Ebola epidemic, 2013-2015
53
Matthew Rollosson, RN, MPH&TM Nurse Epidemiologist Tacoma-Pierce County Health department 2 April 2015
-
Upload
matthew-rollosson -
Category
Health & Medicine
-
view
145 -
download
0
Transcript of Ebola epidemic, 2013-2015

Matthew Rollosson, RN, MPH&TM Nurse Epidemiologist
Tacoma-Pierce County Health department 2 April 2015

Preferred over “Ebola hemorrhagic fever” ◦ Most people with EVD do not have
hemorrhagic symptoms Higher risk for bleeding Disseminated intravascular coagulation Thrombocytopenia
◦ Massive fluid loss due to vomiting and diarrhea ◦ Death is usually due to dehydration and
electrolyte disturbances
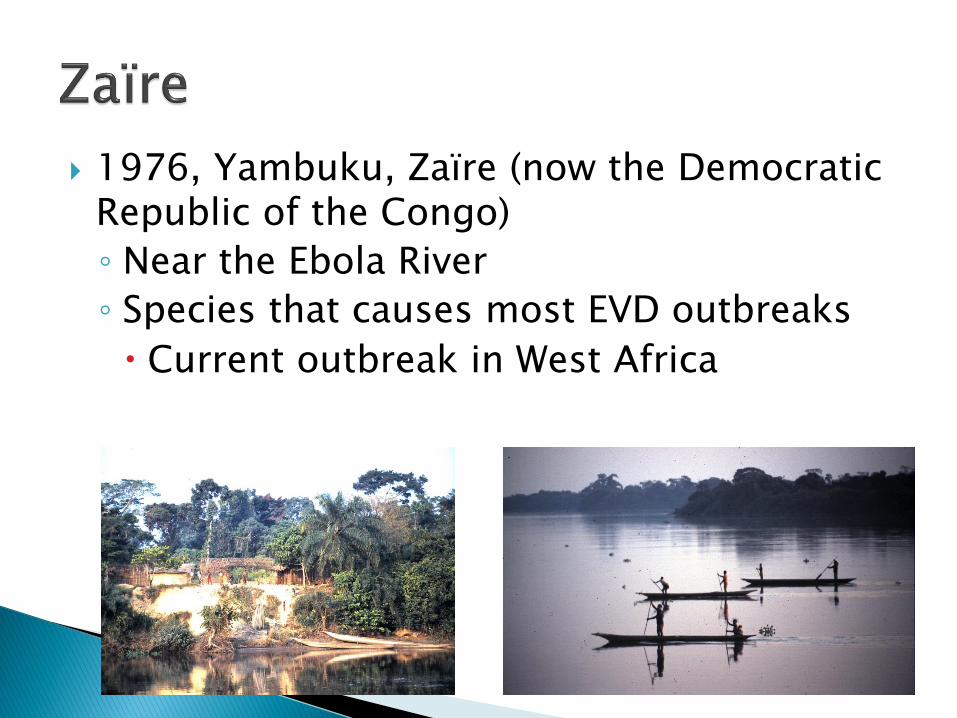
1976, Yambuku, Zaïre (now the Democratic Republic of the Congo)
◦ Near the Ebola River
◦ Species that causes most EVD outbreaks
Current outbreak in West Africa

Fruit bats are most likely the natural reservoir
Infects monkeys and apes ◦ Large die-offs of chimpanzees and gorillas
◦ Reston ebolavirus
Lab workers had serologic evidence of infection
No symptoms
◦ Taï Forest ebolavirus
One human infection
Acquired during autopsy of a chimpanzee
Outbreaks may be associated with hunting or butchering animals or eating infected meat ◦ Bat soup
◦ Bushmeat

Direct contact with blood or body fluids of a symptomatic person ◦ Skin Cuts, abrasion
◦ Mucous membranes ◦ Parenteral Reusing unsterilized needles
Accidental needle sticks
◦ Funeral ceremonies
Respiratory droplets? ◦ Not airborne
Not effectively transmitted by inanimate objects

Incubation period
◦ 2 to 21 days
Mean 6 – 12 days
“Dry” symptoms ◦ Sudden onset
Fever
Muscle pain
Fatigue
May be a transient rash

