98.8 (9.8) 163.5 (22.6) <0.001
Median 52.3 96.6 96.0 164.4
Range 7.7–87.2 74.9–181.7 87.8–113.1 123.3–210.8
Bubble area (%) Mean (SD) 40.6 (7.3) 8.6 (3.7) 19.0 (3.5) 7.5 (2.3) <0.001
Median 39.8 9.0 19.3 7.1
Range 32.2–51.1 3.3–14.0 13.0–25.3 4.7–12.7
* p values based on one-way analysis of variance.
e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 6 8 0 – 1 6 8 71684
maximum recommended power settings with theconventional US gel, whereas a lower power wasnecessitated in 5/10 patients with the TherasonicTM
gel. Similar analgesia was used in all cases exceptone who did not take any analgesia when treatedwith the US gel. In vivo, all patients reportedsignificantly higher pain scores ( p < 0.001) whentreated with TherasonicTM gel (median 8.0) ascompared to treatment using US gel (median 3.5)at similar power setting (Fig. 7). Notably, theminimum overall pain score upon treatment withTherasonicTM gel (range 6–9) was higher than themaximum pain score upon treatment with conven-tional US gel (range 1–5). Stone fragmentationoccurred in 8/10 cases with the TherasonicTM
gel as compared to 6/10 cases with conventionalUS gel.
Fig. 5 – A: Box plot comparing the degree of bubbles formed by t
bubbles. B: Box plot comparing the volume of crater formed in
4. Discussion
Since the introduction of Dornier HM3 lithotriptor inclinical practice by Chaussy et al. [2] in February 1980,extracorporeal shock wave lithotripsy (ESWL) hasevolved tremendously. Size and versatility ofmachines have improved immensely so are theindications of ESWL and requirement of analgesiaor anaesthesia. But ironically the first producedlithotriptor, unmodified Dornier HM3 device, stillremains the most efficacious [1]. Replacement ofthe water bath of the original HM3 device by awater cushion in the subsequent generations ofthe machine was a major advancement [3]. Thishowever requires a coupling medium between thecushion and the body surface to minimise energyloss during transmission. The efficacy of the machine
he different gels in terms of percentage area covered by the
the dummy stones with the four different gels.

Fig. 6 – Correlation of the percentage area covered by the bubbles with the deapth of crater (A) and crater volume (B) for the
entire cohort (N = 40).
e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 6 8 0 – 1 6 8 7 1685
therefore varies depending on the effectiveness ofthis medium. To our knowledge there are nopublished studies objectively analysing the role ofbubbles in a contact medium on the efficacy of ESWL.
In an in vitro model using ten artificial stones ineach arm, we found that the silicon oil andTherasonicTM gel (both with minimal bubble con-tents) were significantly more efficacious thanstandard US gel (with high bubble contents). Butthe best results were achieved when all air bubblesvisible to the naked eye, were excluded from thestandard US gel. The efficacy of ESWL (in terms ofcrater volume) increased significantly with thedecreased bubble contents of the gel in the entirecohort. Although the higher fragmentation ratefollowing treatment with TherasonicTM gel observedin our analysis was likely to be biased as most cases
Fig. 7 – Box plot comparing pain scores reported by the
patients during ESWL with two different ultrasound gels.
Therasonic gelTM (minimal bubbles), US gel (high bubble
content).
were treated with the conventional US gel first, astriking difference in the pain scores with the twogels was clearly evident as each patient served ashis/her own control. The use of TherasonicTM gel,which was more efficacious than the conventionalUS gel in vitro, resulted in significantly higher painin vivo. It can, therefore, be hypothesised thatbubbles in the gel result in dissipation of the energywithin the gel due to cavitation effect. The contactmedia with a higher bubble contents (like theconventional US gel in our study) consequently leadto overall decreased energy transmission to the skinas well as deeper tissues and hence cause less painduring treatment. The variation in the bubblecontents of the gel may also explain the widevariation in the analgesia requirement observed byvarious authors using similar lithotriptors in thepast [7,8]. Conclusions drawn from our in vivo studyare limited by its retrospective nature and smallnumber and warrant further validation in a pro-spective randomised crossover study. Our hypoth-esis is, however, supported by the essentialrequirement of general or regional anaesthesia withthe HM3 device [9] that uses a water bath wherethere is no energy dissipation on the skin surface,yet the treatment is more painful. Cartledge et al.[10] also found that petroleum jelly was 2.3 timesless efficacious in stone disintegration using an invitro model suggesting that the decreased pain withthe use of petroleum jelly noted in previous studies[7,8] could be due to decreased transmission ofshock wave energy to the body tissues presumablydue to higher density or viscosity of the oil basedmedia. In an in vitro study HM3 lithotriptor was notimpressively different from the newer lithotriptors[11] but in vivo HM3 has proved more efficient thanthe newer generation lithotriptor [9] suggesting thatreplacement of the water bath by a coupling agent in

