![Apical Hypertrophic Cardiomyopathy in an African … · to decrease symptoms as well as overall morality [18-20]. The concern associated with overall diagnosis of hypertrophic : cardiomyopathy](https://static.fdocuments.in/doc/165x107/5b5c70a07f8b9ad21d8c33e7/apical-hypertrophic-cardiomyopathy-in-an-african-to-decrease-symptoms-as-well.jpg)
Echocardiographic Diagnosis of Apical Hypertrophic Cardiomyopathy with Optison Contrast
4
Echocardiographic Diagnosis of Apical Hypertrophic Cardiomyopathy with Optison Contrast Jagruti Patel, M.D., Jeremy Michaels, R.D.C.S., Jennifer Mieres, M.D., Smadar Kort, M.D., and Judy R. Mangion, M.D. Division of Cardiology, Department of Medicine, Northshore University Hospital, Manhasset, New York We describe a case of obstructive apical hypertrophic cardiomyopathy in a 61-year-old Caucasian female with a history of chest pain syndrome. The patient was referred to the echo lab by her nuclear cardiologist, who was impressed by her abnormal stress nuclear perfusion scan that showed marked increased uptake of radioisotope at the left ventricular (LV) apex. The patient had deep negative T waves on her electrocardiogram similar to those originally described in the Japanese popula- tion. Transthoracic echocardiography with native harmonic imaging was suboptimal for visualiz- ing LV segments. Therefore, 0.5 cc of Optison contrast was given intravenously, with repeat transthoracic imaging con rming the diagnosis. The patient and her family were referred for addi- tional genetic testing and cardiovascular workup. (ECHOCARDIOGRAPHY, Volume 19, August 2002) apical hypertrophic cardiomyopathy, native harmonic imaging, Optison contrast, diagnosis, genetic testing A 61-year-old Caucasian female with a past medical history of hypertension, elevated cho- lesterol, family history of coronary artery dis- ease, and an abnormal electrocardiogram (ECG) with deep, inverted T waves in V 3 -V 6 , I, and AVL (Fig. 1) was referred to nuclear car- diology for evaluation of intermittent exer- tional chest pain, palpitations, and a new left bundle branch on ECG. The patient had a car- diac catheterization 8 years prior that revealed normal coronary arteries. She was referred for an adenosine sestamibi stress test, which re- vealed myocardial ischemia of the anterior and anterolateral walls and increased radioisotope uptake at the LV apex (Fig. 2). The patient then was referred by her nuclear cardiologist to the Echo lab for an echocardiogram. Two-dimensional transthoracic images were obtained employing second harmonic imaging, which showed grossly normal LV systolic func- tion. These images had poor endocardial border de nition and failed to visualize the LV apex (Fig. 3). Therefore, additional imaging was per- formed with the administration of a 0.5 cc bo- lus injection of Optison contrast. Postcontrast apical four-chamber views demonstrated con- centric LV hypertrophy with severe hypertro- phy of the LV apex and hyperdynamic LV sys- tolic function (Fig. 4). There was apical systolic obstruction with a peak instantaneous gradi- ent of 69 mmHg. There was no systolic anterior motion of the mitral valve. The patient and her family were referred for further testing, including a repeat cardiac catheterization that showed nonobstructive disease of the left anterior descending artery. A Holter monitor was placed and showed nonsus- tained ventricular tachycardia for which the patient was referred for electrophysiological testing. This demonstrated no inducible ven- tricular tachycardia. The patient and her fam- ily were referred for genetic testing and screen- ing echocardiograms. Discussion Hypertrophic cardiomyopathy is a primary disorder of the myocardium with a variety of clinical and morphologic features. Its incidence is as high as 1 in 500 individuals, 1 and it is Address for correspondence and reprint requests: Jagruti Patel, M.D., Division of Cardiology, Northshore University Hospital, 300 Community Drive, Manhasset, New York 11030. Fax: 516-562-3984. Reprinted with permission from ECHOCARDIOGRAPHY, Volume 19, No. 6, August 2002 Copyright ©2002 by Futura Publishing Company, Inc., Armonk, NY 10504-0418 521 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 19, No. 6, 2002
-
Upload
jagruti-patel -
Category
Documents
-
view
213 -
download
1
Transcript of Echocardiographic Diagnosis of Apical Hypertrophic Cardiomyopathy with Optison Contrast

Echocardiographic Diagnosis of ApicalHypertrophic Cardiomyopathy withOptison ContrastJagruti Patel, M.D., Jeremy Michaels, R.D.C.S., Jennifer Mieres, M.D., Smadar Kort, M.D.,and Judy R. Mangion, M.D.