“Wet” symptoms
◦ Vomiting, diarrhea
◦ Bleeding disorders
Gastrointestinal bleeding
Bleeding from venipuncture sites
Mucous membranes
Neurological symptoms

Easily mistaken for other diseases
Health care personnel at risk for infection Outbreaks frequently associated with
transmission in health care facilities
- Hepatitis - Shigellosis
- Malaria - Typhoid fever
- Meningococcemia - Typhus
- Plague - Yellow fever

Frequently infected ◦ Illness not
recognized as EVD
◦ Lack of appropriate PPE
Fewer health care workers available ◦ Death
◦ Flee out of fear of infection

No specific medications to treat EVD
Hydration and electrolyte replacement
◦ Oral rehydration solution (ORS)
◦ Intravenous fluid
Antimalarial
Antibiotics to treat/prevent translocation of bacteria from the GI tract
Nutritional support Fowler et al., 2014
Sodium
Potassium
Glucose ◦ Sodium/glucose
co-transport
◦ Enhanced water absorption
Atia & Buchman, 2009

Death or recovery
◦ 7 to 14 days after symptom onset
◦ Prolonged convalescence
◦ Survivors presumed to be immune
Species-specific neutralizing antibodies
◦ Virus may be present in semen weeks after recovery
Rehydration and electrolyte replacement improve survival

