Eeg Lectures 1
44
EEG Lecture Series By Dr. Stanley C. Igwe (FWACPsych) Consultant Psychiatrist Federal Neuro-Psychiatric Hospital Maiduguri-Nigeria & Clinical Fellow In Clinical Neuro- Physiology Kings College Hospital London
-
Upload
stanley-igwe -
Category
Documents
-
view
196 -
download
10
Transcript of Eeg Lectures 1

EEG Lecture Series
ByDr. Stanley C. Igwe (FWACPsych)
Consultant PsychiatristFederal Neuro-Psychiatric Hospital
Maiduguri-Nigeria&
Clinical Fellow In Clinical Neuro-PhysiologyKings College Hospital
London

EEG Lecture SeriesPart 1
• Brief History of EEG• Uses of EEG• Electrodes Invasive and Non-invasive
electrodes• Electrode Placement systems 10-20 International System Modified Maudsley System
(MMS)

What is Electroencephalogram (EEG)
• Recording of electric activities in the brain by means of electrodes applied to the scalp, to the surface of the brain, or placed within the substance of the brain
• Greek words:• Electro------------ Electrical• Encephalo------- Brain• Gram (ma)-------Picture

Historic Aspect of EEG• Hans Berger (1873-1941) was a German
psychiatrist who developed the first human EEG in 1924.
• Berger was interested in psychophysiology (the study of the relationship between mental processes and the brain) in the hope that the physiological record would provide insight into mental processes.

Hans Berger• He also discovered the alpha wave rhythm known as
"Berger's wave".
• He published his first paper on the human electroencephalogram in 1929
• Berger did not achieve an international reputation until 1934 when Edgar Douglas Adrian a renowned English neurophysiologist, confirmed Berger's findings.

Uses of EEG
• Classification of Epilepsy Syndromes• Monitoring Treatment with AED• Differentiate between epileptic and non-
epileptic events (pseudo-seizure)• Differentiate functional psychiatric syndrome
from organic ones (frontal lobe lesion, Complex Partial Seizures)
• Diagnosis of metabolic disorders and encephalopathies
• Employment and recertification

Uses of EEG
• Diagnosis of dementias (eg. 1- to 2-Hz biphasic and triphasic waves in CJD)
• Monitoring of comatose patient (alpha, spindle, beta, theta and delta coma)
• Localization of brain lesions

Uses of EEG• Use in identification and localization of gross
structural brain lesions replaced by CT and MRI, EEG remains the primary diagnostic test of brain function.
• Unlike fMRI, SPECT, and PET, EEG provides a continuous measure of cortical function with excellent time resolution
• Relatively inexpensive

The source of the EEG signal
• The neurons in the IV and V layers of the cortex have dendrites parallel to each other that generate electric signal
• This electric signal is large enough to cross through layers between the brain and the recording electrodes on the surface (CSF, bone, skin) by volume conduction


Enhancement of electric signal
• Cleaning of scalp to reduce impedance• Use of EEG/ECG electrode paste (electrolyte)
to enhance current flow

TechniqueBasic Elements Needed for EEG
1. Electrodes: to pick up the electrical activity2. Amplifier: to amplify the rhythm since the
are only in microvolt in amplitudes3. Filter: filter out very slow and fast (artifacts)
activities4. Writer unit: To record these rhythms on
paper



Electrodes
• Electrodes make the contact between the patient and the EEG machine (collect the electric input of the EEG apparatus).
• They are two broad types:• Invasive electrodes• Non-invasive electrodes

Invasive electrodesWhy use them?
• Overcomes the resistance to current flow posed by CSF, bones and skin
• Used in pre-surgical investigation for epilepsy surgery where precision is the watchword
• In patients undergoing long term video-EEG recordings using intracranial electrodes (invasive recordings).

Subdural Grids
• Usually have 16-64 electrodes embedded at uniform intervals in a sheet of flexible plastic
• Each electrode is 3 mm in diameter and is made of stainless steel or platinum.
• The grids are inserted via craniotomy while the patient is under general anaesthesia by placing them over the cortex and can record for several weeks.


