
EATING PROBLEMS AND NUTRITIONAL STATUS AFTER STROKE.790994/FULLTEXT01.pdf · EATING PROBLEMS AND...
50
EATING PROBLEMS AND NUTRITIONAL STATUS AFTER STROKE. AKADEMISK AVHANDLING som med vederbörligt tillstånd av Rektorsämbetet vid Umeå Universitet för avläggande av doktorsexamen i medicinsk vetenskap kommer att offentligen försvaras i aulan, Vårdskolan, Gluntens väg 10 B, fredagen den 10 juni 1988 kl 9.00 av Karin Axelsson Umeå 1988
Transcript of EATING PROBLEMS AND NUTRITIONAL STATUS AFTER STROKE.790994/FULLTEXT01.pdf · EATING PROBLEMS AND...
EATING PROBLEMS AND NUTRITIONAL STATUS
AFTER STROKE.
AKADEMISK AVHANDLINGsom med vederbörligt tillstånd av Rektorsämbetet vid Umeå
Universitet för avläggande av doktorsexamen i medicinsk vetenskap kommer att offentligen försvaras i
aulan, Vårdskolan, Gluntens väg 10 B, fredagen den 10 juni 1988 kl 9.00
av
K arin Axelsson
Umeå 1988

UMEÅ UNIVERSITY MEDICAL DISSERTATIONSNew series No 218 - ISSN 0346-6612 ISBN 91-7174-360-X
EATING PROBLEMS AND NUTRITIONAL STATUS AFTER STROKE.
Karin Axelsson, Departments of Advanced Nursing and Medicine, University of Umeå, S-901 85 Umeå, Sweden.
ABSTRACTEating problem s and nutritional status were studied in a
consecutive series of 104 stroke patients admitted to emergency hospital care. During their stay in hospital eating problems were observed in 46 patients. Certain common types of eating problems were identified: aberrant eating behaviour as regards chewing,lokalization or swallowing, eating small amounts, hoarding of food in the mouth, leakage of food from the mouth and unawareness of eating problems. Poor nutritional status occurred in 16 % of the patients on admission and in 22 % on discharge from the stroke unit.
A subgroup of 32 patients hospitalized for 21 days or longer was studied for three weeks. On at least one occasion during these three weeks a poor nutritional status was observed in 18 patients, of whom 17 had eating problems.
All subjects who had eating problems during their hospital stay, plus those patients without eating problems but with neurological deficits and those living in a nursing home one year after the stroke (n=36) were selected for a longitudinal study 18 months after the onset of stroke. Eating problems were identified in 23 of these patients during their hospital stay while 21 had such problems when they were followed up.
Two patients who could not eat due to severe dysphagia (after a stroke) for three years and 18 months respectively , were successfully trained to eat normally. One patient exhibited impaired oral and hypopharyngeal function and the other impaired hypo- pharyngeal function and a spastic crico-pharyngeal muscle. In both patients training in swallowing was the main remedical measure and one of them also had a myotomy of the spastic muscle.
Key words: eating problems, stroke, training in eating, nutritional status, undernutrition, dysphagia, oral apraxia, oral agnosia, nursing diagnosis, prognosis.
UMEÅ UNIVERSITY MEDICAL DISSERTATIONSNew series No 218 - ISSN 0346-6612
From the Departments of Advanced Nursing and Medicine,
University of Umeå Sweden
EATING PROBLEMS AND NUTRITIONAL STATUS
AFTER STROKE
by
Karin Axelsson
Umeå 1988

Copyright © by Karin Axelsson
ISBN 91-7174-360-X
Printed in Sweden by umpac ab Umeå 1988.

Sören, Mikael, Robert and Maria.

CONTENTS
ABBREVIATIONS 4
ABSTRACT 5
ORIGINAL PAPERS 6
INTRODUCTION AND REVIEW OF THE LITERATURE
Eating 7Stroke and stroke care 7Studies on eating and stroke 8Nutritional status 11Nursing diagnoses 13
AIMS OF THE STUDY 15
SUBJECTSDescriptive study 16Case studies 19
METHODS USED IN DESCRIPTIVE STUDY
Eating 19Nutritional status 20Self-care performance 21Inspections of the mouth 21Analysis of data concerning eating 22Statistics 23
METHODS USED IN CASE STUDIES
Single subject design 23Tests of oral and hypopharyngeal functions 23Other assessments 23Relationship aspect of nursing therapeutics 24Training and treatment 25
2

RESULTS
Eating problems in hospital (I) 26Eating problems 18 months after the stroke (II) 27Nutritional status on admission, on dischargeand 18 months after the stroke (II, III) 30Relations between eating problems andnutritional status (II, III, IV) 30Effects of training the swallowing function (V, VI) 30
DISCUSSION
Patient selection 31Methods used in descriptive study 31Methods used in case studies 32Results 33
GENERAL DISCUSSION 35
CONCLUSIONS 37
ACKNOWLEDGEMENTS 3 8
REFERENCES 40
Paper I 49
Paper II 59
Paper III 77
Paper IV 95
Paper V 113
Paper VI 123
3

ABBREVIATIONS
ADL = Activities of daily living
AMC = Arm muscle circumference
Cl = Confidence Interval (95%)
c r = Computerized tomography
Q1.Q3 = First and third quartile
NANDA = North American Nurses Diagnosis Association
TIA = Transient ischemic attack
TSF = Triceps skinfold thickness
4

EATING PROBLEMS AND NUTRITIONAL STATUS AFTER STROKE.
Karin Axelsson, Departments of Advanced Nursing and Medicine, University of Umeå, S-901 85 Umeå, Sweden.
ABSTRACTEating problems and nutritional status were studied in a
consecutive series of 104 stroke patients admitted to emergency hospital care. During their stay in hospital eating problems were observed in 46 patients. Certain common types of eating problems were identified: aberrant eating behaviour as regards chewing, lokalization or swallowing, eating small amounts, hoarding of food in the mouth, leakage of food from the mouth and unawareness of eating problems. Poor nutritional status occurred in 16 % of the patients on admission and in 22 % on discharge from the stroke unit.
A subgroup of 32 patients hospitalized for 21 days or longer was studied for three weeks. On at least one occasion during these three weeks a poor nutritional status was observed in 18 patients, of whom 17 had eating problems.
All subjects who had eating problems during their hospital stay, plus those patients without eating problems but with neurological deficits and those living in a nursing home one year after the stroke (n=36) were selected' for a longitudinal study 18 months after the onset of stroke. Eating problems were identified in 23 of these patients during their hospital stay while 21 had such problems when they were followed up.
Two patients who could not eat due to severe dysphagia (after a stroke) for three years and 18 months respectively, were successfully trained to eat normally. One patient exhibited impaired oral and hypopharyngeal function and the other impaired hypo- pharyngeal function and a spastic crico-pharyngeal muscle. In both patients training in swallowing was the main remedical measure and one of them also had a myotomy of the spastic muscle.
Key words: eating problems, stroke, training in eating, nutritional status, undernutrition, dysphagia, oral apraxia, oral agnosia, nursing diagnosis, prognosis.
5

ORIGINAL PAPERS
This thesis is based on the following papers, which will be referred
to in the text by their Roman numerals:
I: Axelsson K, Norberg A, Asplund K. Eating after a stroke -towards an integrated view. International Journal of Nursing Studies 1984;21:93-9.
II: Axelsson K. Longitudinal study of eating problems instroke patients. Submitted for publication.
III. Axelsson K, Asplund K, Norberg A, Alafuzoff I. Nutritionalstatus in patients with acute stroke. Accepted forpublication in Acta Medica Scandinavica.
IV: Axelsson K, Asplund K, Norberg A, Eriksson S. Eatingproblems and nutritional status in patients with severe stroke. Submitted for publication.
V: Axelsson K, Norberg A, Asplund K. Relearning to eat lateafter a stroke by systematic nursing intervention: a case report. Journal of Advanced Nursing 1986;11:553-9.
VI: Axelsson K, Norberg A, Asplund K, Söderberg O, WenngrenBI. Training of eating after a stroke in a patient with dysphagia of pharyngeal type. Scandinavian Journal of Caring Sciences, in press.
The papers are reprinted with kind permission of the respective journals.

