ECG Rounds July 22, 2004 Adam Oster R4. 14M with Palpitations:
34
ECG Rounds ECG Rounds July 22, 2004 July 22, 2004 Adam Oster R4 Adam Oster R4
-
Upload
reynold-watkins -
Category
Documents
-
view
219 -
download
0
Transcript of ECG Rounds July 22, 2004 Adam Oster R4. 14M with Palpitations:

ECG RoundsECG Rounds
July 22, 2004July 22, 2004
Adam Oster R4Adam Oster R4

14M with Palpitations:14M with Palpitations:

14M with Palpitations14M with Palpitations
Adam Oster
AVRT

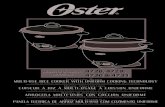
14M in sinus14M in sinus

Accessory Pathway Accessory Pathway SyndromesSyndromes WPW one of many accessory pathway WPW one of many accessory pathway
diseasesdiseases Bundle of KentBundle of Kent Classically 3 features…Classically 3 features… Accessory pathway has longer Accessory pathway has longer
refractory period during long cycle refractory period during long cycle lengths (sinus rhythm) lengths (sinus rhythm)
Can conduct faster than the AVNCan conduct faster than the AVN MC Tachycardia is MC Tachycardia is
– orthodromic AVRT (70-80%)orthodromic AVRT (70-80%)

Orthodromic AVRTOrthodromic AVRT
Usually initiated by PACUsually initiated by PAC– Accessory pathway refractoryAccessory pathway refractory– PAC PAC Anterograde conduction Anterograde conduction
down AVN and retrograde up down AVN and retrograde up accessory pathwayaccessory pathway
– Narrow QRSNarrow QRS

AVRT vs AVNRT: AVRT vs AVNRT: Rosen 2002Rosen 2002

AVNRT vs AVRT:AVNRT vs AVRT:Journal of the American College of Cardiology. May, Journal of the American College of Cardiology. May, 2003.2003.

AVNRT vs AVRTAVNRT vs AVRT
N=148 with ECGs both in narrow-N=148 with ECGs both in narrow-complex SVT and in SRcomplex SVT and in SR
Gold standard was Gold standard was electrophysiologic studies electrophysiologic studies followed by catheter ablation if followed by catheter ablation if necessarynecessary
3 blinded EPs reviewing for3 blinded EPs reviewing for apriori apriori ECG findingsECG findings



AVNRT vs AVRTAVNRT vs AVRT
Adam Oster
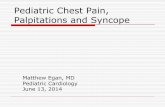
interobserver agreement 84-91%HR=slightly faster in AVRT but not statistically significant (213 vs 199)

AVNRTAVNRT
Adam Oster
psuedowaves likely d/t retrograde P waves that distort the QRS

AVNRTAVNRT

AVNRT vs AVRTAVNRT vs AVRT
Accuracy = 91%
Adam Oster
univariate analyzersuse RP>100msec since this was found in 84% AVRT and only 9% AVNRTP waves more often visible during AVRT (90% vs 30%


AVNRTAVNRT

Usefulness of the ST-Usefulness of the ST-Segment in aVRSegment in aVR
American Journal of Cardiology. December, 2003.American Journal of Cardiology. December, 2003. N=338 in PSVTN=338 in PSVT All had EP studiesAll had EP studies

The ST-segment in aVRThe ST-segment in aVR

AVRTAVRT

AVRTAVRT

Usefulness of the ST-Usefulness of the ST-Segment in aVRSegment in aVR ST seg elevation in AVRST seg elevation in AVR
– For AVRTFor AVRT Sens 71%Sens 71% Spec 70%Spec 70% Accuracy 70%Accuracy 70%

AVRTAVRT

AVNRT vs AVRT:AVNRT vs AVRT:Putting it All TogetherPutting it All Together V1V1
– Psudo r’ Psudo r’ think AVNRT think AVNRT Inferior leadsInferior leads
– Psuedo S Psuedo S think AVNRT think AVNRT ST up in AVRST up in AVR
– Think AVRT (but not only)Think AVRT (but not only)



Management Management PrinciplesPrinciples StabilityStability Narrow vs wideNarrow vs wide Regular vs irregularRegular vs irregular

AF/antidromic/WCT


WPW:WPW:Localising the PathwayLocalising the Pathway LOCATION V1 V2 QRS axis left LOCATION V1 V2 QRS axis left
posteroseptal (type A) +ve +ve posteroseptal (type A) +ve +ve left right lateral (type B) -ve -ve left right lateral (type B) -ve -ve left left lateral (type C) +ve +ve left left lateral (type C) +ve +ve inferior (90 degrees) right inferior (90 degrees) right posteroseptal -ve -ve left posteroseptal -ve -ve left anteroseptal -ve -ve normal anteroseptal -ve -ve normal

Anteroseptal pthwy

AxisAxis


Lt lateral pathway