Epidural strips
• have 4-8 contacts, and are implanted through burr holes in the skull

Epidural strips

Depth electrodes
• Fine wires of stainless steel, platinum or gold, ending in several un-insulated tips 5mm apart.
• They are inserted with the most distal contact located within the region of interest such as the amygdala, the hippocampus, or the orbito-frontal cortex etc.

Advantages of the invasive recordings
• The signals are not attenuated by the skull, and that the rate of artifacts is low

Disadvantage of the invasive recordings
• Samples from a part of the brain therefore a clear hypothesis of the probable epileptic focus is necessary to direct the implantation of the intracranial electrodes.
• Complications occur in 4-14% of patients implanted with invasive electrodes; these include mainly infection, transient neurologic deficit and intracranial haemorrhage

Sphenoid electrodes
• made of stainless steel, silver or platinum wires
• inserted through a needle cannula under the zygomatic arch, and the electrode tip is directed laterally to the foramen ovale to the anterior tip of the temporal lobe.
• The idea behind using the sphenoidal electrodes is record closer to the temporal pole and orbital parts of the frontal lobe

Sphenoid electrodes
• Complications include minor local discomfort, rare infections and the severing of branches of trigeminal and facial nerves.
• These electrodes are still extra-cranial, and the advantage of sphenoidal electrodes over scalp electrodes placed in this region (anterior temporal electrodes) is controversial.

Non-invasive electrodes
• The scalp electrode is the most commonly used of all electrode types in EEG
• It is made of non-polarised material (usually AgAgCl)
• The contact surface is a cupped disc of up to 10mm in diameter and is filled with electrode paste.

Electrode placement
• Several systems used in the past for electrode placement (Gibbsian, Michigan, Houston)
• Greater majority of EEG lab worldwide utilize the 10-20 International System of Electrode Placement
• The Modified Maudsley System (MMS) of electrode placement is used in the UK.

Other electrode applied in EEG recording
• ECG Leads• Respiration• EMG• EOG



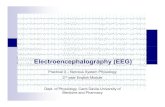
10-20 International System
• This uses stable anatomical points of the skull such as:
• Nasion: point between the forehead and nose
• Inion: bump at back of skull • Preauricular point: small fossa just anterior to
the ear canal

10-20 International System
• Distances between these skull landmarks (nasion to inion; left pre-auricular to right pre-auricular) are measured
• electrodes are spaced 10% or 20% of the total distances between them (which gives the name of this electrode placement system).

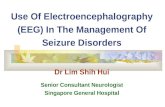
10-20 International System


10-20 International System• Each electrode is identified by two symbols: the first
is a letter – an abbreviation of the underlying region – and the second is a number.
• The alphabetical abbreviations in common use are: FP (fronto-polar), F (frontal), C (central sulcus), P (parietal), O (occipital), and T (temporal).
• Sagittal electrodes (located in the midline) have an additional letter: z (Fz, Cz, and Pz).

• By convention, even-numbered electrodes are located on the right side of the head, and odd-numbered electrodes on the left.
• F7 and F8 are situated close not only to the
frontal cortex (as indicated by their names), but also to the pole of the temporal lobe (thus they record signals from the temporal lobe too).

10-20 International System
• As a minimum standard, 19 electrodes should be used.
• A more dense electrode placement can be achieved by the 10-10 system (modified combinatorial nomenclature), an extension of the 10-20 system, with additional half-distance electrodes located between the ones previously described.

10-10 International System

10-20 International system and MMS compared
• Symmetry: • MMS treat each hemisphere independently
and this adapt to cranial asymmetries
• 10-20 assume perfect symmetry of scalp convexities allowing uniform electrode placement but accuracy may be compromised by cranial asymmetry


Convexity coverage


Universality
• Use of 10-20 international system is universal allowing comparison of data by different labs
• MMS is less universal

Summary
• EEG records the brain electrical activities• First recording by Hans Berger in 1924• EEG electric signals generated from IV & V layer
of the cerebral cortex, transmitted to the scalp by volume conduction
• Signals picked up by electrode, amplified, filtered and the writer unit record the rhythm on paper
• Electrode placement can be invasive or non-invasive
• Although 10-20 system is more universal, MMS covers the lower brain.