
EBOLA VIRUS DISEASE PREPAREDNESS Screening, Detection & Planning.
Ebola Preparedness Protocols Carole DuPerre, RN, BSN, CIC Maine Medical Center Department of Epidemiology and Infection Prevention May 14, 2014
The story of the origin of the Ebola Virus
Ebola Virus Disease (EVD) Viral Hemorrhagic Fever
• Transmitted via blood and body fluids and excreta of symptomatic EVD-infected patients
• Human to Human transmission direct contact w/infected body fluids
• Infectiousness of body fluids increases as patients become more ill
• Incubation: 2 to 21 days; typically 8 – 10 days after exposure
• Communicability: Not before febrile phase and continues to increase with stages of illness as the viral load increase
• Remains from deceased persons are highly infectious
Clinical Presentation
• Signs and symptoms: • Fever >38.6 or 101.5 • Myalgias • Malaise • Anorexia • Diarrhea • Vomiting • Abdominal pain
Emory/Nebraska Experience
• 3-4 days non-specific febrile illness w/chills, myalgias, malaise, anorexia
• GI symptoms • (5-6 days) Diarrhea frequent/profuse (meas in liters) • (1-3) days Vomiting several days
• 5-7 days macular papular rash • Neurological: delirium (day 10), encephalopathy • Hematological: thromobocytopenia, abn LFTs • Multi-organ failure: dehydration, rapid AKI (dialysis) • Lung injury requiring mechanical ventilation
Methods of Control • No specific treatment
• Supportive clinical care
• No vaccine (Sierra Leone trials) • STRIVE: Sierra Leone Trial to Introduce a Vaccine against
Ebola
• Strict infection control protocols, PPE
Definitions • Person under investigation (PUI)
• Clinical criteria, includes fever > 38.0 (100.4), and additional symptoms such as severe headache, muscle pain, vomiting, diarrhea, abdominal pain, or unexplained hemorrhage; AND
• Epidemiologic risk factors within the past 21 days; travel to an area where EVD transmission is active, contact with BBF or human remains of a pt known to or suspected to have EVD or direct handling of bats or non-primates from disease-endemic areas
• Confirmed Case – A case with LAB-ID diagnostic evidence of Ebola virus infection
• Probable Case - A PUI whose epidemiologic risk factors include high or low risk exposure(s)
Definitions (cont) • High Risk exposure – Percutaneous or mucous membrane
exposure to BBF of EVD pt, direct skin contact w/o PPE, processing BBF of confirmed pt w/o appropriate PPE, direct contact with dead body w/o appropriate PPE
• Low Risk exposure – Household contact with an EVD person, other close contact with EVD pt in HCF or community setting, being w/in 3ft of an EVD pt or w/in pts room or care area for prolonged period while not wearing PPE, direct brief contact (i.e., shaking hands) w/o appropriate PPE.
• No known exposure – Having been in country in which an EVD outbreak occurred w/in the past 21 days and having had no high or low risk exposures.
R/O Ebola Patient in ED September 2015
• Young man seeks medical care in ED after sustaining head laceration while bicycling
• Brought to ED by a friend • Screening questions, + travel to W. Africa and fever • Returned from Ghana, West Africa 17 days earlier • R/O Ebola patient, placed in isolation • HERT staff step up to plate , Safety & Emergency Preparedness
Dept come to ensure staff donning/doffing appropriately • Ebola playbook reflects lessons learned during this real live
drill
Infection Control Methods • WHO recommendations: (Enhanced Precautions)
• PPE; Tyvek suit, PAPR, no skin showing, double glove (severity of illness/perception)
• Isolation Room; negative pressure room, no carpet, upholstered furniture and decorative curtains removed
• Staffing; 1:1 nursing care, buddy system, check list • Security; Logs coming and going of staff, visitors, etc. • Special Infectious Disease Unit (SIDU); privacy protection
for high profile infection control issues
IC Methods (cont) • Transportation:
• ED walk in; travel questions, exposure history, triage • Internal MMC clinic including OB triage clinic; travel
questions, exposure history, triage • External MMC; travel questions, exposure history, telephone
conversation with Hospital Epidemiologist • Ambulance; arrive at ED (wet/dry); decontamination bay,
wrap pt or use iso-chamber
IC Methods (cont) • Treating; Safe care will be delivered, treat empirically (i.e.,
malarial tx, blood transfusion) • Testing; POCT, I-stat (limited labs), x-ray, ventilation, dialysis,
conduits for remote technology methods • Cleaning; Germicidal agents w/3 minute contact time (purple
top wipes), daily cleaning high touch surfaces (bed rails, over bed table, equipment), virus shown to be viable up to 6 days in environment, discharge terminal clean, then bleach clean.
