Ebola workforce development - World Bank · Web viewThe frontline STEER training is focused on EVD...
18
FINAL REPORT ON SURVEILLANCE TRAINING TO ENHANCE EBOLA RESPONSE AND READINESS (STEER) IN THE DEMOCRATIC REPUBLIC OF THE CONGO Date: 3 – 15 August 2019 Compiled by: NAME AFFILIATION DESIGNATION Dr. Ditu Kazambu AFENET/DRC Epidemiologist/ Regional Technical Coordinator Dr. Alain Magazani AFENET/DRC Epidemiologist/ Resident Advisor DRC FELTP Dr. Leopold Lubulwa MoH/DRC Epidemiologist, Epidemiology and Surveillance Unit Dr. Yassa Ndjakani CDC Country Office Epidemiologist Dr. Ben Masiira AFENET Secretariat Epidemiologist/ Outbreak Response Coordinator Dr. Herbert Kazoora AFENET Secretariat Epidemiologist/ Ag. Director Programs 1 | Page
Transcript of Ebola workforce development - World Bank · Web viewThe frontline STEER training is focused on EVD...

FINAL REPORT ON SURVEILLANCE TRAINING TO ENHANCE EBOLA
RESPONSE AND READINESS (STEER) IN THE DEMOCRATIC REPUBLIC OF
THE CONGO
Date: 3 – 15 August 2019
Compiled by:
NAME AFFILIATION DESIGNATION
Dr. Ditu Kazambu AFENET/DRC Epidemiologist/ Regional Technical Coordinator
Dr. Alain Magazani AFENET/DRC Epidemiologist/ Resident Advisor DRC FELTP
Dr. Leopold Lubulwa MoH/DRC Epidemiologist, Epidemiology and Surveillance Unit
Dr. Yassa Ndjakani CDC Country Office Epidemiologist
Dr. Ben Masiira AFENET Secretariat Epidemiologist/ Outbreak Response Coordinator
Dr. Herbert Kazoora AFENET Secretariat Epidemiologist/ Ag. Director Programs
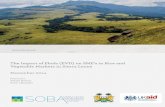
Participants from Beni amd Mbalako attending a training session
1 | P a g e

Executive summary
The Ebola virus disease (EVD) outbreak continues to ravage communities in North Kivu and
Ituri Provinces. The World Bank in collaboration with the Ministry of Health (MOH) and
other technical partners provided funding to implement a training program known as
Surveillance Training to Enhance Ebola Response and Readiness (STEER). This STEER
training aimed at strengthening prevention and control of the spread of the ongoing EVD
outbreak by creating a large workforce of frontline health workers and community health
workers known as relais communautaires (RECOs).
The training strategy adopted involved conducting four STEER trainings targeting
participants from provinces, health zones, health areas and communities in North Kivu and
Ituri Provinces. The four trainings were: training of trainers (ToT), STEER cascade-1,
cascade-2 and cascade-3 (Figure 1). The trainees were frontline health workers selected from
the provincial, health zone and health area levels in the North Kivu Province of DRC.
This report summarizes the four levels of the STEER trainings conducted between 3rd and 15th
August 2019. Overall, the trainees were selected from 20 EVD affected health zones and 332
EVD affected health areas within North Kivu Province. A total of 40 senior health workers,
342 mid-level health workers, 1,665 frontline health workers and 5,107 RECOs from EVD
affected areas were trained. The training focused on detection of EVD, contact tracing, IPC &
WASH, risk communication and psycho-social aspects of Ebola.
The key challenges that affected implementation of the STEER trainings at different levels
included: 1) insecurity in areas around Beni and Butembo which hindered movement of
participants to access training venues, 2) difficulty in communication and coordination due to
very poor or no telephone /internet network in some areas which caused delays in
transmission of the reports, and 3) difficulty in gathering field reports and other related paper
work due to the large number of trainings.
Recommendations include: 1) training of health workers in EVD affected health zones that
were left out in North Kivu, 2) conducting the STEER training in Ituri Province, and 3) close
supportive supervision and mentorship of the trained health workers and community health
workers (RECOs).
2 | P a g e