INTRODUCTION AND REVIEW OF THE LITERATURE
EatingEating is a complex form of behaviour. Normal eating presupposes that different factors interact successfully. The cerebral regulation of hunger and satiation, food palatability, food habits and the ability to perform those motor actions necessary for eating are examples of such factors (1, 2).
Eating problems are to be expected in stroke patients for several reasons. Firstly they are often elderly and there are some problems related to age. The elderly have e.g. been reported to have an increased threshold for both taste and smell (3). Secondly the stroke can lead to impairments that may affect eating for example appetite, perception of food and motor performance.
This thesis will focus on disturbances in eating behaviour supposed to be primarily related to the stroke (cf. 4), and mainly, within this perspective, on the transportation of food from the plate to the mouth, handling it in the mouth and swallowing it.
Stroke and stroke careThe definition of stroke as formulated by the World Health Organization is: "rapidly developed clinical signs of focal (or global) disturbance of cerebral function, lasting more than 24 hours or leading to death, with no apparent causes other than those of vascular origin" (5).
Impairments after stroke include mobility, sensing, cerebral integration and intrapsychological deficits (6). A disturbed function in one arm, in chewing, in facial and swallowing muscles, an altered sensing of food in the mouth, apraxia in one arm and in the mouth, an altered ability to communicate and mental depression can all cause eating problems.
In a study in Söderhamn the incidence of stroke was found to be 2.9/1000 population and year (7). In the Department of Medicine, Umeå University Hospital the proportion of beds used for stroke patients increased from seven to 15 per cent from 1971 to 1981 (8).
7
In January 1978 a six-bed non-intensive stroke unit was established in one of the five wards at the Department of Medicine. Patients are admitted directly from the emergency room. Theadmission criteria are presence of focal neurological dysfunction (without trauma to the head) with a duration not exceeding oneweek or a history of transient ischemic attack (TIA) during the lastweek. Patients with subarachnoid hemorrhage are admitted or transferred to the Department of Neurosurgery (9). When a bed in the unit is available the first patient to fulfil the admission criteria will come to the stroke unit.
During a 16 month period from 1979 to 1981 the unit received 38 per cent of the stroke patients who attended hospital in theUmeå U niversity Hospital catchment area. There were no differences in characteristics and symptoms on admission between the patients in the stroke unit and those treated in the generalmedical wards (10).
The patients in the Umeå stroke unit seem to be comparable to patients reported in other Swedish investigations. In 409 patients with a well-defined stroke diagnosis who were investigated andtreated in the Umeå stroke unit from 1978 to 1982, the male/female ratio was 1.25/1 and the mean age was 72 years. Patients with embolic infarction were the oldest while those withTIA were the youngest (11).
In another study of 325 patients in Söderhamn with a first stroke or TIA the proportions of intracerebral hemorrhage and TIA were similar while a quite large group was not classified (7). The distribution among the diagnostic groups in a study of 264 stroke patients in Stockholm showed a similar distribution to that in theUmeå study (Table 1). The mean age in the group was 73 years ( 12).
Studies on eating and strokeSome stroke patients have described their experience of the disease and the experience of eating as a great discomfort (13, 14). There are a number of reports about eating problems in stroke patients that could be characterized as summaries of the practical knowledge of nurses (e.g. 15-19). In some reports dysphagia is the
8

Table 1. The distribution among different diagnostic groups in three reported studies from various parts of Sweden (11, 7, 12).
Cerebrovasculardiagnoses
Umeå(n=409)
%
Söderham n3(n=325)
%
Stockholm(n=264)
%
Intracerebral hemorrhage 11 15 8
Non-embolic brain infarction 5141b
59
Embolic brain infarction 25 25
TIA 13 13 8
Subarachnoid hemorrhage 0 5 0
Unclassified 0 26 0
a First stroke or TIAb In the study presented as : cerebral infarction.
only eating problem described (e.g. 20, 21). No systematic over-all investigation of eating problems in stroke patients has been found in the literature.
Dysphagia is the only eating problem which is fairly well documented. Some studies concerned disabilities (22). In a community sample of 976 stroke patients an investigation of swallowing during the first week after the stroke was made in 545 patients. Seventeen per cent could not be tested due to decreased consciousness, 12 per cent choked, 5 per cent had abnormal swallowing patterns and 19 per cent were very slow when swallowing was tested by the drinking of water (23).
Other studies connected disabilities to localization of brain damage. In a study of 39 patients with well-defined Wallenberg's
9
syndrome 29 had dysphagia during the acute phase (24). Another study of 35 patients with W allenberg’s syndrome showed dysphagia in 74 per cent of the patients in the acute phase (25). A study of 91 consecutive stroke patients showed a 45 per cent incidence of dysphagia on admission to a stroke unit (26). The dysphagic patients were older and had more severe stroke symptoms than those without dysphagia. The dysphagic patientsalso showed a higher frequency of abnormality in cranial nerve tests. Of the patients who had dysphagia and were alive six weeks after the stroke 71 per cent had had their dysphagia for eight days or less (26).
Further studies concerned both disabilities and impairments in relation to localization of the brain damage. A group of 38 stroke patients with dysphagia consecutively referred for examination by videofluorography was studied (27). Seventeen had brain damage in the left hemisphere, 11 in the right hemisphere and 10 in the brainstem. The most common swallowing problem was delayedreflex (82 per cent) followed by reduced pharyngeal peristalsis (58 per cent), reduced lingual control (50 per cent), reduced laryngeal adduction and cricopharyngeal dysfunction (five per cent each). More than one type of swallowing problems occurred in 76 per cent of the patients investigated (27).
Vague descriptions of patient selection criteria and methods of investigation make it difficult to draw any precise conclusion about the true prevalence and types of dysphagia.
Assessment instruments such as the Katz’ Index of Independence in Activities of Daily Living (28) and the Activity Index developed by Hamrin and Wohlin (29) include eating. Using these indexes andother ADL scales (30) it is possible to register the patients' ability toeat independently.
General assessments of stroke patients' requisites for eating have been presented (31) as well as more specific assessments of oral function (32, 33). Investigations of oral apraxia have been performed in patients with aphasia and an oral apraxia test has been developed (34). Tests of oral perception in healthy subjects showed that they could identify rather complicated forms in the mouth (35).
10

More general guidelines for measures to help the patient with eating difficulties (36-38) as well as techniques for the support, stimulation and training of oral muscles and tongue control (39-41) have also been presented. A programme based on the training of oral muscles and instructions to the patient about the basic process of swallowing followed by training in swallowing water and then smooth food has been successfully used in 15 patients with dysphagia of various origins (42). Training in swallowing based on attempts to stimulate salivation with a lemon/glycerin swab, depression of the tongue, elevation of the larynx by manual pressure simultaneously with instructions in how to swallow has been shown be of benefit in patients with dysphagia (43, 44).
A method for relearning the initiating of swallowing by training the patients suck and then to elevate the larynx and finally to suck on ice chips and swallow, has been applied in seven cases with dysphagia after a stroke (45). Application of an intra-oral palatal training appliance is a method used to stimulate the involuntary swallowing mechanism. This wire loop has been successfully used in 164 stroke patients with dysphagia (46). Myotomy has been used in dysphagic patients with spasm in the cricopharyngeal muscle (47).
The various techniques for training patients with eating problems that have been presented seem to work. Unfortunately, the patients' functional deficits were not always clearly described In patients with dysphagia the hypopharyngeal function was for instance investigated but not the oral or the oesophageal function.
Nutritional statusOne consequence of eating problems could be a reduced intake of food resulting in undernutrition. Undernutrition in hospitalized patients is caused, in addition to decreased intake, by increased expenditure of energy and nutrients (48). Some patients are already undernourished on admission to hospital while others reach this state during their stay.
In a study of 75 patients admitted as emergencies to a medical ward, 22 per cent were undernourished (49). A study of 179 men visiting an outpatient clinic in the USA, showed undernutrition in
11

29 per cent of patients younger than 65 years and in 38 per cent of patients 65 years or more (50). When nutritional status and dietary intake were studied in three Nordic hospitals (Gothenburg, Helsinki and Oslo) 29 per cent of the 56 patients examined were undernourished on admission and during their hospital stay their nutrient intake was reduced by between 25 to 35 per cent of the normal intake at home (51).
In a study of 112 surgical patients, undernutrition was found in 29 per cent (52). Nutritional status in 10 oncological patients treated with radiotherapy showed that four patients had two or more nutritional parameters (four parameters were assessed) below the reference limit before and four patients after the therapy (53).
Assessment of nutritional status in 91 patients in psychogeriatric wards showed undernutrition in 30 per cent (54). In a study of 16 patients in a psychogeriatric ward 50 per cent were undernourished. The mean dietary intake was significantly higher than their calculated needs and the median intake was somewhat higher in the undernourished group than in the well-nourished group (55).
Undernutrition in itself may further reduce the intake and expenditure of energy and nutrients (56). Patients with undernutrition are prone to lesions in the oral mucosa (57), bed sores (58) and infections (59) due to an impaired cell-mediated immune defense (60). Decreased physical activity caused by undernutrition (61) may be detrimental to the early physical rehabilitation of stroke patients. Nutritional deficiencies have been associated with a reduced cognitive function in elderly people (62). Nutritional status has been shown to be an important determinant of the clinical course in different clinical contexts, such as surgery (63) and oncology (64).
Thus, undernutrition occurs in hospitalized patients as well as in patients visiting outpatient clinics but no study of nutritional status in stroke patients was found in the literature. Several interacting factors such as the distribution of meals throughout the day, the composition of food and the interest of the staff influence the nutritional status (65, 66). The role of eating problems as one of the
12

interacting factors in the development of undernutrition was the object of this study.
Nursing diagnosesAny systematic development of methods for treating eating problems must be based on a thorough diagnosis of those problems. Intensive work aimed at developing methods for diagnosing nursing problems is being carried out mainly in the USA (67, 68). Using a deductive approach the North American Nursing Diagnosis Association (NANDA) has presented a list of nursing diagnoses (69). In that list "altered nutrition: less than body requirement" is a diagnostic label and eating problems are specified under it. "Altered nutrition (potential for less than body needs) related to: difficulty chewing and swallowing" (69, p. 109) is an example of a nursing diagnosis concerning eating problems. "Self-care deficit: feeding" is another diagnostic label in the NANDA-list (69, p. 499). "Impaired swallowing" is also included under the heading (69, p. 499). A complete nursing diagnosis concerning eating could be "alteration in nutrition: less than body requirements related to impairedswallowing and chewing defect, related to hemiplegia and related to homonymous hemianopsia" (70).
In another list the nursing diagnoses concerning eating are: "nutrition, alterations in: less than body requirement related to" either "chewing" or "swallowing difficulties" or "anorexia" (71, p. 287) or "self-care deficit related to inability to feed self" (71, p. 374). In a third list the main category concerning eating problems is "self-care deficits in food/fluid intake" (72, p. 164). Examples of labeled nursing diagnoses under that category are: "incapacity or partial incapacity to feed/hydrate self" (72, p. 165) and "partial incapacity to chew/swallow food or fluids" (72, p. 167).
The diagnostic categories presented above all seem to be too vague and general to serve as starting points for the development of specific nursing therapeutics for eating problems. The focus is mainly on nutrition and problems in eating performance are subordinated to it. There are, however, eating problems that are not necessarily related to problems of nutrition.
13