IC Methods (cont) • Laundry/linen and disposable dishes; three bag system
• Clear trash bag w/in room (bag 1) • Clear bag w/in anteroom (bag 2) no-touch technique, wipe outside
of bag w/purple wipe • Red bag w/in anteroom (bag 3) wipe w/purple wipe
• Waste; Red bag everything that leaves room, box at site for incineration
• Visitors/privacy issues; No visitors will be allowed in isolation room, Skype, face time, video conferencing, etc. Will be scheduled, controlled and screened. Compassionate exceptions may be made by the hospital epidemiologist.
IC Methods (cont) • Patient care equipment; minimize dedicated equipment, know
manufacturers recommendations • Specimen collection; Category A, consult with MeCDC prior
to specimen collection, primary container double bagged in two zip-locked biohazard specimen bags, transported in durable, leak-proof secondary containers,
• Discontinuation of precautions; Probable/confirmed cases only after receipt of negative Ebola PCR and approval from Epidemiology dept, duration of positive cases in conjunction w/state & federal authorities on case-by-case basis, Possible cases only when another diagnosis is ruled in
Dallas, Texas • 9/19 Index case departs Liberia • 9/20 Arrives @ Dallas/Fort Worth through Dulles airport • 9/24 He begins having symptoms • 9/25 Seeks medical care at Presbyterian Hsp for fever and
