EFFECT OF ADDING DEXMED ETOMIDINE vs FENTANYL TO ...
120
1 EFFECT OF ADDING DEXMEDETOMIDINE vs FENTANYL TO INTRATHECAL BUPIVACAINE ON SPINAL BLOCK CHARACTERISTICS IN GYNECOLOGICAL PROCEDURES: DOUBLE BLINDED CONTROL STUDY Dissertation submitted to THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY in partial fulfillment for the award of the degree of DOCTOR OF MEDICINE IN ANAESTHESIOLOGY BRANCH X INSTITUTE OF ANAESTHESIOLOGY & CRITICAL CARE MADRAS MEDICAL COLLEGE CHENNAI – 600 003. APRIL 2017
Transcript of EFFECT OF ADDING DEXMED ETOMIDINE vs FENTANYL TO ...

1
EFFECT OF ADDING DEXMEDETOMIDINE vs FENTANYL TO
INTRATHECAL BUPIVACAINE ON SPINAL BLOCK
CHARACTERISTICS IN GYNECOLOGICAL PROCEDURES:
DOUBLE BLINDED CONTROL STUDY
Dissertation submitted to
THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY
in partial fulfillment for the award of the degree of
DOCTOR OF MEDICINE
IN ANAESTHESIOLOGY
BRANCH X
INSTITUTE OF ANAESTHESIOLOGY & CRITICAL CARE
MADRAS MEDICAL COLLEGE
CHENNAI – 600 003.
APRIL 2017
252268
Text Box
CERTIFICATE OF GUIDE
This is to certify that the dissertation entitled, “EFFECT OF ADDING
DEXMEDETOMIDINE vs FENTANYL TO INTRATHECAL
BUPIVACAINE ON SPINAL BLOCK CHARACTERISTICS IN
GYNECOLOGICAL PROCEDURES: DOUBLE BLINDED
CONTROL STUDY” Submitted by Dr. Sivashankari K in partial fulfillment
for the award of the degree of Doctor of Medicine in Anaesthesiology by the
Tamilnadu Dr. M.G.R. Medical University, Chennai is bonafide record of the
work done by her in the INSTITUTE OF ANAESTHESIOLOGY & CRITICAL
CARE, Madras Medical College, during the academic year 2014-2017.
Date:
Place : Chennai
PROF. DR. B.CHANDRIKA,M.D., D.A. PROFESSOR
DEPARTMENT OF ANAESTHESIOLOGY,
INSTITUTE OF OBSTETRICS AND
GYNAECOLOGY,EGMORE,
CHENNAI – 600 005

CERTIFICATE
This is to certify that the dissertation entitled, “EFFECT OF ADDING
DEXMEDETOMIDINE vs FENTANYL TO INTRATHECAL
BUPIVACAINE ON SPINAL BLOCK CHARACTERISTICS IN
GYNECOLOGICAL PROCEDURES: DOUBLE BLINDED
CONTROL STUDY” Submitted by Dr. Sivashankari K in partial
fulfillment for the award of the degree of Doctor of Medicine in
Anaesthesiology by the Tamilnadu Dr. M.G.R. Medical University, Chennai
is bonafide record of the work done by her in the INSTITUTE OF
ANAESTHESIOLOGY & CRITICAL CARE, Madras Medical College,
during the academic year 2014-2017.
PROF DR. B.KALA,M.D;D.A THE DIRECTOR,
INSTITUTE OF ANAESTHESIOLOGY & CRITICAL CARE
MADRAS MEDICAL COLLEGE CHENNAI – 600 003.
DR.M.K. MURALITHARAN M.S, MCH DEAN,
MADRAS MEDICAL COLLEGE &
GOVT. GENERAL HOSPITAL,
CHENNAI – 600 003.
3
DECLARATION
I, Dr. K.Sivashankari, solemnly declare that the dissertation “EFFECT OF
ADDING DEXMEDETOMIDINE vs FENTANYL TO INTRATHECAL
BUPIVACAINE ON SPINAL BLOCK CHARACTERISTICS IN
GYNECOLOGICAL PROCEDURES: DOUBLE BLINDED CONTROL
STUDY” is a bonafide work done by me in the Institute of Anaesthesiology and
Critical Care , Madras Medical College, Chennai, after getting approval from the
Ethical Committee, under the able guidance of Prof.Dr. B.Chandrika, MD.DA,
The Institute of Obstetrics and Gynaecology, Egmore, Chennai. This study was
conducted in Institute of Obstetrics and Gynaecology, Chennai, in partial fulfillment
of the regulations for the award of the degree of M.D (Anaesthesiology),
examination to be held in April 2017.
I have not submitted this dissertation previously to any journal or any university for
the award of any degree or diploma.
DATE : PLACE : CHENNAI DR.K.SIVASHANKARI
252268
Text Box
4
ACKNOWLEDGEMENT
On completion of my dissertation I would like to acknowledge all those
who have made this possible.
I am extremely thankful to Dr. M.K.MURALITHARAN MS, MCH
Dean, MADRAS MEDICAL COLLEGE, for his kind permission to carry out this
study.
I am immensely grateful to PROF. D R . B.KALA, M.D, D.A, Director &
Professor, INSTITUTE OF ANAESTHESIOLOGY & CRITICAL CARE, for her
concern and support in conducting this study.
I am extremely grateful and indebted to my guide PROF. Dr.
B.CHANDRIKA M.D, D.A, Professor of Anaesthesiology, INSTITUTE OF
OBSTETRICS AND GYNAECOLOGY, for her concern, inspiration, meticulous
guidance, expert advice and constant encouragement in preparing this dissertation.
I am extremely thankful to my co-guide Dr. SRIDHAR, M.D, D.A,
Assistant Professor of Anaesthesiology, INSTITUTE OF OBSTETRICS AND
GYNAECOLOGY for his constant support and help in my dissertation work.
I am very much indebted to all my assistant Professors, Department of
Anaesthesiology, Institute of Obstetrics and Gynaecology, Chennai, for their
inspiration, invaluable guidance and supervision at all stages of this study.
I would like to express my thanks to the staff members of the Institute of
Obstetrics and Gynaecology, Chennai, for their ever willing help and cooperation
during the course of this study.
I would like to thank all my colleagues and friends for their whole
252268
Text Box
5
hearted help and advice in carrying out this study.
I am grateful to my family and friends for their moral support and
encouragement.
Last but not the least, I am extremely grateful to all my patients who in
spite of all their sufferings have lent themselves to be a very valuable part of this
study and have helped me to improve my knowledge and complete this
dissertation.
Above all I pay my gratitude to the ALMIGHTY for giving me strength to
complete my work.
252268
Text Box
6
TABLE OF CONTENTS 1.0 INTRODUCTION......................................................................................................................... 1
2.0 AIM OF THE STUDY .................................................................................................................... 2
3.0 SPINAL ANAESTHESIA ................................................................................................................ 3
3.1 ANATOMY ............................................................................................................................. 3
3.2 PHYSIOLOGY OF SUBARACHNOID BLOCK .............................................................................. 5
3.2.1 CEREBROSPINAL FLUID ................................................................................................... 5
3.2.2 MECHANISM OF SPINAL ANAESTHESIA .......................................................................... 6
3.2.3 SPREAD OF LA IN THE SUBARACHNOID SPACE ............................................................... 6
3.2.4 FATE OF LOCAL ANAESTHETICS IN SUBARACHNOID SPACE ........................................... 7
3.2.5 INDICATIONS FOR SUBARACHNOID BLOCK ................................................................... 9
3.2.6 CONTRAINDICATIONS FOR SUBARACHNOID BLOCK ..................................................... 9
4.0 SPINAL ANAESTHESIA — TECHNIQUE ..................................................................................... 10
4.1 PROCEDURE ........................................................................................................................ 10
4.1.1 PREPARATION .............................................................................................................. 10
4.1.2 POSITION ..................................................................................................................... 11
4.1.3 PUNCTURE ................................................................................................................... 11
4. 2 COMPLICATIONS OF SUBRACHNOID BLOCK ....................................................................... 14
5.0 PHARMACOLOGY OF BUPIVACAINE ........................................................................................ 15
5.1 MECHANISM OF ACTION ..................................................................................................... 16
5.2 PHARMACODYNAMICS ....................................................................................................... 16
5.3 PHARMACOKINETICS .......................................................................................................... 16
5.4 METABOLISM ...................................................................................................................... 17
6.0 PHARMACOLOGY OF DEXMEDETOMIDINE ............................................................................. 20
6.1 PHARMACOKINETICS: ......................................................................................................... 21
6.2 ACTIONS: ............................................................................................................................. 22
6.2.1 EFFECTS ON THE CENTRAL NERVOUS SYSTEM: ............................................................ 22
6.2.2 EFFECTS ON THE RESPIRATORY SYSTEM: .................................................................... 23
6.2.3 EFFECTS ON THE CARDIOVASCULAR SYSTEM: ............................................................. 23
6.2.4 DOSAGE AND ADMINISTRATION: ................................................................................ 24
6.2.5 USES: ............................................................................................................................ 24
7.0 FENTANYL PHARMACOLOGY .................................................................................................. 26
7.1 FENTANYL ........................................................................................................................... 26
7.2 PHARMACOKINETICS .......................................................................................................... 29
7.3 FACTORS THAT ALTER PHARMACOKINETICS AND PHARMACODYNAMICS ......................... 30

7
8.0 REVIEW OF LITERATURE .......................................................................................................... 31
9.0 MATERIALS AND METHODS .................................................................................................... 40
9.1 SELECTION OF CASES: ......................................................................................................... 41
9.2 PRE ANAESTHETIC EVALUATION ......................................................................................... 42
9.3 OBSERVATION AND RESULTS .............................................................................................. 47
10.0 STATISTICS ............................................................................................................................ 48
10.1 DISCUSSION ...................................................................................................................... 66
10.2 SUMMARY......................................................................................................................... 74
10.3 CONCLUSION .................................................................................................................... 75
11.0 BIBLIOGRAPHY ...................................................................................................................... 76
Annexure: 1. Ethical Committee 2. Anti‐Plagiarism Screen shot 3. Patient Information Form 4. Patient Concern Form 5. Performa 6. Master Chart
252268
Text Box

1
1.0 INTRODUCTION
Neuraxial blockade notably spinal Anaesthesia is used extensively for lower
abdominal and lower extremity surgeries, because it has several advantages over
general Anaesthesia. Lignocaine and Bupivacaine are the commonly used local
anesthetic agents for spinal anesthesia. The adjuvants like opioids and α2 agonist
are sometimes combined with Local anaesthetic for spinal anaesthesia. The rationale
for combining adjuvants to local anaesthetic drugs is to lower the dose of each
agent, and maintaining analgesic efficacy whilst reducing the incidence and
severity of side effects.
Surgery on the uterus and other genital organs performed under spinal or epidural
block is often accompanied by visceral pain, nausea and vomiting. Fentanyl in
various doses when added to spinal Bupivacaine increase the duration of analgesia.
Dexmedetomidine is a α2-agonist that is approved as an intravenous sedative and co-
analgesic drug.
The study was designed to evaluate the efficacy and adverse effects of 5μg
Dexmedetomidine versus 25μg of Fentanyl when added to 0.5% Hyperbaric
Bupivacaine administered intrathecally in patients undergoing elective abdominal
hysterectomy surgeries.

2
2.0 AIM OF THE STUDY
To compare the effect of adding Dexmedetomidine versus Fentanyl to 0.5%
Hyperbaric Bupivacaine administered intrathecally for abdominal hysterectomy
surgeries.
To evaluate the onset and duration of sensory and motor block.
To assess intra operative haemodynamics
To monitor postoperative analgesia.
Complications

3
3.0 SPINAL ANAESTHESIA
Spinal (subarachnoid/ intrathecal) anaesthesia is a form of central neuraxial
block in which temporary interruption of nerve transmission is achieved by
injection of local anaesthetic and / or adjuvant solutions into the subarachnoid space.
Spinal anaesthesia is one of the most frequently employed methods of regional
anaesthesia.
3.1 ANATOMY
The Vertebral canal extends from the foramen magnum to the sacral hiatus.
It is formed by the dorsal spine, pedicles and laminae of successive vertebrae
(7cervical, 12 thoracic, 5 lumbar, and 5 sacral). The vertebrae are held together by a
series of the anterior and posterior longitudinal ligaments, ligamentum flavum,
interspinous ligament, supraspinous ligament and the intervertebral discs.
The spinal cord, a direct continuation of the medulla oblongata begins at the
upper border of the atlas and terminates distally in the conus medullaris. The distal
termination, because of the differential growth rates between the bony vertebral
canal and central nervous system varies from L3 in the infant, to the lower border of L1
in the adult.
Surrounding the spinal cord in the bony vertebral column are three membranes-
(from inside to outside); the pia mater, arachnoid mater and dura mater. The pia
mater is a highly vascular membrane that closely invests the spinal cord. The
arachnoid mater is a delicate non vascular membrane closely attached to the outer
most duramater.
4
Between the two innermost membranes is the subarachnoid space. In this space
cerebrospinal fluid (CSF), spinal nerves, blood vessels that supply the spinal cord
and dentate ligaments are present. Although the spinal cord ends at the lower border
of L1 in adults, the subarachnoid space continues to S2 level. The outermost
membrane in the spinal cord is the longitudinally organized fibroelastic membrane,
the duramater. This layer is the direct extension of the cranial dura mater and extend
as the spinal duramater from the foramen magnum to S2, where the filum terminale
(as extension of the pia mater beginning at conus medullaris) blends with the
periosteum of the subdural space which contains only small amounts of serous fluid to
allow the dura and arachnoid move over each other. Surrounding the dura mater is
the epidural or extradural space which extends from the foramen magnum to the sacral
hiatus. Posterior to the epidural space is the ligamentum flavum. Immediately
posterior to the ligmentum flavum is the interspinous ligament. Extending from
the external occipital protuberance to the Coccyx, posterior to this structure is the
supraspinous ligament.
Lumbar puncture is routinely done below the L2 vertebrae down to the L5-S1
interspace to avoid damage to the spinal cord which ends at the lower border of L1
vertebrae in adults.

5
3.2 PHYSIOLOGY OF SUBARACHNOID BLOCK 3.2.1 CEREBROSPINAL FLUID
The cerebrospinal fluid (CSF) is an ultrafiltrate of plasma. It is a clear, colourless
fluid found in the spinal and cranial subarachnoid space and in the ventricles of the
brain. The average volume in the adults ranges from 120 to 150 ml of which 35 ml in
the ventricles, 25 ml is in the cerebral subarachnoid space and 75 ml is in the spinal
subarachnoid space. It is secreted by the choroidal plexus at a rate of 0.3-0.4
ml/minute.
Physical characteristics of cerebrospinal fluid
PH 7.4
Specific gravity referred to Water
At body temperature 1.007
At 4 deg C 1.0003
Density 1.0003 g/ml
Baricity 1.000
Pressure 8-12 mm Hg / 70-80 cm H2O
Cells 3-5 /cu.mm
Proteins 20mg/dl
Glucose 45-80 mg/dl
6
The CSF plays an important role in spinal anesthesia. It acts as a media for
dispersion of the local anaesthetic drug to the spinal nerve. An important factor
determining the spread of drugs in the subarachnoid space is the specific gravity of
the injected solution compared with that of CSF.
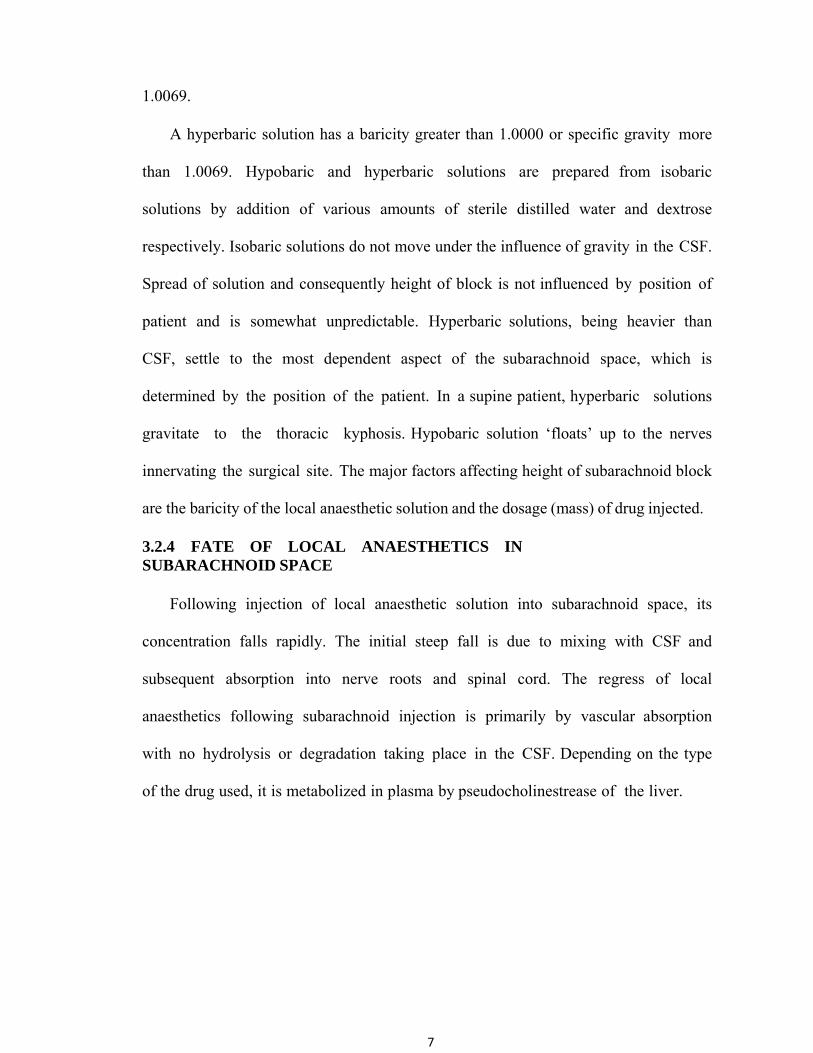
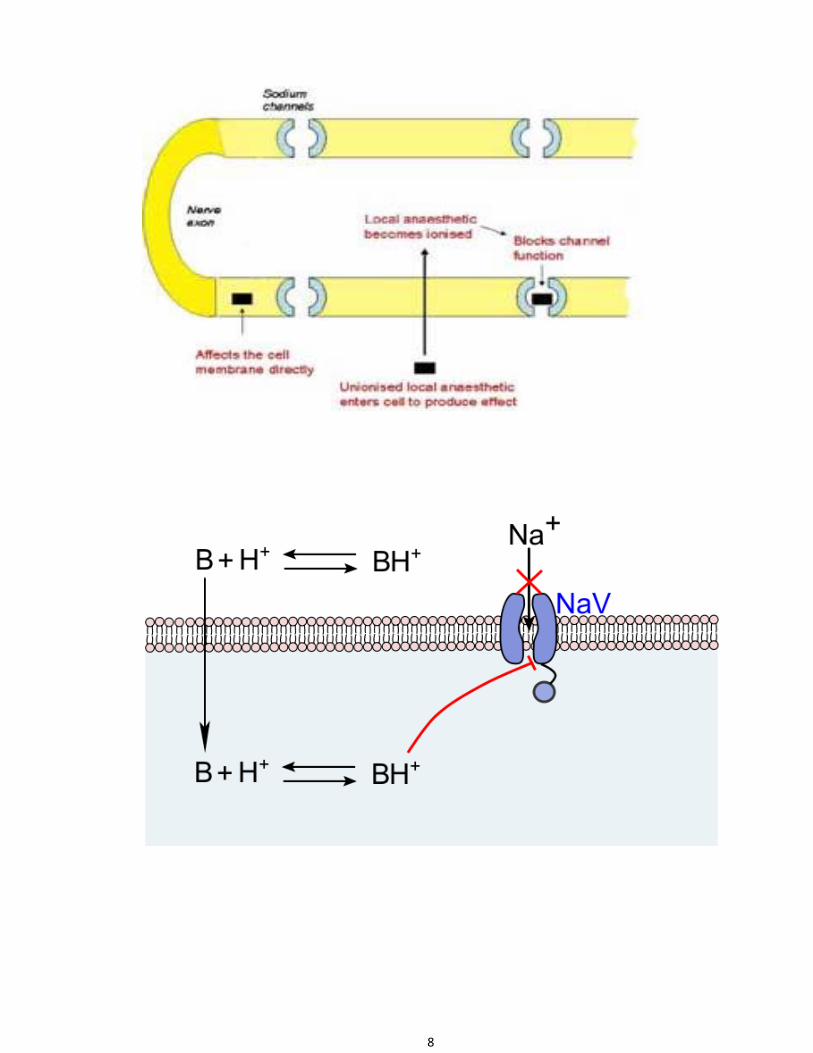
3.2.2 MECHANISM OF SPINAL ANAESTHESIA Injection of local anaesthetics into the spinal CSF allows access to sites of action
both within the spinal cord and the peripheral nerve roots. The nerve roots leaving
the spinal canal are not covered by epineurium and are readily exposed to the local
anaesthetic within the CSF. Therefore afferent impulses leaving via the ventral nerve
roots are blocked during spinal anaesthesia. Spinal local anaesthetics block sodium
channels and electrical conduction in spinal nerve roots. There are also multiple
potential action of local anaesthetics within the spinal cord at different sites. Local
anaesthetics can exert sodium channel block within the dorsal and ventral horns,
inhibiting generation and propagation of electrical activity The order in which nerve
fibers are blocked in spinal anaesthesia is preganglionic sympathetic B fibers
followed by temperature fibers (cold before warmth), fibers carrying pin prick
sensation, touch, deep pressure, and proprioceptive impulses. Recovery usually occurs
in the reverse order.
3.2.3 SPREAD OF LA IN THE SUBARACHNOID SPACE The local anaesthestic solution is diluted in the CSF and therefore its resultant
concentration is less potent than the actual solution . Spread is also determined by
the baricity of the injected solution. Baricity is a ratio comparing the density of
LA solution at a specified temperature to the density of CSF at the same temperature.
A hypobaric solution has a baricity less than 1.0000 or specific gravity less than
7
1.0069.
A hyperbaric solution has a baricity greater than 1.0000 or specific gravity more
than 1.0069. Hypobaric and hyperbaric solutions are prepared from isobaric
solutions by addition of various amounts of sterile distilled water and dextrose
respectively. Isobaric solutions do not move under the influence of gravity in the CSF.
Spread of solution and consequently height of block is not influenced by position of
patient and is somewhat unpredictable. Hyperbaric solutions, being heavier than
CSF, settle to the most dependent aspect of the subarachnoid space, which is
determined by the position of the patient. In a supine patient, hyperbaric solutions
gravitate to the thoracic kyphosis. Hypobaric solution ‘floats’ up to the nerves
innervating the surgical site. The major factors affecting height of subarachnoid block
are the baricity of the local anaesthetic solution and the dosage (mass) of drug injected.
3.2.4 FATE OF LOCAL ANAESTHETICS IN SUBARACHNOID SPACE
Following injection of local anaesthetic solution into subarachnoid space, its
concentration falls rapidly. The initial steep fall is due to mixing with CSF and
subsequent absorption into nerve roots and spinal cord. The regress of local
anaesthetics following subarachnoid injection is primarily by vascular absorption
with no hydrolysis or degradation taking place in the CSF. Depending on the type
of the drug used, it is metabolized in plasma by pseudocholinestrease of the liver.
8

9
3.2.5 INDICATIONS FOR SUBARACHNOID BLOCK
Spinal anaesthesia can be administered safely in,
• Lower abdominal surgeries
• lower limb surgeries
• urological procedures
• obstetric procedures
• gynaecological surgeries
• perineal & rectal surgeries 3.2.6 CONTRAINDICATIONS FOR SUBARACHNOID BLOCK
An absolute contraindication for subarachnoid block is patient refusal. Other
contraindications are:
• local sepsis
• uncorrected coagulopathy
• uncontrolled blood loss/shock
• fixed cardiac output states
• documented allergy to local anaesthetics
• raised intracranial pressure
• neurological disease
• major spine deformities/previous surgery on the spine
• severe cardiac disease

10
4.0 SPINAL ANAESTHESIA — TECHNIQUE
The first step in the successful application of spinal anaesthesia is proper
patient selection. This is accomplished by preanaesthetic evaluation of the patient
through history, physical examination, blood investigation, communication
with the patient and surgical staff about detail of the procedure. Suitable premedication
is given to the patient before performing the subarachnoid block. Intravenous access
through a large bore intravenous cannula is necessary to administer 500-1000 ml of
[15- 20ml/kg] of crystalloid to limit the hypotension that may result from the
sympathetic block produced by spinal anaesthesia. Emergency drugs and equipment
for managing airway should be readily kept. Spinal anaesthesia should be administered
to a cooperative patient who is placed on a table that can be tipped upward or
downward.
4.1 PROCEDURE 4.1.1 PREPARATION
Preparation of the equipment and drugs is essential for performing a
subarachnoid block. The choice of drug is based on the duration of block
desired, the surgical procedure and patient variables. Spinal needles of various
diameters with various types of points are available. Spinal needles fall into two main
categories; those that cut the dura and those designed to separate the dural fibers. The
former includes the Quincke – Babcock needle and the latter include the Greene,
Whitacre and Sprotte needles. In order to keep the incidence of post dural puncture
headache to a minimum, small bore needles with a rounded non- cutting bevel are
preferred.
11
4.1.2 POSITION
The choice of position of the patient for performing the subarachnoid block
depends on a number of factors, the proposed surgery being the most important.
The three primary methods of positioning include lateral decubitus, sitting and prone
positions; each with its own advantages in specific situations. In the lateral decubitus
position, the patient is placed with his back parallel to the edge of the operating table
nearest the anaesthesiologist, with thigh flexed upon the abdomen and neck flexed to
allow the forehead to be as close to the knees as possible. The sitting position is
chosen when low lumbar and sacral levels of anaesthesia are adequate for the
surgical procedure, when obesity or scoliosis make identification of midline
anatomy difficult in the lateral decubitus position or when orthopaedic problems of
the hip and knee exist. The prone position is used primarily for the hypobaric
technique for rectal and perineal procedures.
4.1.3 PUNCTURE
The spinal puncture can be performed either by a midline or a paramedian
approach, usually at the L2-L3. L3-L4 or L4-L5 interspaces. The procedure is
carried out under strict aseptic conditions. The patient’s back is widely prepared
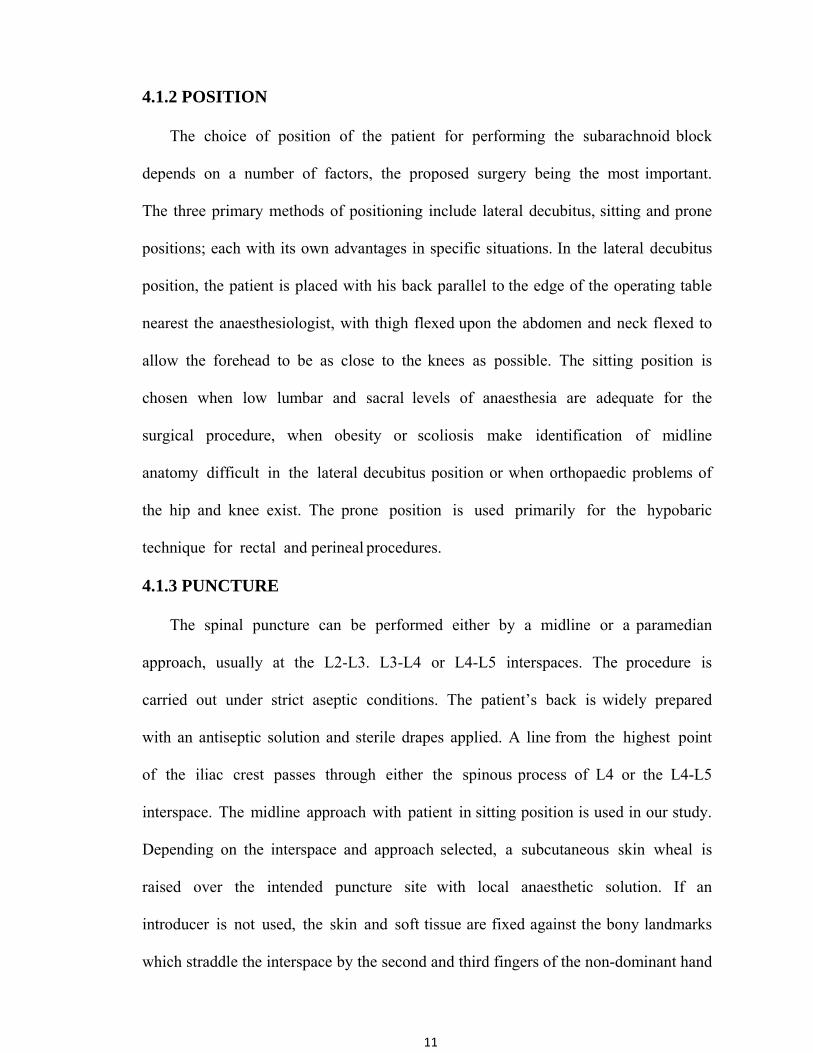
with an antiseptic solution and sterile drapes applied. A line from the highest point
of the iliac crest passes through either the spinous process of L4 or the L4-L5
interspace. The midline approach with patient in sitting position is used in our study.
Depending on the interspace and approach selected, a subcutaneous skin wheal is
raised over the intended puncture site with local anaesthetic solution. If an
introducer is not used, the skin and soft tissue are fixed against the bony landmarks
which straddle the interspace by the second and third fingers of the non-dominant hand

12
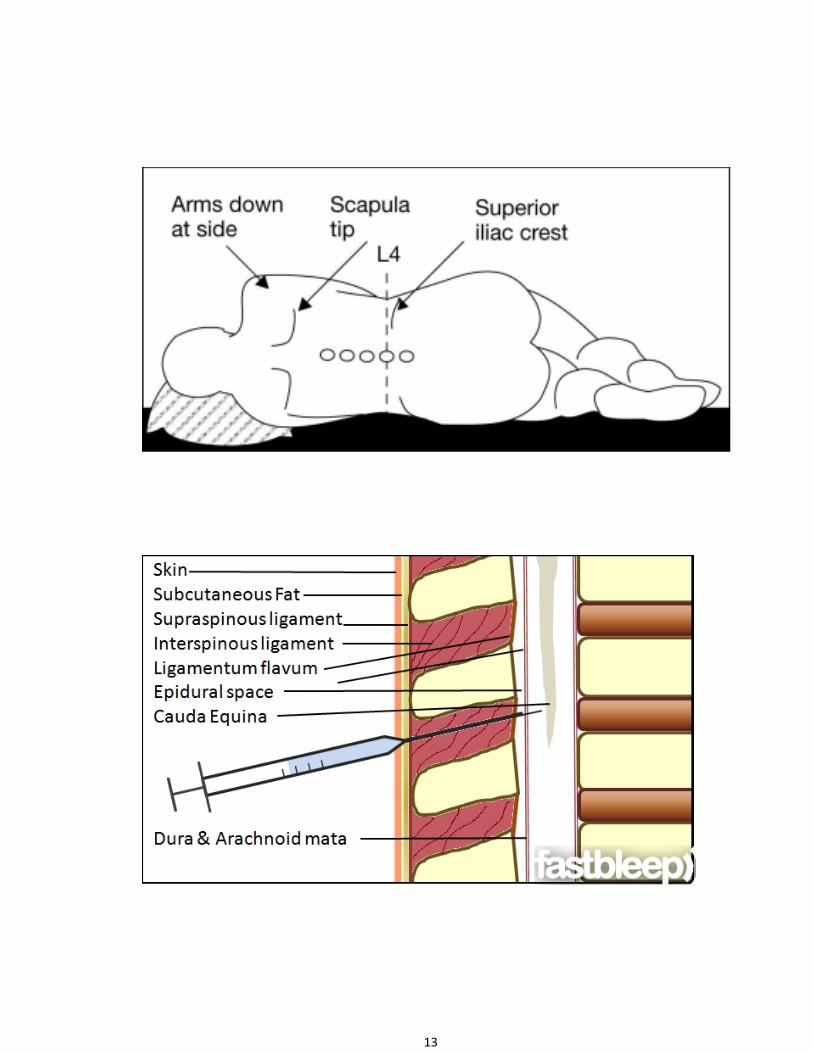
of the anaesthesiologist. The needle is inserted in midline in the middle of the
interspace with bevel parallel to the longitudinal dural fibers. After traversing the
skin and subcutaneous tissue, the needle is advanced in a slightly cephalad direction
with the long axis of the vertebral column. A characteristic change in resistance
occurs as the needle traverses the supraspinous ligament, interspinous ligament,
ligmentatum flavum, dura and pierces the arachnoid which becomes quite
recognisable as experience is gained. The stylet is removed and appearance of
cerebrospinal fluid at the hub of the needle confirms the correct position of the needle
tip. The hub of the needle is firmly held between the thumb and index finger of
the anaesthesiologist’s non-dominant hand and the back of that hand placed against
patient’s back to steady the needle, while syringe containing anaesthetic
solution is firmly attached to the needle.
After confirming the flow of spinal fluid by aspiration, the anaesthetic solution
is injected. The patient is placed in supine position. Cardiovascular and respiratory
functions are monitored. Analgesia is checked by loss of sensation to pinprick.
13
14
4. 2 COMPLICATIONS OF SUBRACHNOID BLOCK IMMEDIATE
1. Hypotension
2. Bradycardia
3. Toxicity due to intravascular injection
4. Allergic reaction to local anaesthetic
5. Hypoventilation (brain stem hypoxia) LATE
1. Post dural puncture headache
2. Retention of urine
3. Backache
4. Meningitis
5. Transient lesions of cauda equina
6. Sixth nerve palsy
7. Anterior spinal artery syndrome
8. Horner’s syndrome
15
5.0 PHARMACOLOGY OF BUPIVACAINE Bupivacaine is an amide local anaesthetic, synthesized by A.F. Ekenstam in 1957 and
brought into clinical use in 1963. It is produced for clinical use in a racemic
mixture, containing equal proportions of the ‘S’ and ‘R’ enantiomers. It is supplied
for clinical use as a hydrochloride salt.
Chemical Structure Description : ± 1 — Buty-N-(2, 6-dimethylphenyl)-2-piperidine
Decarboxamide Hydrochloride monohydrate.
Physico-chemical Profile
Molecular Weight (base) - 288
pKa - 8.1
Solubility in Alchohol - 1 in 8
Water - 1 in 25
Octanol /Water partition coefficient - High
Lipid solubility - 28
Plasma Protein Binding - 95%