e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 6 8 0 – 1 6 8 71686
the newer lithotriptors may result in significant lossof energy transmitted to the focus area in vivo.Similarly, Chan et al. [12] noted that the stone-freerate in the lower pole stones was significantlybetter with the modified HM3 as compared to theMFL 5000 lithotriptor. As the two devices use thesame ellipsoid and shock wave generator but differmainly in the replacement of the water bath in HM3by a water cushion in MFL 5000, it can be inferredthat water bath provides the ideal mechanism fortransmitting shock wave energy into the body andcan be best replaced by a water based bubble-freecontact medium.
5. Conclusions
Based on an in vitro stone model, our resultsconclusively show that the bubbles in the contactmedium significantly reduce the efficacy of ESWLand by carefully eliminating all the visible bubblesfrom the conventionally used ultrasonographic gelduring ESWL, the treatment efficacy can beimproved by up to three times. We also describe anovel method to objectively estimate the degree ofbubbles formed within a contact medium in in vitroexperiments. The variable results with the samecontact medium in the previous studies may also beattributed to the differences in the bubbles contentof the test media. Our results show that a water-based jelly free of bubbles would provide an idealcoupling agent and emphasise the need for furtherresearch to develop an ideal coupling medium inorder to bring the efficiency of the modern litho-triptors closer the gold standard HM3 lithotriptor.
Conflicts of interest
The authors have nothing to disclose.
Acknowledgements
We thank Storz Medical Inc. for providing dummystones and the stone test phantom device for thisstudy. We also acknowledge the help extended by
Editorial CommentFrancis Xavier Keeley Jr., Bristol Urological Institute,Bristol, England
Extracorporeal shock wave lithotripsy (ESWL)is fast becoming an orphan procedure that is often
Michael Newsome and Alan Wagstaff in measuringdimensions of the stone craters.
Sources of funding: Storz Medical Inc. provideddummy stones and the stone test phantom devicefor this study.
References
[1] Lingeman JE, Lifshitz DA, Evan AP. Surgical Management of
Urinary Lithiasis. In: Retik A, Vaughan E, Wein A, editors.
Campbell’s Urology; ed 8th. Philadelphia: Saunders; 2002,
vol 4. p. 3361–451.
[2] Chaussy C, Brendel W, Schmiedt E. Extracorporeally
induced destruction of kidney stones by shock waves.
Lancet 1980;2:1265–8.
[3] Clayman RV, McClennan MD, Garvin TJ, Denstedt JD,
Andriole GL. Lithostar: an electromagnetic acoustic shock
wave unit for extracorporeal lithotripsy. J Endourol
1989;3:307–13.
[4] Skolarikos A, Alivizatos G, de la Rosette J. Extracorporeal
shock wave lithotripsy 25 years later: complications and
their prevention. Eur Urol 2006;50:981–90.
[5] Jain A, Shah TK. Extracorporeal shock wave lithotripsy:
principles and evolution. Urology News 2005;10:7–11.
[6] Eisenberger F, Miller K, Rassweiler J, editors. Stone
Therapy in Urology. New York: Thieme; 1991.
[7] Heidenreich A, Bonfig R, Wilbert DM, Engelmann UH.
Painless ESWL by cutaneous application of vaseline.
Scand J Urol Nephrol 1995;29:155–60.
[8] Becker AJ, Stief CG, Truss MC, Oelke M, Machtens S, Jonas
U. Petroleum jelly is an ideal contact medium for pain
reduction and successful treatment with extracorporeal
shock wave lithotripsy. J Urol 1999;162:18–22.
[9] Graber SF, Danuser H, Hochreiter WW, Studer UE. A pro-
spective randomized trial comparing 2 lithotriptors for
stone disintegration and induced renal trauma. J Urol
2003;169:54–7.
[10] Cartledge JJ, Cross WR, Lloyd SN, Joyce AD. The efficacy
of a range of contact media as coupling agents in
extracorporeal shockwave lithotripsy. BJU Int 2001;88:
321–4.
[11] Teichman JM, Portis AJ, Cecconi PP, Bub WL, Endicott RC,
Denes B, et al. In vitro comparison of shock wave litho-
tripsy machines. J Urol 2000;164:1259–64.
[12] Chan SL, Stothers L, Rowley A, Perler Z, Taylor W, Sullivan
LD. A prospective trial comparing the efficacy and compli-
cations of the modified Dornier HM3 and MFL 5000 litho-
triptors for solitary renal calculi. J Urol 1995;153:
1794–7.
consigned to junior or nonmedical staff. Whatwas once new has become unexciting. With thelack of excitement comes the danger of neglect.
Lithotripsy is unique in being a medical technol-ogy that appears to have worsening outcomes overtime. What has changed since the Dornier HM-3

once ruled the stone kingdom? The shock wavegenerator in the HM-3 was quite crude, the machinewas bulky, and the imaging was rudimentary. Yetmore modern imaging, sleeker design, and sophis-ticated generators have not resulted in better out-comes. Could it be something as basic as thecoupling medium?
In this study, Jain and Shah clearly show thatthe coupling medium makes a considerable
difference in vitro. Their preliminary clinicalresults are also intriguing. Can the ultrasound jellyactually make much of a difference? Only a prop-erly conducted prospective, randomised study cananswer that question. In the meantime, perhapswe should all take a closer look at the media we usefor ESWL. It may be well worth paying closerattention to the small details that can make abig difference.
e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 6 8 0 – 1 6 8 7 1687


