An inductive approach to diagnosing patients' problems has also been presented (73). The nursing diagnosis, according to this method, is seen as a conclusion often based on more than one patient problem. The formulation of the diagnosis may include the interaction between the problems and their causes (74). No list of nursing diagnoses developed by this method has been presented.
The author and co-workers (68) developed a model for a more specific nursing diagnosis of eating problems primarily related to the disease (68). The model is connected to both the WHO classification of impairments, disabilities and handicaps (75) and to the International Classification of Disease (76).
According to this model nursing diagnoses should be formulated in two steps. A general nursing diagnosis is based on observations and interviews and is placed on the level of disabilities. A specific nursing diagnosis is based on specific tests and investigations and is connected with impairments (symptom diagnoses) (Figure 1).
WHO*
ICD°
E .G .
Figure 1. The connection between nursing diagnosis, medical diagnosis and the classifications of impairments, disabilities, handicaps, and diseases. E.G. denotes an example.* Levels in the classification of impairments, disabilities and handicaps (74). The level of handicaps is not described in the model.° Levels according to the International Classification of Diseases (76).This figure is adopted from Vård i Norden 1986;6:309 (ref 68).
DISABILITIES IMPAIRMENTS DISEASE
(PROBLEM/N E E D )
OBSERVEDBEHAVIOUR
SYMPTOM TYPE CAUSE
Problem s in e a tin g D ysphagia
R ig h t-sid e d hem iparesis
O ral a p ra x ia
Brainin fa rc tio n
A trialfibrillation-«'ca rd iacembolus
NURSING F
PR O B L E M
o c u s
G E N E R A LN U R S I N GD IA G N O S I S
WÊÊSSËIËÉv
\Ö lA O N O « IS
S P E C F I C NN U R S I N GD IA G N O S I S
IBBICAU F0 CUFATO-a n a t o m ic a ld ia o n o « «
as r m o o iO A Ld ia g n o s is
14

When this model for the diagnosing of eating problems is compared with the models mentioned above it seems reasonable to suggest that their formulations of diagnoses should be regarded as general diagnoses, and that no specific diagnoses have been presented.
Malnutrition could be regarded as a consequence of eating problems (77) but it could also be seen as part of a cause. Thereforeassessments of nutritional status are an essential element in thecare of the patient with eating problems. The logical connection between eating problems and nutritional problems has to be elaborated.
AIMS OF THE STUDY
The aims of the present study were:
• to identify and describe eating problems and nutritional status instroke patients in the acute phase of the disease and at a long-termfollow-up.
• to explore the interrelations between eating problems and nutritional status in stroke patients.
• to summarize how patients with cerebrovascular disease describe their eating problems some time after the stroke.
• to implement and develop further methods for diagnosing and training severe dysphagia after stroke.
• to suggest general nursing diagnoses.
15

SUBJECTS
Descriptive studyFrom March 1982 to June 1983 all patients admitted to the stroke unit were asked to participate in a study about eating problems and nutritional status (phase 1). One patient did not want to participate. The study included 104 patients (65 males, 39 females). The patients stayed in hospital for 23 days (mean, range 0-117). Paper I includes all patients and Paper III those with a nutritional assessment on admission (n=100, 64 males, 36 females) and on discharge (n=78, 49 males, 29 females). Patients with a hospital stay of 21 days or more (n=32, 22 males, 10 females) were selected for a longitudinal study of eating problems and nutritional status during hospitalization (IV).
Patients identified as having eating problems during their hospital stay were selected for a follow-up 3 months after the stroke (phase 2). Out of the 46 patients who had eating problems in hospital 11 were dead at the time of the study and one declined to participate. Hence 34 persons (23 males, 11 females) were visited in their home or at the institution where they were living. The results have been presented elsewhere (78).
All subjects with eating problems during their hospital stay were selected for a follow up 18 months after the stroke. The same applied to subjects with neurological deficits and those living in a nursing home one year after the stroke, regardless of whether or not eating problems had been present during hospitalization (phase 3). Six patients who had suffered a recurrent stroke before the visit were excluded. The group fulfilling the selection criteria consisted of 36 patients (25 males, 11 females). Their mean age (on admission to hospital) was 72 years. The individuals were visited in their homes or in the place where they lived. Paper II presents the results from this group.
Figure 2 is a description of the distribution of patients among the different substudies and Table 2 describes the patients in Papers I-IV.
16

Paper III Paper I
Patients v i th a v a rd stay 1 21 days n= 32 *
Patients visited after 18 m onths n= 36 *
Patients v i t h i 2 n u tritiona l assessments n= 78
Patients v i th one nu tritional assessment n= 22
Patients v i th no n u tritiona l assessment n= 4
Figure 2. Distribution of patients between the different substudies. * There was an overlap of 15 patients between the two groups.
Times of data collection periods were:phase 1: March 1, 1982 - June 10, 1983 phase 2: June 1982 - September 1983 phase 3: September 1983 - December 1984
17

Five patients
with bilateral
lesions.On
one or
more levels:
room,
time and
his/her own
person.
ö > 2« T3 =f s r . g . .
22 . C/a : h
2
r *2> CTQ
J5Ô '
o3cr
8 S’S'--s.
*3 P hd Û5 ^. 3 cd £5CD S2. CD52. 3a
Go C«
t r oohH *rl O O*H 73 t» 3CD ^3 3Ora 3 .w ? E i3 * 33 H GO P
3 S o 3 - ^ o
2 2! o oO S.H 1/1 à 2 2 «
5 3o 2 3 -gCL ,, CD Çu Ä CDo tî» X- o
00
Cll-i3
00
23CDCL
< STCD CD■S-ÄCD .
f 8 I sP X* co CL
ST pCDpp p :*-<CDP
g > jo o. 5 o— - - QO o- S.O P OS 5 . 5 g 2 3 3 “.p. "3 n>Cl va
PCDPP
0
cr
nH1COOP3
H W 2> | §
O «o ' 3 cr a- oi-t rrÖ.S'
o
n sV 2 °2 3 § ** cr pP H O O P CD < 003 p °CD CO cr o ✓-vS- E2 50►i h.»
I—*•53 3O &
£5oO 3 p
o <g1-1 *3,<-* o ' Oo* 3 cr c/a3 P CD
ero y*
tO tO tO LO -P* LOI-* Lft oo oo u O 'O
^ M to to ^ Oi O os -L
M H U l4̂. —3 —) vo
oo ^o to c/t o oo vo 4l oto
H- Ux oo to
to to tO LO LO LO>—* 4L «o Os U> 00 *0
-P“ to toLO 4L VO ^ 4L
**+ I—* C/» <0 O n -O
to to tO tO LO LO^ LO ON to On to o
LO tO tO►— I— oo *-* o
4LVO 00 L/i
-Oto
VO LO ^ Oto
On to to—4LO
3 hüII £o "g H
LOON
hdphdCD
3 > Il CL
5 3O C/3vaS’”S3 S
4̂00
LOto
T?PhdCD
18
Table 2.
Description
of the
patients in
Papers I
to IV
.