Division of Cardiology, Department of Medicine, Northshore University Hospital, Manhasset,New York
We describe a case of obstructive apical hypertrophic cardiomyopathy in a 61-year-old Caucasianfemale with a history of chest pain syndrome. The patient was referred to the echo lab by her nuclearcardiologist, who was impressed by her abnormal stress nuclear perfusion scan that showed markedincreased uptake of radioisotope at the left ventricular (LV) apex. The patient had deep negative Twaves on her electrocardiogram similar to those originally described in the Japanese popula-tion. Transthoracic echocardiography with native harmonic imaging was suboptimal for visualiz-ing LV segments. Therefore, 0.5 cc of Optison contrast was given intravenously, with repeattransthoracic imaging con�rming the diagnosis. The patient and her family were referred for addi-tional genetic testing and cardiovascular workup. (ECHOCARDIOGRAPHY, Volume 19, August2002)
apical hypertrophic cardiomyopathy, native harmonic imaging, Optison contrast, diagnosis, genetictesting
A 61-year-old Caucasian female with a pastmedical history of hypertension, elevated cho-lesterol, family history of coronary artery dis-ease, and an abnormal electrocardiogram(ECG) with deep, inverted T waves in V3-V6, I,and AVL (Fig. 1) was referred to nuclear car-diology for evaluation of intermittent exer-tional chest pain, palpitations, and a new leftbundle branch on ECG. The patient had a car-diac catheterization 8 years prior that revealednormal coronary arteries. She was referred foran adenosine sestamibi stress test, which re-vealed myocardial ischemia of the anterior andanterolateral walls and increased radioisotopeuptake at the LV apex (Fig. 2). The patientthen was referred by her nuclear cardiologist tothe Echo lab for an echocardiogram.
Two-dimensional transthoracic images wereobtained employing second harmonic imaging,which showed grossly normal LV systolic func-tion. These images had poor endocardial borderde�nition and failed to visualize the LV apex
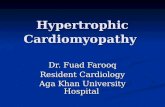
(Fig. 3). Therefore, additional imaging was per-formed with the administration of a 0.5 cc bo-lus injection of Optison contrast. Postcontrastapical four-chamber views demonstrated con-centric LV hypertrophy with severe hypertro-phy of the LV apex and hyperdynamic LV sys-tolic function (Fig. 4). There was apical systolicobstruction with a peak instantaneous gradi-ent of 69 mmHg. There was no systolic anteriormotion of the mitral valve.
The patient and her family were referred forfurther testing, including a repeat cardiaccatheterization that showed nonobstructivedisease of the left anterior descending artery. AHolter monitor was placed and showed nonsus-tained ventricular tachycardia for which thepatient was referred for electrophysiologicaltesting. This demonstrated no inducible ven-tricular tachycardia. The patient and her fam-ily were referred for genetic testing and screen-ing echocardiograms.
Discussion
Hypertrophic cardiomyopathy is a primarydisorder of the myocardium with a variety ofclinical and morphologic features. Its incidenceis as high as 1 in 500 individuals,1 and it is
Address for correspondence and reprint requests: JagrutiPatel, M.D., Division of Cardiology, Northshore UniversityHospital, 300 Community Drive, Manhasset, New York11030. Fax: 516-562-3984.
Reprinted with permission fromECHOCARDIOGRAPHY, Volume 19, No. 6, August 2002
Copyright ©2002 by Futura Publishing Company, Inc., Armonk, NY 10504-0418
521ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech.Vol. 19, No. 6, 2002

transmitted as an autosomal dominant traitwith a high degree of penetrance.2 Echocardi-ography and electrocardiography are essentialfor the diagnosis of hypertrophic cardiomyopa-thy.1 Hypertrophy most commonly involves theinterventricular septum, most frequently in
the upper and middle portions as well as theanterolateral walls. Few patients have pre-dominant hypertrophy of the inferior and lat-eral segments or the posterobasal free wall.2Hypertrophy also can be localized predomi-nantly to the LV apex, as originally described
Figure 1. Baseline electrocardiogram demonstrating giant negative T waves across the precordium, suggestive of apicalhypertrophic cardiomyopathy.
Figure 2. Nuclear perfusion scan obtained using sestamibi-sestamibi protocol (technetium Tc 99 15 Ci at rest and 30 mcipostadenosine infusion) during adenosine stress testing. Note the increased radioisotope uptake at the left ventricular apexand the anterior and anterolateral perfusion defect, further supporting the diagnosis of apical hypertrophic cardiomyopathy.
PATEL, ET AL.
