
Edgewise mechanism
77
Tweed Mechanics
-
Upload
puneet-jain -
Category
Documents
-
view
236 -
download
20
Transcript of Edgewise mechanism

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 1/77
Tweed Mechanics

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 2/77
Graduated from an Angle coursegiven by George Hahn in 1928
Tweed diagnosed & treated casesunder Angle‟s guidance
He held to Angle‟s firm convictionthat one must never extract -for 3 yrs.
High frequency of relapse – discouraging
Important observation-
1) facial balance & post
treatment success related toupright mandibular incisors
2) to get lower incisorsupright, one must prepareanchorage & extract teeth
Dr. Tweed

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 3/77
His technique can be summarized as an anchorage technique.
While most operators were concentrating on how best to moveteeth, he focused himself on how not to move teeth.
To a great extent “cart has been placed before the horse”,
Dr.Tweed placed the horse where it belongs, in front of thecart.
Angle gave orthodontics the edgewise bracket, but Tweed gavethe specialty the appliance

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 4/77
Among his other contributions:-
a) Emphasized the four objectives of orthodontic treatment with emphasis & concern for facial esthetics
b) Developed the concept of uprighting teeth over basal boneesp. lower incisors
c) Made the extraction of teeth for treatment acceptable
d) Enhanced the clinical application of cephalometrics

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 5/77
e ) Developed the diagnostic facial triangle to make cephalometrics a
diagnostic tool & a guide in treatment & evaluation of results
f) He developed the concepts of orderly treatment procedures &introduced anchorage preparation as a major step in treatment
g) He developed a fundamentally sound & consistent preorthodontic guidance program using & popularizing serialextraction of primary & permanent teeth

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 6/77
Over the years several modifications have taken place in theappliance, however the concepts remain the same.
Basic concepts which are cornerstones of modern edgewise orthodontics:-1)Ability to obtain tooth movement in all 3 planes of space with
a single archwire
2)The philosophy of treating to an ideal arch or to Angle‟s
concept of „Line of Occlusion’ The line with which, in form and position according to type,the teeth must
be in harmony if in normal occlusion
3)The use of rectangular or square edgewise arches which if
properly employed can control arch width, arch form, B-Lcrown inclinations, axial root inclinations & incisor crown-root torque

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 7/77
Tweed’s philosophy
Based on the following :-
a) Practically all malocclusions are characterized by a forwardadjustment of teeth in relation to their basal bones --- thisis due to deficiency between the basal bone & toothmaterial
b) The establishment & maintenance of a stable anchorageshould be the initial concern of the operator & is afundamental factor in successful orthodontic treatment
c) Teeth like inanimate objects, best resist the force ofdisplacement when tipped to the angulation that offers themost advantageous mechanics against the pull ofdislodging forces, they are best stabilized when they overliethe basal bone

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 8/77
d)Teeth are most readily moved when their property & powerof mechanical resistance has been primarily reduced
e) All forces emanating from an orthodontic appliance must besynchronized if they are to be most effective in the massstabilization or the mass movement of teeth
f) Nature being an expert mechanic herself, offers biologiccompensations & adjustments when teeth are placed inposition of mechanical advantage for force resistance
g) The dental units will best resist forward displacement when
the buccal teeth are in mild distal axial position & the incisorteeth are in mild lingual axial inclination & overlying asubstantial bony foundation
“ placing the incisors on the ridge”

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 9/77
Every malocclusion exemplifies a denture that is stabilized bybalanced muscular forces & this muscular balance must bepreserved in treatment if stability in the end result is to beaccomplished
( Strang & Thompson )
8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 10/77
8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 11/77
TYBE B :- Maxilla & mandible grow downward & forward with
maxilla growing more rapidly than mandible
- When ANB angle is 4.5 or less prognosis is favorable- Extraoral appliances should be used immediately after
extraction
TYBE B Subdivision :-
-ANB is large & found to be increasing
-Undesirable growth trend, treatment long & difficult

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 12/77
TYPE C :- -Maxilla & mandible grow downward &
forward with mandible growing more than
maxilla-ANB decreasing
-Growth is favourable & treatment is
facilitated by growth
TYPE C Subdivision :-
-mandible grows more than maxilla but only to a
little extent

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 13/77
Basis for diagnosis & treatment planning
Consists of the following :-
1) FMA – the Frankfort mandibular plane angle
2) IMPA – the incisor mandibular plane angle
3) FMIA – the Frankfort mandibular incisorangle
Tweed’s Diagnostic facial triangle