Gase studies ,Papers V and VI are single subject studies. The patients presented were the first two with severe dysphagia who asked for help at the clinic. One patient was 78 years : old when training started. Three years previously he had had a stroke, presumably in the vertebrobasilar vascular territory. After the stroke he was fed by nasogastric tube. The other patient was 65 years old. He had had a stroke of the Wallenberg type one and a half year previously. He was at first fed by nasogastric tube (Clinifeed®) but six months after the stroke he got a Witzel fistula.
METHODS USED IN DESCRIPTIVE STUDIES
EatingOn admission a semistructured interview was performed. It concerned the patient's eating problems at home, gastrointestinal symptoms (including history of peptic ulcer) and feelings ofsickness, vomiting and loss of appetite during the week beforeadmission.
Patients with persisting stroke symptoms were studied by direct structured and unstructured observations during regular meals. A total of 495 observations were made on 82 patients. The observation form was designed for this study. It included 70 variables covering different aspects of eating, e.g. body position during the meal, cutlery used, handling of food in the mouth and swallowing. The observations were repeated during the hospital stay, as a rule more than once a week. There were two observers: a trained enrolled nurse and a research nurse (the author). No noteswere taken during the observation itself, the structuredobservation form was filled in afterwards.
Before the study the two observers practiced observations together and discussed every variable on the observation form in detail until consensus was reached concerning interpretations and registrations. During the data collection period criteria for the variables on the observation form were discussed repeatedly so as to keep the same criteria as in the beginning. Observations of 32
19
meals were made simultaneously by the two observers during the latter part of the study. The inter-observer exact agreement was 88 per cent and no systematic bias was noted.
The research nurse wrote field notes after each contact with a patient and his/her relatives. The field notes focused on eating problems. After the observation of eating the notes mainly focused on factors not included on the observation form. Discussions with the personnel about the patients’ eating problems and measures to help the patients were summarized in the field notes. It was not possible to register all measures systematically. Therefore they are not reported.
At the visit 18 months after the stroke one meal per patient was observed using the same methods as in hospital. Twenty persons were given a standardized meal consisting of potatoes, brawn, pickled beetroot, crispbread and some fluids. Ten ate parts of this and six ate regular food served in the nursing homes. A focused tape-recorded interview concerning eating problems was conducted for 32 of the patients.
Ten patients with eating problems were video-recorded during eating in hospital, six patients once, one twice, two on three and one on six occasions. At the follow-up 18 months after the stroke four of these subjects were video-recorded.
Nutritional statusThe nutritional status was assessed by percentage of reference weight, triceps skinfold thickness (TSF), upper arm muscle circumference (AMC), plasma albumin, serum transferrin and plasma prealbumin. In hospital the assessments were performed on admission and then weekly during the hospital stay. In four patients, who all died within two days, the nutritional status was not assessed. Twenty-two patients were discharged within one week. In these patients only one assessment was performed. Nutritional status also was assessed in patients visited after 18 months.
The body weights were compared with age adjusted reference weights (79) and relative body weight was calculated (III).
20

In hospital the TSF and AMC assessments were performed by two persons. TSF was measured by a Harpenden caliper (80, 81) on both arms. The mid-upper arm circumference was measured on both arms. The mean value of three measurements of TSF and midupper arm circumference was used and AMC was calculated (81, III). Reference data for the anthropometic variables were obtained from age-adjusted reference data on healthy populations in Sweden and the 10th percentile was chosen for the lower limit (82).
Intra-rater exact agreement was 98 per cent and exact agreement between raters was 87 per cent for the TSF measurements. The corresponding figures for AMC were 92 and 88 per cent.
The TSF and AMC measurements from the right arm were used in the analysis of the data from admission. In the analysis of data on discharge and after 18 months the measurements taken on the left arm were chosen when the right arm was paralyzed during the hospital stay (III).
Plasma albumin and serum transferrin were determined by Technicon Auto Analyzer and the prealbumin by immuno- electrophoresis (83). Reference data were obtained from a representative sample of elderly people in the Umeå area (84). Poor nutritional status was defined when two or more of the six nutritional variables fell below the lower reference limit.
Self-care performanceSelf-care performance was assessed by data about the patients' behaviour the first week in hospital and notes in their medical records. After 18 months an interview with the subject, relatives or personnel about self-care performance in the preceding week served as the basis for classification. The Katz' Index of Independence in Activities of Daily Living (28) was used.
Inspections of the mouthDuring the first phase of the study a dentist was associated with the research team for consultations. During hospitalization the patients with persistent symptoms of stroke were subject to regular inspections of the mouth. Lesions of the oral mucosa were registered as was the presence of their own teeth or presence and
21
use of dentures. After 18 months a new inspection of the mouth was made.
Analyses of data concerning eatingData subject to analysis were the structured observation form, field notes, video-records and notations from the inspections of the mouth. When an eating problem was identified in the observations of eating and in discussions with the patient during the stay in hospital, the patient was classified as having eating problems, if the problem lasted for more than one day and measures to treat it were tried. As different types of eating problems and their cueswere identified, each problem was labeled and treated as a concept. Every patient was classified as having or not having eatingproblems during their stay in the ward.
After the first phase of data collection ended a new analysis was performed. It resulted in identification of the eating problems for each patient. When there were video-recordings comparisons with observations were made. A last analysis was performed after the visit to the patients 18 months after their stroke.
The term "assistance with food" denoted the fact that the patientgot help in preparing food on the plate. The term "assisted feeding" meant that the patient got help in putting food in to the mouth. Recordings about assistance with food and assisted feeding were only performed during the observations.
After 18 months the criteria for each eating problem, in addition to those described above, were the patient's descriptions of eating problems expressed in the focused interview. The term "eating small amounts" was used when the subject reported in the interview that they ate much less than before the stroke.
A change in terminology was made during the last analysis. The term "sores in the mouth" was seen as an eating problem in the earlier analyses while in the last one it was regarded as a cause of eating problems. "Inability to perceive part of the tray" was changed to "aberrant eating behaviour as regards localization". Labels for other eating problems were adjusted to describe the forms of behaviour observed.
22

S ta tisticsPaired Student’s t-test was used for comparison of parametric data and the chi-square test and the Fisher test for exact probability were used when testing differences between proportions. Confidence intervals (Cl) were used for some frequencies (95 per cent). The effect of eating disturbances and other variables on nutritional status was estimated in a general linear hypothesis programme. The statistical calculations were performed with SPSS package (85) and SYSTAT (86).
METHODS USED IN CASE STUDIES
Single subject designIn the two case studies (V, VI) a single subject design was used (87, 88). The baselines were, determined by the patients’ history, examinations, tests and test meals. Video-recordings were made once a day.
Tests of oral and hypopharyngeal functionsOral praxiä was tested by a modification of the test developed by DeRenzi and co-workers (34). Small glass fibre objects of different shapes (cube, pyramid, cylinder and sphere) were used to test oral perception. The objects were held by a dental ribbon and placed in the patient’s mouth. The patient was asked to identify each object. For help the patient was presented with a sheet of paper which showed both the tested objects and three distractors as drawnfigures and names. This test was developed from ideas by Landt (35). The ability to recognize smell and taste was tested by routine tests. Cineradiography and manometry were used to examine thehypopharyngeal and the oesophageal structures and functions.
Other assessmentsThe ability to swallow was tested by requests to swallow saliva, teaspoonfulls of water, teaspoonfulls of youghurt and a piece of crisp bread. The ability was evaluated by observations of the swallowing movements and by observations of whether the mouthwas emptied. The patient’s own reports about whether his mouth
23

was emptied were also registered. The amount the patient spat out was measured. Eating, self-care performance, nutritional status, and inspections of the mouth were assessed by the same methods as in the descriptive study.
Test meals, training sessions and regular meals were videorecorded and/or field notes were taken. Interviews about the patients' experiences of not being able to eat, their views on eating and swallowing as well as their experiences of training were tape- recorded.
Relationship aspect of nursing therapeuticsNursing therapeutics can be seen as a communication. This communication consists of a relationship aspect and a content aspect (89). The programmes for training were seen as a content aspect. The relationship between the patient and his trainer was interpreted according to the Erikson theory of 'eight stages of man’ (90). Erikson describes eight crises that follow man throughout life: trust - mistrust (hope); autonomy - shame/doubt (will); initiative - guilt (purpose); industry - inferiority (competence); identity - identity confusion (fidelity); intimacy - isolation (love); generativity - stagnation (care); integrity - despair (wisdom). At each stage of development there is an actual version of all crises. The development of a therapeutic relationship between the patient and his trainer started with dialogues during which the latter tried to understand within which of the eight crises the patient’s primary concerns were. The trainer then approached him according to what she thought the actual crisis required. As the therapeutic relationship developed the patient trusted the trainer, followed the instructions and talked about his concerns. During the final stage of training the trainer gradually took a more passive role and encouraged the patient to become more active and autonomous.
24

Training and treatmentA training programme developed by Heimlich (45, 91) was initially used in the first patient (V). It prescribes training of sucking before training of swallowing as the ability to suck is a prerequisite for swallowing (91). Training in a specific oral movement was given based on the results of the oral apraxia test. Taste and oral tactile gnosia were also trained. Dentures were adjusted in one case (VI).
When the patient was able to initiate and perform swallowing movements he practiced swallowing the kind of food that he could best swallow as indicated by the swallowing test. Furthermore, the patient was trained to swallow instead of clearing his throat when he sensed fluids in it. During the training sessions instructions were sometimes given as commands. More often the patient was given instructions about how to train and then he trained by himself without being disturbed. The training sessions lasted for 20 to 80 minutes (V, VI).
In one of the patients a myotomy of the cricopharyngeal muscle (47) was performed (VI).
When the patient was able to eat, he first got food which was easy to chew. When his ability improved he was given normal food. If the patient needed extra concentration to be able to eat he received instructions about strategies for communication during meals.
Both of the patients trained were cognitively alert and from the beginning highly motivated to train. Each step of the training was carefully explained to the patients who were also given information about the results of tests and investigations.
25