16
5.1 MECHANISM OF ACTION
Bupivacaine acts by inhibition of sodium channels. It acts to block conduction in
the nerves by decreasing or preventing the large transient increases in permeability of
the cell membrane to sodium ions that follows depolarization of the membrane.
Bupivacaine also reduces the permeability of the resting nerve membrane to potassium
as well as sodium ions.
5.2 PHARMACODYNAMICS Bupivacaine has a stabilizing action on all excitable membranes. In the central
nervous system, stimulation can occur producing restlessness, tremors and
convulsions in over dosage. Bupivacaine also causes a reduction in the automaticity of
the heart.
The clinical profile of nerve blockade produced by Bupivacaine differs from that
of lignocaine. It is four times more potent than lignocaine, but the onset of action is
slower. The duration of action is considerably longer. The sensory block produced by
Bupivacaine tends to be more marked than the motor block.
5.3 PHARMACOKINETICS
Bupivacaine is rapidly absorbed from the site of injection. The rate of rise in
plasma Bupivacaine concentration and the peak plasma concentrations obtained
depend on the route of administration. There is also some inter individual variation
and peak systemic concentrations may occur between five (5) and thirty (30) minute
after administration.
17
PHARMACOKINETIC PROFILE
Volume of distribution at steady rate (Vdss) 72 litres
Clearance 0.47 L.min
T 1/2 α 2.7min
T ½ β 28min
T ½ γ 3.5hrs
5.4 METABOLISM
Possible pathways for metabolism of Bupivacaine include aromatic
hydroxylation, N-dealkylation, amide hydrolysis and conjugation. Only the N-
dealkylated metabolite N-desmethylbupivacaine has been measured in blood and urine
after epidural and spinal administration. The degradation of Bupivacaine takes place
in the liver. Renal disease is unlikely to alter the kinetics of Bupivacaine. Less than
10% of the drug is excreted unchanged in urine.
The onset of action of Bupivacaine occurs 20 — 30 minutes after a
peripheral nerve block and duration lasts for 8-9 hours
Clinical Applications
• Infiltration anaesthesia
• Peripheral nerve blocks
• Central neruraxial blocks (intrathecal, epidural and caudal)
Contraindications
• Paracervical block (in obstetrics)
• Known hypersensitivity to amide local anesthetics
• Intravenous regional anaesthesia (IVRA)
18
Preparations Available
0.25%, 0.5% solutions in 10ml and 20ml vials.
5mg/ml (0.5%) Bupivacaine and Plain 80mg dextrose in 4 ml ampoules
for intrathecal injection (Baricity 1.0207)
Recommended Safe Dose
Concentration Used
Maximum Permitted
Dose
0.125%-0.5% 3mg/kg body weight
0.75%(not to be used in obstertric epidurals)
Max.over 4 Hrs—150mg Max.during 24Hrs-400mg
0.5% plain / hyperbaric solution (intrathecal use)
20 mg.
Adverse Reactions
Adverse reactions are associated mainly with excess plasma levels of the drug,
which may be due to over dosage, unintentional intravascular injection or slow
metabolic degradation.
CNS Reactions
Excitation characterized by restlessness, anxiety, dizziness, tinnitus, blurred
vision or tremors possibly proceeding to convulsions, followed by drowsiness,
unconsciousness and cardiac arrest.
19
Cardiovascular System Effects
Part of the cardiac toxicity that occurs from high plasma concentrations of
Bupivacaine occurs because of blockade of cardiac sodium channels. Accidental
intravenous injection of Bupivacaine causes cardiac dysarrthymias, atrioventricular
block, verticular tachycardia and ventricular fibrillation. Pregancy increases
the sensitivity of cardiotoxic effects of Bupivacaine.
Allergic Reactions
Manifests as urticaria, pruritus, angioneurotic edema etc. Cross sensitivity among
members of amide type local anaethetics has been reported.

20
6.0 PHARMACOLOGY OF DEXMEDETOMIDINE
Dexmedetomidine is a highly selective α2 adrenergic agonist that produces
sedation, hypnosis and analgesia.
STRUCTURE OF DEXMEDETOMIDINE CHEMISTRY:-
- 4[cs]-alpha,2,3-Trimethylbenzyl)imidazole
- Dexmedetomedine Hydrochloride is the s-enantiomer of medetomidine
and is chemically described as:
- (+)-4-(s)-[1-(2,3-dimethylphenyl)ethyl]-1H-imidazolemonohydrochloride
Molecular formula: C13H16N2.Hcl
Molecular Weight: 236.74
21
PHARMACOLOGICAL PROFILE:
Dexmedetomidine is highly selective α2 adrenergic agonist. It shows a high
ratio of specificity for the α2 receptor [α2:d1, 1600:1] compared with clonidine
[α2:d1 200:1] making it a complete α2 agonist. Dexmedetomidine belongs to the
imidazole subclass of α2 agonists. Dexmedetomidine is the active s-enantiomer of
meditomedine. It is highly water soluble and is available as a parenteral and
preservative free formulation.
6.1 PHARMACOKINETICS: T1/2-6 minutes. It is 94% protein bound and its concentration ratio in whole blood
and plasma is 0.66.
METABOLISM:
Dexmedetomidine undergoes biotransformation by conjugation [41%], N-
methylation [21%] or hydroxylation followed by conjugation in liver. The inactive
metabolites excreted in urine and faces. The elimination half-life of Dexmedetomidine
is two (2) to three (3) hours, with a context-sensitive half time ranging from four (4)
mins after a ten (10) minute infusion to two hundred and fifty (250) minutes after an 8-
hour infusion. Pharmacokinetics are similar in young adults and elderly.
MECHANISM OF ACTION:
Dexmedetomidine is a highly selective α2 agonist. There are 3 types of α2
adrenoreceptors in humans: α2A, α2B, α3C. The α2A adrenoreceptors are primarily
distributed in the periphery where as α2B and α2C receptors are located in the
Brain and Spinal cord.

22
Presynaptic activation of α2 adrenoreceptors inhibits the release of nor-
epinephrine.
Post synaptic activation of α2-adrenoreceptors in the central nervous system
inhibits sympathetic activity and decreases blood pressure and heart rate producing
sedation and anxiolysis.
Analgesia is produced through binding of dexmedetomidine to α2 adrenergic
receptors in the spinal cord.
The overall response to α2 adrenoreceptor agonists is related to the stimulation of
α2 adrenoreceptors located in the CNS and spinal cord.
Dexmedetomidine produces sedation and hypnosis by action on α2 receptors in
the locus ceruleus and analgesic effect by acting at α2 receptors with in the locus
ceruleus and with in the spinal cord.
6.2 ACTIONS: 6.2.1 EFFECTS ON THE CENTRAL NERVOUS SYSTEM:
SEDATION
The α2 agoinst acts through the endogenous sleep-promoting pathways to exert
their sedative effect.
It produces good sedative effect-yet arousable, alert and able to respond without
becoming uncomfortable. Despite sound levels of sedation with Dexmedetomidine,
there is limited respiratory depression.
ANALGESIA:
The analgesic effects of Dexmedetomidine are complex. They have an
analgesic effects when injected through the intrathecal or epidural route. The
primary site of action is thought to be the spinal cord.

23
Systemic use of Dexmedetomidine shows narcotic sparing. narcotic
requirements were reduced by 50% in patients receiving Dexmedetomidine.
OTHER EFFECTS:
Dexmedetomidine in animal models of incomplete cerebral ischaemia and
reperfusion reduces cerebral narcosis and improves cerebral outcome by reducing
the intra cerebral catecholamine outflow and the reduction of the excitatory
neurotransmitter glutamate during injury.
Dexmedetomidine also reduces muscle rigidity after high-dose opioid
administration.
6.2.2 EFFECTS ON THE RESPIRATORY SYSTEM:
Dexmedetomidine of concentrations producing significant sedation reduces
minute ventilation but retains hyper capnic ventilation response. The changes in
ventilation appeared similar to those observed during natural sleep. Dexmedetomidine
has been implicated in blocking histamine – induced broncho constriction in dogs.
6.2.3 EFFECTS ON THE CARDIOVASCULAR SYSTEM:
The basic effects of Dexmedetomidine on the cardiovascular system are
decreased heart rate, decreased systemic vascular resistance and indirectly decreased
myocardial contractility and systemic Blood pressure.
The effects of Dexmedetomidine on blood pressure shows a Biphasic response
an initial increase in Blood pressure that occurred of 5 mins after administration
[due to the vaso constrictive effects of Dexmedetomidine on peripheral α2
adrenoreceptors] followed by decreased in Blood pressure due to action on central α2
adrenoreceptor activity.
24
The incidence of Hypotension and Bradycardia may be related to the
administration of loading dose. Omitting the loading dose or restricting the dose up
to only 0.4μg/kg reduces the incidence of Hypotension. Giving the loading dose
over 20 minutes also minimizes the transisent Hypertension.
6.2.4 DOSAGE AND ADMINISTRATION:
Dexmedetomidine is supplied in 2ml ampoule, 100μg-ml & 1ml ampoule
50μg/ml. Preservative free
• Loading dose – 0.5 – 1.0μg/kg over to10 minutes
• Maintenance dose – 0.3 – 0.7μg/kg/hr 6.2.5 USES:
Dexmedetomidine has been approved as a short-term sedative for adult intubated
patients in ICU.
1. INTENSIVE CARE UNIT:
• Dexmedetomidine has following advantages for sedation in mechanically
ventilated patients. Decreased requirement for opioids >50% when
compared with propofol or Benzobiazepines.
• Providing adequate sedation with minimal respiratory depression. Can be
used when weaning patients from ventilator.
• Dexmedetomidine has been used in the treatment of alcohol and drug
withdrawal of narcotics, benzodiazepines and recreational drugs.

25
2. ANAESTHESIA:
• Dexmedetomidine at doses of 0.3-0.67μg/kg given 10-15 minutes before
induction attenuates the hemodynamic response to intubation.
• As a premedication 2.5μg/kg IM.
• Used for securing the airway during fibreoptic intubation.
• Sedation during regional Anaesthesia.
• As an anaesthetic adjuvant in Bariatric surgery, sleep apnea patients.
Vascular surgery, CABG surgery, Craniotomy ancurysm,
evoked potential study, thoracic surgery.
CONTRA INDICATIONS:
• Infusions over 24 hrs
• In caesarean deliveries, as the safety has not been studied
• Patients with preexisting Bradycardia and related Bradyarythmias.
• Patients with impaired ventricular function –Ef<30%]
• Hypovolemic or Hypotensive patients.
• Patients with raised intra cranial tension.
26
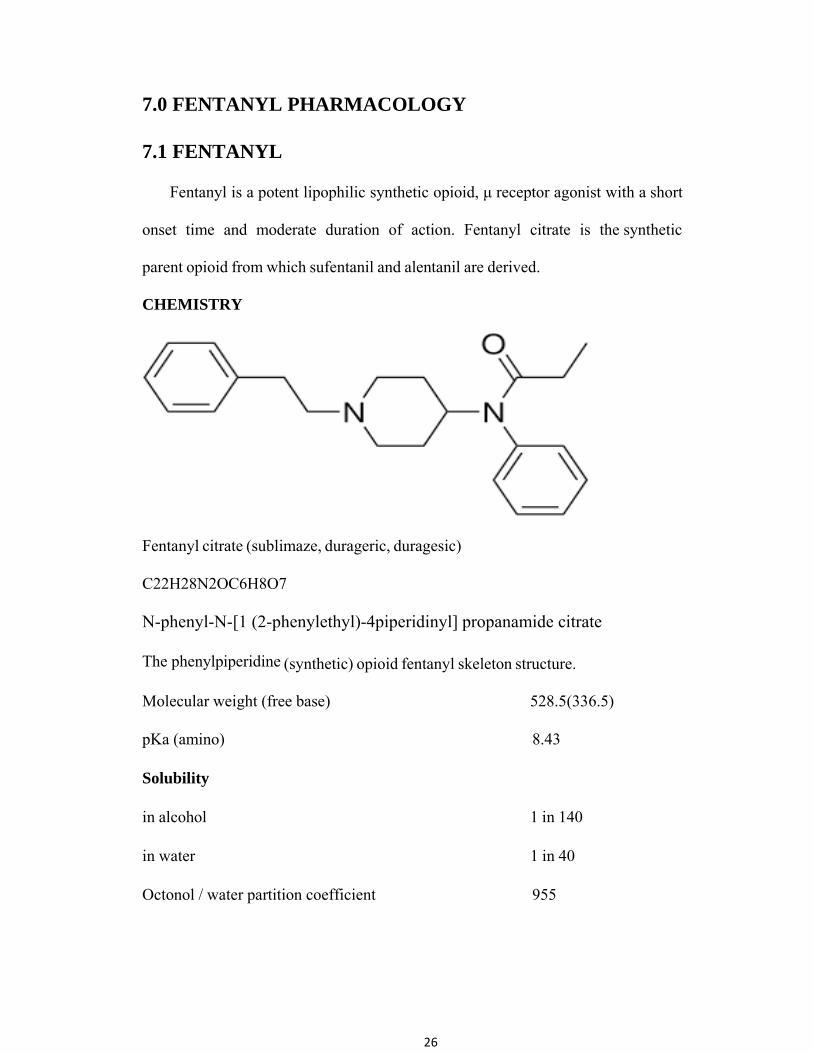
7.0 FENTANYL PHARMACOLOGY 7.1 FENTANYL
Fentanyl is a potent lipophilic synthetic opioid, μ receptor agonist with a short
onset time and moderate duration of action. Fentanyl citrate is the synthetic
parent opioid from which sufentanil and alentanil are derived.
CHEMISTRY
Fentanyl citrate (sublimaze, durageric, duragesic)
C22H28N2OC6H8O7
N-phenyl-N-[1 (2-phenylethyl)-4piperidinyl] propanamide citrate The phenylpiperidine (synthetic) opioid fentanyl skeleton structure.
Molecular weight (free base) 528.5(336.5)
pKa (amino) 8.43 Solubility in alcohol 1 in 140 in water 1 in 40
Octonol / water partition coefficient 955

27
Fentanyl is a μ agonist. It has a more rapid onset and shorter duration of action
than morphine. The greater potency and more rapid onset of action reflect the
greater lipid solubility of fentanyl compared with that of morphine.
Fentanyl produces dose related analgesia. Small doses of 0.5-3.0μgkg-1may be
used as a supplement in spontaneously breathing anaesthetized patients. Doses of
5.0μgkg-1 upward will suppress somatic and autonomic responses to surgical
stimulation in ventilated patients.
Doses of 50μgkg-1 in conjunction with muscle relaxant and mechanical
ventilation, may be used to induce and maintain anaesthesia.
Fentanyl is a potent respiratory depressant and reduces brain stem respiratory
responsiveness to CO2 and peripheral chemoreceptor input during hypoxemia.
Fentanyl exerts minimal effects on the circulation. There is a vagally
mediated bradycardia and a slight fall in systemic vascular resistance.
Skeletal muscle rigidity and clonic movements can hinder mechanical
ventilation. This effect is reversed by naloxone and overcome by neuromuscular
blocking drugs. Rigidity may also occur during emergence from anaesthesia. High dose
fentanyl obtunds the metabolic and hormonal response to surgery.
There is a reduction in metabolic activity following fentanyl and hence in oxygen
consumption. Nausea and vomiting are the result of stimulation of the chemoreceptor
trigger zone. Cough suppression, pupillary constriction and itching of the nose also
occur.

28
Fentanyl has been found to significantly increase intracranial pressure in patients
with severe head injury. Fentanyl also significantly decreases cerebral perfusion
pressure. Fentanyl may cause a rise in biliary intraluminal pressure. Fentanyl will
reduce intraocular pressure independent of changes in arterial blood pressure.
Relative contraindications for fentanyl are
1. Hypovolemia
2. Respiratory inadequacy
3. Raised ICP
29
7.2 PHARMACOKINETICS
A three-compartment model is typically used to describe plasma fentanyl
concentration decay. The lungs exert a significant first pass effect and transiently
take up approximately 75 percent of an injected dose of fentanyl.
As is typical of the fentanyl both volume of distribution (3-6Lkg-1) and
clearance (10-20 mlkg-1 min-1) are high.
Approximately 80% of fentanyl is bound to plasma proteins, and significant
amount (40%) are taken up by red blood cells. As the pKa of fentanyl is high
(8.4) at physiologic pH, it exists mostly in the ionized from (> 90%). Fentanyl’s lipid
solubility is also high, a finding that explains in part its large volume of distribution.
The tissue/blood partition coefficient of fentanyl is found to be 2-30 fold higher
than those of alfentanil. Because fentanyl is distributed so widely in the body, it
must ultimately be returned to the blood to be metabolized in the liver. Fentanyl is
relatively long acting, in large part because of its widespread distribution in body
tissues.
Fentanyl is primarily metabolized in the liver by β-dealkylation and
hydroxylation. Fentanyl has a high hepatic clearance (approaching hepatic blood
flow) and a high hepatic extraction ratio (approaching 1.0). Metabolism begins to
appear in the plasma as early as 1.5 min after injection. Norfentanyl, the primary
metabolite, is detectable in the urine for upto 48 hours after IV fentanyl in
humans. The activity of fentanyl’s metabolites is unclear, but it is thought to be
minimal. Little fentanyl is excreted in the urine unchanged.

30
7.3 FACTORS THAT ALTER PHARMACOKINETICS AND PHARMACODYNAMICS
• Age: The elimination of fentanyl in neonates is prolonged. With
advanced age although pharmacokinetics changes may play a minor role.
• Weight: Fentanyl pharmacokinetics is not grossly different in lean versus
obese subjects.
• Renal failure: For the fentanyl congeners the clinical importance of
kidney failure is less marked.
• Hepatic failure: Reduction in liver blood flow that result from either
liver disease or some other disorder will delay the decline of fentanyl
plasma concentration.
• Cardiopulmonary bypass: Fentanyl pharmacokinetics is extensively
altered by CPB.
• Acid-base changes: Acidosis increase ionized fentanyl in the interstitial
space, draws unionized fentanyl out of the intracellular compartment,
where a 13-fold accumulation of fentanyl occurs, further augmenting
opioid effects, i.e. ventilatory depression.
31
8.0 REVIEW OF LITERATURE
1. Subhi M. Al-Ghanem et al 19(American Journal of applied Science 6[5] 882-
887- 2009) studied to evaluate the onset and duration of sensory and motor
block as well as operative analgesia and adverse effects of
DEXMEDETOMIDINE or fentanyl given intrathecally with plain. Bupivacaine
for spinal anaesthesia. 78 patients were scheduled for vaginal hysterectomy,
vaginal wall repair and tension free vaginal tape were prospectively studied
patients were randomly allocated to receive intrathecally either 10mg of isobaric
bupivacaine plus 5μg of DXM [Group [n=38] or 10mg of isobaric bupivacaine
plus 25μg of fentanyl [Group F n=38], the onset time, peak sensory and motor
level, the regression time for both sensory and motor Blockade, hemodynamic
changes and side effects were recorded. Patients in Group-D had significant
longer sensory and motor block times than patients in Group-F the mean
time of sensory regression to S1 was 274±73 min in group D and 179±41 min
group F [p < 0.001]. The regression time of motor block to reach modified
Bromage 0 was 240±60 min in group D and 179±47 min in Group F [p <
0.001]. The results suggested that 10mg plain Bupivacaine with 5μg DXM
produces prolonged motor and sensory block compared with 25μg Fentanyl.

32
2. Mahmoud M. Al-mustafa 12 (Saudi medical journal 2009 – vol 30 [3];365-370)
et al studied to determine the effect of adding DXM to Bupivacaine for
neuraxial anaesthesia 66 patients were randomlyassigned in 3 groups each
receiving spinal bupivacaine 12.5mg combined with Normal saline (Group N),
DXM 5μg [Group D5] & DXM 10mg [Group D10]. The onset time to reach
T10 sensory and Bromage 3 motor block and the regression times to reach
S1 sensory level and Bromage 0 motor scale were recorded. The mean time of
sensory Block to reach the T10 dermatome was 4.7+/-2.0 minutes in D10 group,
6.3+/-2.7 minutes in D5 and 9.5+/-3.0 minutes in group N. The mean time to reach
Bromage 3 scale was 10.4+/-3.4 minutes in Group D10 13.0+/-3.4 minutes D5
and 18.0+/-3.3 min in Group N. The regression to Bromage 0 was 302.9+/-36.7
min in D10, 246.4+/-25.7 min in D5 and 140.1+/-32.3 minutes in Group N. The
conclusion was dexmedetomidine has a dose dependent effect on the onset and
regression of sensory and motor block when used as an adjuvant to Bupivacaine in
spinal anaesthesia.
3. Kanazi et al 9 (Acta anaesthesion scan 2006;50;222-227) studied to compare the
onset and duration of sensory and motor block as well as the hemodynamic
changes and level of sedation following intrathecal bupivacaine supplemented
with either DXM or clonidine 60 patient received 12mg of 0.5% Bupivacaine
[n=20], Group B, Group D received 12mg 0.5% Bupivacaine with 3μg of DXM
and group C received 12mg of 0.5% Bupivacaine supplement with 30μg of
clonidine. The onset times to reach peak sensory and motor levels and the
33
sensory and motor regression times, were recorded. Hemodynamic changes
and the level of sedation were recorded. Patients in Groups D and C had a
significantly shorter onset time of motor block and significantly longer sensory
and motor regression times than patients in Group B. The mean time of
sensory regression to the S1 segment was 303±75 min in Group D, 272±38
min in group C and 190±48 min in group B. The regression of motor block to
Bromage 0 was 250±76 min in group D, 216±35 min in group C and 163±47
in group B [p valve < 0.001]. The onset and regression times were not
significantly different between groups D and C. The mean arterial pressure, heart
rate and level of sedation were similar in the three groups intra operatively and
post-operatively. DXM (3μg) or clonidine (30μg), when added to intrathecal
Bupivacaine, produces a similar prolongation in the duration of the motor and
sensory block with preserved hemodynamic stability and lack of sedation.
4. Ibrahim. F.A. Khalifa et al 7(Benha MJ Vol 26; 3;Sep 2009) studied the
effect of adding intrathecal dexmedetomidineVs sufentanyl to heavy
bupivacaine for post-op analgesia in patients undergoing inguinal hernia repair.
50 ASA Grade I/II patients, scheduled for elective inguinal hernia repair with
5μg of DXM and 5μg of sufentanyl with heavy bupivacaine 0.5% 2ml onset and
duration of sensory and motor blockade, surgical condition and side effects were
assessed. The duration of effective post-operative analgesia as assessed by VAS
was not statistically significantly in between both groups. Cardio vascular and
respiratory stability was maintained with no significant incidence of side effects in
either group. The addition of DXM 5μg and sufentanil 5μg intrathecally provide
34
improved postoperative analgesia and hemodynamic stability Dexmedetomidine
prolongs the post-op analgesia as sufentanil but with minimal side effects.
5. Antonio Mauro Vieira et al studied the analgesia and sedation promoted by
clonidine or DXM associated to epidural ropivacaine, in the post-operative
period to subcoastal cholecystectomy 40 pts of ASA I & II received clonidine
150μg to epidural ropivacaine 0.75% [20ml], DXM 2μg/kg-1 associated to
epidural ropivacaine 0.75% 20ml. Analgesia and sedation were evaluated 216
and 24 hours anesthetic recovery. Both groups present some grade of sedation in
the moments 2 and 6 hours, with statistically significant difference between the
two moments for DXM group. There has bee analgesia in 6 and 24 hrs in the
DXM group; in the clonidine group, this statistically significant difference was
observed between the periods of 2 and 6 hours and between 2 and 24 hours. The
conclusion was allowed to conclude that the association of clonidine or DXM
to 0.75% ropivacaine induces analgesia and sedation in 2 and 6 hours after
anesthetic recovery in patients submitted to subcostal cholecystectomy and that
clonidine promotes more prolonged analgesia.
6. Saadway et al 15(Acta Anaesthesiol Scand 2009;53;251-256) studied the
effect of DXM on the characteristics of Bupivacaine in a caudal block in
pediatrics. 66 children undergoing unilateral inguinal hernia repair/orchidopexy
were allocated randomly and Group B (n=33) received a caudal injection of
Bupivacaine 2.5mg/ml, 1ml/kg; Group BD(n=33) received the same dose of
Bupivacaine mixed with Dex 1μg/kg during sevoflurane anaesthesia. Processed
EEG [BIS], heart rate, Blood pressure, pulse oximetry and end-tidal sevoflurane
35
were recorded every 5 min. The characteristics of emergence, objective pain
score, sedation score and quality of sleep were recorded post-operatively.
Duration of analgesia and requirement for additional analgesics were noted. The
results were the end-tidal sevoflurane concentration and the incidence of
agitation were significantly lower in the BD group [p < 0.05 ]. The duration of
analgesia was significantly longer (p < 0.001) and the total consumption of
rescue analgesia was significantly lower in Group BD compared with Group B (p
< 0.01). Group BD had better quality of sleep and a prolonged duration of
sedation ( p < 0.05) and the conclusion was caudal Dexmedetomidine seems to
be a promising adjunct to provide excellent analgesia without side effects over a
24hr period. It has the advantage of keeping the patients calm for a prolonged time.
7. El. Hennawy Am et al6 (British Journal of anathesia 2009.aug 103[2];268-
274;Epub 2009. June 18) studied the addition of clonidine or dexmedetomidine
to Bupivacaine prolongs caudal analgesia in children. Undergoing lower
abdominal surgeries. 60 patients [6 months to 6 years] were evenly and randomly
assigned into three groups in a double-blinded manner. After sevoflurane in
oxygen anaesthesia, each patient received a single caudal dose of bupivacaine
0.25% [1ml kg (-1)] combined with either DXM 2μg/kg in normal saline 1ml,
clonidine 2μg/kg in normal saline 1ml or corresponding volume of normal saline
according to group assignment. Hemodynamic variables, end- tidal sevoflurane
and emergence time were monitored. Postoperative analgesia, use of analgesics
and side effects were assessed during the first 24 hr. The results were the
addition of DXM or clonidine to caudal bupivacaine significantly promoted
36
analgesia time [median [95% confidence internal c1]; 16 (14-18) and 12(3-21)h,
respectively] than the use of sevoflurane and emergence time were monitored.
Postoperative analgesia, use of analgesics and side effects were assessed during
the first 24 hr. The results were the addition of DXM or clonidine to caudal
bupivacaine significantly promoted analgesia time [median [95% confidence
internal c1]; 16 (14-18) and 12(3-21)h, respectively] than the use of Bupivacaine
alone [ median (95%c1); 5 (4-6)h] with p<0.001. However, there was no
statistically significant difference between dexmedetomidine and clonidine as
regards the analgesia time (p=0.796). The conclusion was addition of DXM or
clonidine to caudal bupivacaine significantly promoted analgesia in children
undergoing lower abdominal surgeries with no significant advantage of
dexmedetomidine over clonidine and with out an increase in incidence of side
effects.
8. Seewal R et al17 (Regional anathesia pain medicine 2007, Jan-feb 32[1]; 20-6)
studied the effect of adding various doses of fentanyl to 2.2ml of Bupivacaine
(0.5% Hyperbaric] for spinal anaesthestic in non-obstetric population undergoing
superficial lower abdominal surgery. 60 patients received spinal anaesthetic
with 2.2 ml of bupivacaine [0.5% Hyperbaric] and saline [control group], or
Fentanyl 10, 20, 30 or 40 microgram. The volume of injected drug was kept
constant at 3 ml by adding preservative free normal saline for blinding
purposes. Subarachanoid block characteristics, drug-related side effects and post-
operative analgesia requirements were assessed and recorded. Results showed a
significant improvement in quality and duration of analgesia occurred in study

37
groups compared with the control group p < 0.05. However no improvement in
analgesia occurred when the dose of fentanyl added was increased from 10 to
20, 30, 40 microgram. Conclusion was study group significantly improves the
quality and duration of analgesia. Seewal R – Effect of addition of various doses
of fentanyl intrathecally to 0.5% Hyperbaric Bupivacaine on perioperative
analgesia and subarachanoid block characteristics in lower abdominal surgery.
9. Bogra J, srivastara P et al1 (BMC Anaesthesiology 2005 may 17;5[1];5)
studied the synergistic effect of intrathecal fentanyl and bupivacaine in spinal
anaesthesia for caesaran section there by reducing the dose, & side effects,
caused by higher doses of intrathecal bupivacaine in cesarean section. 120
patients divided in to 6 groups, identified as B8, B10, B12.5, and 12.5mg of
bupivacaine and FB8, FB10, FB 12.5 mg received a combination of 12.5μg
intrathecal fentanyl respectively. The parameters taken into consideration were
visceral pain, hemodynamic instability, intraoperative sedation, intraoperative
and post-operative shivering and post operative pain. The results were the
onset of sensory block E0 T6 occurred faster with increasing bupivacaine
doses in bupivacaine only groups and bupivacaine – Fentanyl combination
groups. Lower concentrations of bupivacaine alone could not completely
removed the visceral pain. Blood pressure declined with the increasing
concentration of Bupivacaine and Fentanyl. Incidence of nausea and shivering
reduces significantly whereas, the post operative pain relief and hemodynamics
increased by adding fentanyl. Conclusion was there is synergistic,
potentiating effect of fentanyl on bupivacaine in spinal anesthesia for cesarian
38
section is presented, Fentanyl is able to reduce the dose of bupivacaine and
therefore is harmful effects.
10. Biswas B.N. et al. (2002) conducted a study on forty healthy women of
ASA Gr I Scheduled for elective caesarean section. They were randomly allocated
to receive 2 ml of 0.5% inj Bupivacaine (hyperbaric) with 0.25 ml of normal
saline (Group A n = 20) or 0.25 ml (12.5 µg) fentanyl with (using a tuberculin
syringe) (Group B n = 20) 2 ml of 0.5% inj Bupivacaine (hyperbaric). Pulse rate,
blood pressure, respiratory rate and foetalheart rate were recorded. Patients were
prehydrated with 15 ml kg-1 Ringers lactate solution before spinal anaeshthesia.
The onset and duration of sensory block was assessed by pinprick method. Time
taken from intrathecal injection to the highest level of sensory block and sensory
regression to the L1 dermatome were recorded. The onset and duration of motor
block was noted. Grading of motor block was done as per Bromage score. Pain
was evaluated using a standard 10 cm linear visual analog scale (VAS). The
duration of complete analgesia (Time from SAB to first report of pain) and time of
effective analgesia (Time from subarachnoid injection to first doses of rescue
analgesic) were recorded. Vital parameters and adverse effects, i.e. pruritus,
nausea, vomiting, shivering were recorded. Every 2 minutes for first 20
minutes, then at 15 minutes interval for remainder of operation and thereafter
at 30 minutes interval until patient complained of pain. APGAR scores were
recorded at 1 and 5 minutes after delivery of baby. The highest sensory level
achieved were T7 (T6-T8) and T5 (T4-T6) in group A and B respectively. In
fentanyl group the time taken for sensory level to regress to S1 dermatome were
39
prolonged but duration of motor blocks was not prolonged.
11. Sahar M Siddik Sayyid et al. (2002) conducted a study on 48 parturients
scheduled for elective caesarean delivery. Patients were randomized double
blinded. Patients were all classified as ASA physical status of I and II and had
no contraindication to spinal anaesthesia. The 48 subjects were allocated into
two groups by using sealed envelope technique. The IT fentanyl group received 12
mg hyperbaric bupivacaine 0.75% and 12.5 µg of IT fentanyl (23 patients). The
IV fentanyl group received 12 mg of hyperbaric bupivacaine 0.75% alone (25
patients), mix with CSF to achieve the same volume. In the OT room patient
preloaded with 500 ml of polygeline (hemacel). LP was done in sitting posture.
Immediately after intrathecal administration of drug, 12.5µg inj fentanyl IV
given in the IV fentanyl group. Immediately after SAB patient was put in a
supine position with 15°-20° left lateral tilt and 5L oxygen given via mask.
Blood pressure, pulse rate and SPO2 was measured every minute until delivery
of the baby and at the 3 min interval until the end of the surgery.
Whenever the systolic BP falls 20% below baseline 5 mg of IV ephedrine
administered. Sensory block assessed by pinprick method every minute until
block reached T6 dermatome. There after every 2 min until the maximum
sensory block level was confirmed.
40
9.0 MATERIALS AND METHODS
This study was conducted at the Institute of obstetrics and Gynaencology,Rajiv
gandhi Government general Hospital,MMC, Chennai-600 008 betweenApril 2016 -
July 2016 on 60 patient of ASA physical status Iand11 undergoing Elective Total
abdominal Hysterectomy under subarachnoid block. This study was done after
Government General Hospital Ethical committee approval and a written informed
consent obtained from all the patients included in this study.
Study Design
This study was done in a prospective double blinded randomized manner. Each
group consisted of thirty patients.
Group D
Patients in this group received 3.0 ml of 0.5% hyperbaric bupivacaine + 5μg
[0.5 cc] of preservative free Dexmedetomidine to a total volume of 3.5 ml
intrathecally.
Group F
Patients in this group received 3.0ml of 0.5% hyperbaric bupivacaine + 25μg
[0.5 cc] of Fentanyl to a total volume of 3.5ml intrathecally. The final volume of
injected solution was 3.5ml in both groups.
In this study 0.5% hyperbaric bupivacaine in 8% dextrose, Dexmedetomidine
hydrocholoride 100μg/1ml and preservative free fentanyl 50μ/1ml. All solutions
were prepared by the OT incharge anaesthesiologist under strict aseptic precautions,
uninvolved in the administration of SAB or in the observation of results.

