Echocardiographic Assessment of LV Systolic Function MR. MOHAMMED AL GHAMDI MR. MOHAMMED AL GHAMDI.
43
Echocardiographic Echocardiographic Assessment of LV Assessment of LV Systolic Function Systolic Function MR. MOHAMMED AL GHAMDI MR. MOHAMMED AL GHAMDI
-
Upload
derick-spink -
Category
Documents
-
view
219 -
download
0
Transcript of Echocardiographic Assessment of LV Systolic Function MR. MOHAMMED AL GHAMDI MR. MOHAMMED AL GHAMDI.

Echocardiographic Echocardiographic Assessment of LV Assessment of LV Systolic FunctionSystolic Function
MR. MOHAMMED AL MR. MOHAMMED AL GHAMDIGHAMDI

Causes of LV Systolic Causes of LV Systolic DysfunctionDysfunction
CADCAD HTNHTN Cardiomyopathy (iDCM, HCM, Etoh, Cardiomyopathy (iDCM, HCM, Etoh,
Peripartum, Viral, Infiltrative, Peripartum, Viral, Infiltrative, Toxins, Thyroid Dz., Toxins, Thyroid Dz., Tachyarrythmias)Tachyarrythmias)
Valvular Disease Valvular Disease

Dimensions and AreaDimensions and Area
Parasternal short-axis at level of Parasternal short-axis at level of papillary musclespapillary muscles
Parasternal long-axisParasternal long-axis Apical 4-chamberApical 4-chamber Apical 2-chamberApical 2-chamber




LV Systolic Function LV Systolic Function VariablesVariables
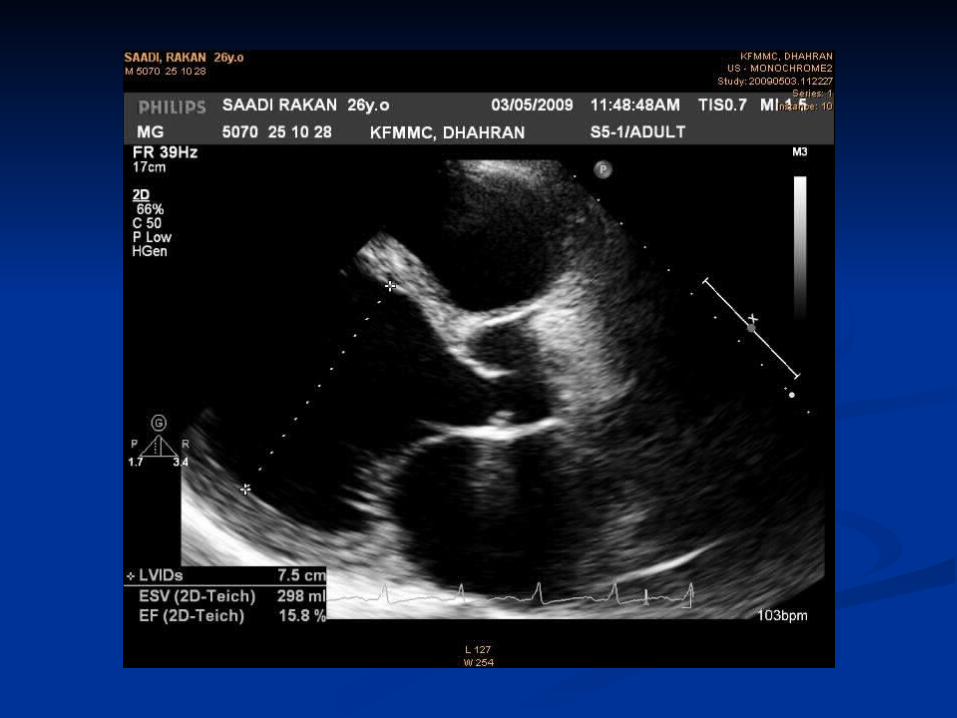
LVEDD – LVESDLVEDD – LVESD FS = -------------------- X 100FS = -------------------- X 100 LVEDD LVEDD Percent change in LV dimension with systolic Percent change in LV dimension with systolic
contractioncontractionFS approximates EF if there are no significant wall FS approximates EF if there are no significant wall
motion abnormalitiesmotion abnormalities
SV = EDV - ESV CO = SV x HR SV = EDV - ESV CO = SV x HR
EDV - ESVEDV - ESV EF = ----------------- X 100EF = ----------------- X 100 EDVEDV