RESULTS
Eating problem s in hospital (I)Different eating problems were observed in 46 of the 104 patients in hospital. In addition six terminally ill patients were not able to eat at all during their hospital stay. The occurrence of eating problems and the localization of the cerebral lesion for the 46 patients are presented in Table 3.
Patients with eating problems stayed longer in the stroke unit than patients without (mean=36 vs 14 days). Only one patient without eating problems was discharged to a long-term clinic while 33 per cent of the patients with eating problems were. None of the patients without eating problems died in the stroke unit while five (11 per cent) of the patients with problems did.
Table 3. The localization of the vascular lesion documented by CT- scan or autopsy in 46 stroke patients with eating problems during hospital stay.
Eating problem Number Vascular territory affected*of patients Right Left V ertebro
carotid carotid basilar
Aberrant eating behaviouras regards
chewing 31 11 12 . 5localization 9 4 2 1swallowing 31 9 13 4
Eating small amounts 23 5 9 4Hoarding of food in the mouth 33 15 12 2Leakage of food from the mouth 31 13 12 2
Unawareness of eating problems 30 12 11 2
Any eating problem 46 15 17 6
* In 10 patients no lesion was found in the CT-scan. In one patientno CT-scan was performed. Three patients had lesions on bothsides.
26
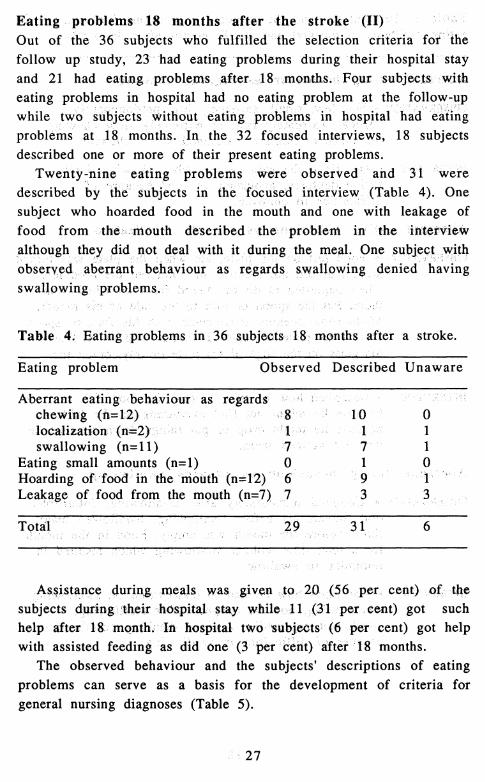
Eating problem s 18 months after the stroke (II)Out of the 36 subjects who fulfilled the selection criteria for the follow up study, 23 had eating problems during their hospital stay and 21 had eating problems after 18 months. Four subjects witheating problems in hospital had no eating problem at the follow-upwhile two subjects without eating problems in hospital had eating problems at 18 months. In the 32 focused interviews, 18 subjects described one or more of their present eating problems.
Twenty-nine eating problems were observed and 31 weredescribed by the subjects in the focused interview (Table 4). One subject who hoarded food in the mouth and one with leakage of food from the mouth described the problem in the interviewalthough they did not deal with it during the meal. One subject with observed aberrant behaviour as regards swallowing denied having swallowing problems.
Table 4. Eating problems in 36 subjects 18 months after a stroke.
Eating problem Observed Described Unaware
Aberrant eating behaviour as regardschewing (n=12) 8 10 0localization (n=2) 1 1 1swallowing (n=11) 7 7 1
Eating small amounts (n=l) 0 1 0Hoarding of food in the mouth (n=12) 6 9 T " 'Leakage of food from the mouth (n=7) 7 3 , . .3 .,.
Total 29 31 6
Assistance during meals was given to 20 (56 per cent) of the subjects during their hospital stay while 11 (31 per cent) got such help after 18 month. In hospital two subjects (6 per cent) got help with assisted feeding as did one (3 per cent) after 18 months.
The observed behaviour and the subjects' descriptions of eating problems can serve as a basis for the development of criteria for general nursing diagnoses (Table 5).
27
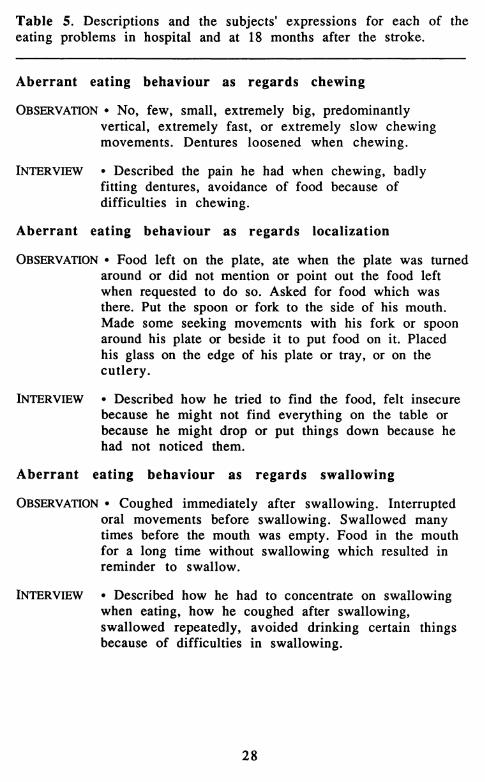
Table 5. Descriptions and the subjects' expressions for each of the eating problems in hospital and at 18 months after the stroke.
A berran t eating behaviour as regards chewing
Observ a tio n • No, few, small, extremely big, predominantlyvertical, extremely fast, or extremely slow chewing movements. Dentures loosened when chewing.
INTERVIEW • Described the pain he had when chewing, badly fitting dentures, avoidance of food because of difficulties in chewing.
A berran t eating behaviour as regards localization
Ob serv a tio n • Food left on the plate, ate when the plate was turned around or did not mention or point out the food left when requested to do so. Asked for food which was there. Put the spoon or fork to the side of his mouth. Made some seeking movements with his fork or spoon around his plate or beside it to put food on it. Placed his glass on the edge of his plate or tray, or on the cutlery.
In t e r v ie w • Described how he tried to find the food, felt insecure because he might not find everything on the table orbecause he might drop or put things down because hehad not noticed them.
A berran t eating behaviour as regards swallowing
Ob serv a tio n • Coughed immediately after swallowing. Interrupted oral movements before swallowing. Swallowed many times before the mouth was empty. Food in the mouth for a long time without swallowing which resulted in reminder to swallow.
In t e r v ie w • Described how he had to concentrate on swallowing when eating, how he coughed after swallowing, swallowed repeatedly, avoided drinking certain things because of difficulties in swallowing.
28

Table 5 cont.
Eating small amounts
Observ a tio n • Ate extremely small amounts (less than half aserving) for more than three days (after 18 months - less than before the stroke).
In t e r v ie w • Described how, as a result of poor appetite, he ate smaller amounts than before the stroke.
Hoarding of food in the mouth
OBSERVATION • Put in food although his mouth was already full.Food protruded from his mouth. Seldom emptied his mouth during the meal. Hoarded food in one or both of his cheeks during the meal. Food left in one or both cheeks after the meal.
INTERVIEW • Described how he rinsed his mouth regularly after meals because there was often food left in it.
Leakage of food from the mouth
Ob ser v a tio n • Food (liquids and/or solid food) dribbled out of his mouth when chewing or when swallowing, when opening his mouth for another fork or spoon with food and/or when talking.
INTERVIEW • Described how he frequently wiped his mouth, how his relatives looked at the leakage from his mouth and how they signalled non-verbally reminding him to wipe it.
Unawareness of eating problems
O bserv a tio n • Did not pay any attention to the problem while eating. Did not spontaneously mention his eating problem.
INTERVIEW • Denied the problem.
This table is also presented in Paper II (Table 2).
29