41
9.1 SELECTION OF CASES:
Inclusion criteria:
Age:30yrs to 50yrs
ASA physical status Iand 11
BMI:<30kg/m2
Surgery:elective surgery
Normal liver and renal function test,coagulation profile
Who have given valid informed consent
Airway: MMS (Modified Mallampatti score) 1 OR 2
Exclusion criteria:
Not satisfying inclusion criteria.
Lack of written informed consent.
Hypersensitivity to the study drug.
Renal or Hepatic dysfunction
Bleeding diathesis
Uncontrolled labile Hypertension & Diabetes mellitus.
Patient refusal.
Infection at injection site.
Patient with anticipated difficult airway.
Patient with abnormal spinal anatomy.

42
9.2 PRE ANAESTHETIC EVALUATION
Patients included in this study underwent through preoperative evaluation
which included the following
History
History of underlying medical illness, previous surgery and hospitalization. Physical examination:
1. Vital signs
2. Height and Weight.
3. Examination of CVS, RS, CNS, Spine
4. Airway assessment. Investigations:
Haemoglobin (Hb), BT, CT, Renal function test (RFT), Blood grouping &
Typing, ECG, Chest X-Ray (CXR), were done. Patient who satisfied the inclusion
criteria were explained about the nature of the study and the anaesthetic procedure and
written informed consent were obtained from all patients included in the study.
PRE LOADING:
In the premedication room pulse rate, BP, RR and sp02 was noted. An IV line
was secured with 16G cannula. Preloading done with RL 500ml over 20-30 minutes.
43
Technique
In the OT appropriate equipment for airway management and emergency drugs
were kept ready. Patient was shifted from the premedication room to OT. The
horizontal position of the operating table was checked and the patient was placed
on it. NIBP, SP02, ECG leads were connected to the patient. Pre operative base line
systolic and diastolic BP, PR, SP02 and RR were recorded. The anesthesiologist who
were unaware of the drug combination performed the SAB and made observations in
all the patients involved in the study. A midline lumbar puncture was performed
using a 25G Quincke needle in Right lateral position. Then patient was placed in
supine position. The time of intrathecal injection was considered as 0 and following
parameter were observed.
Sensory Block
Sensory block was assessed by loss of sensation to cold by cold alcohol swab
along the mid clavicular line bilaterally, immediately after intrathecal injection and
continued every 15sec till loss of cold sensation at T10 level till it reaches peak [T6
level]. The level of sensory block was noted at the end of the surgery and there after
assessment was carried out at 15 mts interval till return of cold sensation at s1
dermatome, duration of sensory block was taken as the time from subarachanoid
injection to return of cold sensation to s1.
44
Motor block
Motor block was assessed using modified BROMAGE Score
Bromage 0 – Patient is able to move the hip, knee and Ankle
Bromage 1 – Patient is unable to move the hip, but is able to move knee & ankle.
Bromage 2 – Patient is unable to move hip & knee but able to move ankle
Bromage 3 – Patient is unable to move hip, knee and ankle.
Assessment of motor block was started immediately after the
intrathecal injection. It was tested every 15 seconds till peak motor block
Bromage score was reached. The regression time for sensory and motor block
were recorded in post operative ward.
Vital Signs and side effects
The systolic and diastolic BP, RR, PR & Sp02 were recorded every 1mt for
5mts and thereafter every 5mts throughout the intra operative period. The above vital
signs at the completion of surgery were noted. Hypotension defined as fall in systolic
BP > 30% from baseline or MAP < 60mm of Hg. This was managed with Inj.
Ephedrine 6mg increments. Bradycardia was defined as heart rate <50/mt and this
was managed with Inj. Atropine 0.01mg/kg iv. Respiratory depression defined as
RR <8/mt and or Sp02 < 85%. This was planned to be managed with bag and mask
ventilation or intubation and IPPV if necessary. Blood loss more than the allowable
loss was replaced with blood. Vomiting was treated with Inj. Emeset 4mg iv.
Pruritus was noted. Since this is a benign subjective symptom which is under
reporting and usually need no treatment and need for any intra-op Analgesia was not
noted.

45
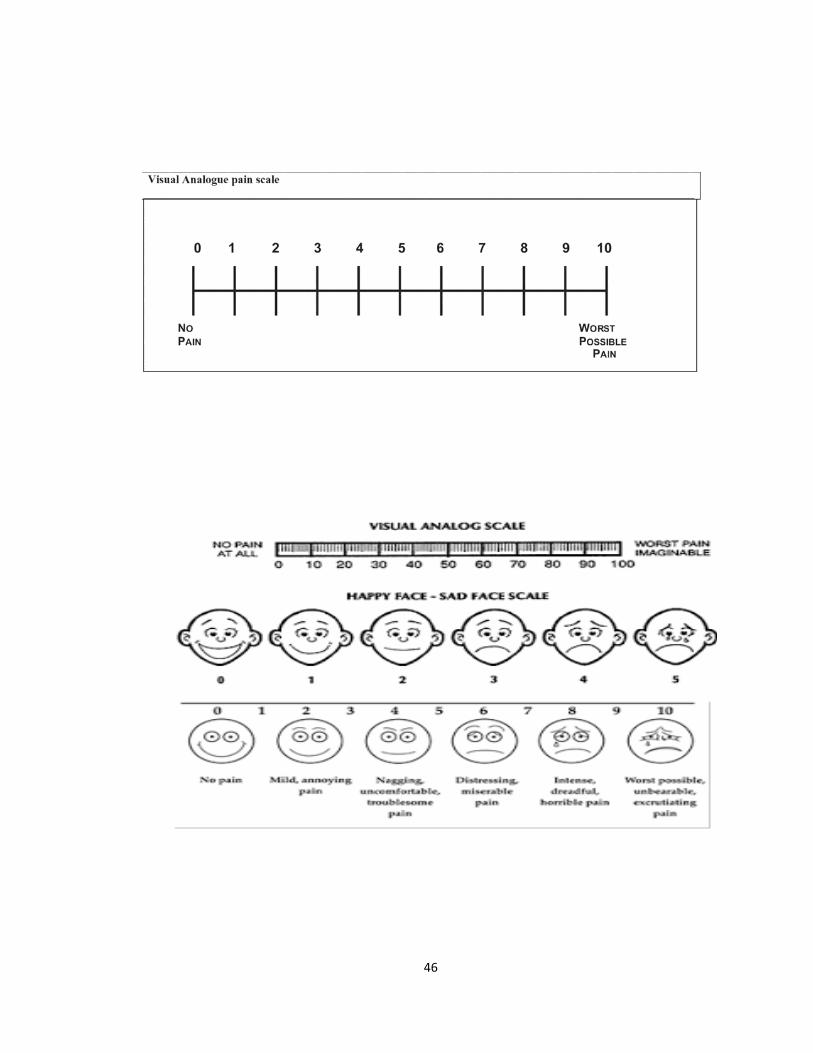
Assessment of pain and duration of analgesia
Pain was assessed by visual analog score
0-No pain.
1-mild pain.
2-Moderate pain.
3-Severe pain.
Quality of surgical anaesthesia:
Surgical ananesthesia was graded as excellent if there was no complaint of pain at
any time during surgery. Good if there was minimal pain or discomfort which was
relieved by a small dose of iv pentazocine 0.5mg/kg and poor if GA has to be
administered.
Assessment in post operative ward:
The patient was shifted to the post operative ward after completion of
surgery. The vitals signs were recorded till the regression of both motor Block
[Bromage 0] & the sensory block [s1] pain was assessed every 15 minutes. When the
patient reaches the pain score 2 or 3Inj. Diclofenac 75mg Im was given. Duration of
effective analgesia was defined as the time interval between onset of SAB and the
time to reach pain score-2 or 3
46
47
9.3 OBSERVATION AND RESULTS
This study was conducted at the institute of Obstetrics and Gynaecology, Egmore,
Chennai. Sixty (60) patients were included in this double blinded randomized
controlled study. The patients were divided into two groups. Patients in Group F
received 3.0ml [15 mg] of 0.5% Hyperbaric Bupivacaine plus 25μg [0.5cc] of Fentanyl
and patients in Group D received 3.0ml [15mg] of 0.5% Hyberbaric Bupivacaine plus
5μg [0.5cc] of Dexmedetomidine (preservative free). Final volume of injected solution
was 3.5cc in both groups.
48
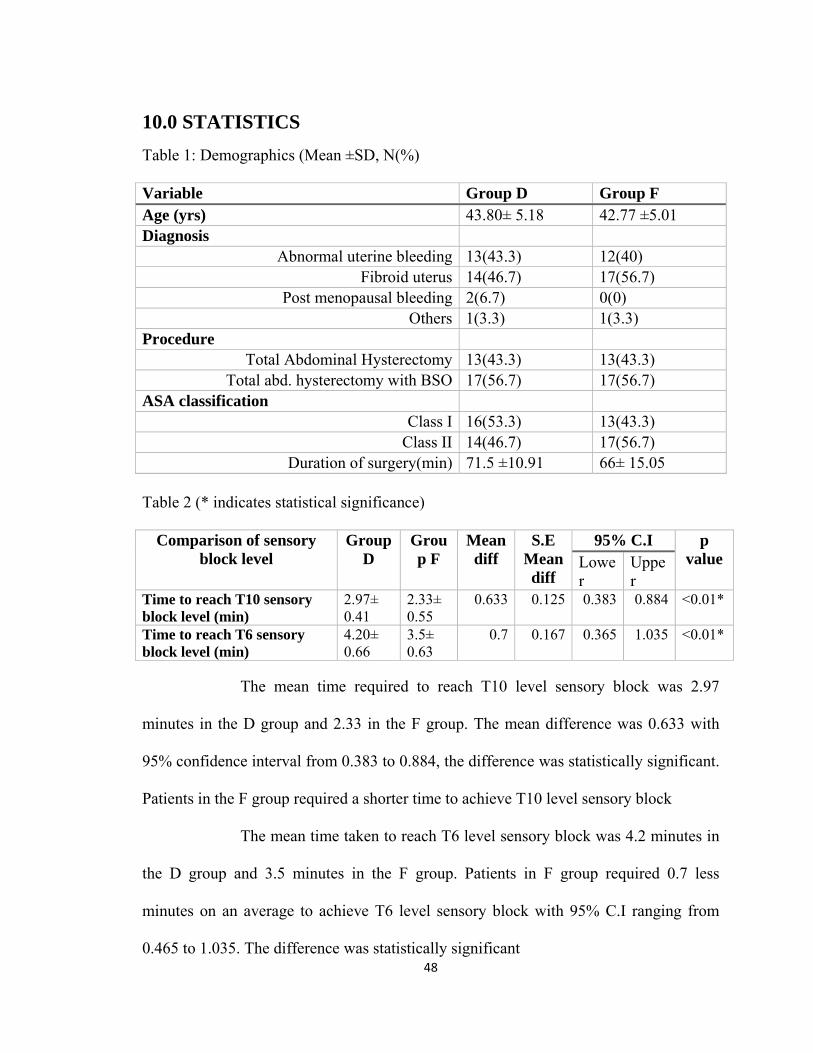
10.0 STATISTICS Table 1: Demographics (Mean ±SD, N(%) Variable Group D Group F Age (yrs) 43.80± 5.18 42.77 ±5.01 Diagnosis
Abnormal uterine bleeding 13(43.3) 12(40) Fibroid uterus 14(46.7) 17(56.7)
Post menopausal bleeding 2(6.7) 0(0) Others 1(3.3) 1(3.3)
Procedure Total Abdominal Hysterectomy 13(43.3) 13(43.3)
Total abd. hysterectomy with BSO 17(56.7) 17(56.7) ASA classification
Class I 16(53.3) 13(43.3) Class II 14(46.7) 17(56.7)
Duration of surgery(min) 71.5 ±10.91 66± 15.05 Table 2 (* indicates statistical significance)
Comparison of sensory block level
Group D
Group F
Mean diff
S.E Mean diff
95% C.I p value Lowe
r Upper
Time to reach T10 sensory block level (min)
2.97± 0.41
2.33± 0.55
0.633 0.125 0.383 0.884 <0.01*
Time to reach T6 sensory block level (min)
4.20± 0.66
3.5± 0.63
0.7 0.167 0.365 1.035 <0.01*
The mean time required to reach T10 level sensory block was 2.97
minutes in the D group and 2.33 in the F group. The mean difference was 0.633 with
95% confidence interval from 0.383 to 0.884, the difference was statistically significant.
Patients in the F group required a shorter time to achieve T10 level sensory block
The mean time taken to reach T6 level sensory block was 4.2 minutes in
the D group and 3.5 minutes in the F group. Patients in F group required 0.7 less
minutes on an average to achieve T6 level sensory block with 95% C.I ranging from
0.465 to 1.035. The difference was statistically significant
49
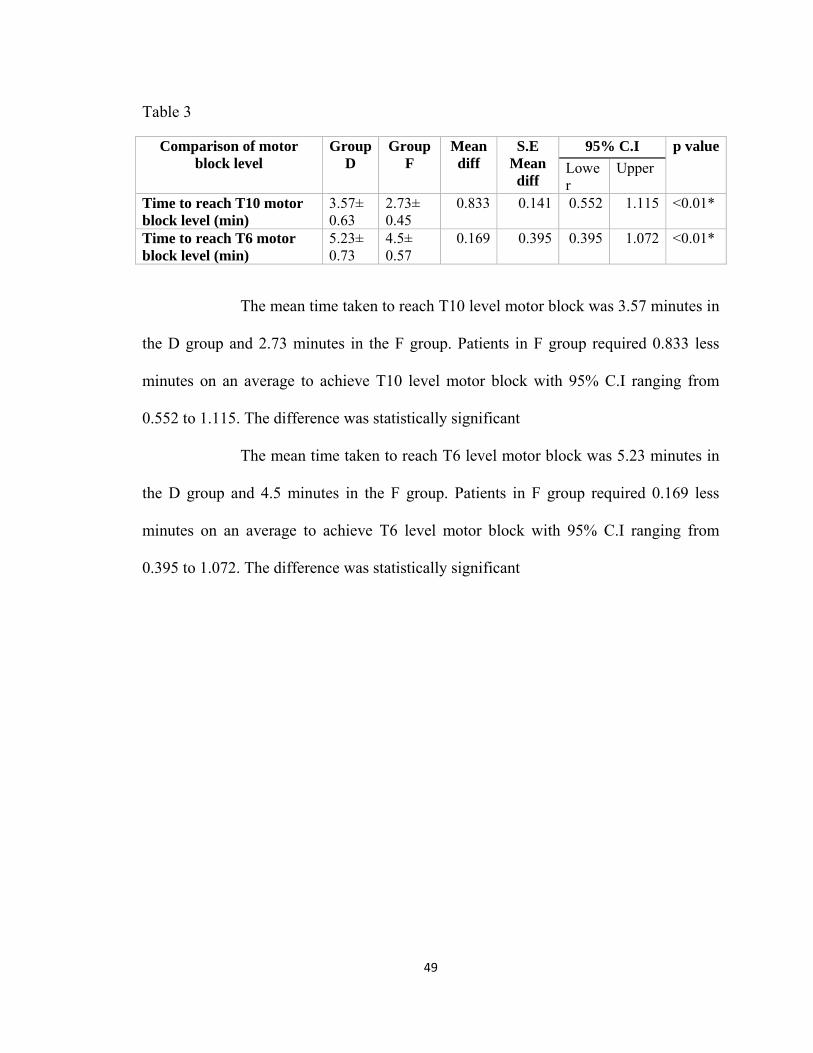
Table 3
Comparison of motor block level
Group D
Group F
Mean diff
S.E Mean diff
95% C.I p value
Lower
Upper
Time to reach T10 motor block level (min)
3.57± 0.63
2.73± 0.45
0.833 0.141 0.552 1.115 <0.01*
Time to reach T6 motor block level (min)
5.23± 0.73
4.5± 0.57
0.169 0.395 0.395 1.072 <0.01*
The mean time taken to reach T10 level motor block was 3.57 minutes in
the D group and 2.73 minutes in the F group. Patients in F group required 0.833 less
minutes on an average to achieve T10 level motor block with 95% C.I ranging from
0.552 to 1.115. The difference was statistically significant
The mean time taken to reach T6 level motor block was 5.23 minutes in
the D group and 4.5 minutes in the F group. Patients in F group required 0.169 less
minutes on an average to achieve T6 level motor block with 95% C.I ranging from
0.395 to 1.072. The difference was statistically significant
50
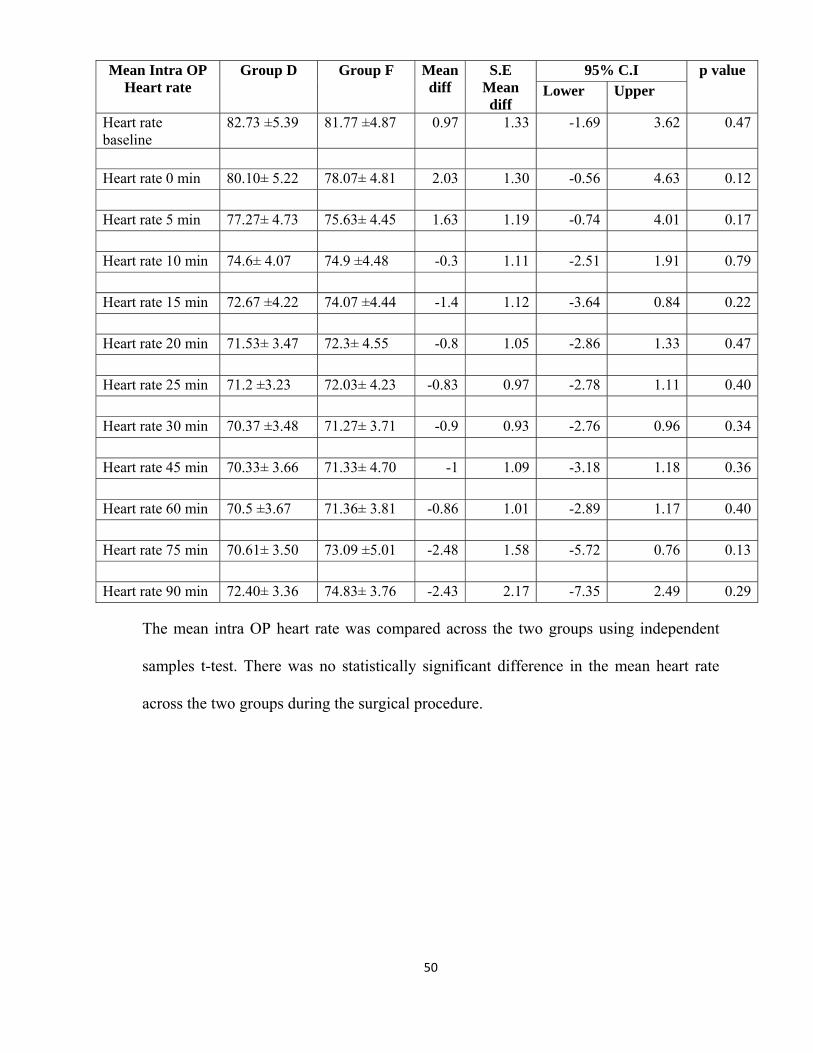
The mean intra OP heart rate was compared across the two groups using independent
samples t-test. There was no statistically significant difference in the mean heart rate
across the two groups during the surgical procedure.
Mean Intra OP Heart rate
Group D Group F Mean diff
S.E Mean diff
95% C.I p value Lower Upper
Heart rate baseline
82.73 ±5.39 81.77 ±4.87 0.97 1.33 -1.69 3.62 0.47
Heart rate 0 min 80.10± 5.22 78.07± 4.81 2.03 1.30 -0.56 4.63 0.12 Heart rate 5 min 77.27± 4.73 75.63± 4.45 1.63 1.19 -0.74 4.01 0.17 Heart rate 10 min 74.6± 4.07 74.9 ±4.48 -0.3 1.11 -2.51 1.91 0.79 Heart rate 15 min 72.67 ±4.22 74.07 ±4.44 -1.4 1.12 -3.64 0.84 0.22 Heart rate 20 min 71.53± 3.47 72.3± 4.55 -0.8 1.05 -2.86 1.33 0.47 Heart rate 25 min 71.2 ±3.23 72.03± 4.23 -0.83 0.97 -2.78 1.11 0.40 Heart rate 30 min 70.37 ±3.48 71.27± 3.71 -0.9 0.93 -2.76 0.96 0.34 Heart rate 45 min 70.33± 3.66 71.33± 4.70 -1 1.09 -3.18 1.18 0.36 Heart rate 60 min 70.5 ±3.67 71.36± 3.81 -0.86 1.01 -2.89 1.17 0.40 Heart rate 75 min 70.61± 3.50 73.09 ±5.01 -2.48 1.58 -5.72 0.76 0.13 Heart rate 90 min 72.40± 3.36 74.83± 3.76 -2.43 2.17 -7.35 2.49 0.29
51
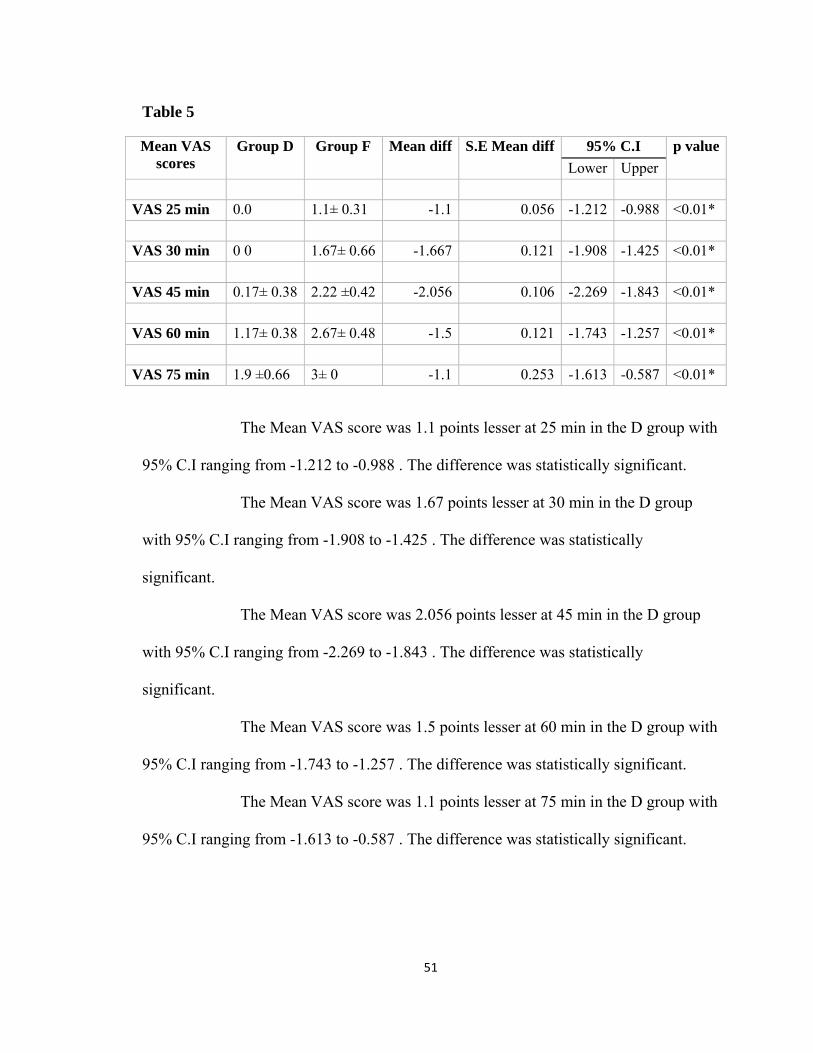
Table 5 Mean VAS
scores Group D Group F Mean diff S.E Mean diff 95% C.I p value
Lower Upper VAS 25 min 0.0 1.1± 0.31 -1.1 0.056 -1.212 -0.988 <0.01* VAS 30 min 0 0 1.67± 0.66 -1.667 0.121 -1.908 -1.425 <0.01* VAS 45 min 0.17± 0.38 2.22 ±0.42 -2.056 0.106 -2.269 -1.843 <0.01* VAS 60 min 1.17± 0.38 2.67± 0.48 -1.5 0.121 -1.743 -1.257 <0.01* VAS 75 min 1.9 ±0.66 3± 0 -1.1 0.253 -1.613 -0.587 <0.01*
The Mean VAS score was 1.1 points lesser at 25 min in the D group with
95% C.I ranging from -1.212 to -0.988 . The difference was statistically significant.
The Mean VAS score was 1.67 points lesser at 30 min in the D group
with 95% C.I ranging from -1.908 to -1.425 . The difference was statistically
significant.
The Mean VAS score was 2.056 points lesser at 45 min in the D group
with 95% C.I ranging from -2.269 to -1.843 . The difference was statistically
significant.
The Mean VAS score was 1.5 points lesser at 60 min in the D group with
95% C.I ranging from -1.743 to -1.257 . The difference was statistically significant.
The Mean VAS score was 1.1 points lesser at 75 min in the D group with
95% C.I ranging from -1.613 to -0.587 . The difference was statistically significant.
52
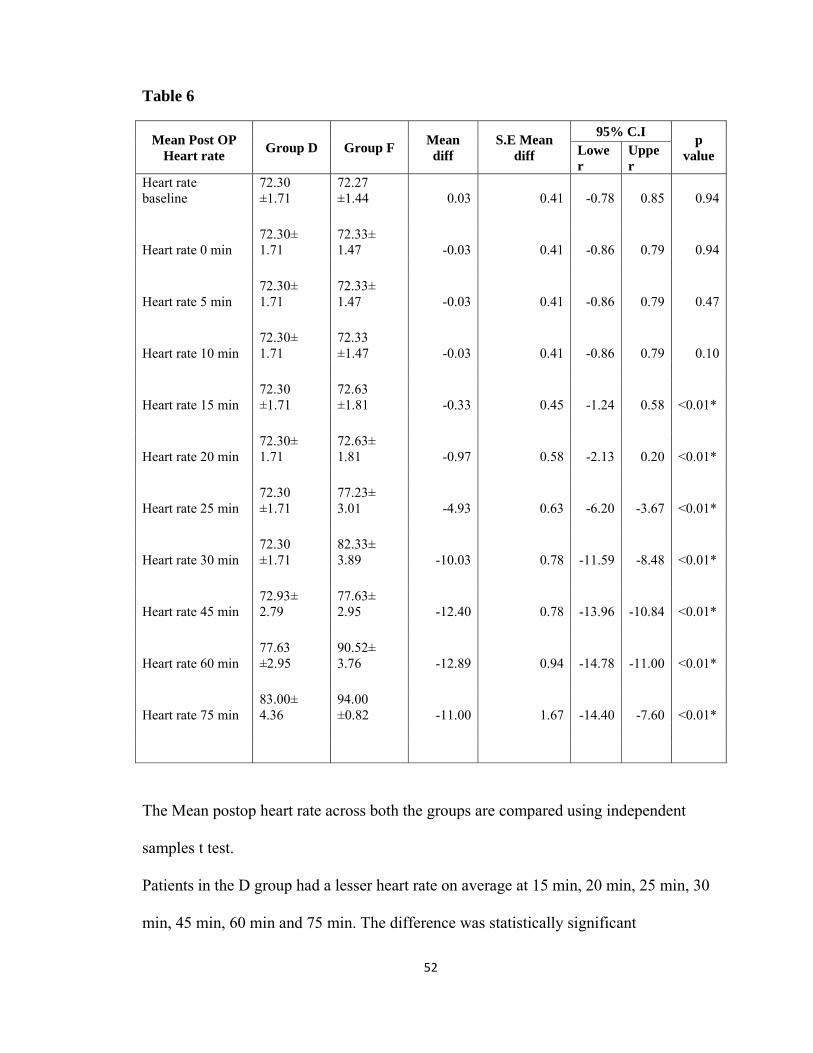
Table 6
Mean Post OP Heart rate
Group D Group F Mean diff
S.E Mean diff
95% C.I p
value Lower
Upper
Heart rate baseline
72.30 ±1.71
72.27 ±1.44 0.03 0.41 -0.78 0.85 0.94
Heart rate 0 min 72.30± 1.71
72.33± 1.47 -0.03 0.41 -0.86 0.79 0.94
Heart rate 5 min 72.30± 1.71
72.33± 1.47 -0.03 0.41 -0.86 0.79 0.47
Heart rate 10 min 72.30± 1.71
72.33 ±1.47 -0.03 0.41 -0.86 0.79 0.10
Heart rate 15 min 72.30 ±1.71
72.63 ±1.81 -0.33 0.45 -1.24 0.58 <0.01*
Heart rate 20 min 72.30± 1.71
72.63± 1.81 -0.97 0.58 -2.13 0.20 <0.01*
Heart rate 25 min 72.30 ±1.71
77.23± 3.01 -4.93 0.63 -6.20 -3.67 <0.01*
Heart rate 30 min 72.30 ±1.71
82.33± 3.89 -10.03 0.78 -11.59 -8.48 <0.01*
Heart rate 45 min 72.93± 2.79
77.63± 2.95 -12.40 0.78 -13.96 -10.84 <0.01*
Heart rate 60 min 77.63 ±2.95
90.52± 3.76 -12.89 0.94 -14.78 -11.00 <0.01*
Heart rate 75 min 83.00± 4.36
94.00 ±0.82 -11.00 1.67 -14.40 -7.60 <0.01*
The Mean postop heart rate across both the groups are compared using independent
samples t test.
Patients in the D group had a lesser heart rate on average at 15 min, 20 min, 25 min, 30
min, 45 min, 60 min and 75 min. The difference was statistically significant
53
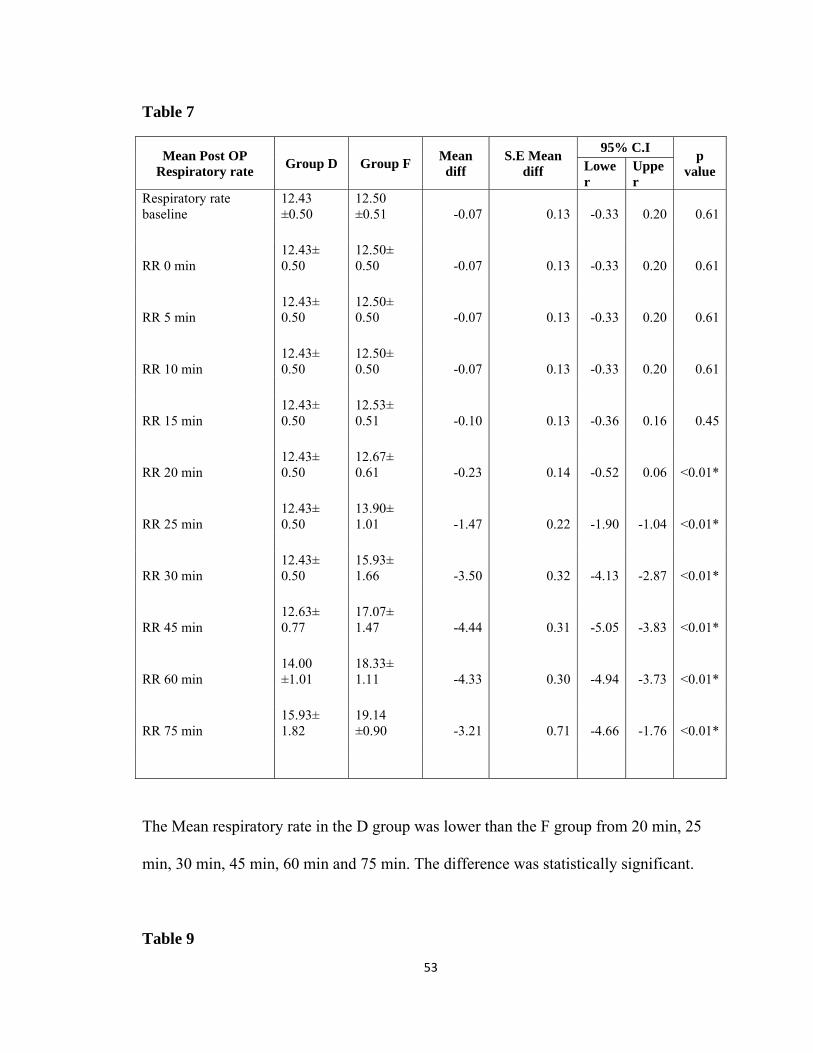
Table 7
Mean Post OP Respiratory rate
Group D Group F Mean diff
S.E Mean diff
95% C.I p
value Lower
Upper
Respiratory rate baseline
12.43 ±0.50
12.50 ±0.51 -0.07 0.13 -0.33 0.20 0.61
RR 0 min 12.43± 0.50
12.50± 0.50 -0.07 0.13 -0.33 0.20 0.61
RR 5 min 12.43± 0.50
12.50± 0.50 -0.07 0.13 -0.33 0.20 0.61
RR 10 min 12.43± 0.50
12.50± 0.50 -0.07 0.13 -0.33 0.20 0.61
RR 15 min 12.43± 0.50
12.53± 0.51 -0.10 0.13 -0.36 0.16 0.45
RR 20 min 12.43± 0.50
12.67± 0.61 -0.23 0.14 -0.52 0.06 <0.01*
RR 25 min 12.43± 0.50
13.90± 1.01 -1.47 0.22 -1.90 -1.04 <0.01*
RR 30 min 12.43± 0.50
15.93± 1.66 -3.50 0.32 -4.13 -2.87 <0.01*
RR 45 min 12.63± 0.77
17.07± 1.47 -4.44 0.31 -5.05 -3.83 <0.01*
RR 60 min 14.00 ±1.01
18.33± 1.11 -4.33 0.30 -4.94 -3.73 <0.01*
RR 75 min 15.93± 1.82
19.14 ±0.90 -3.21 0.71 -4.66 -1.76 <0.01*
The Mean respiratory rate in the D group was lower than the F group from 20 min, 25
min, 30 min, 45 min, 60 min and 75 min. The difference was statistically significant.
Table 9

