ECCMID 2014 Year in Infection Control

of 75
Transcript of ECCMID 2014 Year in Infection Control
-
8/12/2019 ECCMID 2014 Year in Infection Control
1/75
Year in Infection Control
May 2013-April 2014
Part IBarry Cookson
University College, London,
United Kingdom
Declarations: Gojo, Ecolab, Qiagen
Part II
Christina Vandenbroucke-Grauls
VU University medical center, Amsterdam,The Netherlands
Declarations: Biomerieux
-
8/12/2019 ECCMID 2014 Year in Infection Control
2/75
Part 1: Barry Cooksons Topics
Improving evidence base in infection control
Modelling
Surveillance including Surgical, LTCF, Costings
Typing/Tracking Organisms
MRSA
Interventions
Screening/Suppression of MRSA Hand hygiene
-
8/12/2019 ECCMID 2014 Year in Infection Control
3/75
Part 2: Christina Vandenbroucke-Grauls
Topics
Antimicrobial resistance & antibiotic use
ESBL and carbapenemases
Clostridium difficile
The hospital environment
Gender
-
8/12/2019 ECCMID 2014 Year in Infection Control
4/75
The Flos
Florence Nightingale (1820-1910)
-
8/12/2019 ECCMID 2014 Year in Infection Control
5/75
Pubmed & reading 12 Journals
Blogs
Twitter
Sources for Presentations
www.micro-blog.info
Otter & Yezli
http://i-prevent.blogspot.nl A.Voss
www.haicontroversies.blogspot.nlPerencevich, Diekema, Edmond
http://www.micro-blog.info/http://i-prevent.blogspot.nl/http://www.haicontroversies.blogspot.nl/http://www.haicontroversies.blogspot.nl/http://i-prevent.blogspot.nl/http://i-prevent.blogspot.nl/http://i-prevent.blogspot.nl/http://www.micro-blog.info/http://www.micro-blog.info/http://www.micro-blog.info/ -
8/12/2019 ECCMID 2014 Year in Infection Control
6/75
Acknowledge Colleagues help
Sheldon Stone
Olga Paniara
Modelling and Big Data
Ben Cooper, Sarah Deeny & Julie Robotham
ICPIC (Eli Perencevich & Andreas Widmer) ICAAC (Andreas Voss)
2013 ECCMID (Benedetta Allegranzi & Robert Skov)
presentations: complement, augment
Importance of ESCMID CPD library: many are
resource slides as little time to discuss in-depth
-
8/12/2019 ECCMID 2014 Year in Infection Control
7/75
The Flos Special Award of the Year is
Cardiff University Library, Cochrane Archive, University Hospital Llandough.
-
8/12/2019 ECCMID 2014 Year in Infection Control
8/75
1) Improving the quality of the infection control evidence
base: research inform guidelines/guidance
for policies for safer patient care
-
8/12/2019 ECCMID 2014 Year in Infection Control
9/75
Tools for improving the evidence base
of scientific literature
CONSORT for randomized controlled trials (1996)
STROBE for observational studies (2007)
ORION for intermittent time series & outbreaks (2007)
Preferred Reporting Items for Systematic Reviews &
Meta- Analyses (PRISMA) for systematic reviews &
meta analyses (2009)
EQUATOR Network (2006)
http://www.equator-network.org/resource-centre/library-
of health-research-reporting/
STROME-ID (2014)
http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/http://www.equator-network.org/resource-centre/library-of%20health-research-reporting/ -
8/12/2019 ECCMID 2014 Year in Infection Control
10/75
PLoS Med 10(8): e1001504.