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 14/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 15/77
Angle FMA IMPA FMIA
Visual 25 90 65
cephalometric 24.57 86.93 68.20Range 15 – 36 76 – 99 56 – 80
For successful treatment triangle should be attainable
Aim should be to obtain:-FMIA of 70° – 75° ( when FMA = 20 )
FMIA of 65° ( when FMA = 30)
When FMA is less than 20° FMIA should be more than 70° & IMPA should not exceed 94°
He showed that in well balanced faces – IMPA was 90°±5°
For every degree that FMA was in excess of 25° .the incisormandibular angle IMPA would have to be decreased by 1°

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 16/77
Cephalogram or Headplate Correction
Based on the requirements of diagnostic facial triangle
Consists of constructing the triangle on a tracing of the patientslateral ceph and measuring the 3 angles.
According to the FMA measured the required IMPA and FMIAare then constructed on the tracing, involving relocating the axialinclinations of the mandibbular incisors.
This new hypothetical position is considered and the change inarch length is calculated, which is the cephalogram correction
This is added to the arch length discrepancy measured on thecast to give us the total discrepancy.

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 17/77
Tweed summarized his philosophy on which his appliancetherapy is based:-
i) Normal occlusion is best maintained with the mandibularincisors in their normal axial inclination when related to theF-H plane approx. 65°(FMIA)
ii) The ultimate in balance & harmony of facial esthetics isachieved only when the mandibular incisors are positionedover the basal bone
iii) The normal relationship of the mandibular incisors totheir basal bone is the most reliable guide in diagnosis &treatment of cl. I ,cl. II & bimaxillary protrusion cases andalso in attainment of balance & harmony of facial profile &permanence of tooth position

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 18/77
Treatment objectives :-
Facial balance & harmony
Stability of the post treatment dentition
Healthy oral tissues
Efficient mastication
8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 19/77
Anchorage preparation
Stable anchorage – important to prevent forward movementof mandibular denture when cl.II intermaxillary force isapplied
On histological basis Brodie (1937) believes that the strongestanchorage is provided by stable fixation of teeth – to allow aslittle movement as possible
Tweed – anchor teeth best resist the dislodging forces whentheir vertical axes are parallel to the direction which offersthe most advantageous mechanical resistance against the pullof dislodging forces

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 20/77
Strongest anchorage is provided by tipping back the crowns ofthe teeth so that they will have a disto-axial inclination that
will resist a forward pull therefore, first & most important
step in treatment - Anchorage preparation
If anchorage preparation is not done the action of intermaxillaryelastics causes
-elevation of terminal molars & depression of mandibularincisors
-canting of occlusal plane,
-increase in FMA,
-point B drops downward & backward,
-entire mandibular denture is tipped & displaced forward intoprotrusion

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 21/77
Classification of anchorage preparation
First degree -minimal anchorage preparation,
-applicable to all malocclusion with ANB =0
to 4 ,
-total discrepancy does not exceed 10 mm,
-terminal molars must be uprighted & or
maintained in an upright position to
prevent their being elongated when cl. II
intermaxillary force is used .

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 22/77
Second degree -for malocclusions with ANB more than
0° to 4°
-facial esthetics requires to move pointB anteriorly & point A posteriorly i,e
cl. II cases
-usually accompanied by type A, type A
subdiv.,type B & type B subdiv.-degree of distal tipping of mandibular
molars more severe than first degree
anch.prep. – they should be tipped so
that their distal marginal ridges are atgum level