54
Mean Intra OP MAP
Group D Group F Mean diff S.E Mean diff95% C.I
p value Lower Upper
MAP baseline 98.24 ±4.51 94.03 ±7.22 4.21 1.56 1.10 7.33 <0.01*
MAP 0 min 94.82± 4.21 90.7± 6.27 4.08 1.38 1.31 6.84 <0.01*
MAP 5 min 90.02± 2.36 86.55± 5.64 3.47 1.12 1.23 5.70 <0.01*
MAP 10 min 87.17± 3.50 83.01 ±6.60 4.17 1.37 1.43 6.90 <0.01*
MAP 15 min 84.04 ±3.33 80.03 ±5.62 4.01 1.19 1.62 6.40 <0.01*
MAP 20 min 82.06± 79.26 79.26± 5.94 2.80 1.35 0.10 5.50 <0.01*
MAP25 min 80.84±5.29 80.28± 5.48 0.56 1.37 -2.18 3.29 0. 69
MAP 30 min 79.91 ±4.24 81.74± 5.35 -1.83 1.25 -4.33 0.66 0.15
MAP 45 min 80.52± 4.09 79.82± 4.11 0.70 1.11 -1.53 2.92 0.53
MAP 60 min 80.84 ±5.09 79.96± 5.55 0.87 1.84 -2.84 4.59 0.64
MAP 75 min 81.14± 4.08 80.38 ±3.85 0.76 1.90 -3.19 4.71 0.69 The mean intra operative Mean arterial pressure across both the group are compared
using independent samples t test. Patients in the D group had a higher MAP on average
at baseline, 0 min, 5 min, 10 min, 15 min, 20 min. The difference was statistically
significant. There was no significant difference in the intraoperative MAP during 25
min, 30 min, 45 min, 60 min and 75 min
55
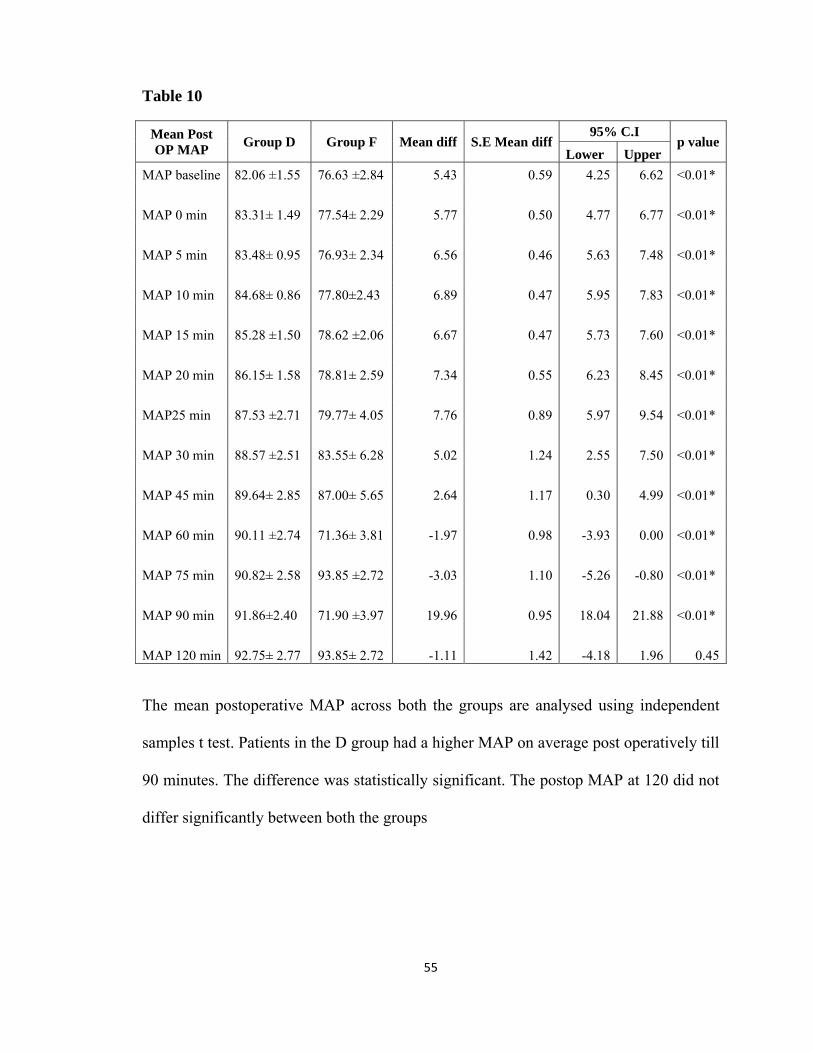
Table 10
Mean Post OP MAP
Group D Group F Mean diff S.E Mean diff95% C.I
p valueLower Upper
MAP baseline 82.06 ±1.55 76.63 ±2.84 5.43 0.59 4.25 6.62 <0.01*
MAP 0 min 83.31± 1.49 77.54± 2.29 5.77 0.50 4.77 6.77 <0.01*
MAP 5 min 83.48± 0.95 76.93± 2.34 6.56 0.46 5.63 7.48 <0.01*
MAP 10 min 84.68± 0.86 77.80±2.43 6.89 0.47 5.95 7.83 <0.01*
MAP 15 min 85.28 ±1.50 78.62 ±2.06 6.67 0.47 5.73 7.60 <0.01*
MAP 20 min 86.15± 1.58 78.81± 2.59 7.34 0.55 6.23 8.45 <0.01*
MAP25 min 87.53 ±2.71 79.77± 4.05 7.76 0.89 5.97 9.54 <0.01*
MAP 30 min 88.57 ±2.51 83.55± 6.28 5.02 1.24 2.55 7.50 <0.01*
MAP 45 min 89.64± 2.85 87.00± 5.65 2.64 1.17 0.30 4.99 <0.01*
MAP 60 min 90.11 ±2.74 71.36± 3.81 -1.97 0.98 -3.93 0.00 <0.01*
MAP 75 min 90.82± 2.58 93.85 ±2.72 -3.03 1.10 -5.26 -0.80 <0.01*
MAP 90 min 91.86±2.40 71.90 ±3.97 19.96 0.95 18.04 21.88 <0.01*
MAP 120 min 92.75± 2.77 93.85± 2.72 -1.11 1.42 -4.18 1.96 0.45 The mean postoperative MAP across both the groups are analysed using independent
samples t test. Patients in the D group had a higher MAP on average post operatively till
90 minutes. The difference was statistically significant. The postop MAP at 120 did not
differ significantly between both the groups
56
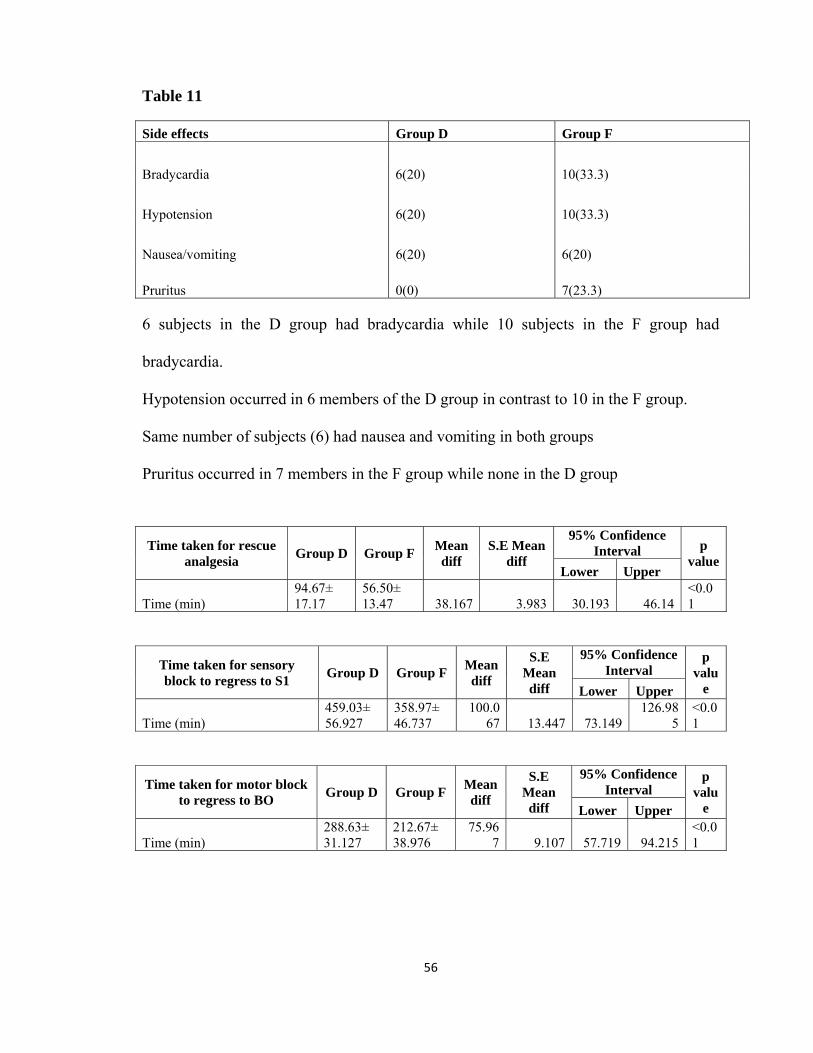
Table 11
Side effects Group D Group F
Bradycardia 6(20) 10(33.3)
Hypotension 6(20) 10(33.3)
Nausea/vomiting 6(20) 6(20)
Pruritus 0(0) 7(23.3) 6 subjects in the D group had bradycardia while 10 subjects in the F group had
bradycardia.
Hypotension occurred in 6 members of the D group in contrast to 10 in the F group.
Same number of subjects (6) had nausea and vomiting in both groups
Pruritus occurred in 7 members in the F group while none in the D group
Time taken for rescue analgesia
Group D Group F Mean diff
S.E Mean diff
95% Confidence Interval p
valueLower Upper
Time (min) 94.67± 17.17
56.50± 13.47 38.167 3.983 30.193 46.14
<0.01
Time taken for sensory block to regress to S1
Group D Group F Mean diff
S.E Mean diff
95% Confidence Interval
p valu
e Lower Upper
Time (min) 459.03± 56.927
358.97± 46.737
100.067 13.447 73.149
126.985
<0.01
Time taken for motor block to regress to BO
Group D Group F Mean diff
S.E Mean diff
95% Confidence Interval
p valu
e Lower Upper
Time (min) 288.63± 31.127
212.67± 38.976
75.967 9.107 57.719 94.215
<0.01
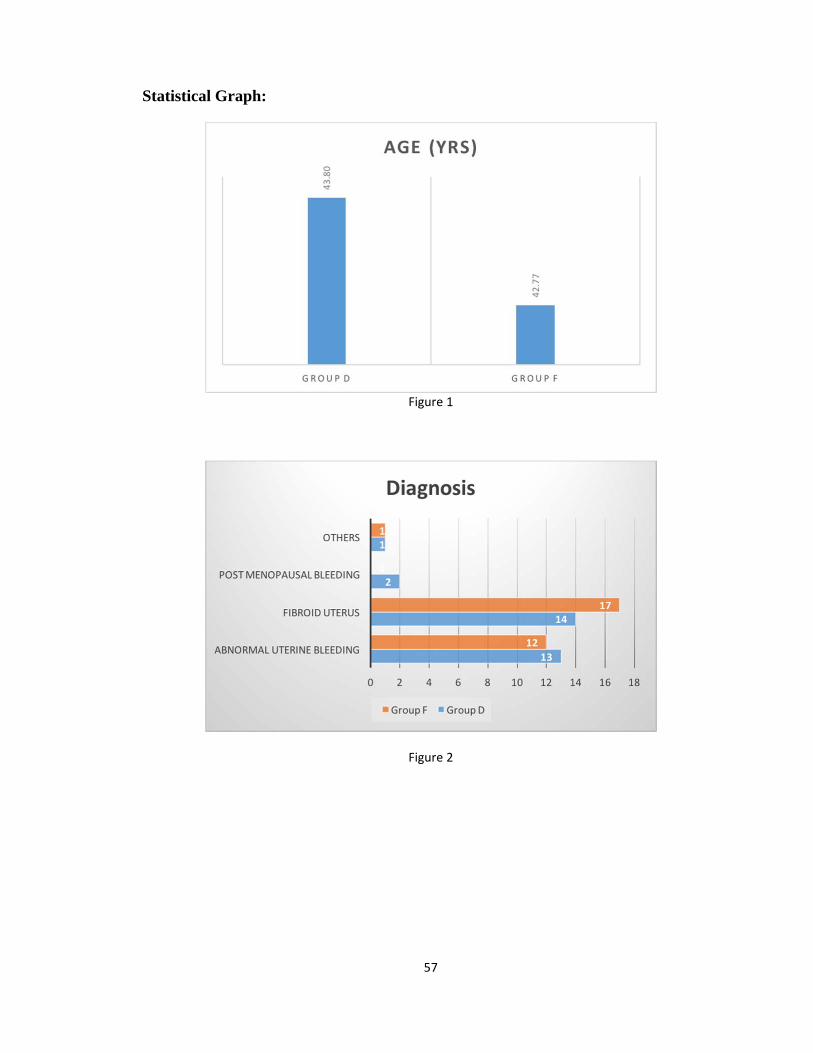
57
Statistical Graph:
Figure 1
Figure 2

58
Figure 3
Figure 4

59
Figure 5
Figure 6
Time taken for rescue analgesia
Group D Group F Mean diff S.E Mean
diff
95% Confidence Interval p value
Lower Upper
Time (min) 94.67± 17.17 56.50± 13.47 38.167 3.983 30.193 46.14 <0.01
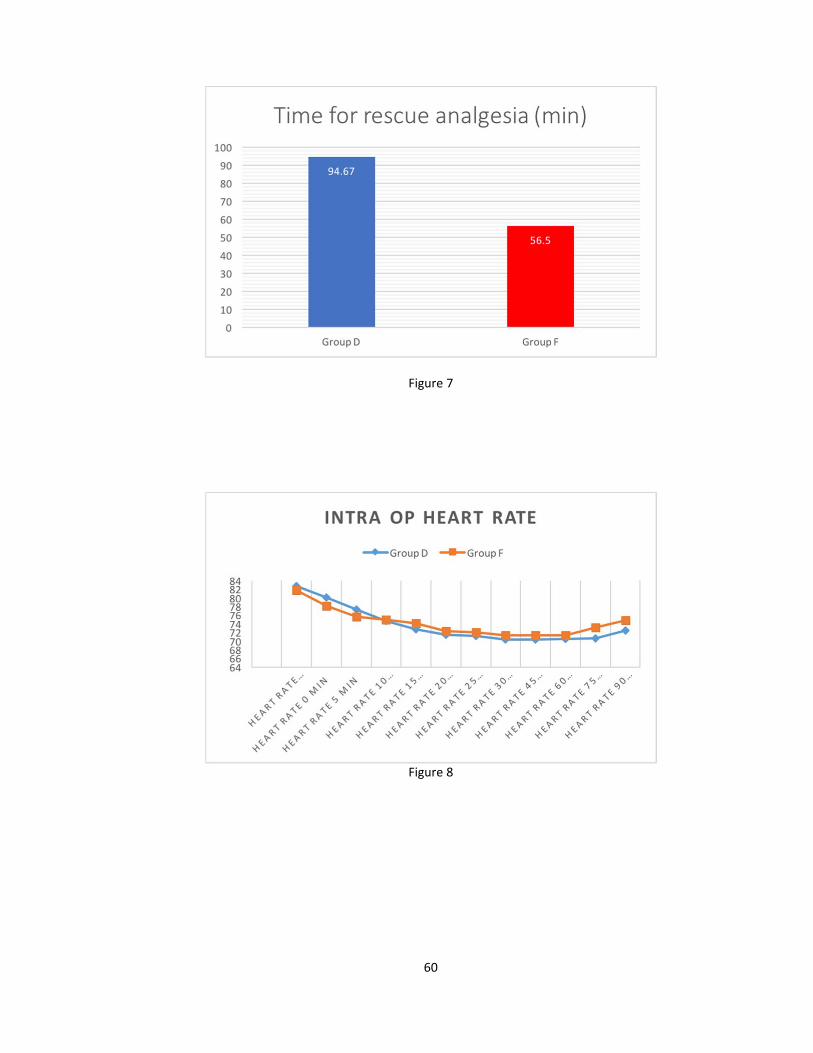
60
Figure 7
Figure 8
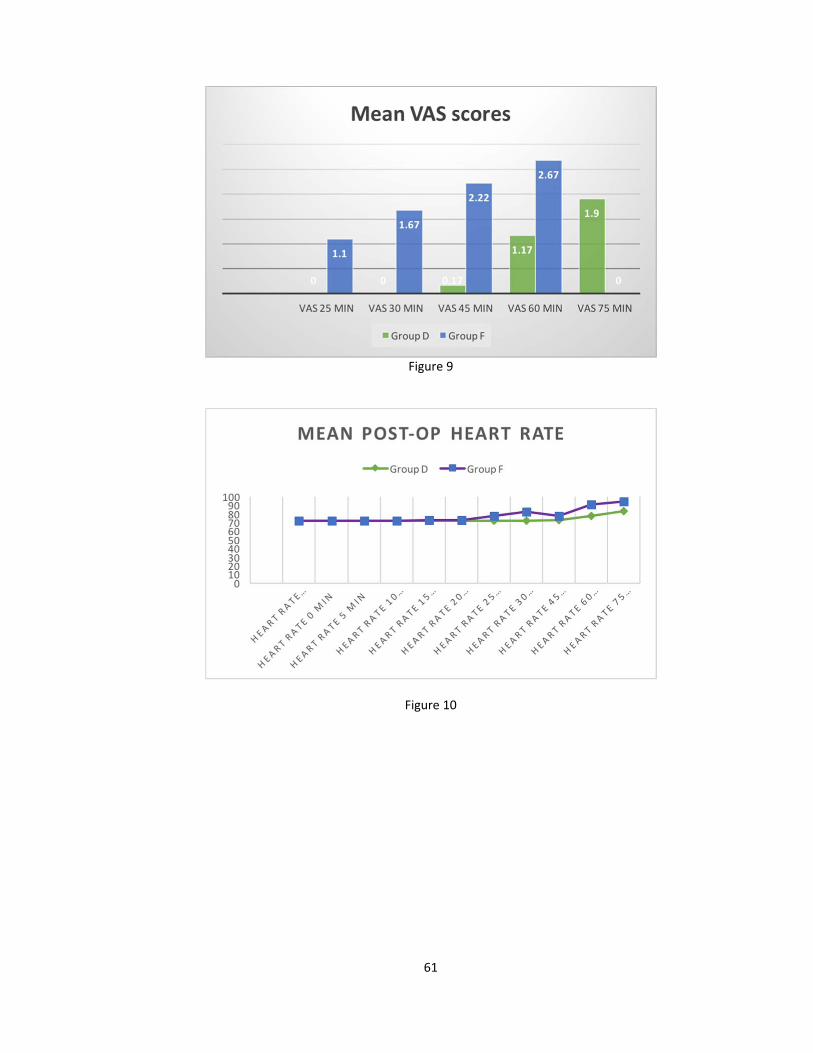
61
Figure 9
Figure 10
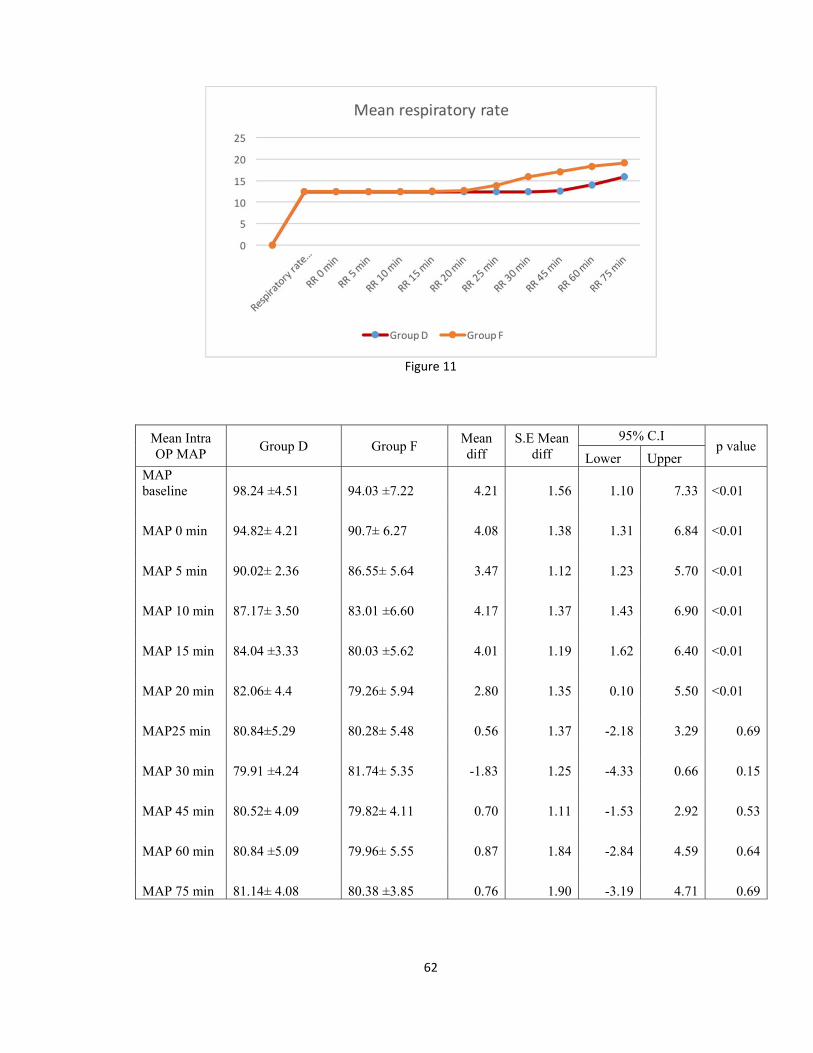
62
Figure 11
Mean Intra OP MAP
Group D Group F Mean diff
S.E Mean diff
95% C.I p value
Lower Upper MAP baseline 98.24 ±4.51 94.03 ±7.22 4.21 1.56 1.10 7.33 <0.01
MAP 0 min 94.82± 4.21 90.7± 6.27 4.08 1.38 1.31 6.84 <0.01
MAP 5 min 90.02± 2.36 86.55± 5.64 3.47 1.12 1.23 5.70 <0.01
MAP 10 min 87.17± 3.50 83.01 ±6.60 4.17 1.37 1.43 6.90 <0.01
MAP 15 min 84.04 ±3.33 80.03 ±5.62 4.01 1.19 1.62 6.40 <0.01
MAP 20 min 82.06± 4.4 79.26± 5.94 2.80 1.35 0.10 5.50 <0.01
MAP25 min 80.84±5.29 80.28± 5.48 0.56 1.37 -2.18 3.29 0.69
MAP 30 min 79.91 ±4.24 81.74± 5.35 -1.83 1.25 -4.33 0.66 0.15
MAP 45 min 80.52± 4.09 79.82± 4.11 0.70 1.11 -1.53 2.92 0.53
MAP 60 min 80.84 ±5.09 79.96± 5.55 0.87 1.84 -2.84 4.59 0.64
MAP 75 min 81.14± 4.08 80.38 ±3.85 0.76 1.90 -3.19 4.71 0.69
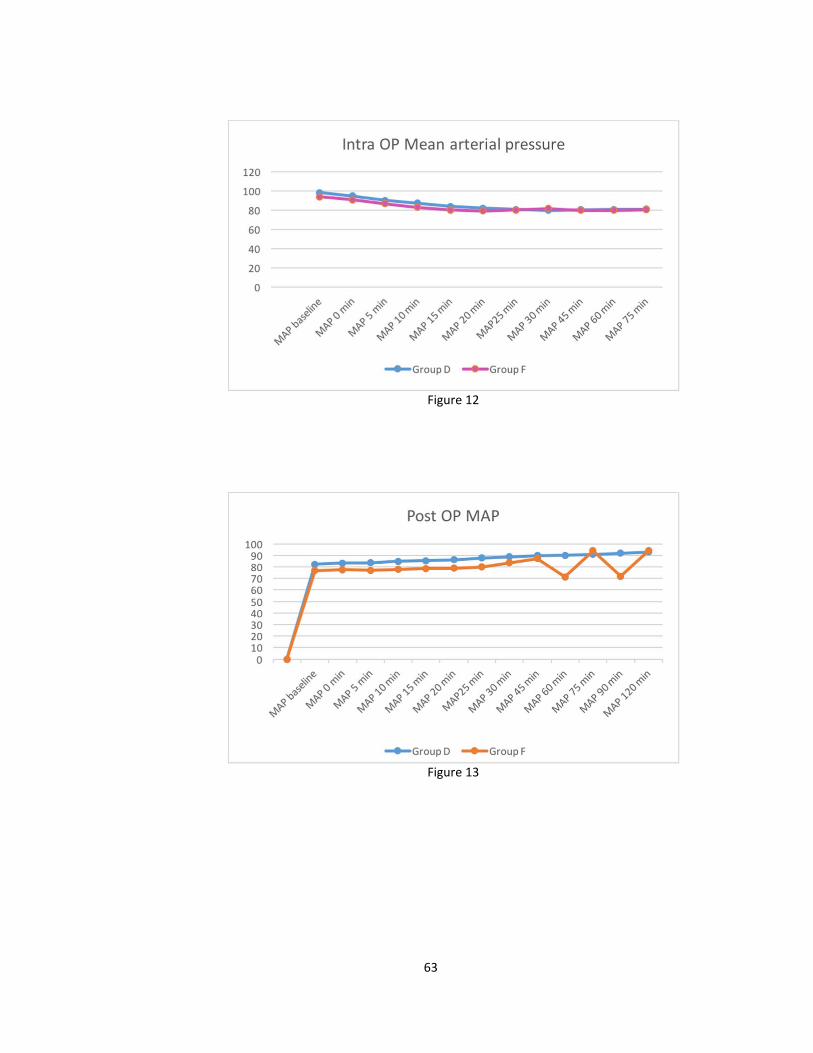
63
Figure 12
Figure 13
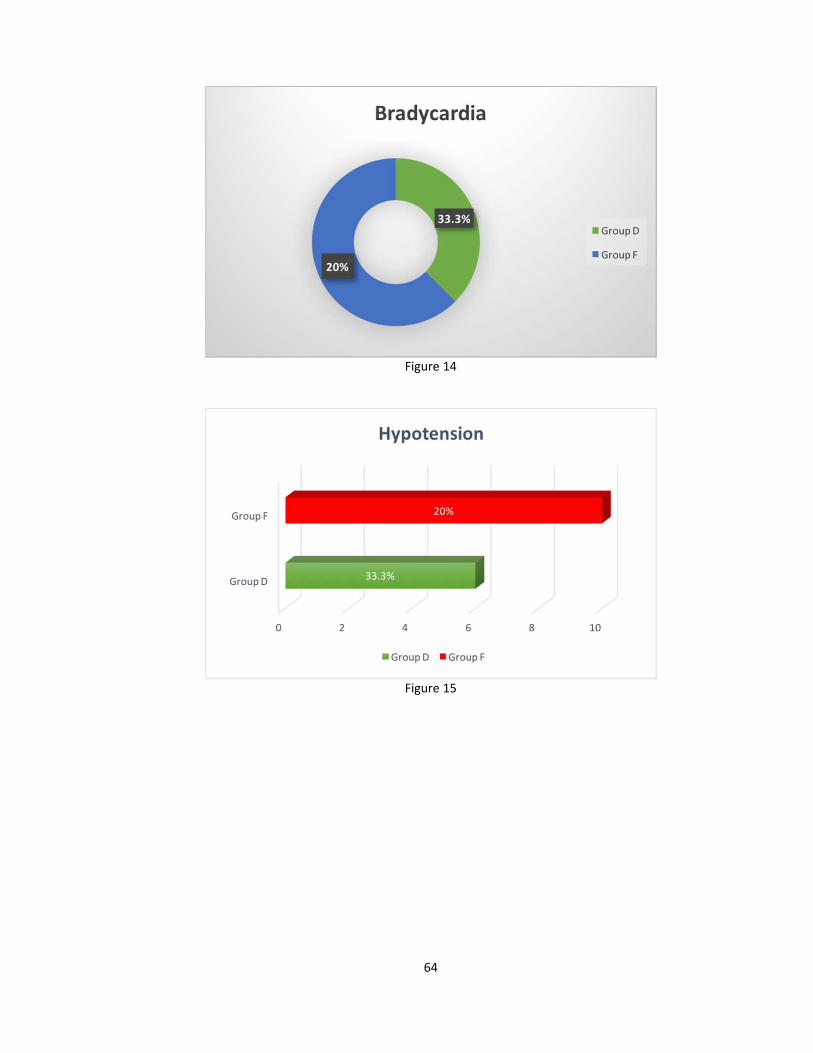
64
Figure 14
Figure 15
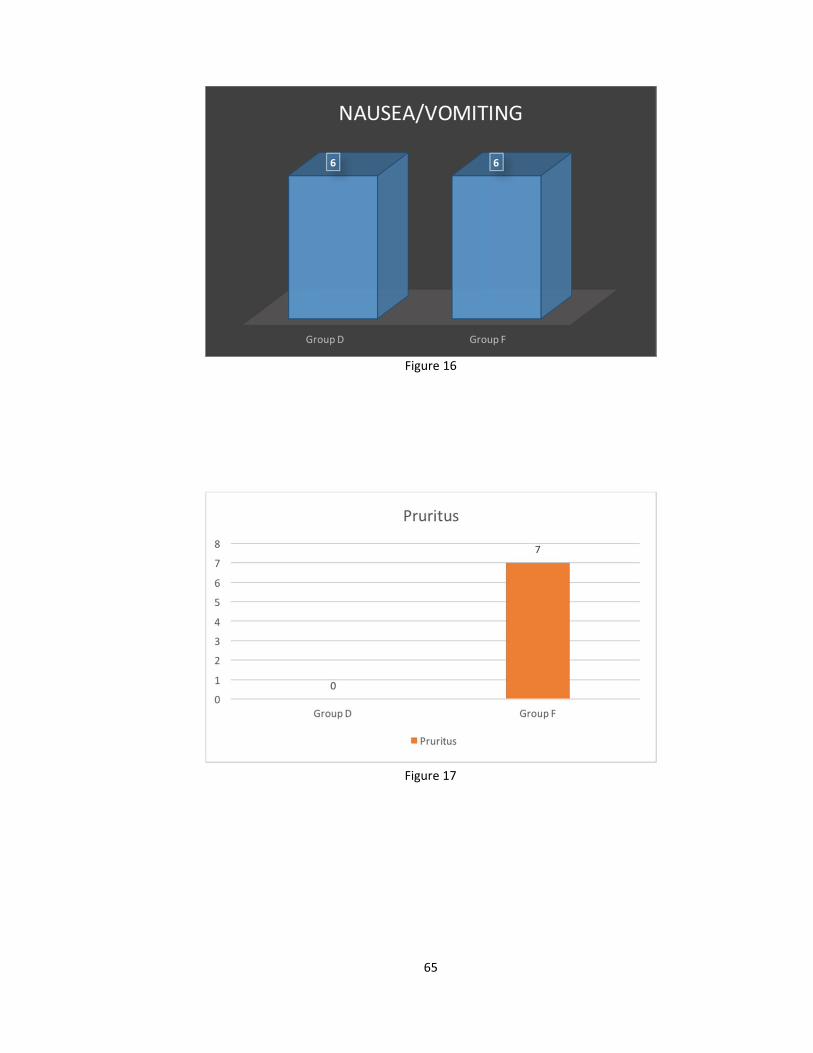
65
Figure 16
Figure 17
66
10.1 DISCUSSION Subarachnoid Block is a commonly used anaesthetic technique for lower
abdominal surgeries.Additives to spinal local anaesthetics Alpha2 agonist like
Dexmedetomidine have been shown to prolong the duration of both sensory and
motor blockade and to provide extended postop analgesia.
In this study 5μg of Dexmedetomidine was added to 15mg [3.0ml] of 0.5%
Hyperbaric Bupivacaine or 25μg of fentanyl added to 15mg [3.0ml] of 0.5%
Hyperbaric Bupivacaine and its efficacy as an adjuvant to subarachanoid Bupivacaine
was studied in 60 patients undergoing elective total abdominal hysterectomy.
ONSET OF SENSORY BLOCK
The mean time to onset of sensory Block (T10 level) was 2.97mins in the
Group D and 2.33 in theGroup F. patients in the F group required a shorter time to
achieve T10 level sensory block.
Subhi M Al-Ghanem et al. who compared the effect of 5μg Dexmedetomidine
Vs fentanyl 25μg in intra operative analgesia and the duration of sensory & motor
block when added to 10mg intrathecal plain Bupivacaine and observed that there
is no statistically significant difference between the two groups as regards to the
onset time of sensory block at T10 level.
Ibrahim F.a. Khalifa et al did a comparative study of adding intrathecal 5μg
Dexmedetomedine and 5μg of sufentanyl to 10mg of heavy Bupivacaine found that
there is no statistically significant difference in the onset of sensory block T10 level
Group D = 5.5±3.7, where Group 57 = 6.2±1.3 p < 0.69.
67
MAXIMUM LEVEL OF SENSORY BLOCK The mean time taken to reach T6 level sensory block was 4.2mins in the Group
D and 3.5mins in the Group F. patients in Fgroup required 0.7less minutes on an
average to achieveT6 level sensory block.Kanazi et al found that there is statistically
no significant difference for the maximal sensory Block for 12mg Bupivacaine
0.5% alone or combined 3μg of Dexmedetomidine or 30μg of clonidine [p = 0.3].
Mahmoud M. Al Mustafa et al found that addition of intrathecal
Dexmedetomidine in increasing doses 5μg, 10mg of Dexmedetomidine with
12.5mg of Spinal Bupivacaine increased the level of sensory block as the dose
of Dexmedetomidine increases.
Ibrahim F.A. Khalifa et al found that there is statistically no significant
difference for the maximal sensory block when compared with 5μg of
Dexmedetomedine and 5μg of sufentanyl to 10mg of heavy Bupivacaine
The study Subhi M. Al Ghanem et al who found that addition of 5μg of
Dexmedetomidine and 25μg of fentanyl with 10mg of isobaric Bupivacaine
intrathecally had no significant difference on the mean time to reach peak sensory
level 19.34 ± 2.87 in Group D and 18.39 ± 2.46 in Group F p = 0.12.
ONSET OF MOTOR BLOCK
The mean time taken to reach T10 level motor block was 3 . 5 7 mins in the
Group D and 2.73 mins in the Group F. Patients in Fgroup required 0.833 less
minutes on an average to achieve T10 level motor block. Ibrahim F. A. Khalifa et al
found that there is statistically no significant difference with 5μg of
Dexmedetomidine and 5μg of sufentanyl to 10mg of heavy Bupivacaine on the
mean time to achieve bromage 3 score.
68
DURATION OF SENSORY BLOCK
In our study the duration of sensory block was 358.97 ± 46.74 mins in Group F
and 459.03 ± 56.93 mins. The addition of 5μg of Dexmedetomidine to Hyperbaric
Bupivacaine significantly prolonged the duration of sensory block. [Intrathecal
Dexmedetomidine when combined with spinal Bupivacaine prolongs the sensory block
by depressing the release of c-fibres transmitters and by hyperolarization of post-
synaptic dorsal horn neurons].
This correlated with the study
• Subhi M. Al-Ghanem et al found that the addition of 5μg of
Dexmedetomidine to 10mg of isobaric Bupivacaine 274.83 ± 73.4
significantly prolong the duration of sensory blockade while 25μg of
fentanyl to 10mg of isobaric Bupivacaine was 179.5±47.4. There was
statistically significant difference among the two groups p < 0.00
[Intrathecal Dexmedetomidine when combined with spinal Bupivacaine
prolongs the sensory block by depressing the release of c-fibers
transmitters and by hyperpolarization of post-synaptic dorsal horn
neurons].
• Kanazi et al found that the addition of 3μg of Dexmedetomidine to 12mg of
intrathecal Bupivacaine or 30μg of clonidine significantly prolonged the
sensory block.
• Al Mustafa MM et al studied that there is a significant difference in the
duration of sensory block among three groups who received spinal
Bupivacaine 12.5mg alone or combined with 5μg of Dexmedetomidine or