How do we quantify LV How do we quantify LV function?function?
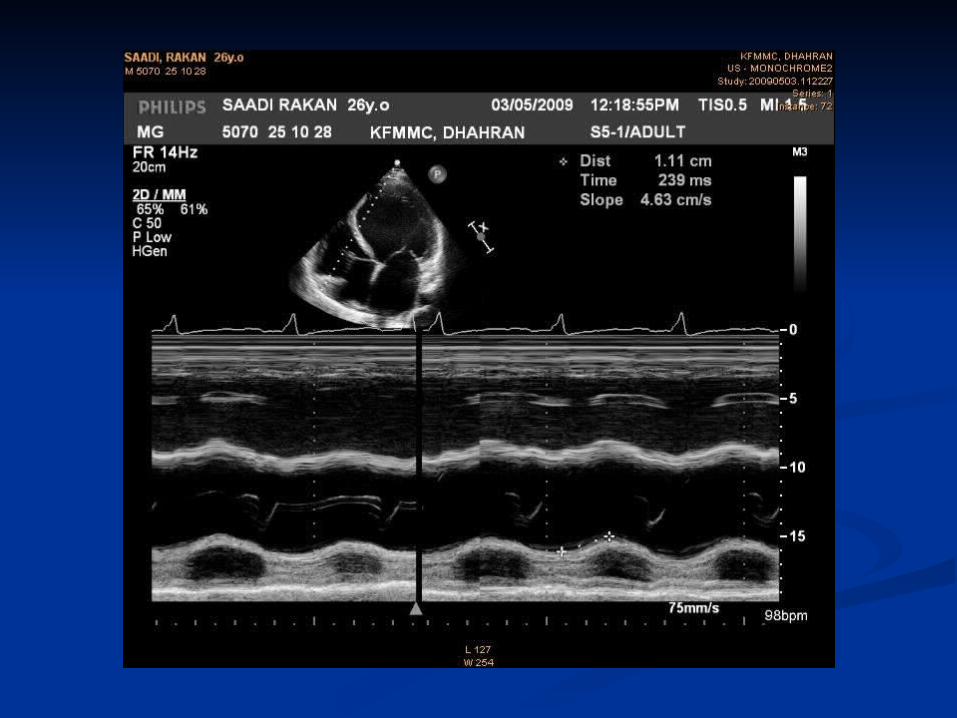
M-Mode M-Mode Modified Simpson’s Method Modified Simpson’s Method Single plane area-length methodSingle plane area-length method Velocity of Circumferential Velocity of Circumferential
ShorteningShortening Mitral Annular ExcursionMitral Annular Excursion E-point to septal separationE-point to septal separation Rate of rise of MR jetRate of rise of MR jet Index of myocardial performanceIndex of myocardial performance Subjective assessmentSubjective assessment

M-Mode QuantificationM-Mode Quantification Uncorrected (LVEDD)2 - (LVESD)2 Uncorrected (LVEDD)2 - (LVESD)2
LVEF = ------------------------------ X 100 LVEF = ------------------------------ X 100
(LVEDD)2(LVEDD)2
If apical contractility is normal (Quinones group):If apical contractility is normal (Quinones group):
Corrected Corrected
LVEF = Unc LVEF + ((100 – Unc LVEF) X 15%)LVEF = Unc LVEF + ((100 – Unc LVEF) X 15%)
5% hypokinetic, 0% akinetic, -5% dyskinetic, -10% 5% hypokinetic, 0% akinetic, -5% dyskinetic, -10% aneurysm aneurysm


Modified Simpson’s Modified Simpson’s MethodMethod
EDV – ESVEDV – ESV
LVEF = --------------- X 100LVEF = --------------- X 100
EDV EDV