doi:10.1371/journal.pmed.1001504
PLOS Med a champion and published previously
STROBE
Evidence that CONSORT & PRISM improved the literature
Published: August 27, 2013Studies also show that the quality of reporting overall
remains suboptimal as not all journals endorse
or enforce the use of reporting guidelines
Comment: this is certainly true for infection control
and related journals
-
8/12/2019 ECCMID 2014 Year in Infection Control
11/75
Reviewed outbreaks reported in So Paulo State, Brazil, &
verify compliance with mandatory outbreak notification
Explored potential for ORION to inform where need to to
improve competencies
Only 15/87 (17%) published outbreaks reported to authorities
Poor/Varied compliance with ORION categories
Background 32% , Objectives 75% , Participants 2%,
Setting 46% , Infection-Related Outcomes13%,
Interventions 52% & Culture-Typing 55%Issue:Missed opportunity to stratify by Journals requirements
for ORION (expected for authors and evaluation by referees)
Pires et al, AJIC 42 (2014) e47-e5
-
8/12/2019 ECCMID 2014 Year in Infection Control
12/75
-
8/12/2019 ECCMID 2014 Year in Infection Control
13/75
-
8/12/2019 ECCMID 2014 Year in Infection Control
14/75
PLoS Med 11(2): e1001603
doi:10.1371/
journal.pmed.1001603
Differences in:
1) Publication format
2) Work processes
3) Author team
Management
4) Statistical methods.
-
8/12/2019 ECCMID 2014 Year in Infection Control
15/75
Current
Emerging
Health Knowledge Ecosystems
Modelling!
PLoS Med 11(2): e1001603
doi:10.1371/
journal.pmed.1001603
o e ng
-
8/12/2019 ECCMID 2014 Year in Infection Control
16/75
o e ngA previous ECCMID Debate (2012)
Audience split on utility!
Everything should bemade as simple as possible,
but not simplerAlbert Einstein
-
8/12/2019 ECCMID 2014 Year in Infection Control
17/75
We argue that usability & stability of a model is an outcome
of the negotiation that occurs within the networks &
discourses surrounding it.
PLoS ONE 8(10): e76277.
doi:10.1371/journal.pone.0076277
PLoS Med 10(10): e1001540.
doi:10.1371/journal.pmed.1001540
We have found evidence to suggest that identification of
uncertainties, combined with their deproblematisation
can act to stabilise the role of scientific modelling in
decision-making
-
8/12/2019 ECCMID 2014 Year in Infection Control
18/75
Clin Microbiol Infect 2013; 19: 993998
Mathematical models play an important role in helpinghealthcare systems to respond to ongoing epidemics or
plan the logistics of various theoretical scenarios
Prediction & model-based management of
epidemics in their early phase are quite unlikely tobecome the norm. far too complex to be predictable
BC: so do we guess: sometimes nothing else is available?
Flu: pnas.org/content/early/2011/10/24/1103002108.short
Internetbiosurveillance systems can detect an outbreak
of an infection more rapidly than ever before.
BC : this may be a bit premature?
-
8/12/2019 ECCMID 2014 Year in Infection Control
19/75
The Flos Honorary Award of the Year goes to Prof Tim Berners-Lee
Inventor of the World Wide Web
25thAnniversary
-
8/12/2019 ECCMID 2014 Year in Infection Control
20/75
3) Surveillance
-
8/12/2019 ECCMID 2014 Year in Infection Control
21/75
Lancet Infect Dis 2014;14: 16068
Dengue & Influenza reviewed
Complement not replace existing systems
Many issues described e.g. Lack of access to internet
Populations vary in internet use and Health-seeking
behaviour (BC: sample migration e.g. Facebook?)
USA poor sensitivity and spatial resolutionnecessary to detect small, localised flu outbreaks
Also see Big Data FT article
-
8/12/2019 ECCMID 2014 Year in Infection Control
22/75
Big data: are we making a big mistake?
FT Magazine: March 28, 2014: Tim Harford
Googles estimates of the spread of flu-like illnesses
were overstated by almost a factor of two. Google cared
about correlation rather than causation
The End of Theory: with enough data, the numbersspeak for themselves .. hopelessly naive where
spurious patterns vastly outnumber genuine discoveries.
When it comes to data, size isnt everything.
Non random.. sampling error USA twittersare disproportionately young, urban/suburban & black
(Sample migration; Super tweeters?)
-
8/12/2019 ECCMID 2014 Year in Infection Control
23/75
Cape Town Sunday Times
Lancet Infect Dis 2014;14: 16068
-
8/12/2019 ECCMID 2014 Year in Infection Control
24/75
Journal of Hospital Infection
-
8/12/2019 ECCMID 2014 Year in Infection Control
25/75
(2014) 34e41
Referral to:
Observed rate
Supra Regiona
specialistHospitals
Created
Same
Collective
-
8/12/2019 ECCMID 2014 Year in Infection Control
26/75
Murchan et al,EMRSA-16 spread in
England and Wales.