69
with 10μg of Dexmedetomidine. He concluded that Dexmedetomidine has
a dose dependent effect on the onset and regression of sensory and motor
block when used in SAB.
DURATION OF MOTOR BLOCK
In our study the mean duration of motor block was 212.67 ± 38.976 mins in
Group F and 288.63 ± 31.12 mins in Group D. The addition of 5μg of
Dexmedetomidine to 0.5% Bupivacaine significantly prolonged the duration of motor
block.
• Subi M. Al-Ghanem et al found in their study that 5μg of
Dexmedetomidine to 0.5% hyperbaric Bupivacaine prolonged effect of
motor blockade than 25μg of fentanyl to 0.5% hyperbaric Bupivacaine
intrathecally.
• Kanazi et al observed that addition of 12mg of Bupivacaine
supplemented with dexmedetomidine and 12mg of Bupivacaine with
30μg of clonidine intrathecally produces similar prolongation in the
duration of motor block when compared 12mg of Bupivacaine alone.
[The prolongation of motor block produced by subarachnoid Hyperbaric
Bupivacaine combined with 5μg of Dexmedetomidine results from
binding these agonist to motor neurons in the dorsal horn of the spinal
cord].
• Mahmoud M. Al Mustafa et al found that Dexmedetomidine has a dose
dependent effect on the duration of motor blockade when added to

70
• Ibrahim F.A Khalifa et al found that the addition of 5μg of
Dexmedetomidine to 2ml of heavy Bupivacaine and 5μg of sufentanyl to
2ml of heavy bupieracaine produces a significant difference in the
duration of motor blockade.
Quality of Surgical anaesthesia The quality of surgical anaesthesia was excellent in both groups. Though studies have shown
• Ibrahim F.A. Khalifa et al found that the quality of surgical anaesthesia
was better in patients received 5μg sufentanyl to 2ml of heavy
Bupivacaine when compared to 5μg of Dexmedetomidine to 2ml of heavy
Bupivacaine
DURATION OF ANALGESIA
In our study the mean time for Rescue analgesia is 56.50 mins in Group F and
94.67 ± 17.17mins which was statistically significant difference in the duration of
analgesia by two groups
Though studies have shown Ibrahim F.A. Khalifa et al found that the addition of 5μg of Dexmedetomidine to
10mg of Hyperbaric Bupivacaine and 5μg of sufentanyl to 10mg of Hyperbaric
Bupivacaine intrathecally produces no significant difference in the duration of pain
relief Group SF = 265.8 ± 112.3, Group D = 240. 2±77.3 mins [p < 08].
71
Complications
In our study the incidence of Hypotension was in 10 subjects in Group F and
6subjects in Group D. The most significant side effects reported about the use of
intrathecal α2 adrenoreceptor agonists are Bradycardia and hypotension. But in
present study these side effects were not significant because small dose of intrathecal
Dexmedetomidine was used.
This correlated with the study
• Kanazi et al studied that the addition of Dexmedetomidine or clonidine to
Bupivacaine did not cause a significant decrease in the Blood pressure
intraoperatively or postoperatively. Intrathecal local anaesthetics block
the sympathetic outflow and reduce the blood pressure. The sympathetic
block is usually near-maximal with the doses used for spinal anaesthesia.
The addition of a low dose of α2 agonist to a high dose of local
anaesthetics does not further affect the near maximal sympatholysis.
• Ibrahim F.A. Khalifa et al found that the addition of 5μg of
Dexmedetomidine to spinal Bupivacaine and 5μg of sufentanyl to spinal
Bupivacaine did not produce a significant difference in the incidence of
hypotension.
• Subi M. Al-Ghanem found that hypotension was more in fentanyl group
than in the Dexmedetomidine group but it did not reach a significant
difference. Mean while, hypotension occurred 25-30 minutes after spinal
injection in 2 patients in the Dexmedetomidine group and one patient in
fentanyl group had mild episodes of Hypotension in PACU.
72
The incidence of brady cardia was in6 subjects Group D and in10 subjects in Group
F .
Ibrahim F.A. Khalifa et al found that there is statistically no significantly
difference in the incidence of Bradycardia in both the groups with 5μg of
sufentanyl to 10mg of 0.5% Bupivacaine and 5μg of Dexmedetomidine to
10mg of 0.5% Bupivacaine.
Subi-M-Al-Ghanem et al found that there is statistically no significant
difference in the incidence of Brady cardia among two groups of 5μg of
Dexmedetomidine to 10mg of isobaric Bupivacaine and 25μg of fentanyl to
10mg of isobaric Bupivacaine intrathecally.
The incidence of pruritus was in 7 subjects in Group F and none in Group D. There
is statistically significant difference among two groups.
This correlates with the study
Ibrahim F.A. Khalifa et al found that there is significant difference in the
incidence of pruritus in the sufentanyl group.
Subi M. Al. Ghanem found that there is statistically significant difference in the
incidence of pruritus. Pruritus after intrathecal fentanyl is reported to be 40-
70% but if was only 13% in present study which can be explained by the fact
that pruritus is a benign subjective symptom which is under reporting and
usually needs to treatment
Bogra J. Srivastara P et al found there is statistically significant difference
in the incidence of pruritus with 10mg of fentanyl, 12.5mg of fentanyl, added
to hyperbaric Bupivacaine.
73
The incidence of vomiting, sedation, was not statistically significant in both the groups.
This correlated with the study
Kanazi et al found that intrathecally administrated α2 agonist have a dose-
dependent sedative effect (36,37). The doses of clonidine and
dexmedotomedine selected in their study were at the lower end of the
dosing spectrum. This explains the lack of sedative effects between the study
groups B and C and the intraoperative anxiety one patient in Group D.

74
10.2 SUMMARY
This double blinded prospective randomized controlled trial was designed to
evaluate the onset and duration of sensory and motor block as well as operative
analgesia and adverse effects of Dexmedetomidine vs fentanyl given intrathecally
with heavy 0.5% Bupivacaine for spinal anaesthesia in patients scheduled for total
abdominal hysterectomy, patients receiving 25μg of fentanyl with 3.0cc of
Bupivacaine intrathecally served as the control.
The Following observations were made:
The addition of Dexmedetomidine significantly prolonged the duration of
sensory and motor block.
The addition of Dexmedetomidine significantly prolonged the time for
demand analgesia.
The addition of Dexmedetomidine intrathecally prolonged onset of sensory
or motor block when compared with fentanyl.
The incidence of side effects was limited to the occurence of Hypotension,
Bradycardia in the groups that received Dexmedetomidine intrathecally.
The incidence of pruritus were more in the groups that received fentanyl
intrathecally.
The addition of Dexmedetomidine intrathecally had similar effect on
sedation when compared to fentanyl.

75
10.3 CONCLUSION
Intrathecal Dexmedetomidine supplementation of spinal block seems to be a
good alternative to intrathecal fentanyl since it produces prolonged sensory block and
motor block. It is evident that this type of block may be more suitable for lower
abdomen and lower extremities surgeries.
A drawback of Dexmedetomidine supplemented spinal block characteristics is the
increase in the duration of motor block which may not suit short term surgical
procedures or ambulatory surgery.
11.0 BIBLIOGRAPHY
1. Bogra, J., Srivastava, P., et. al., Studied the Synergistic Effect
of Intrathecal Fentanyl and Bupivacaine in Spinal Anaesthesia for
LSCS BMC Anaesthesiology 2005 May 17; 5(1); 5.
2. Eisanach J.C. [1996] ; Dekock M. Klimscha W. α2 Adrenergic
Agonists for Reginol Anesthesia. Anesthesiology; 85; 655 – 74
3. Eisanach, JC., Dekock, M., Klimscha, W. α2 Adrenersic against
for Regional Anaesthecia, Anaesthesiology 1996; 85; 655 – 74
4. Fukushima, K., Nishmi, Y., Mor, K, Takeda, J. Effect of
Epidurally Administered Dexmedetomidine on Sympathetic
Activity and Post Operative Pain in Man. Anesth Analg 1996; 82;
5(2).
5. Guo et. al. Dexmedetomidine injection into the Locus Ceruleus
Produces Antinociception Anesthesiology 1996; 84; 873 – 81
6. El. Hennawy Am et. al., addition of Clonidine or
Dexmedetomidine to Bupivacaine Prolong Caudal Analgesia in
Children. British J Anaesth. 2009. Aug 103(2); 268 – 74, Epub
2009, Jun 18.
7. Ibrahim, F.A. Khalifa, A Comparative Study of adding intrathecal
Dexmedetomedine Versus Sufentanyl to Heavy Bupivacaine for
Postop Analgesia in Patients Undergoing Inguinal Hernia Repair –
Benha M J. Vol. 26, No. 3, Sept. 2009.
8. Kalso E. Poyhia R, Rusenberg P. Spinal Nociception by
Dexmedetomidine, a highly selective α2 – advenergic agonist.
Pharmacol. Toxicol 1991; 68; 140 – 3.
9. Kanazi G.E., Effect of Low Dose Dexmedetomidine or Clonidine
on the Characteristic of Bupivacaine Spinal Block Acta
Anaesthesiol Scan 2006; 50; 222 – 227
10. S. Konaki, The Efficecy and Neurotoxicity of Dexmedetomidine
administered via the Epiduarl Route - European Journal of
Anaesthesiology 2008; 403 – 409.
11. Lawhead R.G., Blaxall, H.S. and Bylund, B.D. (1992); Alpha 2A
is the Predominant α2 Adrenergic Receptor Subtype in Human
Spinal Card Anesthesiology 77; 983 – 91
12. Mahmud M. Al-Mustafq, Effect of dexmedotomidine added to
spinal Bupivacaine for Urological Procedures; Saudi Med j 2009;
Vol 30 [3]; 365 – 70.
13. Maroof et. al., Anaesthesiology. It has been used in Epidural Space
in Humans with out any reports of Neurological Deficit –
Anaesthesiology 2004; 101; A495.
14. Pedersen H, Santos CA, Stinberg ES et. Al., Incidence of
Visceral Pain during Cesarean Section; the Effect of Varying
Doses of Spinal Bupivacaine; Anesth Analy 1992; 69; 46 – 9

15. I. Saadawy, Effect of Dexmedetomidine on the Characteristics
of Bupivacaine in a Caudal Block in Pediatrics – Acta
Anaesthesiol Scand 2009; 53; 251 – 256.
16. Salgado PF – Synergistic Effect between Dexmeditomidine and
0.75% Ropivacaine in Epiduaral Anaesthesia – Rev. Assoc. Med
Bias 2008 Mar. – Apr. 54(2); 110 – 5.
17. Seewal, R., Effect of Addition of Various Doses of Fentanyl
intrathecally to 0.5% Bupivacaine on Perioperative Analgesia
and Subarachanoid Block Characteristic in Lower Abdominal
Surgery – Reg. Anesth Pain Med 2007, Jan – Feb 32(1); 20 – 6
18. Seewal, R., Shende, D., Kashyap, L., Mohan, V. Effect of Addition
of Various Doses of Fentanyl Intrathecally to 0.5% Hyperbaric
Bupivacaine on Perioperative Analgesia and Subarachnoid Block
Characteristics in Lowere Abdominal Surgery; a Dose response
Study Reg. Anesth Pain Med. 2007 Jan – Feb; 32(1)-20-6
19. Subhi M. Al-Ghanem, Effect of adding Dexmedetomidine versus
Fentanyl to intrathecal Bupivacaine on Spinal Block for
Gynaecological Procedures; American Journal of Applied
Science 6 [5]; 882 – 887, 2009.
20. DXM enhances the local anaesthestic action of Lignocaine via an
α2 adrenoreceptor – Anesth. Analg 2008; 101; 96 – 101.

21. Effects of Intrathecel Fentanyl, Sufentanil and Placebo with
Bupivacaine for Electric Caesarean Section. Aneshthe Analgesia.,
Dec [85]; 1288 – 93[s].
ANNEXURES

9/23/2016 Turnitin Document Viewer
https://www.turnitin.com/dv?o=707604689&u=1055405315&s=&student_user=1&lang=en_us 1/1
The Tamil Nadu Dr.M.G.R.Medical … 20152015 plagiarism DUE 07Nov20…
Originality GradeMark PeerMark EFFECT OFBY SIVASHANKARI
KARTHIKEYAN
20%SIMILAR OUT OF 0
6
6
6
8
10
6
PAGE: 1 OF 75
Match Overview
1 archive.orgInternet source 1%
2 web.squ.edu.omInternet source 1%
3 www.scielo.brInternet source 1%
4 www.readbag.comInternet source 1%
5 www.isakanyakumari.c…Internet source 1%
6 www.scipub.orgInternet source 1%
7 www.biomedcentral.comInternet source 1%
8 priory.comInternet source 1%
9 upisa.comInternet source 1%
TextOnly Report
Submission author:Assignment t it le:Submission tit le:
File name:File size:
Page count:Word count:
Character count:Submission date:
Submission ID:
Digital ReceiptThis receipt acknowledges that Turnit in received your paper. Below you will f ind the receiptinf ormation regarding your submission.
The f irst page of your submissions is displayed below.
Sivashankari karthikeyan2015-2015 plagiarismEFFECT OF ADDING DEXMEDETO…EFFECT_OF_ADDING_DEXMEDET…1.79M7511,66163,19023-Sep-2016 01:41AM707604689
Copyright 2016 Turnitin. All rights reserved.

INFORMATION TO PARTICIPANTS INVESTIGATOR : Dr. SIVASHANKARI.K NAME OF THE PARTICIPANT: TITLE: “Effect of adding dexmedetomidine versus fentanyl to intrathecal bupivacaine on
spinal block characteristics in gynaecological procedures: A double blind controlled
study”.
You are invited to take part in this research study. We have got approval from the IEC. You
are asked to participate because you satisfy the eligibility criteria. We want to compare
and study the level of sensory and motor block, Intraoperative pain and safety of giving
dexmedetomidine versus fentanyl with bupivacaine on spinal block characteristics in
gynaecological surgery.
WHAT IS THE PURPOSE OF THE RESEARCH:
For gynaecological surgery, Inj dexmedetomidine/fentanyl is added to bupivacaine for
spinal block to study
4. Complication rate
THE STUDY DESIGN: All the patients in the study will be divided into two groups.
Group1‐inj dexmedetomidine with inj bupivacaine(0.5%) for spinal block
Group 2‐inj fentanyl with inj bupivacaine(0.5%)for spinal block
BENEFITS Onset, density and post‐operative analgesia are better with dexmetedomidine than fentanyl
DISCOMFORTS AND RISKS Damage to neuro vascular structure.
Hypotension
Nausea and vomiting
Headache
This intervention has been shown to be well tolerated as shown by previous studies and if
you do not want to participate you will have alternative of setting the standard treatment
and your safety is our prime concern.
1. To evaluate the onset and duration of sensory and motor block
2. To assess intra operative haemodynamics
3. To monitor postoperative analgesia.
Confidentiality of data and details of study and patient details concerned with this
research will be strictly maintained.
Time :
Date :
Place :
Signature / Thumb Impression of Patient Patient Name:
Signature of the Investigator : ____________________________ Name of the Investigator : ____________________________
PATIENT CONSENT FORM
STUDY TITLE: “Effect of adding dexmedetomidine versus fentanyl to intrathecal bupivacaine on spinal block characteristics in gynaecological procedures:A double blind controlled study”
STUDY CENTER: DEPARTMENT OF ANAESTHESIOLOGY,
INSTITUTE OF OBSTETRICS AND GYNAECOLOGY,
RAJIV GANDHI GOVT. GENERAL HOSPITAL,
MADRAS MEDICAL COLLEGE,
CHENNAI‐ 600008.
Participant name: Age: Sex:
I.P.No:
I confirm that I have understood the purpose of procedure for the above
study. I have the opportunity to ask the question and all my questions and doubts have
been answered to my satisfaction.
I have been explained about the pitfall in the procedure. I have been
explained about the safety, advantage and disadvantage of the technique.
I understand that my participation in the study is voluntary and that I am
free to withdraw at anytime without giving any reason.
I understand that investigator, regulatory authorities and the ethics
committee will not need my permission to look at my health records both in respect to
current study and any further research that may be conducted in relation to it, even if I
withdraw from the study. I understand that my identity will not be revealed in any
information released to third parties or published, unless as required under the law. I
agree not to restrict the use of any data or results that arise from the study.
Time:
Date: Signature / thumb impression of
patient
Place: Patient name:
Signature of the investigator:
Name of the investigator:
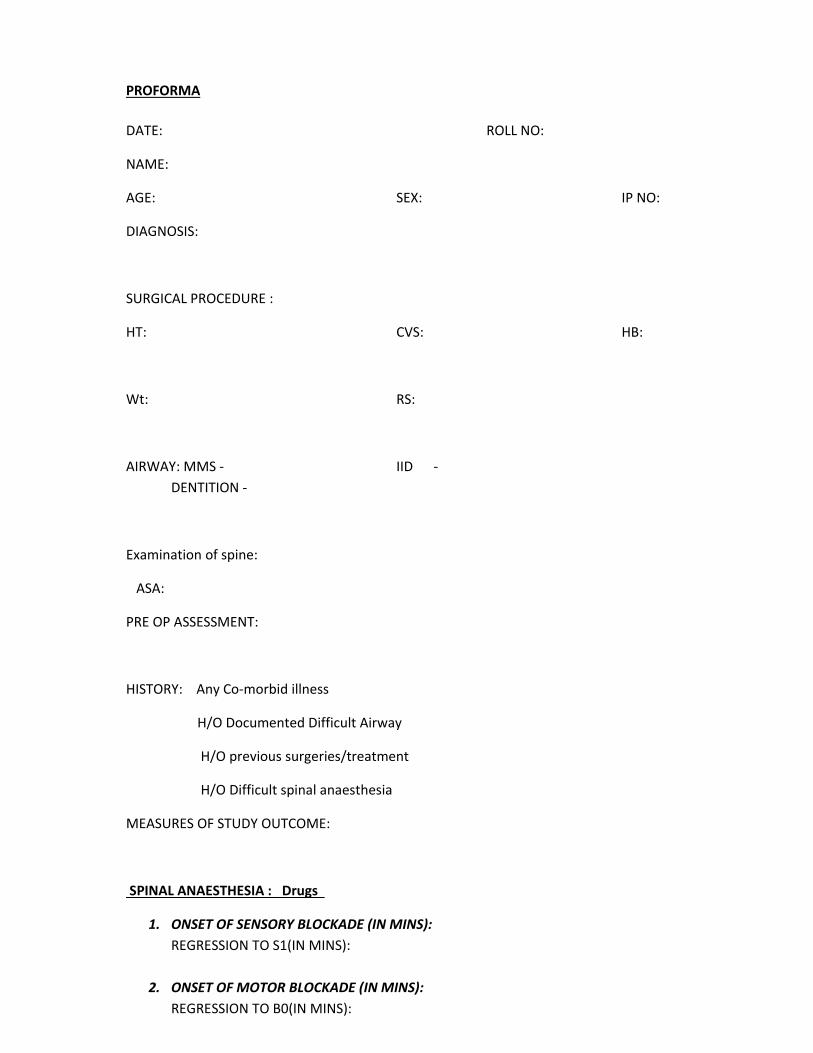
PROFORMA
DATE: ROLL NO:
NAME:
AGE: SEX: IP NO:
DIAGNOSIS:
SURGICAL PROCEDURE :
HT: CVS: HB:
Wt: RS:
AIRWAY: MMS ‐ IID ‐
DENTITION ‐
Examination of spine:
ASA:
PRE OP ASSESSMENT:
HISTORY: Any Co‐morbid illness
H/O Documented Difficult Airway
H/O previous surgeries/treatment
H/O Difficult spinal anaesthesia
MEASURES OF STUDY OUTCOME:
SPINAL ANAESTHESIA : Drugs
1. ONSET OF SENSORY BLOCKADE (IN MINS):
REGRESSION TO S1(IN MINS):
2. ONSET OF MOTOR BLOCKADE (IN MINS):
REGRESSION TO B0(IN MINS):

