Ectopic Pregnancy IGES

of 5
-
Upload
rizal-kudiarto -
Category
Documents
-
view
220 -
download
1
Transcript of Ectopic Pregnancy IGES
-
8/14/2019 Ectopic Pregnancy IGES
1/5
The Role of Minimal Invasive Surgery in the Therapy of Ectopic PregnancyFerdhy Suryadi Suwandinata 1, Hans Rudolf Tinneberg 2, Herbert Situmorang 1
1. Department of Obstetrics and Gynecology, Cipto Mangunkusumo Hospital, University of Indonesia,Jakarta, Indonesia
2. Department of Obstetrics and Gynecology, University Hospital of Giessen, Germany
IntroductionEctopic pregnancy has been recognized for over 400 years, the incidence continues to increase affectingmore than 2% of all pregnancies. The tendency of ectopic pregnancies in the past 25 years has beencorrelated to a number of different risk factors. Theoretically, anything that impedes migration of theconceptus to the uterine cavity can cause ectopic pregnancy. These may be intrinsic anatomic defects inthe tubal epithelium, hormonal factors interfere the transport of the conceptus, or pathologic conditionsas a result from a chronic inflammation that affect normal tubal functioning.
Besides the symptoms commonly associated with early pregnancy, women with ectopic pregnancycommonly experience pelvic pain and bleeding. The pain is often one sided and the bleeding is oftenvariable and may be the only sign of a complication. It should be noted, however, up to 20% of womenwith first trimester bleeding will go on to have a healthy pregnancy. The differential diagnosis for casesof suspected ectopic pregnancies are listed in Table 1. In the 1800s, the mortality associatedwith ectopic pregnancy was >60%. Until 1970, more than 80% of ectopic pregnancies were diagnosedafter rupture, resulting in significant morbidity and mortality. It still accounts for 9% of pregnancyrelated mortality and less than 1% of overall mortality in women. With excellent resolution obtainedfrom pelvic ultrasound, highly sensitive radio-immunoassays for human chorionic gonadotropin (hCG)and increased vigilance by clinicians, greater than 80% of ectopic pregnancies are now diagnosed intactwhich allows for more conservative management.
Awareness of the possibility of an ectopic pregnancy is most critical for early detection. Measurementof hCG with a doubling time of 2-3 days should occur if it is a normal gestation. A note of caution isthat approximately 10% of normal pregnancies do not follow this doubling time, and very early ingestation up to 60% of ectopic pregnancies will follow this doubling time. When hCG levels are>1000 mIU/mL, transvaginal ultrasound is reliable in diagnosing the location of the gestationapproximately 98% of the time. If using an abdominal ultrasound, then the hCG needs to be above 6000mIU/mL to make an accurate diagnosis. Progesterone can also be used to help differentiate aviable from non-viable gestation. A progesterone level of greater than 25 ng/mL is indicative of ahealthy gestation about 97.4% of the time and a level of 5 ng/mL indicates an abnormal pregnancy withalmost 100% sensitivity. Values between 5 and 25 ng/mL are unfortunately more common and thesevalues are more ambiguous.
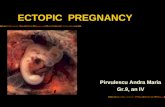
The incidence of ectopic pregnancy based on location has been relatively unchanged for many years.
Figure 1 shows the location of various ectopic pregnancies and their incidence in each location. Theampullary portion of the fallopian tube is the site of the majority of ectopic pregnancies.
Table 1 Differential diagnosis in cases of suspected ectopic pregnancy Spontaneous abortion Ruptured ovarian cyst Corpus luteum hemorragicum Adnexal torsion Pelvic inflammatory disease Endometriosis Urolithiasis Urinary tract infection Appendicitis Other lower gastrointestinal tract disease
-
8/14/2019 Ectopic Pregnancy IGES
2/5
-
8/14/2019 Ectopic Pregnancy IGES
3/5
Figure 1. Unruptured ampullaryectopic pregnancy withintraabdominal bleeding
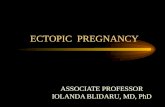
Figure 2. Using a monopoleelectrode, a linear incision ismade on the antimesentericsurface extending 1 to 2 cm overthe thinnest portion of the tube.
Figure 3. The conception tissueis removed by usinglaparoscopic forceps.
-
8/14/2019 Ectopic Pregnancy IGES
4/5
The pregnancy usually protrudes through the incision and slowly slips out of the tube; it is removed byusing hydrodissection or laparoscopic forceps (Figure 3). Forceful irrigation in the tubes opening candislodge the gestation from its implantation. As the pregnancy is pulled out or extrudes from the tube,
some products of conception may adhere to the implantation site by a ligamentous structure containingblood vessels. Using the electrocoagulator, this structure is coagulated before the tissue is removed.Oozing from the tube is common but usually ceases spontaneously. Occasionally, coagulation isnecessary with a defocused laser beam or an electrocoagulator. Depending on the size, the products of conception are removed through a 5- or 10-mm trocar sleeve.