J Clin Microbiol
2004; 57: 345-346.
HAI results, ECDC PPS 2011-2012
-
8/12/2019 ECCMID 2014 Year in Infection Control
27/75
HAI results, ECDC PPS 2011 2012
HAI prevalence:
Overall: 13829/231459patients with 1 HAI
HAI prevalence: 6.0%
Country range: 2.3%-10.8%
15000 HAIs; 1.1 HAI/patient
HAI present at admission: 23%
Same hospital: 55%
33% surgical site infection
HAI during current hospitalisation: 76% of HAIs, prevalence: 4.5%
Median time to onset of HAI: 12 days
Microorganism reported: 45.9%
Prevalence antimicrobial use for treatment of hospitalinfection: 6.4%
95% of patients with HAI received >=1 antimicrobial onday of survey
Source: ECDC PPS, 2011-2012
(1) incl. C. difficileinfections 3.6%
(2) incl. clinical sepsis 5.3%
23%
19%
20%
11%
8%
6%4%
10%
Pneumonia/LRTI
Urinary tract
Surgical site infection
Bloodstream
Gastrointestinal (1)
Systemic (2)
Skin/Soft tissue
Other/unspecified
Type of HAI
30 countries (29 EU/EEA countries+ Croatia), 33 PPSs (networks)
2014:12;7|
Observed vs predicted HAI prevalence by country
-
8/12/2019 ECCMID 2014 Year in Infection Control
28/75
Observed vs predicted HAI prevalence by country,
ECDC PPS 2011-2012
0 2 4 6 8 10 12 14 16 18 20
LatviaRomania
LithuaniaSlovakiaBulgaria
UK-WalesUK-N. Ireland
MaltaHungary
Czech RepublicUK-Scotland
FranceGermany
IrelandLuxembourg
EstoniaCroatia
UK-EnglandAustria
ItalySlovenia
PolandCyprus
BelgiumSweden
NetherlandsFinlandNorway
Spain
GreeceDenmark*
IcelandPortugal
Patients with HAI (%)
Observed HAI prevalence (%)(with 95% confidence interval)
Predicted HAI prevalence (%)(based on case-mix)
http://www.ecdc.europa.eu/en/publications/Publication
althcare-associated-infections-antimicrobial-use-PPS.
Structure & process indicators:
-
8/12/2019 ECCMID 2014 Year in Infection Control
29/75
ppercentage of single room beds
Single room beds in participating hospitals (%): median = 11.1%
Source: ECDC, 2012 (ECDC PPS data as of 23/11/2012)
0 20 40 60 80 100
N of single room beds*100 /Total beds
UK-WalesUK-Scotland
UK-Northern IrelandUK-England
SwedenSpain
SloveniaSlovakiaRomaniaPortugal
PolandNorway
NetherlandsMalta
LuxembourgLithuania
LatviaItaly
IrelandIceland
HungaryGreece
GermanyFranceFinlandEstonia
DenmarkCzech Republic
CyprusCroatia
BulgariaBelgiumAustria
*Poor data representativeness
Alcohol hand rub consumption in acute care
-
8/12/2019 ECCMID 2014 Year in Infection Control
30/75
p
hospitals, ECDC PPS 2011-2012
-
8/12/2019 ECCMID 2014 Year in Infection Control
31/75
HAI PPS 4600 trained
Susan Hopkins lead, HP Agency & HP Scotland
HALT 2 PPS 1700 LTCFs staff trained.Fidelma Fitzpatrick & Tracey Dillane,
HSE & HP Surveillance Centre
-
8/12/2019 ECCMID 2014 Year in Infection Control
32/75
2013:
http://www.ecdc.europa.eu/en/
publications/Publications/infect
ion-control-core-
competencies.pdf2014-15: TRICE-Implementation Strategy includes
IC Course assessments IC/HH WIKI : ESCMID SGs to be involved
Revisiting TRICE IC Resources
Awaiting clearance fo
ECDC-Funded SIGHT Project
-
8/12/2019 ECCMID 2014 Year in Infection Control
33/75
ECDC-Funded SIGHT Project
Should be in Lancet ID (Zing et al)
-
8/12/2019 ECCMID 2014 Year in Infection Control
34/75
Increasing Healthcare Delivery in the Community Increasingly aged populations
Decreasing lengths of hospital stay: HAIs
presenting in the community
Increasing numbers of step-down from hospital andhybrid (Step-Down/Residential) facilities
Issues
with definitions of names of facilities
Lack of surveillance, infection control standards,
guidelines and audit .