3. HEMODYNAMICS: INTRA OPERATIVE
Events Time Systolic BP
(mmHg)
Diastolic BP
(mmHg)
Heart rate
Beats/min
SPO2
Baseline
Immediately
after spinal
anaesthesia
5 mins
10 mins
15 mins
20 mins
30 mins
45 mins
60mins
75 mins
90 mins
2 hrs
2.30hrs
3hrs
3.30hrs
4hrs
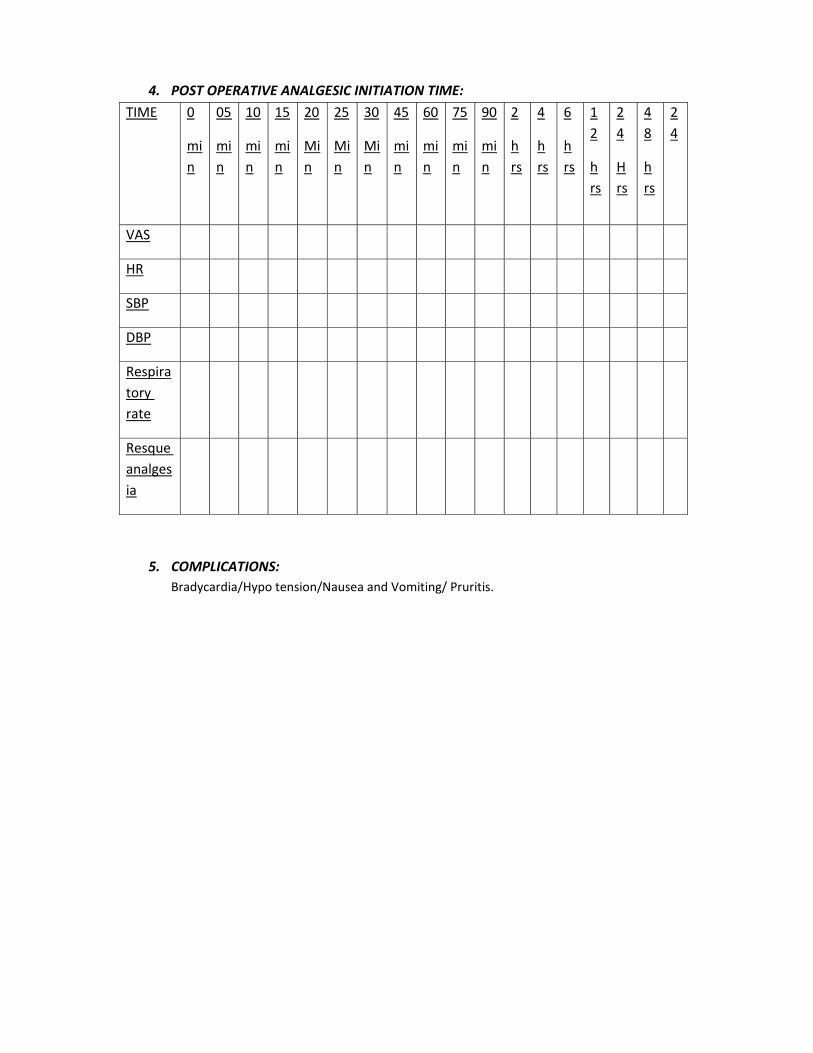
4. POST OPERATIVE ANALGESIC INITIATION TIME:
TIME 0
mi
n
05
mi
n
10
mi
n
15
mi
n
20
Mi
n
25
Mi
n
30
Mi
n
45
mi
n
60
mi
n
75
mi
n
90
mi
n
2
h
rs
4
h
rs
6
h
rs
1
2
h
rs
2
4
H
rs
4
8
h
rs
2
4
VAS
HR
SBP
DBP
Respira
tory
rate
Resque
analges
ia
5. COMPLICATIONS:
Bradycardia/Hypo tension/Nausea and Vomiting/ Pruritis.
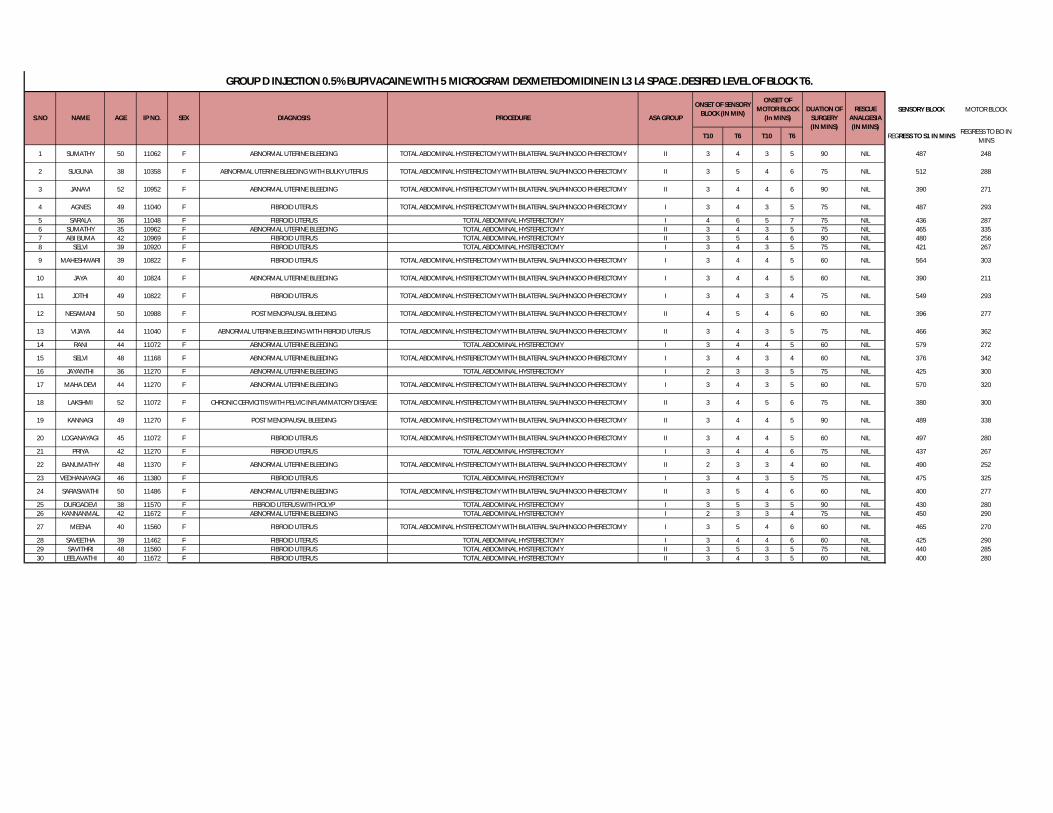
SENSORY BLOCK MOTOR BLOCK
T10 T6 T10 T6 REGRESS TO S1 IN MINSREGRESS TO BO IN
MINS
1 SUMATHY 50 11062 F ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY II 3 4 3 5 90 NIL 487 248
2 SUGUNA 38 10358 F ABNORMAL UTERINE BLEEDING WITH BULKY UTERUS TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY II 3 5 4 6 75 NIL 512 288
3 JANAVI 52 10952 F ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY II 3 4 4 6 90 NIL 390 271
4 AGNES 49 11040 F FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY I 3 4 3 5 75 NIL 487 293
5 SARALA 36 11048 F FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY I 4 6 5 7 75 NIL 436 2876 SUMATHY 35 10962 F ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY II 3 4 3 5 75 NIL 465 3357 ABI BUMA 42 10969 F FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY II 3 5 4 6 90 NIL 480 2568 SELVI 39 10920 F FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY I 3 4 3 5 75 NIL 421 267
9 MAHESHWARI 39 10822 F FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY I 3 4 4 5 60 NIL 564 303
10 JAYA 40 10824 F ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY I 3 4 4 5 60 NIL 390 211
11 JOTHI 49 10822 F FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY I 3 4 3 4 75 NIL 549 293
12 NESAMANI 50 10988 F POST MENOPAUSAL BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY II 4 5 4 6 60 NIL 396 277
13 VIJAYA 44 11040 F ABNORMAL UTERINE BLEEDING WITH FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY II 3 4 3 5 75 NIL 466 362
14 RANI 44 11072 F ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY I 3 4 4 5 60 NIL 579 272
15 SELVI 48 11168 F ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY I 3 4 3 4 60 NIL 376 342
16 JAYANTHI 36 11270 F ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY I 2 3 3 5 75 NIL 425 300
17 MAHA DEVI 44 11270 F ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY I 3 4 3 5 60 NIL 570 320
18 LAKSHMI 52 11072 F CHRONIC CERVICITIS WITH PELVIC INFLAMMATORY DISEASE TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY II 3 4 5 6 75 NIL 380 300
19 KANNAGI 49 11270 F POST MENOPAUSAL BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY II 3 4 4 5 90 NIL 489 338
20 LOGANAYAGI 45 11072 F FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY II 3 4 4 5 60 NIL 497 280
21 PRIYA 42 11270 F FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY I 3 4 4 6 75 NIL 437 267
22 BANUMATHY 48 11370 F ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY II 2 3 3 4 60 NIL 490 252
23 VEDHANAYAGI 46 11380 F FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY I 3 4 3 5 75 NIL 475 325
24 SARASWATHI 50 11486 F ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY II 3 5 4 6 60 NIL 400 277
25 DURGADEVI 38 11570 F FIBROID UTERUS WITH POLYP TOTAL ABDOMINAL HYSTERECTOMY I 3 5 3 5 90 NIL 430 28026 KANNANMAL 42 11672 F ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY I 2 3 3 4 75 NIL 450 290
27 MEENA 40 11560 F FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOO PHERECTOMY I 3 5 4 6 60 NIL 465 270
28 SAVEETHA 39 11462 F FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY I 3 4 4 6 60 NIL 425 29029 SAVITHRI 48 11560 F FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY II 3 5 3 5 75 NIL 440 28530 LEELAVATHI 40 11672 F FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY II 3 4 3 5 60 NIL 400 280
ONSET OF SENSORY BLOCK (IN MIN)
ONSET OF MOTOR BLOCK
(In MINS)DUATION OF
SURGERY (IN MINS)
RESCUE ANALGESIA (IN MINS)
ASA GROUPPROCEDURE
GROUP D INJECTION 0.5% BUPIVACAINE WITH 5 MICROGRAM DEXMETEDOMIDINE IN L3 L4 SPACE .DESIRED LEVEL OF BLOCK T6.
IP NO. DIAGNOSISS.NO NAME AGE SEX
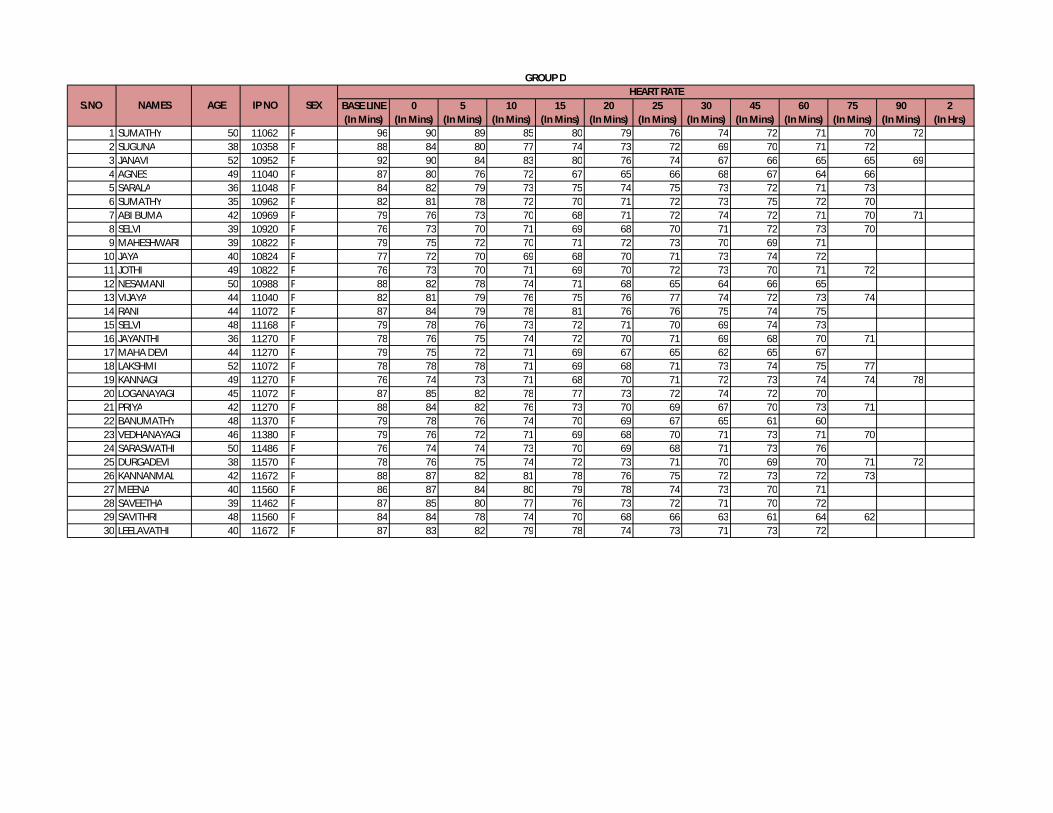
BASE LINE (In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Mins)
45(In Mins)
60 (In Mins)
75(In Mins)
90(In Mins)
2(In Hrs)
1 SUMATHY 50 11062 F 96 90 89 85 80 79 76 74 72 71 70 722 SUGUNA 38 10358 F 88 84 80 77 74 73 72 69 70 71 723 JANAVI 52 10952 F 92 90 84 83 80 76 74 67 66 65 65 694 AGNES 49 11040 F 87 80 76 72 67 65 66 68 67 64 665 SARALA 36 11048 F 84 82 79 73 75 74 75 73 72 71 736 SUMATHY 35 10962 F 82 81 78 72 70 71 72 73 75 72 707 ABI BUMA 42 10969 F 79 76 73 70 68 71 72 74 72 71 70 718 SELVI 39 10920 F 76 73 70 71 69 68 70 71 72 73 709 MAHESHWARI 39 10822 F 79 75 72 70 71 72 73 70 69 71
10 JAYA 40 10824 F 77 72 70 69 68 70 71 73 74 7211 JOTHI 49 10822 F 76 73 70 71 69 70 72 73 70 71 7212 NESAMANI 50 10988 F 88 82 78 74 71 68 65 64 66 6513 VIJAYA 44 11040 F 82 81 79 76 75 76 77 74 72 73 7414 RANI 44 11072 F 87 84 79 78 81 76 76 75 74 7515 SELVI 48 11168 F 79 78 76 73 72 71 70 69 74 7316 JAYANTHI 36 11270 F 78 76 75 74 72 70 71 69 68 70 7117 MAHA DEVI 44 11270 F 79 75 72 71 69 67 65 62 65 6718 LAKSHMI 52 11072 F 78 78 78 71 69 68 71 73 74 75 7719 KANNAGI 49 11270 F 76 74 73 71 68 70 71 72 73 74 74 7820 LOGANAYAGI 45 11072 F 87 85 82 78 77 73 72 74 72 7021 PRIYA 42 11270 F 88 84 82 76 73 70 69 67 70 73 7122 BANUMATHY 48 11370 F 79 78 76 74 70 69 67 65 61 6023 VEDHANAYAGI 46 11380 F 79 76 72 71 69 68 70 71 73 71 7024 SARASWATHI 50 11486 F 76 74 74 73 70 69 68 71 73 7625 DURGADEVI 38 11570 F 78 76 75 74 72 73 71 70 69 70 71 7226 KANNANMAL 42 11672 F 88 87 82 81 78 76 75 72 73 72 7327 MEENA 40 11560 F 86 87 84 80 79 78 74 73 70 7128 SAVEETHA 39 11462 F 87 85 80 77 76 73 72 71 70 7229 SAVITHRI 48 11560 F 84 84 78 74 70 68 66 63 61 64 6230 LEELAVATHI 40 11672 F 87 83 82 79 78 74 73 71 73 72
AGE SEXS.NO NAMESHEART RATE
IP NO
GROUP D
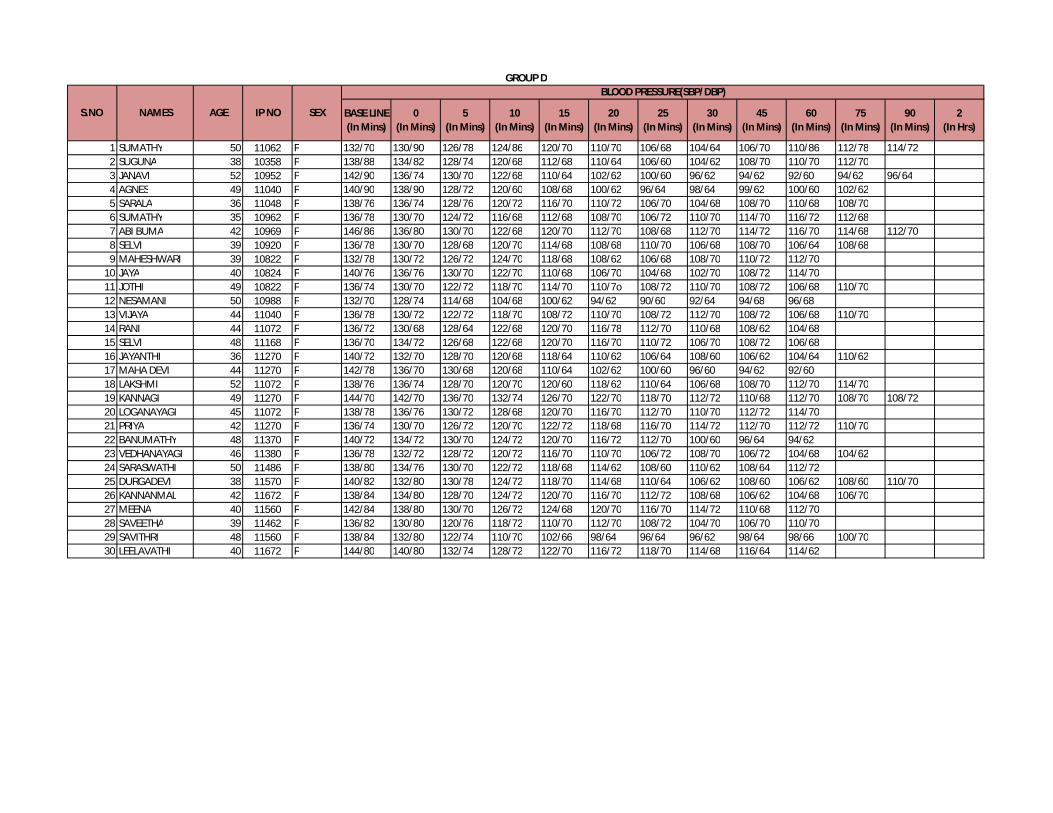
BASE LINE (In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Mins)
45(In Mins)
60 (In Mins)
75(In Mins)
90(In Mins)
2(In Hrs)
1 SUMATHY 50 11062 F 132/70 130/90 126/78 124/86 120/70 110/70 106/68 104/64 106/70 110/86 112/78 114/722 SUGUNA 38 10358 F 138/88 134/82 128/74 120/68 112/68 110/64 106/60 104/62 108/70 110/70 112/703 JANAVI 52 10952 F 142/90 136/74 130/70 122/68 110/64 102/62 100/60 96/62 94/62 92/60 94/62 96/644 AGNES 49 11040 F 140/90 138/90 128/72 120/60 108/68 100/62 96/64 98/64 99/62 100/60 102/625 SARALA 36 11048 F 138/76 136/74 128/76 120/72 116/70 110/72 106/70 104/68 108/70 110/68 108/706 SUMATHY 35 10962 F 136/78 130/70 124/72 116/68 112/68 108/70 106/72 110/70 114/70 116/72 112/687 ABI BUMA 42 10969 F 146/86 136/80 130/70 122/68 120/70 112/70 108/68 112/70 114/72 116/70 114/68 112/708 SELVI 39 10920 F 136/78 130/70 128/68 120/70 114/68 108/68 110/70 106/68 108/70 106/64 108/689 MAHESHWARI 39 10822 F 132/78 130/72 126/72 124/70 118/68 108/62 106/68 108/70 110/72 112/70
10 JAYA 40 10824 F 140/76 136/76 130/70 122/70 110/68 106/70 104/68 102/70 108/72 114/7011 JOTHI 49 10822 F 136/74 130/70 122/72 118/70 114/70 110/7o 108/72 110/70 108/72 106/68 110/7012 NESAMANI 50 10988 F 132/70 128/74 114/68 104/68 100/62 94/62 90/60 92/64 94/68 96/6813 VIJAYA 44 11040 F 136/78 130/72 122/72 118/70 108/72 110/70 108/72 112/70 108/72 106/68 110/7014 RANI 44 11072 F 136/72 130/68 128/64 122/68 120/70 116/78 112/70 110/68 108/62 104/6815 SELVI 48 11168 F 136/70 134/72 126/68 122/68 120/70 116/70 110/72 106/70 108/72 106/6816 JAYANTHI 36 11270 F 140/72 132/70 128/70 120/68 118/64 110/62 106/64 108/60 106/62 104/64 110/6217 MAHA DEVI 44 11270 F 142/78 136/70 130/68 120/68 110/64 102/62 100/60 96/60 94/62 92/6018 LAKSHMI 52 11072 F 138/76 136/74 128/70 120/70 120/60 118/62 110/64 106/68 108/70 112/70 114/7019 KANNAGI 49 11270 F 144/70 142/70 136/70 132/74 126/70 122/70 118/70 112/72 110/68 112/70 108/70 108/7220 LOGANAYAGI 45 11072 F 138/78 136/76 130/72 128/68 120/70 116/70 112/70 110/70 112/72 114/7021 PRIYA 42 11270 F 136/74 130/70 126/72 120/70 122/72 118/68 116/70 114/72 112/70 112/72 110/7022 BANUMATHY 48 11370 F 140/72 134/72 130/70 124/72 120/70 116/72 112/70 100/60 96/64 94/6223 VEDHANAYAGI 46 11380 F 136/78 132/72 128/72 120/72 116/70 110/70 106/72 108/70 106/72 104/68 104/6224 SARASWATHI 50 11486 F 138/80 134/76 130/70 122/72 118/68 114/62 108/60 110/62 108/64 112/7225 DURGADEVI 38 11570 F 140/82 132/80 130/78 124/72 118/70 114/68 110/64 106/62 108/60 106/62 108/60 110/7026 KANNANMAL 42 11672 F 138/84 134/80 128/70 124/72 120/70 116/70 112/72 108/68 106/62 104/68 106/7027 MEENA 40 11560 F 142/84 138/80 130/70 126/72 124/68 120/70 116/70 114/72 110/68 112/7028 SAVEETHA 39 11462 F 136/82 130/80 120/76 118/72 110/70 112/70 108/72 104/70 106/70 110/7029 SAVITHRI 48 11560 F 138/84 132/80 122/74 110/70 102/66 98/64 96/64 96/62 98/64 98/66 100/7030 LEELAVATHI 40 11672 F 144/80 140/80 132/74 128/72 122/70 116/72 118/70 114/68 116/64 114/62
S.NO NAMES AGE SEX
BLOOD PRESSURE(SBP/DBP)GROUP D
IP NO
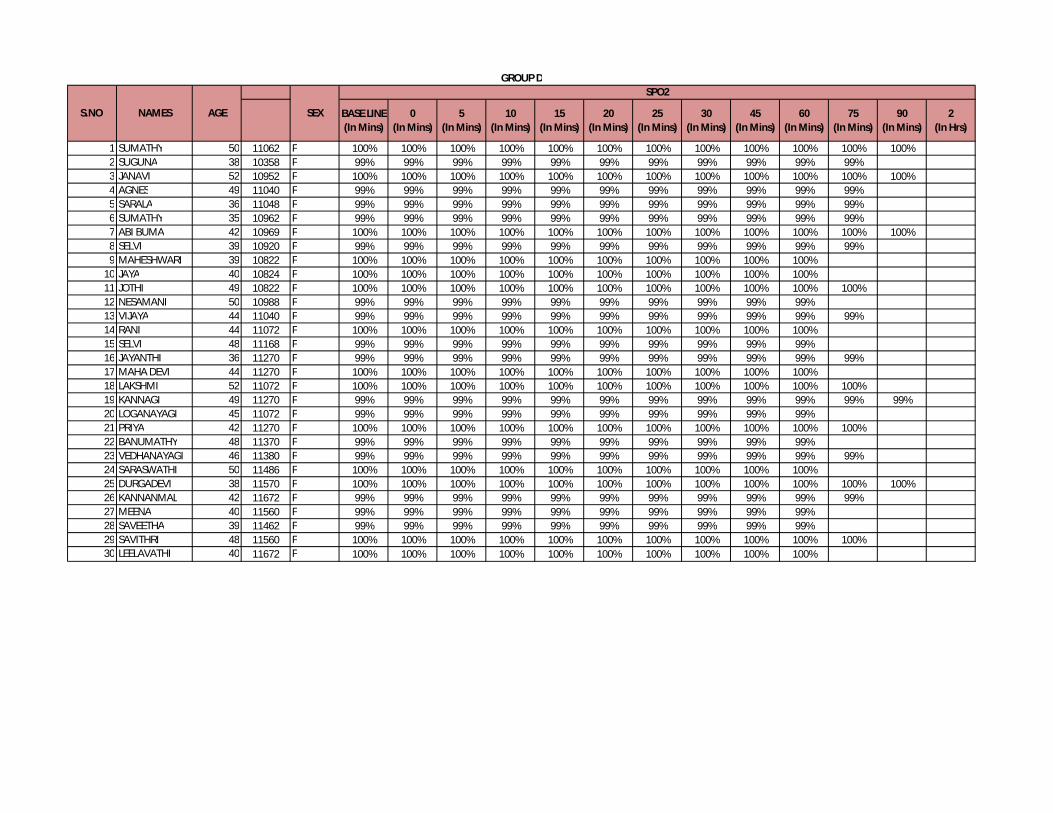
BASE LINE (In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Mins)
45(In Mins)
60 (In Mins)
75(In Mins)
90(In Mins)
2(In Hrs)
1 SUMATHY 50 11062 F 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%2 SUGUNA 38 10358 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%3 JANAVI 52 10952 F 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%4 AGNES 49 11040 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%5 SARALA 36 11048 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%6 SUMATHY 35 10962 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%7 ABI BUMA 42 10969 F 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%8 SELVI 39 10920 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%9 MAHESHWARI 39 10822 F 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
10 JAYA 40 10824 F 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%11 JOTHI 49 10822 F 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%12 NESAMANI 50 10988 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%13 VIJAYA 44 11040 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%14 RANI 44 11072 F 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%15 SELVI 48 11168 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%16 JAYANTHI 36 11270 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%17 MAHA DEVI 44 11270 F 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%18 LAKSHMI 52 11072 F 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%19 KANNAGI 49 11270 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%20 LOGANAYAGI 45 11072 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%21 PRIYA 42 11270 F 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%22 BANUMATHY 48 11370 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%23 VEDHANAYAGI 46 11380 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%24 SARASWATHI 50 11486 F 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%25 DURGADEVI 38 11570 F 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%26 KANNANMAL 42 11672 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%27 MEENA 40 11560 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%28 SAVEETHA 39 11462 F 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%29 SAVITHRI 48 11560 F 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%30 LEELAVATHI 40 11672 F 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
S.NO NAMES AGE SEX
SPO2GROUP D
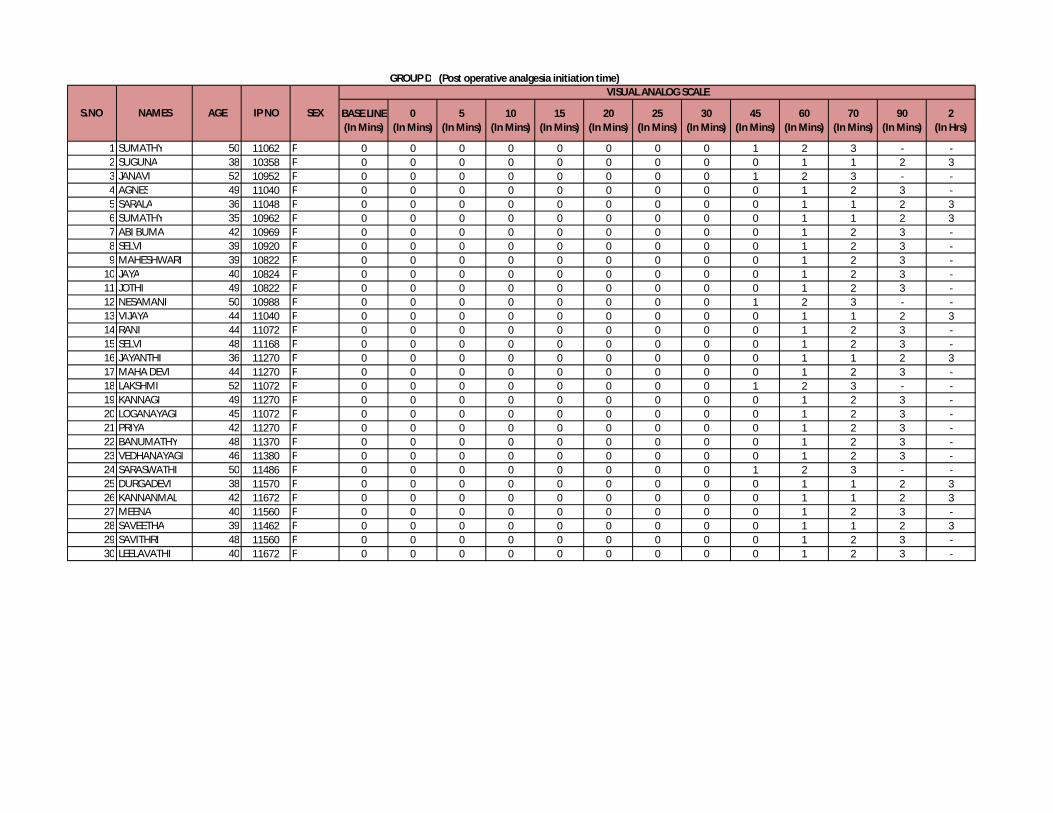
GROUP D (Post operative analgesia initiation time)
BASE LINE (In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Mins)
45(In Mins)
60 (In Mins)
70 (In Mins)
90(In Mins)
2(In Hrs)
1 SUMATHY 50 11062 F 0 0 0 0 0 0 0 0 1 2 3 - -2 SUGUNA 38 10358 F 0 0 0 0 0 0 0 0 0 1 1 2 33 JANAVI 52 10952 F 0 0 0 0 0 0 0 0 1 2 3 - -4 AGNES 49 11040 F 0 0 0 0 0 0 0 0 0 1 2 3 -5 SARALA 36 11048 F 0 0 0 0 0 0 0 0 0 1 1 2 36 SUMATHY 35 10962 F 0 0 0 0 0 0 0 0 0 1 1 2 37 ABI BUMA 42 10969 F 0 0 0 0 0 0 0 0 0 1 2 3 -8 SELVI 39 10920 F 0 0 0 0 0 0 0 0 0 1 2 3 -9 MAHESHWARI 39 10822 F 0 0 0 0 0 0 0 0 0 1 2 3 -
10 JAYA 40 10824 F 0 0 0 0 0 0 0 0 0 1 2 3 -11 JOTHI 49 10822 F 0 0 0 0 0 0 0 0 0 1 2 3 -12 NESAMANI 50 10988 F 0 0 0 0 0 0 0 0 1 2 3 - -13 VIJAYA 44 11040 F 0 0 0 0 0 0 0 0 0 1 1 2 314 RANI 44 11072 F 0 0 0 0 0 0 0 0 0 1 2 3 -15 SELVI 48 11168 F 0 0 0 0 0 0 0 0 0 1 2 3 -16 JAYANTHI 36 11270 F 0 0 0 0 0 0 0 0 0 1 1 2 317 MAHA DEVI 44 11270 F 0 0 0 0 0 0 0 0 0 1 2 3 -18 LAKSHMI 52 11072 F 0 0 0 0 0 0 0 0 1 2 3 - -19 KANNAGI 49 11270 F 0 0 0 0 0 0 0 0 0 1 2 3 -20 LOGANAYAGI 45 11072 F 0 0 0 0 0 0 0 0 0 1 2 3 -21 PRIYA 42 11270 F 0 0 0 0 0 0 0 0 0 1 2 3 -22 BANUMATHY 48 11370 F 0 0 0 0 0 0 0 0 0 1 2 3 -23 VEDHANAYAGI 46 11380 F 0 0 0 0 0 0 0 0 0 1 2 3 -24 SARASWATHI 50 11486 F 0 0 0 0 0 0 0 0 1 2 3 - -25 DURGADEVI 38 11570 F 0 0 0 0 0 0 0 0 0 1 1 2 326 KANNANMAL 42 11672 F 0 0 0 0 0 0 0 0 0 1 1 2 327 MEENA 40 11560 F 0 0 0 0 0 0 0 0 0 1 2 3 -28 SAVEETHA 39 11462 F 0 0 0 0 0 0 0 0 0 1 1 2 329 SAVITHRI 48 11560 F 0 0 0 0 0 0 0 0 0 1 2 3 -30 LEELAVATHI 40 11672 F 0 0 0 0 0 0 0 0 0 1 2 3 -
S.NO NAMES AGE SEX
VISUAL ANALOG SCALE
IP NO
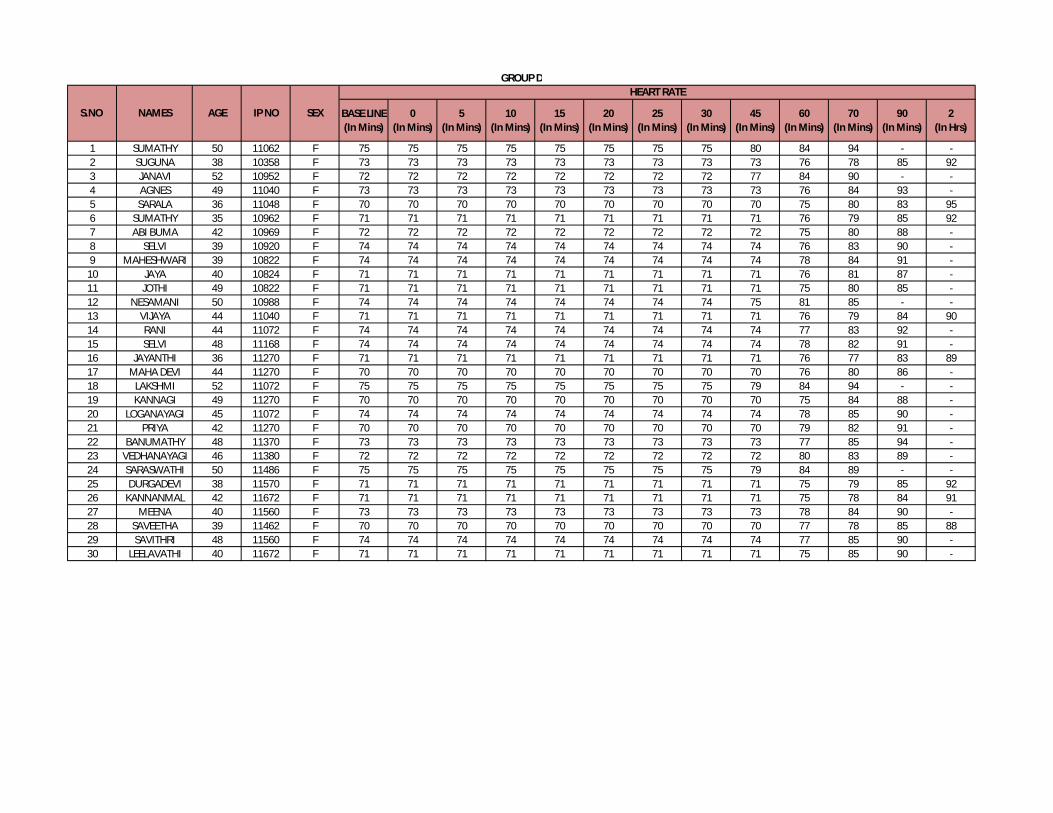
BASE LINE (In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Mins)
45(In Mins)
60 (In Mins)
70 (In Mins)
90(In Mins)
2(In Hrs)
1 SUMATHY 50 11062 F 75 75 75 75 75 75 75 75 80 84 94 - -2 SUGUNA 38 10358 F 73 73 73 73 73 73 73 73 73 76 78 85 923 JANAVI 52 10952 F 72 72 72 72 72 72 72 72 77 84 90 - -4 AGNES 49 11040 F 73 73 73 73 73 73 73 73 73 76 84 93 -5 SARALA 36 11048 F 70 70 70 70 70 70 70 70 70 75 80 83 956 SUMATHY 35 10962 F 71 71 71 71 71 71 71 71 71 76 79 85 927 ABI BUMA 42 10969 F 72 72 72 72 72 72 72 72 72 75 80 88 -8 SELVI 39 10920 F 74 74 74 74 74 74 74 74 74 76 83 90 -9 MAHESHWARI 39 10822 F 74 74 74 74 74 74 74 74 74 78 84 91 -
10 JAYA 40 10824 F 71 71 71 71 71 71 71 71 71 76 81 87 -11 JOTHI 49 10822 F 71 71 71 71 71 71 71 71 71 75 80 85 -12 NESAMANI 50 10988 F 74 74 74 74 74 74 74 74 75 81 85 - -13 VIJAYA 44 11040 F 71 71 71 71 71 71 71 71 71 76 79 84 9014 RANI 44 11072 F 74 74 74 74 74 74 74 74 74 77 83 92 -15 SELVI 48 11168 F 74 74 74 74 74 74 74 74 74 78 82 91 -16 JAYANTHI 36 11270 F 71 71 71 71 71 71 71 71 71 76 77 83 8917 MAHA DEVI 44 11270 F 70 70 70 70 70 70 70 70 70 76 80 86 -18 LAKSHMI 52 11072 F 75 75 75 75 75 75 75 75 79 84 94 - -19 KANNAGI 49 11270 F 70 70 70 70 70 70 70 70 70 75 84 88 -20 LOGANAYAGI 45 11072 F 74 74 74 74 74 74 74 74 74 78 85 90 -21 PRIYA 42 11270 F 70 70 70 70 70 70 70 70 70 79 82 91 -22 BANUMATHY 48 11370 F 73 73 73 73 73 73 73 73 73 77 85 94 -23 VEDHANAYAGI 46 11380 F 72 72 72 72 72 72 72 72 72 80 83 89 -24 SARASWATHI 50 11486 F 75 75 75 75 75 75 75 75 79 84 89 - -25 DURGADEVI 38 11570 F 71 71 71 71 71 71 71 71 71 75 79 85 9226 KANNANMAL 42 11672 F 71 71 71 71 71 71 71 71 71 75 78 84 9127 MEENA 40 11560 F 73 73 73 73 73 73 73 73 73 78 84 90 -28 SAVEETHA 39 11462 F 70 70 70 70 70 70 70 70 70 77 78 85 8829 SAVITHRI 48 11560 F 74 74 74 74 74 74 74 74 74 77 85 90 -30 LEELAVATHI 40 11672 F 71 71 71 71 71 71 71 71 71 75 85 90 -
GROUP D
S.NO NAMES AGE SEX
HEART RATE
IP NO