Nutritional status on admission, on discharge and 18 months after the stroke (II, III)The mean values for the circulating proteins were above the lower reference limits for males and females on admission, on discharge and after 18 months. Subnormal values were most common in plasma albumin. On admission, 16 per cent of the patients had a poor nutritional status. The corresponding figures on discharge and after 18 months were 23 and 11 per cent, respectively. Undernutrition on admission was associated with the female sex, high age and a history of atrial fibrillation. On discharge poor nutritional status was related to infections, the male sex, the intake of cardiovascular drugs and high age. The nine patients who developed poor nutritional status during their hospital stay were all males.
Relations between eating problems and nutritional status (II, III, IV)Of the 18 patients who had a poor nutritional status on discharge 15 had eating problems. The corresponding proportion of those who developed undernutrition in hospital was seven out of nine (III). In the group with a hospital stay of 21 days or more (n=32) 18 had a poor nutritional status at some time during the hospital stay. Of those 17 had eating problems. In a linear hypothesis programme the factors associated with undernutrition were low self-care performance, poor nutritional status on admission and male sex; factors of less importance were energy-containing intravenous infusions, high age, paresis in the right arm and eating problems (IV).
The four subjects with poor nutritional status after 18 months all had eating problems (II).
Effects of training the swallowing function (V, VI)Training was initiated and carried out in hospital. Between the training periods the patients trained at home. The total time for the patients’ hospital stays was 27 and 29 days, respectively. Both subjects have been eating normal food for 3 and 4.5 years after having started to eat normally again, one without any problems and the other still needing more time than usual for eating and with a habit of clearing his throat during eating.
30
DISCUSSION
Patient selectionThe distribution of the patients amongst the various diagnostic groups was comparable with other studies from Umeå (11), Söderhamn (7), and Stockholm (12). The patients in the present study were the youngest (by 1-2 years). The male/female ratio was similar to that in the Umeå study. With regard to distribution of diagnoses, sex and age, the studied group was similar to the other population-based groups. Thus the studied group could be regarded as representative of Swedish stroke patients with exception of patients with subarachnoid hemorrhage. The subgroups (II, III, IV) were selected from a representative sample and therefore with the same selection criteria, the results could be applicable to other stroke groups.
Methods used in descriptive studyAn inductive methodology was applied. No concepts of specific eating problems were formulated at the start of the study. The instruments for observing eating have not been used before. As data on eating problems were collected distinct concepts emerged and were labeled. This type of data analysis was repeated for each phase of the study to make sure that as many phenomena aspossible were included in the concepts. The concepts were relabelled but the new labels did not change the classification of the patients into the different problem-groups made previously. Sores in the mouth was never the only problem a patient had. Thereforethe fact that this phenomenon was regarded as an eating problemin Paper I and as a cause of eating problems in Paper II did not affect the estimation of the prevalence of eating problems.
Reduced independent eating was not a focus for observations to such an extent that it was possible to make descriptions and formulate a concept. Only 'assistance during meals' and 'assisted feeding' were recorded.
Nutritional assessments are dependent on the validity and theprecision of the indicators used. There is no universally accepted single variable that reflects the overall nutritional situation in a
31

patient. Moreover, reference intervals must be reliably defined as to sex, age and probably also ethnical background. In some previous investigations of nutritional status in patient samples, the delineation of 'normal' has relied on arbitrarily chosen limits, such as 80-120 per cent of population mean, set at 100 per cent (81). In this study, statistically defined limits for variables were used where such information was available. The anthropometric data as well as the laboratory reference data obtained in normal ageing Swedish populations and published in the last few years (82, 84) have facilitated the definitions of 'normal' with regard to sex, age and ethnic background. In view of the intricacies involved in each of the nutritional variables at least two of the six indicators should point in the same direction for a patient to be assigned to the group with poor nutritional status. Using this interpretation, it is possible that more subtle forms of undernutrition have not been recognized. Taking all these considerations in mind, it is evident that the nutritional categorization of an individual patient at a given point oftime should be taken as a crude estimate.
Methods used in case studiesThe oral apraxia test developed by DeRenzi and co-workers (34) was modified and has been used to assess the oral phase of swallowing (V, 92). It served this purpose very well. The test, of course, has to be evaluated in a larger sample of subjects.
The oral agnosia test for forms was developed in the research group (V) together with the dentist who was associated with the group. This test has not yet been validated.
The training was based on the results from the tests and the investigations. Papers V and VI are descriptions of only twopatients and a training programme for use in clinical practice would, of course, have to be based on more cases. A more exact description of the circumstances under which different treatmentscan be used is necessary.
The relationship aspect of nursing therapeutics was interpreted according to the Erikson theory (90). These interpretations seemed to fit in the cases studied. More studies are needed in order to elucidate the possibilities and limits of the interpretations.
32

R esultsIt was evident that eating problems were common during the acute phase of the disease. After 18 months most of the patients were aware of their eating difficulties and experienced them as problems. Three months after the stroke the investigation of patients with eating problems in hospital showed that 46 per cent of the problems remained. The corresponding figure was 43 per cent 18 months after the stroke (II). Thus the rate of recovery seemed to be greatest in the first few months after the onset of the disease.
When an eating problem was identified by the research nurse the patient was classified as having eating problems, if the problem lasted for more than one day and measures to treat it were taken. The measures were not reported. However, as measures were probably taken more intensively during the study than in ordinary clinical care this may have influenced the presented recovery from eating problems.
According to the model of diagnosing eating problems in stroke patients (Figure 1), the concepts of eating problems presented (Table 5) could be regarded as general nursing diagnoses. In the single subject studies (V, VI) it was possible to formulate specific nursing diagnoses based on tests and investigations of impairments.
The disabilities, impairments and types of diseases presented in Figure 3 have to be combined in order to form testable hypotheses. Aberrant eating behaviour as regards swallowing could for example be caused by impairment of pharyngeal muscular function, by impairment of sensory function - tactile sensibility (oral agnosia), by impairment of cerebral integration (e.g. oral apraxia) or by a combination of the above-mentioned impairments. Eating small amounts could be caused by impairment of sensory function such as reduced taste and smell or by impairment of mental performance including depression. Studies should be carried out to test these hypotheses. The specific nursing diagnosis connects and partly overlaps the medical symptom diagnosis.
Today validated tests and investigations of impairments after stroke are often lacking but badly needed in clinical practice (93).
33

Figure
3. M
odel for
diagnosing eating
problems
in stroke
patients. *
Adapted
from F
ugl-Meyer
and A
splund (6).
cpc/3V3cpcl
3CPCPCL
2 oCP Ä3 2-
CPp5*
CTQ
B ET° £3 p 00 o CP
oa
& a wCP O g . p 3 . c/3 R 33 Stew g oc» c 00 gB o p
or >g- ?CP
qp p
SL S. 5 .00
o3
po* P °0° 3 ^ oK-. CC» 3
• •S
r*-CP /—*s
<' •3 o a 3 C«* C/33CP CPNI f* 3CPM
O* CP33 CP P 3 C/3rt' a* O P * OP N| r+ Ni
P C P v:N- CP Ni CA*3CP N-. X/i
CP CP 3*N»o 4
3f*CPCP3 CL C/3 3O
N| 00 C/3 CP 3 e>*3p
N|p a 1H** CP3
O O*33 o*OCP 3
CP p\*J «-N*"*•NI 3CP 0x3
00
«CL
p 3 • tr1S c ^ 3o 2 g ^S.v3 2. 3.O 3 P 33 » r g
CP os-s s„ E.3 o2 p ^ P 3C/3 S O ^£p>1
CP c HH ^ 3 i o CP Sg cr > S ’ g . »> § 3 g“ e« « V M i Po o
cr p
00« 2.
d O d cpET. R- s . 3 Ni *o o <y er cp3 <— 3 O P CT*
& 3too ^p o CP gl
► ÿ g i >o S O-
CPcr 3 2
s 2 o - £L .*3 3 ra* ® £»C/3 O O*
C/3
£ Eî>O-3* ^ O 2 oo 3-
2 ^ CP NiCP oCL CT
cT3
Ocr
CPCL
a*CPcrp<o*3
C/3
3
O3
pcr
CPC/3
33p (Ni‘3CP3
H
CP CPPCPC/3
'o ns §a 50 3 cp
3cTc/3
34

The proportion of patients with undernutrition on admission was somewhat lower than in comparable studies (III, 49, 51).Undernutrition on discharge was also lower than that presented in studies of patients in a surgical ward (52) and in psychogeriatric wards (54, 55). In the patient group studied for three weeks thenumber of patients with undernutrition increased from admission to the end of the three weeks. Patients at risk of developing undernutrition during hospitalization were identified. Routine nutritional treatment in the ward together with the measures totreat eating problems carried out during this study were thus insufficient to entirely prevent the development of undernutrition.
The study showed that factors other than eating problems were im portant for developing undernutrition (IV). The measures performed to alleviate eating problems may have reduced thepossibilities to discover a relationship between eating problems and undernutrition. But for ethical and human reasons it was neither reasonable nor possible to perform the study without attempting to help the patients with eating problems.
GENERAL DISCUSSION
Every second stroke patient suffers from eating problems which in many cases will persist 18 months after the stroke (I, II).
Different types of eating problems were identified and described (I, II). The descriptions were developed throughout the study and eventually came to be regarded as general diagnoses concerning eating. This is seen as the first step towards nursing diagnoses that can be used as the basis for the development of specific therapeutics for eating problems.
The general diagnosis gives a detailed description of the eating disability but does not connect it to impairments and/or brain damage.
In the two case studies the diagnoses were developed further to include assessments of impairments and also in one case (VI) localization of the brain damage. These specific diagnoses made it
35

possible to choose specific treatments such as training the performance of a certain oral movement.
The case studies also lead to the development of a method for interpreting the patient’s existential situation according to the Erikson theory of the 'eight stages of man' (90). This diagnostic procedure seems to be important for the implementation of the treatment planned. It is in agreement with the notation by Carnevali (73) that nursing diagnoses should connect the patient’s daily living with his pathology and its treatment as well as his age- related biological status and developmental tasks.
Therefore it is not possible to draw a definitive conclusion about the connection between eating problems and nutrition per se. However, the studies did show that every fifth patient was undernourished. This problem, of course, has to be considered seriously and measures taken to reduce it.
Knowledge of the prognoses for specific eating problems is essential in the planning of treatment (73). The longitudinal study of the course of eating problems treated only by unsystematic measures showed that most problems persisted after 18 months. Both the single subject studies showed that the prognosis for treatment of dysphagia was very good although the patients had had their problems for 1 1/2 and 3 years respectively. Thissuggestion is in agreement with the results from other treatment evaluations (45).
It is essential that further research is conducted to develop specific diagnoses and elucidate the prognosis for different eating problems related to specific impairments. The localization of the brain damage might also turn out to be an important prognostic factor.
The evaluation of nutritional status in stroke patients (II, IV) suggested that the effects of eating problems on nutrition were modest during the acute phase. This could be influenced by the fact that nutritional supply was provided during the ward stay.
As it may become evident that not all types of eating problems can be successfully treated research should also be aimed at prevention of consequences/handicap (other than undernutrition) caused by eating problems.
36