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 23/77
Third degree -severe discrepancy cases – 14-20mm or
more-ANB does not exceed 5°
-generally cl.I bimaxillary cases
-sliding jigs are necessary
-2nd ,1st molars & 2nd premolar must be
tipped to such an extent that the distal
marginal ridges are below the gum level
also called total anchorage preparation
8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 24/77
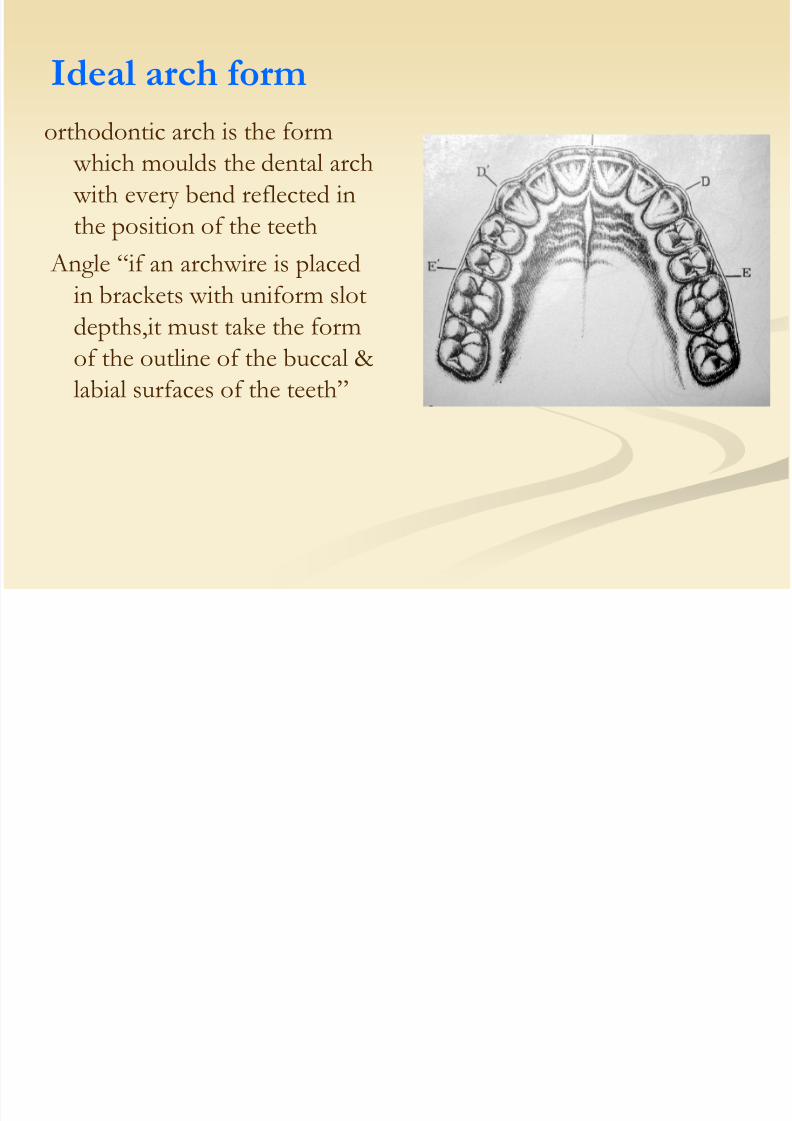
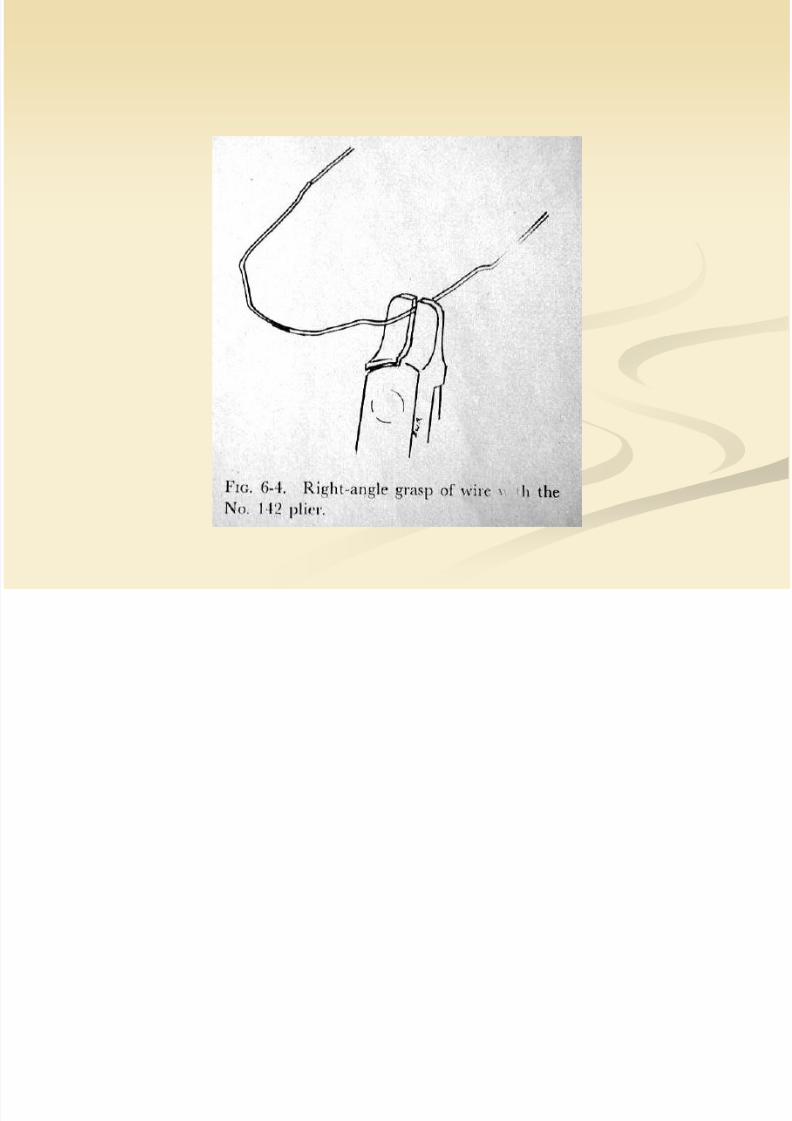
orthodontic arch is the form which moulds the dental arch with every bend reflected inthe position of the teeth
Angle “if an archwire is placed
in brackets with uniform slotdepths,it must take the formof the outline of the buccal &labial surfaces of the teeth”
Ideal arch form