BASE LINE (In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Mins)
45(In Mins)
60 (In Mins)
70 (In Mins)
90(In Mins)
2(In Hrs)
1 SUMATHY 50 11062 F 110/70 112/72 114/68 116/70 114/68 116/70 114/68 120/72 124/70 126/72 128/742 SUGUNA 38 10358 F 108/72 112/70 110/72 112/72 110/70 116/72 118/72 120/70 122/70 120/70 128/74 130/70 134/763 JANAVI 52 10952 F 104/68 106/70 108/68 112/70 110/72 112/68 110/68 112/70 110/72 120/744 AGNES 49 11040 F 102/70 106/68 110/68 112/70 110/72 112/70 114/72 116/70 118/72 120/70 126/72 128/705 SARALA 36 11048 F 106/72 108/74 110/70 112/74 116/70 118/72 120/72 122/72 124/72 126/72 128/74 130/70 132/706 SUMATHY 35 10962 F 102/70 106/74 108/70 110/72 112/72 114/70 110/74 112/72 110/70 112/76 114/72 122/72 126/707 ABI BUMA 42 10969 F 104/72 108/72 108/70 110/74 114/70 116/72 118/74 122/76 124/78 126/78 130/78 128/728 SELVI 39 10920 F 104/68 106/70 108/70 110/70 112/68 114/70 116/72 118/74 120/72 122/70 124/72 128/709 MAHESHWARI 39 10822 F 106/70 108/72 110/70 112/70 114/72 116/70 118/72 120/70 122/72 124/70 122/74 128/76
10 JAYA 40 10824 F 108/68 106/70 108/72 108/74 112/70 114/72 116/72 118/70 120/72 122/70 124/72 128/7211 JOTHI 49 10822 F 104/64 104/68 108/70 110/72 114/74 116/72 118/70 122/72 124/70 122/72 124/70 130/8012 NESAMANI 50 10988 F 106/68 108/68 108/70 110/72 112/70 116/72 118/70 120/72 120/72 122/70 124/7213 VIJAYA 44 11040 F 108/70 110/70 112/72 114/70 114/72 116/70 118/72 120/70 122/72 124/70 130/72 132/74 130/7214 RANI 44 11072 F 106/72 104/70 108/72 112/70 110/72 112/70 114/70 116/74 120/76 122/72 126/74 130/7615 SELVI 48 11168 F 108/72 106/70 110/72 112/72 110/70 114/72 116/70 118/72 120/70 122/70 126/74 124/7216 JAYANTHI 36 11270 F 104/70 106/72 108/70 110/70 112/72 114/70 116/72 118/70 120/72 122/70 124/70 128/78 130/8017 MAHA DEVI 44 11270 F 106/72 108/70 110/70 112/70 110/72 114/70 112/74 118/76 124/78 130/74 132/70 134/7218 LAKSHMI 52 11072 F 108/70 110/72 110/70 112/72 112/70 116/72 118/70 120/74 126/76 124/78 128/7219 KANNAGI 49 11270 F 102/70 106/72 108/70 110/70 112/72 114/74 116/72 120/70 122/72 124/74 122/70 124/7220 LOGANAYAGI 45 11072 F 106/72 106/74 108/72 110/72 112/74 114/72 112/70 118/72 122/70 124/74 128/72 134/7021 PRIYA 42 11270 F 108/68 110/70 112/70 112/72 114/70 118/72 120/70 124/74 128/76 132/78 130/72 136/7022 BANUMATHY 48 11370 F 106/70 112/74 110/72 112/70 114/74 116/76 118/78 122/80 126/82 130/80 132/82 134/8023 VEDHANAYAGI 46 11380 F 110/70 110/72 112/72 114/70 116/74 118/72 122/76 124/78 126/76 124/74 122/70 124/7224 SARASWATHI 50 11486 F 108/72 106/72 108/70 110/72 114/70 118/70 122/76 124/72 126/74 128/72 126/7025 DURGADEVI 38 11570 F 108/70 108/72 110/70 112/72 116/74 118/74 120/76 122/78 124/76 126/78 128/76 128/74 130/7226 KANNANMAL 42 11672 F 106/70 106/72 112/70 112/70 116/72 118/70 120/74 122/74 126/72 128/74 130/70 132/72 130/7427 MEENA 40 11560 F 108/72 110/72 114/70 114/72 116/70 118/72 122/72 124/70 126/72 126/70 128/72 126/7428 SAVEETHA 39 11462 F 110/70 106/72 110/70 112/72 118/74 118/76 124/76 126/70 128/72 128/70 130/74 132/76 130/7829 SAVITHRI 48 11560 F 106/68 108/70 110/70 110/70 112/72 116/70 126/78 128/76 130/74 132/72 134/74 132/7230 LEELAVATHI 40 11672 F 104/70 108/70 108/72 112/72 114/70 114/72 120/74 122/72 126/72 130/72 134/72 136/70
S.NO NAMES AGE SEX
BLOOD PRESSURE(SBP/DBP)
IP NO
GROUP D

BASE LINE (In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Mins)
45(In Mins)
60 (In Mins)
70 (In Mins)
90(In Mins)
2(In Hrs)
1 SUMATHY 50 11062 F 13 13 13 13 13 13 13 13 14 16 19 - -2 SUGUNA 38 10358 F 13 13 13 13 13 13 13 13 13 14 14 17 193 JANAVI 52 10952 F 13 13 13 13 13 13 13 13 14 16 19 - -4 AGNES 49 11040 F 12 12 12 12 12 12 12 12 12 13 15 17 -5 SARALA 36 11048 F 12 12 12 12 12 12 12 12 12 13 14 15 186 SUMATHY 35 10962 F 12 12 12 12 12 12 12 12 12 14 14 16 207 ABI BUMA 42 10969 F 12 12 12 12 12 12 12 12 12 13 15 18 -8 SELVI 39 10920 F 12 12 12 12 12 12 12 12 12 13 17 18 -9 MAHESHWARI 39 10822 F 13 13 13 13 13 13 13 13 13 14 16 20 -
10 JAYA 40 10824 F 13 13 13 13 13 13 13 13 13 14 17 18 -11 JOTHI 49 10822 F 13 13 13 13 13 13 13 13 13 14 17 19 -12 NESAMANI 50 10988 F 12 12 12 12 12 12 12 12 14 16 19 - -13 VIJAYA 44 11040 F 12 12 12 12 12 12 12 12 12 13 14 15 1814 RANI 44 11072 F 12 12 12 12 12 12 12 12 12 14 16 20 -15 SELVI 48 11168 F 13 13 13 13 13 13 13 13 13 14 16 20 -16 JAYANTHI 36 11270 F 12 12 12 12 12 12 12 12 12 13 14 15 1817 MAHA DEVI 44 11270 F 12 12 12 12 12 12 12 12 12 14 17 19 -18 LAKSHMI 52 11072 F 13 13 13 13 13 13 13 13 14 16 19 - -19 KANNAGI 49 11270 F 12 12 12 12 12 12 12 12 12 14 14 16 -20 LOGANAYAGI 45 11072 F 13 13 13 13 13 13 13 13 13 14 17 19 -21 PRIYA 42 11270 F 12 12 12 12 12 12 12 12 12 13 17 18 -22 BANUMATHY 48 11370 F 12 12 12 12 12 12 12 12 12 14 17 19 -23 VEDHANAYAGI 46 11380 F 12 12 12 12 12 12 12 12 12 14 16 20 -24 SARASWATHI 50 11486 F 13 13 13 13 13 13 13 13 14 16 19 - -25 DURGADEVI 38 11570 F 13 13 13 13 13 13 13 13 13 14 14 16 2026 KANNANMAL 42 11672 F 12 12 12 12 12 12 12 12 12 14 14 16 2027 MEENA 40 11560 F 12 12 12 12 12 12 12 12 12 13 15 17 -28 SAVEETHA 39 11462 F 12 12 12 12 12 12 12 12 12 13 14 15 1829 SAVITHRI 48 11560 F 13 13 13 13 13 13 13 13 13 13 15 17 -30 LEELAVATHI 40 11672 F 13 13 13 13 13 13 13 13 13 14 14 16 -
GROUP D
S.NO NAMES AGE SEX
RESPIRATORY RATE
IP NO
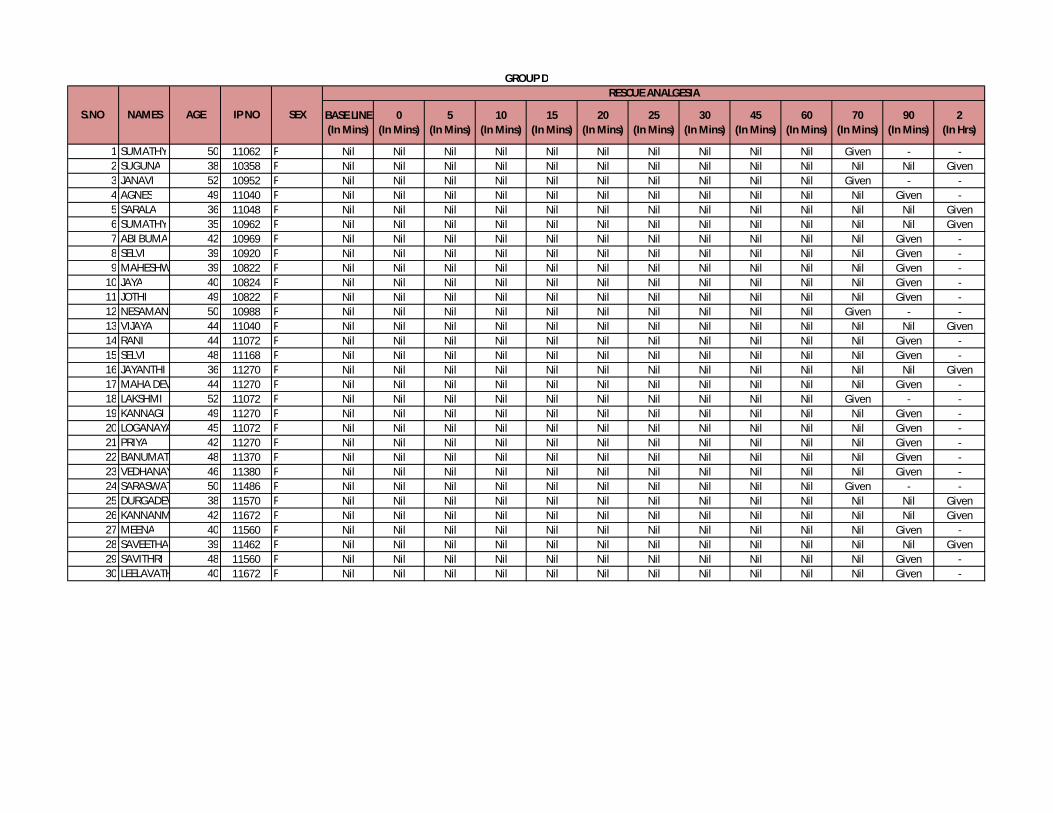
BASE LINE (In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Mins)
45(In Mins)
60 (In Mins)
70 (In Mins)
90(In Mins)
2(In Hrs)
1 SUMATHY 50 11062 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -2 SUGUNA 38 10358 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given3 JANAVI 52 10952 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -4 AGNES 49 11040 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -5 SARALA 36 11048 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given6 SUMATHY 35 10962 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given7 ABI BUMA 42 10969 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -8 SELVI 39 10920 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -9 MAHESHWARI 39 10822 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -
10 JAYA 40 10824 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -11 JOTHI 49 10822 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -12 NESAMANI 50 10988 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -13 VIJAYA 44 11040 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given14 RANI 44 11072 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -15 SELVI 48 11168 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -16 JAYANTHI 36 11270 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given17 MAHA DEVI 44 11270 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -18 LAKSHMI 52 11072 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -19 KANNAGI 49 11270 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -20 LOGANAYAGI 45 11072 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -21 PRIYA 42 11270 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -22 BANUMATHY 48 11370 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -23 VEDHANAYAGI 46 11380 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -24 SARASWATHI 50 11486 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -25 DURGADEVI 38 11570 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given26 KANNANMAL 42 11672 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given27 MEENA 40 11560 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -28 SAVEETHA 39 11462 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given29 SAVITHRI 48 11560 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -30 LEELAVATHI 40 11672 F Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -
GROUP D
S.NO NAMES AGE SEX
RESCUE ANALGESIA
IP NO
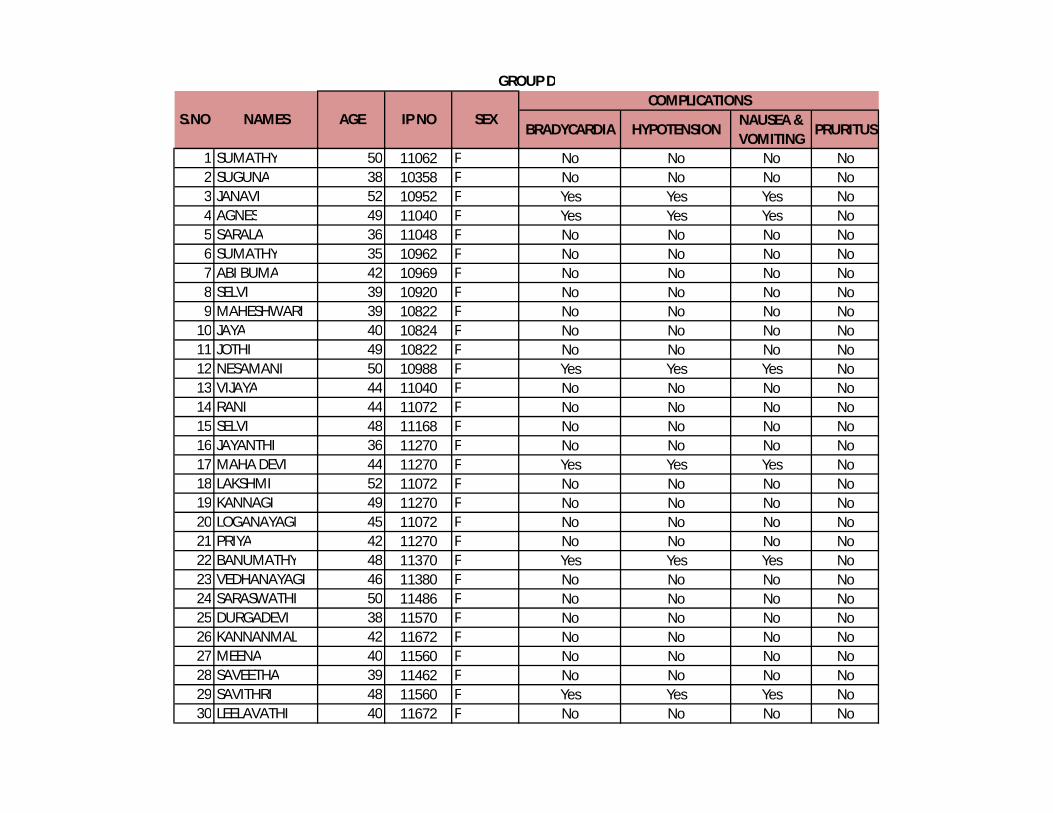
BRADYCARDIA HYPOTENSIONNAUSEA & VOMITING
PRURITUS
1 SUMATHY 50 11062 F No No No No2 SUGUNA 38 10358 F No No No No3 JANAVI 52 10952 F Yes Yes Yes No4 AGNES 49 11040 F Yes Yes Yes No5 SARALA 36 11048 F No No No No6 SUMATHY 35 10962 F No No No No7 ABI BUMA 42 10969 F No No No No8 SELVI 39 10920 F No No No No9 MAHESHWARI 39 10822 F No No No No
10 JAYA 40 10824 F No No No No11 JOTHI 49 10822 F No No No No12 NESAMANI 50 10988 F Yes Yes Yes No13 VIJAYA 44 11040 F No No No No14 RANI 44 11072 F No No No No15 SELVI 48 11168 F No No No No16 JAYANTHI 36 11270 F No No No No17 MAHA DEVI 44 11270 F Yes Yes Yes No18 LAKSHMI 52 11072 F No No No No19 KANNAGI 49 11270 F No No No No20 LOGANAYAGI 45 11072 F No No No No21 PRIYA 42 11270 F No No No No22 BANUMATHY 48 11370 F Yes Yes Yes No23 VEDHANAYAGI 46 11380 F No No No No24 SARASWATHI 50 11486 F No No No No25 DURGADEVI 38 11570 F No No No No26 KANNANMAL 42 11672 F No No No No27 MEENA 40 11560 F No No No No28 SAVEETHA 39 11462 F No No No No29 SAVITHRI 48 11560 F Yes Yes Yes No30 LEELAVATHI 40 11672 F No No No No
GROUP DCOMPLICATIONS
AGE SEXS.NO NAMES IP NO
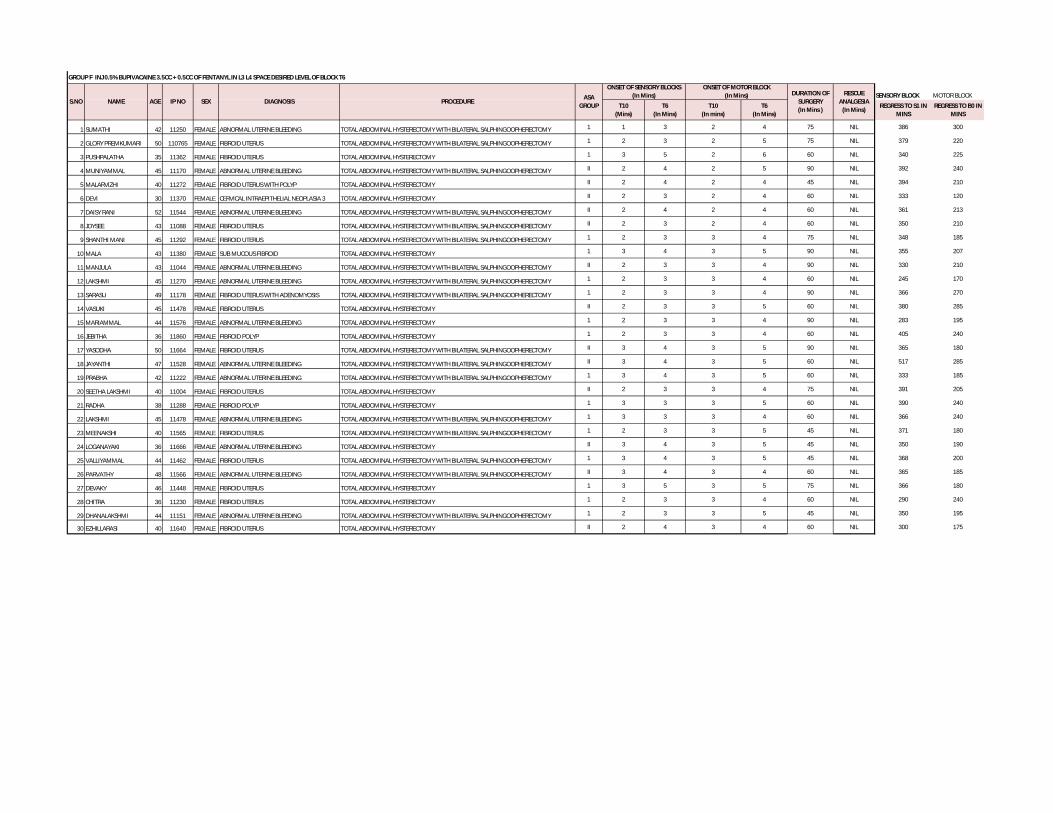
GROUP F INJ 0.5% BUPIVACAINE 3.5CC + 0.5CC OF FENTANYL IN L3 L4 SPACE DESIRED LEVEL OF BLOCK T6
SENSORY BLOCK MOTOR BLOCK
T10 (Mins)
T6 (In Mins)
T10 (In mins)
T6 (In Mins)
REGRESS TO S1 IN MINS
REGRESS TO B0 IN MINS
1 SUMATHI 42 11250 FEMALE ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY 1 1 3 2 4 75 NIL 386 300
2 GLORY PREMKUMARI 50 110765 FEMALE FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY 1 2 3 2 5 75 NIL 379 220
3 PUSHPALATHA 35 11362 FEMALE FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY 1 3 5 2 6 60 NIL 340 225
4 MUNIYAMMAL 45 11170 FEMALE ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY II 2 4 2 5 90 NIL 392 240
5 MALARVIZHI 40 11272 FEMALE FIBROID UTERUS WITH POLYP TOTAL ABDOMINAL HYSTERECTOMY II 2 4 2 4 45 NIL 394 210
6 DEVI 30 11370 FEMALE CERVICAL INTRAEPITHELIAL NEOPLASIA 3 TOTAL ABDOMINAL HYSTERECTOMY II 2 3 2 4 60 NIL 333 120
7 DAISY RANI 52 11544 FEMALE ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY II 2 4 2 4 60 NIL 361 213
8 JOYSEE 43 11088 FEMALE FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY II 2 3 2 4 60 NIL 350 210
9 SHANTHI MANI 45 11292 FEMALE FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY 1 2 3 3 4 75 NIL 348 185
10 MALA 43 11380 FEMALE SUB MUCOUS FIBROID TOTAL ABDOMINAL HYSTERECTOMY 1 3 4 3 5 90 NIL 355 207
11 MANJULA 43 11044 FEMALE ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY II 2 3 3 4 90 NIL 330 210
12 LAKSHMI 45 11270 FEMALE ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY 1 2 3 3 4 60 NIL 245 170
13 SARASU 49 11178 FEMALE FIBROID UTERUS WITH ADENOMYOSIS TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY 1 2 3 3 4 90 NIL 366 270
14 VASUKI 45 11478 FEMALE FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY II 2 3 3 5 60 NIL 380 285
15 MARIAMMAL 44 11576 FEMALE ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY 1 2 3 3 4 90 NIL 283 195
16 JEBITHA 36 11860 FEMALE FIBROID POLYP TOTAL ABDOMINAL HYSTERECTOMY 1 2 3 3 4 60 NIL 405 240
17 YASODHA 50 11664 FEMALE FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY II 3 4 3 5 90 NIL 365 180
18 JAYANTHI 47 11528 FEMALE ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY II 3 4 3 5 60 NIL 517 285
19 PRABHA 42 11222 FEMALE ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY 1 3 4 3 5 60 NIL 333 185
20 SEETHA LAKSHMI 40 11004 FEMALE FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY II 2 3 3 4 75 NIL 391 205
21 RADHA 38 11288 FEMALE FIBROID POLYP TOTAL ABDOMINAL HYSTERECTOMY 1 3 3 3 5 60 NIL 390 240
22 LAKSHMI 45 11478 FEMALE ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY 1 3 3 3 4 60 NIL 366 240
23 MEENAKSHI 40 11565 FEMALE FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY 1 2 3 3 5 45 NIL 371 180
24 LOGANAYAKI 36 11666 FEMALE ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY II 3 4 3 5 45 NIL 350 190
25 VALLIYAMMAL 44 11462 FEMALE FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY 1 3 4 3 5 45 NIL 368 200
26 PARVATHY 48 11566 FEMALE ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY II 3 4 3 4 60 NIL 365 185
27 DEVAKY 46 11448 FEMALE FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY 1 3 5 3 5 75 NIL 366 180
28 CHITRA 36 11230 FEMALE FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY 1 2 3 3 4 60 NIL 290 240
29 DHANALAKSHMI 44 11151 FEMALE ABNORMAL UTERINE BLEEDING TOTAL ABDOMINAL HYSTERECTOMY WITH BILATERAL SALPHINGOOPHERECTOMY 1 2 3 3 5 45 NIL 350 195
30 EZHILLARASI 40 11640 FEMALE FIBROID UTERUS TOTAL ABDOMINAL HYSTERECTOMY II 2 4 3 4 60 NIL 300 175
IP NORESCUE
ANALGESIA(In Mins)
ONSET OF SENSORY BLOCKS (In Mins)
ONSET OF MOTOR BLOCK (In Mins)
S.NO NAME AGE SEX DIAGNOSIS PROCEDUREASA
GROUP
DURATION OF SURGERY (In Mins )

BASE LINE (In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Mins)
45 (In Mins)
60 (In Mins)
65 (In Mins)
70 (In Mins)
75 (In Mins)
90 (In Mins)
1 SUMATHI 42 11250 FEMALE 78 76 74 72 68 70 71 72 76 75 73 70 69 -2 GLORY PREMKUMARI 50 110765 FEMALE 82 74 72 74 75 70 66 64 65 69 70 72 73 -3 PUSHPALATHA 35 11362 FEMALE 90 72 73 74 70 68 69 67 70 70 - - - -4 MUNIYAMMAL 45 11170 FEMALE 86 75 74 73 72 63 65 66 64 62 65 66 67 725 MALARVIZHI 40 11272 FEMALE 84 77 74 73 72 68 69 70 72 - - - - -6 DEVI 30 11370 FEMALE 83 80 78 76 75 72 70 68 69 71 - - - -7 DAISY RANI 52 11544 FEMALE 79 82 80 78 79 76 77 72 70 71 - - - -8 JOYSEE 43 11088 FEMALE 76 86 72 71 78 80 76 72 77 75 - - - -9 SHANTHI MANI 45 11292 FEMALE 80 84 80 78 79 76 74 73 72 70 71 69 71 -
10 MALA 43 11380 FEMALE 72 75 73 72 68 69 71 73 75 77 79 80 81 8211 MANJULA 43 11044 FEMALE 73 72 70 68 69 71 72 75 74 73 72 70 74 7512 LAKSHMI 45 11270 FEMALE 76 70 68 72 73 74 75 77 78 70 - - - -13 SARASU 49 11178 FEMALE 75 76 72 74 75 77 76 71 69 68 70 73 75 7214 VASUKI 45 11478 FEMALE 77 80 78 77 76 74 73 72 70 69 - - - -15 MARIAMMAL 44 11576 FEMALE 78 82 78 79 76 75 73 72 70 69 72 70 69 7516 JEBITHA 36 11860 FEMALE 84 88 84 83 80 81 79 75 73 72 - - - -17 YASODHA 50 11664 FEMALE 85 82 80 79 76 75 74 72 70 69 71 73 75 7318 JAYANTHI 47 11528 FEMALE 86 80 78 76 74 70 68 65 67 70 - - - -19 PRABHA 42 11222 FEMALE 87 80 77 76 72 77 73 74 75 74 - - - -20 SEETHA LAKSHMI 40 11004 FEMALE 90 87 85 84 82 70 68 67 65 80 81 83 82 -21 RADHA 38 11288 FEMALE 88 82 80 84 83 78 72 70 79 72 - - - -22 LAKSHMI 45 11478 FEMALE 86 80 84 83 80 72 74 76 77 73 - - - -23 MEENAKSHI 40 11565 FEMALE 82 79 75 73 68 65 69 70 71 - - - - -24 LOGANAYAKI 36 11666 FEMALE 85 76 74 70 71 72 73 77 78 - - - - -25 VALLIYAMMAL 44 11462 FEMALE 84 74 72 70 69 68 66 70 71 - - - - -26 PARVATHY 48 11566 FEMALE 80 78 76 74 77 79 80 74 70 71 - - - -27 DEVAKY 46 11448 FEMALE 79 72 70 68 66 65 64 67 62 65 66 67 68 -28 CHITRA 36 11230 FEMALE 78 70 69 71 73 74 76 77 74 72 - - - -29 DHANALAKSHMI 44 11151 FEMALE 86 76 75 72 74 70 69 66 62 - - - - -30 EZHILLARASI 40 11640 FEMALE 84 77 74 73 72 70 79 74 75 77 - - - -
S.NO NAMES HEART RATEGROUP F FENTANYL GROUP
AGE SEXIP NO