West African Ebola epidemic traced to a 2-year-old child in Guinea who died from the disease December 6, 2013
◦ First outbreak of EVD in West Africa
March 10 2014: World Health Organization (WHO) notified of an outbreak of an unknown infectious disease characterized by fever, vomiting, and diarrhea in Guinea
Zaïre ebolavirus identified in blood from patients who were hospitalized with the disease
Baize et al., 2014
…modest further intervention efforts at that point could have achieved control.”
WHO Ebola Response Team (2014)
Epidemic spreads to
◦ Liberia in March
◦ Sierra Leone in May
◦ Nigeria in July
August 8, 2014: WHO declared the Ebola epidemic in West Africa a Public Health Emergency of International Concern
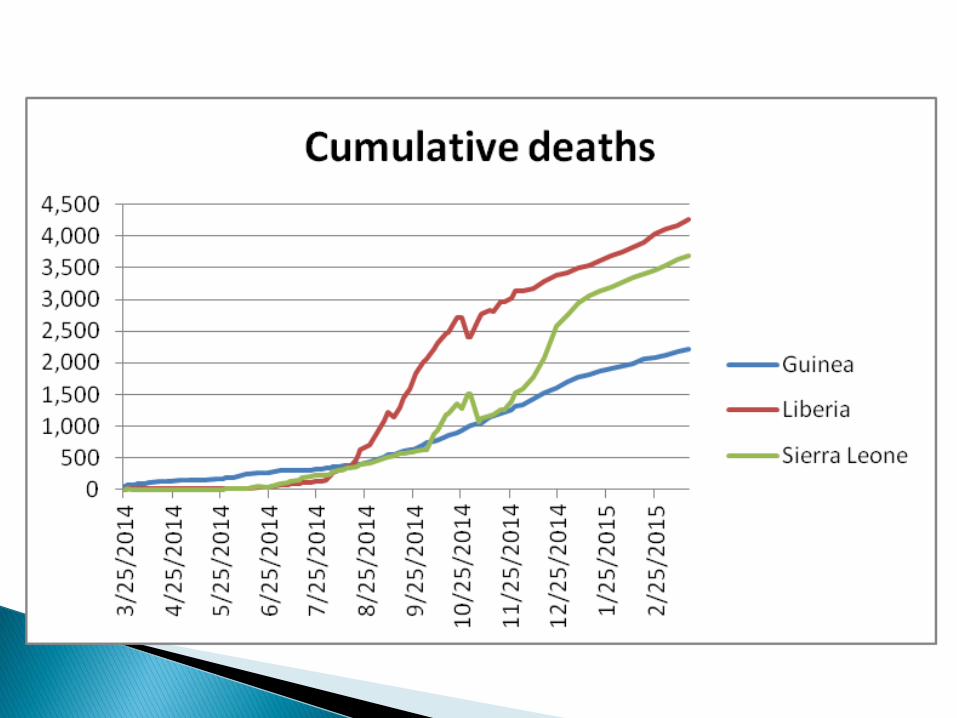
Cases Deaths
Guinea 495 367
Liberia 554 294
Nigeria 13 2
Sierra Leone 717 298
Totals 1,779 961
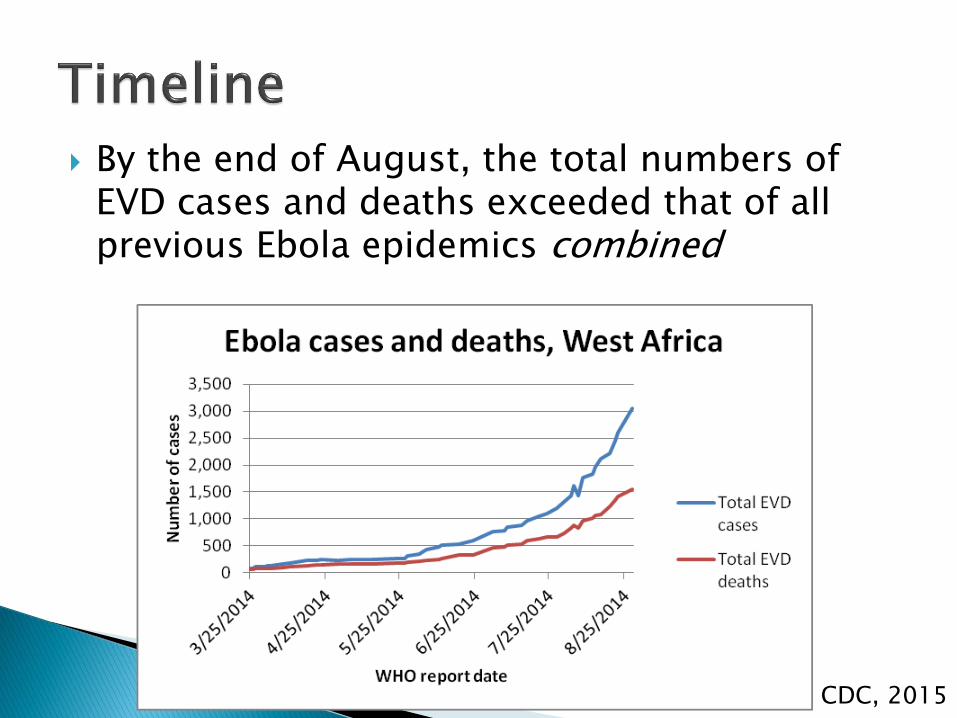
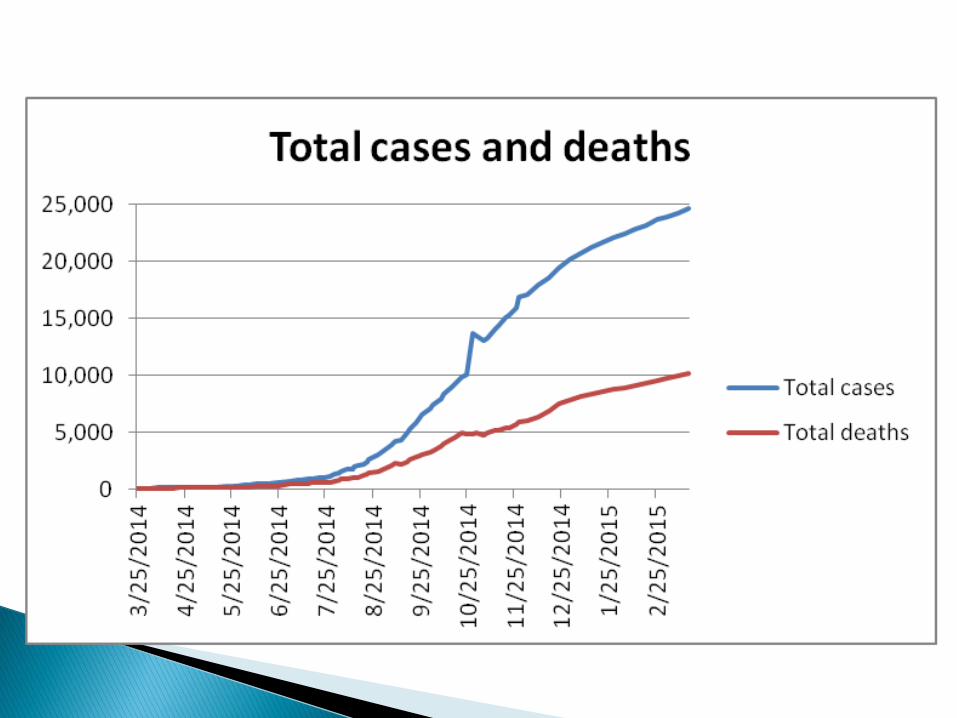
By the end of August, the total numbers of EVD cases and deaths exceeded that of all previous Ebola epidemics combined
CDC, 2015