CONCLUSIONS
The main findings in the studies presented were:
• eating problems occur in half of randomly sampled stroke patients during the acute phase of the disease.
• eating problems remain and are still prevalent long after the cerebrovascular accident.
• identified eating problems are:aberrant eating behaviour as regards chewingaberrant eating behaviour as regards localizationaberrant eating behaviour as regards swallowingeating small amounts hoarding food in the mouth leakage of food from the mouth
• among patients with eating problems, a majority are unaware of their eating problems during the acute phase but there is a time- dependent improvement in awareness.
• undernutrition is common among stroke patients on admission to hospital and the prevalence appears to increase during the hospital stay.
• eating problems do not seem to be a major contributor to shortterm changes in the nutritional status during the acute phase of stroke.
• it is possible to train severe dysphagia late after a stroke
37

ACKNOWLEDGEMENTS
This study was carried out at the Department of Advanced Nursing and Medicine. I wish to thank everyone who in any way has contributed in this study and those who in one way or another have given me valuable help.
I wish to express my sincere gratitude to Professor Astrid Norberg for introducing me to the world of nursing research, for her enthusiasm and encouraging support and for her constructive criticism during these years.
I also wish to express my sincere thanks to Associate Professor Kjell Asplund for scientific advice, encouragement and stimulating criticism.
Special thanks go to:
Professor P. O. Wester for encouragement and support.
Mrs. Eva Lindmark for skilful data collecting.
Irina Alafuzoff, Dr Med Sci, for her analyses of the plasma prealbum in.
Associate Professor Emeritus Doris Carnevali, Seattle, for advice and support in the work with nursing diagnoses.
Professor Thorild Ericsson for stimulating discussions.
Sture Eriksson, Dr Med Sci, for statistical advice.
Mrs. Birgitta Hammarström for never ending patience in computer work.
Ingegerd Johansson, DDS, for computer assistance in the estimation of nutritional intake.
Mrs. Ann-Sofie Kärreby, for assessment of nutritional intake.
Mats Ryberg, DDS, for fruitful discussions and advice in oral investigations.
Mrs. Åsa Sundh, Mrs. Patricia Shrimpton and Fil lie Robert Elston for excellent linguistic revisions.
38

Ove Söderberg, Dr Med Sci, and Dr. Britt-Inger Wenngren for cooperation and support.
The stroke nurses Kristina Östman, Margareta Engde and Margot Helgesson and Head nurse Barbro Lindgren for their interest, support and co-operation.
To the entire staff of the stroke unit for their support and cooperation.
The Nursing Research Group in Umeå for critical discussions and support.
And last but not least to my family, Sören, Mikael, Robert and Maria for their constant support and for helping me to keep the balance between work and other parts of life.
This project was supported by grants from Umeå University, grant No. 7342 from the Swedish Medical Research Council to Karin Axelsson, and grant No. to 6260 to Astrid Norberg, grant No. 81/99 from the Delegation for Social Research, Ministry of Health and Social Affairs, grant No. 82/65 from the Bank of Sweden Tercentenary Foundation, King Gustav V’s and Queen Victoria's Foundation, the Joint Committee of the Northern Health Region of Sweden, Västerbotten County Council, Roussel Nordiska AB, Swedish Nutrition Foundation and the Foundation of 'Gamla Tjänarinnor’.
39

REFERENCES
1. Lytle LD. Control of eating behavior. In: Wurtman RJ,Wurtman JJ, eds. Nutrition and the brain. Voi 2. New York: Raven Press, 1977:1-145.
2. Logue AW. The psychology of eating and drinking. New York: WH Freeman and Company, 1986.
3. Schiffman SS. Taste and smell in disease. N Engl J Med 1983;308:1337-43.
4. Axelsson K, Norberg A, Asplund K. A model for analysis of eating problems. Applied to hospitalised patients with cerebrovascular disease. (Swe). Socialmedicinsk tidskrift 1984;61:350-5.
5. Aho K, Harmsen P, Hatano S, Marquardsen J, Smirnov VE, Strasser T. Cerebrovascular disease in the community: results of a WHO collaborative study. Bull WHO 1980;58:113-30.
6. Fugl-Meyer AR, Asplund K. Cerebrovascular diseases. (Chapt 23). In: Höök O, ed. Medical rehabilitation (Swe). Stockholm: Norstedts, in press.
7. Terént A. A prospective epidemiological survey of cerebrovascular disease in a Swedish community. Ups J Med Sci 1979;84:235-46.
8. Wester PO. Epidemiological aspects and experiences of stroke units. In: Cerebrovascular diseases - care during the acute phase (Swe). Stockholm: SPRI publication, 1984;009:3-8.
9. Strand T. Stroke. Patient characteristics, efficacy of a stroke unit and evaluation of hemodilution therapy. Umeå: Umeå University Medical Dissertations, New series No 163, 1986.
10. Strand T, Asplund K, Eriksson S, Hägg E, Lithner F, Wester PO.A non-intensive stroke unit reduces functional disability and the need for long-term hospitalization. Stroke 1985;16:29-34.
11. Eriksson S, Asplund K, Hägg E, Lithner F, Strand T, Wester PO. Clinical profiles of cerebrovascular disorders in a population- based patient sample. J Chron Dis 1987;40:1025-32.
12. von Arbin M, Britton M, de Faire U, Helmers C, Miah K, Murray V. A study of stroke patients treated in a non-intensive stroke unit or in general medical wards. Acta Med Scand 1980;208:81-5.
13. Halligan F, Hunt LW. Frank’s story. Can Nurse 1979;75:26-31.14. Åhgren CE. The paralysis. Diary notes (Swe). Växjö: LIC
publication and Federation of Swedish County Councils, 1986.15. Guentz S, Navales RD. New approaches to the nursing care of
the stroke patient. Clin Orthop 1978;131:90-6.
40

16. Wainwright H. Feeding problems in elderly disabled patients. Nurs Times 1978;74:542-3.
17. Stillman MJ. Stroke! How to care for a recovering patient. RN 1979;42:49-56, 94.
18. Dudas S. Nursing diagnoses and interventions for the rehabilitation of the stroke patient. Nurs Clin North Am 1986;21:345-57.
19. Myco F. Nursing care of the hemiplegic stroke patient. London: Harper & Row, Publishers, 1983.
20. Breitbach W. Nursing care of the patient with cerebrovascular disease. J Pract Nurs 1980;30:32-3, 39.
21. Hart G. Strokes causing left vs. right hemiplegia: Different effects and nursing implications. Geriatr Nurs 1983;4:39-43.
22. Söder M. ed. Impairment, disability and handicap. Report from a workshop on the WHO-terminology and manual for classification of impairments, disabilities and handicap in Stockholm, 1 October 1984. Geneva: WHO.
23. Wade DT, Hewer RL. Motor loss and swallowing difficulty after stroke: frequency, recovery, and prognosis. Acta Neurol Scand 1987;76:50-4.
24. Currier RD, Giles CL, DeJong RN. Some comments on Wallenberg's lateral medullary syndrome. Neurology 1961;11:778-91.
25. Peterman AF, Siekert RG. The lateral medullary (Wallenberg) syndrome: clinical features and prognosis. Med Clin N Amer 1960;44:887-96.
26. Gordon C, Hewer RL, Wade, DT. Dysphagia in acute stroke.Br Med J 1987;295:411-4.
27. Veis SL, Logemann JA. Swallowing disorders in persons with cerebrovascular accident. Arch Phys Med Rehabil 1985;66:372-5.
28. Katz S, Akpom CA. A measure of primary sociobiological functions. Int J Health Serv 1976;6:493-507.
29. Hamrin E, Wohlin A. Evaluation of the functional capacity of stroke patients through an activity index. Scand J Rehab Med 1982;14:93-100.
30. Bruett TL, Overs RP. A critical review of 12 ADL scales. J Am Phys Ther Ass 1969;49:857-62.
31. Lange C, Svendsen L. The stroke patient's eating and drinking problems (I) (Dan). Klinisk Sygepleje 1987;(2):2-8.
32. Silverman EH, Elfant IL. Dysphagia: an evaluation and treatment program for the adult. Am J Occup Ther 1979;33:382-92.
41