LOW PRIORITY IN MANY COUNTRIES
See: Moro et al, ICHE 2010; 31 (suppl. 1); 559-62 (IPSE WP7)
Cookson et al, J Hosp Infect 2013; 85: 45-53 (HALT 1)
-
8/12/2019 ECCMID 2014 Year in Infection Control
35/75
Carl Suetens
ECDC
Championed HALT
Antoon Gijsens
DG SANCO
Bea Jans
HALT Lead
LTCF a late addition
-
8/12/2019 ECCMID 2014 Year in Infection Control
36/75
Cookson et al, J Hosp Infect 2013; 85: 45-53.
-
8/12/2019 ECCMID 2014 Year in Infection Control
37/75
HALT-1 & 2 Reports
Katrien Latour, Abstract No ECCMI-4351
http://www.ecdc.europa.eu/en/Pages/home.aspx
5thMay 2014
http://www.ecdc.europa.eu/en/Pages/home.aspxhttp://www.ecdc.europa.eu/en/Pages/home.aspx -
8/12/2019 ECCMID 2014 Year in Infection Control
38/75
Additional & increasing burden of AMR organisms
Main increases are in AMR organisms MSSA continuing increases
MRSA increases 7.6%/Y then decreases 4.8%/Y 200
-
8/12/2019 ECCMID 2014 Year in Infection Control
39/75
Surgical Site Infections
(SSIs)
-
8/12/2019 ECCMID 2014 Year in Infection Control
40/75
Korol et al, PLoS ONE 8(12): e83743. doi:10.1371/journal.pone.0083743
1) Challenging:
very rich literature
-
8/12/2019 ECCMID 2014 Year in Infection Control
41/75
very rich literature
many study designs,
settings,
categorizations &
definitions
2) Despite this
they consistently
found associated
SSI risk factors
3) Risk Factors
relate to:
reduced fitness,
patient frailty,
surgery duration,
& complexityBC: Body warming,
glucose control,
triclosan stitches?
-
8/12/2019 ECCMID 2014 Year in Infection Control
42/75
Risk score gauged independent influence of each risk factor
New logistic regression approach of quantifying the influence of
different operative types on SSIs
Model used 181 894 operations for derivation, 181 146 for validation
SSIRS captured 89.7% of the validation population
Web based system available significantly better discrimination than NNIS
Basic Risk SSI Index
Also a simpler SSIRS index permits 30-day SSI risk bedside estimation
without computational aids
BC: Needs external validation. ECDC interested?
van Walraven C, Musselman R. PLoS ONE 2013;8:e67167
-
8/12/2019 ECCMID 2014 Year in Infection Control
43/75
Owens et al, JAMA. 2014;311:709-716
Retrospective analysis: 284, 098 ambulatory surgical procedure
Databases of 1/3 US population in 8 dispersed USA states
Needed postsurgical acute care visits
General, orthopaedic, neuro, gynae, & urologic surgeryLength of stay less than 2 days
SSIs at 14days 3.09 /1000 ambulatory surgical procedures
30days 4.84 /1000 ambulatory surgical procedures
63.7% within 14 days of the surgery: limited risk factor analys 93.2% needed inpatient treatment
Low relative to all causes but significant adverse events
The Post Discharge SurveillanceAn Elephant in the Room!
-
8/12/2019 ECCMID 2014 Year in Infection Control
44/75
An Elephant in the Room!
http://en.wikipedia.org/wiki/Elephant
Difficult to compare studies as
differences in e.g.
Lengths of stay
Operative categories
Definitions of infections
Methods of data collection:
Re-admissions only! Telephone or Patient or
Healthcare worker reporti
If staff/patients are trained
Lack detail so work canbe repeated
-
8/12/2019 ECCMID 2014 Year in Infection Control
45/75
American Journal of Infection Control 41 (2013) 591-6
Journal of Hospital Infection 86 (2014) 127e132
American Journal of Infection Control 41 (2013) 549-53
Ann Intern Med. 2013;159:447-455.