New cases of Ebola virus disease, October 19–November 8, 2014 - CDC
100 bed capacity
◦ 44 confirmed
◦ 56 suspect

Patients referred by
◦ District health officers
◦ Community Care Centers
◦ Other health care facilities
Triage

Suspect ◦ Fever and contact
with an EVD case or dead/sick animal
OR
◦ Fever and other EVD symptoms
OR
◦ Inexplicable bleeding
OR
◦ Inexplicable death WHO 2014
Laboratory confirmed ◦ PCR+
OR
◦ IgM+

Asymptomatic for 3 days
Negative PCR
◦ Both confirmed and suspect cases

Martha Phillips
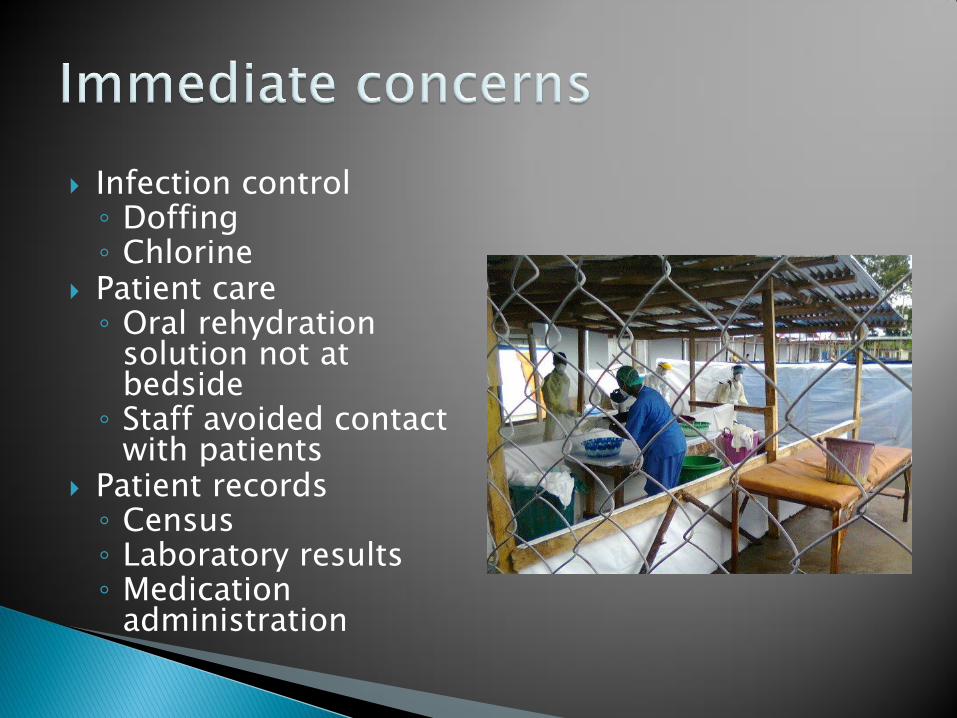
Infection control ◦ Doffing ◦ Chlorine
Patient care ◦ Oral rehydration
solution not at bedside
◦ Staff avoided contact with patients
Patient records ◦ Census ◦ Laboratory results ◦ Medication
administration
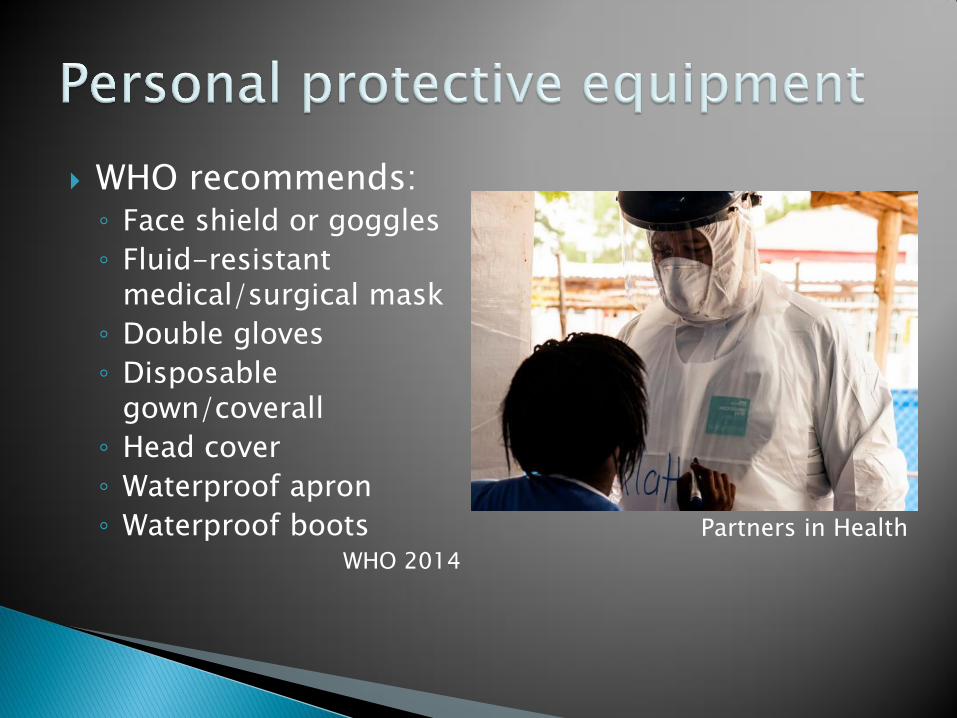
WHO recommends: ◦ Face shield or goggles
◦ Fluid-resistant medical/surgical mask
◦ Double gloves
◦ Disposable gown/coverall
◦ Head cover
◦ Waterproof apron
◦ Waterproof boots WHO 2014
Partners in Health
Tropical Africa
◦ Hot
◦ Humid
According to the CDC,
“Wearing PPE increases the risk for heat-related illnesses.”