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 25/77
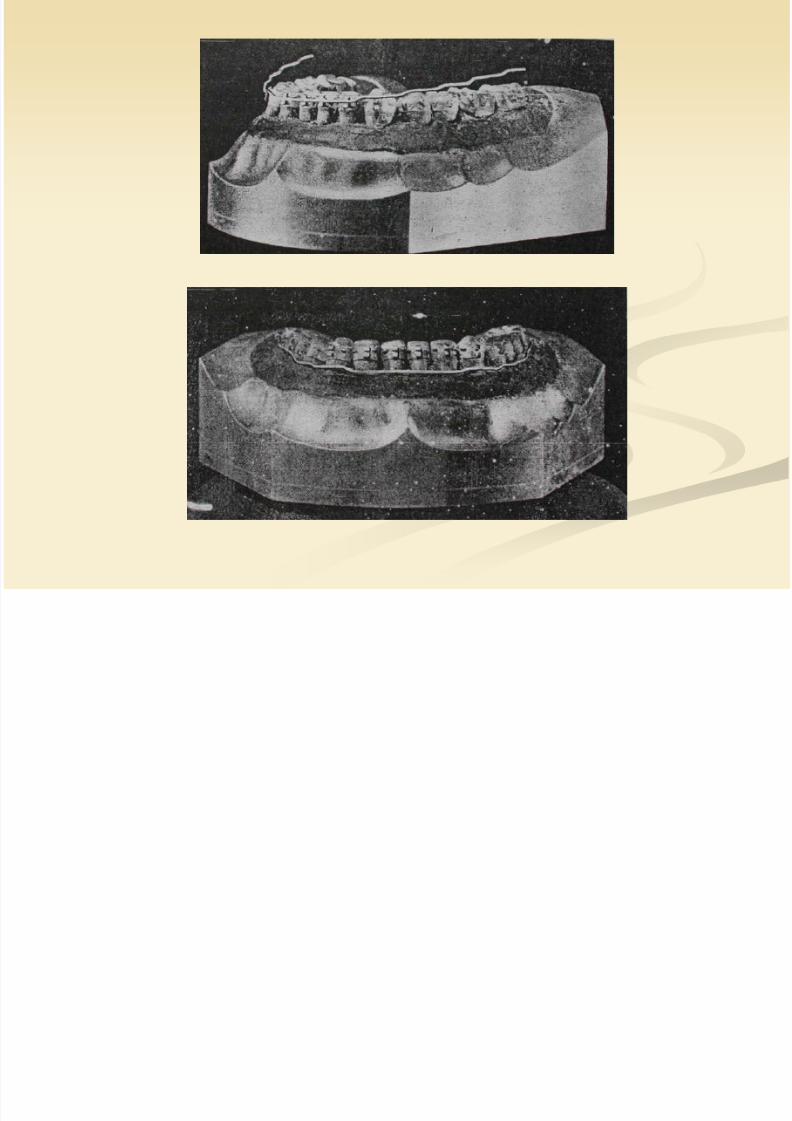
Unique alignment of upper lateral incisor – thinner labio-lingually & short crown length
Contact points lie on an ellipsoid curve
There is a straight line from canine to mesio buccal cusp of firstmolar, but beyond that it curves inward progressively
Bonwill-Hawley diagram is widely used to decide arch form
General pattern – decided by studying the original models & ofthe muscle behavior of the patient rather than based upon widths of teeth themselves