522 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 19, No. 6, 2002

in the Japanese population and discovered sub-sequently in the non-Japanese population aswell.1-3 Apical hypertrophic cardiomyopathydescribed in the Japanese population is associ-ated with a spade-like appearance of the LVcavity, and frequently but not always is asso-ciated with a giant T wave inversion (. 10 mmdeep) in the precordial leads.4
Apical hypertrophy in Japanese patientsgenerally tends to be clinically benign, and thisnonfamilial disease occurs predominantly inolder men and is frequently associated withhypertension.4 However, in North Americanpatients studied by Louie and Maron,4 mildhypertension was insuf�cient to explain signif-icant hypertrophy. They also reported that 9 of23 patients had evidence of genetic transmis-sion. Apical hypertrophic cardiomyopathy gen-erally is not associated with a LV out�ow tractobstruction6 but can be associated with a mid-or apical LV cavity obstruction. Our patientpresented with an LV apical peak gradient of69 mmHg by continuous-wave Doppler and apeak gradient of 100 mmHg by cardiac cathe-terization.
Little is known about the prognosis of thesepatients. Generally, patients are asymptomat-ic.4 However, our patient had symptoms of an-gina and palpitations in the setting of nonob-structive coronary artery disease. Decreased�ow reserve secondary to increased wall stressand possibly small vessel coronary disease arepostulated mechanisms for anginal symptoms,possibly resulting in apical infarction.1,5 Pa-tients can have a LV out�ow tract obstruction,serious arrhythmia, and angina. Therefore, ap-propriate workup and genetic screening shouldbe considered in these patients. Despite nativeharmonic imaging, the diagnosis of apical hy-pertrophic cardiomyopathy was not readily ap-parent in our patient until imaging was re-peated with 0.5 cc of Optison contrast. Thiscase illustrates the important role of ultra-sound contrast agents in reliably diagnosing allforms of cardiomyopathy when baseline trans-thoracic images are suboptimal. Thanigaraj etal. reported two patients who appeared to haveLV thrombus on transthoracic echocardiogra-phy using second harmonic imaging, whichsubsequently was diagnosed accurately as api-cal hypertrophic cardiomyopathy using Opti-son contrast.6 More recently, Soman et al. alsoreported a case of apical hypertrophic cardio-myopathy in a patient presenting with anginawho required the use of Optison contrast inorder to make this diagnosis.7 We concludethat it is critical that the diagnosis of apicalhypertrophic cardiomyopathy be made accu-rately since this entity can present with syn-cope from LV out�ow tract obstruction, ar-rhythmia, and angina, and in many cases, isfamilial, which requires screening for familymembers. Since the diagnosis of apical hyper-trophic cardiomyopathy can be missed easily
Figure 3. Suboptimal two-dimensional transthoracicapical four-chamber view obtained using second harmonicimaging.
Figure 4. Two-dimensional transthoracic apical four-chamber view obtained using second harmonic imagingwith the addition of the 0.5 cc of Optison contrast. This ishighly consistent with apical hypertrophic cardiomyopathy.Note the classic spade-like appearance of the left ventricularcavity.
AN UNUSUAL CASE OF APICAL HYPERTROPHIC CARDIOMYOPATHY
523ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech.Vol. 19, No. 6, 2002

even with the latest imaging techniques usingsecond harmonics, the use of second-generationcontrast agent such as Optison may be vital inestablishing this diagnosis when baseline im-ages are suboptimal.
References
1. Webb JG, Sasson Z, Rakowski H, et al: Apical hyper-trophic cardiomyopathy clinical follow- up and diag-nostic correlates. J Am Coll Cardiol 1990;15:83–90.
2. Weyman A: Principles and Practice of Echocardiogra-phy, 2nd Edition. Lea and Febiger, Pennsylvania,1994, pp. 781–817.
3. Seidman, C: The genetic basis of hypertrophic cardio-
myopathy. Brigham and Womens’ Hospital. Cardiol-ogy Rounds 2000;4.
4. Louie EK, Maron BJ: Apical hypertrophic cardiomy-opathy: Clinical and two-dimensional echocardio-graphic assessment. Ann Int Med 1987;106:663– 670.
5. Gerson, MC: Cardiac Nuclear Medicine, 2nd Edition.McGrawHill, New York, 1991, pp. 507–511.
6. Thanigaraj S, Perez JE: Apical hypertrophic cardio-myopathy: Echocardiographic diagnosis with the useof intravenous contrast image enhancement. J AmerSoc Echocardiogr 2000;13:146–149
7. Soman P, Swinburn J, Callister M, et al: Apical hy-pertrophic cardiomyopathy: Bedside diagnosis by in-travenous contrast echocardiography. J Am Soc Echo-cardiogr 2001;14:311–313.
PATEL, ET AL.
524 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 19, No. 6, 2002