Hydration
Electrolyte replacement
◦ Oral rehydration solution
Doffing PPE safely takes time
◦ Go to the toilet before donning PPE!
Rest
Skin care
◦ Cuts and abrasions are portals of entry




Ebolaviruses ◦ Lipid envelope Derived from host cell ◦ Destroyed by Alcohol Chlorine Heat Detergents Soap UV light

CDC ◦ May restrict travel into the U.S. and between states
◦ No authority within states
◦ Recommendations
CDC does not recommend “quarantining” asymptomatic individuals with some or low risk of infection
Washington State follows CDC guidance on travelers returning from Ebola-affected countries ◦ Some of my colleagues who live in other states
haven’t been as fortunate

Travelers entering the U.S. from Ebola-affected counties must be screened at one of five airports
Categorized according to risk
Health departments of counties of residence notified

Risk Exposure Monitoring (asymptomatic)
High risk Needle-stick from a symptomatic patient
Contact with body fluids from a symptomatic patient without appropriate PPE
Contact with a dead body without PPE
Direct active monitoring
Controlled movement
Exclusion from workplace, public places
Some risk Direct contact with a symptomatic person while wearing appropriate PPE
Direct active monitoring
Health officer may impose additional restrictions, if appropriate
Low (but not zero) risk
Having been in a country with widespread Ebola transmission without known exposure
Active monitoring No restrictions on
work, travel, or public places

Local health department: ◦ Active monitoring Self-reporting of temperature and EVD
symptoms Twice daily 21 days
◦ Direct active monitoring Self-reporting of temperature and EVD
symptoms Twice daily
Direct observation of contact by health department personnel 21 days

United States
◦ 10/11/14 to 3/24/15
11,361 travelers screened.
◦ 3/16/15 to 3/22/15
1,989 people in active or direct active monitoring
CDC