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 26/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 27/77
Movements necessary to bring the teeth into the line ofocclusion are of three kinds – first, second and third order
First order bends-
-horizontal change relative to the line of occlusion-also called in -out bends
-do not alter the horizontal plane of the wire
-the action & reaction of these bends affect expansion or
contraction-used to move individual teeth
-the interaction of bends can affect the third order positionof the teeth if expansionary forces are used
Three orders of tooth movement
8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 28/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 29/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 30/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 31/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 32/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 33/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 34/77
Second order bends
-represent a vertical change
-also called tip/angulation
-used to tip posterior teethmesially or distally-may be
tip back or tip forwardbends

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 35/77
8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 36/77
8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 37/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 38/77
Third order bends
-torsional change (with the line of occlusion serving as axis)-also called torque or inclination movement
-used to obtain axial changes in the bucco-lingual or
labio-lingual root & crown axis on one or more teeth
-involves twisting of the wire

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 39/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 40/77
Labial and Lingual torque in Wires

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 41/77
Lingual torque Labial torque

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 42/77
Lingual torque with lingual spring pressureby the archwire
Lingual torquecombined withlabial spring action

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 43/77
Labial torquecombined with labial spring
Labial torquecombined with lingual spring

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 44/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 45/77
Incorporation of torque

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 46/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 47/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 48/77
Other tooth movements
Opening spacesClosing spaces

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 49/77
Effect on teeth mesial and distal to loop

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 50/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 51/77

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 52/77
Activation with ligature traction
Distalization of molar + space opening for 2nd premolar

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 53/77
Opening spaces in anterior region
8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 54/77
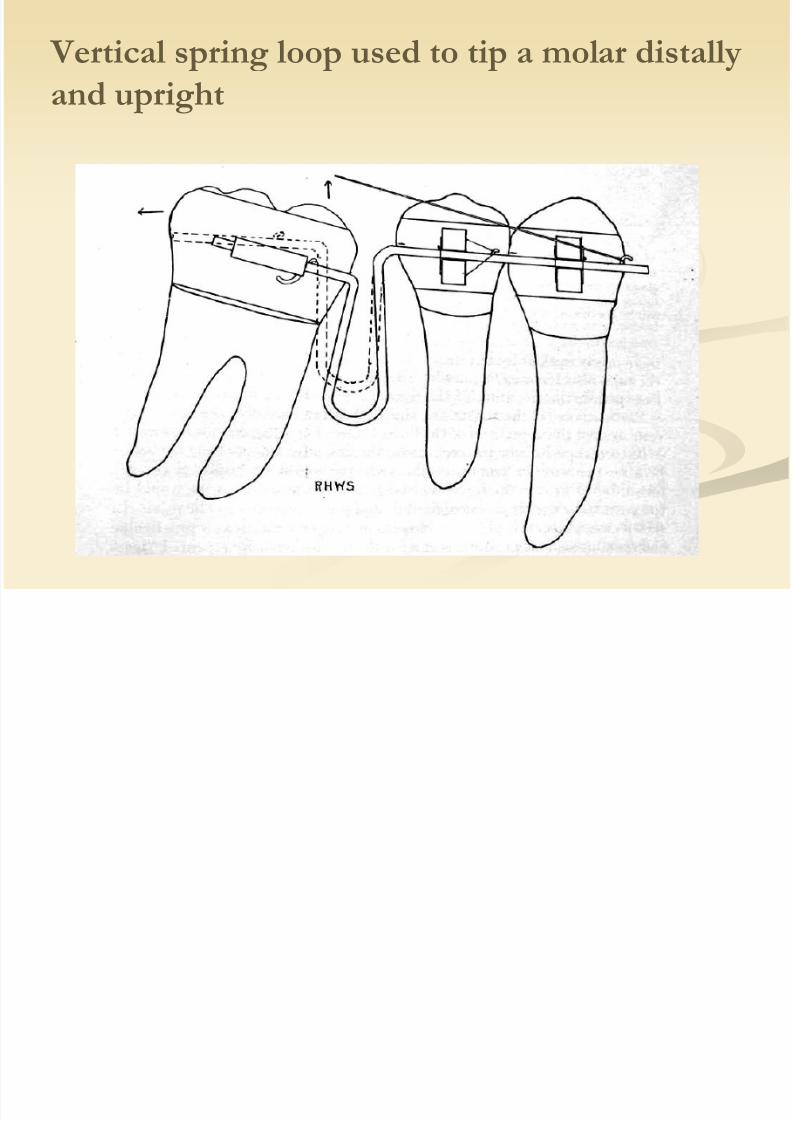
Vertical spring loop used to tip a molar distally
and upright