Post Discharge Surveillance (PDS)
-
8/12/2019 ECCMID 2014 Year in Infection Control
46/75
J Hospital Infect 2013; 84: 267
(& refs to two previous letters)
Disputes including English HPA (PHE) SSI system do not
bench mark PDS data
Brisbane group supported English HPA responding:
Until a valid & cost-effective solutionPDS is found donot bench mark.
Hospitals are required to undertake PDS, so the data can
be used for internal (i.e. local) quality improvement
Should not be required to submit PDS data for publicscrutiny or be penalized for not doing so.
-
8/12/2019 ECCMID 2014 Year in Infection Control
47/75
-
8/12/2019 ECCMID 2014 Year in Infection Control
48/75
Raschka et al, AJIC 2013;41: 773-7
19% less selected HAIs over 4 years
Cost avoidance of at least $9 million
80% in last two years!
(so enormous potential: useful to quote internationally)
Interesting methodology Vancouver regional
Canadian Inf. control
programme
Standardized policies,
procedures, and initiatives(including hand hygiene
campaign)
Th Fl E t di A i f th Y
-
8/12/2019 ECCMID 2014 Year in Infection Control
49/75
The Flos Extraordinary Anniversary of the Year
60 years since description
of DNAs structure
Watson, Crick,
(Franklin and Wilkins)
http://www.chemheritage.org/discover/online-resources/chemistry-in-history/themes/biomolecules/dna/watson-crick-wilkins-franklin.aspx
4) Typing & Tracking HAI Organisms
-
8/12/2019 ECCMID 2014 Year in Infection Control
50/75
Lancet Infect Dis 2014; 14: 34152
-
8/12/2019 ECCMID 2014 Year in Infection Control
51/75
Medline database
searches with terms
Infection
&
Molecular Epidemiology
No papers/100K/year
-
8/12/2019 ECCMID 2014 Year in Infection Control
52/75
20 items added to 22 item STROBE checklist
Should advance the quality & transparency of
scientific reporting, with clear benefits for
evidence reviews & health-policy decision making
Lancet Infect Dis 2014; 14: 34152
Lancet Infect Dis 2014; 14: 34152
-
8/12/2019 ECCMID 2014 Year in Infection Control
53/75
Optimisation of NGS information for Infection Control TeamsSee also :Humphries & Coleman Letter: http://dx.doi.org/10.1016/j.jhin.2013.05.002
-
8/12/2019 ECCMID 2014 Year in Infection Control
54/75
Educate users (STROME-ID) e.g. strengths and limitations
Clear objectives to ensure optimises patient care/safety
Interpretation needs detailed epidemiological data
Golden fleece TIMELY automatic appropriate simplified
discriminant data : (TATs not stated in many papers!)
Dialogue with reference laboratories and others with expertise
this area to optimize its potential.
Consider accreditation requirements for Reference labs
National information considered National funding ref Public Health aspects
See also :Humphries & Coleman Letter: http://dx.doi.org/10.1016/j.jhin.2013.05.002
-
8/12/2019 ECCMID 2014 Year in Infection Control
55/75
Ehrlich & Post JAMA Internal Medicine 2013;173: 1406-06
Struelens and Brisse. Euro Surveill. 2013;18(4):pii=20386.
Editorialand several very useful papers in issuealso look at: Price et al, CID 2014;58:60918
Invited paper: interesting analysis of potential
MRSA
-
8/12/2019 ECCMID 2014 Year in Infection Control
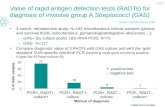
56/75
MRSA
Melo Christino et al Lancet 2013;382:205 (20 July 2013)
-
8/12/2019 ECCMID 2014 Year in Infection Control
57/75
Melo-Christino et al, Lancet 2013;382:205 (20 July 2013)
vanA +MRSA strain in Europe from Portuguese patient USA MRSA type (ST105, SCCmectype II: common
HAI strain in Portugal)
No epidemiological links to USA
vanA source may a wound VRE
Treatment progressing and no spread thus far
-
8/12/2019 ECCMID 2014 Year in Infection Control
58/75
Emerged in Brazil following multiple vancomycin courses
No spread so far: died with GNR BSI
Related to community USA 300 strain: has bsa CA MRSA
operon PVL negative
Perhaps element originated from a GRE in another patient
in the same room: patient also positive (late)
Transferable to other S aureus (WOW!!!!!) Worrying : USA 300 clades common globally
Rossi et al, N Engl J Med 2014;370:1524-31
Strommenger et al J Antimicrob Chemoth
-
8/12/2019 ECCMID 2014 Year in Infection Control
59/75
174 SA and MRSA of CC8 (including CA USA300) from 5 Continents
1957-2008 Phylogeny explored at 112 genetic housekeeping loci, AMR and
diverse mobile genetic elements
9 clades: 8 independent SCCmec acquisitions : started in mid-1970s.