Washington State
◦ 131 low risk
◦ 20 some risk
Pierce County
◦ 10 low risk
◦ 2 some risk
No high risk contacts in Washington State
No cases of EVD in Washington State


a person suspected of having EVD is seen in health care facility in Pierce County?
◦ Don’t panic ◦ Call TPCHD
a person the health department is monitoring develops a fever and/or symptoms of EVD? ◦ The health department will arrange transportation to an
appropriate health care facility for evaluation
It’s probably not EVD ◦ Malaria ◦ Gastroenteritis ◦ Influenza


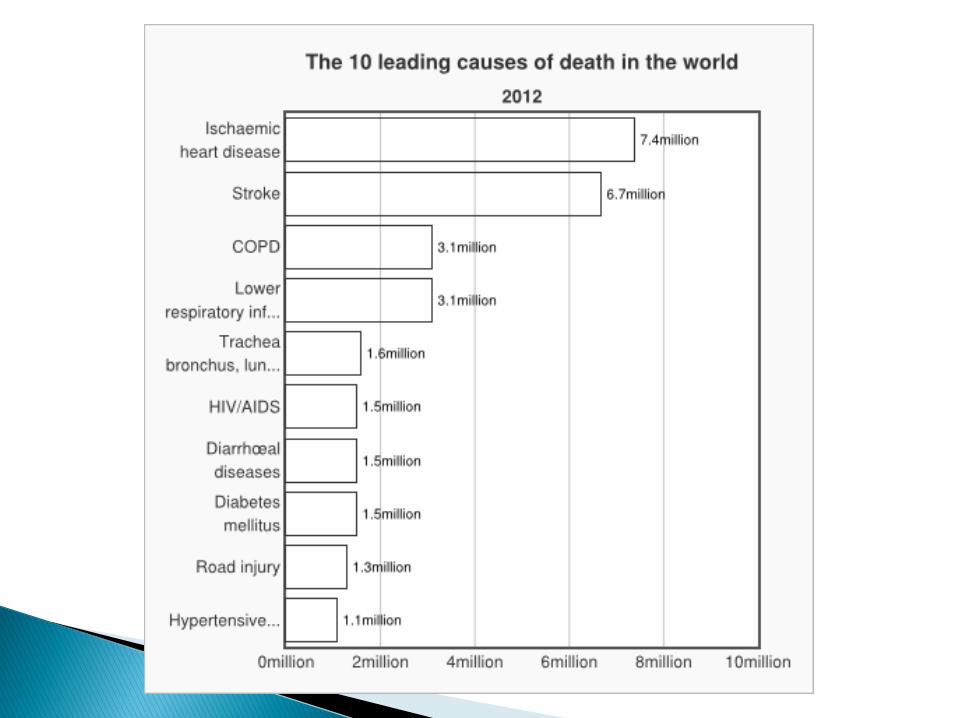
Infectious diseases
◦ Tuberculosis: 1,500,000
◦ Malaria: 584,000
Children under 5 years of age: 453,000
◦ Measles: 145,700
◦ Pertussis (whooping cough): 89,000


Atia, A. N. & Buchman, A. L. (2009). Oral rehydration solutions in non-cholera diarrhea: a review. American Journal of Gastroenterology, 104(6), 2596-2604.
Bausch, D. G., Towner, J. S., Dowell, S. F., Kaducu, F., Lukwiya, M., Sanchez, A., et al. (2007). Assessment of the risk of Ebola virus transmission from bodily fluids and fomites. Journal of Infectious Diseases, 196(Supple. 2), S142-S147.
Baize, S., Pannetier, D., Oestereich, L., Rieger, T., Koivogui, L., Magassouba, N., et al. (Emergence of Zaire Ebola virus disease in Guinea. New England Journal of Medicine, 371(15),1418-1425. doi:10.1056/NEJMoa1404505.
Blumberg, L., Enria, D., & Bausch, D. G. (2014). Viral hemorrhagic fevers. In J. Farrar, P. J. Hotez, T. Junghanss, G. Kang, D. Lalloo, & N. J. White (Eds.) Manson's tropical diseases, 23rd Ed. [Electronic version]. Elsevier.
Centers for Disease Control and Prevention. (October 3, 2014). Ebola virus disease outbreak – Nigeria, July-September, 2014. Morbidity and Mortality Weekly Report, 63(39), 867-872. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6339a5.htm.

