Educational Innovation in the Augusta University Internal ...
57
EDUCATIONAL INNOVATION IN THE AUGUSTA UNIVERSITY INTERNAL MEDICINE RESIDENCY By: Thaddeus Y. Carson, FACP, MD Clerkship Director, Associate Program Director and Assistant Professor in the Department of Internal Medicine at Augusta University
Transcript of Educational Innovation in the Augusta University Internal ...

EDUCATIONAL INNOVATION IN THE AUGUSTA UNIVERSITY INTERNAL
MEDICINE RESIDENCYBy: Thaddeus Y. Carson, FACP, MD
Clerkship Director, Associate Program Director and
Assistant Professor in the Department of Internal Medicine
at Augusta University

Disclosure
■ Dr. Carson reports no actual or potential conflicts of interest in relation to this
program or presentation.

CME Information■ Completion and submission of the evaluation with identification of take home strategies are required for CME
credit awards.
■ This activity requires one hour for completion.
■ This CME activity was planned and produced in accordance with the ACCME Essentials.
■ The GRU Medical College of Georgia is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
■ The GRU Medical College of Georgia designates this educational activity for a maximum of 1 AMA PRA Category 1 Credit™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
■ Other Health Care Professionals: This course offers 1 Continuing Education Contact Hour by the Georgia Regents University.
■ Original release date: 12/6/2016
■ Expiration date: 12/6/2017

Objectives of Presentation
■ Determine what makes an effective noon conference curriculum
■ Define and explain the advantages of a 4+2 scheduling system
■ Describe the Internal Medicine Residency’s Medical Economics Curriculum
■ Recognize the advantages of a blended learning environment on the Internal
Medicine inpatient wards

IMPLEMENTING AN ACCESSIBLE AND EFFECTIVE INTERNAL
MEDICINE RESIDENCY NOON CONFERENCE CURRICULUM
By: Thaddeus Y. Carson, MD, FACP
Clerkship Director, Associate Program Director and
Assistant Professor in the Department of Internal Medicine
at Augusta University

Background
■ Board Pass Rate
■ Variability in Noon Conference Educational Value for Board Preparation
■ Missing Nightfloat Education

3 Part Plan for Addressing Accessibility and Effectiveness
■ Part 1: Standardization of Noon Conference
Lecture Material
■ Part 2: Accessibility
■ Part 3: Measures of Effectiveness/
Accountability

3 Part Plan for Addressing Accessibility and Effectiveness
■ Part 1: Standardization of Noon Conference
Lecture Material

Part 1: Standardization of Noon Conference Lecture Material
■ Now based on American Board of Internal Medicine board certification examination
blueprint.

ABIM Blueprint

ABIM Blueprint

Part 1: Standardization of Noon Conference Lecture Material
■ Now based on American Board of Internal Medicine board certification examination blueprint.
■ Moved to 18 month curriculum so the entire curriculum repeats twice during residency and gives more time to spend covering the ABIM topics
■ Coordination of Lecturers by Division Chiefs.
■ Strong Departmental “buy-in”.


3 Part Plan for Addressing Accessibility and Effectiveness
■ Part 1: Standardization of Noon Conference
Lecture Material
■ Part 2: Accessibility

Part 2: Accessibility

Part 2: Accessibility
■ Possible Future project:
– Allowing attendance credit to those who watch noon conferences online.

3 Part Plan for Addressing Accessibility and Effectiveness
■ Part 1: Standardization of Noon Conference
Lecture Material
■ Part 2: Accessibility
■ Part 3: Measures of Effectiveness/
Accountability

Part 3: Measures of Effectiveness
■ Continue Annual ABIM In-Service Exams and tracking ABIM Board Certification pass
percentages.
■ 2nd/3rd Year MKSAP Reading/Questions
■ End of Block MedStudy Quizzes

Part 3: Measures of Effectiveness

Quiz Results



Part 3: Measures of Effectiveness
■ Continue Annual ABIM In-Service Exams and tracking ABIM Board Certification pass
percentages.
■ 2nd/3rd Year MKSAP Reading/Questions
■ End of Block MedStudy Quizzes

3 Part Plan for Addressing Accessibility and Effectiveness
■ Part 1: Standardization of Noon Conference
Lecture Material
■ Part 2: Accessibility
■ Part 3: Measures of Effectiveness/
Accountability

4+2 SCHEDULING SYSTEM
By: Thaddeus Y. Carson, MD, FACP
Lee Ann Merchen, MD, FACP

Distinctives that set GRU apart: 4 + 2

How’d we come up with 4 + 2?
■ IV.A.1.b) Residency training is primarily an educational experience in
■ patient-centered care. The educational efforts of faculty and
■ residents should enhance the quality of patient care, and the
■ education of the residents. At least 1/3 of the residency training
must occur in the ambulatory setting and at least 1/3 must occur in
the inpatient setting. Emergency medicine may count for no more
■ than two weeks toward the required 1/3 ambulatory time. (Detail)