Normal E point to septal separation is < 6 mmWith reduced lvef, EPSS may be increased.
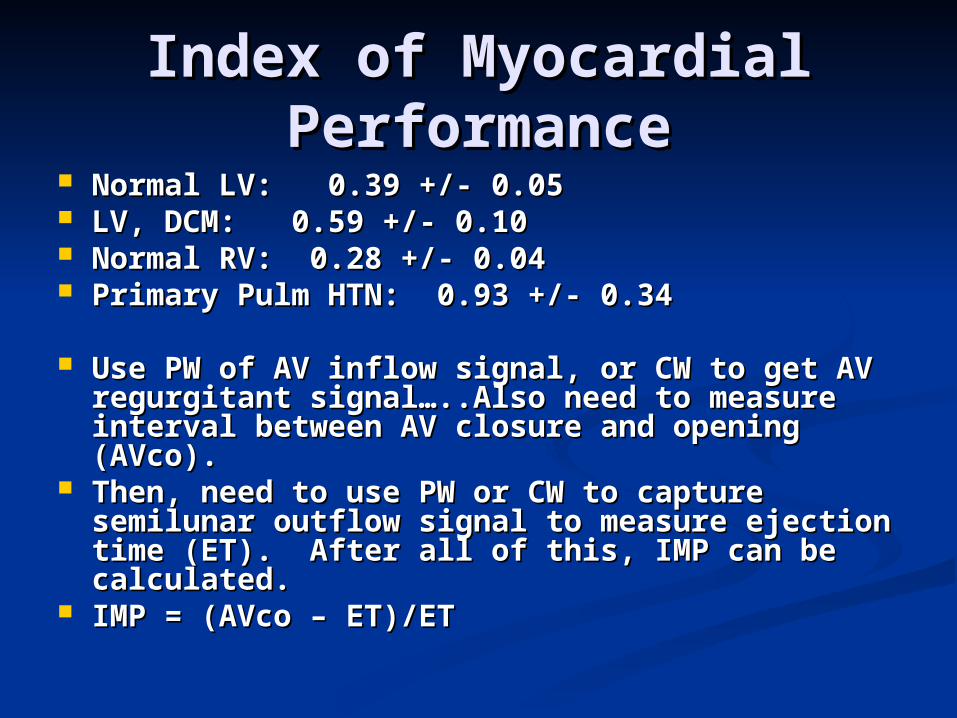
Index of Myocardial Index of Myocardial PerformancePerformance
Normal LV: 0.39 +/- 0.05Normal LV: 0.39 +/- 0.05 LV, DCM: 0.59 +/- 0.10LV, DCM: 0.59 +/- 0.10 Normal RV: 0.28 +/- 0.04Normal RV: 0.28 +/- 0.04 Primary Pulm HTN: 0.93 +/- 0.34Primary Pulm HTN: 0.93 +/- 0.34
Use PW of AV inflow signal, or CW to get AV Use PW of AV inflow signal, or CW to get AV regurgitant signal…..Also need to measure regurgitant signal…..Also need to measure interval between AV closure and opening interval between AV closure and opening (AVco).(AVco).
Then, need to use PW or CW to capture Then, need to use PW or CW to capture semilunar outflow signal to measure ejection semilunar outflow signal to measure ejection time (ET). After all of this, IMP can be time (ET). After all of this, IMP can be calculated.calculated.
IMP = (AVco – ET)/ET IMP = (AVco – ET)/ET