Centers for Disease Control and Prevention. (November 20, 2014). Interim guidance for healthcare workers providing care in West African countries affected by the Ebola outbreak: limiting heat burden while wearing personal protective equipment (PPE). http://www.cdc.gov/vhf/ebola/hcp/limiting-heat-burden.html.
Centers for Disease Control and Prevention. (November 21, 2014). Update: Ebola virus disease epidemic – West Africa, November 2014. Morbidity and Mortality Weekly Report, 63(46),1064-1066. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6346a6.htm.
Centers for Disease Control and Prevention. (December 12, 2014). Ebola virus disease in health are workers – Sierra Leone, 2014. Morbidity and Mortality Weekly Report, 36(49), 1168-1171. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6349a6.htm.
Centers for Disease Control and Prevention. (2015). 2014 Ebola outbreak in West Africa – cumulative reported cases in Guinea, Liberia, and Sierra Leone. http://www.cdc.gov/vhf/ebola/csv/graph1-cumulative-reported-cases-all.csv
Centers for Disease Control and Prevention. (2015). Outbreaks chronology: Ebola virus disease. http://www.cdc.gov/vhf/ebola/outbreaks/history/chronology.html.
Centers for Disease Control and Prevention (2015). Experiences of CDC and Emory Healthcare in Managing Persons Under Investigation for Ebola. http://emergency.cdc.gov/coca/calls/2015/callinfo_033115.asp
Fowler, R. A., Fletcher, T., Fischer, W. A., Lomontagne, F., Jacob, S., Brett-Major, D., et al. (2014). Caring for critically ill patients with Ebola virus disease. Perspectives from West Africa. American Journal of Respiratory and Critical Care Medicine, 190(7), 733-737. doi:10.1164/rccm.201408-1514CP.
Geisbert, T. W. (2014). Marburg and Ebola hemorrhagic fevers (Filoviruses). In J. E. Bennett, R. Dolin, & M. J. Blaser (Eds.). Mandell, Douglas, and Bennett's principles and practice of infectious diseases, 8th Ed. [Electronic version]. Elsevier.

Hartman, A. L. (2013). Ebola and Marburg virus infections. In, A. J. Magill, D. R. Hill, T. Solomon, & E. T. Ryan (Eds.) Hunter's tropical medicine, 9th Ed. [Electronic version]. Elsevier.
Schieffelin, J. S., Shaffer, J. G., Goba, A., Gbakie, M., Gire, S. K., Colubri, A., et al. (2014). Clinical illness and outcomes in patients with Ebola in Sierra Leone. New England Journal of Medicine, 371(22), 2092-2100. doi:10.1056/NEJMoa1411680
World Health Organization. (March 30, 2014). Ebola virus disease in Liberia. http://www.who.int/csr/don/2014_03_30_ebola_lbr/en.
World Health Organization. (May 26, 2014). Ebola virus disease, West Africa – update. http://www.who.int/csr/don/2014_05_28_ebola/en.
World Health Organization. (August 8, 2014). Ebola virus disease update – West Africa. http://www.who.int/csr/don/2014_08_08_ebola/en.
World Health Organization. (August 9, 2014). Case definition recommendations for Ebola or Marburg Virus Diseases. http://www.who.int/csr/resources/publications/ebola/ebola-case-definition-contact-en.pdf.

World Health Organization (October 31, 2014). Personal protective equipment (PPE) in the contact of Filovirus disease outbreak response: technical specification for PPE equipment to be used by health workers providing clinical care for patients. http://apps.who.int/iris/bitstream/10665/137411/1/WHO_EVD_Guidance_SpecPPE_14.1_eng.pdf.
World Health Organization. (2014). Ebola outbreak response: maps. Global Alert and Response (GAR). http://www.who.int/csr/disease/ebola/maps/en.
World Health Organization. (2014). Global Health Observatory Data Repository. http://apps.who.int/gho/data/node.main.A1444.
World Health Organization Ebola Response Team. (2014). Ebola virus disease in West Africa – the first 9 months of the epidemic and forward projections. New England Journal of Medicine, 371(16), 1481-1495. doi:10.1056/NEJMoa1411100.