BASE LINE(In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
30 (In Min)
45 (In Mins)
60 (In Mins)
75 (In Mins)
90 (In Mins)
1 SUMATHI 42 11250 FEMALE 136/70 130/68 124/70 120/68 114/64 110/70 112/72 108/70 110/72 108/702 GLORY PREMKUMARI 50 110765 FEMALE 128/74 126/76 120/72 116/54 110/70 114/70 118/72 116/70 112/58 108/683 PUSHPALATHA 35 11362 FEMALE 110/64 112/70 106/64 102/60 98/62 94/60 98/64 100/64 102/684 MUNIYAMMAL 45 11170 FEMALE 148/90 136/88 130/80 122/76 108/68 100/60 99/64 90/60 100/60 101/54 104/685 MALARVIZHI 40 11272 FEMALE 132/80 136/82 126/76 116/70 104/62 98/60 94/58 100/606 DEVI 30 11370 FEMALE 133/70 130/68 124/70 120/68 114/64 110/70 112/72 108/70 110/727 DAISY RANI 52 11544 FEMALE 142/87 138/75 130/73 126/75 120/70 118/65 120/70 118/68 112/708 JOYSEE 43 11088 FEMALE 134/69 126/72 118/67 115/67 118/67 115/69 110/70 112/68 105/659 SHANTHI MANI 45 11292 FEMALE 128/68 130/70 132/72 128/71 120/70 118/67 110/65 115/72 110/70 114/71
10 MALA 43 11380 FEMALE 120/70 128/72 126/68 130/70 115/65 100/65 98/60 95/60 98/61 112/64 101/6211 MANJULA 43 11044 FEMALE 131/69 138/73 132/70 129/68 122/62 125/65 120/70 110/62 122/72 115/67 110/6812 LAKSHMI 45 11270 FEMALE 130/77 126/72 115/65 104/60 115/68 120/71 105/62 110/62 108/5913 SARASU 49 11178 FEMALE 138/76 125/70 115/63 100/66 98/60 92/62 100/70 124/65 118/61 108/69 112/6214 VASUKI 45 11478 FEMALE 135/85 128/75 125/74 130/72 115/70 100/64 110/69 109/74 100/7015 MARIAMMAL 44 11576 FEMALE 145/90 130/83 120/75 125/70 115/67 120/72 105/65 112/61 120/70 100/70 110/7516 JEBITHA 36 11860 FEMALE 125/72 110/70 108/64 101/65 100/60 119/66 125/70 115/74 110/6517 YASODHA 50 11664 FEMALE 136/90 136/88 130/80 122/76 108/68 100/60 105/64 112/65 100/60 101/54 104/6818 JAYANTHI 47 11528 FEMALE 120/67 118/63 105/62 95/60 99/62 90/60 108/67 120/69 112/6519 PRABHA 42 11222 FEMALE 135/85 128/75 125/74 130/72 115/70 100/64 110/69 109/74 100/7020 SEETHA LAKSHMI 40 11004 FEMALE 135/75 130/70 132/72 128/71 110/68 95/62 90/60 115/72 110/70 120/7021 RADHA 38 11288 FEMALE 125/72 110/70 108/64 101/65 100/60 119/66 125/70 115/74 110/6522 LAKSHMI 45 11478 FEMALE 130/77 126/72 115/65 104/60 115/68 120/71 105/62 110/62 108/5923 MEENAKSHI 40 11565 FEMALE 140/80 130/75 118/70 102/65 90/56 94/62 98/68 105/6224 LOGANAYAKI 36 11666 FEMALE 125/72 110/70 108/64 101/65 100/60 119/66 125/70 130/7425 VALLIYAMMAL 44 11462 FEMALE 132/80 136/82 126/76 116/70 104/62 108/60 118/58 120/6126 PARVATHY 48 11566 FEMALE 134/69 126/72 118/67 115/67 118/67 115/69 110/70 112/68 105/6527 DEVAKY 46 11448 FEMALE 120/65 104/69 120/70 115/63 110/69 90/62 92/61 95/64 105/65 118/6028 CHITRA 36 11230 FEMALE 130/75 124/72 115/71 122/68 130/70 115/65 100/68 120/68 117/6229 DHANALAKSHMI 44 11151 FEMALE 130/74 122/62 115/68 101/61 94/57 99/59 110/62 122/6830 EZHILLARASI 40 11640 FEMALE 134/69 126/72 118/67 115/67 118/67 115/69 110/70 112/68 105/65
BLOOD PRESSURE(SBP/DBP)S.NO NAMES AGE SEXIP NO
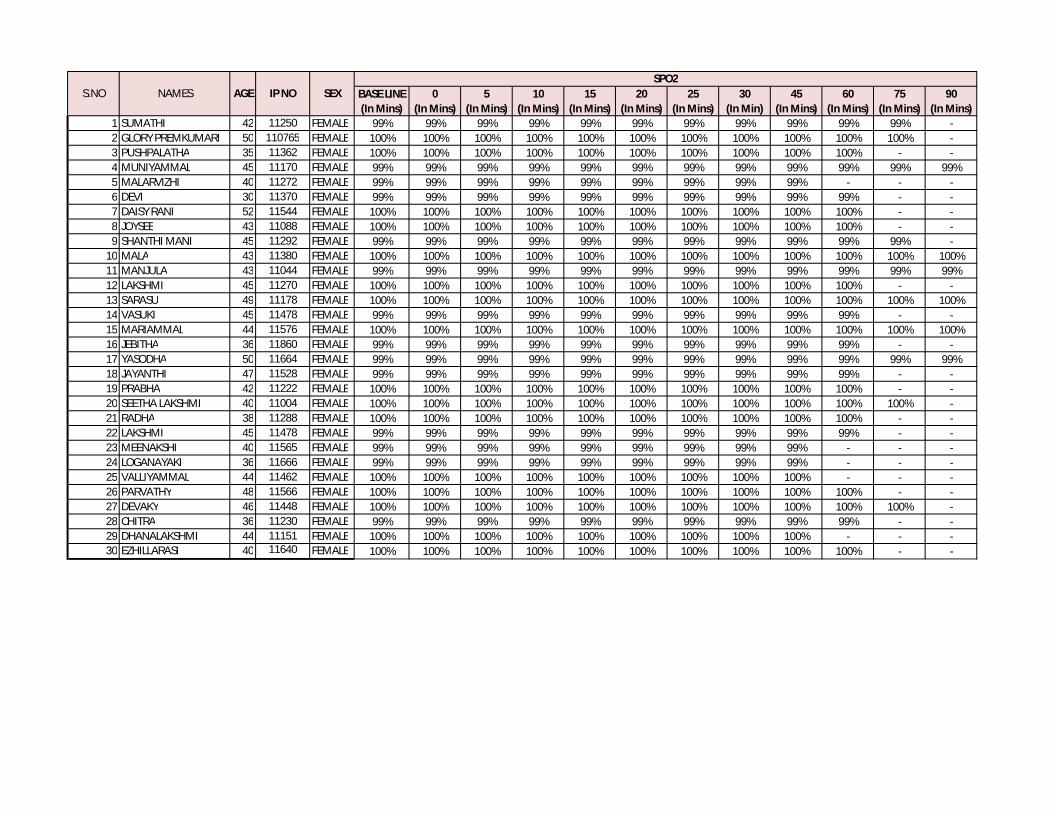
BASE LINE(In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Min)
45 (In Mins)
60 (In Mins)
75 (In Mins)
90 (In Mins)
1 SUMATHI 42 11250 FEMALE 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% -2 GLORY PREMKUMARI 50 110765 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% -3 PUSHPALATHA 35 11362 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% - -4 MUNIYAMMAL 45 11170 FEMALE 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%5 MALARVIZHI 40 11272 FEMALE 99% 99% 99% 99% 99% 99% 99% 99% 99% - - -6 DEVI 30 11370 FEMALE 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% - -7 DAISY RANI 52 11544 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% - -8 JOYSEE 43 11088 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% - -9 SHANTHI MANI 45 11292 FEMALE 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% -
10 MALA 43 11380 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%11 MANJULA 43 11044 FEMALE 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%12 LAKSHMI 45 11270 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% - -13 SARASU 49 11178 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%14 VASUKI 45 11478 FEMALE 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% - -15 MARIAMMAL 44 11576 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%16 JEBITHA 36 11860 FEMALE 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% - -17 YASODHA 50 11664 FEMALE 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%18 JAYANTHI 47 11528 FEMALE 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% - -19 PRABHA 42 11222 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% - -20 SEETHA LAKSHMI 40 11004 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% -21 RADHA 38 11288 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% - -22 LAKSHMI 45 11478 FEMALE 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% - -23 MEENAKSHI 40 11565 FEMALE 99% 99% 99% 99% 99% 99% 99% 99% 99% - - -24 LOGANAYAKI 36 11666 FEMALE 99% 99% 99% 99% 99% 99% 99% 99% 99% - - -25 VALLIYAMMAL 44 11462 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% - - -26 PARVATHY 48 11566 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% - -27 DEVAKY 46 11448 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% -28 CHITRA 36 11230 FEMALE 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% - -29 DHANALAKSHMI 44 11151 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% - - -30 EZHILLARASI 40 11640 FEMALE 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% - -
AGE SEXSPO2
S.NO NAMES IP NO

Baseline (In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Mins)
45 (In Mins)
60 (In Mins)
75 (In Mins)
90 (In Mins)
1 SUMATHI 42 11250 FEMALE 0 0 0 0 0 0 1 1 2 3 - -2 GLORY PREMKUMARI 50 110765 FEMALE 0 0 0 0 0 0 1 2 3 - - -3 PUSHPALATHA 35 11362 FEMALE 0 0 0 0 0 0 1 1 2 3 - -4 MUNIYAMMAL 45 11170 FEMALE 0 0 0 0 0 0 1 1 2 2 3 -5 MALARVIZHI 40 11272 FEMALE 0 0 0 0 0 1 2 3 - - - -6 DEVI 30 11370 FEMALE 0 0 0 0 0 0 1 2 2 3 - -7 DAISY RANI 52 11544 FEMALE 0 0 0 0 0 0 1 1 2 2 3 -8 JOYSEE 43 11088 FEMALE 0 0 0 0 0 0 1 1 2 3 - -9 SHANTHI MANI 45 11292 FEMALE 0 0 0 0 0 0 1 1 2 2 3 -
10 MALA 43 11380 FEMALE 0 0 0 0 0 0 1 1 2 3 - -11 MANJULA 43 11044 FEMALE 0 0 0 0 0 0 1 2 3 - - -12 LAKSHMI 45 11270 FEMALE 0 0 0 0 0 0 1 2 2 3 - -13 SARASU 49 11178 FEMALE 0 0 0 0 0 1 2 3 - - - -14 VASUKI 45 11478 FEMALE 0 0 0 0 0 0 1 2 2 3 - -15 MARIAMMAL 44 11576 FEMALE 0 0 0 0 0 0 1 1 2 3 - -16 JEBITHA 36 11860 FEMALE 0 0 0 0 0 0 1 1 2 2 3 -17 YASODHA 50 11664 FEMALE 0 0 0 0 0 1 2 3 - - - -18 JAYANTHI 47 11528 FEMALE 0 0 0 0 0 0 1 2 2 3 - -19 PRABHA 42 11222 FEMALE 0 0 0 0 0 0 1 2 2 3 - -20 SEETHA LAKSHMI 40 11004 FEMALE 0 0 0 0 0 0 1 2 3 - - -21 RADHA 38 11288 FEMALE 0 0 0 0 0 0 1 1 2 2 3 -22 LAKSHMI 45 11478 FEMALE 0 0 0 0 0 0 1 2 2 3 - -23 MEENAKSHI 40 11565 FEMALE 0 0 0 0 0 0 1 2 3 - - -24 LOGANAYAKI 36 11666 FEMALE 0 0 0 0 0 0 1 1 2 2 3 -25 VALLIYAMMAL 44 11462 FEMALE 0 0 0 0 0 0 1 2 2 3 - -26 PARVATHY 48 11566 FEMALE 0 0 0 0 0 0 1 2 3 - - -27 DEVAKY 46 11448 FEMALE 0 0 0 0 0 0 1 2 3 - - -28 CHITRA 36 11230 FEMALE 0 0 0 0 0 0 1 1 2 2 3 -29 DHANALAKSHMI 44 11151 FEMALE 0 0 0 0 0 0 1 1 2 3 - -30 EZHILLARASI 40 11640 FEMALE 0 0 0 0 0 0 1 2 2 3 - -
AGE SEX
GROUP A - FENTANYL(Post operative analgesia initiation time)
S.NO NAMESVISUAL ANALOG SCALE
IP NO

Baseline (In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Mins)
45 (In Mins)
60 (In Mins)
75 (In Mins)
90 (In Mins)
1 SUMATHI 42 11250 FEMALE 72 72 72 72 73 73 75 78 84 90 - -2 GLORY PREMKUMARI 50 110765 FEMALE 74 74 74 74 76 78 80 87 89 - - -3 PUSHPALATHA 35 11362 FEMALE 74 74 74 74 76 76 79 79 84 92 - -4 MUNIYAMMAL 45 11170 FEMALE 72 72 72 72 72 72 75 77 80 85 93 -5 MALARVIZHI 40 11272 FEMALE 73 73 73 73 75 79 84 92 - - - -6 DEVI 30 11370 FEMALE 72 72 72 72 72 72 75 80 83 94 - -7 DAISY RANI 52 11544 FEMALE 70 70 70 70 70 70 75 79 83 85 95 -8 JOYSEE 43 11088 FEMALE 73 73 73 73 73 73 77 80 85 94 - -9 SHANTHI MANI 45 11292 FEMALE 74 74 74 74 74 74 75 80 83 87 94 -
10 MALA 43 11380 FEMALE 72 72 72 72 72 72 75 80 84 92 - -11 MANJULA 43 11044 FEMALE 75 75 75 75 75 75 80 85 89 - - -12 LAKSHMI 45 11270 FEMALE 70 70 70 70 70 70 75 80 84 94 - -13 SARASU 49 11178 FEMALE 73 73 73 73 75 79 85 91 - - - -14 VASUKI 45 11478 FEMALE 72 72 72 72 72 72 77 83 85 92 - -15 MARIAMMAL 44 11576 FEMALE 74 74 74 74 74 74 75 80 84 93 - -16 JEBITHA 36 11860 FEMALE 71 71 71 71 71 71 75 80 83 85 94 -17 YASODHA 50 11664 FEMALE 73 73 73 73 73 79 85 91 - - - -18 JAYANTHI 47 11528 FEMALE 72 72 72 72 72 72 77 83 85 94 - -19 PRABHA 42 11222 FEMALE 72 72 72 72 72 72 77 83 85 93 - -20 SEETHA LAKSHMI 40 11004 FEMALE 71 71 71 71 71 71 75 80 87 - - -21 RADHA 38 11288 FEMALE 70 70 70 70 70 70 75 80 83 85 93 -22 LAKSHMI 45 11478 FEMALE 74 74 74 74 74 74 77 83 85 94 - -23 MEENAKSHI 40 11565 FEMALE 71 71 71 71 71 71 77 85 93 - - -24 LOGANAYAKI 36 11666 FEMALE 72 72 72 72 72 72 75 80 84 87 95 -25 VALLIYAMMAL 44 11462 FEMALE 71 71 71 71 71 71 75 80 83 94 - -26 PARVATHY 48 11566 FEMALE 74 74 74 74 74 74 78 84 90 - - -27 DEVAKY 46 11448 FEMALE 72 74 74 74 74 74 77 85 92 - - -28 CHITRA 36 11230 FEMALE 70 70 70 70 70 70 75 80 83 85 94 -29 DHANALAKSHMI 44 11151 FEMALE 74 74 74 74 74 74 80 80 85 92 - -30 EZHILLARASI 40 11640 FEMALE 71 71 71 71 71 74 77 85 89 94 - -
AGE SEXHEART RATE
SNO NAMES IP NO
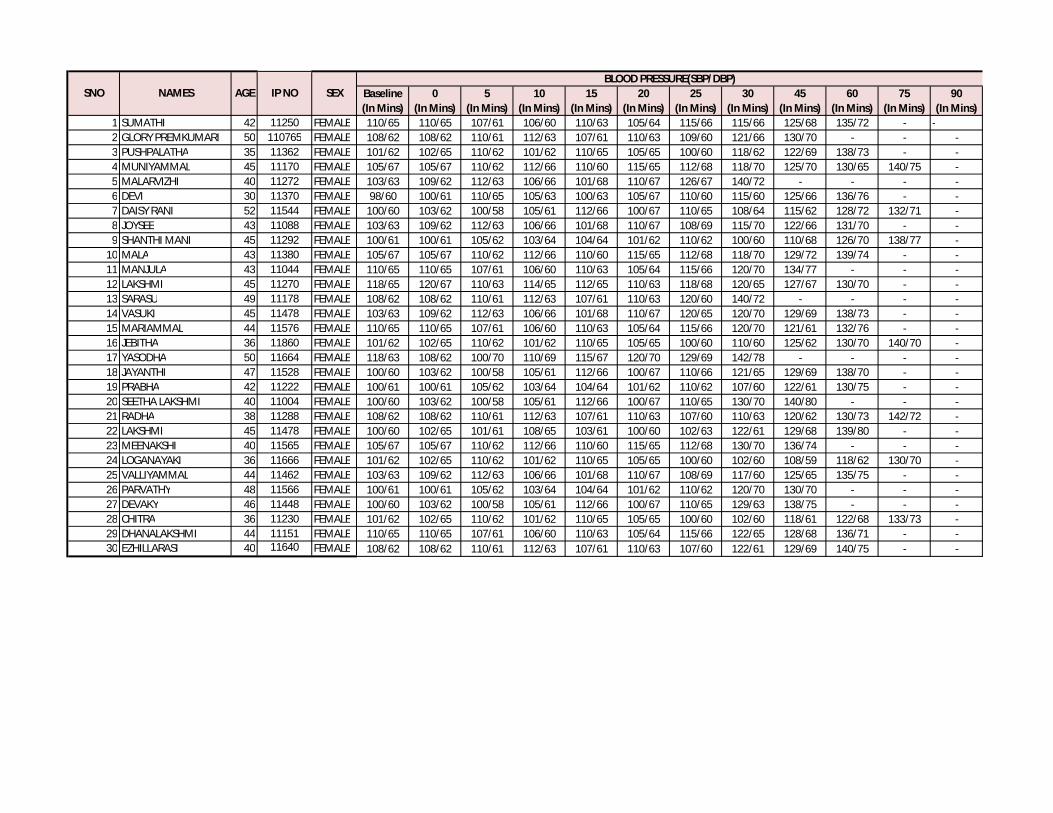
Baseline (In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Mins)
45 (In Mins)
60 (In Mins)
75 (In Mins)
90 (In Mins)
1 SUMATHI 42 11250 FEMALE 110/65 110/65 107/61 106/60 110/63 105/64 115/66 115/66 125/68 135/72 - -2 GLORY PREMKUMARI 50 110765 FEMALE 108/62 108/62 110/61 112/63 107/61 110/63 109/60 121/66 130/70 - - -3 PUSHPALATHA 35 11362 FEMALE 101/62 102/65 110/62 101/62 110/65 105/65 100/60 118/62 122/69 138/73 - -4 MUNIYAMMAL 45 11170 FEMALE 105/67 105/67 110/62 112/66 110/60 115/65 112/68 118/70 125/70 130/65 140/75 -5 MALARVIZHI 40 11272 FEMALE 103/63 109/62 112/63 106/66 101/68 110/67 126/67 140/72 - - - -6 DEVI 30 11370 FEMALE 98/60 100/61 110/65 105/63 100/63 105/67 110/60 115/60 125/66 136/76 - -7 DAISY RANI 52 11544 FEMALE 100/60 103/62 100/58 105/61 112/66 100/67 110/65 108/64 115/62 128/72 132/71 -8 JOYSEE 43 11088 FEMALE 103/63 109/62 112/63 106/66 101/68 110/67 108/69 115/70 122/66 131/70 - -9 SHANTHI MANI 45 11292 FEMALE 100/61 100/61 105/62 103/64 104/64 101/62 110/62 100/60 110/68 126/70 138/77 -
10 MALA 43 11380 FEMALE 105/67 105/67 110/62 112/66 110/60 115/65 112/68 118/70 129/72 139/74 - -11 MANJULA 43 11044 FEMALE 110/65 110/65 107/61 106/60 110/63 105/64 115/66 120/70 134/77 - - -12 LAKSHMI 45 11270 FEMALE 118/65 120/67 110/63 114/65 112/65 110/63 118/68 120/65 127/67 130/70 - -13 SARASU 49 11178 FEMALE 108/62 108/62 110/61 112/63 107/61 110/63 120/60 140/72 - - - -14 VASUKI 45 11478 FEMALE 103/63 109/62 112/63 106/66 101/68 110/67 120/65 120/70 129/69 138/73 - -15 MARIAMMAL 44 11576 FEMALE 110/65 110/65 107/61 106/60 110/63 105/64 115/66 120/70 121/61 132/76 - -16 JEBITHA 36 11860 FEMALE 101/62 102/65 110/62 101/62 110/65 105/65 100/60 110/60 125/62 130/70 140/70 -17 YASODHA 50 11664 FEMALE 118/63 108/62 100/70 110/69 115/67 120/70 129/69 142/78 - - - -18 JAYANTHI 47 11528 FEMALE 100/60 103/62 100/58 105/61 112/66 100/67 110/66 121/65 129/69 138/70 - -19 PRABHA 42 11222 FEMALE 100/61 100/61 105/62 103/64 104/64 101/62 110/62 107/60 122/61 130/75 - -20 SEETHA LAKSHMI 40 11004 FEMALE 100/60 103/62 100/58 105/61 112/66 100/67 110/65 130/70 140/80 - - -21 RADHA 38 11288 FEMALE 108/62 108/62 110/61 112/63 107/61 110/63 107/60 110/63 120/62 130/73 142/72 -22 LAKSHMI 45 11478 FEMALE 100/60 102/65 101/61 108/65 103/61 100/60 102/63 122/61 129/68 139/80 - -23 MEENAKSHI 40 11565 FEMALE 105/67 105/67 110/62 112/66 110/60 115/65 112/68 130/70 136/74 - - -24 LOGANAYAKI 36 11666 FEMALE 101/62 102/65 110/62 101/62 110/65 105/65 100/60 102/60 108/59 118/62 130/70 -25 VALLIYAMMAL 44 11462 FEMALE 103/63 109/62 112/63 106/66 101/68 110/67 108/69 117/60 125/65 135/75 - -26 PARVATHY 48 11566 FEMALE 100/61 100/61 105/62 103/64 104/64 101/62 110/62 120/70 130/70 - - -27 DEVAKY 46 11448 FEMALE 100/60 103/62 100/58 105/61 112/66 100/67 110/65 129/63 138/75 - - -28 CHITRA 36 11230 FEMALE 101/62 102/65 110/62 101/62 110/65 105/65 100/60 102/60 118/61 122/68 133/73 -29 DHANALAKSHMI 44 11151 FEMALE 110/65 110/65 107/61 106/60 110/63 105/64 115/66 122/65 128/68 136/71 - -30 EZHILLARASI 40 11640 FEMALE 108/62 108/62 110/61 112/63 107/61 110/63 107/60 122/61 129/69 140/75 - -
SNO NAMES AGE SEXBLOOD PRESSURE(SBP/DBP)
IP NO
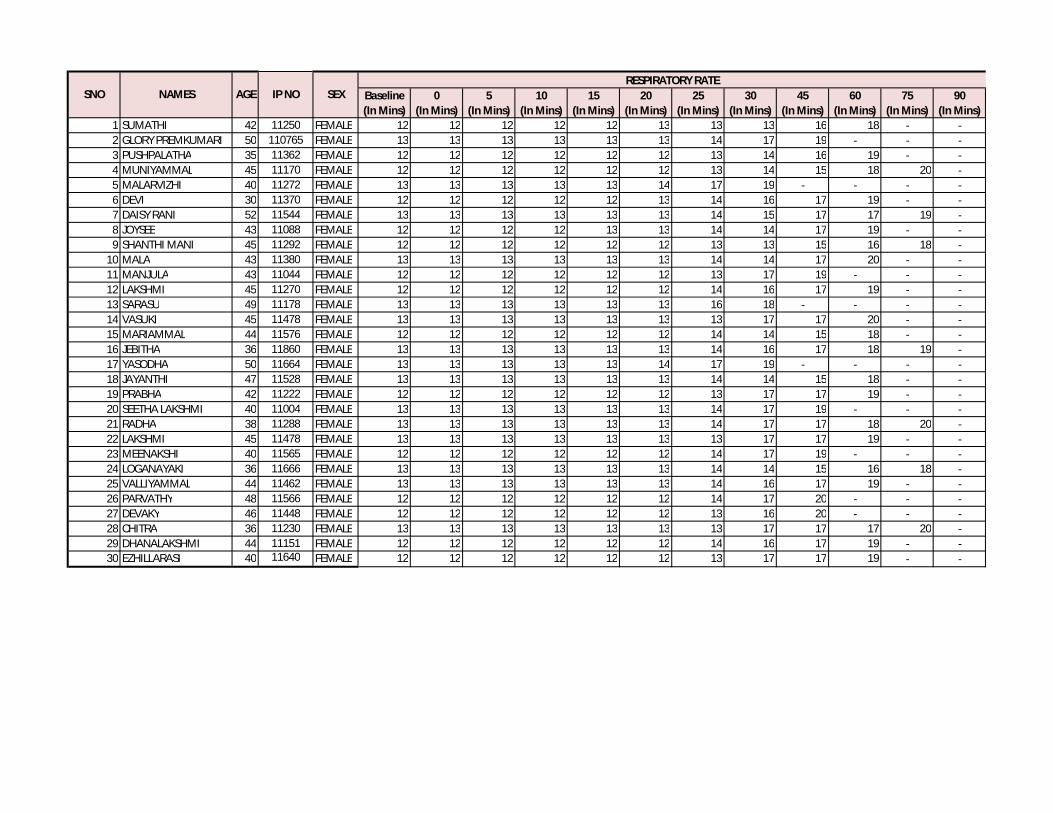
Baseline (In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Mins)
45 (In Mins)
60 (In Mins)
75 (In Mins)
90 (In Mins)
1 SUMATHI 42 11250 FEMALE 12 12 12 12 12 13 13 13 16 18 - -2 GLORY PREMKUMARI 50 110765 FEMALE 13 13 13 13 13 13 14 17 19 - - -3 PUSHPALATHA 35 11362 FEMALE 12 12 12 12 12 12 13 14 16 19 - -4 MUNIYAMMAL 45 11170 FEMALE 12 12 12 12 12 12 13 14 15 18 20 -5 MALARVIZHI 40 11272 FEMALE 13 13 13 13 13 14 17 19 - - - -6 DEVI 30 11370 FEMALE 12 12 12 12 12 13 14 16 17 19 - -7 DAISY RANI 52 11544 FEMALE 13 13 13 13 13 13 14 15 17 17 19 -8 JOYSEE 43 11088 FEMALE 12 12 12 12 13 13 14 14 17 19 - -9 SHANTHI MANI 45 11292 FEMALE 12 12 12 12 12 12 13 13 15 16 18 -
10 MALA 43 11380 FEMALE 13 13 13 13 13 13 14 14 17 20 - -11 MANJULA 43 11044 FEMALE 12 12 12 12 12 12 13 17 19 - - -12 LAKSHMI 45 11270 FEMALE 12 12 12 12 12 12 14 16 17 19 - -13 SARASU 49 11178 FEMALE 13 13 13 13 13 13 16 18 - - - -14 VASUKI 45 11478 FEMALE 13 13 13 13 13 13 13 17 17 20 - -15 MARIAMMAL 44 11576 FEMALE 12 12 12 12 12 12 14 14 15 18 - -16 JEBITHA 36 11860 FEMALE 13 13 13 13 13 13 14 16 17 18 19 -17 YASODHA 50 11664 FEMALE 13 13 13 13 13 14 17 19 - - - -18 JAYANTHI 47 11528 FEMALE 13 13 13 13 13 13 14 14 15 18 - -19 PRABHA 42 11222 FEMALE 12 12 12 12 12 12 13 17 17 19 - -20 SEETHA LAKSHMI 40 11004 FEMALE 13 13 13 13 13 13 14 17 19 - - -21 RADHA 38 11288 FEMALE 13 13 13 13 13 13 14 17 17 18 20 -22 LAKSHMI 45 11478 FEMALE 13 13 13 13 13 13 13 17 17 19 - -23 MEENAKSHI 40 11565 FEMALE 12 12 12 12 12 12 14 17 19 - - -24 LOGANAYAKI 36 11666 FEMALE 13 13 13 13 13 13 14 14 15 16 18 -25 VALLIYAMMAL 44 11462 FEMALE 13 13 13 13 13 13 14 16 17 19 - -26 PARVATHY 48 11566 FEMALE 12 12 12 12 12 12 14 17 20 - - -27 DEVAKY 46 11448 FEMALE 12 12 12 12 12 12 13 16 20 - - -28 CHITRA 36 11230 FEMALE 13 13 13 13 13 13 13 17 17 17 20 -29 DHANALAKSHMI 44 11151 FEMALE 12 12 12 12 12 12 14 16 17 19 - -30 EZHILLARASI 40 11640 FEMALE 12 12 12 12 12 12 13 17 17 19 - -
AGE SEXSNO NAMESRESPIRATORY RATE
IP NO

Baseline (In Mins)
0 (In Mins)
5 (In Mins)
10 (In Mins)
15 (In Mins)
20 (In Mins)
25 (In Mins)
30 (In Mins)
45 (In Mins)
60 (In Mins)
75 (In Mins)
90 (In Mins)
1 SUMATHI 42 11250 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -2 GLORY PREMKUMARI 50 110765 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Given - - - 3 Given3 PUSHPALATHA 35 11362 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - - 2 Nil4 MUNIYAMMAL 45 11170 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - 1 Nil5 MALARVIZHI 40 11272 FEMALE Nil Nil Nil Nil Nil Nil Nil Given - - - - 0 Nil6 DEVI 30 11370 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -7 DAISY RANI 52 11544 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -8 JOYSEE 43 11088 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -9 SHANTHI MANI 45 11292 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -
10 MALA 43 11380 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -11 MANJULA 43 11044 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Given - - -12 LAKSHMI 45 11270 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -13 SARASU 49 11178 FEMALE Nil Nil Nil Nil Nil Nil Nil Given - - - -14 VASUKI 45 11478 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -15 MARIAMMAL 44 11576 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -16 JEBITHA 36 11860 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -17 YASODHA 50 11664 FEMALE Nil Nil Nil Nil Nil Nil Nil Given - - - -18 JAYANTHI 47 11528 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -19 PRABHA 42 11222 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -20 SEETHA LAKSHMI 40 11004 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Given - - -21 RADHA 38 11288 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -22 LAKSHMI 45 11478 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -23 MEENAKSHI 40 11565 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Given - - -24 LOGANAYAKI 36 11666 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -25 VALLIYAMMAL 44 11462 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -26 PARVATHY 48 11566 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Given - - -27 DEVAKY 46 11448 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Given - - -28 CHITRA 36 11230 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil Given -29 DHANALAKSHMI 44 11151 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -30 EZHILLARASI 40 11640 FEMALE Nil Nil Nil Nil Nil Nil Nil Nil Nil Given - -
AGE SEXSNO NAMESRESCUE ANALGESIA
IP NO
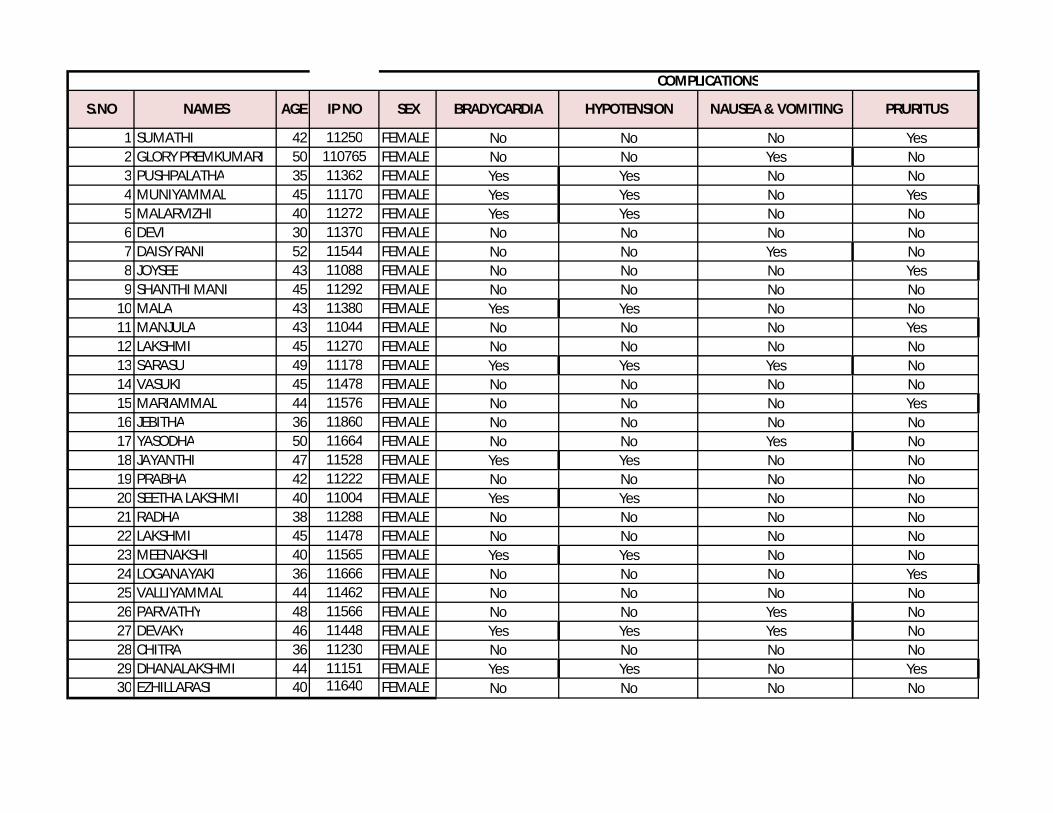
1 SUMATHI 42 11250 FEMALE No No No Yes2 GLORY PREMKUMARI 50 110765 FEMALE No No Yes No3 PUSHPALATHA 35 11362 FEMALE Yes Yes No No4 MUNIYAMMAL 45 11170 FEMALE Yes Yes No Yes5 MALARVIZHI 40 11272 FEMALE Yes Yes No No6 DEVI 30 11370 FEMALE No No No No7 DAISY RANI 52 11544 FEMALE No No Yes No8 JOYSEE 43 11088 FEMALE No No No Yes9 SHANTHI MANI 45 11292 FEMALE No No No No
10 MALA 43 11380 FEMALE Yes Yes No No11 MANJULA 43 11044 FEMALE No No No Yes12 LAKSHMI 45 11270 FEMALE No No No No13 SARASU 49 11178 FEMALE Yes Yes Yes No14 VASUKI 45 11478 FEMALE No No No No15 MARIAMMAL 44 11576 FEMALE No No No Yes16 JEBITHA 36 11860 FEMALE No No No No17 YASODHA 50 11664 FEMALE No No Yes No18 JAYANTHI 47 11528 FEMALE Yes Yes No No19 PRABHA 42 11222 FEMALE No No No No20 SEETHA LAKSHMI 40 11004 FEMALE Yes Yes No No21 RADHA 38 11288 FEMALE No No No No22 LAKSHMI 45 11478 FEMALE No No No No23 MEENAKSHI 40 11565 FEMALE Yes Yes No No24 LOGANAYAKI 36 11666 FEMALE No No No Yes25 VALLIYAMMAL 44 11462 FEMALE No No No No26 PARVATHY 48 11566 FEMALE No No Yes No27 DEVAKY 46 11448 FEMALE Yes Yes Yes No28 CHITRA 36 11230 FEMALE No No No No29 DHANALAKSHMI 44 11151 FEMALE Yes Yes No Yes30 EZHILLARASI 40 11640 FEMALE No No No No
S.NO NAMES PRURITUSNAUSEA & VOMITING
COMPLICATIONS
HYPOTENSIONBRADYCARDIAAGE SEXIP NO