Background
The Ebola virus disease (EVD) outbreak response in North Kivu and Ituri Provinces has been
challenging due to the under-resourced health system. Effective EVD control measures
include active surveillance (i.e. case detection and reporting), effective infection prevention
and control (IPC) at healthcare facilities and risk communication. Currently, health workers
(HWs) in DRC’s highest risk health zones lack training and experience in surveillance, IPC,
and risk communication. Accordingly, health facilities continue to be an important source of
EVD propagation, with nosocomial cases linked to lack of adherence to IPC standards. Up to
144 health care workers (HCWs) had been affected by EVD by 23 July 2019.
The World Bank and the US Centers for Disease Control and Prevention (CDC) in
partnership with the Ministry of Health (MoH) have provided funding to implement Frontline
Surveillance Training to Enhance Ebola Response and Readiness (STEER). The frontline
STEER training is focused on EVD surveillance (case identification and reporting), infection
prevention and control (IPC) and risk communication. Frontline STEER will use a train-the-
trainers model that fits within and strengthens the existing DRC Field Epidemiology Training
Program (FETP) to rapidly scale-up a national cadre of HWs familiar with EVD detection
and response. Capacitating HWs to quickly identify suspect EVD cases and apply principles
of isolation, reporting, and infection control is a critical intervention for stopping the current
and future EVD outbreaks.
Building on DRC’s very successful FETP model, STEER will create a surge workforce of
facility-based HWs and community health workers known as relais communautaires
(RECOs) with knowledge in basic epidemiology and outbreak response principles relevant to
the healthcare setting (e.g. surveillance/case detection, IPC and risk communication) through
a mentorship model of training, similar to FETP-Frontline. Mentors included FETP
graduates, course facilitators from WHO, CDC and AFENET and other experienced public
health officials. The trainings focused on HCWs in EVD-affected health zones and health
areas but can be scaled-up to reach other high-risk health zones.
3 | P a g e

The training strategy (STEER training cascade model)
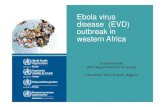
The training strategy adopted by the MoH and technical partners is summarized in figure 1
below. In brief, the agreed strategy involved conducting STEER trainings at three different
levels of the health system (health zones, health areas and community) in North Kivu
Province in DRC. The first STEER training was a training of trainers (ToT) involving 40
senior HCWs from North Kivu provincial level and the EVD affected health zones. During
cascade-1 STEER training, 20 HCWs trained during the ToT trained an average of 18 health
care workers in affected health zones. During cascade-2, each of the 18 health workers
trained 5 frontline HCWs in health areas. During cascade-3, each of the trained frontline
HCWs trained 3 community health workers (RECOs).
Figure 1: The STEER cascade model
4 | P a g e

Training objectives: ToT, cascade-1 & 2 trainings
1. Prevent the spread of Ebola disease to unaffected communities, ensuring early
detection, isolation and alerting of suspected EVD cases, occurring in health facilities,
affected and unaffected health areas in affected high-risk provinces of North Kivu and
Ituri.
2. Create a large workforce of health workers in health facilities with knowledge of the
basic principles of epidemiology and response to epidemics, which are essential for the
health system through a mentoring-based training model.
Training objectives: cascade-3 training
1. Report suspected cases of EVD.
2. Prevent the transmission of diseases using IPC methods.
3. Communicate to the community the risks using an effective way.
Training methods
The STEER trainings were conducted in EVD affected health zones and health areas in North
Kivu. The ToT training was delivered by national level trainers from several organizations
that included MoH, AFENET, CDC and WHO and the sessions were delivered by using
power point presentations, group discussions and practical exercises. The day-1 training
materials were delivered by the facilitators. From day-2 onwards, the presentations, practical
sessions and group exercises were led by the participants under close monitoring and
supervision by the facilitators.
Cascade-1 trainings were facilitated by the ToT trainees and the sessions were conducted
using power point presentations, exercises, simulations, micro-lessons and interactive
sessions. Day-1 training materials were delivered by the facilitators. From day-2 onwards, the
presentations, practical sessions and group exercises were led by the participants under close
monitoring and supervision by the facilitators, technical officers from the AFENET partner
organizations and FETP graduates.
Cascade-2 trainings were facilitated by the trainees from cascade-1 training and the heads of
the health zones. The sessions were conducted using power point presentations, exercises,
simulations, micro-lessons and interactive sessions. Day-1 training materials were delivered
5 | P a g e

by the facilitators. From day-2 onwards, the presentations led by the cascade-2 trainees
themselves.
Cascade-3 trainings were facilitated by the trainees from cascade-2 training. The training
sessions were conducted using pictures to illustrate how to identify and report a case of
Ebola. The sessions were interactive and the RECOs were allowed to ask as many questions
and possible.
All the teaching materials for these trainings were reviewed by technical officers from the
partner organizations (MoH, AFENET, CDC and WHO). Similarly, the trainings were
supervised by technical officers from these organizations, teams from the provincial division
of health, health zone and health area leadership, and FETP graduates who are currently
based in EVD outbreak areas.
6 | P a g e

Training achievements
A total of 2,047 HCWs were trained by AFENET and other partner organisations, of which
40 were senior HCWs trained during the ToT training, 342 were HCWs during cascade-1
(selected from health zones and health areas) and 1,665 were frontline HCWs during cascade-
2 (Figure 2). In addition to the HCWs, a total of 5,107 RECOs during the cascade-3 training
(Figure 2). The RECOs were selected from 332 EVD affected health areas within 20 health
zones in North Kivu Province (Figure 3).
Figure 2: Training achievements under each level of the STEER training
7 | P a g e