Assessment of Regional Assessment of Regional FunctionFunction
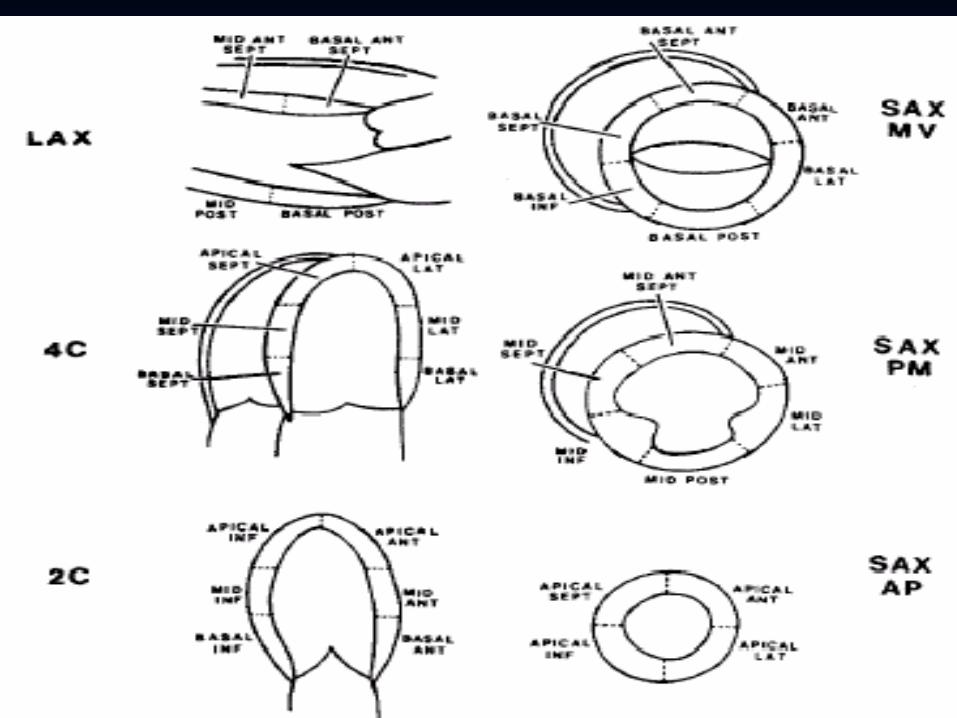
Based on grading wall motion Based on grading wall motion divided into the 16 (17) segment divided into the 16 (17) segment model as proposed by the American model as proposed by the American Society of EchocardiographySociety of Echocardiography
Each segment can be viewed in Each segment can be viewed in multiple tomographic planes multiple tomographic planes




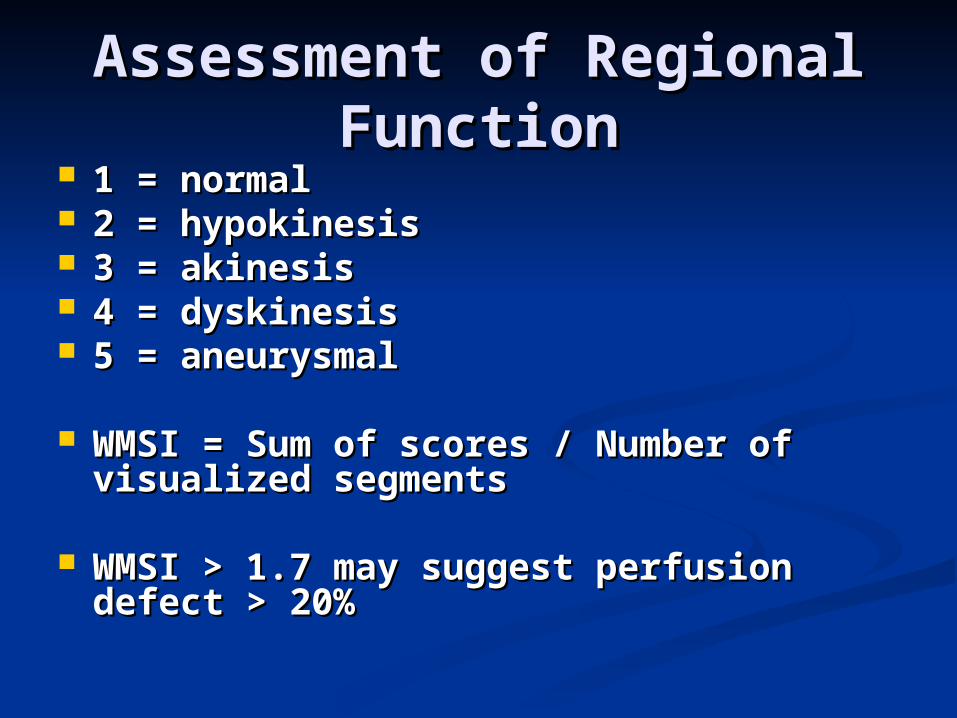
Assessment of Regional Assessment of Regional FunctionFunction
1 = normal1 = normal 2 = hypokinesis2 = hypokinesis 3 = akinesis3 = akinesis 4 = dyskinesis4 = dyskinesis 5 = aneurysmal5 = aneurysmal
WMSI = Sum of scores / Number of WMSI = Sum of scores / Number of visualized segmentsvisualized segments
WMSI > 1.7 may suggest perfusion WMSI > 1.7 may suggest perfusion defect > 20%defect > 20%