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 55/77
Vertical spring loop used for root paralleling
D bl i l i l ili f
8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 56/77
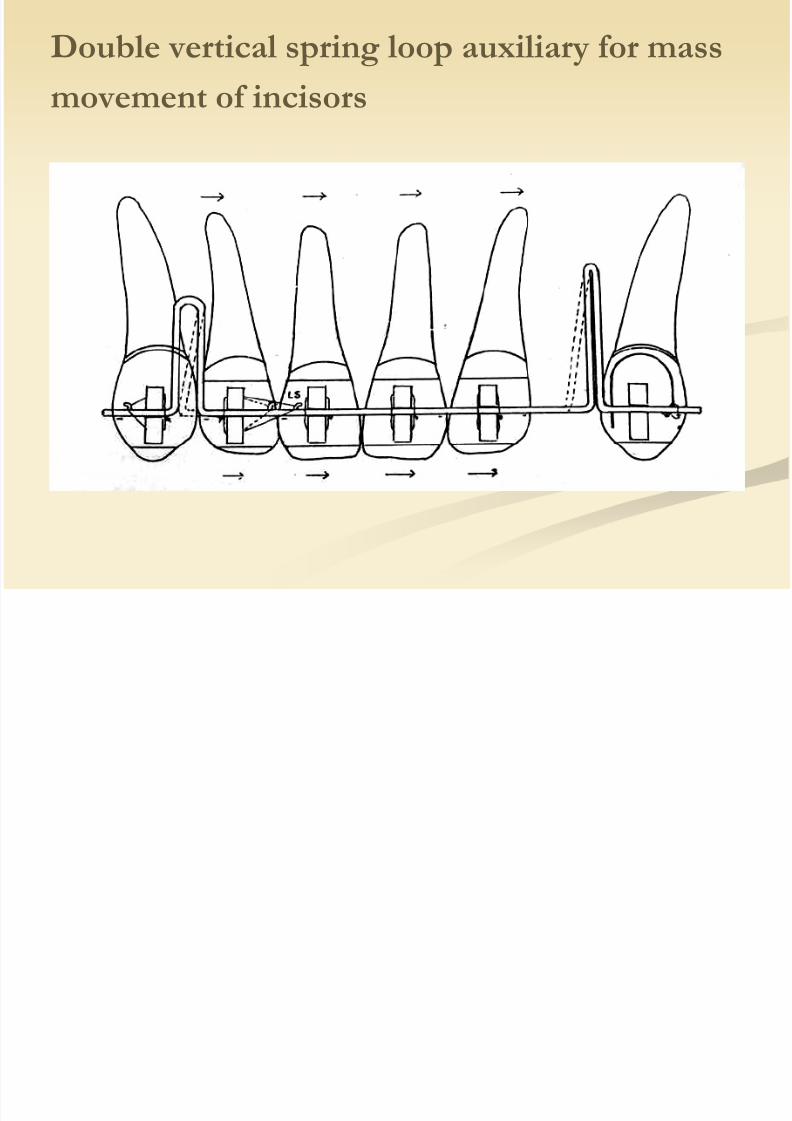
Double vertical spring loop auxiliary for mass
movement of incisors