Pop Quiz: What is 4 + 2?
■ A: Six
■ B: Trick question…..
■ C: Schedule that allows dedicated
outpatient time for “real life”
experience
■ D: Something Merchen made up....
28

Pop Quiz: What is 4 + 2?
■ A: Six
■ B: Trick question…..
■ C: Schedule that allows dedicated
outpatient time for “real life”
experience
■ D: Something Merchen made up....
29


Benefits of 4 + 2
From our residents:
■ No more interruptions in the
outpatient practice
■ I have clear, dedicated outpatient
elective time
■ The ability to have a block of time
dedicated to outpatient care! I love
the curriculum
From our patients:
■ I know I can see my doctor in the
morning or the afternoon
■ My results are given to me right
away!
■ My care is thorough and detailed
■ Firms of “Care” mean someone can
always take care of me.
31

Challenges of 4 +2
Schedules!
■ Within groups, schedules can be
tight
■ Complete equality is not possible;
some will have more outpatient plus
2 than others
■ The only “back up” resident is on
+2
Outpatient
■ Are two days every six weeks
adequate outpatient care?
Residents interested in primary care
are seeking more time
■ Is patient follow up reasonable in
this “tempo” of training?

MEDICAL ECONOMICS AND PRACTICE MANAGEMENT
12.6.16
David J. Fallaw, MD
Chief Medical Information Officer

Medical Economics
• How do I negotiate a contract?
• When do I learn coding and
billing?
• What percentage of the GDP is
spent on health care in the US?
• How much is that MRI?
• Why does that Band-aid cost
$15?
I didn’t know
insurers could do
that!!
Yes I can
negotiate like
that!

Medical Economics CurriculumHealth Policy
• Medical Terminology
• US Healthcare System—Overview
• US Healthcare System—HMO/MCOs/Insurance
• US Healthcare System—CMS and the RUC
• International Healthcare Systems
• Accountable Care Organizations
• Healthcare Reform/Affordable Care Act
• Core Measures
• Pay for Performance
• Meaningful Use/MACRA/MIPS
• Fraud and Abuse Law
The Cost Conundrum
• Value Based Medicine
• Cost of Medicine
• Value Based Purchasing (HCAPS & Quality
Measures)
Medical Legal
• Medical Errors and Sentinel Events
• Quality Improvement
• Tort Liability and Risk Management
• Contract Law
• Employment Law
Practice Management
• Billing and Coding
• RVUs/DRGs
• Basic Accounting and Practice Expense
• Measuring Physician Productivity
• EHRs & the Impact of Technologies in Practice
• Choosing a Practice: Market Analysis and
Projecting Practice Success
• Patient Centered Medical Home
• The Medical Interview
• Credentialing
• Curriculum Vitae
• Employee Benefits
• VA vs. Private Practice Medicine
• Academic Medicine
• Hospital Medicine
• Alternative Practices (Concierge)
• Time Management and Improving Efficiency
• Recruiting and Keeping Staff
• Scheduling and Front Desk Operations
• Healthcare Informatics
Financial Planning
• Future Financial Planning
• Managing Medical School Loans

Medical Economics CurriculumACP Legislative Day at the Capital
Practice Site Visits/Discussions as available
• Center for Primary Care
• Southern Family Care
• Christ Community Clinic (FQHC)
• University Hospitalists
• Aiken Internal Medicine
• Nephrology Associates of Augusta
Exercises in Billing and Coding Improvement
Future
• Collaborate with TRP to initiate a resident driven Quality Improvement Research Project

New Patient Visit (Outpatient)
CPT 99201 99202 99203 99204 99205
CC
HPI
ROS
PFSH
1 1
1
1-3/1-2 pb*
2-9
1
4/3+ prob*
10+
3
4/3+ prob*
10+
3
Exam 1 2+ 5+ 8+ 8+
MDM 2/3
#Dx
Data
Risk
1
0
No meds
1
0
No meds
2
2
1 stable prob
2+ minor
prob
1 new no w/u
or 3 stable
3
Rx med; refer
to Risk List
1 new c W/U,
2+ worse, 4+
4
Life
threatening
MDM Straight-
forward
Straight-
forward
Low Moderate High
Time 10 20 30 45 60
3/3 Parts needed; *”status of”

Return Patient Visit (Outpatient)
CPT 99211 99212 99213 99214 99215
CC
HPI
ROS
PFSH
1 1 1/1-2 prob*
1
4/1-2 prob*
2-9
1
4/3+ prob*
10+
3
Exam 1 2+ 2+ 5+ 8+
MDM 2/3
#Dx
Data
Risk
Nurse
Visit, Does
Not Need
MD
1
0
No meds
2
2
1 stable prob
2+ minor
prob
1 new no w/u
or 3 stable
3
Rx med; 2+
chronic; refer
to Risk List
1 new c W/U,
2+ worse, 4+
4
Life
threatening
MDM Straight-
forward
Straight-
forward
Low Moderate High
Time 5 10 15 25 40
2/3 Parts needed; *”status of”