88% carried plasmidic rep gene sequences (5 rep genes and eight repfamilies)
Increasing and stable AMR (9 classes) during the evolution of several
lineages, including USA300. (Comment: check pedigree of different
strains.)
Diverse virulence determinants
Perhaps WILL become a multiple resistant MRSA?
(USA300 now a hospital MRSA)
Strommenger et al, J Antimicrob Chemoth
2014; 69: 616622
-
8/12/2019 ECCMID 2014 Year in Infection Control
60/75
4 new MRSA mecA/C negative from 3 ST types from
Scottish patients
Perhaps due to identified amino acid substitutions in
their endogenous PBPs 1, 2 & 3?
Not BORSA strains, as resistant to both oxacillin &
cefoxitin
Need for vigilance ref molecular MRSA assays &
possible new drug target resistance MUST NOT ABANDON PHENOTYPIC TESTING
Xiaoliang et al, J Antimicrob Chemother 2014; 69: 594597
-
8/12/2019 ECCMID 2014 Year in Infection Control
61/75
A 55-pound or greater Hog producesat least 10 gallons of manure a day (!)
Manure spread on surrounding Iowan
fields
MRSA can be aerosolized from thismanure to human food or water
sources.
Carrel et al, Infect Control Hosp Epidemiol 2014;35(2):190-192
BetterPho
McKinnell et al, ICHE 2013; 34(: 161170
-
8/12/2019 ECCMID 2014 Year in Infection Control
62/75
McKinnell et al, ICHE2013; 34(: 161 170
Often ignored in studies & national screening programmes
Systematic review 1966-2012: 23 papers: 39,497 patients
Few studies looked at >1 such extra nasal site!
ICU admission: detects ~1/3 more
Hospital admission: >6% MRSA incidence: extra 37%
-
8/12/2019 ECCMID 2014 Year in Infection Control
63/75
CDC EIP-ABCs sentinel laboratory-based MRSA casefinding identified MRSA cultures in 9 US metropolitan areas
from 2005 through 2011
Detailed risk factor analyses for HA- & CA-MRSA
In 2011 invasive MRSA infections (80 461) 31% lower than in
2005
Dantes et al, JAMA Intern Med. 2013;173(21):1970-1978.
Dantes et al, JAMA Intern Med. 2013;173(21):1970-1978
-
8/12/2019 ECCMID 2014 Year in Infection Control
64/75
CA MRSA Stable: epidemiology
incomplete e.g. home/LTCF
Interventions
-
8/12/2019 ECCMID 2014 Year in Infection Control
65/75
Culture, Organisational &Behavioural Aspects
-
8/12/2019 ECCMID 2014 Year in Infection Control
66/75
Behavioural AspectsCulture
Excellent reviews: De Bono et al,J Hosp Infect.2014; 86:
1-6 and Borg,J Hosp Infect 2014; 86:161-68
Essential www site of Geert Hofstede
http://geerthofstede.com/dimensions-of-national-cultures
Hand Hygiene Studies Utilizing Shared Accountability and Financial Incentives
Talbot et al, ICHE2013; 34: 1129-1136
Positive deviance study: Marra et al,AJIC2013;41:984-8
Real-time assessment practice using a TheoreticalBehavioural Domains Framework. Fuller et al,AJIC
2014;42:106-10
Hot Topics!
U i l MRSA S i
http://geerthofstede.com/dimensions-of-national-cultureshttp://geerthofstede.com/dimensions-of-national-cultureshttp://geerthofstede.com/dimensions-of-national-cultureshttp://geerthofstede.com/dimensions-of-national-cultureshttp://geerthofstede.com/dimensions-of-national-cultureshttp://geerthofstede.com/dimensions-of-national-cultureshttp://geerthofstede.com/dimensions-of-national-cultureshttp://geerthofstede.com/dimensions-of-national-cultureshttp://geerthofstede.com/dimensions-of-national-cultureshttp://geerthofstede.com/dimensions-of-national-cultureshttp://geerthofstede.com/dimensions-of-national-cultures -
8/12/2019 ECCMID 2014 Year in Infection Control
67/75
Universal MRSA Screening
Universal MRSA Decolonisation/Suppression
Hammers to crack walnuts?