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 57/77
General plan of treatment
Treatment divided into 3 phases:-
a)Anchorage preparation
b)Distal enmasse movement of maxillary buccal segments
c)Establishing correct denture form & completing treatmentobjectives
8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 58/77
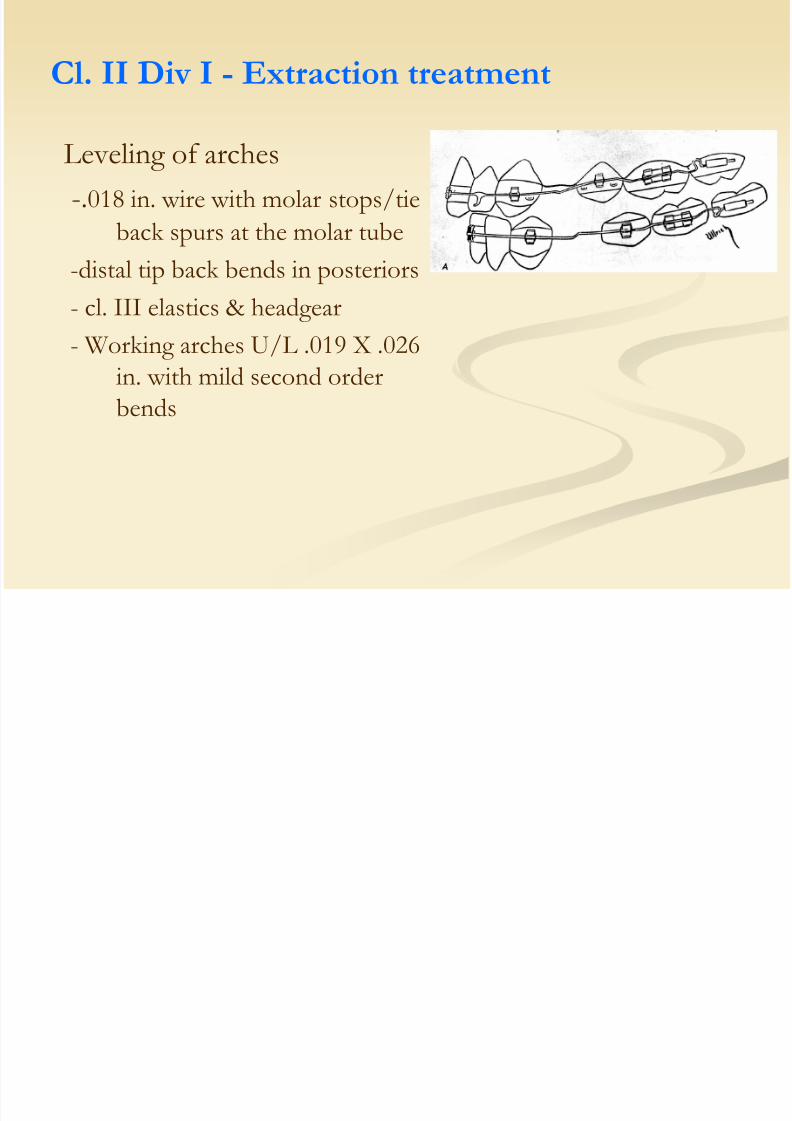
Cl. II Div I - Extraction treatment
Leveling of arches
-.018 in. wire with molar stops/tie
back spurs at the molar tube
-distal tip back bends in posteriors
- cl. III elastics & headgear
- Working arches U/L .019 X .026in. with mild second orderbends
Uprighting of canines - horizontal loops soldered mesial to

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 59/77
Uprighting of canines horizontal loops soldered mesial to
second premolars and a staple attached to anterior end ofloop
-ligature tied from here to distal staple on canineCanine bracket is not engaged in the wire
8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 60/77
Anchorage preparation
1) placing mandibular incisors upright
2) changing axial inclinations of the maxillary incisors, to makethem less resistant to distal movement
3) changing the axial inclinations of buccal teeth to a more distalaxial inclination

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 61/77
.021 X .027 stabilization wire with mild second orderbends in upper arch
.019 X .026 in working wire inlower arch with tip backbends & sliding jigs to bearpressure on 2nd premolar
bracket
cl. III elastics are worn
Once anchorage preparation inlower arch done – reverse the
mechanics
cl. II elastics are worn
Distal enmasse movement of maxillary

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 62/77
Canine retraction
U/L .019 X .026 archwires with second order bends & opencoil springs compressed mesial to canines are inserted
Cl. III elastics aid in distal movement of mandibular canineHeadgear applied to upper arch aids in upper canine retraction
Distal enmasse movement of maxillary
buccal segments

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 63/77
Incisor retraction
Using .019 X .026 archwire with closed Bull loop distal tocanine – activated 1mm every 3 wks.
Mandibular incisors are retracted to an FMIA of 65° in cl.Icases & 70° in cl.II cases

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 64/77
Maxillary incisor retraction completed with heavier .021 X .027in. wire, reduced posterior to lateral incisors & passed free
of canineStrong lingual root torque in upper wire for bodily retraction

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 65/77
to facilitate retraction, stops are soldered 3mm mesial to 2nd premolar brackets
Coil springs compressed against the stops and tied to the entireposterior segment
Correction of cl II relationship