MAS Dashboard and MU Reports

CMS Timeline for MIPS (Merit-Based Incentive Payment System)
Performance Year 1
50%
10%
15%
25%

0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
Pre Eval Post Eval
I have a good understanding of practice valuation
Strongly Agree
Agree
No Opinion
Disagree
Strongly Disagree
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
Pre Eval Post Eval
I have a good understanding of how to measure physician productivity
Strongly Agree
Agree
No Opinion
Disagree
Strongly Disagree
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
Pre Eval Post Eval
I have a good understanding of coding procedures
Strongly Agree
Agree
No Opinion
Disagree
Strongly Disagree
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
Pre Eval Post Eval
Understanding the different types of health care delivery (e.g. Medicare, Medicaid, VA,
Commercial/Traditional Indemnity, Self-pay) is an important factor in practicing medicine
Strongly Agree
Agree
No Opinion
Disagree
Strongly Disagree

Medical Economics Data
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
2011-2012 2012-2013 2014-2015 2015-2016
Medical Economics Data 2011-2016
Pre-Test
Post-Test
Overall Average Pre-Test Score 59.99%
Overall Average Post-Test Score 91.18%

IMPLEMENTING AN EFFECTIVE BLENDED LEARNING
ENVIRONMENT
By: Thaddeus Y. Carson, MD, FACP
Christos Hatzigeorgiou, DO, MPH, FACP
Tasha R. Wyatt, PhD

BackgroundThe notion of “anytime, anyplace” communication
is characteristic of the millennial population which has facilitated the growth of blended learning environments.
There is an increase in the use of web-based collaborative software in undergraduate & graduate education.
There are limited reports of use of this communication platform in medical education.
Study Hypothesis:
The integration of a collaborative software application in a high demand, inpatient clinical rotation will positively influence medical education and important components of the learning process.

Methods■ We compared the usefulness and functionality of several
software options: (1) Department hard-drive (2) Share-Point (3) Desire2Learn (4) Cerner social media application and (5) Box.
■ Of these choices, “Box” was chosen based on several factors:
■ - Ease of use (collaborative & interactive potential)
■ - Portability (smart phone / tablet operational)
■ - Alerts and HIPPA compliance

Methods
■ “Box” was implemented into Internal Medicine ward rotations and
learners were assessed on their acceptance of “Box” and its
perceived impact in the following areas:
■ - Learning environment
■ - Communication of goals
■ - Feedback
■ - Promotion of self-directed learning

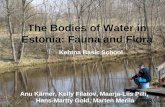
Results: Preliminary Survey Data
8.3%
8.3%
50.0%
8.3%
8.3%
8.3%
33.3%
25.0%
16.7%
16.7%
8.3%
50.0%
8.3%
41.7%
33.3%
33.3%
25.0%
50.0%
25.0%
33.3%
66.7%
41.7%
16.7%
66.7%
66.7%
66.7%
33.3%
50.0%
41.7%
33.3%
25.0%
41.7%
25.0%
41.7%
41.7%
33.3%
16.7%
16.7%
16.7%
25.0%
8.3%
41.7%
16.7%
33.3%
41.7%
33.3%
16.7%
25.0%
25.0%
0 0.2 0.4 0.6 0.8 1
I liked using a social media tool to further ward communications.
I was an active user of this social media tool.
Using a social media tool took time away from my clinical responsibilities.
I would like to use a social media tool on future Internal Medicine wards.
I would like to use a social media tool on other rotations.
Using Box improved the learning environment.
Using Box motivated me to ask questions.
Using Box promoted additional opportunities for patient discussion.
With the inclusion of Box, my attending was more likely to respond to my questions.
With the inclusion of Box, my attending provided clearer performance goals.
Feedback with Box was more specific.
Box offered more opportunities to respond to attending feedback.
Concerning corrective feedback, I prefer it written with Box compared to verbal…
My experience with Box motivated me to read more about my patients.
Box helped me develop ownership over my own learning.
Strongly Disagree Disagree Neither Agree nor Disagree Agree Strongly Agree

Results:Learners responded with the following trends regarding practical use of “Box” and its impact
on learning:
Most learners (>90%) thought that a social media tool offered more opportunities for communication and would like to use a social media tool on future clinical rotations (>70%).
The following areas were positively assessed (>60%):
* Improved learning environment and features of feedback
* Promotion of self-directed learning
* Clarity of expectations and goals
* Enhanced opportunities for patient discussion and attending
response to learners’ questions
* Development of ownership over personal learning
Box did not motivate learners to ask more questions (58%).









Questions?