Figure 3: Distribution of health zones where STEER trainings were conducted
The team accomplished delivery of the following topics during the STEER trainings:
Ebola situation in the country
Ebola virus disease: signs, symptoms and transmission
Detection and suspicion of Ebola
Community case definitions
Active community case search
Utilization of a thermoflash
Contact tracing and follow-up
IPC and WASH (wash kit, chlorine, hand hygiene, cleaning and decontamination,
community body management, ring IPC)
Psychosocial aspects of EVD
Risk communication
8 | P a g e

Challenges
Ongoing insecurity in areas around Beni and Butembo which hindered movement of
participants from access training venues
Difficulty in communication and coordination due to very poor or no telephone /internet
network in some areas which caused significant delays in transmission of the reports to
the AFENET.
The large number of trainings that were conducted in health areas made it very difficult
to compile field reports and other related paper work from the facilitators.
Some of the EVD affected health zones and health areas were not trained due to
inadequate funding.
Recommendations
1. Training of health workers in EVD affected health zones in North Kivu Province that
were not trained during this phase of training.
2. Conduct the STEER training in Ituri Province to support EVD prevention and control
in this province.
3. The trained health workers and community health workers (RECOs) will require close
supportive supervision and continuous mentorship.
9 | P a g e

APPENDICES
Appendix 1: Training schedule for the ToT STEER training
Appendix 2: Training schedule for the STEER Cascade-1 & cascade-2 trainings
Time Topic
Day 1: Objectives: 1. Detect and identify suspected cases of EVD 2. Use training methods that will help put the new skills into practice 08:00-08:30 Arrival and registration of participants
08:30-09:15 Welcome and presentation of participants, including their role in the fight against EVD
09:15-09:45 General information on Ebola09:45-10:00 Coffee break10:00-10:45 Detection and Identification of EVD alert cases and suspected cases10:45-11:00 Group Exercise (Algorithm Sheet)11:30-12:15 Using thermos-flash, + practice
12:15-13:00 Create and revise a descriptive list
13:00-14:00 Lunch break
14:00-16:15 Supervision and mentoring others
16:30-17:00 Review and evaluation of the day
17:00-17:30 Facilitators debriefDay 2:Objectives: 1. Implement follow-up contacts 2. Analyze data for quality08:00-08:30 Revision Day 1 and orientation of day 2
8:30-10:00 Understanding chains of transmission
10:00-11:00 Introduction to contact follow-up
11:00-11:15 Coffee break11:15-12:15 Contacts under follow-up: report cards
10 | P a g e

12:15-13:00 Contacts under follow-up: What to do if a contact:• Not at home• Begins to have signs and symptoms of EVD
13:00-14:00 Lunch Break14:00-14:45 Community deaths
15:00-16:00 Follow-up supervision of contacts
16:00-17:00 What to do if you encounter an alert or suspicious case
17:00-17:15 Review, evaluation of the day, and start a business plan
17:15-17:45 Facilitators debrief
Day 3: Objectives: 1. IPC practices when screening patients 2. Effective community engagement3. Preparation for field activities08:00-08:15 Revision Day 2 and orientation of the day
08:15-09:45 Nosocomial infections and Introduction to IPC and WASH09:15-09:45 Triage09:45-10:45 Injection safety (SOP & Practical sessions)10:45-11:00 Coffee break11:00-12:00 Cleaning / Decontamination of soiled surfaces and linens (SOP &
practical session)
12:00-13:00 Biomedical waste management (SOP & practical session)
13:00-14:00 Lunch Break14:00-15:00 EDS & SWAB15:00-16:00 Psychological aspects16:00-17:15 Risk Communication and Community Engagement17:15-17:30 Review, workshop evaluation, Way forward
11 | P a g e

Appendix 3: Training schedule for the STEER Cascade-3 of RECOs
Heures Sujets8h00-8h30 Arrivée et enregistrement des participants8h30-9h15 Accueil et présentation des participants9h15-9h30 Ebola en RDC et dans notre zone de sante: Echanges sur le rôle de
chaque participant dans la lutte contre Ebola
9h30-10h15 Généralités sur Ebola (P1)10h15-11h00 Détection et Identification (P2)11h00-11h15 Pause-Café11h15-11h30 Exercice collectif (Feuille Algorithme)11h30-12h00 Recherche active des cas12h00-12h30 Utilisation de thermoflash (P10)12h30-13h15 Listage et suivi de contact13h15-14h15 Pause Répas14h15-15h15 PCI Communautaire
• Kit Wash (composition)Séance pratique• Hygiène des mains• Solution chlorée• Nettoyage et Décontamination des surfaces et linges
souillées• Gestion des corps dans la communauté (EDS) • Stratégie multimodale• Ring PC
15h15-16h30 Communication des risques et engagements communautaires• Aspects psychologiques• Circuit de l’information
16h30-17h00 Révision, évaluation de la journée, et plan d’action
12 | P a g e