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 66/77
Correction of cl. II relationshipNow, mand. arch - .021 X .027 in.
max.arch -.019 X .026 in. with accentuated tip
back bendsMand. arch tied back to receive cl. II elastics while maxillary
archwire is not tied backIntermaxillary hooks soldered mesial to maxillary caninesClass II elastics worn till normal cusp relation is achieved

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 67/77
Final space closure & detailed tooth positioning -.019 X .026 in.max. & mand. ideal arches, coil springs compressed mesialto 2nd molar tubes until space closure is completed
Completion procedure

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 68/77
Vertical elastics are used forseating cusps if bite is open
In case of a deepening of bite abiteplate is used along withbox elastics to increase the
vertical opening to thedesired level.
Biteplate is retained for 3-4months to allow for osseous
develpoment.
8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 69/77
cl. II div.1 – non-extraction treatment
Preparation of anchorage in the lower arch
Preparation of anchorage in the upper arch
Distal enmasse movement of maxillary arch
Detailed positioning of teeth
A h P i

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 70/77
Anchorage Preparation
Anchorage preparation in mandibular arch
Initial leveling & alignment - .016 or .018 round wires
Working arch wire .019 X .026 in. with coordinated tip back bendscl. III intermaxillary hooks soldered mesial to canine
Loop stops are made mesial to molar tubes but the archwire not
tied to molar anchor teeth

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 71/77
Upper arch is stabilized -.021 X .027 in.wire with mild tip backbends
Intermediate pull headgear mesial to canine is used to augmentthe anchorage - min. 14 hrs./day
Distal pull by headgear – twice as much as mesial pull on thearch by cl. III elastics
During day – light cl. III
During night – heavy cl. III
Distal tip back bends increased slightly every 2-3 wks.
b h

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 72/77
Stabilization arch -.021 X .027 in. wire with same degree of
tip back bends as in working archwire
Passive in mandibular incisor region
Total time required – aprrox. 4 mons.
Anchorage preparation in upper arch
Excessive inclination of the proclined upper incisors is reducedby using .018 in. round wire
Important – this provides unfavorable stationary anchorage &
resist distal / lingual movement of the teeth
Heavy stabilization wire with mild second order bends is placed
Enmasse distal movement of maxillary

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 73/77
Upper arch wire -.021 X .027 in. reduced distal to lateralincisors
Mild lingual crown torque if incisors are proclinedIntermaxillary hooks on archwire – patient put on cl. II elastics
Watch out for mandibular anchorage – any signs of mobility,increase the tip back bends After 3 wks. – tip back bends in the maxillary arch are
increased, stronger elastic force is applied until normalrelation of teeth attained
Mild palatal root torque in anteriorsContinue till incisors in edge – edge relation & posteriors in
good occlusion
y
arch

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 74/77
Proper seating of cusps is obtained by fitting correlated U & Lideal arches carrying vertical spurs for vertical elasticsbetween them
Detailed positioning of teeth
Bimaxillary dentoalveolar protrusion

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 75/77
Two types of cases:-
1)Axial inclinations of all the teeth in the arch inclinedabnormally forward (both in cl.I & cl. II cases ), dentalarches are more or less well aligned
2) Axial inclinations of teeth in buccal segments fairly upright,
irregular & crowdedSteps in treatment :- Anchorage preparation in lower arch
Anchorage preparation in upper arch
Extraction of four premolars Multiple loops .016 in. archwire U/L used for alignment
Space closure done using looped archwire
Bimaxillary dentoalveolar protrusion

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 76/77
Objective:-
1)To correct abnormal buccolingual inclination of all posteriorteeth in both arches
2)Constrict the mandibular arch which is too broad3)Expand the maxillary arch which is too narrow
4)Move maxillary arch forward enmasse, using
mandibular arch as stationary anchorage
Treatment of cl.III malocclusion
S i

8/13/2019 Edgewise mechanism
http://slidepdf.com/reader/full/edgewise-mechanism 77/77
Steps in treatment -
Initial .016 in. round wires After 2 wks. ,.021X .027 in. U/L ideal archesBrass wire hooks mesial to canineMandibular archwire is bent considerably narrower than the
ideal & torque is placed in the buccal segment
Step forward 2nd
order bends placed in maxillary posteriorsegment (direct opp. of tip back bends)Intermaxillary elastics from lingual of maxillary molar to hook
mesial to mandibular canine When cross bite is corrected – archwires are reshaped to the
ideal Treatment continued until the maxillary teeth have moved
forward enmasse into occlusion with teeth in mandibulararch.


