Tubal Resection
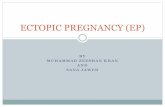
Resection of the tubal segment that contains the gestation is preferable to salpingotomy for anisthmicpregnancy or a ruptured tube or if hemostasis is difficult to obtain. Segmental resection is done withbipolar electrosurgery, fiber lasers, CO2 laser, sutures, or stapling devices. Bloodless segmental
resection is achieved by grasping the proximal and distal boundaries of the tubal segment containingthe gestation with a Kleppinger forceps and coagulating them from the antimesenteric surface to themesosalpinx. The segment is cut with laparoscopic scissors or a laser, with little risk of bleeding.The mesosalpinx under the pregnancy is coagulated, with particular attention given to the arcuateanastomosing branches of the ovarian and uterine vessels.[64] After coagulation, the mesosalpinx is cut.The material is then removed through a trocar sleeve.
Figure 4. No suture is needed toadapt the tubal wall.
Figure 5. Tubal resection.
-
8/14/2019 Ectopic Pregnancy IGES
5/5
SalpingectomySalpingectomy is chosen by the presence of uncontrolled bleeding, tubal destruction by the EUP, and arecurrent pregnancy in the same tube. This operation is done by progressively coagulating and cuttingthe mesosalpinx, beginning with the proximal isthmic portion and progressing to the fimbriated end of the tube. It is separated from the uterus by using bipolar coagulation and scissors or a laser. The isolatedsegment containing the EUP is removed intact or in sectioned parts through the 10-mm trocar sleeve.
Products of conception can be placed in an Endo-bag and removed (Figure 9.4.8). Occasionally, apatient is admitted overnight to be observed for postoperative bleeding and to receive emotional supportfrom the infertility team.
Salpingectomy or SalpingotomyThere has been considerable debate about whether salpingectomy or salpingostomy should be done. Thepossible advantages of removing the tube completely include almost entirely eliminating the risk of persistent trophoblast and that of a subsequent ectopic pregnancy, whereas the possible advantage of conserving the fallopian tube is that future fertility is preserved.[40] There are no randomized controlledtrials published that specifically compare laparoscopic or open salpingectomy and salpingotomy.There are four cohort studies that specifically compare laparoscopic tube-sparing and radical treatmentsof ectopic pregnancy.[6770] Silva et al. [67] examined reproductive outcomes prospectively in 143women undergoing laparoscopic salpingectomy or laparoscopic salpingotomy. The intrauterinepregnancy rates were similar when comparing the two groups (intrauterine pregnancy in 60% of subjects after salpingotomy versus 54% after salpingectomy; relative risk 1.11). In a study of 155 women, Job-Spira et al. [68] reported subsequent intrauterine pregnancy rates with salpingotomythat were comparable to those following salpingectomy (hazard ratio, 1.22). The cumulative pregnancyrates at 1 year were 72.4% after salpingotomy and 56.3% after salpingectomy. In a study byMol et al.[69] of a cohort of 135 women, the fecundity rate ratio when comparing laparoscopic salpingotomy withsalpingectomy during the 18-month follow-up period was 1.4 for women with a healthy contralateraltube and 3.1 for women with contralateral tubal disease.The 3-year cumulative pregnancy rate was 62% after salpingotomy and 38% after salpingectomy. In astudy by Bangsgaard et al. [70] reviewing a cohort of 276 women undergoing salpingotomy orsalpingectomy, the subsequent cumulative pregnancy rate at 7 years was 89% following salpingotomyand 66% following salpingectomy. The hazard ratio for intrauterine pregnancy following salpingectomywas 0.63 when comparedwith salpingotomy. Regardless of the type of surgery, contralateral tubalabnormalities predispose the patient to recurrent ectopic pregnancy.There was no significant difference in the risk of repeat ectopic pregnancy (17% after conservativesurgery and 16% after radical surgery).[70]Salpingotomy remains the definitive and universal treatment for EUP in women who arehemodynamically stable and who wish to preserve their fertility.[1,2] The reproductive performanceafter salpingotomy appears to be equivalent to or better than that after salpingectomy, but the recurrentEUP rate may be slightly greater. Salpingectomy may be necessary for women with uncontrolledbleeding, recurrent ectopic pregnancy in the same tube, a severely damaged tube, or a tubal gestational
sac greater than 5 cm in diameter.[1]
ConclusionEctopic pregnancy remains an increasing health problem. Its incidence continues to rise, parallelingincrease in the incidence of the risk factors, such as sexually transmitted diseases. With improvedminimally invasive techniques, the surgical management of this worrisome condition can beaccomplished with minimal trauma and maximal preservation of fertility. Minimally invasive surgeryhas lower morbidity, shorter hospital stays and decreased costs as well as decreased need forpostoperative analgesia, and achieves superior pregnancy rates to laparotomy.