abdominal pain. Tells nurse he had travelled from Africa but was sent home.
• 9/28 Returns to hsp by ambulance placed in isolation • 9/30 He tests positive for Ebola
Dallas (cont) • 10/2 His family confined to their home • 10/8 Index dies • 10/10 1st nurse who provided care goes to hsp w/fever and tests
positive for Ebola • 10/13 2nd nurse who helped care for index flies back to Dallas
from Cleveland (visited mother on 10/8 in preparation for a wedding)
• 10/14 2nd nurse reports Ebola sx and placed on precautions • 10/15 2nd nurse transferred to Emery Univ Hsp, 1st nurse is
improving
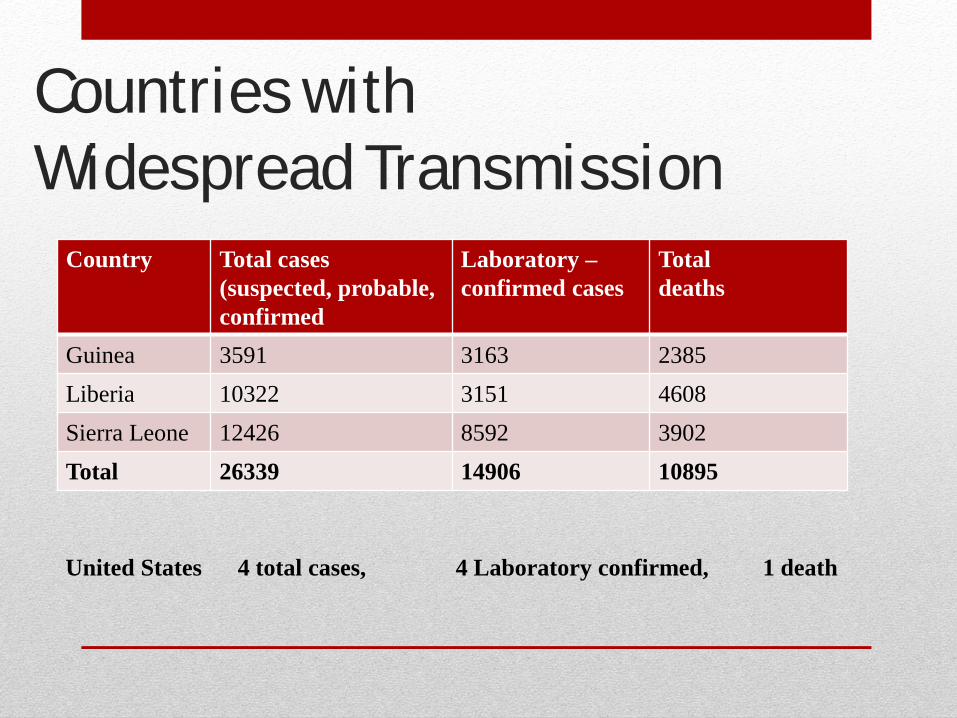
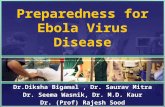
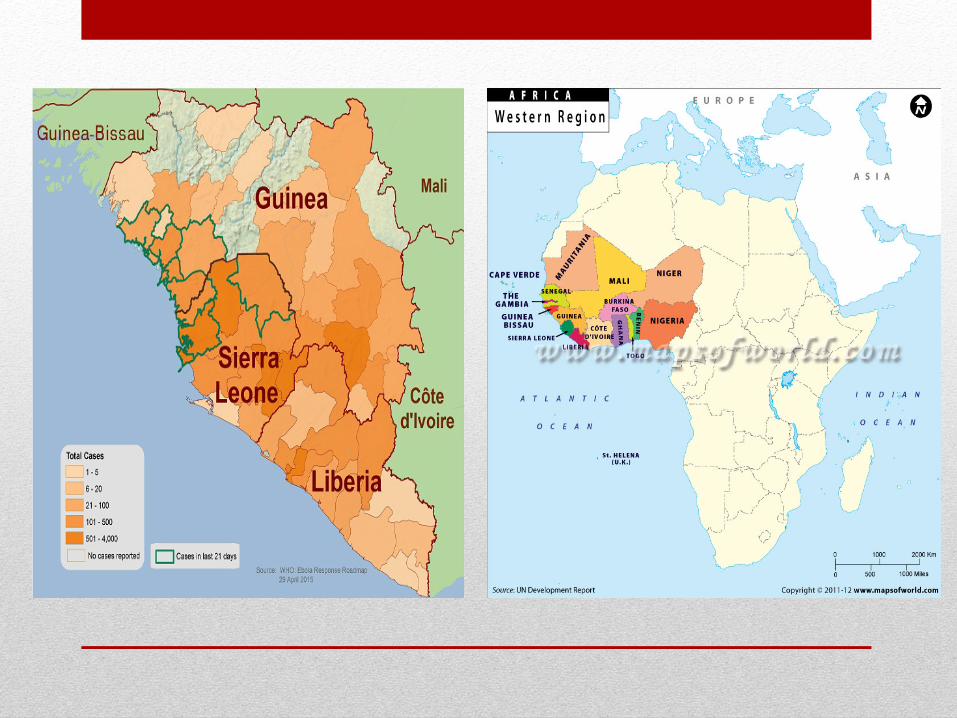
Countries with Widespread Transmission
Country Total cases (suspected, probable, confirmed
Laboratory –confirmed cases
Total deaths
Guinea 3591 3163 2385 Liberia 10322 3151 4608 Sierra Leone 12426 8592 3902 Total 26339 14906 10895
United States 4 total cases, 4 Laboratory confirmed, 1 death
References • http://www.cdc.gov/vhf/ebola • http://apps.who.int/ebola/ • http://www.emoryhealthcare.org/emory-university-hospital-
atlanta/ • http://emergency.cdc.gov/coca/calls/ • Heymann, David L. MD. Control of Communicable Diseases
Manual 20th Edition. Washington, D.C. American Public Health Association. (2015): 173-178. Print.