Assessment of Regional Assessment of Regional FunctionFunction
Qualitative estimation errors due to:Qualitative estimation errors due to:
Underestimation of EF due to endocardial Underestimation of EF due to endocardial echo dropout echo dropout
and seeing mostly epicardial motionand seeing mostly epicardial motion
Underestimation of EF with enlarged LV Underestimation of EF with enlarged LV cavity; a large cavity; a large
LV can eject more blood with less LV can eject more blood with less endocardial motionendocardial motion
Overestimation of EF with a small LV cavityOverestimation of EF with a small LV cavity
Significant segmental wall motion Significant segmental wall motion abnormalities abnormalities





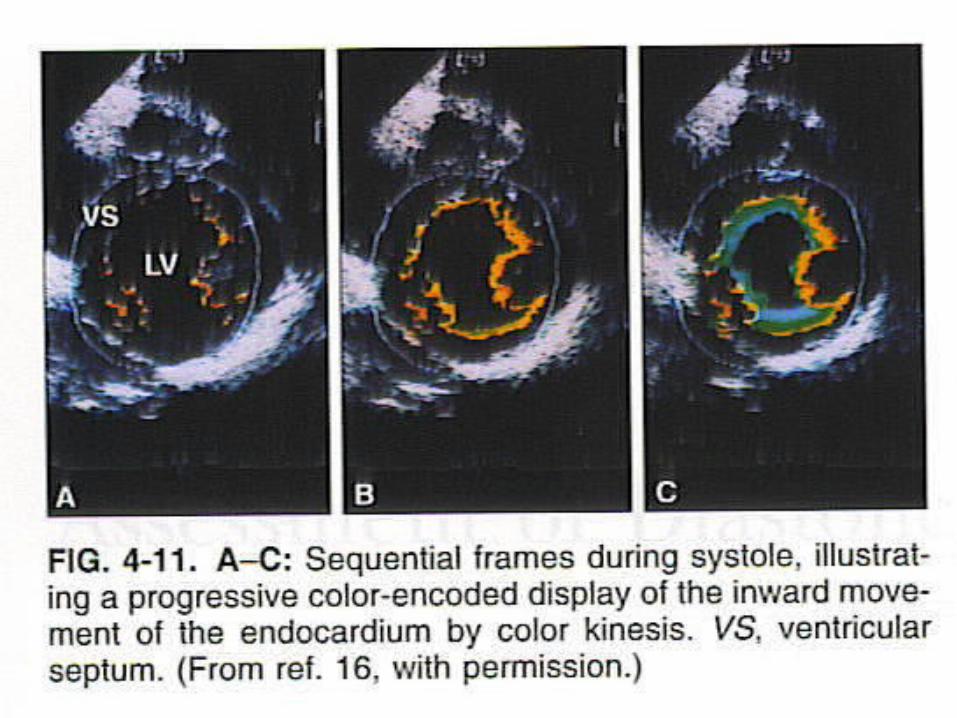
Doppler Tissue Imaging for Doppler Tissue Imaging for Wall Motion AnalysisWall Motion Analysis
Myocardium is color-coded according Myocardium is color-coded according to velocity to velocity
On P-Short Axis view, normal LV On P-Short Axis view, normal LV anterior wall motion during systole is anterior wall motion during systole is blue (away from transducer), and the blue (away from transducer), and the posterior wall motion is red (toward posterior wall motion is red (toward transducer); akinesis will have no colortransducer); akinesis will have no color