See posts on:
http://haicontroversies.blogspot.com
&
NEJM Letters
English Universal MRSA Screening
http://haicontroversies.blogspot.com/http://haicontroversies.blogspot.com/ -
8/12/2019 ECCMID 2014 Year in Infection Control
68/75
1) NOW Audit: Fuller et, al PLoS ONE 8(9): e74219
Implementation of universal screening was poor
Admission Screening performed on:
Emergency admissions 61% (median 67.3%)
Electives 81% (median 59.4%)
Very low MRSA admission prevalence:
Emergencies 1%: Electives 0.6%
Inpatient MRSA prevalence 3.3% (6% for original model)
2) Modelling
Consultation underway suggesting stopping universalscreening
Universal Decolonisation/SuppressionA Horizontal Strategy
-
8/12/2019 ECCMID 2014 Year in Infection Control
69/75
gy
Lee et al, 2013 doi 10.11.36/bmjopen-2013-003126
Derde et al,Lancet Infect Dis
2014; 14: 3139
Huang et al, N Engl J Med 2013. DOI: 10.1056/NEJMoa1207290
First RCT
Universal Antiseptic Use Risks
(Horizontal Strategies)
-
8/12/2019 ECCMID 2014 Year in Infection Control
70/75
( Horizontal Strategies )
At what rates of resistant organisms is it cost effective?
Mupirocin needed: how effective is it in reducing infections?
Increasing side effects?
How and how often used, rotate them?
What is best antiseptic to use e.g. octenidine? Inactive chlorhexidine/soap formulations?
Increasing disinfectant/antiseptic resistance
Increased quantities used
Sumps of bacteria e.g. leaking abscesses, suppurating
tracheostomies
Universal Antiseptic Use Risks
-
8/12/2019 ECCMID 2014 Year in Infection Control
71/75
(Horizontal Strategies)
Surveillance issues
Locally: short lengths of stay, not detect damaged
organisms
Nationally: no surveillance
Resistance cut-off agreements review?
Maillard et al,Microb. Drug Res., 2013
doi:10.1089/mdr.2013.0039
Morissey et al, PLoS One. 2014; 9: e86669.
doi:10.1371/journal.pone.0086669
Universal versus Targeted MRSA Screening?
-
8/12/2019 ECCMID 2014 Year in Infection Control
72/75
g gDeeny et al, JHI 2013
More efficient use of resources
Less potential for resistance to antiseptics
J Hosp Infect 2013; 85: 33-44
Hand hygiene
-
8/12/2019 ECCMID 2014 Year in Infection Control
73/75
Schweizer, et.al, Clinical Infectious Diseases 2014;58:24859
-
8/12/2019 ECCMID 2014 Year in Infection Control
74/75
Only 39 quasi-experimental & 4 cluster & 2 RCTs /8,148 studies
over 12 years
Insufficient studies to assess single interventions!How can we design bundles?
No of bundle components was not associated with greater effect:
Include one or two interventions tripled compliance
Include >two produced doubling of compliance
Two bundles effective and Three studies of each:
Education, Reminders, Feedback: OR (pooled) : 1.45 (1.12, 1.94)
If add Administrative Support, & alcoholic handrubs :
OR (pooled): 1.82 (1.69-1.97)
Rock et al, American Journal of Infection Control 41 (2013) 994-6
-
8/12/2019 ECCMID 2014 Year in Infection Control
75/75
Conclusion: HH before donning nonsterile gloves does not decrease
already low bacterial counts on gloves. HH before donning nonsterile
gloves may be unnecessary?
Comment: Saves time: will HCWs confuse with sterile glove usage
especially when stressed?
Use of scents in training1/3 increase in complianceComment: Effectiveness for: different staff? Sustained?
In real workplace? Pavlovian approach ethical? Own life.
Birnbach et al J Hosp Infect 2013;85: 79-81.