33. Stratton M. Behaviorial assessment scale of oral functions in feeding. Am J Occup Ther 1981;35:719-21.
34. De Renzi E, Pieczuro A, Vignolo LA. Oral apraxia and aphasia. Cortex 1966;2:50-73.
35. Landt H. Oral recognition of forms and oral muscular coordination ability in dentulous subjects of various ages. Laboratory cross-sectional studies with special reference to the effects of learning. Swed Dent J 1974;67, Suppl 5.
36. Yen PK. Special help for eating problems. Geriatr Nurs 1983;4:257-8.
37. Larsen GL. Rehabilitating dysphagia: mechanica, paralytica, pseudobulbar. J Neurosurg Nurs 1976;8:14-17.
38. Hargrove R. Feeding the severely dysphagic patient. J Neurosurg Nurs 1980;12:102-7.
39. Buckley JE, Addicks CL, Maniglia J. Feeding patients with dysphagia. Nurs Forum 1976;15:69-85.
40. Lange C, Svendsen L. The stroke patient's eating and drinking problems (II) (Dan). Klinisk Sygepleje 1987;(3):15-20.
41. Cockcroft G, Ray M. Feeding problems in stroke. Nurs Mirror 1985;160:26-9.
42. Griffin KM. Swallowing training for dysphagic patients. Arch Phys Med Rehabil 1974;55:467-70.
43. Larsen GL. Rehabilitation for dysphagia paralytica. J Speech Hear Disord 1972;37:187-94.
44. Larsen GL. Conservative management for incomplete dysphagia paralytica. Arch Phys Med Rehabil 1973;54:180-5.
45. Heimlich HJ. Rehabilitation of swallowing after stroke. Ann Otol Rhinol Laryngol 1983;92:357-9.
46. Selley WG. Swallowing difficulties in stroke patients: a new treatment. Age Ageing 1985;14:361-5.
47. Calcaterra TC, Kadell BM, Ward PH. Dysphagia secondary to cricopharyngeal muscle dysfunction. Arch Otolaryngol 1975; 101:726-9.
48. Warnold I, Falkheden T, Hultén B, Isaksson B. Energy intake and expenditure in selected groups of hospital patients. Am J Clin Nutr 1978;31:742-9.
49. Albiin N, Asplund K, Bjermer L. Nutritional status of medical patients on emergency admission to hospital. Acta Med Scand 1982;212:151-6.
50. Linn BS, Jensen J. Malnutrition and immunocompetence in older and younger outpatients. South Med J 1984;77:1098- 102.
42

51. Sandström B, Alhaug J, Einarsdottir K, Simpura EM, Isaksson B. Nutritional status, energy and protein intake in general medical patients in three Nordic hospitals. Hum Nutr Appi Nutr 1985;39A:87-94.
52. Symreng T, Anderberg B, Kågedal B, Norr A, Schildt B, SjödahlR. Nutritional assessment and clinical course in 112 electivesurgical patients. Acta Chir Scand 1983;149:657-62.
53. Sandahl C, Rönnlund U, Hardell L. Nutritional status in patients with radiotherapy treatment of head-and-neck cancer (Swe). Näringsforskning 1984;28:14-20.
54. Asplund K, Normark M, Petterson V. Nutritional assessment ofpsychogeriatric patients. Age Ageing 1981;10:87-94.
55. Sandman PO, Adolfsson R, Nygren C, Hallmans G, Winblad B. Nutritional status and dietary intake in institutionalized patients with Alzheimer's disease and multiinfarct dementia. J Am Geriatr Soc 1987;35:31-8.
56. Lawrence W Jr. Effects of cancer on nutrition. Impaired organ system effects. Cancer 1979;43:2020-9.
57. Dreizen S. Clinical manifestations of malnutrition. Oral and cutaneous lesions appearing late in life may be the telltale signs of long-standing nutritional deficiency. Geriatrics 1974;29:97-103.
58. Ek AC. Prediction of pressure sore development. In: Ek AC. Pressure sores - a problem in nursing care. Linköping: Linköping University Medical Dissertation, No 195, 1985, IV:1-17.
59. Chandra RK. Nutrition, immunity, and infection: Present knowledge and future directions. Lancet 1983;1:688-91.
60. Chandra RK, Baker M, Kumar V. Body composition, albumin levels, and delayed cutaneous cell-mediated immunity. Nutr Res 1985;5:679-84.
61. Gorsky RD, Calloway DH. Activity pattern changes with decreases in food energy intake. Hum Biol 1983; 55:577-86.
62. Goodwin JS, Goodwin JM, Garry PJ. Association between nutritional status and cognitive functioning in a healthy elderly population. JAMA 1983;249:2917-21.
63. Brodén G, Bark S, Nordenvall B, Backman L. Nutritional assessment and postoperative morbidity. A prospective study in 286 consecutive surgical patients. Acta Chir Scand suppl 1984;520:27-32.
64. Nixon DW, Heymsfield SB, Cohen AE et al. Protein-calorie under-nutrition in hospitalized cancer patients. Am J Med 1980;68:683-90.
43
65. Isaksson B. How to avoid malnutrition during hospitalization? Hum Nutr Appi Nutr 1982;36A:367-73.
66. Isaksson B. Management and organization of modern hospital nutrition care. Bibl Nutr Dieta 1985;35:95-105.
67. Iyer PW, Taptich BJ, Bernocchi-Losey D. Nursing process and nursing diagnosis. Philadelphia: WB Saunders Company, 1986.
68. Axelsson K, Norberg A, Asplund K. Nursing diagnoses applied to eating problems in patients with cerebrovascular disease (Swe). Vård i Norden 1986;6:306-10.
69. McLane AM. ed. Classification of nursing diagnoses.Proceedings of the seventh conference. North American Nursing Diagnosis Association. St. Louis: The CV Mosby Company, 1987.
70. Tilton CN, Maloof M. Diagnosing the problems in stroke. Am J Nurs 1982;82:596-601.
71. Carpenito LJ. Nursing diagnosis. Application to clinical practice. Philadelphia: JB Lippincott Company, 1983.
72. Campbell C. Nursing diagnosis and intervention in nursing practice. New York: Wiley & Sons, 1984.
73. Carnevali DL, Mitchell PH, Woods NF, Tanner CA. Diagnostic reasoning in nursing. Philadelphia: JB Lippincott Company, 1984.
74. Carnevali DL. Nursing care planning: diagnosis and management. Philadelphia: JB Lippincott Company, 1983.
75. World Health Organization. International classification of impairments, disabilities, and handicaps. A manual of classification relating to the consequences of disease. Geneva: World Health Organization, 1980.
76. The National Swedish Board of Health and Welfare. Classification of diseases 1987. Systematic list. Swedish version of International Classification of Diseases, Ninth Revision (ICD-9) (Swe). Stockholm: Liber, 1986.
77. Norberg A, Athlin E, Winblad B. A model for the assessment of eating problems in patients with Parkinson's disease. J Adv Nurs 1987;12:473-81.
78. Axelsson K, Norberg A, Asplund K. Eating problems after stroke - occurrence and course. In: Nursing research - does it make a difference? Proceedings, 2nd open conference London, 10th - 13th April, 1984. 1985:381-7.
79. Bengtsson C, Hultén B, Larsson B, Noppa H, Steen B, Warnold I. New weight-height tables in Swedish middle-aged and elderly men and women (Swe). Läkartidningen 1981;78:3152-4.
44

80. Edwards DAW, Hammond WH, Healy MJR, Tanner JM, Whitehouse RH. Design and accuracy of calipers for measuring subcutaneous tissue thickness. Br J Nutr 1955;9:133-43.
81. Blackburn GL, Benotti PN, Bistrian BR et al. Nutritional assessment and treatment of hospital malnutrition. Infusionsther 1979;6:238-50.
82. Symreng T. Arm anthropometry in a large reference population and in surgical patients. Hum Nutr Clin Nutr 1982;1:211-19.
83. Laurell CB. Quantitative estimation of proteins by electrophoresis in agarose gel containing antibodies. Anal Biochem 1966;15:45-52.
84. Österlind PO, Alafuzoff I, Löfgren AC et al. Blood components in an elderly population. Gerontology 1984;30:247-52.
85. Nie NH, Hull CH, Jenkins JG, Steinbrenner K, Bent DH. SPSS. Statistical package for the social sciences. Second edition. New York: McGraw-Hill Book Company, 1975.
86. Wilkinson L. SYSTAT: The system for statistics. Evanston, IL: SYSTAT Inc, 1986.
87. Barlow DH, Hersen M. Single case experimental designs. Strategies for studying behavior change. New York: Pergamon press, 1984.
88. Bimbrauer JS, Peterson CR, Solnick JV. Design and interpretation of studies of single subjects. Am J Ment Defic 1974;79:191-203.
89. Watzlawick P, Bavelas JB, Jackson DD. Pragmatics of human communication. A study of interactional patterns, pathologies, and paradoxes. New York: WW Norton & Company, 1967.
90. Erikson EH. The life cycle completed. A review. New York:W.W. Norton & Company, 1982.
91. Heimlich HJ, O'Connor TW. Relearning the swallowing process. Ann Otol 1979;88:794-7.
92. Athlin E, Norberg A, Axelsson K, Möller A, Nordström G. Aberrant eating behaviour in elderly Parkinsonian patients with and without dementia. Analysis of video-recorded meals. M anuscript.
93. Asplund K. Clinimetrics in stroke research. Stroke 1987;18:528-530.
45



