SummarySummary LV Mass Quantification: M-mode, Area-LV Mass Quantification: M-mode, Area-
length method, Truncated ellipsoid length method, Truncated ellipsoid method, and Subjective assessment. method, and Subjective assessment.
LV Volume Quantification: M-mode, LV Volume Quantification: M-mode, Subjective assessmentSubjective assessment
LV Function Quantification: Modified LV Function Quantification: Modified Simpson’s and Subjective Assessment Simpson’s and Subjective Assessment by region………….Also by M-mode, by region………….Also by M-mode, Single plane area length method, Single plane area length method, Velocity of Circumferential Shortening, Velocity of Circumferential Shortening, Mitral Annular Excursion, EPSS, Rate Mitral Annular Excursion, EPSS, Rate of Rise of MR jet, Index of myocardial of Rise of MR jet, Index of myocardial performance, etc…….. performance, etc……..
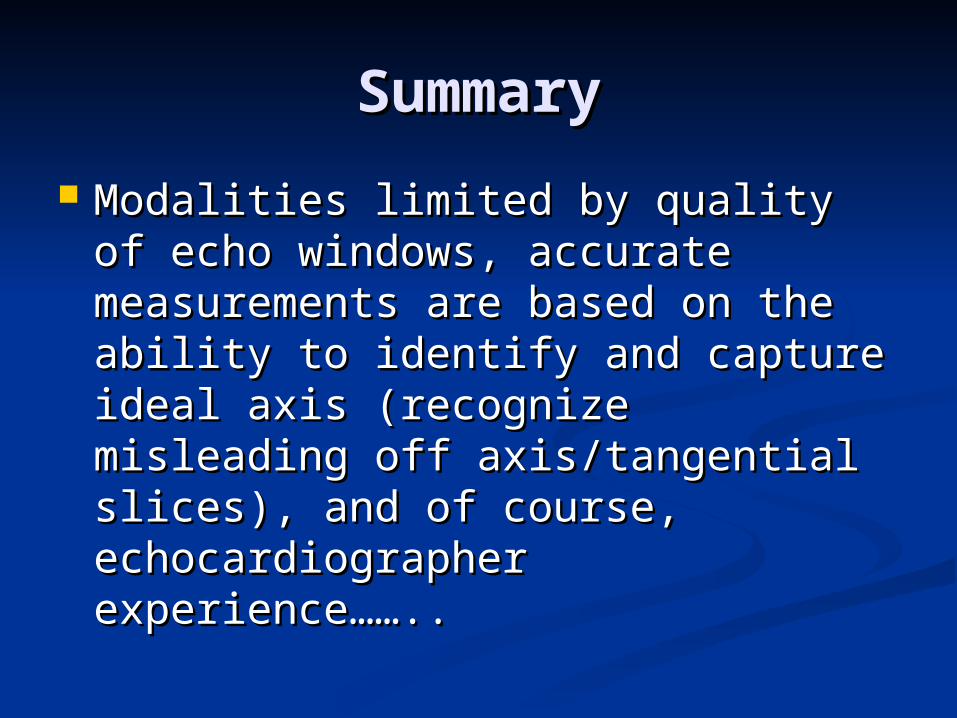
SummarySummary
Modalities limited by quality of echo Modalities limited by quality of echo windows, accurate measurements windows, accurate measurements are based on the ability to identify are based on the ability to identify and capture ideal axis (recognize and capture ideal axis (recognize misleading off axis/tangential slices), misleading off axis/tangential slices), and of course, echocardiographer and of course, echocardiographer experience…….. experience……..

CORONARY ARTERY CORONARY ARTERY SUPPLYSUPPLY
Regional wall analysis correlates Regional wall analysis correlates well with coronary artery supplywell with coronary artery supply
LAD – anterior, septumLAD – anterior, septum RCA – inferior, basal septumRCA – inferior, basal septum Circumflex – lateral, posteriorCircumflex – lateral, posterior

LV SYSTOLIC FUNCTION-LV SYSTOLIC FUNCTION-EYEBALL ASSESSMENTEYEBALL ASSESSMENT
Experienced operatorExperienced operator Quick and easyQuick and easy SubjectiveSubjective